-
7/25/2019 bacteraemia endocarditis.pdf
1/13
Daptomycin for endocarditis and/or bacteraemia: a
systematicreview of the experimental and clinical evidence
Matthew E. Falagas1,2*, Konstantina P. Giannopoulou1, Fotinie
Ntziora1
and Konstantinos Z. Vardakas1
1Alfa Institute of Biomedical Sciences (AIBS), Athens, Greece;
2Department of Medicine, Tufts University School
of Medicine, Boston, MA, USA
Received 8 February 2007; returned 21 March 2007; revised 30
March 2007; accepted 11 April 2007
Background: Endocarditis and bacteraemia are devastating
infections with high mortality. Gram-
positive cocci are the most commonly isolated pathogens. In an
era of multidrug-resistant pathogens,
the evaluation of new treatment options is important. Daptomycin
is a cyclic lipopeptide that is activeagainst most of these
pathogens. Furthermore, it is a bactericidal antibiotic, a factor
that is frequently
considered in the choice of treatment of patients with
bacteraemia and endocarditis.
Methods: We performed a systematic review of the evidence for
the effectiveness of daptomycin in the
treatment of patients and animals with endocarditis and/or
bacteraemia. We searched PubMed and
Scopus databases for relevant studies. Case reports, case
series, controlled trials, randomized
controlled trials and comparative studies using experimental
animal models were included.
Results: The most reliable information comes from the single
multicentre randomized controlled trial
conducted on this issue, which showed that daptomycin is a
promising antibiotic for the treatment of
patients with Staphylococcus aureusbacteraemia and endocarditis.
The experimental models indicate
that the combination of daptomycin with rifampicin or gentamicin
can improve outcomes further.
Finally, in several of the published relevant case reports
daptomycin was administered in patients with
haematological malignancies.
Conclusions: Daptomycin is a promising antibiotic that has been
already approved for the treatment ofpatients with right-sided
endocarditis and bacteraemia. However, the available clinical
evidence is
limited and further evaluation of the antibiotic is warranted.
The commonly reported de novo develop-
ment of resistance is a major concern that may limit its use.
More controlled trials are needed,
especially for patients infected with multidrug-resistant
Gram-positive cocci, comparing daptomycin
with other available treatment options, including glycopeptides
and oxazolidinones.
Keywords: lipopeptides, antibiotics, treatment
Introduction
Endocarditis and bacteraemia are devastating infections
associ-
ated with considerable mortality, which reaches 16% to 25% ofthe
affected individuals.
14Their microbiology includes both
Gram-positive and Gram-negative bacteria as well as fungi.
Among the Gram-positive microbes, the highly resistant
staphy-
lococcal and enterococcal species are of extreme importance
because they are related with more severe disease and higher
mortality.5
Antibiotics with bactericidal activity have been considered
the gold standard for the treatment of patients with deep
tissue
infections such as endocarditis and bacteraemia. Daptomycin,
a
fermentation product produced by Streptomyces roseosporus, isa
cyclic lipopeptide antibiotic with potent bactericidal activity
against most Gram-positive organisms, including multiple
antibiotic-resistant strains.6
The activity of daptomycin depends
on the presence of physiological levels of free calcium.
Daptomycin has a novel mechanism of actioninsertion into
and disruption of the functional integrity of the
Gram-positive
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . .
*Correspondence address. Alfa Institute of Biomedical Sciences
(AIBS), 9 Neapoleos Street, 151 23 Marousi,
Greece.Tel:30-694-611-0000; Fax:30-210-683-9605; E-mail:
[email protected]
Journal of Antimicrobial Chemotherapy (2007) 60, 719
doi:10.1093/jac/dkm137
Advance Access publication 4 June 2007
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . .
7
# The Author 2007. Published by Oxford University Press on
behalf of the British Society for Antimicrobial Chemotherapy. All
rights reserved.For Permissions, please e-mail:
[email protected]
-
7/25/2019 bacteraemia endocarditis.pdf
2/13
plasma membranewhich results in rapid loss of membrane
potential, cessation of macromolecular synthesis and cell
death.7
It has been approved for the treatment of patients with skin
and
soft tissues infections. Although it has been recently
approved
for the treatment of patients with bacteraemia and
right-sided
endocarditis, the available evidence to date for its
effectiveness
for the treatment of such patients is limited. Thus, we sought
to
review systematically the available evidence, including
animal
and human studies, regarding the effectiveness and safety
ofdaptomycin for the treatment of endocarditis and bacteraemia.
Methods
Literature search
We carried out a systematic review of the current evidence for
the
effectiveness of daptomycin in the treatment of patients and
animals
with endocarditis and/or bacteraemia. Two authors (K. P. G.
and
F. N.) independently searched PubMed (January 1985 to
January
2007) and Scopus (19862006) in order to identify articles
appro-
priate for inclusion in the review. They also searched reference
lists
of retrieved articles for other relevant papers. Search terms
included
daptomycin, endocarditis, heart disease and bacteremia.
Study selection and data extraction
Potentially relevant studies were selected according to title
and
abstract review of all initially identified articles. Case
reports, case
series, controlled trials, randomized controlled trials (RCTs)
and
studies using experimental animal models were included,
while
review articles were excluded from this review.
