Embed Size (px)
Citation preview

Research ArticleBacteriological Assessment of the Indoor Air of DifferentHospitals of Kathmandu District
ArzuKunwar SamyuktaTamrakarShyaronPoudel SonySharmaandPramilaParajuli
Department of Microbiology St Xavierrsquos College Kathmandu 44600 Nepal
Correspondence should be addressed to Arzu Kunwar arzukunwar01gmailcom
Received 2 January 2019 Revised 21 February 2019 Accepted 13 March 2019 Published 8 April 2019
Academic Editor Joseph Falkinham
Copyright copy 2019 Arzu Kunwar et al )is is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
Nosocomial infection is the infection that has been caught in a hospital and is potentially caused by organisms that are not susceptibleto antibiotics Nosocomial infections are transmitted directly or indirectly through air andmay cause different types of infections)isstudy was undertaken with an objective to determine the prevalence of nosocomial bacteria present in hospital indoor environment Atotal of 16 air samples were taken from general wards and emergency wards of 8 different hospitals using an impactor air sampler innutrient agar mannitol salt agar blood agar cetrimide agar and MacConkey agar )e bacteriological agents were isolated andidentified by cultural characteristics Gram staining and biochemical tests and their antibiotic susceptibility pattern was determinedusing CLSI Guideline 2015 According to the European Union Guidelines to GoodManufacturing Practices the hospitals were underC- and D-grade air quality According to the European Commission most of the hospitals were intermediately polluted Out of 16indoor air samples 4718 of Staphylococcus aureus and 182 Pseudomonas spp were isolated CoNS Streptococcus sppMicrococcusspp andBacillus spp andGram-negative bacteria Ecoli and Proteus spp were identified)e bacterial loadwas found to be high in theemergency ward (558) in comparison to that in the general ward (442) )ere is statistically no significant difference betweenbacterial load and 2 wards (general and emergency) of different hospitals and among different hospitals )e most effective antibioticagainst S aureus was gentamicin (8181) and ofloxacin (8181) Among the antibiotics used for Pseudomonas spp ceftriaxone(833) and ofloxacin (833) were effective High prevalence of S aureus and Gram-negative bacteria was found in this study it istherefore important to monitor air quality regularly at different hospitals to prevent HAI
1 Introduction
A hospital-acquired infection (HAI) also known as a nos-ocomial infection is an infection that is acquired in ahospital or other healthcare facility Such an infection can beacquired by susceptible patients in hospital nursing homerehabilitation facility outpatient clinic or other clinicalsettings by various means Healthcare staff can spread in-fection in addition to contaminated equipment bed linensor air droplets )e infection can originate from the outsideenvironment another infected patient staff that may beinfected or in some cases the source of the infection cannotbe determined In some cases the microorganism originatesfrom the patientrsquos own skin microbiota becoming oppor-tunistic after surgery or other procedures that compromisethe protective skin barrier Although the patient may have
contracted the infection from their own skin the infection isstill considered nosocomial since it develops in thehealthcare setting [1] )e main source of microorgan-ism is human beings as they are discharged throughhuman activities like coughing sneezing laughing and eventalking [2]
Nosocomial infections are one of the most seriouscomplications in hospital settings affecting patients in ICUimmunosuppressed people hospital staff and people havingfrequent encounter with healthcare facilities Nosocomialinfections in ICU patients lead to use of broad-spectrumantibiotics and emergence of antibiotic-resistant microor-ganisms which ultimately cause high morbidity mortalityand treatment cost of infection along with a prolongedhospital stay It has been observed that most prevalentnosocomial infection-causing bacteria like Staphylococcus
HindawiInternational Journal of MicrobiologyVolume 2019 Article ID 5320807 9 pageshttpsdoiorg10115520195320807
aureus and Pseudomonas spp are developing highmultidrugresistance leading to birth of MDRSA and MDRPAeventually causing ineffective drug treatment [3]
Gas dust particles water vapor and air contain mi-croorganisms )ere are vegetative cells and spores ofbacteria fungi algae viruses and protozoal cysts Since air isoften exposed to sunlight it has higher temperature and lessmoisture Air serves as transport or dispersal medium formicroorganism therefore they occur in relatively smallnumber in air when compared with soil and water [4]
)e air found inside the building is referred to as indoorair)emost common genera of bacteria found in indoor airare Staphylococci Bacilli and Clostridium [5] MRSA(methicillin-resistant Staphylococcus aureus) andgentamicin-resistant Gram-negative bacteria are found to beserious nowadays [1] People spend 80ndash90 of their timein indoor environments by breathing on average 14m3 of airper day Moreover the environmental and physical factorsmainly include temperature humidity air exchange rate airmovement and building structures location poor designventilation system as well as interior redesign respectivelywhich enhance microorganismrsquos growth and multiplicationin the indoor atmosphere [5]
A review made by the WHO on the number of epide-miological studies showed that there is sufficient evidencefor an association between indoor dampness-related factorsand a wide range of effects on respiratory health includingasthma development asthma exacerbation current asthmarespiratory infections upper respiratory tract symptomscough wheeze and dyspnoea [6]
Hence this study provides clear data of microbial airquality and respective bacterial loads in indoor air of hos-pitals of Kathmandu district Kathmandu having an area of395 km2 is the most densely populated district of Nepal)erefore we conducted research in hospitals located incomparatively high population density area which repre-sented major areas of Kathmandu district Identificationsucceeded by antimicrobial susceptibility pattern of thebacteria isolated from the indoor air of hospitals was de-termined by using multiple drugs Globally the emergenceof drug-resistant bacteria is posing as a threat in deliveranceof effective medical care Once a person contracts nosoco-mial infection the initial step for management of the in-fection is antibiotic administration )e commonly usedantibiotics for nosocomial agents Staphylococcus spp andPseudomonas spp were identified and the susceptibility ofthe organisms to antibiotics was recorded )erefore westudied antibiotic resistance which is well pronounced indeveloping countries like Nepal so as to alert clinicians andassist them in proper treatment decisions and propermanagement of such patients
2 Materials and Methodology
21 Materials
211 Equipment Impactor air sampler autoclave hot airoven incubator microscope refrigerator weighing machinegas burners inoculating loop andwires were used in this study
212 Microbiological Media Nutrient broth triple sugariron agar nutrient agar simmons citrate agar mannitol saltagar sulphur indole motility media MacConkey agaroxidativefermentative agar urease broth Mueller-Hintonagar cetrimide agar methyl red-Voges-Proskauer brothand blood agar were used in this study
213 Chemicals and Reagents Barrittrsquos reagent oxidasereagent Kovacrsquos reagent crystal violet Gram iodineacetone-alcohol Safranin blood plasma normal salinehydrogen peroxide nitrate reagent A and nitrate reagent Bwere used in this study
214 Antibiotic Discs All the antibiotic discs used for thesusceptibility tests were from HiMedia Laboratories PvtLimited Bombay India )e antibiotics used were as fol-lows ampicillin ofloxacin erythromycin ceftriaxonegentamicin amikacin chloramphenicol ceftazidime andcotrimoxazole
22 Miscellaneous Conical flasks cotton distilled waterdropper forceps glass slides cover slips immersion oilLysol measuring cylinder Petri dishes pipettes spatula testtubes and cotton swab
3 Methodology
31 Study Area Two wardsmdashemergency ward and generalwardmdashof different hospitals of Kathmandu district werechosen for the comparative study of hospital indoor airmicroflora using a microbiological air sampler
32 Sample Collection We performed an active impactorsampling method by using ldquoHi-Airrdquo air sampler )e heightof the sampler is 54 cm which is also the sampling height Asprementioned we had only one sampler due to which wecollected samples one after another We allocated two dif-ferent sites in the emergency and general wards of thehospitals Sampling from both the wards of one hospital wasdone in a same day whereas the sampling from differenthospitals was performed on different days
Impactor samplers use a solid or adhesive medium suchas agar gel Typically air is drawn into the sampling head bya pump or fan and accelerated through a perforated plate(sieve samplers) [7] A standard plate of nutrient agar (totalcount) mannitol salt agar (specifically for Staphylococcusaureus) blood agar (specifically for Streptococcus species)MacConkey agar (specifically for Gram-negative bacteria)and cetrimide agar (specifically for Pseudomonas species)was aseptically prepared and used
)e impeller speed of 2500 rpmndash2600 rpm was so ad-justed that 100 liters of air was sampled every minuteaccording to the catalogue of the air sampler We had a totalof 5 plates for each ward and a single agar plate was placed inthe air sampler for 5minutes so that 500 liters of air wassampled )erefore the sampling time at one ward was25minutes with a preparation time of 15minutes Overall
2 International Journal of Microbiology
our sampling period was 80minutes in one hospital As weperformed sampling on two different days a week so ourtotal sampling period for 8 hospitals was 1month
33 Transportation of the Sample Immediately after col-lection of samples the Petri plates were taken to the Lab-oratory of Microbiology of St Xavierrsquos College )ese Petriplates were incubated in an inverted position at 37degC for24 hrs
34 Microbiological Examination of the Sample After in-cubation total plate count was done on the basis of growthon NA plates )e colony characteristics were studied frommannitol salt agar MacConkey agar blood agar andcetrimide agar After this the colonies were subjected toGram staining )en for Gram-positive organisms bio-chemical tests such as catalase oxidase and coagulase andOF tests were performed whereas for Gram-negative or-ganisms biochemical tests such as IMViC TSIA ureasecatalse oxidase and OF tests were performed
35 Antibiotic Sensitivity Test Among the identified Gram-positive cocci and Gram-negative bacteria only Staphylo-coccus aureus and Pseudomonas spp were further tested fortheir AST pattern respectively For this representativecolonies were selected and were suspended in nutrient brothand the suspension was standardized with respect to 05McFarland solutions )e susceptibility of the isolated or-ganisms towards the antibiotics was tested by usingKirbeyndashBauerrsquos Method on Mueller-Hinton agar (CLSI2015) [8]
For Staphylococcus aureus gentamicin cotrimoxazoleampicillin erythromycin ofloxacin and chloramphenicolwere used And for Pseudomonas spp amoxicillin cef-triaxone cefotaxime imipenem and ofloxacin were used
36 Statistical Analysis )e data thus generated were an-alyzed by simple mean value percentage and test of sig-nificance by using two-way ANOVA to determinesignificant differences between the bacterial load and dif-ferent wards and also between the hospitals where the levelof significance was 5 for the analysis
Test statistics under H0 the two ANOVA F-statistics are
Fcal MSCMSE
Fcal MSRMSE
(1)
where MSCmean sum of square of variation due to col-umns MSRmean sum of square of variation due torows and MSEmean sum of square of variation due toerrors [9]
37 Limitations(i) As we are undergraduate students our research
work was carried out in college laboratory )ere
were several group projects simultaneously runningin the laboratory where we all shared same spaceinstruments and resources like Petri plates tubesmedia and incubator
(ii) )e project being a part of bachelorrsquos curriculumwas conducted alongside our academic classes Ourresearch time was limited to 5 working days with5 hours per day in the college laboratory
(iii) From each air sample plates we required peculiarcolonies on nutrient agar to be further processedand subcultured Our prospected methodol-ogy required around 50ndash60 number of Petri platesfor complete processing of a single air sampleplate
)e above-mentioned reasons limited our ability to carryout our duplicate samples We therefore decided to focuson original samples rather than the duplicate samples
4 Results
)e following formula was used to calculate bacterial load(cfum3)
Pr N1N
+1
Nminus 1+
1Nminus 2
+ middot middot middot +1
Nminus r + 11113874 1113875 (2)
where Pr probable statistical total r number of CFUcounted on 90mm Petri dish and N total number of holesin the sampling head 380 holes [10]
)e maximum growth of bacteria was observed inemergency wards (5572) as compared to general wards(442) of different hospitals High bacterial load (348 cfum3) and low bacterial load (58 cfum3) were found in the airof hospitals H4 and H7 respectively
Out of 8 hospitals general wards of 3 hospitals (H1 H7and H8) and emergency wards of 3 hospitals (H3 H5 andH7) showed a C-grade air quality And general wards of 5hospitals (H2 H3 H4 H5 and H6) and emergency wards of5 hospitals (H1 H2 H4 H6 and H8) were under D-gradeair quality
Among 8 hospitals general wards of H7 and H8 andemergency wards of H3 and H7 showed a very low degree ofbacterial air pollution (Table 1)
Out of 8 hospitals Staphylococcus aureus was isolatedfrom 7 hospitals including both general and emergencywards )e maximum percentage (1003) of S aureus wasfound to be isolated from the general ward of H2 and theleast percentage of isolates (121) was found to be also fromthe general ward of H6 )e result is shown in Table 2
41 Occurrence of Pseudomonas spp in Different HospitalsOut of 8 hospitals Pseudomonas spp was isolated only from1 hospital ie H1 in its general ward with the no of 6colonies (182)
42 Occurrence of Gram-Positive Bacteria Other than Saureus in Different Hospitals Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcus spp
International Journal of Microbiology 3
in 3 hospitals whereas Micrococcus spp was isolated fromonly 1 hospital And Bacillus spp was isolated from 7hospitals
43 Occurrence of Gram-Negative Bacteria Other thanPseudomonas spp in Different Hospitals Out of 8 hospitalsEcoli was isolated from 2 hospitals and Proteus spp wasisolated from only 1 hospital
Among 8 hospitals 3 hospitals were divided as hospitalsin busy area and 5 were divided as hospitals in less busy areaS aureus was isolated from 3 hospitals in busy area and 4hospitals in less busy area Micrococcus spp and Pseudo-monas spp were isolated only from H4 semiprivate hospitalin busy area and H1 government hospital in less busy arearespectively )e result is shown in Table 3 (busy area refersto the area having high annual patients flow less busy arearefers to the area having comparatively low annual patientsflow)
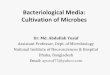
Figure 1 demonstrates that the occurrence of Staphy-lococcus aureus was found to be maximum covering 7 out of8 hospitals followed by CoNS in 6 out of 8 hospitalsStreptococcus spp and E coli were found to be in three andtwo hospitals respectively And the frequency of occurrenceofMicrococcus spp Proteus spp and Pseudomonas spp wasfound to be very least ie only in one hospital
Figure 2 demonstrates that Staphylococcus aureus wasfound to be present in general ward and emergency ward of 6and 5 hospitals respectively which was followed by CONSin the general and emergency wards of 3 and 4 hospitalsrespectively However Micrococcus spp and E Coli werepresent in both the general and emergency wards of onehospital In contrast Proteus spp and Pseudomonas sppwere only present in general wards of only one hospitalStreptococcus spp was present in general and emergencyward of 1 and 2 hospitals And Bacillus spp was present inboth the general and emergency ward of 3 and 4 hospitalsrespectively
)e most effective antibiotic against isolated Staphylo-coccus aureus was gentamicin (8181) and ofloxacin(8181) and the least effective was chloramphenicol(3636) and erythromycin (3636)
)e most effective antibiotic against isolated Pseudo-monas spp was ceftriaxone (833) and ofloxacin (833)and least effective was cefotaxime (166)
5 Discussion
Microbiological quality assessment of indoor air is one of themost vital investigations to determine the microbial indoorair pollution )e information on the indoor microbialconcentrations of airborne bacteria is necessary both toestimate the health hazard and to create standards for indoorair-quality control [5]
)ere was a presence of certain bacterial load inemergency and general wards of 8 hospitals where the study
Table 1 Grading of hospitals according to European Union Guidelines to Good Manufacturing Practices
S N Hospitals Number of colonies in general ward(calculated)
Air quality(grade)
Number of colonies in emergency ward(calculated)
Air quality(grade)
1 H1 96 C 116 D2 H2 172 D 128 D3 H3 132 D 26 C4 H4 206 D 142 D5 H5 110 D 82 C6 H6 108 D 114 D7 H7 28 C 30 C8 H8 44 C 102 DTotal 896 740
Table 2 Number and percentage of Staphylococcus aureus indifferent wards of the hospital
S N HospitalsNumber of organism ()
Emergency ward General ward1 H1 Nil 19 (577)2 H2 20 (483) 33 (1003)3 H3 Nil Nil4 H4 18 (434) 11 (334)5 H5 16 (386) 23 (699)6 H6 16 (386) 4 (121)7 H7 6 (144) Nil8 H8 Nil 5 (151)Total 76 95)e percentage of isolated S aureus was calculated on the basis of total platecount on NA
0
Stap
hylo
cocc
us a
ureu
s
CoN
S
E co
li
Prot
eus s
pp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
12345678
Num
ber o
f hos
pita
ls
Figure 1 Prevalence of the microorganisms in different hospitals
4 International Journal of Microbiology
was carried out From Table 4 we can observe that amongthe two wards emergency ward was found to have highbacterial load (5572) in comparison to general ward(442) A contrast result was obtained in a study conductedby Awosika et al [11] where out of nine wards the highbacterial load was found to be in medical ward (25)whereas the least bacterial load was recorded in emergencyunit (2) Humid room environment presence of un-hygienic attached toilets poor waste management systemand high number of patients in a single room personnel andvisitors occupying the hospital might be the reasons for highbacterial load in emergency ward in this study
According to the European Union Guidelines to GoodManufacturing Practices (Table 5) indoor air possessinggreater than 100 cfum3 and 200 cfum3 bacterial loads isreferred to as C- and D-grade air quality respectively In ourstudy Table 1 demonstrates that all the general wards andemergency wards of 8 hospitals were under C- and D-gradeair quality)is might be because at the time of this study allwards were at their maximum capacity as of visitors in andout the wards the high density of patients in the wardswhich resulted in more shedding of bacteria and agitation ofair Besides the environmental factors led to poor indoor airquality
Among all the 8 hospitals studied general ward of H7and H8 and emergency ward of H3 and H7 compara-tively showed a good air quality According to SanitaryStandards for NonIndustrial Premises European Com-mission (Table 6) indoor air having bacterial load lt50 cfum3 is considered to be of good air quality Most of thehospitals as shown in Table 7 were under intermediatedegree of air pollution as the bacterial load present in thosehospitals was in the range of 100ndash500 cfum3 According tothe work conducted by WHO experts total bacterial load
should not exceed 1000 cfum3 Similarly in this study allthe hospitals had bacterial load less than 1000 cfum3 in-dicating a satisfactory level of air quality
