Embed Size (px)
DESCRIPTION
Back Pain . Definitions . The term ‘acute’ is used to describe pain that has been present for less than three months it does not refer to the severity or quality of pain. Chronic pain is pain that has been present for at least three months . - PowerPoint PPT Presentation
Citation preview

BACK PAIN

DEFINITIONS The term ‘acute’ is used to describe pain that has been
present for less than three months it does not refer to the severity or quality of pain.
Chronic pain is pain that has been present for at least three months .
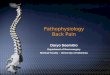
Definition of thoracic spinal pain developed by the International Association for the Study of Pain:
• Pain perceived anywhere in the region bounded superiorly by a transverse line through the tip of the spinous process of T1, inferiorly by a transverse line through the tip of the spinous process of T12, and laterally by vertical lines tangential to the most lateral margins of the erector spinae muscles. This area can be divided into upper, middle and lower thirds.
• Pain felt lateral to this area is defined as posterior chest wall pain, and does not constitute thoracic spinal pain.

EPIDEMIOLOGY Lifetime incidence of back pain exceeds 70% in most
industrialized nations. Back pain occurs at all ages and is the most common reason for work disability in patients younger than 40 years.
IncidenceAbout one half of the population will report back pain
over 12 months.Prevalence15,000 to 20,000 per 100,000 persons is the average 1-
year prevalence.

CASE STUDYPaul is a 44-year-old man presenting at your surgery
with a 3 to 4-week history of pain without a history of significant injury. He states his pain is in his lower back and radiating across his lower back and into the top of his buttocks. There is no pain radiating down Paul’s legs.
Paul describes his pain as worse by the end of the day, and exacerbated by sitting for long periods. Paul thinks his pain started after a game of tennis…

HISTORY AND EXAMINATION Undertake a thorough history and physical examination
to assess for the presence of serious clinical conditions (red and yellow flags)



RED AND YELLOW FLAGS More red flag tables in the document. (from John Murtagh’s
General Practice, 4th edn.) Yellow flags are pyschosocial factors shown to be indicative of
long-term chronicity and disability:• A negative attitude that back pain is harmful or potentially
severely disabling• Fear avoidance behaviour and reduced activity levels• An expectation that passive, rather than active, treatment
will be beneficial• A tendency to depression, low morale, and social withdrawal• Social or financial problems

MANAGEMENT Advise to resume normal activities as soon as possible
and to “let pain be their guide” as to the appropriate level of activity. Explain that this will help to relieve symptoms and reduce the risk of chronic disability.
Encourage a prompt return to work—although manual handling may be an issue, and training in lifting may be advisable. Discuss whether you might need to liaise with their workplace.



THERAPEUTIC GUIDELINES Analgesics and NSAIDs in acute exacerbations of low back pain can be
useful to facilitate maintenance of activity rather than simply to relieve pain. The drug used should give adequate relief for this purpose without adverse effects.
Patients should be reassured that some pain with exercise can be expected and that this does not imply continuing damage.
1) paracetamol 1 g orally, 4- to 6-hourly up to a maximum dose of 4 g dailyor paracetamol modified-release 1.33 g orally, 8-hourly AND/OR 2) an NSAID orally The goal of treatment is reduction rather than complete abolition
of pain, and this must be clearly explained to the patient.

TO IMAGE OR NOT? Imaging tests are not recommended in acute non-
specific low back pain in the absence of clinical ‘red flags’. (Level III-2 evidence).
The majority of imaging tests for acute low back pain presentations find no abnormalities, or only minor changes. Imaging findings are not strongly associated with acute low back pain symptoms.
Unnecessary x-rays and CTs subject the patient to risks of radiation exposure.
The Australian guideline Evidence-Based Management of Acute Musculoskeletal Pain recommends against routine use of plain x-rays or other imaging tests such as magnetic resonance imaging (MRI) or computerised tomography (CT) in the absence of red flags in non-specific low back pain of less than 12 weeks duration. This guideline states that x-rays are unhelpful in identifying the cause of pain and do not contribute to greater improvement in a patient’s physical function, pain or disability.

PATIENTS’ WANTSConsumers expect to know the cause of their pain and
receive advice on how best to deal with itKendrick et al, BMJ 2001;322:400-5• Providing an X-ray of the lumbar spine did not improve
consumer satisfaction in the short term (at 3 months), but…at 9 months, participants who received an X-ray were significantly more satisfied with the care they received at their most recent consultation.
Deyo RA and Diehl AK Spine 1986;11:28-30• Patient satisfaction seems to be linked to the provision of
good information, and adequate explanation of the problem and advice on how to manage it.
• Patients who were not satisfied with the information provided were more likely to believe that they should have had more tests done.

INVESTIGATIONS Other investigations to consider are: • FBE (full blood examination) and ESR (erythrocyte sedimentation
rate. It is a test that indirectly measures how much inflammation is in the body, very high levels occur with multiply myeloma)
• serum alkaline phosphatase• serum electrophoresis for multiple myeloma• Bence-Jones protein analysis• Brucella agglutination test • blood culture for pyogenic infection and bacterial endocarditis• tuberculosis studies• HLA-B27 antigen for spondyloarthropathies • ECG or ECG stress tests (suspected angina)• gastroscopy or barium studies (peptic ulcer)• MRI


REFERENCES References: http://www.nhmrc.gov.au/publications/synopses/cp94syn.htm
NHRMC Evidence-based management of acute musculoskeletal pain
Back Pain: Medical Topics: First Consult John Murtagh’s General Practice, 4th ed. Low back pain and
thoracic back pain About ESR:
http://www.nlm.nih.gov/medlineplus/ency/article/003638.htm
http://www.bmj.com/content/326/7388/535.full Chronic back pain: 10 minute consult
www.bmj.com/content/327/7414/541.full.pdf Acute back pain: 10 minute consult
NPS lecture on Managing acute low back pain in primary care





















![Back Talk - Back Pain Rescue[1]](https://img.pdfslide.net/doc/110x75/577d35821a28ab3a6b90a19c/back-talk-back-pain-rescue1.jpg)




