Embed Size (px)
Citation preview
8/8/2019 Back to School Package Forms
http://slidepdf.com/reader/full/back-to-school-package-forms 1/7
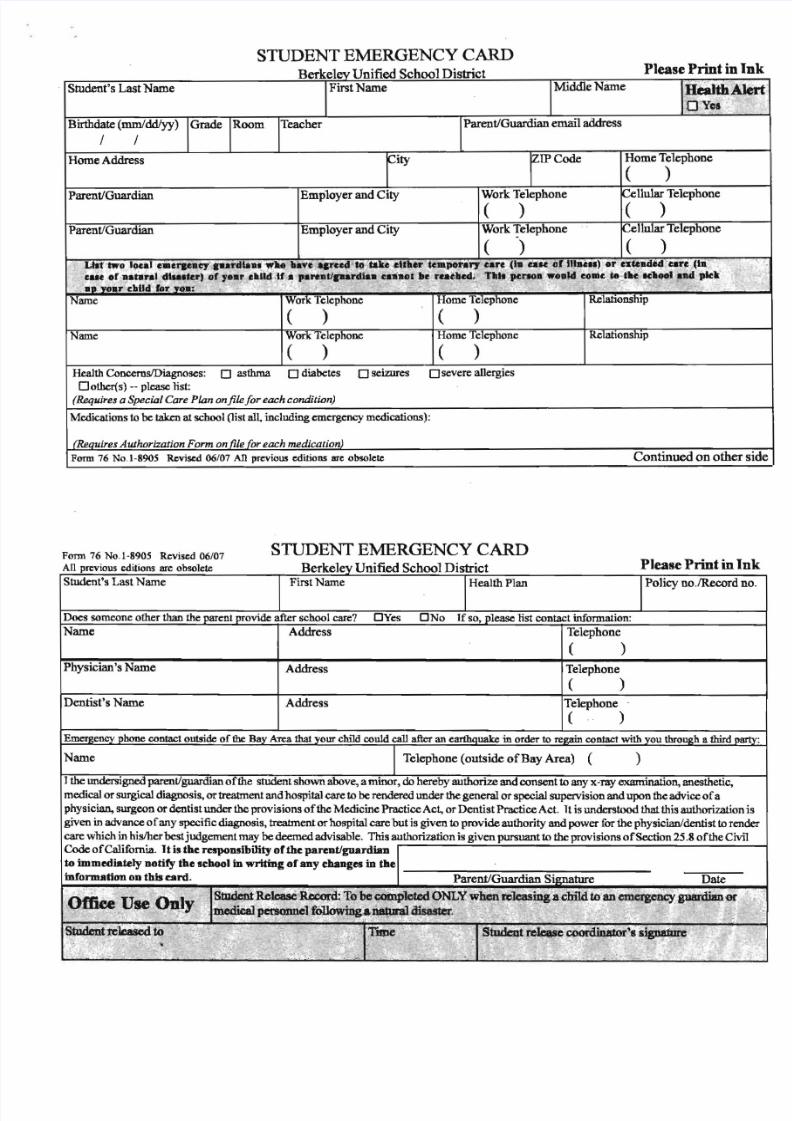
STUDENT EMERGENCY CARDPlease Print in IB k 1 U 'fied Sch ID ' tr ic tr e e y m 0 0 IS
Student'S Last Name First Name Middle Name Helalth'Al<n Y ~ f:
Birthdate (mmJddIyy) Grade Room Teacher Parent/Guardian ematl address
/ /
Home Address City r IP Code Home Telephone
( )Parent/Guardian Employer and City Work Telephone Cellular Telephone
( ) ( )Parent/Guardian Employer and City Work Telephone ~ e n u 1 a rTelephone
( ) ( )~ q " olocal ._ e l ' l e a n ' i a . l ' d l a a " ~ l l 4 I haveqrced t ~' ;~ e" t l t " ' e rt u I ~ " ' r ycar. · (la calC .of n h U ~ )OJ: e x t c a d * d~~ e , ( l ~·. .ca. . . r.atar.1 di . . . ter} 0' y.ar cllUd 'ln '" pareatlpardlaa . a . n t l I e' 1 ' c a t " ' ~, TII . 'Wnoa :wo.,1d e o ~ c t e} ' c 1C1i1tOIa.d pte\: L .. . y o . r· ~ J a l l df. r Yoa: . . . . : ,;" . . ' . , ' ".-; '.. ~ " •
Name Work Telephone Home Telephone Re1ationship
( ) ( )Name Work Telephone Home Telephone Re1ationship
( ) ( )
Health ConcernslDiagnoses: o asthma o diabetes o seizures o severe allergiesOother(s) -- please list:
(Requires a Special Care Plan onfilefor each condition)
Medications to be taken at school (list all, including emergency medications):
(R£Quires AuJhorization Fonn on file (or each medication)Form 76 No .1-8905 Revised 06/07 An previous editions are obsolete Continued on other s
STUDENT EMERGENCY CARDFonn 76 No. 1-8905 Revised 06/07
An previous editions are obsolete B k 1 U 'fied S h J D' Please Print in Inr ee y m c 0 0 IstriCtStudent's Last Name First Name Health Plan Policy no ,!Record no.
