-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
1/14
173
CHAPTER 8
Bacterial and transplacentalinfection
Mark Anthony and James Gray
CONTENTS
Introduction
Bacterial structure and classifi cation
Streptococci explained
Genes and genomes
Antibiotic structure and mechanismsof action
Bacterial resistance
Antibiotic choice in neonatal units
Routes of infection
Early-onset sepsis
Mode of acquisition of infection
Group B streptococcal infection
Other bacterial causes of early-
onset sepsis
Late-onset sepsis
Low-virulence commensals
Pathogenic bacteria
Transplacental infections
Toxoplasma gondiiCytomegalovirus (CMV)
Varicella-zoster virus (VZV)
Listeria monocytogenes
Summary
Key points for practice
INTRODUCTION
The perinatal period is the highest-risk period in life for
acquiring a serious bacterialinfection. In almost every measured
aspect, babies immune responses are less thanthose of children and
adults, including macrophage and neutrophil killing,
cytokineresponses, and antibody production. Transplacental
acquisition of antibody, andantibody and macrophages from colostrum
all help to counter this relative immunedeficit in term babies.
Preterm babies, though, receive less protective maternal anti-body
and have greater immune immaturity. Skin and the normal bacterial
flora help
defend against pathogenic bacterial invasion, but the skin
barrier is often breachedby intravenous lines in premature babies,
and the flora is frequently abnormal due
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
2/14
174 A FOUNDATION FOR NEONATAL CARE
to early antibiotic selective pressure and exposure to
antibiotic-resistant bacteriaresident in neonatal units. For all of
these reasons, babies and especially those bornpremature are
vulnerable to infection.
BACTERIAL STRUCTURE AND CLASSIFICATION
Bacteria are differentiated into two broad groups by Grams
stain, named after theeighteenth-century Dane, Hans Christian Gram.
Bacteria are categorised by theirability to retain colour after
crystal violet staining and acetone destaining. Bacteriathat retain
the stain have a thick outer peptidoglycan cell wall and are
referred toas Gram-positive bacteria, whereas those that lose
colour and take up a pink basicfuchsin counter-stain have a thinner
cell wall and are referred to as Gram-negative.Bacteria can also be
differentiated by their shape into cocci or bacilli. All of
thecommon neonatal bacterial pathogens are either Gram-positive
cocci or Gram-negative bacilli, with the exception ofL.
monocytogenes, which is a Gram-positive
bacillus (see Table 8.1).
TABLE 8.1 Common Gram-positive and Gram-negative neonatal
bacterial
pathogens
Classification Bacterial species Commonly used
antibiotics
Gram-positive cocci
causing chorioamnionitis
Streptococcus agalactiae
(group B streptococcus)
Benzylpenicillin
Cefotaxime*
Gram-positive cocci
causing late-onset sepsis
Staphylococcus epidermidis
(coagulase negative staphylococcus)Staphylococcus aureus
(coagulase positive staphylococcus)
Enterococcus spp.
Streptococcus agalactiae
Vancomycin/
TeicoplaninFlucloxacillin
Vancomycin/
Teicoplanin
Benzylpenicillin
Cefotaxime*
Gram-positive bacilli
causing fetal/early-onset
neonatal sepsis
Listeria monocytogenes Ampicillin**
Gram-negative bacillicausing chorioamnionitis
Escherichia coli GentamicinCefotaxime***
Gram-negative bacilli
causing late-onset sepsis
Escherichia coli
Pseudomonas aeruginosa
Klebsiella pneumoniae
Serratia marcescens
Enterobacter cloacae
Gentamicin
Cefotaxime***
Meropenem****
Notes:
* Cefotaxime used when meningitis is suspected or proven.
** Listeria monocytogenes is not sensitive to
cephalosporins.
*** Cefotaxime is used with an aminoglycoside to give double
Gram-negative cover or when meningitisis suspected or proven.
**** Meropenem is used when an organism is resistant to
aminoglycosides and/or cephalosporins.
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
3/14
BACTERIAL AND TRANSPLACENTAL INFECTION 175
The distinction between Gram-positive cocci and Gram-negative
bacilli is animportant one because Gram staining assists with early
identification of the organ-ism, and because different antibiotics
are effective against these two broad categoriesof bacteria. Thus,
Gram-stain information can direct initial antibiotic choice.