Out of 8 hospitals which can be seen in Table 2Staphylococuus aureus (4718) was isolated from 7 hos-pitals Among the two wards general ward showed a highoccurrence of S aureus (2885) than emergency ward(1833) S aureus a normal flora of the human body re-siding in the nasal passage is a leading pathogen causingnosocomial infection because of which among all the Gram-positive cocci isolated S aureus was the targeted Gram-positive organism of this study )e most common source ofS aureus is sneezing In a similar study done by Qudiesatet al [14] in selected hospitals of Zarqa city Jordan S aureus(162) was found to be the predominant organism
Other isolated and identified Gram-positive cocci in thisstudy were CoNS Streptococcus spp and Micrococcus sppOut of 8 hospitals they were isolated from 6 3 and 1hospitals respectively interpreted in Table 2 In a studycarried out by Sapkota et al [15] they screened out S aureus(571) followed byMicrococcus spp (26) CoNS (299)and Gram-negative bacteria from the air culture of gov-ernment hospitals of Nepal Streptococcus spp a causativeagent of severe pneumonia associated with nosocomial in-fection was isolated from 3 hospitals Bacillus spp was alsopredominantly isolated from 5 hospitals Common speciesof Bacillus exhibit a wide range of physiologic abilities thatallow them to live in every natural environment [8]
In this study Pseudomonas spp was isolated fromgeneral ward of only one hospital H1 (182) given withinTable 2 A contrast result was obtained in a study carried outby Nandalal and Somashekar [16] where the prevalence ofPseudomonas spp was found in almost all sites (38 cfum3))e occurrence of Pseudomonas spp in only H1 in our studymight be due to poor sanitation of hospital environment andmedical equipment )ere was a lack of regular risk as-sessment of water system of the hospital (H1) building dueto which we observed stagnant water in the hospitalrsquos toiletsand bathrooms Stagnant water is known as breeding groundfor Pseudomonas spp [17] and this could be a cause ofpersistence of this bacterium in this hospital Also presenceof patients infected with Pseudomonas spp within thesampling site might have led to occurrence of Pseudomonasspp in our study
E coli was isolated from both wards of one hospital andProteus spp was also isolated from only one hospital asshown in Figure 2 )e presence of members of Enter-obacteriaceae in this study might be due to the presence oftoilets in the same hall of emergency ward which led to thedirect contact of the patients with the organisms as these arethe intestinal microflora of our human body which even-tually led to the airborne condition of these organisms
As shown in Table 3 this study categorizes the hospitalson the basis of the crowd of people and traffic of vehicles asbusy and less busy We targeted hospitals located in areashaving high population density And then after surveyingtheir annual report on the patients flow we ranked hospitalson the basis of obtained data ultimately categorizing theminto busy and less busy In our study the busy hospitals had
0
1
2
3
4
5
6
7
General wardEmergency ward
Stap
hylo
cocc
us sp
p
CoN
S
E co
liPr
oteu
s spp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
Figure 2 Prevalence of bacteria in general and emergency wards ofdifferent hospitals
International Journal of Microbiology 5
an annual patientrsquos flow ranging from around 13000 up to 400000 and the less busy hospitals had an annual patientsflow from around 4000 up to 7000)erefore busy hospitalsare those hospitals located in highly crowded location interms of people and vehicles Another classification pre-sented in Table 3 of the hospitals was done on the basis ofGovernment private and semiprivate organizationsAmong the hospitals located in busy area H5 a privatehospital showed a high prevalence of Saurues whereas H4being a semiprivate hospital showed a presence of Micro-coccus spp Similarly among the hospitals located in lessbusy area H2 a government hospital had high prevalence ofS aureus and Pseudomonas spp was isolated only from H1which is also a government hospital located in less busy area
)e dampness situation of the building might have cre-ated favorable condition for the bacterial growth which canbe dispersed through droplets and then maintained in aerialsuspension which can have health risk among people )erelative humidity of the air has shown to be of major im-portance in the survival ofmicroorganisms)emechanism istotally related to organismrsquos surface biochemistry One
mechanism that explains the loss of viability in associationwith very low relative humidity is structural change in thelipid bilayer of the cell membrane as the water is lost from thecell Cell membrane bilayer changes from the typical crys-talline structures to the gel phase )is structural phasetransition affects cell surface protein configuration and ulti-mately results in inactivation of the cell In general Gram-negative bacteria react unfavorably to the desiccation whereasGram-positive bacteria are more tolerant to desiccation [18])is can be possible reasoning for more prevalence of Gram-positive bacteria Hence the most important means foravoiding adverse health effects is minimization of persistentdampness and microbial growth on interior surfaces and inbuilding structures And also it was stated by the WHO thatdampness situation has to be considered as the risk indicatorfor health risk of biological contaminants of indoor air [5]
F test was applied to study the difference in air qualitybetween the wards of every hospital and between hospitals Byusing the formula mentioned in (1) Fcal and Ftab were cal-culated Since Fcal (092 00131) is less than Ftab (5991 379)the null hypothesis H0 is accepted )e statistical analysisshowed that there is no significant difference in the con-centrations of bacteria between general and emergency wards)is explains that both the wards of all the eight differenthospitals which were studied had a similar bacterial loadstatistically Similarly there are no significant differences inthe concentrations of bacteria between the hospitals
In this study gentamicin and ofloxacin were found to be8181 effective towards isolates of S aureus as shown inTable 8 Hence it can be used as drug of choice for the
Table 3 Prevalence of S aureus and Pseudomonas spp in context with the condition and type of the organization
S N Condition Organization HospitalsNumber of organisms
S aureus Pseudomonas spp
1 Busy
Government mdash mdash mdash
Private H5 39 NilH6 20 Nil
Semiprivate H4 29 Nil
2 Less busy
Government H1 19 6H2 53 Nil
Private H7 6 NilH8 5 Nil
Semiprivate H3 Nil Nil
Table 4 Distribution of bacterial load in different wards of different hospitals
S N HospitalsNumber of colonies (observed) Number of colonies (calculated)
(cfum3) TotalEmergency ward General ward Emergency ward General ward
1 H1 43 52 96 116 2122 H2 75 57 172 128 3003 H3 59 11 132 26 1584 H4 88 63 206 142 3485 H5 49 37 110 82 1926 H6 48 51 108 114 2227 H7 12 12 28 30 588 H8 42 46 44 102 146Total 414 (5572) 329 (442)
Table 5 Standards for air quality evaluation according to EuropeanUnion Guidelines to Good Manufacturing Practice (EuropeanCommission 2008) [12]
S N Grade Cfum3 Cfuplate1 A lt1 lt12 B 10 53 C 100 504 D 200 100
6 International Journal of Microbiology
treatment of nosocomial infections caused by SaureusIsolated S aureus was found to be less susceptible toerythromycin (3636) and chloramphenicol (3636)
Asia is one of the epicenters of antimicrobial resistanceworldwide and this is an increasing public health concernMDR pathogens have been widely disseminated both inhospitals and throughout communities in many countries[19] )e relative frequency of P aeruginosa as a nosocomialpathogen has increased although wide variations are seenamong individual medical centers Pseudomonas aeruginosacontinues to be a major pathogen among patients with im-munosuppressant cystic fibrosis malignancy and trauma[20] Despite the high prevalence of MDR or XDR Pseudo-monas in Asia the clinical consequences of antimicrobialresistance are not fully understood in many Asian countriesIn a Korean hospital antimicrobial resistance especially toceftazidime and imipenem adversely affected the outcomes ofpatients with Pseudomonas aeruginosa bacteraemia Rates ofcarbapenem-resistant Pseudomonas were very high andMDRnonfermenters were highly prevalent in Asian countries[20] In this study (Table 9) Pseudomonas spp was highlysusceptible to ceftriaxone (833) and ofloxacin (833) Andit was resistant to imipenem It might be because of themutation of genes Due to the higher sensitivity towardsceftriaxone and ofloxacin it can be used as a drug of choice forthe treatment of nosocomial infections caused by this bac-terium (Tables 10 and 11)
6 Conclusion
From the 8 hospital samples processed in this study 245isolates of 8 different bacterial species were obtained Bothof the wards (general and emergency) of all the eighthospitals were found to be under C- and D-grade of airquality According to Sanitary Standard for Non-IndustrialPremises European Commission the majority of generalwards of 5 hospitals were found to be intermediatelypolluted and similar results were found in the case ofemergency wards of 5 hospitals High bacterial load wasfound to be present in H4 (348 cfum3) which is a semi-private hospital located in busy area And low bacterial loadwas found in H7 (58 cfum3) which is a private hospitallocated in less busy area Staphylococcus aureus (4718)was one of the major organisms isolated from 7 out of 8hospitals Pseudomonas spp (182) was isolated from
Table 6 Evaluation of air quality according to the sanitary standards for nonindustrial premises (CEC 1993) [13]
S N Group of microbes Range values (Cfum3) Air pollution degree1 Bacteria lt50 Very low2 Bacteria 50ndash100 Low3 Bacteria 100ndash500 Intermediate4 Bacteria 500ndash2000 High5 Bacteria gt2000 Very high
Table 7 Air pollution degree according to Sanitary Standards For Non-Industrial Premises European Commission
S N Hospitals Number of colonies in general ward(calculated)
Air pollution(degree)
Number of colonies in emergency ward(calculated)
Air pollution(degree)
1 H1 96 Low 116 Intermediate2 H2 172 Intermediate 128 Intermediate3 H3 132 Intermediate 26 Very low4 H4 206 Intermediate 142 Intermediate5 H5 110 Intermediate 82 Low6 H6 108 Intermediate 114 Intermediate7 H7 28 Very low 30 Very low8 H8 44 Very low 102 IntermediateTotal 896 740
Table 8 Antibiotic susceptibility pattern of Staphylococcus aureus
Antibiotics usedSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Gentamicin 9 8181 1 625 1 625 11Cotrimoxazole 5 4545 2 1818 4 3636 11Ampicillin 6 5454 3 2727 2 1818 11Erythromycin 4 3636 5 4545 2 1818 11Ofloxacin 9 8181 0 0 2 1818 11Chloramphenicol 4 3636 3 2727 4 3636 11
Table 9 Antibiotic susceptibility pattern of Pseudomonas spp
AntibioticsSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Amoxycillin 4 6667 2 333 0 0 6Ceftriaxone 5 833 1 166 0 0 6Cefotaxime 1 166 2 333 3 50 6Imipenem 0 0 0 0 6 100 6Ofloxacin 5 833 1 166 0 0 6
International Journal of Microbiology 7
general ward of only one hospital Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcusspp in 3 hospitals whereas Micrococcus spp was isolatedfrom only 1 hospital and Bacillus spp was isolated from 7hospitals (Figure 1) Out of 8 hospitals Ecoli was isolatedfrom 2 hospitals and Proteus spp was isolated from only 1hospital While performing the antibiotic susceptibility testfor S aureus it was found to be highly susceptible togentamicin (8181) and ofloxacin (8181) whereas it wasless susceptible to erythromycin (3636) and chloram-phenicol (3636) Similarly in the case of AST of Pseu-domonas spp it was found to be susceptible to ceftriaxone(833) and ofloxacin (833) whereas Pseudomonas sppdid not show susceptibility against imipenem )e highbacterial concentrations of air obtained in this study mightbe potential risk factors for spread of nosocomial infectionin respective hospitals
Data Availability
Further data related to this study can be made available uponrequest
Conflicts of Interest
)e authors declare that they have no conflicts of interest
Acknowledgments
It is with immense gratitude that we acknowledge ourrespected supervisor Mrs Pramila Parajuli LecturerDepartment of Microbiology St Xavierrsquos College Mai-tighar for her continuous support patience constructivesuggestion and expert guidance throughout the researchwork We are indebted to Mr Sudhakar Pant HODDepartment of Microbiology St Xavierrsquos College forproviding us opportunity to designate this project Weowe a deepest gratitude to all the respected lecturers forsharing their knowledge regarding this project and lab
staff members MrGopi Neupane and Mrs Anju LamaDepartment of Microbiology St Xavierrsquos College fortheir kind support Also we consider it an honour to workwith the administration staff members and nursing in-charge of the hospitals and thank them for their co-operation and generous technical support during theresearch work Along with our project group members weshare the credit of our work with all our acquaintance thathelped us in the course of conducting the research workFinally it gives us great pleasure in acknowledging thesupport and help of our family for their blessings con-tinuous motivation encouragement and unambiguoussupport throughout as always which brought us this farWe were a group of four members involved in this re-search and each individual had a share of Nrs 7000 witha total cost of Nrs 28000
References
[1] P Srikanth S Sudharsanam and R andSteinberg ldquoBio-aerosols in indoor environment composition health effectsand analysisrdquo Indian Journal of Medical Microbiology vol 26no 4 pp 302ndash312 2008
[2] R M Klevens J R Edwards C L Richards et al ldquoEstimatinghealth care-associated infections and deaths in US hospitalsrdquoPublic Health Reports vol 122 no 2 pp 160ndash166 2007
[3] B Ozer B C O Akkurt N Duran Y Onlen L Savas andS Turhanoglu ldquoEvaluation of nosocomial infections and riskfactors in critically ill patientsrdquo Medical Science Monitorvol 17 no 3 pp PH17ndashPH22 2011
[4] Isolation and Identification of Air Microflora in MicrobiologyLaboratoryosun State Polytechnic researchCluecom IreeNigeria 2015 httpsnairaprojectcomprojects1465html
[5] S F Hayleeyesus and A M Manaye ldquoMicrobiological qualityof indoor air in university librariesrdquo Asian Pacific Journal ofTropical Biomedicine vol 4 no 1 pp S312ndashS317 2014
[6] M J Mendell A G Mirer K Cheung et al ldquoHealth effectsassociated with dampness and mouldrdquo inWho Guidelines forIndoor Air Quality Dampness and Mould WHO RegionalOffice for Europe Copenhangen Denmark 2009 httpswwwncbinlmnihgovbooksNBK143940
[7] R Lawley ldquoSomething in the air monitoring airborne microor-ganismsrdquo Food Engineering and Ingredients pp 6ndash10 2009
[8] Clinical and Laboratory Standards Institute (CLSI) Antimi-crobial Susceptibility Testing Standards 2015
[9] A B Sthapit R P Yadav S P Khanal and P M DongolApplied Statistics Analysis of Variance-ANOVA AsmitaBooks Publishers amp Distributors (P) Ltd Kathmandu Nepal2014
[10] A A Anderson ldquoNew sampler for the collection sizing andenumeration of viable air borne particlesrdquo Journal of Bacte-riology vol 76 pp 471ndash484 1958
Table 10 Zone of size standard interpretative chart (HiMedia Catalogue 2017-18) Staphylococcus spp [21]
Antimicrobial agent Symbol Disc content Resistant (mm or less) Intermediate (mm) Sensitive (mm or more)Ampicillin AMP 10 μg 28 mdash 29Chloramphenicol C 30 μg 12 13ndash17 18Cotrimoxazole COT 25 μg 10 11ndash15 16Erythromycin E 15 μg 13 14ndash22 23Gentamicin GEN 10 μg 12 13ndash14 15Ofloxacin OF 5 μg 14 15ndash17 18
Table 11 Zone of size standard interpretative chart (HiMediaCatalogue 2017-18) Pseudomonas spp [21]
Antibiotics Sensitive Intermediate ResistantAmoxycillin 17 14ndash16 13Ceftriaxone 21 14ndash20 13Cefotaxime 23 15ndash22 14Imipenem 16 14-15 13Ofloxacin 16 13ndash15 12
8 International Journal of Microbiology
[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

aureus and Pseudomonas spp are developing highmultidrugresistance leading to birth of MDRSA and MDRPAeventually causing ineffective drug treatment [3]
Gas dust particles water vapor and air contain mi-croorganisms )ere are vegetative cells and spores ofbacteria fungi algae viruses and protozoal cysts Since air isoften exposed to sunlight it has higher temperature and lessmoisture Air serves as transport or dispersal medium formicroorganism therefore they occur in relatively smallnumber in air when compared with soil and water [4]
)e air found inside the building is referred to as indoorair)emost common genera of bacteria found in indoor airare Staphylococci Bacilli and Clostridium [5] MRSA(methicillin-resistant Staphylococcus aureus) andgentamicin-resistant Gram-negative bacteria are found to beserious nowadays [1] People spend 80ndash90 of their timein indoor environments by breathing on average 14m3 of airper day Moreover the environmental and physical factorsmainly include temperature humidity air exchange rate airmovement and building structures location poor designventilation system as well as interior redesign respectivelywhich enhance microorganismrsquos growth and multiplicationin the indoor atmosphere [5]
A review made by the WHO on the number of epide-miological studies showed that there is sufficient evidencefor an association between indoor dampness-related factorsand a wide range of effects on respiratory health includingasthma development asthma exacerbation current asthmarespiratory infections upper respiratory tract symptomscough wheeze and dyspnoea [6]
Hence this study provides clear data of microbial airquality and respective bacterial loads in indoor air of hos-pitals of Kathmandu district Kathmandu having an area of395 km2 is the most densely populated district of Nepal)erefore we conducted research in hospitals located incomparatively high population density area which repre-sented major areas of Kathmandu district Identificationsucceeded by antimicrobial susceptibility pattern of thebacteria isolated from the indoor air of hospitals was de-termined by using multiple drugs Globally the emergenceof drug-resistant bacteria is posing as a threat in deliveranceof effective medical care Once a person contracts nosoco-mial infection the initial step for management of the in-fection is antibiotic administration )e commonly usedantibiotics for nosocomial agents Staphylococcus spp andPseudomonas spp were identified and the susceptibility ofthe organisms to antibiotics was recorded )erefore westudied antibiotic resistance which is well pronounced indeveloping countries like Nepal so as to alert clinicians andassist them in proper treatment decisions and propermanagement of such patients
2 Materials and Methodology
21 Materials
211 Equipment Impactor air sampler autoclave hot airoven incubator microscope refrigerator weighing machinegas burners inoculating loop andwires were used in this study
212 Microbiological Media Nutrient broth triple sugariron agar nutrient agar simmons citrate agar mannitol saltagar sulphur indole motility media MacConkey agaroxidativefermentative agar urease broth Mueller-Hintonagar cetrimide agar methyl red-Voges-Proskauer brothand blood agar were used in this study
213 Chemicals and Reagents Barrittrsquos reagent oxidasereagent Kovacrsquos reagent crystal violet Gram iodineacetone-alcohol Safranin blood plasma normal salinehydrogen peroxide nitrate reagent A and nitrate reagent Bwere used in this study
214 Antibiotic Discs All the antibiotic discs used for thesusceptibility tests were from HiMedia Laboratories PvtLimited Bombay India )e antibiotics used were as fol-lows ampicillin ofloxacin erythromycin ceftriaxonegentamicin amikacin chloramphenicol ceftazidime andcotrimoxazole
22 Miscellaneous Conical flasks cotton distilled waterdropper forceps glass slides cover slips immersion oilLysol measuring cylinder Petri dishes pipettes spatula testtubes and cotton swab
3 Methodology
31 Study Area Two wardsmdashemergency ward and generalwardmdashof different hospitals of Kathmandu district werechosen for the comparative study of hospital indoor airmicroflora using a microbiological air sampler
32 Sample Collection We performed an active impactorsampling method by using ldquoHi-Airrdquo air sampler )e heightof the sampler is 54 cm which is also the sampling height Asprementioned we had only one sampler due to which wecollected samples one after another We allocated two dif-ferent sites in the emergency and general wards of thehospitals Sampling from both the wards of one hospital wasdone in a same day whereas the sampling from differenthospitals was performed on different days