Does someone other than the parent provide after school care? DYes DNo If so, please list contact information:Name Address Telephone
( )Pbysician's Name Address Telephone
( )Dentist 's Name Address Telephone
( )~ e n c yphone contact outside of the Bay Area that your child could ca1l after an earthquake in order to ~ contact with you t h r o ~ hIi thirdJlar
Name ~ Telephone (outside o f Ba y Area) ( )
J the tmdersigned parent/guardian of the student shown above, a minor, do hereby authorize and consent to any x-ray examination, anesthetic,medical or surgical diagnosis, or treatment and hospital care to be rendered tmder the general or special supervision and upon the advire o f aphysician, surgeon or ~ t i s tunder the provisions o f the Medicine Practire Act, or Dentist Practire Act. T is understood that this authorizationgiven in advanre o f an y specificdiagnosis, treatment or hospital care bu t is given to provide authority an d power for th e physician/dentist to rendcare which in hislher best judgement may be deemed advisable. This authorization is given pursuant to the provisions of Section 25.8 of the CivIlCode ofCalifomia. I t is th e responsibility of th e pareotlguardiaDto immediately notify the school in writing of an y changes in th ein fOl" l lUl t ion 0 0 this tard, Parent/Guardian Signature Date
,Office ,Use 01\1y ._~ t u d e n t R e ~ b c o t d :To be cOlllpleted ONLY w1ren~ 1 c a s.i D g a c b t 1 dtaan eincrgency.guai"dian«~ p e t s o n n e l f ~;t 1 a 1 U r a 1 C J i s a s t e r, . ~ } : . ~ .' , . "
, , "". . .. ., ' ~ . . . . . .. • .' 1 . I . ' ~ ,
S ~ t n : ~'i o t·L .." tJf1e ' . v ~ ,r e k i l s ~~ r ' 8sigliaime~£ t f ..