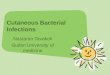
The cell walls of Gram-positive and Gram-negative bacteria
differ in the quantityand cellular location of the cell wall
peptidoglycan (see Figure 8.1). In Gram-positivebacteria, a thick
layer of peptidoglycan lies outside of a single bacterial cell
mem-brane. In this location, the enzymes that create the
petidoglycan are vulnerable toattack by-lactam and glycopeptide
antibiotics. Gram-negative bacteria, in contrast,have a thin
peptidoglycan cell wall that is sandwiched between inner and
outermembranes. In this location the peptidoglycan matrix is hidden
from immediateaccess by cell-wall-acting antibiotics, which must
first cross the outer membrane toexert their action.
FIGURE 8.1 Bacterial cell wall composition
Streptococci explained
Streptococcal colonies when cultured on sheep blood agar produce
either nohaemolysis (-haemolytic; e.g. enterococci), green partial
haemolysis resulting fromthe action of peroxides (-haemolytic; e.g.
S. viridans), or a clear zone of completehaemolysis caused by
haemolysins (-haemolytic; e.g. S. agalactiae or S.
pyogenes).Rebecca Lancefield classified -haemolytic streptococci in
1933 by antibody reactivitywith cell-wall antigens (see Table 8.2),
to give Lancefield groups A, B, C, etc. GroupB streptococci (S.
agalactiae) are further subdivided by serological responses to
thepolysaccharide capsule, into serotypes IaVIII. Microbiology
laboratories will reportthe identity of an infecting streptococcal
species firstly as Gram-positive chainsvisualised by microscopy,
then as -, - or non-haemolytic. Subsequently, where
appropriate, the laboratory will determine the Lancefield group
and/or species, andfinally it will report the antibiotic resistance
profile. A -haemolytic streptococcus
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
4/14
176 A FOUNDATION FOR NEONATAL CARE
causing newborn sepsis could be either S. pyogenes (GAS) or S.
agalactiae (GBS); but,in this era it is likely to be GBS rather
than GAS, as newborn disease and puerperalfever caused by the
latter is now rare (see Box 8.11).
TABLE 8.2 Streptococcal classifi cation explained
Species Lancefield group* Serotype** Haemolysis
S. pyogenes Group A (GAS)
S. agalactiae Group B (GBS) IaVIII
Enterococcus spp. Group D variable
Viridans streptococci
S. pneumoniae
Notes:
* Lancefield group is defined by serological responses to
cell-wall antigens.
** Serotype of GBS is defined by serological responses to the
capsular polysaccharide.
Diseases caused by different streptococci
GAS historical cause of puerperal feverGBS and occasionally
viridans streptococci cause ascending infection, chori-oamnionitis,
and early-onset sepsisEnterococci cause late-onset sepsis, for
instance via central venous lines
Genes and genomesGenome sequencing is the process in which the
DNA code of every gene in an organ-ism is identified, thus
providing a blue-print of the genes and the proteins that are
BOX 8.1 PUERPERAL FEVER
Puerperal fever is caused by locally invasive S. pyogenes (GAS)
in which the motherdevelops a streptococcal tissue infection and
then septicaemia, and the newborn can
become secondarily infected. The pathological process is
different from ascending
infection caused by S. agalactiae (GBS).Ignaz Semmelweiss in
1844, at the Vienna General Hospital, noted that puerperal
fever, also called childbed fever, was responsible for maternal
perinatal deaths. The
mortality reached 16% of all women in labour in the ward
training doctors, whereasthe mortality was only 2% in the ward
training midwifery students. Student doctors
were undertaking autopsies in the morning on women who had died
of puerperal fever,and then examining mothers in labour in the
afternoon, and since the students werenot washing their hands, GAS
was passed each day to otherwise healthy women.
Semmelweiss was the first to propose hand washing with
chlorinated lime to
control the spread of healthcare-associated infections.
Hand-washing still needsreinforcing today, over 150 years later;
and lack of hand washing is responsible for
the spread of virulent and multi-resistant organisms in
hospitals.
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
5/14
BACTERIAL AND TRANSPLACENTAL INFECTION 177
necessary for the organism to live. The larger the genome, the
more adaptable is theorganism (see Box 8.2). Gram-negative
bacteria, for instance, have large genomes andcan survive and
multiply for long periods in the environment; whereas many
Gram-positive bacteria are highly adapted to and need the
environment of an animal host,
for instance S. agalactiae. Genome-sequencing technology will
ultimately lead to thedevelopment of new antibiotics and vaccines;
and in the future, during outbreaks,strains will be tracked by
genome sequencing of each isolate.
BOX 8.2 BACTERIA, GENES AND GENOMES
Bacteria usually have a single circular chromosome, containing
2000+ genes. Ingeneral, the more genes within a chromosome, the
more adaptable is the organismto living in different environments.