Consequently, any study assessing the effectiveness and safety
of
daptomycin for the treatment of endocarditis or bacteraemia was
eli-
gible for inclusion in the review. Animal studies were eligible
for
inclusion in the review only if the studied animals were
randomly
assigned to each treatment group. A group of animals receiving
no
treatment should have been included in the study. No restriction
on
the studied microorganism was set. Decreases in the number
of
colony forming units of the vegetations or sterilization of
the
resected valves were the primary outcomes in these studies.
In case reports and case series, patients receiving treatment
with
daptomycin for endocarditis or bacteraemia were evaluable for
the
analysis, if age, gender, medical history, reason for
daptomycin
administration and/or outcome of the infection were available.
All
patients with endocarditis according to Dukes criteria who
received
daptomycin as a monotherapy or as a part of the regimen were
included.8,9 Bacteraemia was defined as culture of1 blood
sample
that yielded Gram-positive cocci (2 for coagulase-negative
staphy-
lococci) and clinical profile compatible with a diagnosis of
bacterae-
mia with one of the following findings: fever, chills,
leucocytosis
with prominent left shift, changes in vital signs, signs of
septicshock (decreased peripheral perfusion or hypotension) and
petechiae
or purpura.
Case reports and case series were excluded if no data
regarding
the effectiveness of daptomycin for the treatment of patients
with
endocarditis and bacteraemia were available. Reports that used
dap-
tomycin for the treatment of infections due to microorganisms
that
were not susceptible to this antibiotic were excluded. In
addition,
case reports were excluded when the duration of daptomycin
admin-
istration was not adequate for the treatment of such
patients.
All controlled trials and RCTs identified through the search
process were eligible for inclusion in the review. Effectiveness
of
treatment, adverse events due to the studied medications and
mor-
tality were the outcome measures for the trials.
The treatment outcome was defined as cure when the patient
general status had improved, the blood cultures were negative,
and
in the cases of endocarditis the transthoracic echocardiograph
(TTE)
or transoesophageal echocardiograph (TEE) revealed no evidence
of
persistent vegetations on the infected valve according to the
infor-
mation provided by the authors of each case report.
Treatment
outcome was defined as improvement when there were no signs
ofpersistent infection (negative blood cultures, no evidence of
persist-
ent vegetations) but the duration of the treatment period was
not
adequate or the infection relapsed after discharge from hospital
or
the patient died due to other reasons during the same
hospitalization
but there was evidence for resolution of the infection. Duration
of
treatment was considered as adequate when it lasted for a week
or
more. Treatment failure was defined as persistence of signs,
symp-
toms and laboratory or imaging findings of infective
endocarditis or
bacteraemia despite appropriate antibiotic treatment with
daptomy-
cin, relapse of the infection or death due to infective
endocarditis or
bacteraemia or their complications.
ResultsIn total, 102 potentially relevant articles identified
from the
PubMed database; 6 additional articles were identified from
the
Scopus database. Thus, 108 articles were examined for
potential
inclusion in our review. Seventy-three studies were excluded
from the review because they were not directly relevant to
the
focus of our study or because daptomycin administration was
not appropriate. Finally, 35 studies were selected for
further
evaluation and are presented in the Tables below.
Experimental models
A summary of the available evidence regarding the
effectiveness
of daptomycin for the treatment of endocarditis in
experimentalmodels is shown in Table 1.
1020Eleven reports of experimental
models of aortic valve endocarditis in rats and rabbits
comparing
the effectiveness of daptomycin with vancomycin,
teicoplanin,
amoxicillin and penicillin G were conducted. Several strains
of potential pathogens were used. The most common
Gram-positive coccus used in these models was Staphylococcus
aureus [six strains of methicillin-susceptible S. aureus
(MSSA)
and five strains of methicillin-resistant S. aureus (MRSA)]
followed by Enterococcus spp. [three strains of vancomycin-
resistant Enterococcus (VRE) and seven strains of
vancomycin-
susceptibleEnterococcus].
MRSA endocarditis models.In all models, the administration
of
daptomycin resulted in a significant reduction of the
bacterial
counts of the aortic vegetations in comparison with the
no-treatment arm. In addition, two models reported that the
addition of rifampicin in the daptomycin regimen resulted in
a
further significant reduction in the counts of vegetations
when
compared with daptomycin alone.11,12
The assumption that the
administration of daptomycin twice daily could result in a
better
outcome than its administration in a single dose12
was not veri-
fied in other models.13
There was no significant difference in the
effectiveness of daptomycin in comparison with vancomycin
and teicoplanin. The number of sterile valves after
Systematic review
8
-
7/25/2019 bacteraemia endocarditis.pdf
3/13
http://jac.oxfordjournals.org/
-
7/25/2019 bacteraemia endocarditis.pdf
4/13
http://jac.oxfordjournals.org/
-
7/25/2019 bacteraemia endocarditis.pdf
5/13
administration of daptomycin varied between models (range
10% to 100%), but there was no difference between daptomycin
and glycopeptides in the individual models. None of the
models
compared daptomycin with linezolid or quinupristin
dalfopristin.
MSSA endocarditis models. The available data from experimen-
tal models are contradictory. In one model, the administration
of
daptomycin twice daily (5 mg/kg every 12 h) was more effectivein
reducing bacterial counts of vegetations than 10 mg/kg of
daptomycin once daily and vancomycin twice daily.12
In two
other models, daptomycin in adequate dosage was either more
effective than or at least as effective as vancomycin,
depending
on the strain used for infection.15,16
Finally, daptomycin was as
effective as antistaphylococcal penicillins in reducing
bacterial
counts of aortic valve vegetations.15,18
Accordingly, more
excised valves were sterilized after the administration of
dapto-
mycin than with vancomycin; on the contrary,
antistaphylococ-
cal penicillins were as effective as daptomycin on this
issue.
