Embed Size (px)
Citation preview

I N V I T E D A R T I C L E M E D I C A L M I C R O B I O L O G YL. Barth Reller and Melvin P. Weinstein, Section Editors
Background and Rationale for Revised Clinicaland Laboratory Standards Institute InterpretiveCriteria (Breakpoints) for Enterobacteriaceaeand Pseudomonas aeruginosa: I. Cephalosporinsand Aztreonam
Michael N. Dudley,1 Paul G. Ambrose,2 Sujata M. Bhavnani,2 William A. Craig,3 Mary Jane Ferraro,4 andRonald N. Jones;5 for the Antimicrobial Susceptibility Testing Subcommittee of the Clinical and Laboratory StandardsInstitute1Rempex Pharmaceuticals, San Diego, California; 2Institute for Clinical Pharmacodynamics, Inc, Latham, New York; 3Department of Medicine,University of Wisconsin School of Medicine, Madison; 4Massachusetts General Hospital and Harvard Medical School, Boston; 5JMI Laboratories,North Liberty, Iowa
Widespread resistance in Enterobacteriaceae and Pseudomonas aeruginosa to cephalosporin and monobactamantibiotics due to extended-spectrum β-lactamases (ESBLs) has resulted in the need for reassessment of theinterpretative criteria (breakpoints) established for these agents more than 2 decades ago. Following extensiveevaluation, the Clinical and Laboratory Standards Institute recently adopted and published new breakpointsfor these agents for use in clinical laboratories and provided updated recommendations for use of the ESBLscreening test. This paper summarizes the background and supportive rationale for new interpretative criteriafor cephalosporins and aztreonam for testing Enterobacteriaceae.
Keywords. breakpoints; Enterobacteriaceae; cephalosporins; Pseudomonas; CLSI.
β-Lactam antimicrobial agents are highly useful fortreating infections caused by Enterobacteriaceae. Newgenerations of agents, including methoxyimino cepha-losporins and monobactams, with great stability tothese enzymes were developed in the 1980s; however,the dissemination of extended-spectrum β-lactamases(ESBLs) that hydrolyze these agents as well earlier-generation β-lactams have changed the potency ofthese drugs against most Enterobacteriaceae. Earlyobservations on the response to cephalosporins in in-fections due to ESBLs among Enterobacteriaceae
suggested reduced clinical efficacy, particularly whenthe drugs were used at lower doses [1, 2].
In addition, there have been advances in the under-standing of the relationship between the minimum in-hibitory concentration (MIC), drug resistance, and drugexposure (pharmacokinetics/pharmacodynamics [PK-PD]) and outcomes in nonclinical models of infectionand clinical trials for β-lactam antibiotics [3]. This un-derstanding has been applied in setting in vitro suscept-ibility criteria (breakpoints) for antimicrobial agents [4].
The data and approach used to set the originalbreakpoints for cefotaxime vs Enterobacteriaceae servedas a basis for setting breakpoints for other extended-spectrum cephalosporins. Analysis of the data availableat the time these breakpoints were established showedthat the data supporting a susceptible breakpoint valueof ≤8 mg/L were inadequate compared to currentapproaches for establishing susceptibility breakpoints.In the only large surveillance database available atthe time, >95% of gram-negative isolates had MICs
Received 6 January 2012; accepted 9 January 2013; electronically published18 January 2013.
Correspondence: Michael N. Dudley, PharmD, FIDSA, Rempex Pharmaceuticals,11535 Sorrento Valley Rd, San Diego, CA 92121 ([email protected]).
Clinical Infectious Diseases 2013;56(9):1301–9© The Author 2013. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/cit017
MEDICAL MICROBIOLOGY • CID 2013:56 (1 May) • 1301
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

≤1 mg/L [5]. In the cefotaxime clinical trial database, clinicalresponse rates declined slightly for cefotaxime MICs ≥32 com-pared to lower values; however, most organisms had MICs <8mg/L, consistent with the surveillance data. Organisms withhigher MICs were limited to Acinetobacter species and Pseu-domonas aeruginosa. Thus, it appears that the best support forthe original cefotaxime breakpoints came from studies of pa-tients with Acinetobacter infections, in which the bacteriologiceradication rates were 98%, 89%, and 50% for strains withMICs of ≤8, 16, and ≥32, respectively [5]. In addition to datafrom cefotaxime clinical trials, pharmacologic and PK-PD datawere also considered but limited to assessment of peak drugconcentrations (based on the rarely used 2-g dose) related tothe MICs; more modern concepts of f T >MIC (percentage ofa dosing interval in which free-drug concentrations exceed theMIC) being important for β-lactam antibiotics had not been de-veloped at the time. Thus, the original cefotaxime breakpointsfor Enterobacteriaceae were based upon rudimentary PK-PDconsiderations, and observations on clinical or microbiologicalresponses in infections due to P. aeruginosa and Acinetobacter,as they were the only organisms with MICs in the higher rangein the era prior to dissemination of ESBLs. The breakpointsselected from this analysis then served as a basis for assigningbreakpoints to subsequent cephalosporins and aztreonam,regardless of their pharmacokinetics or dosage regimen.