Impactor samplers use a solid or adhesive medium suchas agar gel Typically air is drawn into the sampling head bya pump or fan and accelerated through a perforated plate(sieve samplers) [7] A standard plate of nutrient agar (totalcount) mannitol salt agar (specifically for Staphylococcusaureus) blood agar (specifically for Streptococcus species)MacConkey agar (specifically for Gram-negative bacteria)and cetrimide agar (specifically for Pseudomonas species)was aseptically prepared and used
)e impeller speed of 2500 rpmndash2600 rpm was so ad-justed that 100 liters of air was sampled every minuteaccording to the catalogue of the air sampler We had a totalof 5 plates for each ward and a single agar plate was placed inthe air sampler for 5minutes so that 500 liters of air wassampled )erefore the sampling time at one ward was25minutes with a preparation time of 15minutes Overall
2 International Journal of Microbiology
our sampling period was 80minutes in one hospital As weperformed sampling on two different days a week so ourtotal sampling period for 8 hospitals was 1month
33 Transportation of the Sample Immediately after col-lection of samples the Petri plates were taken to the Lab-oratory of Microbiology of St Xavierrsquos College )ese Petriplates were incubated in an inverted position at 37degC for24 hrs
34 Microbiological Examination of the Sample After in-cubation total plate count was done on the basis of growthon NA plates )e colony characteristics were studied frommannitol salt agar MacConkey agar blood agar andcetrimide agar After this the colonies were subjected toGram staining )en for Gram-positive organisms bio-chemical tests such as catalase oxidase and coagulase andOF tests were performed whereas for Gram-negative or-ganisms biochemical tests such as IMViC TSIA ureasecatalse oxidase and OF tests were performed
35 Antibiotic Sensitivity Test Among the identified Gram-positive cocci and Gram-negative bacteria only Staphylo-coccus aureus and Pseudomonas spp were further tested fortheir AST pattern respectively For this representativecolonies were selected and were suspended in nutrient brothand the suspension was standardized with respect to 05McFarland solutions )e susceptibility of the isolated or-ganisms towards the antibiotics was tested by usingKirbeyndashBauerrsquos Method on Mueller-Hinton agar (CLSI2015) [8]
For Staphylococcus aureus gentamicin cotrimoxazoleampicillin erythromycin ofloxacin and chloramphenicolwere used And for Pseudomonas spp amoxicillin cef-triaxone cefotaxime imipenem and ofloxacin were used
36 Statistical Analysis )e data thus generated were an-alyzed by simple mean value percentage and test of sig-nificance by using two-way ANOVA to determinesignificant differences between the bacterial load and dif-ferent wards and also between the hospitals where the levelof significance was 5 for the analysis
Test statistics under H0 the two ANOVA F-statistics are
Fcal MSCMSE
Fcal MSRMSE
(1)
where MSCmean sum of square of variation due to col-umns MSRmean sum of square of variation due torows and MSEmean sum of square of variation due toerrors [9]
37 Limitations(i) As we are undergraduate students our research
work was carried out in college laboratory )ere
were several group projects simultaneously runningin the laboratory where we all shared same spaceinstruments and resources like Petri plates tubesmedia and incubator
(ii) )e project being a part of bachelorrsquos curriculumwas conducted alongside our academic classes Ourresearch time was limited to 5 working days with5 hours per day in the college laboratory
(iii) From each air sample plates we required peculiarcolonies on nutrient agar to be further processedand subcultured Our prospected methodol-ogy required around 50ndash60 number of Petri platesfor complete processing of a single air sampleplate
)e above-mentioned reasons limited our ability to carryout our duplicate samples We therefore decided to focuson original samples rather than the duplicate samples
4 Results
)e following formula was used to calculate bacterial load(cfum3)
Pr N1N
+1
Nminus 1+
1Nminus 2
+ middot middot middot +1
Nminus r + 11113874 1113875 (2)
where Pr probable statistical total r number of CFUcounted on 90mm Petri dish and N total number of holesin the sampling head 380 holes [10]
)e maximum growth of bacteria was observed inemergency wards (5572) as compared to general wards(442) of different hospitals High bacterial load (348 cfum3) and low bacterial load (58 cfum3) were found in the airof hospitals H4 and H7 respectively
Out of 8 hospitals general wards of 3 hospitals (H1 H7and H8) and emergency wards of 3 hospitals (H3 H5 andH7) showed a C-grade air quality And general wards of 5hospitals (H2 H3 H4 H5 and H6) and emergency wards of5 hospitals (H1 H2 H4 H6 and H8) were under D-gradeair quality
Among 8 hospitals general wards of H7 and H8 andemergency wards of H3 and H7 showed a very low degree ofbacterial air pollution (Table 1)
Out of 8 hospitals Staphylococcus aureus was isolatedfrom 7 hospitals including both general and emergencywards )e maximum percentage (1003) of S aureus wasfound to be isolated from the general ward of H2 and theleast percentage of isolates (121) was found to be also fromthe general ward of H6 )e result is shown in Table 2
41 Occurrence of Pseudomonas spp in Different HospitalsOut of 8 hospitals Pseudomonas spp was isolated only from1 hospital ie H1 in its general ward with the no of 6colonies (182)
42 Occurrence of Gram-Positive Bacteria Other than Saureus in Different Hospitals Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcus spp
International Journal of Microbiology 3
in 3 hospitals whereas Micrococcus spp was isolated fromonly 1 hospital And Bacillus spp was isolated from 7hospitals
43 Occurrence of Gram-Negative Bacteria Other thanPseudomonas spp in Different Hospitals Out of 8 hospitalsEcoli was isolated from 2 hospitals and Proteus spp wasisolated from only 1 hospital
Among 8 hospitals 3 hospitals were divided as hospitalsin busy area and 5 were divided as hospitals in less busy areaS aureus was isolated from 3 hospitals in busy area and 4hospitals in less busy area Micrococcus spp and Pseudo-monas spp were isolated only from H4 semiprivate hospitalin busy area and H1 government hospital in less busy arearespectively )e result is shown in Table 3 (busy area refersto the area having high annual patients flow less busy arearefers to the area having comparatively low annual patientsflow)
Figure 1 demonstrates that the occurrence of Staphy-lococcus aureus was found to be maximum covering 7 out of8 hospitals followed by CoNS in 6 out of 8 hospitalsStreptococcus spp and E coli were found to be in three andtwo hospitals respectively And the frequency of occurrenceofMicrococcus spp Proteus spp and Pseudomonas spp wasfound to be very least ie only in one hospital
Figure 2 demonstrates that Staphylococcus aureus wasfound to be present in general ward and emergency ward of 6and 5 hospitals respectively which was followed by CONSin the general and emergency wards of 3 and 4 hospitalsrespectively However Micrococcus spp and E Coli werepresent in both the general and emergency wards of onehospital In contrast Proteus spp and Pseudomonas sppwere only present in general wards of only one hospitalStreptococcus spp was present in general and emergencyward of 1 and 2 hospitals And Bacillus spp was present inboth the general and emergency ward of 3 and 4 hospitalsrespectively
)e most effective antibiotic against isolated Staphylo-coccus aureus was gentamicin (8181) and ofloxacin(8181) and the least effective was chloramphenicol(3636) and erythromycin (3636)
)e most effective antibiotic against isolated Pseudo-monas spp was ceftriaxone (833) and ofloxacin (833)and least effective was cefotaxime (166)
5 Discussion
Microbiological quality assessment of indoor air is one of themost vital investigations to determine the microbial indoorair pollution )e information on the indoor microbialconcentrations of airborne bacteria is necessary both toestimate the health hazard and to create standards for indoorair-quality control [5]
)ere was a presence of certain bacterial load inemergency and general wards of 8 hospitals where the study
Table 1 Grading of hospitals according to European Union Guidelines to Good Manufacturing Practices
S N Hospitals Number of colonies in general ward(calculated)
Air quality(grade)
Number of colonies in emergency ward(calculated)
Air quality(grade)
1 H1 96 C 116 D2 H2 172 D 128 D3 H3 132 D 26 C4 H4 206 D 142 D5 H5 110 D 82 C6 H6 108 D 114 D7 H7 28 C 30 C8 H8 44 C 102 DTotal 896 740
Table 2 Number and percentage of Staphylococcus aureus indifferent wards of the hospital
S N HospitalsNumber of organism ()
Emergency ward General ward1 H1 Nil 19 (577)2 H2 20 (483) 33 (1003)3 H3 Nil Nil4 H4 18 (434) 11 (334)5 H5 16 (386) 23 (699)6 H6 16 (386) 4 (121)7 H7 6 (144) Nil8 H8 Nil 5 (151)Total 76 95)e percentage of isolated S aureus was calculated on the basis of total platecount on NA
0
Stap
hylo
cocc
us a
ureu
s
CoN
S
E co
li
Prot
eus s
pp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
12345678
Num
ber o
f hos
pita
ls
Figure 1 Prevalence of the microorganisms in different hospitals
4 International Journal of Microbiology
was carried out From Table 4 we can observe that amongthe two wards emergency ward was found to have highbacterial load (5572) in comparison to general ward(442) A contrast result was obtained in a study conductedby Awosika et al [11] where out of nine wards the highbacterial load was found to be in medical ward (25)whereas the least bacterial load was recorded in emergencyunit (2) Humid room environment presence of un-hygienic attached toilets poor waste management systemand high number of patients in a single room personnel andvisitors occupying the hospital might be the reasons for highbacterial load in emergency ward in this study
According to the European Union Guidelines to GoodManufacturing Practices (Table 5) indoor air possessinggreater than 100 cfum3 and 200 cfum3 bacterial loads isreferred to as C- and D-grade air quality respectively In ourstudy Table 1 demonstrates that all the general wards andemergency wards of 8 hospitals were under C- and D-gradeair quality)is might be because at the time of this study allwards were at their maximum capacity as of visitors in andout the wards the high density of patients in the wardswhich resulted in more shedding of bacteria and agitation ofair Besides the environmental factors led to poor indoor airquality
Among all the 8 hospitals studied general ward of H7and H8 and emergency ward of H3 and H7 compara-tively showed a good air quality According to SanitaryStandards for NonIndustrial Premises European Com-mission (Table 6) indoor air having bacterial load lt50 cfum3 is considered to be of good air quality Most of thehospitals as shown in Table 7 were under intermediatedegree of air pollution as the bacterial load present in thosehospitals was in the range of 100ndash500 cfum3 According tothe work conducted by WHO experts total bacterial load
should not exceed 1000 cfum3 Similarly in this study allthe hospitals had bacterial load less than 1000 cfum3 in-dicating a satisfactory level of air quality
Out of 8 hospitals which can be seen in Table 2Staphylococuus aureus (4718) was isolated from 7 hos-pitals Among the two wards general ward showed a highoccurrence of S aureus (2885) than emergency ward(1833) S aureus a normal flora of the human body re-siding in the nasal passage is a leading pathogen causingnosocomial infection because of which among all the Gram-positive cocci isolated S aureus was the targeted Gram-positive organism of this study )e most common source ofS aureus is sneezing In a similar study done by Qudiesatet al [14] in selected hospitals of Zarqa city Jordan S aureus(162) was found to be the predominant organism
Other isolated and identified Gram-positive cocci in thisstudy were CoNS Streptococcus spp and Micrococcus sppOut of 8 hospitals they were isolated from 6 3 and 1hospitals respectively interpreted in Table 2 In a studycarried out by Sapkota et al [15] they screened out S aureus(571) followed byMicrococcus spp (26) CoNS (299)and Gram-negative bacteria from the air culture of gov-ernment hospitals of Nepal Streptococcus spp a causativeagent of severe pneumonia associated with nosocomial in-fection was isolated from 3 hospitals Bacillus spp was alsopredominantly isolated from 5 hospitals Common speciesof Bacillus exhibit a wide range of physiologic abilities thatallow them to live in every natural environment [8]
In this study Pseudomonas spp was isolated fromgeneral ward of only one hospital H1 (182) given withinTable 2 A contrast result was obtained in a study carried outby Nandalal and Somashekar [16] where the prevalence ofPseudomonas spp was found in almost all sites (38 cfum3))e occurrence of Pseudomonas spp in only H1 in our studymight be due to poor sanitation of hospital environment andmedical equipment )ere was a lack of regular risk as-sessment of water system of the hospital (H1) building dueto which we observed stagnant water in the hospitalrsquos toiletsand bathrooms Stagnant water is known as breeding groundfor Pseudomonas spp [17] and this could be a cause ofpersistence of this bacterium in this hospital Also presenceof patients infected with Pseudomonas spp within thesampling site might have led to occurrence of Pseudomonasspp in our study
E coli was isolated from both wards of one hospital andProteus spp was also isolated from only one hospital asshown in Figure 2 )e presence of members of Enter-obacteriaceae in this study might be due to the presence oftoilets in the same hall of emergency ward which led to thedirect contact of the patients with the organisms as these arethe intestinal microflora of our human body which even-tually led to the airborne condition of these organisms
As shown in Table 3 this study categorizes the hospitalson the basis of the crowd of people and traffic of vehicles asbusy and less busy We targeted hospitals located in areashaving high population density And then after surveyingtheir annual report on the patients flow we ranked hospitalson the basis of obtained data ultimately categorizing theminto busy and less busy In our study the busy hospitals had
0
1
2
3
4
5
6
7
General wardEmergency ward
Stap
hylo
cocc
us sp
p
CoN
S
E co
liPr
oteu
s spp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
Figure 2 Prevalence of bacteria in general and emergency wards ofdifferent hospitals
International Journal of Microbiology 5
an annual patientrsquos flow ranging from around 13000 up to 400000 and the less busy hospitals had an annual patientsflow from around 4000 up to 7000)erefore busy hospitalsare those hospitals located in highly crowded location interms of people and vehicles Another classification pre-sented in Table 3 of the hospitals was done on the basis ofGovernment private and semiprivate organizationsAmong the hospitals located in busy area H5 a privatehospital showed a high prevalence of Saurues whereas H4being a semiprivate hospital showed a presence of Micro-coccus spp Similarly among the hospitals located in lessbusy area H2 a government hospital had high prevalence ofS aureus and Pseudomonas spp was isolated only from H1which is also a government hospital located in less busy area
)e dampness situation of the building might have cre-ated favorable condition for the bacterial growth which canbe dispersed through droplets and then maintained in aerialsuspension which can have health risk among people )erelative humidity of the air has shown to be of major im-portance in the survival ofmicroorganisms)emechanism istotally related to organismrsquos surface biochemistry One
mechanism that explains the loss of viability in associationwith very low relative humidity is structural change in thelipid bilayer of the cell membrane as the water is lost from thecell Cell membrane bilayer changes from the typical crys-talline structures to the gel phase )is structural phasetransition affects cell surface protein configuration and ulti-mately results in inactivation of the cell In general Gram-negative bacteria react unfavorably to the desiccation whereasGram-positive bacteria are more tolerant to desiccation [18])is can be possible reasoning for more prevalence of Gram-positive bacteria Hence the most important means foravoiding adverse health effects is minimization of persistentdampness and microbial growth on interior surfaces and inbuilding structures And also it was stated by the WHO thatdampness situation has to be considered as the risk indicatorfor health risk of biological contaminants of indoor air [5]
F test was applied to study the difference in air qualitybetween the wards of every hospital and between hospitals Byusing the formula mentioned in (1) Fcal and Ftab were cal-culated Since Fcal (092 00131) is less than Ftab (5991 379)the null hypothesis H0 is accepted )e statistical analysisshowed that there is no significant difference in the con-centrations of bacteria between general and emergency wards)is explains that both the wards of all the eight differenthospitals which were studied had a similar bacterial loadstatistically Similarly there are no significant differences inthe concentrations of bacteria between the hospitals
In this study gentamicin and ofloxacin were found to be8181 effective towards isolates of S aureus as shown inTable 8 Hence it can be used as drug of choice for the
Table 3 Prevalence of S aureus and Pseudomonas spp in context with the condition and type of the organization
S N Condition Organization HospitalsNumber of organisms
S aureus Pseudomonas spp
1 Busy
Government mdash mdash mdash
Private H5 39 NilH6 20 Nil
Semiprivate H4 29 Nil
2 Less busy
Government H1 19 6H2 53 Nil
Private H7 6 NilH8 5 Nil
Semiprivate H3 Nil Nil
Table 4 Distribution of bacterial load in different wards of different hospitals
S N HospitalsNumber of colonies (observed) Number of colonies (calculated)
(cfum3) TotalEmergency ward General ward Emergency ward General ward
1 H1 43 52 96 116 2122 H2 75 57 172 128 3003 H3 59 11 132 26 1584 H4 88 63 206 142 3485 H5 49 37 110 82 1926 H6 48 51 108 114 2227 H7 12 12 28 30 588 H8 42 46 44 102 146Total 414 (5572) 329 (442)
Table 5 Standards for air quality evaluation according to EuropeanUnion Guidelines to Good Manufacturing Practice (EuropeanCommission 2008) [12]
S N Grade Cfum3 Cfuplate1 A lt1 lt12 B 10 53 C 100 504 D 200 100
6 International Journal of Microbiology
treatment of nosocomial infections caused by SaureusIsolated S aureus was found to be less susceptible toerythromycin (3636) and chloramphenicol (3636)
Asia is one of the epicenters of antimicrobial resistanceworldwide and this is an increasing public health concernMDR pathogens have been widely disseminated both inhospitals and throughout communities in many countries[19] )e relative frequency of P aeruginosa as a nosocomialpathogen has increased although wide variations are seenamong individual medical centers Pseudomonas aeruginosacontinues to be a major pathogen among patients with im-munosuppressant cystic fibrosis malignancy and trauma[20] Despite the high prevalence of MDR or XDR Pseudo-monas in Asia the clinical consequences of antimicrobialresistance are not fully understood in many Asian countriesIn a Korean hospital antimicrobial resistance especially toceftazidime and imipenem adversely affected the outcomes ofpatients with Pseudomonas aeruginosa bacteraemia Rates ofcarbapenem-resistant Pseudomonas were very high andMDRnonfermenters were highly prevalent in Asian countries[20] In this study (Table 9) Pseudomonas spp was highlysusceptible to ceftriaxone (833) and ofloxacin (833) Andit was resistant to imipenem It might be because of themutation of genes Due to the higher sensitivity towardsceftriaxone and ofloxacin it can be used as a drug of choice forthe treatment of nosocomial infections caused by this bac-terium (Tables 10 and 11)
6 Conclusion
From the 8 hospital samples processed in this study 245isolates of 8 different bacterial species were obtained Bothof the wards (general and emergency) of all the eighthospitals were found to be under C- and D-grade of airquality According to Sanitary Standard for Non-IndustrialPremises European Commission the majority of generalwards of 5 hospitals were found to be intermediatelypolluted and similar results were found in the case ofemergency wards of 5 hospitals High bacterial load wasfound to be present in H4 (348 cfum3) which is a semi-private hospital located in busy area And low bacterial loadwas found in H7 (58 cfum3) which is a private hospitallocated in less busy area Staphylococcus aureus (4718)was one of the major organisms isolated from 7 out of 8hospitals Pseudomonas spp (182) was isolated from