Enterococcus spp. endocarditis models. Enterococcus faecalis
was the infecting organisms in six models.10,14,1720
In all of
them, treatment with daptomycin was as effective as
glycopep-tides and penicillins in reducing the bacterial count of
aortic
valve vegetations. Daptomycin was more effective than amoxi-
cillin or ampicillin alone when penicillin-resistant isolates
were
used, but this difference was eliminated when the
combination
of amoxicillin with gentamicin or ampicillin with sulbactam
was
used.
VRE endocarditis models. Two models used VRE faecium as
the offending organism10,13
Daptomycin was as effective as tei-
coplanin for the reduction of bacterial counts of aortic
valve
vegetations. The combination of daptomycin with gentamicin
was the single most effective regimen that resulted in a
signifi-
cant reduction of the bacterial counts of the vegetations as
well
as an increased number of sterile valves. Daptomycin was
moreeffective than amoxicillin for the treatment of endocarditis
due
to VRE faecium, but it was as effective as amoxicillin for
VRE
faecalisendocarditis.10
Bacteraemia models. One experimental model with S. aureus
bacteraemia has been conducted, in which daptomycin was com-
pared with vancomycin.21
Two different dosage regimens were
used for each antibiotic. There was no significant difference
in
survival in any of the four treatment groups.
Case reports and case series
Endocarditis. A summary of the evidence from published case
reports and case series to date with use of daptomycin for
the
treatment of patients with bacterial endocarditis is shown
in
Table 2.2233
A total of 19 cases were retrieved. Information
regarding the demographics, clinical data, type of heart
valve
and other variables were not reported in a few cases, thus
the
denominator varies in the following proportions of cases;
47.3%
(9/19) of the affected individuals were men. The median age
of
patients was 60.5 years (range 1392). Prosthetic valve
infective
endocarditis accounted for 10.5% (2/19) of cases. Three
patients
had undergone bone marrow transplantation, three patients
had
chronic renal failure, two had coronary artery disease and
two
had systemic lupus erythematosus. No history was available
for
seven of the included patients.
Blood cultures were performed and proved positive for all
but one of the reviewed patients. S. aureus was the
predominant
isolated pathogen (seven isolates of MRSA and five isolates
of
MSSA) followed by VRE (four isolates). Vancomycin-
susceptible E. faecalis, coagulase-negative Staphylococcus
and
Corynebacterium striatum were the remaining isolates. One of
the blood cultures yielded two microorganisms (MRSA andE.
faecalis).
In most cases, the reason for administration of daptomycin
was treatment failure with other antibiotics (mainly
vancomycin
15/19, 79%) or combinations of antibiotics. In one case,
dapto-
mycin was administered because there was increased
possibility
for adverse effects from linezolid administration to a
patient
with splenectomy and bone marrow transplantation. In another
patient, daptomycin was administered empirically because a
sta-
phylococcal infection was presumed. Finally, no reason was
reported for one case.
The median duration of daptomycin administration was 28
days (range 8 91). The outcome at the end of treatment was
good for the majority of patients with endocarditis treated
with
daptomycin (11/19 cases, 57.8%). One of these patients died
ofco-morbidity during the follow-up period and one more due to
relapse of the infection. The general status as well as the
labora-
tory and/or imaging findings of three (15.8%) additional
patients
improved after the administration of daptomycin; one of
these
patients died after withdrawal of life support due to severe
hae-
morrhagic pancreatitis and acute respiratory distress
syndrome.
Failure of treatment with daptomycin was seen in five cases
(26.3%); four of these patients died. The overall mortality of
the
reviewed case reports was 38.9% (7/18).
Information regarding the possible adverse effects
associated
with daptomycin administration was available in 10 cases.
Adverse
effects developed in five patients (50). Increase in the levels
of
creatine kinase (CK) was reported in four of them; the
remaining
patient developed mild deterioration of renal function.
Twopatients discontinued treatment with daptomycin. One of
these patients required intubation after the development of
eosinophilic pneumonia that was attributed to the daptomycin
administration. None of the treated isolates developed
resistance
or decreased susceptibility to daptomycin.
Bacteraemia. A summary of the evidence from published case
reports and case series to date with use of daptomycin for the
treat-
ment of patients with bacteraemia is shown in Table
3.28,3444
A total of 41 cases was retrieved. Information regarding the
demo-
graphics, clinical data, type of heart valve and other
variables
were not reported in a few cases, thus the denominator varies
in
the following proportions of cases; 58.5% (24/41) of the
affected
individuals were men. The median age of patients was 58
years
(range 18 87). Sixteen patients had haematological diseases
(including acute myeloid leukaemia) and nine of them had
under-
gone bone marrow transplantation, four patients had chronic
renal
failure, four had bone and joint infections, two had liver
cirrhosis
and two had pyelonephritis. No history was available for 12 of
the
included patients.
Blood cultures were performed and proved positive for all
but one of the reviewed patients. VRE (24/47 isolates,
51.1%)
was the predominant isolated pathogen followed by S. aureus
[12 isolates of MRSA (25.5%) and 2 isolates of MSSA (4.3%)].