Bacteria with smaller genomes tend to encode
fewer enzymes and nutrient transporters and have less metabolic
flexibility for
instance, S. agalactiaeis highly adapted to living only within
an animal host and notin the outside environment. P. aeruginosa, in
comparison, has a large genome, lots of
metabolic capability, and can live almost anywhere where there
is moisture.
Bacteria may carry antibiotic resistance genes on plasmids,
transposons andintegrated phages all are forms of mobile elements
that can spread themselves
between bacteria.
A plasmid is a transferable circle of DNA, usually much smaller
than the genomeitself, and sometimes contains genes for bacterial
conjugation (the process by which
plasmids are transferred from one bacterial species to
another).
Transposons and phages are other forms of mobile genetic
elements that canjump between bacterial species, and which often
carry advantages genes such as
those encoding antibiotic resistance.
Bacterial species Genome
size*
Number
of genes
Lifestyle
S. agalactiae 2.21 Mb 2094 Commensal of animals and manS. aureus
2.83 Mb 2623 Commensal of animals and man
E. coliK12 4.63 Mb 4289 Commensal of animals and man, able
to
survive in the environment
K. pneumoniae 5.92 Mb 5814 Commensal of animals and man
P. aeruginosa 6.26 Mb 5565 Soil organism found in a wide variety
of
habitats, and part of the normal human flora
*1 Mb = 1 000 000 base pairs
ANTIBIOTIC STRUCTURE AND MECHANISMS OF ACTION
Three classes of antibiotic are predominantly used in neonatal
intensive care settings:-lactams, glycopeptides and
aminoglycosides. The first class, -lactam antibiotics,include
benzylpenicillin and flucloxacillin (penicillins), cefotaxime (a
cephalosporin)
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
6/14
178 A FOUNDATION FOR NEONATAL CARE
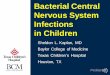
and meropenem (a carbapenem see Figure 8.2). Although
structurally very different,they all share a common feature, a
-lactam ring that is an analogue of D-alanine-D-alanine, the
dipeptide that is the building block of petidoglycan. The
-lactamring binds to and inhibits the transpeptidase enzymes (also
called penicillin-bindingproteins) that are necessary for forming
cross-links between peptidoglycan mol-ecules. Disruption of the
cell wall in this way causes bacterial lysis. Hence,
-lactamantibiotics are usually bactericidal (causing cell death).
Group B streptococcus is
universally sensitive to benzylpenicillin, and hence this
antibiotic remains a goodchoice for first-line treatment of
early-onset sepsis.Vancomycin (see Figure 8.2) and teicoplanin also
act on the peptidoglycan cell wall.
For various reasons, including inability to reach the
peptidoglycan layer in Gram-negative bacteria, glycopeptides are
only active against Gram-positive bacteria.
Gentamicin (see Figure 8.2), tobramycin, and amikacin are
aminoglycosideantibiotics that work by impeding the 30S subunit of
bacterial ribosomes, therebypreventing protein synthesis.
Aminoglycoside-exposed bacteria do not die immedi-ately; lack of
new protein production prevents bacterial replication and
eventuallyleads to bacterial death. Aminoglycosides are effective
against many Gram-negative
bacteria, and against some Gram-positive bacteria, notably
having a synergisticaction with flucloxacillin against S. aureus.
By contrast, streptococci and entero-cocci are resistant to
aminoglycosides, resulting from poor uptake of the antibiotic.
-lactam ring
O N
S
H
N
O
O
OH
O
O
O
F
H
S
N
N
Cl
NH
HO
H2N O
H
SS
NO
O
O
N
N
H
N
OH
O
O
O
NH
N
S
H H
O
OH
N
HO
O
O
OH
HO
HO
HN
H3C
H3C
H2N
H2N
NH2
NH2
CH3
O
O
O
O
O O
O
O
O
Cl
O
OH
OH OH
OH
NH2
OH
NHCH3
ClO O
O
O
O
O
O
HO
HO
H
HOOC
HN
H
N
H
N
H2N
H
N N
H
N
H
OHOH
Benzylpenicillin
Flucloxacillin
Meticillin
Gentamicin
Meropenem
Cefotaxime
Vancomycin
FIGURE 8.2 Antibiotic structures
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
7/14
BACTERIAL AND TRANSPLACENTAL INFECTION 179
However, when combined with a cell-wall-active antibiotic,
aminoglycosides can havesome synergistic bactericidal effect
against these bacteria.