Extended-Spectrum β-LactamasesAlthough many ESBL-producing Enterobacteriaceae havecephalosporins and aztreonam MICs far in excess of the origi-nal Clinical and Laboratory Standards Institute (CLSI) andFood and Drug Administration (FDA) resistance breakpoints,many clinical isolates have MICs that fell within the existing“susceptible” category. The identification of this “gap,” as wellas uncertainty concerning the clinical response in infectionsdue to these strains, led to the development of ESBL screeningand phenotypic confirmatory tests that would detect theseenzymes in susceptible Escherichia coli and Klebsiella species(and later Proteus mirabilis). A key aspect in the use and re-porting of the results from ESBL testing was the direction toclinical laboratories that a positive confirmatory ESBL testshould result in the reporting of all cephalosporins and aztreo-nam as “resistant” regardless of the MIC values.
Although the ESBL test identified isolates of E. coli, Klebsi-ella species, and P. mirabilis that produced these enzymes, itcreated a considerable increase in workload for clinical micro-biology laboratories. Moreover, the test did not consider otherclinically important β-lactamases not inhibited by clavulanicacid (eg, ampC). Many clinical isolates possess mixtures ofESBLs plus ampC β-lactamases; these strains could have a nega-tive ESBL test and MICs in the susceptible category, but in arange where clinical response appeared to be compromised with
usual dosage regimens. The number of strains in this categorywas significant; data from the 2000–2003 Sentry programshowed that among a sample of 11 913 isolates of Enterobacter-iaceae, 931 had MICs of 4 μg/mL or 8 μg/mL to ceftazidime orceftriaxone (susceptible, but satisfying CLSI criteria for perform-ing the ESBL screening test). Of these 931 isolates, E. coli orKlebsiella species accounted for only approximately half (422 or45% for ceftazidime, and 528 or 57% for ceftriaxone) of theEnterobacteriaceae isolates with elevated MICs (R. Jones, un-published observations). Thus, a considerable number of Enter-obacteriaceae with elevated MICs would not undergo ESBLtesting, leaving clinical microbiology laboratories with no alter-native other than to report these isolates as susceptible.
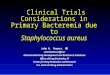
What Is Important in Bacterial Killing and Efficacy—the MIC orthe Type of β-Lactamase Produced?A key issue in evaluating susceptibility breakpoints with newresistance mechanisms is whether PK-PD relationships forfully susceptible, wild-type bacteria are altered by different re-sistance mechanisms. Specifically, would ESBL-producing En-terobacteriaceae appear to be more “resistant” in treatmentsettings, regardless of the MIC, and require higher/more fre-quent dosing? (That is, do ESBL-producing strains require ahigher percentage of a dosage interval during which free-drugconcentrations remain above the MIC [f T >MIC] to achieveacceptable levels of efficacy in vivo?) Using ESBL-producingisolates in mouse models of infection, Andes and Craig evalu-ated different cephalosporins in the treatment of Enterobacter-iaceae producing various β-lactamases. These studies clearlyestablished that PK-PD relationships for efficacy of cephalo-sporins against ESBL- or non-ESBL–producing isolates inanimal models were similar (Figure 1) [6]. Thus, drug re-sponse in vivo for various β-lactamases was predicted by theMIC and existing PK-PD metrics, negating the need for addi-tional factors or different f T >MIC targets for ESBL-andnon-ESBL–producing Enterobacteriaceae.