Systematic review
11
-
7/25/2019 bacteraemia endocarditis.pdf
6/13
http://jac.oxfordjournals.org/
-
7/25/2019 bacteraemia endocarditis.pdf
7/13
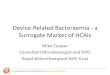
Mohanet al.30 M/75 right knee replacement, DM, CAD,
CHF, CABG, AV replacement,
non-ST elevation MI
prostheti c AV MRSA vancomyci n (9),
linezolid (2)
treatment failure,
patient refused
surgery
6 mg/kg/day (11) no
Shah and Murillo31 F/46 haemodialysis-dependent CRF,
removal of infected femoral
graft used to repair a
pseudoaneurysm
TV C. striatum linezolid, vancomycin treatment failure,
allergy to
vancomycin
6 mg/kg/every 2
days (42)
daptomycin/
rifampicin
no
Stevens and
Edmond32F/25 SLE, ESRD, MV regurgitation,
haemolytic anaemia, MV
replacement
prostheti c MV VR Efaecium l in ez ol id ( 10 ) n ot a ca nd id
at e f or
surgery,
possible
treatment failure
8 mg/kg/day
(14, 77)
daptomycin/
gentamicin/
rifampicin
no
Veligandlaet al.33 F/26 splenectomy, autologous BMT,
ITP, SLE, disc herniation
MV MRSA,
E. faecalis
quinupristin/dalfopristin
(18), linezolid/tobrarmycin/
rifampicin (10)
high risk for
adverse effectsrelated to
linezolid
6 mg/kg/day (15) NA
AE, adverse effects; AF, atrial fibrillation; AV, aortic valve;
CA, coronary artery; CK, creatine kinase; iv, intravenous; MV,
mitral valve; NA, not availablTV, tricuspid valve.Co-morbidities:
AML, acute myelogenous leukaemia; ARDS, acute respiratory distress
syndrome; BMT, bone marrow transplantation; CABG, coronary artCHF,
congestive heart failure; CML, chronic myelogenous leukaemia; CRF,
chronic renal failure; DM, diabetes mellitus; ESRD, end stage renal
disease; IE-tive endocarditis with unknown valvular involvement;
ITP, idiopathic thrombocytopenic purpura; MI, myocardial
infarction; MOF, multiple organ failurRA, rheumatoid arthritis;
SLE, systemic lupus erythematosus; TKP, total knee
prosthesis.Responsible pathogens: CoNS, coagulase negative
Staphylococcus; MRSA (SCV), methicillin-resistant S. aureus (small
colony variant); MSSA, methicresistant Enterococcus.aPatient
developed complications (5 mm mobile density on the aortic valve
verified by transoesophageal echocardiography, C3C6 osteomyelitis,
a posteriosplenic infarct and progressive renal failure) while
being treated for bacteraemia that necessitated cardiac and
neurosurgical interventions.b
Patient was discharged and readmitted.13
byguestonDecember13,2015 http://jac.oxfordjournals.org/
Downloadedfrom
http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/
-
7/25/2019 bacteraemia endocarditis.pdf
8/13
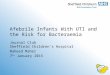
Table 3. Case reports and case series regarding the use of
daptomycin for the treatment of patients with bacteraemia
Referen ce Sex/age Co -morbidity Site of in fection Isolated
path ogens
Previous
antibiotic
treatment
(duration, days)
Reason for
daptomycin
administration
Dosage and
duration of
daptomycin
treatment (days)
Development
of daptomycin
resistance
during
treatment
Burns34 M/54 morbid obesity, chronic
right hip arthroplasty
infection
bacteraemia MRSA levofloxacin,
vancomycin
(3),vancomycin/
gentamicin (4)
treatment failure 6 mg/kg/day
daptomycin/
rifampicin/vancomycin/
gentamicin (4),
6 mg/kg/every 2
days
daptomycin/
rifampicin (38),
6 mg/kg/day
daptomycin/
rifampicin (14)
no
Greenet al.35 F/62 myelofibrosis, allogenic
bone marrow transplant,
acute-on-chronic RF,
haemodialysis
bacteraemia P. aeruginosa,
K. pneumoniae,
Enterococcus
spp., E. durans
cefazolin,
levofloxacin
treatment failure
and known
history of
VRE
6 mg/kg/every 2
days (20)
yes
Kvirikadze
et al.36
M/74 CAD, HT, DM, AML bacteraemia VRE faecium ceftazidime
treatment failure 4 mg/kg/day (14) no
F/58 Endometrial Ca, total
hysterectomy, bilateral
salpingo-oophorectomy,
chemotherapy, acute
cholecystitis,
percutaneous
cholecystectomy
bacteraemia methicillin-resistant
Staphylococcus
lugdunensis,
VRE faecium
vancomycin/
piperacillin/
tazobactam/
tobramycin
treatment failure 4 mg/kg/day (26) no
Martyet al.37 M/61 AML, non-myeloablative
allogeneic HscT,
GVHD
bacteraemia,
osteomyelitis,
discitis
MRSA linezolid (4),
vancomycin/
gentamicin (3)
treatment failure 6 mg/kg/day
daptomycin/
gentamicin
(21,6)
yes
Papadopoulos
et al.38
F/45 refractory AML,
chemotherapy
bacteraemia VRE faecium linezolid (14),
linezolid/
aztreonam/
levofloxacin/
aciclovir/
amphotericin/
azithromycin
treatment failure daptomycin/
meropenem/
caspofungin/
metronidazole/
levofloxacin/
aciclovir 6 mg/
kg/day (10)
NA
Poutsiakaet al.