BACTERIAL RESISTANCE
Many bacteria, especially Gram-negatives, are resistant to
penicillins because theyproduce -lactamases enzymes that break the
-lactam ring. Commonly encoun-tered -lactamases may act on
penicillins (penicillinases) and cephalosporins(cephalosporinases).
Flucloxacillin was developed because its additional
side-chainprotects it from the action of the S. aureus
b-lactamase.
Meticillin-resistant S. aureus (MRSA) and meticillin-resistant
coagulase-negativestaphylococci are resistant to virtually all
b-lactams because of alteration of thetarget site in the cell wall
to which the antibiotics bind. Meticillin was a precursorto the
development of flucloxacillin, and is no longer commercially
available (seeFigure 8.2).
Cefotaxime and meropenem (see Figure 8.2) are not susceptible to
penicillinases,and are therefore useful antibiotics for treatment
of both Gram-positive and Gram-negative bacteria. Meropenem has an
extremely wide spectrum of action, so goodthat it abolishes the
normal bacterial flora and predisposes to Candida infection, asdo
cephalosporins. Cefotaxime resistance can be mediated by
alternative b-lactamses,the cephalosporinases, and meropenem
resistance can also occur by metalloenzymesthat hydrolyse all
-lactams. Carbapenem-resistant isolates are currently rare in
mostdeveloped countries.-lactamases are encoded by genes that can
reside on plasmids,transposons or integrated phages (see Box 8.2),
and most are transferable betweenbacterial strains and species.
Some Gram-negative bacteria are aminoglycoside resistant, due
either to transfer-able resistance genes encoding enzymes that
break down the antibiotic, or to pooruptake, or mutation of the
ribosomal targets so that the aminoglycoside cannotbind.
ANTIBIOTIC CHOICE IN NEONATAL UNITS
The use of broad-spectrum first-line antibiotics (e.g.
ampicillin and cefotaxime) ona neonatal unit encourages more
antibiotic-resistant flora on babies compared withusing
narrow-spectrum antibiotics (see Figure 8.3). For this reason, most
neonatalunits use relatively narrow-spectrum antibiotics wherever
possible. For instance,
benzylpenicillin and gentamicin are given for initial therapy of
suspected early-onsetsepsis, aimed at treating S. agalactiae and E.
coli infections. Not all neonatal unitsdo this, however. Some units
use cefotaxime for first-line empiric antibiotic therapybecause of
ease of administration, and to avoid toxicity of aminoglycosides
and theneed for monitoring levels. Flucloxacillin and gentamicin
are often used for suspectedlate-onset sepsis, directed at S.
aureus and Gram-negative bacteria. Glycopeptides,vancomycin or
teicoplanin, are used to replace flucloxacillin when long-line
infectionis suspected, to treat coagulase negative staphylococcal
and enterococcal infections.A third-generation cephalosporin (e.g.
cefotaxime) is often added to the empiricregimen when meningitis is
suspected or proven.
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
8/14
180 A FOUNDATION FOR NEONATAL CARE
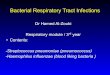
FIGURE 8.3 Broad-spectrum antibiotics encourage multi-resistant
bacterial fl ora on
neonatal units
In a Dutch cross-over study, the resistance profile of
colonising Gram-negative bacteria wasdetermined over a period of
one year. Neonatal unit A used amoxicillin and cefotaxime for
sixmonths, and neonatal unit B used penicillin and tobramycin, and
then the units switched theirregimens. When a unit used the
broad-spectrum combination of ampicillin and cefotaximetheir babies
were more frequently colonised with Gram-negative bacteria and
these isolateswere almost all resistant to the broad-spectrum
antibiotics used. When the narrow-spectrumantibiotics, penicillin
and tobramycin, were given, the babies were infrequently colonised
withGram-negative bacilli and when they were they were usually
sensitive to these antibiotics.1
ROUTES OF INFECTION
Routes of infection are transplacental, ascending, and
post-partum. The organismsthat most commonly cause neonatal
infection (see Table 8.1) are described to high-light the
pathogenic mechanisms. Ascending and post-partum infections are
usuallycaused by bacteria, whereas transplacental infections are
usually caused by virusesand parasites. Listeria monocytogenes is
an exception. Post-partum viral infectionsare not the subject of
this chapter.
Bacterial infection in the neonatal period can be categorised as
either early-onsetor late-onset sepsis, and the cut-off between the
two categories is variously definedas anywhere between 48 hours and
a week old. A more useful definition is a patho-genic one.