. < ~ " ".. .' , ~ . ", ~ . ,.,,' . " ~ : . . . , , ~ <)
'M . ' ' ..,; . , . , , - ".. .. . "0 •• ;.:
8/8/2019 Back to School Package Forms
http://slidepdf.com/reader/full/back-to-school-package-forms 2/7
------------------------ - - - - -
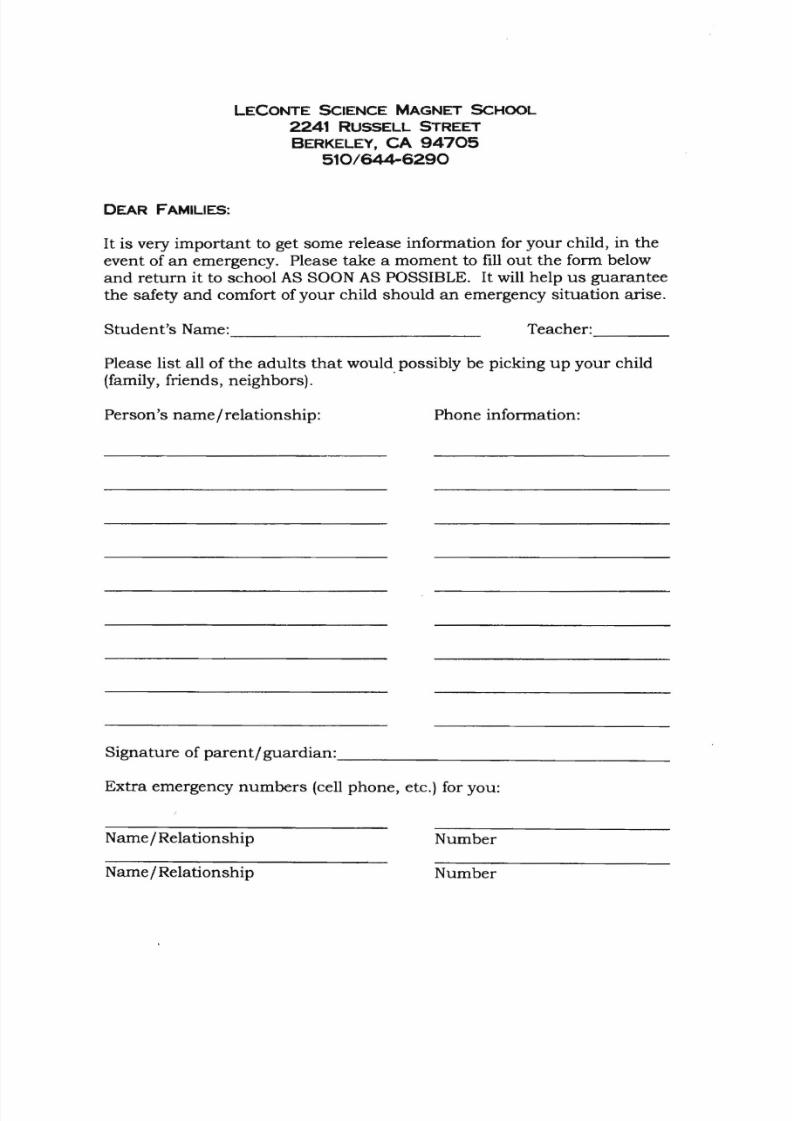
LECONTE SCIENCE MAGNET SCHOOL 2 2 4 1 RUSSELL STREET BERKELEY, C A 9 4 7 0 5
5 1 0 / 6 4 4 - 6 2 9 0
DEAR FAMILIES:
It is very important to get some release information for your child, in theevent of an emergency. Please take a moment to fill out the form belowand re turn i t to school AS SOON AS POSSIBLE. I t will help u s guaranteethe safety and comfort of your child should an emergency si tuation arise.
Student 's Name: Teacher:
Please list al l of the adul ts that would possibly be picking up your child(family, friends, neighbors). .