39 M/49 AML, allogenic HscT bacteraemia VRE faecium none
according toprotocol (B)a6 mg/kg/day (1),
then 3 mg/kg/
every 12 days
(15)
NA
M/70 AML bacteraemia VRE faecium none according to
protocol (B)a
1st 6 mg/kg/day
(1), then
2.25 mg/kg/
every 18 h (13)
2nd 6 mg/kg/
day (1), then
2.25 mg/kg/
every 18 h, then
4 mg/kg/day
(14)
NA
14
byguestonDecember13,2015 http://jac.oxfordjournals.org/
Downloadedfrom
http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/http://jac.oxfordjournals.org/
-
7/25/2019 bacteraemia endocarditis.pdf
9/13
http://jac.oxfordjournals.org/
-
7/25/2019 bacteraemia endocarditis.pdf
10/13
http://jac.oxfordjournals.org/
-
7/25/2019 bacteraemia endocarditis.pdf
11/13
Gram-negative bacteria (three isolates), coagulase-negative
Staphylococcus (two isolates), vancomycin-resistant
Leuconostoc mesenteroides (two isolates), vancomycin-
susceptibleEnterococcus durans (one isolate) and
Streptococcus
pneumoniae(one isolate) were the remaining isolates.
In most cases, the reason for administration of daptomycin
was treatment failure with another antibiotic [mainly
vancomy-
cin (16/33, 48.5%) and linezolid (8/33, 24.2%)] or a
combination
of antibiotics. In 11 cases, daptomycin was administered
accord-ing to a therapeutic protocol. No reason was reported for
five
cases.
The median duration of daptomycin administration was 14
days (range 3 56). The outcome at the end of treatment was
good for the majority of patients with bacteraemia treated
with
daptomycin (27/41 cases, 65.9%). One of these patients died
of
co-morbidity during the follow-up period. Failure of
treatment
with daptomycin was seen in 14 cases (34.1%); 10 of these
patients died. The overall mortality of the reviewed case
reports
was 26.8% (11/41). Adverse effects developed in six patients
for
whom data on this issue were available. Increase in the levels
of
creatinine kinase (CK) was reported in one of them; the
other
patients developed renal failure. Five of the treated
isolates
developed resistance to daptomycin during the treatment
period.However, no data were available for 32 patients.
Randomized controlled trials
Only one open-label RCT45
was conducted comparing daptomy-
cin with antistaphylococcal penicillins or vancomycin
(standard
therapy), in combination with gentamicin for the treatment
of
patients with endocarditis or bacteraemia due to
methicillin-
susceptible and methicillin-resistant S. aureus. Patients were
ran-
domly assigned with the use of a centralized
computer-generated
block randomization schedule that was designed to achieve a
1:1
ratio of patients. All data were reviewed regularly by an
indepen-
dent committee. Of the 246 randomized patients, 235 were
eli-
gible for the analysis of effectiveness. Overall, daptomycin
andstandard therapy were equally effective for the treatment of
patients with endocarditis and bacteraemia (61% versus 60.9%
at the end of treatment and 44.2% versus 41.7% at the
test-of-cure visit 42 days after the end of treatment).
Success
rates favoured daptomycin over vancomycin among patients
who were infected with MRSA (44.4% for daptomycin versus
31.8% for standard therapy, P 0.28), but were higher among
patients receiving standard therapy for MSSA infection
(44.6%
for daptomycin versus 48.6% for standard therapy, P 0.74).
The authors did not distinguish between patients with
definite
endocarditis and bacteraemia on this issue. In patients with
base-
line diagnosis of definite and possible MRSA endocarditis,
dap-
tomycin was also more effective than standard therapy, but
without statistical significance (41.7% versus 28.9%).
Daptomycin was as effective as standard therapy for the
treat-
ment of patients with staphylococcal (both MRSA and MSSA)
definite endocarditis (32.1% versus 36.0%) and bacteraemia
(47.8% versus 43.3%). Patients with MRSA bacteraemia and
right-sided endocarditis showed similar success rates when
treated with either daptomycin or vancomycin, suggesting
that
daptomycin may be considered an alternative to vancomycin in
the management of these infections.
Elevated CK levels were reported in more patients treated
with daptomycin (6.7% versus 0.9%, P 0.04), while more
patients receiving standard therapy had renal impairment
(18.1%
versus 6.7%, P 0.009). The number of patients treated with
gentamicin was higher in the standard therapy group (93%
versus 0.8%). The MIC for seven isolates increased from
base-
line values in patients treated with daptomycin, but none of
these isolates developed resistance to daptomycin; however,
six
of these seven patients had microbiological failure. Increase
in
the MIC of vancomycin was also noticed in four isolates.
Finally, mortality was similar between the compared regimens(15%
versus 16%).
Several limitations of this RCT should be taken into
account.