Table 6 Evaluation of air quality according to the sanitary standards for nonindustrial premises (CEC 1993) [13]
S N Group of microbes Range values (Cfum3) Air pollution degree1 Bacteria lt50 Very low2 Bacteria 50ndash100 Low3 Bacteria 100ndash500 Intermediate4 Bacteria 500ndash2000 High5 Bacteria gt2000 Very high
Table 7 Air pollution degree according to Sanitary Standards For Non-Industrial Premises European Commission
S N Hospitals Number of colonies in general ward(calculated)
Air pollution(degree)
Number of colonies in emergency ward(calculated)
Air pollution(degree)
1 H1 96 Low 116 Intermediate2 H2 172 Intermediate 128 Intermediate3 H3 132 Intermediate 26 Very low4 H4 206 Intermediate 142 Intermediate5 H5 110 Intermediate 82 Low6 H6 108 Intermediate 114 Intermediate7 H7 28 Very low 30 Very low8 H8 44 Very low 102 IntermediateTotal 896 740
Table 8 Antibiotic susceptibility pattern of Staphylococcus aureus
Antibiotics usedSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Gentamicin 9 8181 1 625 1 625 11Cotrimoxazole 5 4545 2 1818 4 3636 11Ampicillin 6 5454 3 2727 2 1818 11Erythromycin 4 3636 5 4545 2 1818 11Ofloxacin 9 8181 0 0 2 1818 11Chloramphenicol 4 3636 3 2727 4 3636 11
Table 9 Antibiotic susceptibility pattern of Pseudomonas spp
AntibioticsSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Amoxycillin 4 6667 2 333 0 0 6Ceftriaxone 5 833 1 166 0 0 6Cefotaxime 1 166 2 333 3 50 6Imipenem 0 0 0 0 6 100 6Ofloxacin 5 833 1 166 0 0 6
International Journal of Microbiology 7
general ward of only one hospital Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcusspp in 3 hospitals whereas Micrococcus spp was isolatedfrom only 1 hospital and Bacillus spp was isolated from 7hospitals (Figure 1) Out of 8 hospitals Ecoli was isolatedfrom 2 hospitals and Proteus spp was isolated from only 1hospital While performing the antibiotic susceptibility testfor S aureus it was found to be highly susceptible togentamicin (8181) and ofloxacin (8181) whereas it wasless susceptible to erythromycin (3636) and chloram-phenicol (3636) Similarly in the case of AST of Pseu-domonas spp it was found to be susceptible to ceftriaxone(833) and ofloxacin (833) whereas Pseudomonas sppdid not show susceptibility against imipenem )e highbacterial concentrations of air obtained in this study mightbe potential risk factors for spread of nosocomial infectionin respective hospitals
Data Availability
Further data related to this study can be made available uponrequest
Conflicts of Interest
)e authors declare that they have no conflicts of interest
Acknowledgments
It is with immense gratitude that we acknowledge ourrespected supervisor Mrs Pramila Parajuli LecturerDepartment of Microbiology St Xavierrsquos College Mai-tighar for her continuous support patience constructivesuggestion and expert guidance throughout the researchwork We are indebted to Mr Sudhakar Pant HODDepartment of Microbiology St Xavierrsquos College forproviding us opportunity to designate this project Weowe a deepest gratitude to all the respected lecturers forsharing their knowledge regarding this project and lab
staff members MrGopi Neupane and Mrs Anju LamaDepartment of Microbiology St Xavierrsquos College fortheir kind support Also we consider it an honour to workwith the administration staff members and nursing in-charge of the hospitals and thank them for their co-operation and generous technical support during theresearch work Along with our project group members weshare the credit of our work with all our acquaintance thathelped us in the course of conducting the research workFinally it gives us great pleasure in acknowledging thesupport and help of our family for their blessings con-tinuous motivation encouragement and unambiguoussupport throughout as always which brought us this farWe were a group of four members involved in this re-search and each individual had a share of Nrs 7000 witha total cost of Nrs 28000
References
[1] P Srikanth S Sudharsanam and R andSteinberg ldquoBio-aerosols in indoor environment composition health effectsand analysisrdquo Indian Journal of Medical Microbiology vol 26no 4 pp 302ndash312 2008
[2] R M Klevens J R Edwards C L Richards et al ldquoEstimatinghealth care-associated infections and deaths in US hospitalsrdquoPublic Health Reports vol 122 no 2 pp 160ndash166 2007
[3] B Ozer B C O Akkurt N Duran Y Onlen L Savas andS Turhanoglu ldquoEvaluation of nosocomial infections and riskfactors in critically ill patientsrdquo Medical Science Monitorvol 17 no 3 pp PH17ndashPH22 2011
[4] Isolation and Identification of Air Microflora in MicrobiologyLaboratoryosun State Polytechnic researchCluecom IreeNigeria 2015 httpsnairaprojectcomprojects1465html
[5] S F Hayleeyesus and A M Manaye ldquoMicrobiological qualityof indoor air in university librariesrdquo Asian Pacific Journal ofTropical Biomedicine vol 4 no 1 pp S312ndashS317 2014
[6] M J Mendell A G Mirer K Cheung et al ldquoHealth effectsassociated with dampness and mouldrdquo inWho Guidelines forIndoor Air Quality Dampness and Mould WHO RegionalOffice for Europe Copenhangen Denmark 2009 httpswwwncbinlmnihgovbooksNBK143940
[7] R Lawley ldquoSomething in the air monitoring airborne microor-ganismsrdquo Food Engineering and Ingredients pp 6ndash10 2009
[8] Clinical and Laboratory Standards Institute (CLSI) Antimi-crobial Susceptibility Testing Standards 2015
[9] A B Sthapit R P Yadav S P Khanal and P M DongolApplied Statistics Analysis of Variance-ANOVA AsmitaBooks Publishers amp Distributors (P) Ltd Kathmandu Nepal2014
[10] A A Anderson ldquoNew sampler for the collection sizing andenumeration of viable air borne particlesrdquo Journal of Bacte-riology vol 76 pp 471ndash484 1958
Table 10 Zone of size standard interpretative chart (HiMedia Catalogue 2017-18) Staphylococcus spp [21]
Antimicrobial agent Symbol Disc content Resistant (mm or less) Intermediate (mm) Sensitive (mm or more)Ampicillin AMP 10 μg 28 mdash 29Chloramphenicol C 30 μg 12 13ndash17 18Cotrimoxazole COT 25 μg 10 11ndash15 16Erythromycin E 15 μg 13 14ndash22 23Gentamicin GEN 10 μg 12 13ndash14 15Ofloxacin OF 5 μg 14 15ndash17 18
Table 11 Zone of size standard interpretative chart (HiMediaCatalogue 2017-18) Pseudomonas spp [21]
Antibiotics Sensitive Intermediate ResistantAmoxycillin 17 14ndash16 13Ceftriaxone 21 14ndash20 13Cefotaxime 23 15ndash22 14Imipenem 16 14-15 13Ofloxacin 16 13ndash15 12
8 International Journal of Microbiology
[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

our sampling period was 80minutes in one hospital As weperformed sampling on two different days a week so ourtotal sampling period for 8 hospitals was 1month
33 Transportation of the Sample Immediately after col-lection of samples the Petri plates were taken to the Lab-oratory of Microbiology of St Xavierrsquos College )ese Petriplates were incubated in an inverted position at 37degC for24 hrs
34 Microbiological Examination of the Sample After in-cubation total plate count was done on the basis of growthon NA plates )e colony characteristics were studied frommannitol salt agar MacConkey agar blood agar andcetrimide agar After this the colonies were subjected toGram staining )en for Gram-positive organisms bio-chemical tests such as catalase oxidase and coagulase andOF tests were performed whereas for Gram-negative or-ganisms biochemical tests such as IMViC TSIA ureasecatalse oxidase and OF tests were performed
35 Antibiotic Sensitivity Test Among the identified Gram-positive cocci and Gram-negative bacteria only Staphylo-coccus aureus and Pseudomonas spp were further tested fortheir AST pattern respectively For this representativecolonies were selected and were suspended in nutrient brothand the suspension was standardized with respect to 05McFarland solutions )e susceptibility of the isolated or-ganisms towards the antibiotics was tested by usingKirbeyndashBauerrsquos Method on Mueller-Hinton agar (CLSI2015) [8]
For Staphylococcus aureus gentamicin cotrimoxazoleampicillin erythromycin ofloxacin and chloramphenicolwere used And for Pseudomonas spp amoxicillin cef-triaxone cefotaxime imipenem and ofloxacin were used
36 Statistical Analysis )e data thus generated were an-alyzed by simple mean value percentage and test of sig-nificance by using two-way ANOVA to determinesignificant differences between the bacterial load and dif-ferent wards and also between the hospitals where the levelof significance was 5 for the analysis
Test statistics under H0 the two ANOVA F-statistics are
Fcal MSCMSE
Fcal MSRMSE
(1)
where MSCmean sum of square of variation due to col-umns MSRmean sum of square of variation due torows and MSEmean sum of square of variation due toerrors [9]
37 Limitations(i) As we are undergraduate students our research
work was carried out in college laboratory )ere
were several group projects simultaneously runningin the laboratory where we all shared same spaceinstruments and resources like Petri plates tubesmedia and incubator
(ii) )e project being a part of bachelorrsquos curriculumwas conducted alongside our academic classes Ourresearch time was limited to 5 working days with5 hours per day in the college laboratory
(iii) From each air sample plates we required peculiarcolonies on nutrient agar to be further processedand subcultured Our prospected methodol-ogy required around 50ndash60 number of Petri platesfor complete processing of a single air sampleplate
)e above-mentioned reasons limited our ability to carryout our duplicate samples We therefore decided to focuson original samples rather than the duplicate samples
4 Results
)e following formula was used to calculate bacterial load(cfum3)
Pr N1N
+1
Nminus 1+
1Nminus 2
+ middot middot middot +1
Nminus r + 11113874 1113875 (2)
where Pr probable statistical total r number of CFUcounted on 90mm Petri dish and N total number of holesin the sampling head 380 holes [10]
)e maximum growth of bacteria was observed inemergency wards (5572) as compared to general wards(442) of different hospitals High bacterial load (348 cfum3) and low bacterial load (58 cfum3) were found in the airof hospitals H4 and H7 respectively
Out of 8 hospitals general wards of 3 hospitals (H1 H7and H8) and emergency wards of 3 hospitals (H3 H5 andH7) showed a C-grade air quality And general wards of 5hospitals (H2 H3 H4 H5 and H6) and emergency wards of5 hospitals (H1 H2 H4 H6 and H8) were under D-gradeair quality
Among 8 hospitals general wards of H7 and H8 andemergency wards of H3 and H7 showed a very low degree ofbacterial air pollution (Table 1)
Out of 8 hospitals Staphylococcus aureus was isolatedfrom 7 hospitals including both general and emergencywards )e maximum percentage (1003) of S aureus wasfound to be isolated from the general ward of H2 and theleast percentage of isolates (121) was found to be also fromthe general ward of H6 )e result is shown in Table 2
41 Occurrence of Pseudomonas spp in Different HospitalsOut of 8 hospitals Pseudomonas spp was isolated only from1 hospital ie H1 in its general ward with the no of 6colonies (182)
42 Occurrence of Gram-Positive Bacteria Other than Saureus in Different Hospitals Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcus spp
International Journal of Microbiology 3
in 3 hospitals whereas Micrococcus spp was isolated fromonly 1 hospital And Bacillus spp was isolated from 7hospitals
43 Occurrence of Gram-Negative Bacteria Other thanPseudomonas spp in Different Hospitals Out of 8 hospitalsEcoli was isolated from 2 hospitals and Proteus spp wasisolated from only 1 hospital
Among 8 hospitals 3 hospitals were divided as hospitalsin busy area and 5 were divided as hospitals in less busy areaS aureus was isolated from 3 hospitals in busy area and 4hospitals in less busy area Micrococcus spp and Pseudo-monas spp were isolated only from H4 semiprivate hospitalin busy area and H1 government hospital in less busy arearespectively )e result is shown in Table 3 (busy area refersto the area having high annual patients flow less busy arearefers to the area having comparatively low annual patientsflow)
Figure 1 demonstrates that the occurrence of Staphy-lococcus aureus was found to be maximum covering 7 out of8 hospitals followed by CoNS in 6 out of 8 hospitalsStreptococcus spp and E coli were found to be in three andtwo hospitals respectively And the frequency of occurrenceofMicrococcus spp Proteus spp and Pseudomonas spp wasfound to be very least ie only in one hospital
Figure 2 demonstrates that Staphylococcus aureus wasfound to be present in general ward and emergency ward of 6and 5 hospitals respectively which was followed by CONSin the general and emergency wards of 3 and 4 hospitalsrespectively However Micrococcus spp and E Coli werepresent in both the general and emergency wards of onehospital In contrast Proteus spp and Pseudomonas sppwere only present in general wards of only one hospitalStreptococcus spp was present in general and emergencyward of 1 and 2 hospitals And Bacillus spp was present inboth the general and emergency ward of 3 and 4 hospitalsrespectively
)e most effective antibiotic against isolated Staphylo-coccus aureus was gentamicin (8181) and ofloxacin(8181) and the least effective was chloramphenicol(3636) and erythromycin (3636)
)e most effective antibiotic against isolated Pseudo-monas spp was ceftriaxone (833) and ofloxacin (833)and least effective was cefotaxime (166)
5 Discussion
Microbiological quality assessment of indoor air is one of themost vital investigations to determine the microbial indoorair pollution )e information on the indoor microbialconcentrations of airborne bacteria is necessary both toestimate the health hazard and to create standards for indoorair-quality control [5]
)ere was a presence of certain bacterial load inemergency and general wards of 8 hospitals where the study
Table 1 Grading of hospitals according to European Union Guidelines to Good Manufacturing Practices
S N Hospitals Number of colonies in general ward(calculated)
Air quality(grade)
Number of colonies in emergency ward(calculated)
Air quality(grade)
1 H1 96 C 116 D2 H2 172 D 128 D3 H3 132 D 26 C4 H4 206 D 142 D5 H5 110 D 82 C6 H6 108 D 114 D7 H7 28 C 30 C8 H8 44 C 102 DTotal 896 740
Table 2 Number and percentage of Staphylococcus aureus indifferent wards of the hospital
S N HospitalsNumber of organism ()
Emergency ward General ward1 H1 Nil 19 (577)2 H2 20 (483) 33 (1003)3 H3 Nil Nil4 H4 18 (434) 11 (334)5 H5 16 (386) 23 (699)6 H6 16 (386) 4 (121)7 H7 6 (144) Nil8 H8 Nil 5 (151)Total 76 95)e percentage of isolated S aureus was calculated on the basis of total platecount on NA
0
Stap
hylo
cocc
us a
ureu
s
CoN
S
E co
li
Prot
eus s
pp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
12345678
Num
ber o
f hos
pita
ls
Figure 1 Prevalence of the microorganisms in different hospitals
4 International Journal of Microbiology
was carried out From Table 4 we can observe that amongthe two wards emergency ward was found to have highbacterial load (5572) in comparison to general ward(442) A contrast result was obtained in a study conductedby Awosika et al [11] where out of nine wards the highbacterial load was found to be in medical ward (25)whereas the least bacterial load was recorded in emergencyunit (2) Humid room environment presence of un-hygienic attached toilets poor waste management systemand high number of patients in a single room personnel andvisitors occupying the hospital might be the reasons for highbacterial load in emergency ward in this study
According to the European Union Guidelines to GoodManufacturing Practices (Table 5) indoor air possessinggreater than 100 cfum3 and 200 cfum3 bacterial loads isreferred to as C- and D-grade air quality respectively In ourstudy Table 1 demonstrates that all the general wards andemergency wards of 8 hospitals were under C- and D-gradeair quality)is might be because at the time of this study allwards were at their maximum capacity as of visitors in andout the wards the high density of patients in the wardswhich resulted in more shedding of bacteria and agitation ofair Besides the environmental factors led to poor indoor airquality
Among all the 8 hospitals studied general ward of H7and H8 and emergency ward of H3 and H7 compara-tively showed a good air quality According to SanitaryStandards for NonIndustrial Premises European Com-mission (Table 6) indoor air having bacterial load lt50 cfum3 is considered to be of good air quality Most of thehospitals as shown in Table 7 were under intermediatedegree of air pollution as the bacterial load present in thosehospitals was in the range of 100ndash500 cfum3 According tothe work conducted by WHO experts total bacterial load
should not exceed 1000 cfum3 Similarly in this study allthe hospitals had bacterial load less than 1000 cfum3 in-dicating a satisfactory level of air quality
Out of 8 hospitals which can be seen in Table 2Staphylococuus aureus (4718) was isolated from 7 hos-pitals Among the two wards general ward showed a highoccurrence of S aureus (2885) than emergency ward(1833) S aureus a normal flora of the human body re-siding in the nasal passage is a leading pathogen causingnosocomial infection because of which among all the Gram-positive cocci isolated S aureus was the targeted Gram-positive organism of this study )e most common source ofS aureus is sneezing In a similar study done by Qudiesatet al [14] in selected hospitals of Zarqa city Jordan S aureus(162) was found to be the predominant organism
Other isolated and identified Gram-positive cocci in thisstudy were CoNS Streptococcus spp and Micrococcus sppOut of 8 hospitals they were isolated from 6 3 and 1hospitals respectively interpreted in Table 2 In a studycarried out by Sapkota et al [15] they screened out S aureus(571) followed byMicrococcus spp (26) CoNS (299)and Gram-negative bacteria from the air culture of gov-ernment hospitals of Nepal Streptococcus spp a causativeagent of severe pneumonia associated with nosocomial in-fection was isolated from 3 hospitals Bacillus spp was alsopredominantly isolated from 5 hospitals Common speciesof Bacillus exhibit a wide range of physiologic abilities thatallow them to live in every natural environment [8]
In this study Pseudomonas spp was isolated fromgeneral ward of only one hospital H1 (182) given withinTable 2 A contrast result was obtained in a study carried outby Nandalal and Somashekar [16] where the prevalence ofPseudomonas spp was found in almost all sites (38 cfum3))e occurrence of Pseudomonas spp in only H1 in our studymight be due to poor sanitation of hospital environment andmedical equipment )ere was a lack of regular risk as-sessment of water system of the hospital (H1) building dueto which we observed stagnant water in the hospitalrsquos toiletsand bathrooms Stagnant water is known as breeding groundfor Pseudomonas spp [17] and this could be a cause ofpersistence of this bacterium in this hospital Also presenceof patients infected with Pseudomonas spp within thesampling site might have led to occurrence of Pseudomonasspp in our study
E coli was isolated from both wards of one hospital andProteus spp was also isolated from only one hospital asshown in Figure 2 )e presence of members of Enter-obacteriaceae in this study might be due to the presence oftoilets in the same hall of emergency ward which led to thedirect contact of the patients with the organisms as these arethe intestinal microflora of our human body which even-tually led to the airborne condition of these organisms
As shown in Table 3 this study categorizes the hospitalson the basis of the crowd of people and traffic of vehicles asbusy and less busy We targeted hospitals located in areashaving high population density And then after surveyingtheir annual report on the patients flow we ranked hospitalson the basis of obtained data ultimately categorizing theminto busy and less busy In our study the busy hospitals had
0
1
2
3
4
5
6
7
General wardEmergency ward
Stap
hylo
cocc
us sp
p
CoN
S
E co
liPr
oteu
s spp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
Figure 2 Prevalence of bacteria in general and emergency wards ofdifferent hospitals