Person's name/relat ionship: Phone information:
Signature of paren t i guardian: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ ___
Extra emergency numbers (cell phone, etc.) for you:
Name / Relationship Number
Name / Relationship Number
8/8/2019 Back to School Package Forms
http://slidepdf.com/reader/full/back-to-school-package-forms 3/7
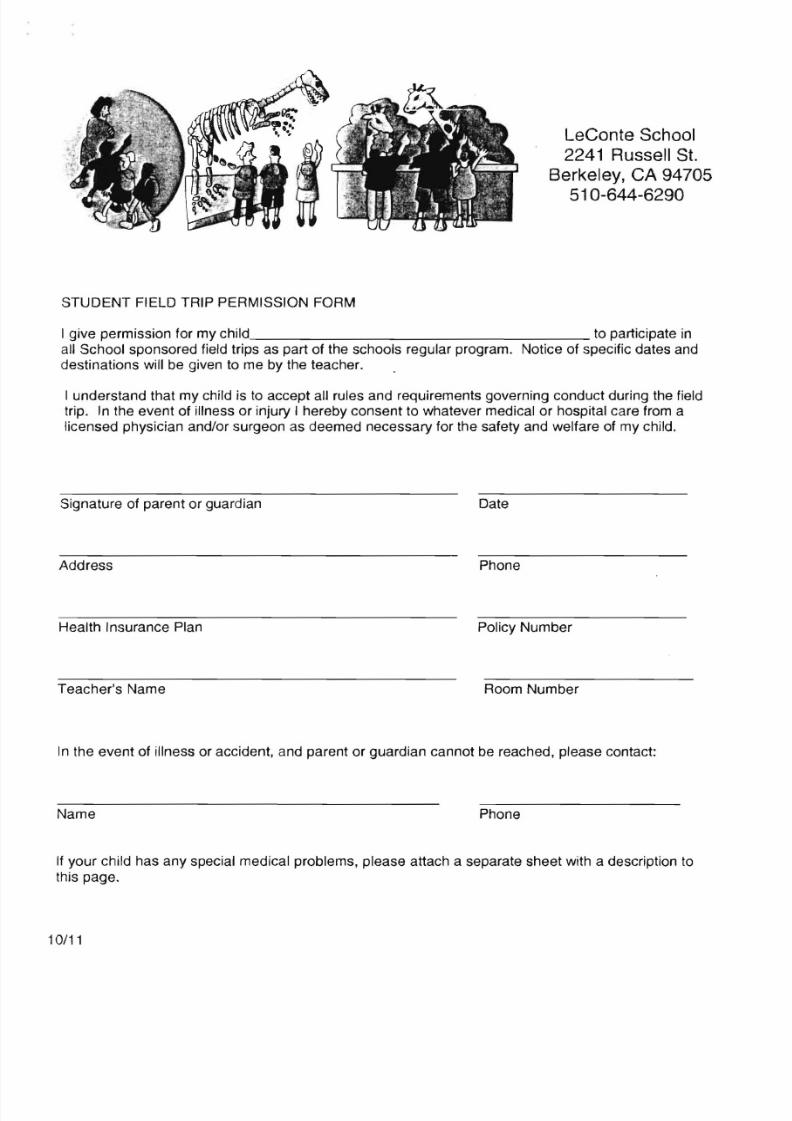
LeConte School2241 Russell St.
Berkeley, CA 9470551 0-644-6290
STUDENT FIELD TRIP PERMISSION FORM
I give permission for my child to participate in
all School sponsored field trips as part of the schools regular program. Notice of specific dates anddestinations will be given to me by the teacher.
I understand that my child is to accept all rules and requirements governing conduct during the fieldtrip. In the event of illness or injury I hereby consent to whatever medical or hospital care from alicensed physician and/or surgeon as deemed necessary for the safety and welfare of my child.
Signature of parent or guardian Date
Address Phone
Health Insurance Plan Policy Number
Teacher's Name Room Number
In the event of illness or accident, and parent or guardian cannot be reached, please contact:
Name Phone
If your child has any special medical problems, please attach a separate sheet with a description tothis page.
10/11
8/8/2019 Back to School Package Forms
http://slidepdf.com/reader/full/back-to-school-package-forms 4/7
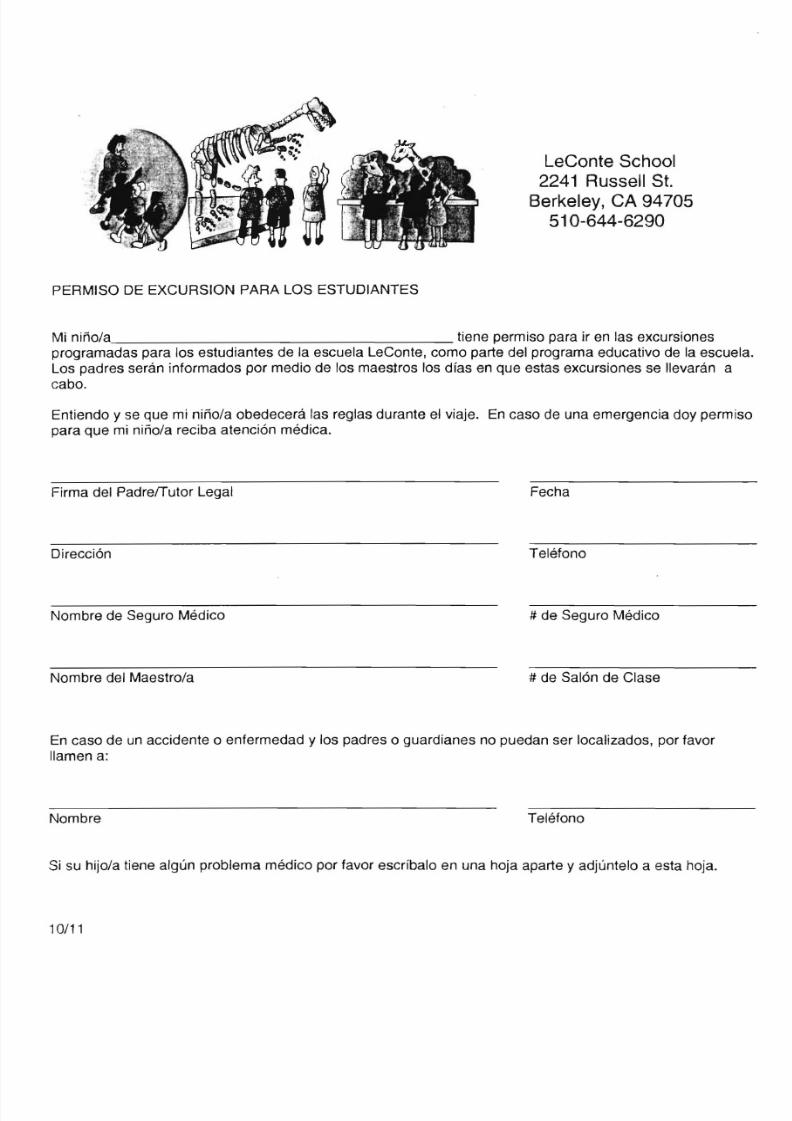
LeConte School2241
Russell St.Berkeley, CA 94705510-644-6290
PERMISO DE EXCURSION PARA LOS ESTUDIANTES
Mi nifio/a tiene permiso para ir en las excursionesprogramadas para los estudiantes de la escuela LeConte, como parte del programa e d u c a t i v ~de la escuela.Los padres seran informados por medio de los maestros los dfas en que estas excursiones se lIevaran acabo.
Entiendo y se que mi nifio/a obedecera las reglas durante el viaje. En caso de una emergencia doy permisopara que mi nifio/a reciba atenci6n medica.
Firma del Padre/Tutor Legal Fecha
Direcci6n Telefono
Nombre de Seguro Medico # de Seguro Medico
Nombre del Maestro/a # de Sal6n de Clase
En caso de un accidente 0 enfermedad y los padres 0 guardianes no puedan ser localizados, por favorIlamen a:
Nombre Telefono
Si su hijo/a tiene algun problema medico por favor escrfbalo en una hoja aparte y adjuntelo a esta hoja.