First, the number of enrolled patients with left-sided S.
aureus
endocarditis was very small and the treatment success in
this
group of patients was very low (11.1% versus 22.2% for
dapto-
mycin and standard therapy, respectively). Second, although
not
statistically significant, treatment failure due to persistent
or
relapsingS. aureus infection was more common in the daptomy-
cin than the standard therapy group (15.8% versus 9.6%, P
0.17). On the other hand, treatment failure due to
discontinu-
ation of antibiotic administration because of adverse
effects
(mainly impairment of renal function) was more common in the
standard therapy than the daptomycin group (14.8% versus
6.7%, P 0.06); gentamicin was administered to more patientsin
the standard therapy group. Third, the criteria for treatment
success were very strict and consequently, the reported
clinical
success was very low. The authors considered as treatment
failure all patients that did not have a blood culture drawn at
the
test-of-cure visit 42 days after the end of treatment,
regardless of
their clinical status. Similarly, all patients who
discontinued
treatment due to adverse effects associated with study
antibiotics
were considered as treatment failures. Finally, only patients
with
S. aureusinfections were enrolled in this RCT.
Discussion
The available evidence regarding the treatment of patients
withendocarditis and bacteraemia due to Gram-positive cocci
with
daptomycin is limited. The most reliable information comes
from the single multicentre RCT conducted on this issue,
which
had some important limitations. The most important of these
limitations was the small number of enrolled patients with
final
diagnosis of endocarditis and especially those with
left-sided
endocarditis. However, this RCT provides valuable
information
regarding patients with bacteraemia. Daptomycin seems to be
an
equal alternative to vancomycin and antistaphylococcal
penicil-
lins for the treatment of patients with S. aureus
bacteraemia.
In the majority of the relevant case reports, daptomycin was
administered when treatment of patients with endocarditis or
bacteraemia with other potentially effective antibiotics
(includ-
ing glycopeptides and linezolid) had failed. Thus far,
vancomy-
cin and, in patients who can not tolerate vancomycin or
treatment had failed, linezolid are the recommended
antibiotics
for the treatment of patients with endocarditis due to
multidrug-resistant Gram-positive cocci according to the
American Heart Association.46,47
The available data suggest that
daptomycin could also be considered for the treatment of
patients with endocarditis due to Gram-positive cocci, but
more
data are necessary.
In the published case reports, several patients receiving
treat-
ment with daptomycin for bacteraemia or endocarditis had a
Systematic review
17
-
7/25/2019 bacteraemia endocarditis.pdf
12/13
history of acute leukaemia or had received haemopoietic
stem-
cell transplantation. These patients are at higher risk for
develop-
ment of infections and increased mortality. Daptomycin seems
to be an alternative choice for the treatment of such
patients,
especially when treatment with vancomycin has failed.
Although linezolid can also be effective, its administration for
a
long period is associated with haematological adverse
effects
that may prohibit its use in patients with haematological
abnormalities.The available experimental models suggested that
the combi-
nation of daptomycin with rifampicin or gentamicin could
enhance its activity in vivo against MRSA and VRE. However,
in the single RCT conducted on the issue, daptomycin was
barely ever combined with any other antibiotic. On the
contrary,
gentamicin was added in 93% of the patients treated with
vanco-
mycin or antistaphylococcal penicillins. Whether this could
explain the non-significant more treatment failures reported
for
daptomycin in patients with persistent S. aureus infections
enrolled in the RCT should be an issue of further research.
Data
from animal studies can be used as a guide for future
research,
but should never be considered as strong evidence for
treatment
options in humans.
The main adverse effect noted in the studied patients
wasmyopathy associated with an increase in CK serum levels.
Animal studies have demonstrated that myopathy was specific
to
skeletal muscles. The skeletal myopathy was associated with
minimal degeneration that was associated with inflammation
at
high doses; the inflammation did not further contribute to
muscle damage, and there was regeneration without
fibrosis.48
In
one of the case reports, the authors stated that
rhabdomyolysis
also occurred. Others also reported cases of renal damage
associated with the use of daptomycin. It should be noted
that
increased caution is required in treating patients with renal
dys-
function because prolonged exposure to higher serum levels
of
daptomycin may elicit myopathy, which in turn may
deteriorate
renal function.
Development of resistance is among the most importantissues
regarding antibiotic use. There are several reports of
increase in the minimal inhibitory concentration or de novo
development of resistance during treatment with daptomycin.
In
many of these reports, these phenomena were associated with
treatment failures or even death. It is noteworthy that in
these
reports the duration of daptomycin administration was
relatively
short (range 14 27 days). Future studies should try to
evaluate
whether the combination of daptomycin with other antibiotics
effective against Gram-positive bacteria would reduce the
resistance rates reported to date for daptomycin.
Further research is needed regarding the most appropriate
regimen for the treatment of patients with endocarditis due
to
resistant Gram-positive cocci like MRSA,
methicillin-resistant
coagulase-negative staphylococci and VRE. The currently
avail-
able antibiotics (vancomycin, teicoplanin, linezolid,
daptomycin,
tigecycline and dalbavancin) are promising, but RCTs compar-
ing these agents are lacking while treatment failure and
mor-
tality remain high. Therefore, more data are also needed
regarding the effectiveness of combination therapy with
rifampi-
cin and/or aminoglycosides.
In conclusion, although daptomycin has already been
approved for the treatment of patients with right-sided
endocar-
ditis and bacteraemia, the available evidence is limited and
further evaluation of the antibiotic is warranted. The
commonly
reported de novo development of resistance is a major
concern
that may limit its use for the treatment of life-threatening
infec-
tions. The combination of daptomycin with other antibiotics
active against multi-antibiotic resistant strains could result
in
better outcomes and fewer cases of daptomycin-resistant
Gram-positive cocci. However, there are no clinical data
support-
ing this issue. Accordingly, daptomycin should be used with
caution and preferably when standard treatments have failed,
in
order to preserve this potentially effective drug for future
use.
Funding
None.
Transparency declarations
None to declare.
References
1. Moreillon P, Que YA. Infective endocarditis. Lancet2004;
363:
13949.
2. Mylonakis E, Calderwood SB. Infective endocarditis in
adults.
N Engl J Med2001;345: 131830.
3. Habib G. Management of infective endocarditis. Heart2006;
92:
12430.
4. Laupland KB, Gregson DB, Zygun DAet al. Severe
bloodstream
infections: a population based assessment. Crit Care Med2004;
32:
9927.
5. Cosgrove SE, Sakoulas G, Perencevich ENet al. Comparison
of
mortality associated with methicillin-resistant and methicillin
sensitive
Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect
Dis
2003;36: 539.6. Critchley IA, Draghi DC, Sahm DF et al. Activity
of daptomycin
against susceptible and multidrug-resistant Gram-positive
pathogens
collected in the SECURE study (Europe) during 20002001.
J Antimicrob Chemother2003;51: 63949.
7. Silverman JA, Perlmutter NG, Shapiro HM. Correlation of
dapto-
mycin bactericidal activity and membrane depolarization in
Staphylococcus aureus. Antimicrob Agents Chemother 2003; 47:
253844.
8. Durack DT, Lukes AS, Bright DK. New criteria for diagnosis
of
infective endocarditis: utilization of specific
echocardiographic findings.
Duke Endocarditis Service.Am J Med1994;96: 2009.
9. Li JS, Sexton DJ, Mick N et al. Proposed modifications to
the
Duke criteria for the diagnosis of infective endocarditis. Clin
Infect Dis
2000;30: 6338.
10. Vouillamoz J, Moreillon P, Giddey M et al. Efficacy of
daptomy-cin in the treatment of experimental endocarditis due to
susceptible
and multidrug-resistant enterococci.J Antimicrob
Chemother2006;58:
120814.
11. Sakoulas G, Eliopoulos GM, Alder J et al. Efficacy of
daptomy-
cin in experimental endocarditis due to
methicillin-resistant
Staphylococcus aureus. Antimicrob Agents Chemother 2003; 47:
17148.
12. Voorn GP, Kuyvenhoven J, Goessens WH et al. Role of
toler-
ance in treatment and prophylaxis of experimental
Staphylococcus
aureus endocarditis with vancomycin, teicoplanin, and
daptomycin.
Antimicrob Agents Chemother1994;38: 48793.
Systematic review
18
-
7/25/2019 bacteraemia endocarditis.pdf
13/13
13. Caron F, Kitzis MD, Gutmann L et al. Daptomycin or
teicoplanin
in combination with gentamicin for treatment of experimental
endocar-
ditis due to a highly glycopeptide-resistant isolate of
Enterococcus
faecium.Antimicrob Agents Chemother1992;36: 26116.
14. Ramos MC, Grayson ML, Eliopoulos GM et al. Comparison of
daptomycin, vancomycin, and ampicillin-gentamicin for treatment
of
experimental endocarditis caused by penicillin-resistant
enterococci.
Antimicrob Agents Chemother1992;36: 18649.
15. Cantoni L, Glauser MP, Bille J. Comparative efficacy of
dapto-
mycin, vancomycin, and cloxacillin for the treatment of
Staphylococcus
aureusendocarditis in rats and role of test conditions in this
determi-
nation.Antimicrob Agents Chemother1990;34: 234853.
16. Kaatz GW, Seo SM, Reddy VN et al. Daptomycin compared
with teicoplanin and vancomycin for therapy of experimental
Staphylococcus aureus endocarditis. Antimicrob Agents
Chemother
1990;34: 20815.
17. Hindes RG, Willey SH, Eliopoulos GMet al. Treatment of
exper-
imental endocarditis caused by a b-lactamase-producing strain
of
Enterococcus faecalis with high-level resistance to
gentamicin.
Antimicrob Agents Chemother1989;33: 101922.
18. Kennedy S, Chambers HF. Daptomycin (LY146032) for
preven-
tion and treatment of experimental aortic valve endocarditis in
rabbits.
Antimicrob Agents Chemother1989;33: 15225.
19. Bush LM, Boscia JA, Kaye D. Daptomycin (LY146032)
treatmentof experimental enterococcal endocarditis. Antimicrob
Agents
Chemother1988;32: 87781.
20. Eliopoulos GM, Willey S, Reiszner E et al. In vitro and in
vivo
activity of LY 146032, a new cyclic lipopeptide antibiotic.
Antimicrob
Agents Chemother1986;30: 5325.
21. Smith K, Cobbs G, Dill R et al. Daptomycin versus
vancomycin
treatment for Staphylococcus aureus bacteremia in a murine
model.
Chemotherapy1990;36: 42834.
22. Akins RL, Haase MR, Levy EN. Pharmacokinetics of
daptomycin
in a critically ill adolescent with vancomycin-resistant
enterococcal
endocarditis.Pharmacotherapy2006;26: 6948.
23. Carlyn CJ, Baltch AL, George MJ et al. Daptomycin in the
treat-
ment of persistent bacteremia with invasive complications caused
by a
small colony variant of methicillin-resistant Staphylococcus
aureus in
an orthopedic patient. Infect Dis Clin Pract2006;14: 3948.24.
Cunha BA, Eisenstein LE, Hamid NS. Pacemaker-induced
Staphylococcus aureus mitral valve acute bacterial endocarditis
com-
plicated by persistent bacteremia from a coronary stent: cure
with pro-
longed/high-dose daptomycin without toxicity. Heart Lung 2006;
35:
20711.
25. Hayes D, Jr, Anstead MI, Kuhn RJ. Eosinophilic pneumonia
induced by daptomycin.Infect2007;54: e2113.