International Journal of Microbiology 5
an annual patientrsquos flow ranging from around 13000 up to 400000 and the less busy hospitals had an annual patientsflow from around 4000 up to 7000)erefore busy hospitalsare those hospitals located in highly crowded location interms of people and vehicles Another classification pre-sented in Table 3 of the hospitals was done on the basis ofGovernment private and semiprivate organizationsAmong the hospitals located in busy area H5 a privatehospital showed a high prevalence of Saurues whereas H4being a semiprivate hospital showed a presence of Micro-coccus spp Similarly among the hospitals located in lessbusy area H2 a government hospital had high prevalence ofS aureus and Pseudomonas spp was isolated only from H1which is also a government hospital located in less busy area
)e dampness situation of the building might have cre-ated favorable condition for the bacterial growth which canbe dispersed through droplets and then maintained in aerialsuspension which can have health risk among people )erelative humidity of the air has shown to be of major im-portance in the survival ofmicroorganisms)emechanism istotally related to organismrsquos surface biochemistry One
mechanism that explains the loss of viability in associationwith very low relative humidity is structural change in thelipid bilayer of the cell membrane as the water is lost from thecell Cell membrane bilayer changes from the typical crys-talline structures to the gel phase )is structural phasetransition affects cell surface protein configuration and ulti-mately results in inactivation of the cell In general Gram-negative bacteria react unfavorably to the desiccation whereasGram-positive bacteria are more tolerant to desiccation [18])is can be possible reasoning for more prevalence of Gram-positive bacteria Hence the most important means foravoiding adverse health effects is minimization of persistentdampness and microbial growth on interior surfaces and inbuilding structures And also it was stated by the WHO thatdampness situation has to be considered as the risk indicatorfor health risk of biological contaminants of indoor air [5]
F test was applied to study the difference in air qualitybetween the wards of every hospital and between hospitals Byusing the formula mentioned in (1) Fcal and Ftab were cal-culated Since Fcal (092 00131) is less than Ftab (5991 379)the null hypothesis H0 is accepted )e statistical analysisshowed that there is no significant difference in the con-centrations of bacteria between general and emergency wards)is explains that both the wards of all the eight differenthospitals which were studied had a similar bacterial loadstatistically Similarly there are no significant differences inthe concentrations of bacteria between the hospitals
In this study gentamicin and ofloxacin were found to be8181 effective towards isolates of S aureus as shown inTable 8 Hence it can be used as drug of choice for the
Table 3 Prevalence of S aureus and Pseudomonas spp in context with the condition and type of the organization
S N Condition Organization HospitalsNumber of organisms
S aureus Pseudomonas spp
1 Busy
Government mdash mdash mdash
Private H5 39 NilH6 20 Nil
Semiprivate H4 29 Nil
2 Less busy
Government H1 19 6H2 53 Nil
Private H7 6 NilH8 5 Nil
Semiprivate H3 Nil Nil
Table 4 Distribution of bacterial load in different wards of different hospitals
S N HospitalsNumber of colonies (observed) Number of colonies (calculated)
(cfum3) TotalEmergency ward General ward Emergency ward General ward
1 H1 43 52 96 116 2122 H2 75 57 172 128 3003 H3 59 11 132 26 1584 H4 88 63 206 142 3485 H5 49 37 110 82 1926 H6 48 51 108 114 2227 H7 12 12 28 30 588 H8 42 46 44 102 146Total 414 (5572) 329 (442)
Table 5 Standards for air quality evaluation according to EuropeanUnion Guidelines to Good Manufacturing Practice (EuropeanCommission 2008) [12]
S N Grade Cfum3 Cfuplate1 A lt1 lt12 B 10 53 C 100 504 D 200 100
6 International Journal of Microbiology
treatment of nosocomial infections caused by SaureusIsolated S aureus was found to be less susceptible toerythromycin (3636) and chloramphenicol (3636)
Asia is one of the epicenters of antimicrobial resistanceworldwide and this is an increasing public health concernMDR pathogens have been widely disseminated both inhospitals and throughout communities in many countries[19] )e relative frequency of P aeruginosa as a nosocomialpathogen has increased although wide variations are seenamong individual medical centers Pseudomonas aeruginosacontinues to be a major pathogen among patients with im-munosuppressant cystic fibrosis malignancy and trauma[20] Despite the high prevalence of MDR or XDR Pseudo-monas in Asia the clinical consequences of antimicrobialresistance are not fully understood in many Asian countriesIn a Korean hospital antimicrobial resistance especially toceftazidime and imipenem adversely affected the outcomes ofpatients with Pseudomonas aeruginosa bacteraemia Rates ofcarbapenem-resistant Pseudomonas were very high andMDRnonfermenters were highly prevalent in Asian countries[20] In this study (Table 9) Pseudomonas spp was highlysusceptible to ceftriaxone (833) and ofloxacin (833) Andit was resistant to imipenem It might be because of themutation of genes Due to the higher sensitivity towardsceftriaxone and ofloxacin it can be used as a drug of choice forthe treatment of nosocomial infections caused by this bac-terium (Tables 10 and 11)
6 Conclusion
From the 8 hospital samples processed in this study 245isolates of 8 different bacterial species were obtained Bothof the wards (general and emergency) of all the eighthospitals were found to be under C- and D-grade of airquality According to Sanitary Standard for Non-IndustrialPremises European Commission the majority of generalwards of 5 hospitals were found to be intermediatelypolluted and similar results were found in the case ofemergency wards of 5 hospitals High bacterial load wasfound to be present in H4 (348 cfum3) which is a semi-private hospital located in busy area And low bacterial loadwas found in H7 (58 cfum3) which is a private hospitallocated in less busy area Staphylococcus aureus (4718)was one of the major organisms isolated from 7 out of 8hospitals Pseudomonas spp (182) was isolated from
Table 6 Evaluation of air quality according to the sanitary standards for nonindustrial premises (CEC 1993) [13]
S N Group of microbes Range values (Cfum3) Air pollution degree1 Bacteria lt50 Very low2 Bacteria 50ndash100 Low3 Bacteria 100ndash500 Intermediate4 Bacteria 500ndash2000 High5 Bacteria gt2000 Very high
Table 7 Air pollution degree according to Sanitary Standards For Non-Industrial Premises European Commission
S N Hospitals Number of colonies in general ward(calculated)
Air pollution(degree)
Number of colonies in emergency ward(calculated)
Air pollution(degree)
1 H1 96 Low 116 Intermediate2 H2 172 Intermediate 128 Intermediate3 H3 132 Intermediate 26 Very low4 H4 206 Intermediate 142 Intermediate5 H5 110 Intermediate 82 Low6 H6 108 Intermediate 114 Intermediate7 H7 28 Very low 30 Very low8 H8 44 Very low 102 IntermediateTotal 896 740
Table 8 Antibiotic susceptibility pattern of Staphylococcus aureus
Antibiotics usedSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Gentamicin 9 8181 1 625 1 625 11Cotrimoxazole 5 4545 2 1818 4 3636 11Ampicillin 6 5454 3 2727 2 1818 11Erythromycin 4 3636 5 4545 2 1818 11Ofloxacin 9 8181 0 0 2 1818 11Chloramphenicol 4 3636 3 2727 4 3636 11
Table 9 Antibiotic susceptibility pattern of Pseudomonas spp
AntibioticsSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Amoxycillin 4 6667 2 333 0 0 6Ceftriaxone 5 833 1 166 0 0 6Cefotaxime 1 166 2 333 3 50 6Imipenem 0 0 0 0 6 100 6Ofloxacin 5 833 1 166 0 0 6
International Journal of Microbiology 7
general ward of only one hospital Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcusspp in 3 hospitals whereas Micrococcus spp was isolatedfrom only 1 hospital and Bacillus spp was isolated from 7hospitals (Figure 1) Out of 8 hospitals Ecoli was isolatedfrom 2 hospitals and Proteus spp was isolated from only 1hospital While performing the antibiotic susceptibility testfor S aureus it was found to be highly susceptible togentamicin (8181) and ofloxacin (8181) whereas it wasless susceptible to erythromycin (3636) and chloram-phenicol (3636) Similarly in the case of AST of Pseu-domonas spp it was found to be susceptible to ceftriaxone(833) and ofloxacin (833) whereas Pseudomonas sppdid not show susceptibility against imipenem )e highbacterial concentrations of air obtained in this study mightbe potential risk factors for spread of nosocomial infectionin respective hospitals
Data Availability
Further data related to this study can be made available uponrequest
Conflicts of Interest
)e authors declare that they have no conflicts of interest
Acknowledgments
It is with immense gratitude that we acknowledge ourrespected supervisor Mrs Pramila Parajuli LecturerDepartment of Microbiology St Xavierrsquos College Mai-tighar for her continuous support patience constructivesuggestion and expert guidance throughout the researchwork We are indebted to Mr Sudhakar Pant HODDepartment of Microbiology St Xavierrsquos College forproviding us opportunity to designate this project Weowe a deepest gratitude to all the respected lecturers forsharing their knowledge regarding this project and lab
staff members MrGopi Neupane and Mrs Anju LamaDepartment of Microbiology St Xavierrsquos College fortheir kind support Also we consider it an honour to workwith the administration staff members and nursing in-charge of the hospitals and thank them for their co-operation and generous technical support during theresearch work Along with our project group members weshare the credit of our work with all our acquaintance thathelped us in the course of conducting the research workFinally it gives us great pleasure in acknowledging thesupport and help of our family for their blessings con-tinuous motivation encouragement and unambiguoussupport throughout as always which brought us this farWe were a group of four members involved in this re-search and each individual had a share of Nrs 7000 witha total cost of Nrs 28000
References
[1] P Srikanth S Sudharsanam and R andSteinberg ldquoBio-aerosols in indoor environment composition health effectsand analysisrdquo Indian Journal of Medical Microbiology vol 26no 4 pp 302ndash312 2008
[2] R M Klevens J R Edwards C L Richards et al ldquoEstimatinghealth care-associated infections and deaths in US hospitalsrdquoPublic Health Reports vol 122 no 2 pp 160ndash166 2007
[3] B Ozer B C O Akkurt N Duran Y Onlen L Savas andS Turhanoglu ldquoEvaluation of nosocomial infections and riskfactors in critically ill patientsrdquo Medical Science Monitorvol 17 no 3 pp PH17ndashPH22 2011
[4] Isolation and Identification of Air Microflora in MicrobiologyLaboratoryosun State Polytechnic researchCluecom IreeNigeria 2015 httpsnairaprojectcomprojects1465html
[5] S F Hayleeyesus and A M Manaye ldquoMicrobiological qualityof indoor air in university librariesrdquo Asian Pacific Journal ofTropical Biomedicine vol 4 no 1 pp S312ndashS317 2014
[6] M J Mendell A G Mirer K Cheung et al ldquoHealth effectsassociated with dampness and mouldrdquo inWho Guidelines forIndoor Air Quality Dampness and Mould WHO RegionalOffice for Europe Copenhangen Denmark 2009 httpswwwncbinlmnihgovbooksNBK143940
[7] R Lawley ldquoSomething in the air monitoring airborne microor-ganismsrdquo Food Engineering and Ingredients pp 6ndash10 2009
[8] Clinical and Laboratory Standards Institute (CLSI) Antimi-crobial Susceptibility Testing Standards 2015
[9] A B Sthapit R P Yadav S P Khanal and P M DongolApplied Statistics Analysis of Variance-ANOVA AsmitaBooks Publishers amp Distributors (P) Ltd Kathmandu Nepal2014
[10] A A Anderson ldquoNew sampler for the collection sizing andenumeration of viable air borne particlesrdquo Journal of Bacte-riology vol 76 pp 471ndash484 1958
Table 10 Zone of size standard interpretative chart (HiMedia Catalogue 2017-18) Staphylococcus spp [21]
Antimicrobial agent Symbol Disc content Resistant (mm or less) Intermediate (mm) Sensitive (mm or more)Ampicillin AMP 10 μg 28 mdash 29Chloramphenicol C 30 μg 12 13ndash17 18Cotrimoxazole COT 25 μg 10 11ndash15 16Erythromycin E 15 μg 13 14ndash22 23Gentamicin GEN 10 μg 12 13ndash14 15Ofloxacin OF 5 μg 14 15ndash17 18
Table 11 Zone of size standard interpretative chart (HiMediaCatalogue 2017-18) Pseudomonas spp [21]
Antibiotics Sensitive Intermediate ResistantAmoxycillin 17 14ndash16 13Ceftriaxone 21 14ndash20 13Cefotaxime 23 15ndash22 14Imipenem 16 14-15 13Ofloxacin 16 13ndash15 12
8 International Journal of Microbiology
[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

in 3 hospitals whereas Micrococcus spp was isolated fromonly 1 hospital And Bacillus spp was isolated from 7hospitals
43 Occurrence of Gram-Negative Bacteria Other thanPseudomonas spp in Different Hospitals Out of 8 hospitalsEcoli was isolated from 2 hospitals and Proteus spp wasisolated from only 1 hospital
Among 8 hospitals 3 hospitals were divided as hospitalsin busy area and 5 were divided as hospitals in less busy areaS aureus was isolated from 3 hospitals in busy area and 4hospitals in less busy area Micrococcus spp and Pseudo-monas spp were isolated only from H4 semiprivate hospitalin busy area and H1 government hospital in less busy arearespectively )e result is shown in Table 3 (busy area refersto the area having high annual patients flow less busy arearefers to the area having comparatively low annual patientsflow)
Figure 1 demonstrates that the occurrence of Staphy-lococcus aureus was found to be maximum covering 7 out of8 hospitals followed by CoNS in 6 out of 8 hospitalsStreptococcus spp and E coli were found to be in three andtwo hospitals respectively And the frequency of occurrenceofMicrococcus spp Proteus spp and Pseudomonas spp wasfound to be very least ie only in one hospital
Figure 2 demonstrates that Staphylococcus aureus wasfound to be present in general ward and emergency ward of 6and 5 hospitals respectively which was followed by CONSin the general and emergency wards of 3 and 4 hospitalsrespectively However Micrococcus spp and E Coli werepresent in both the general and emergency wards of onehospital In contrast Proteus spp and Pseudomonas sppwere only present in general wards of only one hospitalStreptococcus spp was present in general and emergencyward of 1 and 2 hospitals And Bacillus spp was present inboth the general and emergency ward of 3 and 4 hospitalsrespectively
)e most effective antibiotic against isolated Staphylo-coccus aureus was gentamicin (8181) and ofloxacin(8181) and the least effective was chloramphenicol(3636) and erythromycin (3636)
)e most effective antibiotic against isolated Pseudo-monas spp was ceftriaxone (833) and ofloxacin (833)and least effective was cefotaxime (166)
5 Discussion
Microbiological quality assessment of indoor air is one of themost vital investigations to determine the microbial indoorair pollution )e information on the indoor microbialconcentrations of airborne bacteria is necessary both toestimate the health hazard and to create standards for indoorair-quality control [5]
)ere was a presence of certain bacterial load inemergency and general wards of 8 hospitals where the study
Table 1 Grading of hospitals according to European Union Guidelines to Good Manufacturing Practices
S N Hospitals Number of colonies in general ward(calculated)
Air quality(grade)
Number of colonies in emergency ward(calculated)
Air quality(grade)
1 H1 96 C 116 D2 H2 172 D 128 D3 H3 132 D 26 C4 H4 206 D 142 D5 H5 110 D 82 C6 H6 108 D 114 D7 H7 28 C 30 C8 H8 44 C 102 DTotal 896 740
Table 2 Number and percentage of Staphylococcus aureus indifferent wards of the hospital
S N HospitalsNumber of organism ()
Emergency ward General ward1 H1 Nil 19 (577)2 H2 20 (483) 33 (1003)3 H3 Nil Nil4 H4 18 (434) 11 (334)5 H5 16 (386) 23 (699)6 H6 16 (386) 4 (121)7 H7 6 (144) Nil8 H8 Nil 5 (151)Total 76 95)e percentage of isolated S aureus was calculated on the basis of total platecount on NA
0
Stap
hylo
cocc
us a
ureu
s
CoN
S
E co
li
Prot
eus s
pp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
12345678
Num
ber o
f hos
pita
ls
Figure 1 Prevalence of the microorganisms in different hospitals
4 International Journal of Microbiology
was carried out From Table 4 we can observe that amongthe two wards emergency ward was found to have highbacterial load (5572) in comparison to general ward(442) A contrast result was obtained in a study conductedby Awosika et al [11] where out of nine wards the highbacterial load was found to be in medical ward (25)whereas the least bacterial load was recorded in emergencyunit (2) Humid room environment presence of un-hygienic attached toilets poor waste management systemand high number of patients in a single room personnel andvisitors occupying the hospital might be the reasons for highbacterial load in emergency ward in this study
According to the European Union Guidelines to GoodManufacturing Practices (Table 5) indoor air possessinggreater than 100 cfum3 and 200 cfum3 bacterial loads isreferred to as C- and D-grade air quality respectively In ourstudy Table 1 demonstrates that all the general wards andemergency wards of 8 hospitals were under C- and D-gradeair quality)is might be because at the time of this study allwards were at their maximum capacity as of visitors in andout the wards the high density of patients in the wardswhich resulted in more shedding of bacteria and agitation ofair Besides the environmental factors led to poor indoor airquality
Among all the 8 hospitals studied general ward of H7and H8 and emergency ward of H3 and H7 compara-tively showed a good air quality According to SanitaryStandards for NonIndustrial Premises European Com-mission (Table 6) indoor air having bacterial load lt50 cfum3 is considered to be of good air quality Most of thehospitals as shown in Table 7 were under intermediatedegree of air pollution as the bacterial load present in thosehospitals was in the range of 100ndash500 cfum3 According tothe work conducted by WHO experts total bacterial load
should not exceed 1000 cfum3 Similarly in this study allthe hospitals had bacterial load less than 1000 cfum3 in-dicating a satisfactory level of air quality
Out of 8 hospitals which can be seen in Table 2Staphylococuus aureus (4718) was isolated from 7 hos-pitals Among the two wards general ward showed a highoccurrence of S aureus (2885) than emergency ward(1833) S aureus a normal flora of the human body re-siding in the nasal passage is a leading pathogen causingnosocomial infection because of which among all the Gram-positive cocci isolated S aureus was the targeted Gram-positive organism of this study )e most common source ofS aureus is sneezing In a similar study done by Qudiesatet al [14] in selected hospitals of Zarqa city Jordan S aureus(162) was found to be the predominant organism
Other isolated and identified Gram-positive cocci in thisstudy were CoNS Streptococcus spp and Micrococcus sppOut of 8 hospitals they were isolated from 6 3 and 1hospitals respectively interpreted in Table 2 In a studycarried out by Sapkota et al [15] they screened out S aureus(571) followed byMicrococcus spp (26) CoNS (299)and Gram-negative bacteria from the air culture of gov-ernment hospitals of Nepal Streptococcus spp a causativeagent of severe pneumonia associated with nosocomial in-fection was isolated from 3 hospitals Bacillus spp was alsopredominantly isolated from 5 hospitals Common speciesof Bacillus exhibit a wide range of physiologic abilities thatallow them to live in every natural environment [8]
In this study Pseudomonas spp was isolated fromgeneral ward of only one hospital H1 (182) given withinTable 2 A contrast result was obtained in a study carried outby Nandalal and Somashekar [16] where the prevalence ofPseudomonas spp was found in almost all sites (38 cfum3))e occurrence of Pseudomonas spp in only H1 in our studymight be due to poor sanitation of hospital environment andmedical equipment )ere was a lack of regular risk as-sessment of water system of the hospital (H1) building dueto which we observed stagnant water in the hospitalrsquos toiletsand bathrooms Stagnant water is known as breeding groundfor Pseudomonas spp [17] and this could be a cause ofpersistence of this bacterium in this hospital Also presenceof patients infected with Pseudomonas spp within thesampling site might have led to occurrence of Pseudomonasspp in our study