10/11

8/8/2019 Back to School Package Forms
http://slidepdf.com/reader/full/back-to-school-package-forms 5/7
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Berkeley Unified School District
Media Permission 2010 - 2011 School Year
There are many opportunities in which parents, teachers, the press orothers would like to photograph or film our students. The BUSD and ourpartners (i.e., the PTA or the Berkeley Public Education Foundation[BPEFJ) value these images as compelling ways to share and urgesupport for the work of our teachers and students. Photo opportunitiesarise over the course of the school year, usually with little warning ortime to contact parents for permission. We recognize that some familieswould prefer their children not appear, even unidentified, in any print orelectronic media. Having this form on file will ensure that your wishesare followed. Please complete and return to your school.
o I do not wish to have my child's name or face to be used in anyprint or media.
o My child's photograph, with no identification, may be used byBUSD or its partners (i.e., PTA, BPEF with District approval) inprint or other media related to school events or activities.
o My child's name and photograph may be used by BUSD or itspartners (Le., PTA, BPEF with District approval) in print or othermedia related to school events or activities.
Student Name:
School Name: LECONTE ELEMENTARY SCHOOL
Parent/Guardian Signature Date
8/8/2019 Back to School Package Forms
http://slidepdf.com/reader/full/back-to-school-package-forms 6/7
Berkeley Unified School District Parent Authorization for Release of Information to City of Berkeley Public Health Division
Please help us keep your student/s healthy!BUSD and the City of Berkeley Public Health Division have formed a new partnership to better meet the healthcare and health education needs of students and families. Through the School-Linked Health Services Program,Berkeley Public Health Division win now help BUSD accomplish the following objectives:
• complete documentation and follow-up on immunizations and health screenings,
• work with uninsured families to obtain health insurance and healthcare services,
• assist with the development of care plans for students with unique healthcare needs during the school day,
In order to do this work effectively, Th e School-Linked Health Services Program needs basic information aboutthe healthcare status of BUSD students. By signing this document, you are consenting to BUSD sharing withBerkeley Public Health Division information from the following documents containing information about yourchild:
1. Your child's Student Emergency Card
2. Your child's
immunization record3. Your child's results from health screenings conducted at school , including dental, hearing, vision, and
scoliosis
Th e information supplied in these documents will only be shared with Berkeley Public Health. NO OTHERORGANIZATION WILL BE GIVEN THIS INFORMATION. This information will be used by Berkeley PublicHealth Division for the following purposes only:
• Contacting families regarding potentially unmet health needs (based on health screening results) and withinformation about nollow cost health insurance.
• Assisting the schools with the coordination of care plans for students with unique healthcare needs duringthe school day.
Please contact the BUSD Office of Family and Community Partnerships, Maya Hernandez, 644-8991 or City Of BerkeleySchool-Linked Health Services Program, Kate Graves, 981-7677 with any questions, comments or concerns.
Please tear off and return to the main office at your childlren 's school---------------Parent Authorization fo r Release of Information to Berkeley Public Health---------------
I consent to BUSD providing healthcare information to City of Berkeley Public Health Division from thefollowing sources:
• My child ' s Student Emergency Card
• My child's Immunization Record• My child's results from mandated health screenings (dental, vision, hearing, scoliosis)
Name of School: ___ ______________ _
Student 's Name: ___ _ _ _____________ Birthdate: ______ _
*Signature of ParenUGuardian: Date: ________ _
This release is only validfor one year from the date of signature
*California Education Code. Section 49075 states: "A school district may permit access to pupil records to any person for whom a parent of the pupil has executed writtenconsent specifying the records to be released and identifying the party or class of parties to whom the records may be released. The recipient mu st be notified that the
transmission of the information to others without the written consent of the parent is prohibited. The consent notice shall be permanently kept with the record file ."