Early-onset sepsis originates in utero (typically once the
membranes haveruptured) and disease is usually clinically obvious
soon after birth or within the first2448 hours; whereas bacteria
causing late-onset sepsis are usually acquired after
birth.
1 4 8 12 16 20 24 29 32 36 40 44 48 52
1 4 8 12 16 20 24 29 32 36 40 44 48 52
Amoxicillin-cefotaxime regimen
Penicillin-tobramycin regimen
Penicillin-tobramycin regimen
Amoxicillin-cefotaxime regimen
NICU A
NICU B
Isolates of bacilli resistant toempiric antibiotic regimen of
unit
Isolates of bacilli sensitive toempiric antibiotic regimen of
unitbut resistant to antibiotic regimenof other unit
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
9/14
BACTERIAL AND TRANSPLACENTAL INFECTION 181
EARLY-ONSET SEPSIS
Mode of acquisition of infection
Almost all early-onset infections are caused by bacteria that
have ascended into theamniotic fluid from the vaginal flora. We
know that this is the route of infection
because in newborn infected twins, the first twin to be born is
always infected whereasthe second twin may or may not be (see Box
8.3). Chorioamnionitis is the initialevent and the baby becomes
secondarily infected, first with pneumonia, because thelungs are in
direct contiguity with amniotic fluid. Depending on the duration
andthe density of pneumonia, the organism then seeds into the
bloodstream and fromthere to the blood-brain barrier and into the
cerebro-spinal fluid to cause meningitis.All babies with
early-onset bacterial sepsis therefore have pneumonia, but they
maynot have bacteraemia or septicaemia, and meningitis is
relatively rare.
Amniotic fluid obtained by amniocentesis at > 30 weeks
gestation from womenwith apparently intact membranes contains
bacteria in a small percentage of samples,
implying that low-grade seeding of the amniotic fluid with
bacteria occasionallyoccurs. The vast majority of bacteria cannot
survive in amniotic fluid; amniotic fluidin vitro has strong
anti-bacterial properties, and does not support the growth of
manybacterial species, the exceptions being Escherichia coli,
Streptococcus agalactiae, andoccasionally other streptococci.
BOX 8.3 EARLY-ONSET SEPSIS
Invasion of the amniotic fluid by bacteria from the birth canal
leads to chorioamnionitis.
The fetus is secondarily infected, and develops pneumonia and
the newborn baby
has respiratory signs of early-onset sepsis. For every seven
babies with S. agalactiae(GBS) pneumonia, only one will have a
positive blood culture, and very few will have
meningitis.
Twin 2 sterile amniotic fluid
Twin 1 chorioamnionitis
Chorioamnionitis is caused by
bacteria that colonise the birthcanal
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
10/14
182 A FOUNDATION FOR NEONATAL CARE
Group B streptococcal infection
S. agalactiae (group B streptococcus; GBS) chorioamnionitis only
occurs in womenwho are colonised with the organism, and the risk of
chorioamnionitis in carriers isincreased markedly by prolonged
rupture of membranes > 18 hours. S. agalactiae, in
vitro, can reach a density of 10
8
to 10
9
bacteria/mL of amniotic fluid in much less timethan 18 hours. S.
agalactiae can also invade amniotic membranes in vitro, hence it
islikely that chorioamnionitis in vivo can be established even
without prior rupture ofmembranes, and that S. agalactiae is one
cause of premature rupture of membranesand preterm labour.
The proven S. agalactiae infection rate in the UK is 0.5
cases/1000 births, whereasthe probable infection rate is 3.6
cases/1000 births or 1:280 births. These rates maybe an
underestimate of the potential magnitude of the problem because at
the timewhen these UK prospective observational studies were done,
many obstetricianswere giving intrapartum antibiotic prophylaxis to
attempt to prevent early-onset S.
agalactiae sepsis. Probable infection is carefully defined as
likely infection in babiesfrom whom S. agalactiae is recovered from
surface swabs taken at birth, and whohave respiratory distress and
radiographic changes of pneumonia. Thus, for everyseven babies with
S. agalactiae pneumonia only one has detectable bacteraemia.
Theproven infection rate enormously underestimates the burden ofS.
agalactiae disease for instance, the UK has a birth rate of ~650
000 babies/year, which equates to only~300 proven infections/year.
However, the probable real infection rate is seven timeshigher,
equating to 2300 infections/year in the UK, or, in an average sized
maternityunit of 5000 deliveries, 18 infections per year.
Other bacterial causes of early-onset sepsisE. coli is a less
frequent cause of early-onset sepsis, and occasionally infection
iscaused by other streptococci, such as -haemolytic S. viridans.
The limited rangeof pathogens causing early-onset sepsis means that
it is mostly appropriate to usenarrow-spectrum benzylpenicillin and
an aminoglycoside for first-line treatment.Anaerobic bacteria
occasionally also cause chorioamnionitis, often as part of
mixed-organism infections, but the pathogenic potential of the
anaerobes is low, and thebacteria are usually sensitive to
penicillin. Gardnerella vaginalis is a Gram-variablebacterium that
is associated with vaginosis, and which is occasionally isolated
fromsurface swabs of babies with signs of early-onset pneumonia. It
is more likely to be
a marker organism of difficult-to-culture anaerobes, rather than
being a neonatalpathogen per se. Listeria monocytogenes is
discussed later in the chapter.
LATE-ONSET SEPSIS
Infections occurring after the first day or two of life have a
different pathogenesis toearly-onset sepsis. These infections are
acquired ex-utero, and fall into two groups commensals with low
virulence that have gained iatrogenic access to normallysterile
sites (such as coagulase-negative staphylococcal central venous
line infection),or invasive bacteria with real pathogenic
potential, such as serotype III S. agalactiaeinfections.
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
11/14
BACTERIAL AND TRANSPLACENTAL INFECTION 183
Low-virulence commensals
Staphylococci (both S. aureus and coagulase-negative
staphylococcus), enterococci,and Gram-negative bacteria gain access
to sterile sites, blood or lungs, usually bytracking along plastic
or lodging on plastic and establishing a foothold.
Bacteria in the mouth may gain access to and cause infection in
the normallysterile respiratory tract of ventilated babies.
Oropharyngeal surveillance cultures caninform antibiotic choice for
ventilation-associated pneumonia, prior to endotra-cheal cultures
becoming available. Such surveillance cultures, however, do not
giveclues to the likely identity of bacteria causing late-onset
sepsis in the absence ofpneumonia.
Central venous lines are the usual source of late-onset sepsis
on neonatal units,and the culpable organisms are skin commensals,
staphylococci, or intestinal organ-isms such as enterococci and
Gram-negative bacilli. Some of these infections willoccur from loss
of sterility at connection ports, and others will arise from
bacteria
seeding into the bloodstream from the intestine, and forming
microcolonies on insitu plastic.
Pathogenic bacteria
Bacteria causing late-onset sepsis include S. agalactiae, S.
aureus causing skin infec-tions and then seeding elsewhere if
untreated, and those organisms that cause urinarytract
infections.
A specific sub-group ofS. agalactiae cause late-onset infection;
most isolatesare capsular serotype III and/or multilocus sequence
type ST-17 strains. Diseaseis different from early-onset S.
agalactiae sepsis in that there does not have to be
pneumonia; blood spread is usually low-grade bacteraemia rather
than septicaemia,and the presenting feature is focal S. agalactiae
infection, such as septic arthritis ormeningitis. Serotype
III/ST-17 strains almost certainly have a genetic propensity
forcausing invasive disease. Hence, these strains are likely to be
intestinal commensals fora period of time, much the same as for the
other S. agalactiae serotypes, but at somepoint in time the
serotype III/ST-17 strains are able to breach the mucosal
barrierand establish bacteraemia. Early-onset S. agalactiae sepsis
may be seen as a chanceevent in which any serotype ofS. agalactiae
finds itself in the normally sterile amni-otic fluid; the organism
has sufficient defence mechanisms to protect itself againsthost
innate immunity; it establishes chorioamnionitis, and the fetus is
incidentally
affected. In contrast, in late-onset S. agalactiae infection,
disease propensity is relatedto the organisms ability to cause
disease.
When S. agalactiae disease occurs in the few days after birth,
the route of infectionis likely to have been of the early-onset
type if the baby has pneumonia, and of thelate-onset type if the
baby has focal disease without pneumonia. The distinctionbetween
early- and late-onset S. agalactiae sepsis is important because
severe illnessor death in early-onset sepsis is potentially
preventable by the administration ofintrapartum antibiotic
prophylaxis by the obstetrician or as a result of the
neonatolo-gist identifying respiratory distress and treating the
newborn baby early.
Late-onset sepsis is not preventable by intrapartum antibiotic
administration, andthe signs of impending illness are more subtle
and dont necessarily include signs ofpneumonia.
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
12/14
184 A FOUNDATION FOR NEONATAL CARE
TRANSPLACENTAL INFECTIONS
Parasites, viruses and one bacterium may be acquired by a fetus.
The organismsinclude Toxoplasma gondii; rubella; members of the
Herpesviridae cytomegalovi-rus (CMV), herpesvirus (HSV), and
varicella-zoster (chickenpox virus VZV); and
Listeria monocytogenes. Maternal primary infection leads to
parasitaemia, viraemiaor bacteraemia and the organism spreads via
the placenta to infect the fetus, usuallycausing damage that can be
seen on placental histology after birth. Depending onthe stage of
fetal development, the damage to the baby can be anything from
asymp-tomatic to profound.
Toxoplasma gondii
Toxoplasma gondii is a protozoan parasite whose definitive host
is the cat. Othermammals and man are secondary hosts. It is only in
cat-family members that theparasite has its sexual cycle, in which
the organism replicates in the intestine and
eggs are shed in their millions in faeces. In other mammals and
man the organism isacquired either through eating undercooked meat
or vegetables contaminated withparasite eggs. Toxoplasmosis in an
immune pregnant woman is usually asymptomaticor causes only
subclinical illness. However, the fetus is at risk of severe
damage, withCNS and eye involvement caused by the parasite invading
and destroying neuronaland retinal cells, leading to microcephaly
or hydrocephalus with brain destructionand/or chorioretinitis.
Mid-trimester, weeks 204, is the period of greatest risk to
thefetus before 20 weeks gestation the risk of acquisition is low,
and after 30 weeks,fetal immunity is sufficiently mature to control
the infection without CNS damage.
Cytomegalovirus (CMV)Fetal disease and neuronal damage occur
following early-gestation acquisition ofCMV, and can result from
maternal primary infection or from secondary reactivationof
maternal CMV. The fetal liver, lungs, intestine and brain may be
damaged withconjugated hyperbilirubinaemia, pneumonitis, intestinal
inflammation and neuro-nal damage. CMV has an especial propensity
for causing sensorineural hearing loss.Reactivation of maternal CMV
is less likely to cause severe fetal disease, presumablybecause
there is some degree of protective maternal immunity. Some studies
withsmall numbers of patients given ganciclovir intravenously for
six weeks, commenc-ing in the neonatal period, have suggested a
lower rate of hearing loss in the treated
babies. If hearing is improved in the treated group, this may be
a surrogate markerof better global neurodevelopmental outcome.
However, the evidence that treatmentis effective is far from
definitive, with the studies undertaken so far being flawed bylack
of follow-up. For this reason, national ganciclovir treatment
guidelines do notyet exist.
Varicella-zoster virus (VZV)
Chickenpox in pregnancy can be life-threatening for the mother,
and transplacentalspread establishes chickenpox in the fetus. The
fetus may recover with no lastingeffects, or dermatomal
reactivation throughout the remainder of pregnancy can leadto
circumferential scarring, limb deformity or even limb loss.
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
13/14
BACTERIAL AND TRANSPLACENTAL INFECTION 185
Maternal chickenpox in the peripartum period can lead to
infection in the new-born baby. In keeping with other
transplacental infections, the newborn baby canhave liver
involvement and pneumonitis. The mortality is reported as up to
30%,but this figure likely reflects publication bias. When a fetus
is exposed to maternal
chickenpox just prior to delivery, disease can be severe as
there is no transplacentaltransfer of maternal protective
anti-varicella antibody. In this situation, varicella-zoster
immunoglobulin protects against severe disease evolving after the
incubationperiod of 1021 days.
Listeria monocytogenes
Listeria is a Gram-positive bacillus that lives in soil and
contaminates crops. It isacquired through ingestion of contaminated
food, particularly soft cheeses andundercooked meats. The organism
grows well at fridge temperatures of 48 C.Following maternal
infection, transplacental spread occurs to the fetus. The
placenta
and newborn baby may be covered in miliary granulomata
(granuloma infantisep-tica). Most cases are associated with
maternal symptomatic flu-like illness, indicatingthat bacteraemia
in the mother is necessary. Amoxycillin or ampicillin are the
mosteffective antibiotics when tested in vitro against Listeria,
but in vivo benzylpenicil-lin may be as effective. As this fact is
difficult to prove, on the rare occasion thata baby has a proven
Listeria infection it is prudent to administer amoxycillin
orampicillin.
SUMMARY
Bacteria can be divided into two broad groups by the Gram stain.
Gram-positive cocci
include Streptococcus spp. and Staphylococcus spp. and are
sensitive to -lactam andglycopeptide antibiotics. Gram-negative
bacteria include E. coli, P. aeruginosa, etc.,and are sensitive to
aminoglycosides, cephalosporins, and the higher order -lactamssuch
as meropenem. Neonatal units generally aim to have empiric
antibiotic regi-mens that promote the narrowest-spectrum antibiotic
use, as broad-spectrumantibiotics lead to babies being colonised
with Gram-negative flora that is resistantto the antibiotics.
Early-onset sepsis commences with ascending infection, and leadsto
chorioamnionitis, then pneumonia in the fetus, then septicaemia +/
meningitis.Empirical treatment with penicillin and an
aminoglycoside covers the two main caus-ative organisms, S.
agalactiae (group B streptococcus) and E. coli. Late-onset sepsis
is
caused either by low-grade commensals obtaining access to
normally sterile sites (e.g.tracking along plastic endotracheal
tubes to the lung or along central venous lines tothe bloodstream),
or by organisms that are hyper-virulent and which have a
propen-sity to cause disease (e.g. serotype III/ST-17 S.
agalactiae). Late-onset sepsis that isseen on neonatal units is
predominantly caused by low-grade commensals from theskin (e.g.
coagulase-negative staphylococci) or from the intestine (e.g.
enterococcior Gram-negative bacilli). Empiric initial treatment for
suspected late-onset sepsisshould be with narrow-spectrum
antibiotics for instance, flucloxacillin or a glyco-peptide, and an
aminoglycoside; and broad-spectrum antibiotics (e.g. cefotaximeor
meropenem) should be reserved for the treatment of known
antibiotic-resistantGram-negative bacilli, and only occasionally
used when a baby is deteriorating oninitial narrow-spectrum agents.
Newborn babies may acquire infections in utero, and
-
7/29/2019 Bacterial and Transplacental Infections _ Mark Anthony
and James Gray
14/14
186 A FOUNDATION FOR NEONATAL CARE
predominantly these infections are parasites (Toxoplasma) or
viruses (rubella andthe Herpesviridae family members).
KEY POINTS FOR PRACTICE
Bacteria causing neonatal infections can be divided into two
broad groups by
the Gram stain.Gram-positive bacteria include Streptococcusspp.
and Staphylococcusspp. andare sensitive to -lactam and glycopeptide
antibiotics.Gram-negative bacteria include Escherichia coli, and
Pseudomonas, Klebsiellaand Serratia species, and are sensitive to
aminoglycosides, cephalosporins, andthe higher-order -lactams such
as meropenem.Neonatal units should aim to have narrow-spectrum
empiric antibioticregimens, as broad-spectrum antibiotics lead to
colonisation with resistantGram-negative flora.
The sequence of systemic infection in early-onset sepsis is
ascending: chori-oamnionitis, then pneumonia in the fetus, then
septicaemia +/ meningitis.Empiric treatment with penicillin and an
aminoglycoside covers the two maincausative organisms of
early-onset sepsis S. agalactiae (group B streptococ-cus) and E.
coli.Late-onset sepsis is caused either by low-grade commensals
obtaining accessto normally sterile sites (e.g. tracking along
plastic endotracheal tubes to thelung or along central venous lines
to the bloodstream), or by organisms that arehyper-virulent and
which have a propensity to cause disease (e.g. serotype III/ST-17S.
agalactiae).
Late-onset sepsis that is seen on neonatal units is
predominantly caused bylow-grade commensals from the skin (e.g.
coagulase-negative staphylococci) ormore virulent organisms from
the intestine (e.g. enterococci or
Gram-negativebacilli).Narrow-spectrum antibiotics are best for the
empiric treatment of suspectedlate-onset sepsis for instance,
flucloxacillin or a glycopeptide combined withan
aminoglycoside.Broad-spectrum antibiotics (e.g. cefotaxime or
meropenem) are mostlyreserved for the treatment of known
antibiotic-resistant Gram-negative bacilli,or used when a baby is
deteriorating on initial narrow-spectrum agents.
Newborn babies may have acquired infections in utero.
Predominantly theseinfections are parasites or viruses.
REFERENCE
1 De Man P, Verhoeven BAN, Verburgh HA, et al. An antibiotic
policy to prevent emergence
of resistant bacilli. Lancet. 2000; 355: 9738.
FURTHER READING
Rennie JM. Robertsons Textbook of Neonatology. 4th ed.
Amsterdam: Elsevier; 2005.
Isaacs D, Moxon ER. Handbook of Neonatal Infections: a practical
guide. 2nd ed. London: Balliere
Tindall; 1999.