E coli was isolated from both wards of one hospital andProteus spp was also isolated from only one hospital asshown in Figure 2 )e presence of members of Enter-obacteriaceae in this study might be due to the presence oftoilets in the same hall of emergency ward which led to thedirect contact of the patients with the organisms as these arethe intestinal microflora of our human body which even-tually led to the airborne condition of these organisms
As shown in Table 3 this study categorizes the hospitalson the basis of the crowd of people and traffic of vehicles asbusy and less busy We targeted hospitals located in areashaving high population density And then after surveyingtheir annual report on the patients flow we ranked hospitalson the basis of obtained data ultimately categorizing theminto busy and less busy In our study the busy hospitals had
0
1
2
3
4
5
6
7
General wardEmergency ward
Stap
hylo
cocc
us sp
p
CoN
S
E co
liPr
oteu
s spp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
Figure 2 Prevalence of bacteria in general and emergency wards ofdifferent hospitals
International Journal of Microbiology 5
an annual patientrsquos flow ranging from around 13000 up to 400000 and the less busy hospitals had an annual patientsflow from around 4000 up to 7000)erefore busy hospitalsare those hospitals located in highly crowded location interms of people and vehicles Another classification pre-sented in Table 3 of the hospitals was done on the basis ofGovernment private and semiprivate organizationsAmong the hospitals located in busy area H5 a privatehospital showed a high prevalence of Saurues whereas H4being a semiprivate hospital showed a presence of Micro-coccus spp Similarly among the hospitals located in lessbusy area H2 a government hospital had high prevalence ofS aureus and Pseudomonas spp was isolated only from H1which is also a government hospital located in less busy area
)e dampness situation of the building might have cre-ated favorable condition for the bacterial growth which canbe dispersed through droplets and then maintained in aerialsuspension which can have health risk among people )erelative humidity of the air has shown to be of major im-portance in the survival ofmicroorganisms)emechanism istotally related to organismrsquos surface biochemistry One
mechanism that explains the loss of viability in associationwith very low relative humidity is structural change in thelipid bilayer of the cell membrane as the water is lost from thecell Cell membrane bilayer changes from the typical crys-talline structures to the gel phase )is structural phasetransition affects cell surface protein configuration and ulti-mately results in inactivation of the cell In general Gram-negative bacteria react unfavorably to the desiccation whereasGram-positive bacteria are more tolerant to desiccation [18])is can be possible reasoning for more prevalence of Gram-positive bacteria Hence the most important means foravoiding adverse health effects is minimization of persistentdampness and microbial growth on interior surfaces and inbuilding structures And also it was stated by the WHO thatdampness situation has to be considered as the risk indicatorfor health risk of biological contaminants of indoor air [5]
F test was applied to study the difference in air qualitybetween the wards of every hospital and between hospitals Byusing the formula mentioned in (1) Fcal and Ftab were cal-culated Since Fcal (092 00131) is less than Ftab (5991 379)the null hypothesis H0 is accepted )e statistical analysisshowed that there is no significant difference in the con-centrations of bacteria between general and emergency wards)is explains that both the wards of all the eight differenthospitals which were studied had a similar bacterial loadstatistically Similarly there are no significant differences inthe concentrations of bacteria between the hospitals
In this study gentamicin and ofloxacin were found to be8181 effective towards isolates of S aureus as shown inTable 8 Hence it can be used as drug of choice for the
Table 3 Prevalence of S aureus and Pseudomonas spp in context with the condition and type of the organization
S N Condition Organization HospitalsNumber of organisms
S aureus Pseudomonas spp
1 Busy
Government mdash mdash mdash
Private H5 39 NilH6 20 Nil
Semiprivate H4 29 Nil
2 Less busy
Government H1 19 6H2 53 Nil
Private H7 6 NilH8 5 Nil
Semiprivate H3 Nil Nil
Table 4 Distribution of bacterial load in different wards of different hospitals
S N HospitalsNumber of colonies (observed) Number of colonies (calculated)
(cfum3) TotalEmergency ward General ward Emergency ward General ward
1 H1 43 52 96 116 2122 H2 75 57 172 128 3003 H3 59 11 132 26 1584 H4 88 63 206 142 3485 H5 49 37 110 82 1926 H6 48 51 108 114 2227 H7 12 12 28 30 588 H8 42 46 44 102 146Total 414 (5572) 329 (442)
Table 5 Standards for air quality evaluation according to EuropeanUnion Guidelines to Good Manufacturing Practice (EuropeanCommission 2008) [12]
S N Grade Cfum3 Cfuplate1 A lt1 lt12 B 10 53 C 100 504 D 200 100
6 International Journal of Microbiology
treatment of nosocomial infections caused by SaureusIsolated S aureus was found to be less susceptible toerythromycin (3636) and chloramphenicol (3636)
Asia is one of the epicenters of antimicrobial resistanceworldwide and this is an increasing public health concernMDR pathogens have been widely disseminated both inhospitals and throughout communities in many countries[19] )e relative frequency of P aeruginosa as a nosocomialpathogen has increased although wide variations are seenamong individual medical centers Pseudomonas aeruginosacontinues to be a major pathogen among patients with im-munosuppressant cystic fibrosis malignancy and trauma[20] Despite the high prevalence of MDR or XDR Pseudo-monas in Asia the clinical consequences of antimicrobialresistance are not fully understood in many Asian countriesIn a Korean hospital antimicrobial resistance especially toceftazidime and imipenem adversely affected the outcomes ofpatients with Pseudomonas aeruginosa bacteraemia Rates ofcarbapenem-resistant Pseudomonas were very high andMDRnonfermenters were highly prevalent in Asian countries[20] In this study (Table 9) Pseudomonas spp was highlysusceptible to ceftriaxone (833) and ofloxacin (833) Andit was resistant to imipenem It might be because of themutation of genes Due to the higher sensitivity towardsceftriaxone and ofloxacin it can be used as a drug of choice forthe treatment of nosocomial infections caused by this bac-terium (Tables 10 and 11)
6 Conclusion
From the 8 hospital samples processed in this study 245isolates of 8 different bacterial species were obtained Bothof the wards (general and emergency) of all the eighthospitals were found to be under C- and D-grade of airquality According to Sanitary Standard for Non-IndustrialPremises European Commission the majority of generalwards of 5 hospitals were found to be intermediatelypolluted and similar results were found in the case ofemergency wards of 5 hospitals High bacterial load wasfound to be present in H4 (348 cfum3) which is a semi-private hospital located in busy area And low bacterial loadwas found in H7 (58 cfum3) which is a private hospitallocated in less busy area Staphylococcus aureus (4718)was one of the major organisms isolated from 7 out of 8hospitals Pseudomonas spp (182) was isolated from
Table 6 Evaluation of air quality according to the sanitary standards for nonindustrial premises (CEC 1993) [13]
S N Group of microbes Range values (Cfum3) Air pollution degree1 Bacteria lt50 Very low2 Bacteria 50ndash100 Low3 Bacteria 100ndash500 Intermediate4 Bacteria 500ndash2000 High5 Bacteria gt2000 Very high
Table 7 Air pollution degree according to Sanitary Standards For Non-Industrial Premises European Commission
S N Hospitals Number of colonies in general ward(calculated)
Air pollution(degree)
Number of colonies in emergency ward(calculated)
Air pollution(degree)
1 H1 96 Low 116 Intermediate2 H2 172 Intermediate 128 Intermediate3 H3 132 Intermediate 26 Very low4 H4 206 Intermediate 142 Intermediate5 H5 110 Intermediate 82 Low6 H6 108 Intermediate 114 Intermediate7 H7 28 Very low 30 Very low8 H8 44 Very low 102 IntermediateTotal 896 740
Table 8 Antibiotic susceptibility pattern of Staphylococcus aureus
Antibiotics usedSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Gentamicin 9 8181 1 625 1 625 11Cotrimoxazole 5 4545 2 1818 4 3636 11Ampicillin 6 5454 3 2727 2 1818 11Erythromycin 4 3636 5 4545 2 1818 11Ofloxacin 9 8181 0 0 2 1818 11Chloramphenicol 4 3636 3 2727 4 3636 11
Table 9 Antibiotic susceptibility pattern of Pseudomonas spp
AntibioticsSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Amoxycillin 4 6667 2 333 0 0 6Ceftriaxone 5 833 1 166 0 0 6Cefotaxime 1 166 2 333 3 50 6Imipenem 0 0 0 0 6 100 6Ofloxacin 5 833 1 166 0 0 6
International Journal of Microbiology 7
general ward of only one hospital Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcusspp in 3 hospitals whereas Micrococcus spp was isolatedfrom only 1 hospital and Bacillus spp was isolated from 7hospitals (Figure 1) Out of 8 hospitals Ecoli was isolatedfrom 2 hospitals and Proteus spp was isolated from only 1hospital While performing the antibiotic susceptibility testfor S aureus it was found to be highly susceptible togentamicin (8181) and ofloxacin (8181) whereas it wasless susceptible to erythromycin (3636) and chloram-phenicol (3636) Similarly in the case of AST of Pseu-domonas spp it was found to be susceptible to ceftriaxone(833) and ofloxacin (833) whereas Pseudomonas sppdid not show susceptibility against imipenem )e highbacterial concentrations of air obtained in this study mightbe potential risk factors for spread of nosocomial infectionin respective hospitals
Data Availability
Further data related to this study can be made available uponrequest
Conflicts of Interest
)e authors declare that they have no conflicts of interest
Acknowledgments
It is with immense gratitude that we acknowledge ourrespected supervisor Mrs Pramila Parajuli LecturerDepartment of Microbiology St Xavierrsquos College Mai-tighar for her continuous support patience constructivesuggestion and expert guidance throughout the researchwork We are indebted to Mr Sudhakar Pant HODDepartment of Microbiology St Xavierrsquos College forproviding us opportunity to designate this project Weowe a deepest gratitude to all the respected lecturers forsharing their knowledge regarding this project and lab
staff members MrGopi Neupane and Mrs Anju LamaDepartment of Microbiology St Xavierrsquos College fortheir kind support Also we consider it an honour to workwith the administration staff members and nursing in-charge of the hospitals and thank them for their co-operation and generous technical support during theresearch work Along with our project group members weshare the credit of our work with all our acquaintance thathelped us in the course of conducting the research workFinally it gives us great pleasure in acknowledging thesupport and help of our family for their blessings con-tinuous motivation encouragement and unambiguoussupport throughout as always which brought us this farWe were a group of four members involved in this re-search and each individual had a share of Nrs 7000 witha total cost of Nrs 28000
References
[1] P Srikanth S Sudharsanam and R andSteinberg ldquoBio-aerosols in indoor environment composition health effectsand analysisrdquo Indian Journal of Medical Microbiology vol 26no 4 pp 302ndash312 2008
[2] R M Klevens J R Edwards C L Richards et al ldquoEstimatinghealth care-associated infections and deaths in US hospitalsrdquoPublic Health Reports vol 122 no 2 pp 160ndash166 2007
[3] B Ozer B C O Akkurt N Duran Y Onlen L Savas andS Turhanoglu ldquoEvaluation of nosocomial infections and riskfactors in critically ill patientsrdquo Medical Science Monitorvol 17 no 3 pp PH17ndashPH22 2011
[4] Isolation and Identification of Air Microflora in MicrobiologyLaboratoryosun State Polytechnic researchCluecom IreeNigeria 2015 httpsnairaprojectcomprojects1465html
[5] S F Hayleeyesus and A M Manaye ldquoMicrobiological qualityof indoor air in university librariesrdquo Asian Pacific Journal ofTropical Biomedicine vol 4 no 1 pp S312ndashS317 2014
[6] M J Mendell A G Mirer K Cheung et al ldquoHealth effectsassociated with dampness and mouldrdquo inWho Guidelines forIndoor Air Quality Dampness and Mould WHO RegionalOffice for Europe Copenhangen Denmark 2009 httpswwwncbinlmnihgovbooksNBK143940
[7] R Lawley ldquoSomething in the air monitoring airborne microor-ganismsrdquo Food Engineering and Ingredients pp 6ndash10 2009
[8] Clinical and Laboratory Standards Institute (CLSI) Antimi-crobial Susceptibility Testing Standards 2015
[9] A B Sthapit R P Yadav S P Khanal and P M DongolApplied Statistics Analysis of Variance-ANOVA AsmitaBooks Publishers amp Distributors (P) Ltd Kathmandu Nepal2014
[10] A A Anderson ldquoNew sampler for the collection sizing andenumeration of viable air borne particlesrdquo Journal of Bacte-riology vol 76 pp 471ndash484 1958
Table 10 Zone of size standard interpretative chart (HiMedia Catalogue 2017-18) Staphylococcus spp [21]
Antimicrobial agent Symbol Disc content Resistant (mm or less) Intermediate (mm) Sensitive (mm or more)Ampicillin AMP 10 μg 28 mdash 29Chloramphenicol C 30 μg 12 13ndash17 18Cotrimoxazole COT 25 μg 10 11ndash15 16Erythromycin E 15 μg 13 14ndash22 23Gentamicin GEN 10 μg 12 13ndash14 15Ofloxacin OF 5 μg 14 15ndash17 18
Table 11 Zone of size standard interpretative chart (HiMediaCatalogue 2017-18) Pseudomonas spp [21]
Antibiotics Sensitive Intermediate ResistantAmoxycillin 17 14ndash16 13Ceftriaxone 21 14ndash20 13Cefotaxime 23 15ndash22 14Imipenem 16 14-15 13Ofloxacin 16 13ndash15 12
8 International Journal of Microbiology
[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

was carried out From Table 4 we can observe that amongthe two wards emergency ward was found to have highbacterial load (5572) in comparison to general ward(442) A contrast result was obtained in a study conductedby Awosika et al [11] where out of nine wards the highbacterial load was found to be in medical ward (25)whereas the least bacterial load was recorded in emergencyunit (2) Humid room environment presence of un-hygienic attached toilets poor waste management systemand high number of patients in a single room personnel andvisitors occupying the hospital might be the reasons for highbacterial load in emergency ward in this study
According to the European Union Guidelines to GoodManufacturing Practices (Table 5) indoor air possessinggreater than 100 cfum3 and 200 cfum3 bacterial loads isreferred to as C- and D-grade air quality respectively In ourstudy Table 1 demonstrates that all the general wards andemergency wards of 8 hospitals were under C- and D-gradeair quality)is might be because at the time of this study allwards were at their maximum capacity as of visitors in andout the wards the high density of patients in the wardswhich resulted in more shedding of bacteria and agitation ofair Besides the environmental factors led to poor indoor airquality
Among all the 8 hospitals studied general ward of H7and H8 and emergency ward of H3 and H7 compara-tively showed a good air quality According to SanitaryStandards for NonIndustrial Premises European Com-mission (Table 6) indoor air having bacterial load lt50 cfum3 is considered to be of good air quality Most of thehospitals as shown in Table 7 were under intermediatedegree of air pollution as the bacterial load present in thosehospitals was in the range of 100ndash500 cfum3 According tothe work conducted by WHO experts total bacterial load
should not exceed 1000 cfum3 Similarly in this study allthe hospitals had bacterial load less than 1000 cfum3 in-dicating a satisfactory level of air quality
Out of 8 hospitals which can be seen in Table 2Staphylococuus aureus (4718) was isolated from 7 hos-pitals Among the two wards general ward showed a highoccurrence of S aureus (2885) than emergency ward(1833) S aureus a normal flora of the human body re-siding in the nasal passage is a leading pathogen causingnosocomial infection because of which among all the Gram-positive cocci isolated S aureus was the targeted Gram-positive organism of this study )e most common source ofS aureus is sneezing In a similar study done by Qudiesatet al [14] in selected hospitals of Zarqa city Jordan S aureus(162) was found to be the predominant organism
Other isolated and identified Gram-positive cocci in thisstudy were CoNS Streptococcus spp and Micrococcus sppOut of 8 hospitals they were isolated from 6 3 and 1hospitals respectively interpreted in Table 2 In a studycarried out by Sapkota et al [15] they screened out S aureus(571) followed byMicrococcus spp (26) CoNS (299)and Gram-negative bacteria from the air culture of gov-ernment hospitals of Nepal Streptococcus spp a causativeagent of severe pneumonia associated with nosocomial in-fection was isolated from 3 hospitals Bacillus spp was alsopredominantly isolated from 5 hospitals Common speciesof Bacillus exhibit a wide range of physiologic abilities thatallow them to live in every natural environment [8]
In this study Pseudomonas spp was isolated fromgeneral ward of only one hospital H1 (182) given withinTable 2 A contrast result was obtained in a study carried outby Nandalal and Somashekar [16] where the prevalence ofPseudomonas spp was found in almost all sites (38 cfum3))e occurrence of Pseudomonas spp in only H1 in our studymight be due to poor sanitation of hospital environment andmedical equipment )ere was a lack of regular risk as-sessment of water system of the hospital (H1) building dueto which we observed stagnant water in the hospitalrsquos toiletsand bathrooms Stagnant water is known as breeding groundfor Pseudomonas spp [17] and this could be a cause ofpersistence of this bacterium in this hospital Also presenceof patients infected with Pseudomonas spp within thesampling site might have led to occurrence of Pseudomonasspp in our study
E coli was isolated from both wards of one hospital andProteus spp was also isolated from only one hospital asshown in Figure 2 )e presence of members of Enter-obacteriaceae in this study might be due to the presence oftoilets in the same hall of emergency ward which led to thedirect contact of the patients with the organisms as these arethe intestinal microflora of our human body which even-tually led to the airborne condition of these organisms
As shown in Table 3 this study categorizes the hospitalson the basis of the crowd of people and traffic of vehicles asbusy and less busy We targeted hospitals located in areashaving high population density And then after surveyingtheir annual report on the patients flow we ranked hospitalson the basis of obtained data ultimately categorizing theminto busy and less busy In our study the busy hospitals had
0
1
2
3
4
5
6
7
General wardEmergency ward
Stap
hylo
cocc
us sp
p
CoN
S
E co
liPr
oteu
s spp
Pseu
dom
onas
spp
Stre
ptoc
occu
s spp
Bacil
lus s
pp
Micr
ococ
cus s
pp
Figure 2 Prevalence of bacteria in general and emergency wards ofdifferent hospitals
International Journal of Microbiology 5
an annual patientrsquos flow ranging from around 13000 up to 400000 and the less busy hospitals had an annual patientsflow from around 4000 up to 7000)erefore busy hospitalsare those hospitals located in highly crowded location interms of people and vehicles Another classification pre-sented in Table 3 of the hospitals was done on the basis ofGovernment private and semiprivate organizationsAmong the hospitals located in busy area H5 a privatehospital showed a high prevalence of Saurues whereas H4being a semiprivate hospital showed a presence of Micro-coccus spp Similarly among the hospitals located in lessbusy area H2 a government hospital had high prevalence ofS aureus and Pseudomonas spp was isolated only from H1which is also a government hospital located in less busy area
)e dampness situation of the building might have cre-ated favorable condition for the bacterial growth which canbe dispersed through droplets and then maintained in aerialsuspension which can have health risk among people )erelative humidity of the air has shown to be of major im-portance in the survival ofmicroorganisms)emechanism istotally related to organismrsquos surface biochemistry One