8/8/2019 Back to School Package Forms
http://slidepdf.com/reader/full/back-to-school-package-forms 7/7
Distrito Escolar Unificado de BerkeleyAutorizacion del Padre de Familia Para Proporcionar Informacion a la Division de Salud PUblica de la Ciudad de Berkeley
.Por favor ayudenos a mantener a suls estudiante/s saludables!EI Distrito Escolar de Berkeley (BUSD) y la Divisi6n de Salud Publica de la Ciudad de Berkeley han formadouna nueva colaboraci6n entre sf para servir de una mejor manera el cuidado de salud y las necesidades deeducaci6n referentes a la salud de los estudiantes y sus familias . Mediante el Program a de Servicios de SaludEntrelazados con la Escuela (School-Linked Health Services), la Divisi6n de Salud Publica de Berkeley ayudanial BUSD a lograr los siguientes objetivos:
• completar la documentaci6n y realizar un seguimiento en las vacunas y revisiones de salud,• trabajar con las familias sin seguro medico para obtener dicho seguro y servicios para el cuidado de salud,
• ayudar con el desarrollo de planes para el cuidado de los estudiantes con necesidades de salud unicas durante el dfaescolar,
En orden de realizar este trabajo de una manera efectiva, El Programa de Servicios de Salud Entrelazados con laEscuela necesita informaci6n basica acerca del estado de salud de los estudiantes del BUSD.Alfirmar este documento , usted da su consentimiento para que BUSD comparta con la Division de SaludPublica de Berkeley informacion acerca de su niiioia la cual se encuentra en los siguientes documentos:
1. Tarjeta de Emergencia de su nino/a
2. Expediente de vacunas de su nino/a3 . Resultados de las evaluaciones de salud de su nino/a que se han realizado en la escuela, dentales, auditivas, visi6n
y escoliosis
La informaci6n que se obtenga en estos documentos sera compartida unicamente con el Departamento de SaludPublica de Berkeley. ESTA INFORMACION NO SE COMPARTIRA CON NINGUNA OTRAORGANIZACION. Esta informaci6n sera usada por la Divisi6n de Salud Publica de Berkeley unicamente paralos siguientes prop6sitos:
• Contactar a las familias en 10 referente a necesidades potenciales de sa Iud que no han sido atendidas (basado enlos resultados de la evaluaci6n de salud) y con informaci6n acerca de seguro medico a bajo/sin costo .
• Asistir a las escuelas con la coordinaci6n de planes para el cuidado de los estudiantes con necesidades de saludunicas durante el dfa escolar.
Por favor comunfquese con la Oficina de Colaboraci6n con las Familias y la Comunidad, Maya Hernandez,644-8991 0 con el Programa de Servicios de Salud Entrelazados con la Escuela de la Ciudad de Berkeley, KateGraves , 981-7677 con preguntas, comentarios 0 preocupaciones .
Por favor corte y devuelva a fa oficina principal de la escuela de su/s niiio/a/s---------------Autorizacwn del Padre de Familia Para Proporcionar Informacwn a Salud Publica de Berkeley···········
Yo doy mi consentimiento a BUSD para que provea la informaci6n del cuidado de salud a la Divisi6n de SaludPublica de la Ciudad de Berkeley de los siguientes documentos:
• Tarjeta de Emergencia de mi nino/a
• Expediente de vacunas de mi nino/a
• Resultados de las evaluaciones de salud de mi nino/a que se han realizado en la escuela (dental, visi6n,auditiva, escoliosis)
Nombre de la Escuela: _________________ _
Nombre del Estudiante: _______________ _ Fecha de Nacimiento: _____ _
*Firma del Padre 0 Tutor: ______________ _ Fecha: ________ _
Esta autorizaci6n es valida unicamente por un an a a partir de la fecha de la firma*EI C6digo de Educaci6n de California, Secci6n 49075 declara: "Un disLrito escolar puede permiLir acceso a los expedientes del alumno acualquier persona a Ja cual el padre del alumno ha ejecutado un consenLimiento por escrito especificando los expedientes que se van aproporcionar e identificando al grupo 0 a la clasificaci6n del grupo al cual se Ie van a proporcionar los expedientes. Quien los recibe debese r notificado/a que la Lransmisi6n de I a informaci6n a oLros sin la autorizaci6n po r escriLo del padre del alumno es prohibida . La hoja de
consentimiento debe eSLar permanentemente guardada con el expedienLe .





