Despite these experimental data, other researchers haveheld that ESBL-producing Enterobacteriaceae will fail treat-ment with cephalosporins and aztreonam, regardless of MICvalue. Careful inspection of many reports of cephalosporintreatment “failure” of infections caused by ESBL-producingEnterobacteriaceae with low MICs involved inadequate dosageregimens that would provide suboptimal PK-PD exposures,and would be expected to fail on these criteria [1, 7, 8]. In areview of published clinical outcomes in patients with E. colior Klebsiella species bacteremia, Andes and Craig compiledclinical response data based on β-lactamase production (in-cluding ESBLs) and cephalosporin MIC used in treatment [6].Of 42 cases identified, reduced clinical response was associatedwith increasing MIC, with a considerable decrease in efficacyfor cephalosporin MICs >2 mg/L (Table 1; [6]). These data
1302 • CID 2013:56 (1 May) • MEDICAL MICROBIOLOGY
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

were concordant with the above-described results in experi-mental models of infection where comparable f T >MICs tothose obtained in humans demonstrated that the MIC and PKdata, not the β-lactamase resistance mechanism, was the bestpredictor of in vivo efficacy.
Reevaluating and Setting BreakpointsThe CLSI consensus process provides formal procedures forsetting or revising susceptibility breakpoints [9]. CLSI’s “M23”document specifically outlines several reasons for the reassess-ment of susceptibility breakpoints that applied to the cephalo-sporins and aztreonam, including:
• New resistance mechanisms (eg, ESBLs);
• New PK-PD data, including better understanding of PK-PD data not previously available or recognized;
• Recognition that new breakpoints would simplify testingand eliminate need for additional tests to detect specific resis-tance mechanisms;
• Elimination of differences in breakpoints between CLSI andother organizations setting breakpoints (eg, European Commit-tee on Antimicrobial Susceptibility Testing [EUCAST], FDA);
• Interpretive criteria established using organisms of severalspecies.
Of note, considerable data on PK-PD in animals andhumans had emerged in the 2 decades following the initialapproval and marketing of these agents. When this knowledgewas applied, analyses indicated that the existing breakpointswere inconsistent with the current approach that was beingapplied to newer antimicrobial agents.
SUMMARY OF DATA EXAMINED TOGENERATE NEW MIC INTERPRETIVE CRITERIAFOR CEPHALOSPORINS ANDENTEROBACTERIACEAE
Clinical, PK-PD, and MIC distribution data constituted thetypes of information that were considered in revising the break-points. While highly desirable, clinical data from controlled oreven uncontrolled trials were few, largely due to lack of contem-porary studies and lapse of patent and market exclusivity thatresulted in lack of the industry sponsor interest. Some retro-spective series describing clinical response with ESBL producingisolates were available [1, 2, 6–8], but critical information con-cerning MIC, concomitant drug treatment, site of infection,and cephalosporin dosage regimen was usually not available.Thus, information beyond that provided in the response tocephalosporins by MIC assessment conducted by Craig et al [6]was not available. This resulted in increased dependence ofother data, particularly PK-PD analyses.
PK-PD ConsiderationsPK-PD analyses using available data were conducted to deter-mine if usual FDA-approved cephalosporin and aztreonamdosage regimens could provide target levels of drug exposuresassociated with bacterial killing in vivo for organisms withMICs at and below the selected susceptibility breakpoint. The
Figure 1. Comparison of the percentage of a dosing interval in whichfree-drug concentrations exceed the MIC (T > MIC) required for 4 ad-vanced generation cephalosporins (cefotaxime, ceftazidime, ceftriaxone,and cefepime) against drug-susceptible and -resistant strains of Escheri-chia coli, Klebsiella species, Enterobacter species, and Serratia speciesproducing varying β-lactamases in a murine thigh infection model. Theβ-lactamases were well-characterized in these strains and includedampC, OXA1, OXA2, and TEM1 as well as the extended-spectrum β-lac-tamases (ESBLs) TEM3, TEM7, TEM12, TEM26, SHV2, SHV4, SHV5,SHV7, CTXM2, and CTXM3. The cephalosporins were tested at 4–6dosage regimens administered over 24 h that produced T > MIC valuesranging between 0 and 100% in the neutropenic mouse thigh modelof infection. The relationship between time above MIC and bacterialkilling was similar in ESBL-producing and non-ESBL–producing strains [6].Abbreviations: CFU, colony-forming unit; ESBL, extended-spectrumβ-lactamase; MIC, minimum inhibitory concentration.
Table 1. Clinical Outcome by Minimum Inhibitory Concentrationin 42 Patients With Bacteremia Due to Escherichia coli andKlebsiella pneumoniae Producing Various β-Lactamases TreatedWith Cephalosporin Monotherapy
MIC, mg/L % Response % Failure
≤1 81 19
2 67 334 27 73
≥8 11 89
Abbreviation: MIC, minimum inhibitory concentration.
Source: Craig et al [6].
MEDICAL MICROBIOLOGY • CID 2013:56 (1 May) • 1303
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

strength of this approach is that a consistent target level of ex-posure (eg, f T >MIC of 50%) could be compared across severalagents with different pharmacokinetic properties but within thesame drug class. These analyses compared the expected dura-tion that free-drug serum or plasma concentrations of an anti-microbial exceeded several MIC values. Information on humanpharmacokinetics, MICs, and target f T >MIC values for ceph-alosporins were compiled from the literature. Pharmacokineticparameters used in simulation were drawn from studies innormal volunteers because reliable patient or population phar-macokinetic data were not available for a majority of olderdrugs (PK parameters for drugs are listed in SupplementaryTable 1). Simulation approaches such as that implemented inMonte Carlo methods can be used to generate f T >MIC valuesfor a population of individuals to determine the proportion ofsimulated patients that would expected to achieve a target levelof exposure (eg, f T >MIC of ≥50%) [4, 10].
Because PK data from only noncompartmental pharmacoki-netic analyses of the drugs were largely available, a simple phar-macokinetic model was chosen for generating f T >MIC values:
Hours above MIC ¼ lnðDose=VdÞ � ln MIClz
;
where λz is the slope of the terminal slope of the serum concen-tration vs time curve, MIC is the value for possible breakpointMICs, and Vd is the volume of distribution adjusted forunbound drug (generally, Varea or Vβ was used for simulations).
Data were compiled for f T >MIC values of 40%–60% usingseveral dosage regimens. Where possible, the lowest US FDA-approved dosage regimen covering indications other thanurinary tract infections was considered in susceptibility break-point decisions; in some cases, the most frequently useddosage regimen or a dosage regimen that would avoid splittingMIC distributions (see below) was used. For purposes of con-sistency for comparisons among drugs, f T >MIC of 50% wasthe nominal target selected for comparisons and susceptibilitybreakpoint selection. For cephalosporins, this value corre-sponds with approximately a 1 log decline in bacterial countsin the neutropenic mouse thigh infection model and other in-fection models. The susceptible PK-PD breakpoint value wasselected to be the MIC value that attained a PK-PD target in90% of simulated patients for each drug. In general, lowervalues for PK-PD target attainment were used in decisions onan “intermediate” category.
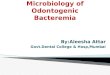
Results of the Monte Carlo simulations for each drug anddosage regimen are shown in Figure 2.
MIC DistributionsThe distribution of MICs for a cephalosporin or aztreonam forE. coli and Klebsiella pneumoniae from the Sentry 2001–2003
surveillance database were examined where available. This anal-ysis considered how new breakpoints might shift populations oforganisms, and whether a “peak” in the MIC distribution mightfall on a susceptible breakpoint; the latter is problematic giventhat inherent variability in the test could result in a changed cat-egory interpretation (eg, susceptible to intermediate).
Inspection of MIC distributions and PK-PD breakpointsshowed that for most drugs, the change in susceptible break-point for each drug resulted in shifting most ESBL-producingisolates into the nonsusceptible category; this is not surprisingas most of the PK-PD derived breakpoints also centeredaround the MICs used for the ESBL screening test. For keyextended-spectrum cephalosporins (ie, ceftriaxone and ceftazi-dime) and aztreonam, peak of the MIC distribution remainedbelow the new susceptible breakpoints identified by the PK-PD analysis (eg, MIC <2 or 4 mg/L).
The MIC distributions for E. coli and K. pneumoniae pre-sented some issues for the PK-PD breakpoints identified forsome agents. For cefuroxime, a lower susceptible breakpointseemed to be indicated for the dosage regimen of 750 mgevery 8 hours, but this would have bisected the major bacterialpopulations. Ultimately, interpretative criteria remained un-changed, but a higher dosage regimen that supported a sus-ceptible breakpoint was selected (1.5 g every 6 hours). Forcefazolin, lower breakpoints were provisionally selected thatshifted the majority of isolates into the intermediate or resis-tant ranges; susceptibility breakpoints for cefazolin were sub-sequently revised upward in 2011 and a higher dosageregimen was used as support (ie, 2 g every 8 hours [11]).
Revised MIC Interpretive Standards and Corresponding ZoneDiameter BreakpointsTable 2 shows the previous and revised susceptible break-points, with corresponding PK-PD target attainment data. Inmost cases, the susceptible breakpoints were reduced 2- to 4-fold from pre-2010 values. Notably, changes in breakpointswere referenced to a dosage regimen for the drug used fortreatment of infection. In contrast to previous susceptiblebreakpoints, approximately 90% of patients receiving the indi-cated dosage regimen would be expected to have f T >MIC ofat least 50% for the new susceptibility breakpoints.
Analysis of MIC and zone diameters for disk testing of a largecollection of clinical isolates was performed and identified corre-sponding zone diameter cutoffs that met criteria for acceptanceaccording the CLSI documents (Table 3) [9, 11, 12].
SPECIAL ISSUES
Cefepime Susceptibility BreakpointsAfter review of clinical and PK-PD data and MIC distribu-tions for cefepime, breakpoints were not changed; however,
1304 • CID 2013:56 (1 May) • MEDICAL MICROBIOLOGY
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

Figure 2. Percentage probability of pharmacokinetic/pharmacodynamic target attainment for cephalosporins and aztreonam. Line plots show thepercent of 10 000 simulated patients expected to attain f T > MIC (percentage of a dosing interval in which free-drug concentrations exceed theminimum inhibitory concentration) targets of 40%, 50%, or 60% with indicated dosage regimen. Bars show minimum inhibitory concentration distri-butions for isolates of Escherichia coli and Klebsiella pneumoniae from Sentry Surveillance 2001–2003. Abbreviation: MIC, minimum inhibitoryconcentration.
MEDICAL MICROBIOLOGY • CID 2013:56 (1 May) • 1305
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

higher, FDA-approved dosage regimens of at least 1 g every 8hours or 2 g every 12 hours were referenced as support for theexisting breakpoints. These dosage regimens provided compa-rable levels of PK-PD target attainment for an f T >MICtarget of approximately 50% at the susceptible breakpoint of8 mg/L. Review of reported clinical failures due to susceptiblebacteria based on these breakpoints were likely associated withunderdosing of cefepime (doses <3 g/day) [1, 7]. (Note:
Although supported by the data available at the time of thereassessment, CLSI plans to reevaluate these breakpoints inlight of recently published data on safety and efficacy [13] anddifferences between CLSI and EUCAST breakpoints.)
Cephalothin Susceptibility BreakpointsPK-PD analyses revealed that the susceptible breakpoint forcephalothin needed to be substantially lower to be consistent
Table 2. Summary of Pharmacokinetic/Pharmacodynamic Target Attainment for Cephalosporins and Aztreonam for Previous and NewSusceptibility Breakpoints for Enterobacteriaceae, Reviewed by the Clinical and Laboratory Standards Institute
Drug Dosage Regimen
Pre-2010 Susceptible Breakpoint New Susceptible Breakpoint
CommentsValue (mg/L)% PK-PD
Target Attainmenta Value (mg/L)% PK-PD
Target Attainmenta
Cefuroxime 1.5 g IV q8h 8 94 8 94 Unchanged but qualifiedby a higher-dosageregimen
Cefotaxime 1 g IV q8h 8 3 1 89
Ceftriaxone 1 g IV q24h 8 0 1 99
Ceftizoxime 1 g IV q12h 8 3 1 99Ceftazidime 1 g IV q8h 8 81 4 100
Aztreonam 1 g IV q8h 8 54 4 94
Cefepime 1 g IV q8h or 2 g IVq12h
8 91–95 8 91–95 Unchanged, but qualifiedby higher-dosageregimens
Cefamandole 1 g IV q6h 8 23 … …b
Cefmetazole 1 g IV q8h 16 0 … …b
Cefoperazone 1 g IV q8h 16 0 … …b
Cefotetan 1 g IV 12h 16 8 … …b
Abbreviations: FDA, Food and Drug Administration; IV, intravenous; PK-PD, pharmacokinetic/pharmacodynamic, q6h, every 6 hours; q8h, every 8 hours; q12h,every 12 hours; q24h, every 24 hours.a Percentage target attainment represents the percentage of patients from a Monte Carlo simulation that would have free-drug serum concentrations exceedingthe susceptible breakpoint for at least 50% of the dosage interval.b New breakpoints could not be established for this agent based on limited data. This agent has limited availability in many countries. If considering using thisagent for Escherichia coli, Klebsiella species, or Proteus species, extended-spectrum β-lactamase (ESBL) testing should be performed. If isolates test ESBLpositive, the isolate should be considered resistant to this agent.
Table 3. Revised and Pre-2010 Clinical and Laboratory Standards Institute Breakpoints for Cephalosporins and Aztreonam forEnterobacteriaceae
Drug (Dosage)a
MIC (μg/mL) Disk (mm)
Revised Pre-2010 Revised Pre-2010
S I R S I R S I R S I R
Aztreonam (1 g q8h) ≤4 8 ≥16 ≤8 16 ≥32 ≥21 18–20 ≤17 ≥22 16–21 ≤15Cefotaxime (1 g q8h) ≤1 2 ≥4 ≤8 16–32 ≥64 ≥26 23–25 ≤22 ≥23 15–22 ≤14Ceftazidime (1 g q8h) ≤4 8 ≥16 ≤8 16 ≥32 ≥21 18–20 ≤17 ≥18 15–17 ≤14Ceftizoxime (1 g q12h) ≤1 2 ≥4 ≤8 16–32 ≥64 ≥25 22–24 ≤21 ≥20 15–19 ≤14Ceftriaxone (1 g q24h) ≤1 2 ≥4 ≤8 16–32 ≥64 ≥23 20–22 ≤19 ≥21 14–20 ≤13
Abbreviations: I, intermediate; MIC, minimum inhibitory concentration; q8h, every 8 hours; q12h, every 12 hours; q24h, every 24 hours; R, resistant;S, susceptible.a Minimum dosage linked to breakpoints.
1306 • CID 2013:56 (1 May) • MEDICAL MICROBIOLOGY
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

with the other cephalosporins used against Enterobacteriaceae.Because cephalothin is no longer marketed in the UnitedStates and many other countries, the subcommittee originallyplanned to remove the existing breakpoints. However, the sub-committee further considered previous recommendations andpractice by clinical laboratories of applying cephalothininterpretative criteria to predict the activity of certain oralcephalosporins for urinary tract isolates of Enterobacteriaceae.Although these correlations were established more thana decade ago, the existing cephalothin breakpoints wereretained for use only to predict results for oral cephalosporinswith FDA-approved indications for treatment of urinarytract infections (cefadroxil, cefpodoxime, cephalexin, andloracarbef ).
ESBL Screening TestWhen using the revised breakpoints, routine testing for ESBLs(screen plus phenotypic confirmation test) is no longer re-quired. Although ESBL testing no longer has utility in treat-ment decisions when the new breakpoints are employed, thesubcommittee recognized that the test may have utility insome settings for purposes of epidemiologic investigations andinfection control practice. In addition, it may be necessary forsome institutions to continue temporarily using the ESBL test(and CLSI’s pre-2010 recommendations for interpretative cri-teria) until their laboratories are able to validate and imple-ment the revised MIC or disk breakpoints.
Pseudomonas aeruginosaFollowing revision of Enterobacteriaceae breakpoints, a similarassessment was made by the subcommittee for P. aeruginosa.Similar to the Enterobacteriaceae, there were no clinical datato assist in identifying susceptibility breakpoints for cephalo-sporins and aztreonam, and thus PK-PD data and MIC distri-butions comprised the primary data to support decisionsconcerning revised breakpoints. The subcommittee recognizedthat only a few cephalosporins and aztreonam had clin-ical utility for P. aeruginosa infections. Thus, susceptibility
breakpoints for only ceftazidime, cefepime, and aztreonamwere reconsidered.
Studies in animal models of P. aeruginosa infection showthat similar PK-PD metrics are associated with efficacy in vivoand in vitro models of infection, similar to that determinedfor Enterobacteriaceae [3]. Thus, susceptibility breakpointssimilar to those determined for Enterobacteriaceae were con-sidered; however, in contrast to Enterobacteriaceae, the distri-bution of MICs for P. aeruginosa isolates for aztreonam,cefepime, and ceftazidime were significantly higher, withmode values falling between 2 and 4 mg/L (Table 4). Thus,the doses and susceptibility breakpoints used for Enterobacter-iaceae were likely unsuitable for use with P. aeruginosa.
PK-PD target attainment of higher dose regimens stillwithin existing FDA-approved ranges was examined to deter-mine if the existing susceptibility breakpoints would providesuitable PK-PD target attainment in simulated patients whilenot bisecting the MIC distribution of P. aeruginosa. Thus, theexisting susceptibility breakpoints for cefepime, ceftazidime,and aztreonam were retained, but dosage regimens supportingthese breakpoints were added. Given the poorer potencyand lack of clinical usefulness of other cephalosporins forP. aeruginosa infections, the previously published susceptibilitybreakpoints of these agents against this organism were removedfrom CLSI tables. Approved susceptibility breakpoints andsupportive dosage information are provided in Table 5.
IMPLEMENTATION OF NEW BREAKPOINTS
There are no regulatory barriers that prevent clinical laborato-ries from using revised susceptibility breakpoints for patientcare. Although the susceptibility breakpoints were publishedin CLSI documents in provisional form in 2010 and final formin 2011, barriers to implementation remain, particularly inlaboratories using commercial FDA-approved automated sus-ceptibility testing systems. However, laboratories can imple-ment these susceptibility breakpoints immediately through use
Table 4. Minimum Inhibitory Concentration Distributions of Clinical Isolates of Pseudomonas aeruginosa from North America, LatinAmerica, and Europe (7846 strains From SENTRY Program, 2005–2009)
% at MIC (μg/mL)
Antimicrobial ≤0.12 0.25 0.5 1 2 4 8 16 32 64 128 >128
Aztreonam 0.4 0.9 1.0 1.4 5.5 38.6 17.2 14.6 … … … 20.4Cefepime 0.1 0.4 1.1 14.2 29.5 17.6 14.3 11.8 … … … 11.1
Ceftazidime … … … 11.2 39.0 16.8 7.5 5.8 … … … 19.7
Ceftriaxone … 0.1 0.3 0.5 0.6 1.4 4.3 7.2 14.0 … … 71.7
Underlined values indicate mode value.
Abbreviation: MIC, minimum inhibitory concentration.
MEDICAL MICROBIOLOGY • CID 2013:56 (1 May) • 1307
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

of the disk test, or by conducting an appropriate in-housevalidation study. The Infectious Diseases Society of Americahas posted on its website guidance for such validation pro-tocols (http://www.idsociety.org/Antimicrobial_Susceptibility_Testing/) [14].
SUMMARY
Increasing resistance of Enterobacteriaceae and Pseudomonasspecies to β-lactam antimicrobial agents necessitated reconsid-eration of susceptibility breakpoints for these agents. Becausedata from controlled clinical trials pre- or postregistrationwere not available, PK-PD principles from clinical and non-clinical data were applied for usual FDA-approved dosage reg-imens of these agents. This enabled these “older agents” to bebrought to the level of standards and “best practice” of PK-PDcurrently applied for newer drugs.
Publication of revised CLSI interpretive standards forcephalosporins and aztreonam for Enterobacteriaceae andP. aeruginosa was accomplished after several years of carefulanalysis of clinical, microbiological, and clinical data using theconsensus process. Although some regulatory issue remain tobe solved (eg, FDA approval of breakpoint changes in auto-mated susceptibility testing devices), clinical laboratories canimplement the revised susceptibility breakpoints using thecorrelate zone diameter cutoffs, Etest methods, or by followingprocedures for validating broth dilution MIC methods froman automated susceptibility testing device in their own labora-tories. Infectious disease clinicians, antimicrobial stewardshipprograms, and clinical microbiology laboratories are encour-aged to implement the revised interpretive criteria to optimizeantimicrobial therapy of infections due to Enterobacteriaceaeand P. aeruginosa with these agents.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online(http://cid.oxfordjournals.org/). Supplementary materials consist of dataprovided by the author that are published to benefit the reader. Theposted materials are not copyedited. The contents of all supplementarydata are the sole responsibility of the authors. Questions or messagesregarding errors should be addressed to the author.
Notes
Acknowledgments. The contributions of other members of the CLSIEnterobacteriaceae Working Group (Laurie Thrupp, Stephen Jenkins, JoanFung-Tomc, and Karen Bush) and the CLSI Subcommittee on Antimicro-bial Susceptibility Testing (Frank Cockerill, George Eliopoulos, DavidHecht, Janet Hindler, James Jorgensen, Mair Powell, Jana Swenson, FredTenover, John Turnidge, Mel Weinstein, Matthew Wikler, and BarbaraZimmer) on the development of new interpretive criteria areacknowledged.Potential conflicts of interest. All authors: No reported conflicts.All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to thecontent of the manuscript have been disclosed.
References
1. Patterson DL, Ko WC, Von Gottberg A, et al. Outcome of cephalo-sporin treatment for serious infections due to apparently susceptibleorganisms producing extended-spectrum beta-lactamases: implicationfor the clinical microbiology laboratory. J Clin Microbiol 2001; 39:2206–12.
2. Pitout JDD. Infections with extended-spectrum beta-lactamase-producing Enterobacteriaceae: changing epidemiology and drug treat-ment choices. Drugs 2010; 70:313–30.
3. Ambrose PG, Bhavnani SM, Rubino CM, et al. Pharmacokinetics-pharmacodynamics of antimicrobial therapy: it’s not just for miceanymore. Clin Infect Dis 2007; 44:79–86.
4. Dudley MN, Ambrose PG. Pharmacodynamics in the study of drugresistance and establishing in vitro susceptibility breakpoints: readyfor prime time. Curr Opin Microbiol 2000; 3:515–21.
5. Thornsberry C, Jones RN, Barry AL, Fuchs PC. Antimicrobial sus-ceptibility tests with cefotoxime and correlation with clinical bacterio-logic response. Rev Infect Dis 1982; 4(suppl):S316–24.
Table 5. Revised Minimum Inhibitory Concentration Breakpoints, Dosage Regimens, and Pharmacodynamic-Pharmacokinetic TargetAttainment for Ceftazidime, Cefepime, and Aztreonam Against Pseudomonas aeruginosa
Drug Dosage
MIC Breakpoints
Susceptible Intermediate Resistant% PK-PD Target Attainmentat Susceptible Breakpointa
Ceftazidime 1 g q6h or ≤8 16 ≥32 100
2 g IV q8hAztreonam 1 g q6h or ≤8 16 ≥32 94
2 g IV q8h
Cefepime 1 g IV q8h or ≤8 16 ≥32 91–952 g IV q12h
Abbreviations: IV, intravenous; MIC, minimum inhibitory concentration; PK-PD, pharmacokinetic/pharmacodynamic; q6h, every 6 hours; q8h, every 8 hours; q12h,every 12 hours.a Percentage PK-PD target attainment represents the percent of simulated patients with f T >MIC (percentage of a dosing interval in which free-drugconcentrations exceed the MIC) of at least 50%.
1308 • CID 2013:56 (1 May) • MEDICAL MICROBIOLOGY
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

6. Andes D, Craig WA. Treatment of infections with ESBL-producingorganisms: pharmacokinetic and pharmacodynamic considerations.Clin Microbiol Infect 2005; 11(suppl 6):10–7.
7. Bhat SV, Peleg AY, Lodise TP, et al. Failure of current cefepime break-points to predict clinical outcomes of bacteremia caused by gram-negative organisms. Antimicrob Agents Chemother 2007; 51:4390–5.
8. Bhavnani S, Ambrose PG, Craig WA, Dudley MN, Jones RN. Out-comes evaluation of patients with ESBL- and non-ESBL-producing Es-cherichia coli and Klebsiella species as defined by CLSI referencemethods: report from the Sentry Antimicrobial Surveillance Program.Diag Microbiol Infect Dis 2006; 54:231–6.
9. Clinical and Laboratory Standards Institute (CLSI). Development of InVitro Susceptibility Testing Criteria and Quality Control Parameters;Approved Guideline—Third Edition. CLSI document M23-A3 (ISBN1-56238-680-8). Clinical and Laboratory Standards Institute, 940 WestValley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2008.
10. Drusano GL, Preston SL, Hardalo C, et al. Use of preclinical data forselection of a phase II/III dose for evernimicin and identification of apreclinical MIC breakpoint. Antimicrob Agents Chemother 2001;45:13–22.
11. Turnidge JD. Cefazolin and Enterobacteriaceae: rationale for revisedsusceptibility testing breakpoints. Clin Infect Dis 2011; 52:917–24.
12. Jones RN, Craig WA, Ambrose PG, Dudley MN, Pottumarthy S.Reevalution of Enterobacteriaceae MIC/disk diffusion zone diameterregression scattergrams for 9 beta-lactams: adjustments of breakpointsfor strains producing extended spectrum beta-lactamases. DiagnMicrobiol Infect Dis 2005; 52:235–46.
13. Kalil AC. Is cefepime safe for clinical use? A Bayesian viewpoint.J Antimicrob Chemother 2011; 66:1207–9.
14. Infectious Diseases Society of America. Alert: antimicrobial suscepti-bility testing. Available at: http://www.idsociety.org/Antimicrobial_Susceptibility_Testing/. Accessed 22 January 2013.
MEDICAL MICROBIOLOGY • CID 2013:56 (1 May) • 1309
at University of W
isconsin-Madison on A
ugust 7, 2013http://cid.oxfordjournals.org/
Dow
nloaded from