mechanism that explains the loss of viability in associationwith very low relative humidity is structural change in thelipid bilayer of the cell membrane as the water is lost from thecell Cell membrane bilayer changes from the typical crys-talline structures to the gel phase )is structural phasetransition affects cell surface protein configuration and ulti-mately results in inactivation of the cell In general Gram-negative bacteria react unfavorably to the desiccation whereasGram-positive bacteria are more tolerant to desiccation [18])is can be possible reasoning for more prevalence of Gram-positive bacteria Hence the most important means foravoiding adverse health effects is minimization of persistentdampness and microbial growth on interior surfaces and inbuilding structures And also it was stated by the WHO thatdampness situation has to be considered as the risk indicatorfor health risk of biological contaminants of indoor air [5]
F test was applied to study the difference in air qualitybetween the wards of every hospital and between hospitals Byusing the formula mentioned in (1) Fcal and Ftab were cal-culated Since Fcal (092 00131) is less than Ftab (5991 379)the null hypothesis H0 is accepted )e statistical analysisshowed that there is no significant difference in the con-centrations of bacteria between general and emergency wards)is explains that both the wards of all the eight differenthospitals which were studied had a similar bacterial loadstatistically Similarly there are no significant differences inthe concentrations of bacteria between the hospitals
In this study gentamicin and ofloxacin were found to be8181 effective towards isolates of S aureus as shown inTable 8 Hence it can be used as drug of choice for the
Table 3 Prevalence of S aureus and Pseudomonas spp in context with the condition and type of the organization
S N Condition Organization HospitalsNumber of organisms
S aureus Pseudomonas spp
1 Busy
Government mdash mdash mdash
Private H5 39 NilH6 20 Nil
Semiprivate H4 29 Nil
2 Less busy
Government H1 19 6H2 53 Nil
Private H7 6 NilH8 5 Nil
Semiprivate H3 Nil Nil
Table 4 Distribution of bacterial load in different wards of different hospitals
S N HospitalsNumber of colonies (observed) Number of colonies (calculated)
(cfum3) TotalEmergency ward General ward Emergency ward General ward
1 H1 43 52 96 116 2122 H2 75 57 172 128 3003 H3 59 11 132 26 1584 H4 88 63 206 142 3485 H5 49 37 110 82 1926 H6 48 51 108 114 2227 H7 12 12 28 30 588 H8 42 46 44 102 146Total 414 (5572) 329 (442)
Table 5 Standards for air quality evaluation according to EuropeanUnion Guidelines to Good Manufacturing Practice (EuropeanCommission 2008) [12]
S N Grade Cfum3 Cfuplate1 A lt1 lt12 B 10 53 C 100 504 D 200 100
6 International Journal of Microbiology
treatment of nosocomial infections caused by SaureusIsolated S aureus was found to be less susceptible toerythromycin (3636) and chloramphenicol (3636)
Asia is one of the epicenters of antimicrobial resistanceworldwide and this is an increasing public health concernMDR pathogens have been widely disseminated both inhospitals and throughout communities in many countries[19] )e relative frequency of P aeruginosa as a nosocomialpathogen has increased although wide variations are seenamong individual medical centers Pseudomonas aeruginosacontinues to be a major pathogen among patients with im-munosuppressant cystic fibrosis malignancy and trauma[20] Despite the high prevalence of MDR or XDR Pseudo-monas in Asia the clinical consequences of antimicrobialresistance are not fully understood in many Asian countriesIn a Korean hospital antimicrobial resistance especially toceftazidime and imipenem adversely affected the outcomes ofpatients with Pseudomonas aeruginosa bacteraemia Rates ofcarbapenem-resistant Pseudomonas were very high andMDRnonfermenters were highly prevalent in Asian countries[20] In this study (Table 9) Pseudomonas spp was highlysusceptible to ceftriaxone (833) and ofloxacin (833) Andit was resistant to imipenem It might be because of themutation of genes Due to the higher sensitivity towardsceftriaxone and ofloxacin it can be used as a drug of choice forthe treatment of nosocomial infections caused by this bac-terium (Tables 10 and 11)
6 Conclusion
From the 8 hospital samples processed in this study 245isolates of 8 different bacterial species were obtained Bothof the wards (general and emergency) of all the eighthospitals were found to be under C- and D-grade of airquality According to Sanitary Standard for Non-IndustrialPremises European Commission the majority of generalwards of 5 hospitals were found to be intermediatelypolluted and similar results were found in the case ofemergency wards of 5 hospitals High bacterial load wasfound to be present in H4 (348 cfum3) which is a semi-private hospital located in busy area And low bacterial loadwas found in H7 (58 cfum3) which is a private hospitallocated in less busy area Staphylococcus aureus (4718)was one of the major organisms isolated from 7 out of 8hospitals Pseudomonas spp (182) was isolated from
Table 6 Evaluation of air quality according to the sanitary standards for nonindustrial premises (CEC 1993) [13]
S N Group of microbes Range values (Cfum3) Air pollution degree1 Bacteria lt50 Very low2 Bacteria 50ndash100 Low3 Bacteria 100ndash500 Intermediate4 Bacteria 500ndash2000 High5 Bacteria gt2000 Very high
Table 7 Air pollution degree according to Sanitary Standards For Non-Industrial Premises European Commission
S N Hospitals Number of colonies in general ward(calculated)
Air pollution(degree)
Number of colonies in emergency ward(calculated)
Air pollution(degree)
1 H1 96 Low 116 Intermediate2 H2 172 Intermediate 128 Intermediate3 H3 132 Intermediate 26 Very low4 H4 206 Intermediate 142 Intermediate5 H5 110 Intermediate 82 Low6 H6 108 Intermediate 114 Intermediate7 H7 28 Very low 30 Very low8 H8 44 Very low 102 IntermediateTotal 896 740
Table 8 Antibiotic susceptibility pattern of Staphylococcus aureus
Antibiotics usedSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Gentamicin 9 8181 1 625 1 625 11Cotrimoxazole 5 4545 2 1818 4 3636 11Ampicillin 6 5454 3 2727 2 1818 11Erythromycin 4 3636 5 4545 2 1818 11Ofloxacin 9 8181 0 0 2 1818 11Chloramphenicol 4 3636 3 2727 4 3636 11
Table 9 Antibiotic susceptibility pattern of Pseudomonas spp
AntibioticsSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Amoxycillin 4 6667 2 333 0 0 6Ceftriaxone 5 833 1 166 0 0 6Cefotaxime 1 166 2 333 3 50 6Imipenem 0 0 0 0 6 100 6Ofloxacin 5 833 1 166 0 0 6
International Journal of Microbiology 7
general ward of only one hospital Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcusspp in 3 hospitals whereas Micrococcus spp was isolatedfrom only 1 hospital and Bacillus spp was isolated from 7hospitals (Figure 1) Out of 8 hospitals Ecoli was isolatedfrom 2 hospitals and Proteus spp was isolated from only 1hospital While performing the antibiotic susceptibility testfor S aureus it was found to be highly susceptible togentamicin (8181) and ofloxacin (8181) whereas it wasless susceptible to erythromycin (3636) and chloram-phenicol (3636) Similarly in the case of AST of Pseu-domonas spp it was found to be susceptible to ceftriaxone(833) and ofloxacin (833) whereas Pseudomonas sppdid not show susceptibility against imipenem )e highbacterial concentrations of air obtained in this study mightbe potential risk factors for spread of nosocomial infectionin respective hospitals
Data Availability
Further data related to this study can be made available uponrequest
Conflicts of Interest
)e authors declare that they have no conflicts of interest
Acknowledgments
It is with immense gratitude that we acknowledge ourrespected supervisor Mrs Pramila Parajuli LecturerDepartment of Microbiology St Xavierrsquos College Mai-tighar for her continuous support patience constructivesuggestion and expert guidance throughout the researchwork We are indebted to Mr Sudhakar Pant HODDepartment of Microbiology St Xavierrsquos College forproviding us opportunity to designate this project Weowe a deepest gratitude to all the respected lecturers forsharing their knowledge regarding this project and lab
staff members MrGopi Neupane and Mrs Anju LamaDepartment of Microbiology St Xavierrsquos College fortheir kind support Also we consider it an honour to workwith the administration staff members and nursing in-charge of the hospitals and thank them for their co-operation and generous technical support during theresearch work Along with our project group members weshare the credit of our work with all our acquaintance thathelped us in the course of conducting the research workFinally it gives us great pleasure in acknowledging thesupport and help of our family for their blessings con-tinuous motivation encouragement and unambiguoussupport throughout as always which brought us this farWe were a group of four members involved in this re-search and each individual had a share of Nrs 7000 witha total cost of Nrs 28000
References
[1] P Srikanth S Sudharsanam and R andSteinberg ldquoBio-aerosols in indoor environment composition health effectsand analysisrdquo Indian Journal of Medical Microbiology vol 26no 4 pp 302ndash312 2008
[2] R M Klevens J R Edwards C L Richards et al ldquoEstimatinghealth care-associated infections and deaths in US hospitalsrdquoPublic Health Reports vol 122 no 2 pp 160ndash166 2007
[3] B Ozer B C O Akkurt N Duran Y Onlen L Savas andS Turhanoglu ldquoEvaluation of nosocomial infections and riskfactors in critically ill patientsrdquo Medical Science Monitorvol 17 no 3 pp PH17ndashPH22 2011
[4] Isolation and Identification of Air Microflora in MicrobiologyLaboratoryosun State Polytechnic researchCluecom IreeNigeria 2015 httpsnairaprojectcomprojects1465html
[5] S F Hayleeyesus and A M Manaye ldquoMicrobiological qualityof indoor air in university librariesrdquo Asian Pacific Journal ofTropical Biomedicine vol 4 no 1 pp S312ndashS317 2014
[6] M J Mendell A G Mirer K Cheung et al ldquoHealth effectsassociated with dampness and mouldrdquo inWho Guidelines forIndoor Air Quality Dampness and Mould WHO RegionalOffice for Europe Copenhangen Denmark 2009 httpswwwncbinlmnihgovbooksNBK143940
[7] R Lawley ldquoSomething in the air monitoring airborne microor-ganismsrdquo Food Engineering and Ingredients pp 6ndash10 2009
[8] Clinical and Laboratory Standards Institute (CLSI) Antimi-crobial Susceptibility Testing Standards 2015
[9] A B Sthapit R P Yadav S P Khanal and P M DongolApplied Statistics Analysis of Variance-ANOVA AsmitaBooks Publishers amp Distributors (P) Ltd Kathmandu Nepal2014
[10] A A Anderson ldquoNew sampler for the collection sizing andenumeration of viable air borne particlesrdquo Journal of Bacte-riology vol 76 pp 471ndash484 1958
Table 10 Zone of size standard interpretative chart (HiMedia Catalogue 2017-18) Staphylococcus spp [21]
Antimicrobial agent Symbol Disc content Resistant (mm or less) Intermediate (mm) Sensitive (mm or more)Ampicillin AMP 10 μg 28 mdash 29Chloramphenicol C 30 μg 12 13ndash17 18Cotrimoxazole COT 25 μg 10 11ndash15 16Erythromycin E 15 μg 13 14ndash22 23Gentamicin GEN 10 μg 12 13ndash14 15Ofloxacin OF 5 μg 14 15ndash17 18
Table 11 Zone of size standard interpretative chart (HiMediaCatalogue 2017-18) Pseudomonas spp [21]
Antibiotics Sensitive Intermediate ResistantAmoxycillin 17 14ndash16 13Ceftriaxone 21 14ndash20 13Cefotaxime 23 15ndash22 14Imipenem 16 14-15 13Ofloxacin 16 13ndash15 12
8 International Journal of Microbiology
[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

an annual patientrsquos flow ranging from around 13000 up to 400000 and the less busy hospitals had an annual patientsflow from around 4000 up to 7000)erefore busy hospitalsare those hospitals located in highly crowded location interms of people and vehicles Another classification pre-sented in Table 3 of the hospitals was done on the basis ofGovernment private and semiprivate organizationsAmong the hospitals located in busy area H5 a privatehospital showed a high prevalence of Saurues whereas H4being a semiprivate hospital showed a presence of Micro-coccus spp Similarly among the hospitals located in lessbusy area H2 a government hospital had high prevalence ofS aureus and Pseudomonas spp was isolated only from H1which is also a government hospital located in less busy area
)e dampness situation of the building might have cre-ated favorable condition for the bacterial growth which canbe dispersed through droplets and then maintained in aerialsuspension which can have health risk among people )erelative humidity of the air has shown to be of major im-portance in the survival ofmicroorganisms)emechanism istotally related to organismrsquos surface biochemistry One
mechanism that explains the loss of viability in associationwith very low relative humidity is structural change in thelipid bilayer of the cell membrane as the water is lost from thecell Cell membrane bilayer changes from the typical crys-talline structures to the gel phase )is structural phasetransition affects cell surface protein configuration and ulti-mately results in inactivation of the cell In general Gram-negative bacteria react unfavorably to the desiccation whereasGram-positive bacteria are more tolerant to desiccation [18])is can be possible reasoning for more prevalence of Gram-positive bacteria Hence the most important means foravoiding adverse health effects is minimization of persistentdampness and microbial growth on interior surfaces and inbuilding structures And also it was stated by the WHO thatdampness situation has to be considered as the risk indicatorfor health risk of biological contaminants of indoor air [5]
F test was applied to study the difference in air qualitybetween the wards of every hospital and between hospitals Byusing the formula mentioned in (1) Fcal and Ftab were cal-culated Since Fcal (092 00131) is less than Ftab (5991 379)the null hypothesis H0 is accepted )e statistical analysisshowed that there is no significant difference in the con-centrations of bacteria between general and emergency wards)is explains that both the wards of all the eight differenthospitals which were studied had a similar bacterial loadstatistically Similarly there are no significant differences inthe concentrations of bacteria between the hospitals
In this study gentamicin and ofloxacin were found to be8181 effective towards isolates of S aureus as shown inTable 8 Hence it can be used as drug of choice for the
Table 3 Prevalence of S aureus and Pseudomonas spp in context with the condition and type of the organization
S N Condition Organization HospitalsNumber of organisms
S aureus Pseudomonas spp
1 Busy
Government mdash mdash mdash
Private H5 39 NilH6 20 Nil
Semiprivate H4 29 Nil
2 Less busy
Government H1 19 6H2 53 Nil
Private H7 6 NilH8 5 Nil
Semiprivate H3 Nil Nil
Table 4 Distribution of bacterial load in different wards of different hospitals
S N HospitalsNumber of colonies (observed) Number of colonies (calculated)
(cfum3) TotalEmergency ward General ward Emergency ward General ward
1 H1 43 52 96 116 2122 H2 75 57 172 128 3003 H3 59 11 132 26 1584 H4 88 63 206 142 3485 H5 49 37 110 82 1926 H6 48 51 108 114 2227 H7 12 12 28 30 588 H8 42 46 44 102 146Total 414 (5572) 329 (442)
Table 5 Standards for air quality evaluation according to EuropeanUnion Guidelines to Good Manufacturing Practice (EuropeanCommission 2008) [12]
S N Grade Cfum3 Cfuplate1 A lt1 lt12 B 10 53 C 100 504 D 200 100
6 International Journal of Microbiology
treatment of nosocomial infections caused by SaureusIsolated S aureus was found to be less susceptible toerythromycin (3636) and chloramphenicol (3636)
Asia is one of the epicenters of antimicrobial resistanceworldwide and this is an increasing public health concernMDR pathogens have been widely disseminated both inhospitals and throughout communities in many countries[19] )e relative frequency of P aeruginosa as a nosocomialpathogen has increased although wide variations are seenamong individual medical centers Pseudomonas aeruginosacontinues to be a major pathogen among patients with im-munosuppressant cystic fibrosis malignancy and trauma[20] Despite the high prevalence of MDR or XDR Pseudo-monas in Asia the clinical consequences of antimicrobialresistance are not fully understood in many Asian countriesIn a Korean hospital antimicrobial resistance especially toceftazidime and imipenem adversely affected the outcomes ofpatients with Pseudomonas aeruginosa bacteraemia Rates ofcarbapenem-resistant Pseudomonas were very high andMDRnonfermenters were highly prevalent in Asian countries[20] In this study (Table 9) Pseudomonas spp was highlysusceptible to ceftriaxone (833) and ofloxacin (833) Andit was resistant to imipenem It might be because of themutation of genes Due to the higher sensitivity towardsceftriaxone and ofloxacin it can be used as a drug of choice forthe treatment of nosocomial infections caused by this bac-terium (Tables 10 and 11)
6 Conclusion
From the 8 hospital samples processed in this study 245isolates of 8 different bacterial species were obtained Bothof the wards (general and emergency) of all the eighthospitals were found to be under C- and D-grade of airquality According to Sanitary Standard for Non-IndustrialPremises European Commission the majority of generalwards of 5 hospitals were found to be intermediatelypolluted and similar results were found in the case ofemergency wards of 5 hospitals High bacterial load wasfound to be present in H4 (348 cfum3) which is a semi-private hospital located in busy area And low bacterial loadwas found in H7 (58 cfum3) which is a private hospitallocated in less busy area Staphylococcus aureus (4718)was one of the major organisms isolated from 7 out of 8hospitals Pseudomonas spp (182) was isolated from
Table 6 Evaluation of air quality according to the sanitary standards for nonindustrial premises (CEC 1993) [13]
S N Group of microbes Range values (Cfum3) Air pollution degree1 Bacteria lt50 Very low2 Bacteria 50ndash100 Low3 Bacteria 100ndash500 Intermediate4 Bacteria 500ndash2000 High5 Bacteria gt2000 Very high
Table 7 Air pollution degree according to Sanitary Standards For Non-Industrial Premises European Commission
S N Hospitals Number of colonies in general ward(calculated)
Air pollution(degree)
Number of colonies in emergency ward(calculated)
Air pollution(degree)
1 H1 96 Low 116 Intermediate2 H2 172 Intermediate 128 Intermediate3 H3 132 Intermediate 26 Very low4 H4 206 Intermediate 142 Intermediate5 H5 110 Intermediate 82 Low6 H6 108 Intermediate 114 Intermediate7 H7 28 Very low 30 Very low8 H8 44 Very low 102 IntermediateTotal 896 740
Table 8 Antibiotic susceptibility pattern of Staphylococcus aureus
Antibiotics usedSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Gentamicin 9 8181 1 625 1 625 11Cotrimoxazole 5 4545 2 1818 4 3636 11Ampicillin 6 5454 3 2727 2 1818 11Erythromycin 4 3636 5 4545 2 1818 11Ofloxacin 9 8181 0 0 2 1818 11Chloramphenicol 4 3636 3 2727 4 3636 11
Table 9 Antibiotic susceptibility pattern of Pseudomonas spp
AntibioticsSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Amoxycillin 4 6667 2 333 0 0 6Ceftriaxone 5 833 1 166 0 0 6Cefotaxime 1 166 2 333 3 50 6Imipenem 0 0 0 0 6 100 6Ofloxacin 5 833 1 166 0 0 6
International Journal of Microbiology 7
general ward of only one hospital Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcusspp in 3 hospitals whereas Micrococcus spp was isolatedfrom only 1 hospital and Bacillus spp was isolated from 7hospitals (Figure 1) Out of 8 hospitals Ecoli was isolatedfrom 2 hospitals and Proteus spp was isolated from only 1hospital While performing the antibiotic susceptibility testfor S aureus it was found to be highly susceptible togentamicin (8181) and ofloxacin (8181) whereas it wasless susceptible to erythromycin (3636) and chloram-phenicol (3636) Similarly in the case of AST of Pseu-domonas spp it was found to be susceptible to ceftriaxone(833) and ofloxacin (833) whereas Pseudomonas sppdid not show susceptibility against imipenem )e highbacterial concentrations of air obtained in this study mightbe potential risk factors for spread of nosocomial infectionin respective hospitals
Data Availability
Further data related to this study can be made available uponrequest
Conflicts of Interest
)e authors declare that they have no conflicts of interest
Acknowledgments