26. Hirschwerk D, Ginocchio CC, Bythrow M et al. Diminished
sus-
ceptibility to daptomycin accompanied by clinical failure in a
patient
with methicillin-resistant Staphylococcus aureus bacteremia.
Infect
Control Hosp Epidemiol2006;27: 3157.
27. Paez AS, Brown RB, Wilk PA et al. Rapid loss of
daptomycin
susceptibility in methicillin-resistant Staphylococcus aureus
blood
culture isolates from an infective endocarditis patient. Inf Dis
Clin
Practice2006;14: 3224.
28. Segreti JA, Crank CW, Finney MS. Daptomycin for the
treatment
of gram-positive bacteremia and infective endocarditis: a
retrospective
case series of 31 patients. Pharmacotherapy2006;26: 34752.
29. Cunha BA, Hamid N, Kessler H et al. Daptomycin cure
after
cefazolin treatment failure of methicillin-sensitive
Staphylococcus
aureus(MSSA) tricuspid valve acute bacterial endocarditis from a
per-
ipherally inserted central catheter (PICC) line. Heart Lung2005;
34:
4427.
30. Mohan SS, McDermott BP, Cunha BA. Methicillin-resistant
Staphylococcus aureus prosthetic aortic valve endocarditis
with
paravalvular abscess treated with daptomycin. Heart Lung2005;
34:
6971.
31. Shah M, Murillo JL. Successful treatment of
Corynebacterium
striatum endocarditis with daptomycin plus rifampin. Ann
Pharmacother2005;39: 17414.
32. Stevens MP, Edmond MB. Endocarditis due to vancomycin-
resistant enterococci: case report and review of the literature.
Clin
Infect Dis2005;41: 113442.
33. Veligandla SR, Louie KR, Malesker MA et al. Muscle
painassociated with daptomycin.Ann Pharmacother2004;38: 18602.
34. Burns CA. Daptomycin-rifampin for a recurrent MRSA joint
infec-
tion unresponsive to vancomycin-based therapy. Scand J Infect
Dis
2006;38: 1336.
35. Green MR, Anasetti C, Sandin RL et al. Development of
dapto-
mycin resistance in a bone marrow transplant patient with
vancomycin-
resistant Enterococcus durans. J Oncol Pharm Pract 2006; 12:
17981.
36. Kvirikadze N, Suseno M, Vescio T et al. Daptomycin for
the
treatment of vancomycin resistant Enterococcus faecium
bacteremia.
Scand J Infect Dis2006;38: 2902.
37. Marty FM, Yeh WW, Wennersten CB et al. Emergence of a
clini-
cal daptomycin-resistant Staphylococcus aureus isolate during
treat-
ment of methicillin-resistant Staphylococcus aureus bacteremia
and
osteomyelitis. J Clin Microbiol2006;44: 5957.
38. Papadopoulos S, Ball AM, Liewer SE et al. Rhabdomyolysis
during therapy with daptomycin. Clin Infect Dis2006;42:
e10810.
39. Poutsiaka DD, Skiffington S, Miller KB et al. Daptomycin in
the
treatment of vancomycin-resistantEnterococcus faeciumbacteremia
in
neutropenic patients.J Infect2007;54: 56771.
40. Mangili A, Bica I, Snydman DR et al.
Daptomycin-resistant,
methicillin-resistant Staphylococcus aureus bacteremia. Clin
Infect Dis
2005;40: 105860.
41. Munoz-Price LS, Lolans K, Quinn JP. Emergence of
resistance
to daptomycin during treatment of vancomycin-resistant
Enterococcus
faecalisinfection.Clin Infect Dis2005;41: 5656.
42. Lewis JS, 2nd, Owens A, Cadena J et al. Emergence of
dapto-
mycin resistance in Enterococcus faeciumduring daptomycin
therapy.
Antimicrob Agents Chemother2005;49: 16645.
43. Golan Y, Poutsiaka DD, Tozzi S et al. Daptomycin for
line-
related Leuconostoc bacteraemia. J Antimicrob Chemother2001;
47:
3645.
44. Garrison MW, Rotschafer JC, Crossley KB. Suboptimal effect
of
daptomycin in the treatment of bacteremias. South Med J1989;
82:
14145.
45. Fowler VG, Jr, Boucher HW, Corey GR et al . S. aureus
Endocarditis, Bacteremia Study Group. Daptomycin versus
standard
therapy for bacteremia and endocarditis caused by
Staphylococcus
aureus.N Engl J Med2006;355: 65365.
46. Baddour LM, Wilson WR, Bayer AS et al. Infective
endocarditis:
diagnosis, antimicrobial therapy, and management of
complications: a
statement for healthcare professionals from the Committee on
Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council
onCardiovascular Disease in the Young, and the Councils on
Clinical
Cardiology, Stroke, and Cardiovascular Surgery and
Anesthesia,
American Heart Association: endorsed by the Infectious
Diseases
Society of America.Circulation2005;111: e394434.
47. Falagas ME, Manta KG, Ntziora F et al. Linezolid for the
treat-
ment of patients with endocarditis: a systematic review of the
published
evidence.J Antimicrob Chemother2006;58: 27380.
48. Oleson FB, Jr, Berman CL, Kirkpatrick JB et al.
Once-daily
dosing in dogs optimizes daptomycin safety. Antimicrob
Agents
Chemother2000;44: 294853.
Systematic review
19