It is with immense gratitude that we acknowledge ourrespected supervisor Mrs Pramila Parajuli LecturerDepartment of Microbiology St Xavierrsquos College Mai-tighar for her continuous support patience constructivesuggestion and expert guidance throughout the researchwork We are indebted to Mr Sudhakar Pant HODDepartment of Microbiology St Xavierrsquos College forproviding us opportunity to designate this project Weowe a deepest gratitude to all the respected lecturers forsharing their knowledge regarding this project and lab
staff members MrGopi Neupane and Mrs Anju LamaDepartment of Microbiology St Xavierrsquos College fortheir kind support Also we consider it an honour to workwith the administration staff members and nursing in-charge of the hospitals and thank them for their co-operation and generous technical support during theresearch work Along with our project group members weshare the credit of our work with all our acquaintance thathelped us in the course of conducting the research workFinally it gives us great pleasure in acknowledging thesupport and help of our family for their blessings con-tinuous motivation encouragement and unambiguoussupport throughout as always which brought us this farWe were a group of four members involved in this re-search and each individual had a share of Nrs 7000 witha total cost of Nrs 28000
References
[1] P Srikanth S Sudharsanam and R andSteinberg ldquoBio-aerosols in indoor environment composition health effectsand analysisrdquo Indian Journal of Medical Microbiology vol 26no 4 pp 302ndash312 2008
[2] R M Klevens J R Edwards C L Richards et al ldquoEstimatinghealth care-associated infections and deaths in US hospitalsrdquoPublic Health Reports vol 122 no 2 pp 160ndash166 2007
[3] B Ozer B C O Akkurt N Duran Y Onlen L Savas andS Turhanoglu ldquoEvaluation of nosocomial infections and riskfactors in critically ill patientsrdquo Medical Science Monitorvol 17 no 3 pp PH17ndashPH22 2011
[4] Isolation and Identification of Air Microflora in MicrobiologyLaboratoryosun State Polytechnic researchCluecom IreeNigeria 2015 httpsnairaprojectcomprojects1465html
[5] S F Hayleeyesus and A M Manaye ldquoMicrobiological qualityof indoor air in university librariesrdquo Asian Pacific Journal ofTropical Biomedicine vol 4 no 1 pp S312ndashS317 2014
[6] M J Mendell A G Mirer K Cheung et al ldquoHealth effectsassociated with dampness and mouldrdquo inWho Guidelines forIndoor Air Quality Dampness and Mould WHO RegionalOffice for Europe Copenhangen Denmark 2009 httpswwwncbinlmnihgovbooksNBK143940
[7] R Lawley ldquoSomething in the air monitoring airborne microor-ganismsrdquo Food Engineering and Ingredients pp 6ndash10 2009
[8] Clinical and Laboratory Standards Institute (CLSI) Antimi-crobial Susceptibility Testing Standards 2015
[9] A B Sthapit R P Yadav S P Khanal and P M DongolApplied Statistics Analysis of Variance-ANOVA AsmitaBooks Publishers amp Distributors (P) Ltd Kathmandu Nepal2014
[10] A A Anderson ldquoNew sampler for the collection sizing andenumeration of viable air borne particlesrdquo Journal of Bacte-riology vol 76 pp 471ndash484 1958
Table 10 Zone of size standard interpretative chart (HiMedia Catalogue 2017-18) Staphylococcus spp [21]
Antimicrobial agent Symbol Disc content Resistant (mm or less) Intermediate (mm) Sensitive (mm or more)Ampicillin AMP 10 μg 28 mdash 29Chloramphenicol C 30 μg 12 13ndash17 18Cotrimoxazole COT 25 μg 10 11ndash15 16Erythromycin E 15 μg 13 14ndash22 23Gentamicin GEN 10 μg 12 13ndash14 15Ofloxacin OF 5 μg 14 15ndash17 18
Table 11 Zone of size standard interpretative chart (HiMediaCatalogue 2017-18) Pseudomonas spp [21]
Antibiotics Sensitive Intermediate ResistantAmoxycillin 17 14ndash16 13Ceftriaxone 21 14ndash20 13Cefotaxime 23 15ndash22 14Imipenem 16 14-15 13Ofloxacin 16 13ndash15 12
8 International Journal of Microbiology
[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

treatment of nosocomial infections caused by SaureusIsolated S aureus was found to be less susceptible toerythromycin (3636) and chloramphenicol (3636)
Asia is one of the epicenters of antimicrobial resistanceworldwide and this is an increasing public health concernMDR pathogens have been widely disseminated both inhospitals and throughout communities in many countries[19] )e relative frequency of P aeruginosa as a nosocomialpathogen has increased although wide variations are seenamong individual medical centers Pseudomonas aeruginosacontinues to be a major pathogen among patients with im-munosuppressant cystic fibrosis malignancy and trauma[20] Despite the high prevalence of MDR or XDR Pseudo-monas in Asia the clinical consequences of antimicrobialresistance are not fully understood in many Asian countriesIn a Korean hospital antimicrobial resistance especially toceftazidime and imipenem adversely affected the outcomes ofpatients with Pseudomonas aeruginosa bacteraemia Rates ofcarbapenem-resistant Pseudomonas were very high andMDRnonfermenters were highly prevalent in Asian countries[20] In this study (Table 9) Pseudomonas spp was highlysusceptible to ceftriaxone (833) and ofloxacin (833) Andit was resistant to imipenem It might be because of themutation of genes Due to the higher sensitivity towardsceftriaxone and ofloxacin it can be used as a drug of choice forthe treatment of nosocomial infections caused by this bac-terium (Tables 10 and 11)
6 Conclusion
From the 8 hospital samples processed in this study 245isolates of 8 different bacterial species were obtained Bothof the wards (general and emergency) of all the eighthospitals were found to be under C- and D-grade of airquality According to Sanitary Standard for Non-IndustrialPremises European Commission the majority of generalwards of 5 hospitals were found to be intermediatelypolluted and similar results were found in the case ofemergency wards of 5 hospitals High bacterial load wasfound to be present in H4 (348 cfum3) which is a semi-private hospital located in busy area And low bacterial loadwas found in H7 (58 cfum3) which is a private hospitallocated in less busy area Staphylococcus aureus (4718)was one of the major organisms isolated from 7 out of 8hospitals Pseudomonas spp (182) was isolated from
Table 6 Evaluation of air quality according to the sanitary standards for nonindustrial premises (CEC 1993) [13]
S N Group of microbes Range values (Cfum3) Air pollution degree1 Bacteria lt50 Very low2 Bacteria 50ndash100 Low3 Bacteria 100ndash500 Intermediate4 Bacteria 500ndash2000 High5 Bacteria gt2000 Very high
Table 7 Air pollution degree according to Sanitary Standards For Non-Industrial Premises European Commission
S N Hospitals Number of colonies in general ward(calculated)
Air pollution(degree)
Number of colonies in emergency ward(calculated)
Air pollution(degree)
1 H1 96 Low 116 Intermediate2 H2 172 Intermediate 128 Intermediate3 H3 132 Intermediate 26 Very low4 H4 206 Intermediate 142 Intermediate5 H5 110 Intermediate 82 Low6 H6 108 Intermediate 114 Intermediate7 H7 28 Very low 30 Very low8 H8 44 Very low 102 IntermediateTotal 896 740
Table 8 Antibiotic susceptibility pattern of Staphylococcus aureus
Antibiotics usedSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Gentamicin 9 8181 1 625 1 625 11Cotrimoxazole 5 4545 2 1818 4 3636 11Ampicillin 6 5454 3 2727 2 1818 11Erythromycin 4 3636 5 4545 2 1818 11Ofloxacin 9 8181 0 0 2 1818 11Chloramphenicol 4 3636 3 2727 4 3636 11
Table 9 Antibiotic susceptibility pattern of Pseudomonas spp
AntibioticsSensitive Intermediate Resistant
TotalNumber () Number () Number ()
Amoxycillin 4 6667 2 333 0 0 6Ceftriaxone 5 833 1 166 0 0 6Cefotaxime 1 166 2 333 3 50 6Imipenem 0 0 0 0 6 100 6Ofloxacin 5 833 1 166 0 0 6
International Journal of Microbiology 7
general ward of only one hospital Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcusspp in 3 hospitals whereas Micrococcus spp was isolatedfrom only 1 hospital and Bacillus spp was isolated from 7hospitals (Figure 1) Out of 8 hospitals Ecoli was isolatedfrom 2 hospitals and Proteus spp was isolated from only 1hospital While performing the antibiotic susceptibility testfor S aureus it was found to be highly susceptible togentamicin (8181) and ofloxacin (8181) whereas it wasless susceptible to erythromycin (3636) and chloram-phenicol (3636) Similarly in the case of AST of Pseu-domonas spp it was found to be susceptible to ceftriaxone(833) and ofloxacin (833) whereas Pseudomonas sppdid not show susceptibility against imipenem )e highbacterial concentrations of air obtained in this study mightbe potential risk factors for spread of nosocomial infectionin respective hospitals
Data Availability
Further data related to this study can be made available uponrequest
Conflicts of Interest
)e authors declare that they have no conflicts of interest
Acknowledgments
It is with immense gratitude that we acknowledge ourrespected supervisor Mrs Pramila Parajuli LecturerDepartment of Microbiology St Xavierrsquos College Mai-tighar for her continuous support patience constructivesuggestion and expert guidance throughout the researchwork We are indebted to Mr Sudhakar Pant HODDepartment of Microbiology St Xavierrsquos College forproviding us opportunity to designate this project Weowe a deepest gratitude to all the respected lecturers forsharing their knowledge regarding this project and lab
staff members MrGopi Neupane and Mrs Anju LamaDepartment of Microbiology St Xavierrsquos College fortheir kind support Also we consider it an honour to workwith the administration staff members and nursing in-charge of the hospitals and thank them for their co-operation and generous technical support during theresearch work Along with our project group members weshare the credit of our work with all our acquaintance thathelped us in the course of conducting the research workFinally it gives us great pleasure in acknowledging thesupport and help of our family for their blessings con-tinuous motivation encouragement and unambiguoussupport throughout as always which brought us this farWe were a group of four members involved in this re-search and each individual had a share of Nrs 7000 witha total cost of Nrs 28000
References
[1] P Srikanth S Sudharsanam and R andSteinberg ldquoBio-aerosols in indoor environment composition health effectsand analysisrdquo Indian Journal of Medical Microbiology vol 26no 4 pp 302ndash312 2008
[2] R M Klevens J R Edwards C L Richards et al ldquoEstimatinghealth care-associated infections and deaths in US hospitalsrdquoPublic Health Reports vol 122 no 2 pp 160ndash166 2007
[3] B Ozer B C O Akkurt N Duran Y Onlen L Savas andS Turhanoglu ldquoEvaluation of nosocomial infections and riskfactors in critically ill patientsrdquo Medical Science Monitorvol 17 no 3 pp PH17ndashPH22 2011
[4] Isolation and Identification of Air Microflora in MicrobiologyLaboratoryosun State Polytechnic researchCluecom IreeNigeria 2015 httpsnairaprojectcomprojects1465html
[5] S F Hayleeyesus and A M Manaye ldquoMicrobiological qualityof indoor air in university librariesrdquo Asian Pacific Journal ofTropical Biomedicine vol 4 no 1 pp S312ndashS317 2014
[6] M J Mendell A G Mirer K Cheung et al ldquoHealth effectsassociated with dampness and mouldrdquo inWho Guidelines forIndoor Air Quality Dampness and Mould WHO RegionalOffice for Europe Copenhangen Denmark 2009 httpswwwncbinlmnihgovbooksNBK143940
[7] R Lawley ldquoSomething in the air monitoring airborne microor-ganismsrdquo Food Engineering and Ingredients pp 6ndash10 2009
[8] Clinical and Laboratory Standards Institute (CLSI) Antimi-crobial Susceptibility Testing Standards 2015
[9] A B Sthapit R P Yadav S P Khanal and P M DongolApplied Statistics Analysis of Variance-ANOVA AsmitaBooks Publishers amp Distributors (P) Ltd Kathmandu Nepal2014
[10] A A Anderson ldquoNew sampler for the collection sizing andenumeration of viable air borne particlesrdquo Journal of Bacte-riology vol 76 pp 471ndash484 1958
Table 10 Zone of size standard interpretative chart (HiMedia Catalogue 2017-18) Staphylococcus spp [21]
Antimicrobial agent Symbol Disc content Resistant (mm or less) Intermediate (mm) Sensitive (mm or more)Ampicillin AMP 10 μg 28 mdash 29Chloramphenicol C 30 μg 12 13ndash17 18Cotrimoxazole COT 25 μg 10 11ndash15 16Erythromycin E 15 μg 13 14ndash22 23Gentamicin GEN 10 μg 12 13ndash14 15Ofloxacin OF 5 μg 14 15ndash17 18
Table 11 Zone of size standard interpretative chart (HiMediaCatalogue 2017-18) Pseudomonas spp [21]
Antibiotics Sensitive Intermediate ResistantAmoxycillin 17 14ndash16 13Ceftriaxone 21 14ndash20 13Cefotaxime 23 15ndash22 14Imipenem 16 14-15 13Ofloxacin 16 13ndash15 12
8 International Journal of Microbiology
[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

general ward of only one hospital Out of 8 hospitals CoNSwas isolated from 6 hospitals followed by Streptococcusspp in 3 hospitals whereas Micrococcus spp was isolatedfrom only 1 hospital and Bacillus spp was isolated from 7hospitals (Figure 1) Out of 8 hospitals Ecoli was isolatedfrom 2 hospitals and Proteus spp was isolated from only 1hospital While performing the antibiotic susceptibility testfor S aureus it was found to be highly susceptible togentamicin (8181) and ofloxacin (8181) whereas it wasless susceptible to erythromycin (3636) and chloram-phenicol (3636) Similarly in the case of AST of Pseu-domonas spp it was found to be susceptible to ceftriaxone(833) and ofloxacin (833) whereas Pseudomonas sppdid not show susceptibility against imipenem )e highbacterial concentrations of air obtained in this study mightbe potential risk factors for spread of nosocomial infectionin respective hospitals
Data Availability
Further data related to this study can be made available uponrequest
Conflicts of Interest
)e authors declare that they have no conflicts of interest
Acknowledgments
It is with immense gratitude that we acknowledge ourrespected supervisor Mrs Pramila Parajuli LecturerDepartment of Microbiology St Xavierrsquos College Mai-tighar for her continuous support patience constructivesuggestion and expert guidance throughout the researchwork We are indebted to Mr Sudhakar Pant HODDepartment of Microbiology St Xavierrsquos College forproviding us opportunity to designate this project Weowe a deepest gratitude to all the respected lecturers forsharing their knowledge regarding this project and lab
staff members MrGopi Neupane and Mrs Anju LamaDepartment of Microbiology St Xavierrsquos College fortheir kind support Also we consider it an honour to workwith the administration staff members and nursing in-charge of the hospitals and thank them for their co-operation and generous technical support during theresearch work Along with our project group members weshare the credit of our work with all our acquaintance thathelped us in the course of conducting the research workFinally it gives us great pleasure in acknowledging thesupport and help of our family for their blessings con-tinuous motivation encouragement and unambiguoussupport throughout as always which brought us this farWe were a group of four members involved in this re-search and each individual had a share of Nrs 7000 witha total cost of Nrs 28000
References
[1] P Srikanth S Sudharsanam and R andSteinberg ldquoBio-aerosols in indoor environment composition health effectsand analysisrdquo Indian Journal of Medical Microbiology vol 26no 4 pp 302ndash312 2008
[2] R M Klevens J R Edwards C L Richards et al ldquoEstimatinghealth care-associated infections and deaths in US hospitalsrdquoPublic Health Reports vol 122 no 2 pp 160ndash166 2007
[3] B Ozer B C O Akkurt N Duran Y Onlen L Savas andS Turhanoglu ldquoEvaluation of nosocomial infections and riskfactors in critically ill patientsrdquo Medical Science Monitorvol 17 no 3 pp PH17ndashPH22 2011
[4] Isolation and Identification of Air Microflora in MicrobiologyLaboratoryosun State Polytechnic researchCluecom IreeNigeria 2015 httpsnairaprojectcomprojects1465html
[5] S F Hayleeyesus and A M Manaye ldquoMicrobiological qualityof indoor air in university librariesrdquo Asian Pacific Journal ofTropical Biomedicine vol 4 no 1 pp S312ndashS317 2014
[6] M J Mendell A G Mirer K Cheung et al ldquoHealth effectsassociated with dampness and mouldrdquo inWho Guidelines forIndoor Air Quality Dampness and Mould WHO RegionalOffice for Europe Copenhangen Denmark 2009 httpswwwncbinlmnihgovbooksNBK143940
[7] R Lawley ldquoSomething in the air monitoring airborne microor-ganismsrdquo Food Engineering and Ingredients pp 6ndash10 2009
[8] Clinical and Laboratory Standards Institute (CLSI) Antimi-crobial Susceptibility Testing Standards 2015
[9] A B Sthapit R P Yadav S P Khanal and P M DongolApplied Statistics Analysis of Variance-ANOVA AsmitaBooks Publishers amp Distributors (P) Ltd Kathmandu Nepal2014
[10] A A Anderson ldquoNew sampler for the collection sizing andenumeration of viable air borne particlesrdquo Journal of Bacte-riology vol 76 pp 471ndash484 1958
Table 10 Zone of size standard interpretative chart (HiMedia Catalogue 2017-18) Staphylococcus spp [21]
Antimicrobial agent Symbol Disc content Resistant (mm or less) Intermediate (mm) Sensitive (mm or more)Ampicillin AMP 10 μg 28 mdash 29Chloramphenicol C 30 μg 12 13ndash17 18Cotrimoxazole COT 25 μg 10 11ndash15 16Erythromycin E 15 μg 13 14ndash22 23Gentamicin GEN 10 μg 12 13ndash14 15Ofloxacin OF 5 μg 14 15ndash17 18
Table 11 Zone of size standard interpretative chart (HiMediaCatalogue 2017-18) Pseudomonas spp [21]
Antibiotics Sensitive Intermediate ResistantAmoxycillin 17 14ndash16 13Ceftriaxone 21 14ndash20 13Cefotaxime 23 15ndash22 14Imipenem 16 14-15 13Ofloxacin 16 13ndash15 12
8 International Journal of Microbiology
[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

[11] S A Awosika F A Olajubu and N A Amusa ldquoMicrobi-ological assessment of indoor air of a teaching hospital inNigeriardquo Asian Pacific Journal of Tropical Biomedicine vol 2no 6 pp 465ndash468 2012
[12] European Commission Enterprise and Industry DirectorateGeneral Volume 4 EU Guidelines to Good ManufacturingPractice European Commission Enterprise and IndustryDirectorate Brussels Belgium 2008
[13] CEC Commission of the European Communities ldquoIndoor airquality and its impact on manrdquo Report no 12 BiologicalParticles in Indoor Environments Commission of the Eu-ropean Communities Brussels Belgium 1993
[14] K Qudiesat K Abu-Elteen A Elkarmi M Hamad andM Abusasaud ldquoAssessment of airborne pathogens inhealthcare settingsrdquo African Journal of Microbiology Researchvol 3 no 2 pp 066ndash076 2009
[15] B Sapkota G K Gupta S K Shrestha A Pradhan P Karkiand A )apa ldquoMicrobiological burden in air culture atvarious units of a tertiary care government hospital in NepalrdquoAustralasian Medical Journal vol 9 no 1 pp 1ndash7 2016
[16] P Nandalal and R K Somashekhar ldquoPrevalence of Staphy-lococcus aureus and Pseudomonas aeruginosa in indoor airflora of a district hospital Mandya Karnatakardquo Journal OfEnvironmental Biology vol 28 no 2 pp 197ndash200 2007
[17] Special Report Pseudomonas in Hospitals httpswwwbuildingbetterhealthcarecouknewsarticle_pageSpecial_report_Pseudomonas_in_hospitals75712
[18] I L Pepper and S E Dowd Aero Microbiology-Environmental Microbiology Elsevier Inc AmsterdamNetherlands 2009
[19] A Cross J R Allen J Burke et al ldquoNosocomial infectionsdue to pseudomonas aeruginosa review of recent trendsrdquoClinical Infectious Diseases vol 5 no 5 pp S837ndashS845 1983
[20] C I Kang and J H Song ldquoAntimicrobial resistance in Asiacurrent epidemiological and clinical implicationsrdquo Infectionamp Chemotherapy vol 45 no 1 pp 22ndash31 2013
[21] HiMedia Catalogue Antimicrobial TestingndashZone Size In-terpretative Chart 237ndash294 HiMedia Laboratories Mum-bai India 2017 httphimedialabscomcatalogue2017indexhtml268z
International Journal of Microbiology 9
Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom

Hindawiwwwhindawicom
International Journal of
Volume 2018
Zoology
Hindawiwwwhindawicom Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Hindawiwwwhindawicom Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Neuroscience Journal
Hindawiwwwhindawicom Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Biochemistry Research International
ArchaeaHindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Genetics Research International
Hindawiwwwhindawicom Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Enzyme Research
Hindawiwwwhindawicom Volume 2018
International Journal of
MicrobiologyHindawiwwwhindawicom
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwwwhindawicom