Embed Size (px)
Citation preview

1
Geriatric Pharmacology: Tools for the HealthCare Professionals
Steven Atkinson PA-C, MS Geriatric Internal Medicine – Denver, CO
Adjunct Faculty – University of Utah
Mindful Geriatrics LLC
Avoid disturbing others:
Please turn off cell phones and pagers during the presentation.
Thank You for coming today- We really appreciate it!
Objectives 1. Apply techniques and identify strategies to avoid
adverse drug events and drug disease interactions.
2. Develop individualized monitoring plans for geriatric patients through the evaluation of high risk medications.
3. Identify at least three new guideline recommendations related to geriatric pharmacology.

2
Drug Utilization Elderly utilize approximately 45% of
prescriptions.
Amongst those Americans over 60, more than 76% used 2 or more prescriptions and 37% used 5 or more prescription medications.
Qiuping Gu et al. Prescription Drug Use Continues to Increase: US Prescription Drug Data for 2007-2008. NCHS Data Brief No. 42, September 2010.
Drug Utilization Amongst the Elderly
The most commonly used types of prescription drugs amongst older adults were: – cholesterol lowering – beta-blockers – diuretics
Qiuping Gu et al. Prescription Drug Use Continues to Increase: US Prescription Drug Data for 2007-2008. NCHS Data Brief No. 42, September 2010.
The “Concept” of a “Pill”
Getting a medication is driven into our medical system. Use is driven BOTH by patients and physicians. In the United States, 75% of initial consults result in a
script. Scripts signify the end of the consultation. Scripts mean “something has been done.” Patients can feel “cheated” if no script. Physicians “give in” to demands.

3
Why This Doesn’t Work in Geriatrics
Physiologic changes can make the elderly more sensitive to a drugs effects.
Chronic disease affects an elderly person’s responses to drugs.
Up to 30% of hospital admissions of patients aged 65 and over are due to Adverse Drug Events (ADEs)
Hanlon JT, Schmader KE, et al. Adverse drug events in high risk older outpatients. J Am Geriatr Soc 1997;45:945-948.
The Pathophysiology of Aging
Generalities of Physiologic Aging
Total body water decreases Lean body mass decreases Body fat increases Blood protein decreases Hepatic blood flow decreases Renal blood flow is decreased Decreased baroreceptor response

4
Aging and Pharmacokinetics Pharmacokinetics describes how the body affects
a specific drug taken into the body.
Aging and Pharmacokinetics Absorption
– the process of a substance entering the blood circulation. It is described by its bioavailability.
Distribution – the dispersion or dissemination of substances throughout the
fluids and tissues of the body.
Metabolism – how a drug is converted from its parent compound into its
daughter metabolites. These alternate compounds may be pharmacologically active or inactive.
Elimination – the process of removal of compounds from the body.
Absorption
The process of a substance entering the blood circulation. It is described by its bioavailability.

5
Factors Affecting Absorption Alterations in physiology for the elderly
– gastric acid secretion is decreased – gastric pH is increased – decreased GI blood flow – decreased GI motility – decrease in pancreatic trypsin
Aging and Absorption
Despite this, overall amount absorbed (bioavailability) tends to be unchanged in the elderly EXCEPT FOR……
Factors Affecting Absorption
Vitamin use can affect absorption – calcium, magnesium, iron
Enteral feedings can affect absorption Taking medications that influence gastric pH Dysphagia

6
Distribution
The dispersion or dissemination of substances throughout the fluids and tissues of the body.
Aging and Distribution
Alterations in physiology for the elderly – lean body weight and total body water is
decreased (up to 20%) – there are increases in body fat (female > male)
up to 35% – overall decreases in serum albumin which leads
to lower protein binding – Plasma volume decreases by 8-10%
The Quick and Dirty About Distribution
Serum levels of water soluble drugs may go down.
Serum levels of fat soluble drugs may go up.
Gives meaning to the phrase: “Start low and go slow”

7
Examples of Medications with Altered Distribution
APAP Meperidine
Amiodorone Methadone
Cimetidine NSAIDS
Diazepam Phenytoin
Digoxin Phenobarbital
Ethanol Quinine
Gentamicin Theophylline
Metabolism
How a drug is converted from its parent
compound into its daughter metabolites. These alternate compounds may be pharmacologically active or inactive.
Metabolism Metabolic clearance by the liver may be
reduced as a consequence of: – decreased hepatic blood flow – decreased liver size and mass

8
Metabolic Pathways
Pathway Effect Examples
Phase I: oxidation, hydroxylation, dealkylation, reduction
Conversion to metabolites of lesser, equal, or greater
diazepam, quinidine, piroxicam, theophylline
Phase II: glucuronidation, conjugation, or acetylation
Conversion to inactive metabolites
lorazepam, oxazepam, temazepam
*** Keep this in mind with the elderly: Phase II hepatic metabolism are generally preferred in the elderly due to inactive metabolites which decreases accumulation
Farho, L. Geriatric Pharmacology. Last accessed online 2/13/2011.
The Oxidative Pathway
Oxidative pathway is also known as the Cytochrome P450/CYP450/P450 system.
This system explains why drug-drug interactions can occur
Why is the CYP System Important?
Why? – Inhibitors and inducers of CYP could lead to
increased/decreased bioavailability and thereby increase the possibility of overdosing or adverse drug events.
Guengerich FP (January 2008). "Cytochrome p450 and chemical toxicology". Chem. Res. Toxicol. 21 (1): 70–83.

9
Cytochrome P450 It accounts for nearly 75% of the total number of
metabolic reactions. There are “families” of CYP (usually called substrates).
Guengerich FP (January 2008). "Cytochrome p450 and chemical toxicology". Chem. Res. Toxicol. 21 (1): 70–83.
A Closer Look at the Cytochrome System
To “Re”Iterate Inhibitors: block the metabolic activity of one or more of
the CYP450 enzymes. This means an inhibitor can result in a clinically significant INCREASE in pharmacologic effects of drugs.
Inducers: increase CYP450 enzyme activity by increasing enzyme synthesis. This means an inducer can result in a clinically significant decrease in pharmacologic effects of drugs.

Examples of Drugs with CYP450 Effects Inhibitors Inducers
All Tricyclic Antidepressants Carbamazepine
Amiodorone Phenytoin
Buproprion Phenobarbital
Cimetidine Quinine
Ciprofloxacin Nicotine
Diltiazem / Verapamil Rifampin
Duloxetine / Paroxetine / Fluvoxamine St. Johns Wart
Keto- and Itraconazole Topiramate
Meperidine Valproic Acid
Methadone
Metoclopramide
Inhibitors: block the metabolic activity of one or more of the CYP450 enzymes which leads to a decrease in metabolism, a decrease in clearance and an increase in concentration. Inducers: increase CYP450 enzyme activity by increasing enzyme synthesis
INHIBITORS - CYTOCHROME P450 (CYP) ENZYMES DRUG TABLE
CYP1A2
CYP2B6
CYP2C8
CYP2C9
CYP2C19
CYP2D6
CYP2E1
CYP3A4
Amiodarone Atazanavir Cimetidine Ciprofloxacin Citalopram Clarithromycin Diltiazem Enoxacin Erythromycin Estradiol Fluvoxamine Interferon Isoniazid Ketoconazole Methoxsalen Mibefradil Tegaserod
Thiopeta Ticlopidine
Anastrozole Ezetimibe Gemfibrozil Montelukast Nicardipine Sulfinpyrazone Trimethoprim
Amiodarone Atazanavir Cimetidine Clopidogrel Cotrimoxazole Delavirdine Disulfiram Efavirenz Fenofibrate Fluconazole Fluorouracil Fluoxetine Fluvastatin Fluvoxamine Gemfibrozil Imatinib Isoniazid Itraconazole Ketoconazole Leflunomide Lovastatin Methoxsalen Metronidazole* Mexiletine Modafinil Nalidixic acid Norethindrone Norfloxacin Omeprazole Contraceptives Paroxetine Phenylbutazone Probenecid
Cimetidine Citalopram Delavirdine Efavirenz Felbamate Fluconazole Fluoxetine Fluvastatin Fluvoxamine Indomethacin Isoniazid Ketoconazole Lansoprazole Modafinil Omeprazole Oxcarbazepine Probenecid Ticlodipine Topiramate
Abiraterone Amiodarone Asenapine Buproprion Celecoxib Chloroquine Chlorpheniramine Chlorpromazine Cimetidine Cinacalcet Citalopram Clemastine Clomipramine Cocaine Darifenacin Desipramine Diphenhydramine Doxepin Doxorubicin Duloxetine Escitalopram Febuxostat Fluoxetine Fluphenazine Halofantrine Haloperidol Hydroxychloroquine Hydroxyzine Imatinib Levomepromazine
Disulfiram
Amiodarone Amprenavir Aprepitant Atazanavir Boceprevir Cimetidine Ciprofloxacin Clarithromycin Cyclosporine Danazol Delavirdine Diltiazem Efavirenz Erythromycin Ethinyl Estradiol Ezetimibe (p) Fluconazole Fluoxetine Fluvoxamine Gestodene Imatinib Indinavir Isoniazid Itraconazole Ketoconazole* Methylprednisolone Mibefradil Miconazole Mifepristone Nefazodone Nelfinavir Nicardipine

11
INHIBITORS - CYTOCHROME P450 (CYP) ENZYMES DRUG TABLE
CYP1A2
CYP2B6
CYP2C8
CYP2C9
CYP2C19
CYP2D6
CYP2E1
CYP3A4
See previous slide
See previous slide
See previous slide
Cont from previous slide Sertraline Sulfamethoxazole* Sulfaphenazole Sulfonamides Tacrine Teniposide Ticlodipine Tipranavir Troleandomycin Voriconazole Zafirlukast Zileuton
See previous slide
Cont from previous slide Methadone Metoclopramide Mibefradil Midodrine Moclobemide Nefazodone Norfluoxetine Paroxetine Perphenazine Propafenone Propranolol Quinacrine Quinidine Ranitidine Ranolazine Ritonavir Sertraline Tegaserod Terbinafine Thioridazine Ticlodipine Tipranavir Tripelennamine
See previous slide
Cont from previous slide Norethindrone Norfloxacin Norfluoxetine Oxiconazole Posaconazole Prednisone Quinine Ranolazine Ritonavir Saquinavir Sertraline Telaprevir Telithromycin Troleandomycin Verapamil Voriconazole Zafirlukast Zileutin
http://www.pharmacologyweekly.com/content/pages/medications-herbs-cytochrome-p450-cyp-inhibitors
INDUCERS - CYTOCHROME P450 (CYP) ENZYMES DRUG TABLE
CYP1A2
CYP2B6
CYP2C8
CYP2C9
CYP2C19
CYP2D6
CYP2E1
CYP3A4
Carbamazepine Clotrimazole Phenobarbital Phenytoin Primidone Psoralen Smoking
Barbiturates Phenobarbital Phenytoin Primidone Roflumilast
Carbamazepine Phenytoin Rifabutin Rifampin
Aprepitant Barbiturates Carbamazepine Primidone Rifampin Vigabatrin
Barbiturates Norethindrone Phenytoin Rifampin
Carbamazepine Ethanol Phenobarbital Phenytoin Primidone Rifampin
4-methyl- Pyrazole Ethanol Isoniazid
Amprenavir Barbiturates CarbamazepineClotrimazole DexamethasonEfavirenz Ethosuximide Griseofulvin Modafinil Nevirapine Oxcarbazepine Phenobarbital Phenytoin Prednisone Primidone Rifabutin Rifampin Rifapentine Ritonavir Topiramate
http://www.pharmacologyweekly.com/content/pages/medications-herbs-cytochrome-p450-cyp-inducers

12
An Example Inducers
– Olanzapine's clearance is increased by 98% in smokers.1
– In one study, smokers were found to have an approximate fivefold-lower dose-corrected steady-state plasma olanzapine concentration compared with nonsmokers.2
– What would happen if that smoker decided to quit? What would you do?
Carrillo JA, Herraiz AG, Ramos SI et al. Role of the smoking-induced cytochrome P450 (CYP) 1A2 and polymorphic CYP2D6 in steady-state concentration of olanzapine. J Clin Psychopharmacol. 2003; 23:119-27.
Fulton B, Goa KL. Olanzapine. A review of its pharmacological properties and therapeutic efficacy in the management of schizophrenia and related psychoses. Drugs. 1997; 53:281-98.
Interaction of Other Substances
Grapefruit juice inhibits CYP3A4-mediated metabolism.
Elimination
The process of removal of compounds from the body.

13
Important Concepts in Drug Elimination
Half-life (t1/2) – time for a drug to decline by 50% in the serum
(expressed as hours). – It takes approximately 5 half-lives for a drug to reach
Steady State.
Steady State – time for a drug to reach a “state” where it’s
essentially the same in the blood stream at all times.
Clearance – Measurement by which a drug is removed from the
body expressed as per unit of time (mL/min or L/hr).
Why is that Important?
Reduced elimination drug accumulation and toxicity
Effects of Aging on the Kidney In general, there is a:
– kidney size – renal blood flow – tubular secretion
Leads to a decrease in glomerular filtration rate (GFR)

14
The Problem with Creatinine
Serum creatinine alone is NOT an accurate description of kidney function in the elderly. – lean body mass lower creatinine production
Creatinine Clearance and Age
Limitations in Estimating CrCl
In pts, particularly those who are cachectic, muscle mass is markedly reduced and SCr (serum creatinine) is affected. – As a consequence, you may overshoot actual
CrCl Cockcroft-Gault Equation
Weight in kg and SCr is the serum creatinine concentration in mg/dl.

15
Why GFR Matters
Stages of Chronic Kidney Disease (CKD) and GFR
Definition of Chronic Kidney Disease (CKD) – Persistent eGFR <60mL/min/1.73m2 on two tests at
least three months apart
Important stages in Geriatrics – Stage III – eGFR 30-59 (moderately dec GFR) – Stage IV – eGFR 15-29 (severely dec GFR) – Stage V – kidney failure
Stages of Chronic Kidney Disease (CKD) and GFR
A GFR < 50mL/min/1.73m2 is associated with an increased risk of death (esp. for patients LESS than 75 years of age).
GL Smith et al. Renal impairment and outcomes in heart failure. Systematic review and meta-analysis. Journal of the American College of Cardiology 2006 47: 1987-1996.
GL Smith. Serum urea nitrogen, creatinine, and estimators of renal function. Mortality in older patients with cardiovascular disease. Archives of Internal Medicine 2006 166: 1134-1142.

16
Creatinine Clearance and GFR
GFRMDRD/IDMS = 175 x (Scr)-1.154 x (Age)-0.203
x (0.742 if female) x (1.212 if African American)
Bottom Line
Using GFR instead of CrCl will help minimize adverse drug reactions but if CrCl is desired in a GERIATRIC PATIENT, studies indicate that CrCl is an acceptable predictor.
Spruill WJ et al. Comparison of estimated glomerular filtration rate with estimated creatinine clearance in the dosing of drugs requiring adjustments in elderly patients with declining renal function. Am J Geriatr Pharmacother. 2008 Aug;6(3):153-60.
GFR/CrCl Calculator http://nkdep.nih.gov/lab-evaluation/gfr-calculators/adults-conventional-unit.asp
http://www.globalrph.com/crcl.cgi
Epocrates is also a good FREE resource that can be used

17
Drugs with Decreased Renal Elimination Examples of drugs with a decrease in clearance:
– abx (cephalosporins, PCNs, tetracycline, aminoglycosides, quinolones) – allopurinol – amantadine – atenolol – colchicine – digoxin – furosemide – gabapentin – H2 blockers – hydrochlorothiazide – lithium – phenobarbital/phenytoin/valproic acid – procainamide – theophylline – vancomycin – warfarin
Precautions using CrCl
Precautions in CrCl are based on a SINGLE value – CrCl < 30mL/min
Example: Creatinine Clearance vs. GFR in a Caucasian Female. She is
5’5” and weighs 64 kg
To convert lbs to kg… divide the patients wt in lbs by 2.2. Example: 150lbs/2.2= 68.2kg
Age Serum Cr CrCl GFR
30 1.1 64 62
50 1.1 52 56
70 1.1 41 49
85 1.1 32 47

18
Why These Billing Codes Matters
Code for CKD = 585
CKD III – 585.3 CKD IV – 585.4 CKD V – 585.5
Let’s insurance companies know the nature
of the difficult patients we see!
Knowing This Helps with Pharmacodynamics
Pharmacodynamics is the study of the biochemical and physiological effects of drugs on the body or on microorganisms or parasites within or on the body.
It also addresses the mechanisms of drug action and the relationship between drug concentration and effect.
This is just another way of saying: What does the drug do to the body and how long will it be in there?
What Does it Mean Again?
More importantly it means that older patients can have altered sensitivities to medications— – benzos – opioids – anti-cholinergic meds – dopaminergic meds – anti-HTN

19
Understand Kidney Function and Pharmacodynamics
Having an understanding of what renal function is like, means there is less chance you will “harm” a patient by dosing in “higher” than expected doses.
Remember… the majority of drug studies are NOT done on those patients aged 75
and greater.
Optimal Pharmacotherapy
This is a balance between overprescribing and under prescribing – correct drug – correct dose – targets the appropriate condition – is NECESSARY for the patient

20
Optimal Pharmacotherapy
Avoid “a pill for every ill”
ALWAYS consider non-pharmacological therapies
Consequences of Overprescribing
1. Adverse drug events (ADEs) 2. Drug-Drug Interactions 3. Anorexia 4. Decreased quality of life 5. Non-compliance with medications 6. Increased unnecessary cost
A Quick Focus on Anorexia
Anorexia/Wt Loss and the Elderly – In Geriatrics, we are taught to think of cancer – I’m telling you to think FIRST about
medications as the cause elderly patients who lost 5 percent of their body
weight in one month were found to be four times more likely to die within one year
Ryan C, Bryant E, Eleazer P, Rhodes A, Guest K. Unintentional weight loss in long-term care: predictor of mortality in the elderly. South Med J. 1995;88:721–4.

21
Cancer Cause More Likely to be Meds
Etiology of Unintentional Weight Loss in the Elderly
Diagnosis Incidence of Diagnosis (Nursing Home Residents)
Cancer 7%
Medication Effect 14%
Huffman, GB. Evaluating and Treating Unintentional Weight Loss in the Elderly. Am Fam Physician. 2002 Feb 15;65(4):640-651.
Table adapted with permission from Huffman, GB and American Family Physician.
Looking at Adverse Drug Events
Adverse Drug Events (ADEs)
ADEs are defined as ANY injury resulting from drug therapy.
More than 95% of ADEs that occur in the elderly and ARE considered predictable; approximately 50% are considered preventable.
Hamilton HJ, Gallagher PF et al. Inappropriate prescribing and adverse drug events in older people. BMC Geriatrics 2009, 9:5.

22
Why Learn about ADE’s? Over 2 MILLION serious ADEs annually.
Account for over 100,000 DEATHS annually.
Fatal ADEs rank between 4th and 6th in the
United States.
In nursing home patients, ADE rate is 350,000 patients annually (approx 66%).
Bond CA, Raehl CL, Adverse Drug Reactions in United States Hospitals. Pharmacotherapy. 2006;26(5):601-608.
Lazarou J et al. JAMA. 1998.279(15): 1200-1206.
Fick, DM et al. Updating the Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. Arch Intern Med. 2003;163:2716-2724.
“If medication related problems were ranked as a disease, it
would be the fifth leading cause of death in the US!”
*Beers MH. Arch Internal Med. 2003
Reasons It’s so High
In the United States, 75% initial consults result in a script.
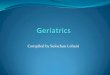
ADEs increase expodentially after 5 or more medications.

23
Cresswell K M et al. Br Med Bull 2007;83:259-274
The relationship between adverse drug effects and number of drugs
The Prescribing Cascade
Drug 1
ADE perceived as a new medical condition
Drug 2
ADE perceived as a new medical condition
Drug 3
Rochon PA, Gurwitz JH. Optimizing drug treatment in elderly people: the prescribing cascade. BMJ 1997;315:1097.
Examples – NSAIDs -> HTN-> antihypertensive therapy initiated
– Metoclopramide-> Parkinsonism-> carbidopa/levodopa initiated
– NSAIDs-> blood in stool-> H2 blocker-> delirium-> haldol initiated
– HCTZ-> gout-> NSAIDs-> antihypertensive initiated
– OTC pseudoephedrine-> urinary retention-> alpha blocker
– Antipsychotic-> EPS-> primidone
– Parkinsonian” features-> carbidopa/levodopa-> hallucinations->
antipsychotics added
– ChI’s-> Urinary Incontinence > Oyxbutinin

24
Risk Factors for ADEs
1. ≥ 6 medications 2. ≥ 6 chronic conditions (drug-disease
interactions) 3. ≥ 12 medication doses/day 4. GFR < 60 mL/min 5. Prior adverse drug event 6. Age ≥ 85 7. Having a low ideal body weight
Adapted from Fouts M, Hanlon J, Pieper C, Perfetto E, Feinberg J. Identification of elderly nursing facility residents at high risk for drug-related problems. Consult Pharm 1997;12:1103-11.
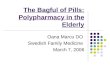
Most Common Medications Associated with ADEs in the Elderly
Adapted from: Polypharmacy and Adverse Drug Reactions (ADR) in the Elderly. Last accessed online July 7, 2011. Used with Permission from Professor Graham Davies Professor of Clinical Pharmacy & Therapeutics. http://www.bgscv.org.uk/presentations/assets/Professor%20Graham%20Davies.ppt
Most frequent drug class causing ADEs %
Cardiovascular active agents Analgesics (opioids/benzos) Antibiotics Hypoglycemic agents Psychotropic agents Anticoagulants Others (NSAIDS, Anticholinergics)
34 18 15 10 7 5 11
Common Drug-Disease Interactions
Combination Risk
NSAIDs + CHF Thiazolidinediones + CHF
Fluid retention; CHF exacerbation
BPH + anticholinergics Urinary retention
CCB + constipation Narcotics + constipation Anticholinergics + constipation
Exacerbation of constipation
Metformin Increased risk of lactic acidosis (Cr cutoff is 1.4 in &, Cr cutoff is 1.5 in %)
NSAIDs + gastropathy Increased ulcer and bleeding risk
NSAIDs + HTN Fluid retention; decreased effectiveness of diuretics

25
Why ADE’s Occur
Increases as the number of medications increase. Increases as the age of the patient increases. Multiple practioners – more hands in the pot. Increases with patient frailty. Increases when patients “pharmacy shop.” Prescribing pressures contribute. Drug promotion contributes. A multitude of new medications for prevention. Limited consultative time. Habit.
Seymour RM, Routledge PA. Important drug-drug interactions in the elderly. Drugs Aging. 1998 Jun;12(6):485-94.
What Can You Take From This?
Guiding Principles for Prescribing in the Elderly
It is possible to arrive at a group of medications that have clear relevance to
care, that is scientifically valid, usable, and feasible and doesn’t place the patient at a
significant risk!

26
Principles of Prescribing in the Elderly 1. Evaluate the need for the drug therapy.
- CONSIDER the quality of life measure of the drug.
- CONSIDER non-pharmacologic agents first! 2. Avoid prescribing prior to having a high “index of suspicion” for a
diagnosis. 3. Know the pharmacologic effects of the drugs prescribed.
- rule out side effects as a cause of new symptoms such as confusion or memory loss.
4. Use a few drugs well, rather than many drugs poorly. 5. Start “low” and go “slow.” 6. Titrate drugs to response (understand t1/2). 7. Avoid initiating two agents at the same time if possible. 8. AVOID intermittent schedules if possible. 9. Give SIMPLE instructions. 10. Follow-up shortly after initiating any “new” medication. 11. Review and re-review the treatment plan regularly. Discontinue drug
therapy when it’s no longer needed. 12. Eliminate PRN medications.
Additional Practical Guidelines for Prescribers
Consider risk vs. benefit. Use simplest regimen possible. Consider drug-drug interactions. Consider drug-disease interactions (discussed
earlier). Avoid the “prescribing cascade.” Attempt to prescribe a drug that will treat more
than one existing problem. Determine therapeutic endpoints and plan for
assessment. Adjust doses for renal and hepatic impairment in
the elderly.
Avoiding Polypharmacy
Review medications regularly and each time a new medication started or dose is changed.
Maintain accurate medication records (include vitamins, OTCs, and herbals).
Have clinic patients bring in their “Brown-Bag” if applicable at least annually and get your staff to go through this.

27
Avoiding Polypharmacy Understand side effect profiles Identify risk factors for an ADE
– http://www.drugs.com/drug_interactions.html
Consider the risk versus benefit ratio Keep dosing simple (qD or BID) Ask about or review the compliance of
medications Don’t use medications to treat side effects of
other medications Ask pharmacist for help identifying interactions Consider what you can discontinue!!
Individualizing a Monitoring Plan 1. Review current drug therapy (substitute with safer
alternatives) and discuss it with the patient. 2. Discontinue unnecessary therapy (use the
algorithm or base it on knowledge of risks). 3. Consider and discuss nonpharmacologic
approaches with the patient FIRST. 4. Reduce the dose of medications when feasible and
appropriate. 5. Consider adverse drug event for ANY new
symptom. 6. Simplify the dosing schedule. 7. Prescribe beneficial and medically necessary
therapy.
What Should We Avoid?

28
The Role of the Practioner
Living up to Mantra’s of Geriatric Medicine - “do no harm” - “start low and go slow”
Ten Medications the Elderly Should Avoid NSAIDs Digoxin (in doses > .125mg) Certain diabetic drugs
– glyburide (Diabeta, Micronase), chlorpropamide (Diabinese)
Muscle relaxants – cyclobenzaprine (Flexeril), methocarbamol (Robaxin), and carisoprodol (Soma)
• Certain meds for anxiety and/or insomnia – diazepam (Valium), alprazolam (Xanax), or chlordiazepoxide (Librium) and
sleeping pills such as zaleplon (Sonata) and zolpidem (Ambien)
Anticholinergic drugs Pain Relievers like meperidine (Demerol) Certain Over-the-Counter Products
– diphenhydramine (Benadryl) and chlorpheniramine (AllerChlor, Chlor-Trimeton) (particularly in men with an enlarged prostate). over-the-counter sleep products, like Tylenol PM
If you are NOT being treated for psychosis, AVOID using Antipsychotics – haloperidol (Haldol), risperidone (Risperdal), or quetiapine (Seroquel).
AVOID Estrogen pills and patches Adapted from: The American Geriatrics Society April 2012

29
Ten Medications the Elderly Should Avoid NSAIDs Digoxin (in doses > .125mg) Certain diabetic drugs
– glyburide (Diabeta, Micronase), chlorpropamide (Diabinese)
Muscle relaxants – cyclobenzaprine (Flexeril), methocarbamol (Robaxin), and carisoprodol (Soma)
• Certain meds for anxiety and/or insomnia – diazepam (Valium), alprazolam (Xanax), or chlordiazepoxide (Librium) and
sleeping pills such as zaleplon (Sonata) and zolpidem (Ambien)
Anticholinergic drugs Pain Relievers like meperidine (Demerol) Certain Over-the-Counter Products
– diphenhydramine (Benadryl) and chlorpheniramine (AllerChlor, Chlor-Trimeton) (particularly in men with an enlarged prostate). over-the-counter sleep products, like Tylenol PM
If you are NOT being treated for psychosis, AVOID using Antipsychotics – haloperidol (Haldol), risperidone (Risperdal), or quetiapine (Seroquel).
AVOID Estrogen pills and patches Adapted from: The American Geriatrics Society April 2012

30
Beers 2012
The drugs to follow (IN THE TABLES) are “classified” as inappropriate for elderly persons. – 2012 updates include: new evidence of potentially inappropriate meds. grading the strength and quality of each
recommendation. exceptions into the criteria.
The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. AGS updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012. FOR ALL THE SLIDES THAT FOLLOW WITH BEERS 2012.
The MOST Common

31
Anticholinergics(First Generation Antihistamines)
Organ System or Therapeutic Category or Drug
Rationale
Recommendation
Quality/ Strength
First‐generation antihistamines
Highly anticholinergic; clearance reduced with advanced age, and tolerance develops when used as hypnotic; greater risk of confusion, dry mouth, constipation, and other anticholinergic effects and toxicity. Use of diphenhydramine in special situations such as acute treatment of severe allergic reaction may be appropriate.
Avoid
Hydroxyzine and promethazine high; all others moderate/strong
brompheniramine carbinoxamine* chlorpheniramine clemastine cyproheptadine
dexbrompheniramine*
dexchlorpheniramine*
diphenhydramine (oral)
doxylamine
hydroxyzine promethazine (Phenergan)
triprolidine*
*new on updated Beers
Anti-infective
Organ System or Therapeutic
Category or Drug Rationale
Recommendation
Quality /Strength
Nitrofurantoin*
Potential for pulmonary toxicity; safer alternatives available; lack of efficacy in patients with low GFR d/t inadequate drug concentration in the urine.
Avoid for long‐term suppression; avoid in pts with
low GFR
Moderate / Strong
*new on updated Beers

32
Adapted from:
Stone N, Ashraf M, et al. Surveillance Definitions of Infections in Long-Term Care Facilities: Revisiting the McGeer Criteria. Infect Cont Hosp Ep. 2012;33(10): 965-977.

33
Cardiovascular Medications Organ System or
Therapeutic Category or Drug
Rationale
Recommendation
Quality /Strength
Alpha1 blockers:
High risk of orthostatic hypotension; not recommended as routine treatment for HTN; alternative agents have superior risk/benefit profile.
Avoid use as an antihypertensive
Moderate/Strong
doxazosin prazosin* terazosin*
Alpha agonists, central
High risk of adverse CNS effects; may cause bradycardia and orthostatic hypotension; not recommended as routine treatment for hypertension.
Avoid clonidine as a first‐line antihypertensive. Avoid others as listed.
Low/ Strong
clonidine guanabenz* guanfacine* methyldopa reserpine (>.1mg/d)*
Antiarrhythmic drugs
Data suggest that rate control yields better balance of benefits and harms (than rhythm control) for most older adults. Amiodorone is asst with multiple toxicities, including thyroid disease, pulmonary disorders, and QT‐interval prolongation.
Avoid antiarrhythmic drugs as first‐line treatment of atrial
fibrillation.
High / Strong
amiodarone dofetilide* dronedarone* flecainide* ibutilide* procainamide propafenone quinidine sotalol*
*new on updated Beers
Cardiovascular Medications Organ System or
Therapeutic Category or Drug
Rationale
Recommendation
Quality /Strength
Digoxin >0.125mg/day
In heart failure, higher dosages associated with no additional benefit and may increase risk of toxicity; slow renal clearance may lead to risk of toxic effects.
Avoid
Low / Strong
Nifedipine, immediate release
Potential for hypotension; risk of precipitating myocardial ischemia.
Avoid
High / Strong
*new on updated Beers
Spironolactone (>25mg/d)
In heart failure, the risk of hyperkalemia is higher in older adults especially if taking > 25mg/d or taking concomitant NSAID, ACE, ARB or K+
Avoid in pts with heart failure or with low GFR
Moderate/Strong

34
Thoughts about BP in Geriatrics
Use symptoms as your indicator as to what is acceptable control of BP in the frail elderly1,2... but get it to goal in the face of no symptoms.3
Complications resulting from falls are the leading cause of death from injury in men and women older than age 65.1
Low SBP (≤128mmHg) was independently associated with a greater progression of cognitive decline in older patients with dementia and MCI.4
1. Durso SC, Sullivan GM, eds. Geriatrics Review Syllabus: A Core Curriculum in Geriatric Medicine. 8th ed. New York: American Geriatrics Society; 2013.
2. James PA, Oparil S, Carter BL, et al; 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8). JAMA. Published online December 18, 2013.
3. Beckett NS, Peters R. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008 May 1;358(18):1887-98. 4. Mossello E, PieraccioliM, Nesti N, et al. Effects of low blood pressure in cognitively impaired elderly patients treated with antihypertensive
drugs [published online March 2, 2015]. JAMA Intern
Cardiovascular Medications Organ System or
Therapeutic Category or Drug
Rationale
Recommendation
Quality /Strength
*new on updated Beers
Spironolactone (>25mg/d)
In heart failure, the risk of hyperkalemia is higher in older adults especially if taking > 25mg/d or taking concomitant NSAID, ACE, ARB or K+
Avoid in pts with heart failure or with low GFR
Moderate/Strong

35
Central Nervous System Organ System or
Therapeutic Category or Drug
Rationale
Recommendation
Quality /Strength
Benzodiazepines (short/int’d acting) Older adults have increased sensitivity to BZDs and slower metabolism of long‐acting agents. In general, all BZDs increase risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents in older adults. May be appropriate for seizure disorders, rapid eye movement sleep disorders, benzo withdrawal, ethanol withdrawal, severe generalized anxiety disorder, periprocedural anesthesia, end‐of‐life.
Avoid BZD (any type) for treatment of insomnia, agitation, or delirium
High / Strong
alprazolam estazolam* lorazepam oxazepam* temazepam triazolam
Benzodiazepines (long acting)
clorazepate* chlordiazepoxide‐amitriptyline clidinium‐chlordiazepoxide clonazepam diazepam flurazepam quazepam
*new on updated Beers
The Risk of Benzo’s
Use of near-daily benzodiazepines for >180 days was associated with a 1.5-fold increase in risk of AD after adjusting for multiple potential confounders, including anxiety, depression, and insomnia.
A dose-response effect was observed, with longer exposure and longer-half life drugs associated with increased risk.
Billioti de Gage s, Moride Y et al. Benzodiazepine use and risk of Alzheimer’s disease: case-control study. BMJ 2014;349:g5205.

36
Central Nervous System Organ System or
Therapeutic Category or Drug
Rationale
Recommendation
Quality /Strength
Tertiary TCAs
Highly anticholinergic, sedating, and cause orthostatic hypotension; safety profile of doxepin (≤6mg/d) is comparable with placebo.
Avoid
High / Strong
amitriptyline chlordiazepoxide‐amitriptyline clomipramine doxepin > 6mg/d imipramine perphenazine‐amitriptyline trimipramine*
Antipsychotics, first (conventional) and second (atypical) generation
Increase risk of CVA and mortality in persons with dementia.
Avoid
Moderate / Strong
Nonbenzodiazepine hypnotics
BZD‐receptor agonists that have adverse events similar to those of BZDs in older adults (delirium, falls, fractures); minimal improvement in sleep latency and duration.
Avoid chronic use (>90 days)
High / Strong
eszopiclone* zolpidem* zaleplon*
*new on updated Beers
Endocrine Organ System or Therapeutic
Category or Drug
Rationale
Recommendation
Quality/ Strength
Androgens
Potential for cardiac problem and contraindicated in men with prostate CA.
Avoid unless indicated for mod/severe hypogonadism.
Moderate / Weak
methyltestosterone* testosterone*
Estrogens with or without progestins
Evidence of carcinogenic potential (breast and endometrium); lack of cardioprotective effect and cognitive protection in older women.
Avoid oral and topical patch; Topical vaginal cream is
acceptable.
Oral and patch: strong
Topical: weak
Insulin, sliding scale
Higher risk of hypoglycemia without improvement in hyperglycemia management regardless of care setting.
Avoid
Moderate / Strong
*new on updated Beers
Sulfonylureas (long duration) Chlorpropamide: prolonged half‐life causing prolonged hypoglycemia; causes SIADH. Glyburide: greater risk of prolonged hypoglycemia in older adults.
Avoid
High / Strong
chlorpropamide glyburide*

37
Endocrine Organ System or Therapeutic
Category or Drug
Rationale
Recommendation
Quality/ Strength
Sulfonylureas (long duration)
Chlorpropamide: prolonged half‐life causing prolonged hypoglycemia; causes SIADH. Glyburide: greater risk of prolonged hypoglycemia in older adults.
Avoid
High / Strong
chlorpropamide glyburide*
*new on updated Beers
Which sulfonylurea would be a good option if you needed to use one?
Analgesia Organ System or Therapeutic
Category or Drug
Rationale
Recommendation
Quality/ Strength
Non‐COX‐selective NSAIDs, oral
Increases risk of GI bleeding and PUD in high‐risk groups, including those aged > 75 or taking orals or parenteral corticosteroids, anticoagulants, or antiplatelet agents. Use of PPI or misoprostol reduces but doesn’t eliminate risk. Upper GI ulcers, gross bleeding or perforation by NSAIDs occur in approximately 1% of patients treated for 3‐6 months and in approximately 2‐4% of patients for 1 year. These trends continue with longer duration of use.
Avoid chronic use unless other altneratives are not
effective and patient can take GI protective agent (PPI or
misoprostol)
Moderate/ Strong
ASA > 325mg/dl diclofenac* diflunisal* etodolac* fenoprofen* ibuprofen* ketoprofen* meclofenamate* mefenamic acid* meloxicam* nabumetone* naproxen oxaprozin piroxicam sulindac* tolmetin
Indomethacin Ketorolac, including parenteral
Increases risk of GI hemorrhage and PUD in high‐risk groups. Of all the NSAIDs, indomethacin has the most adverse effects.
Avoid
Indomethacin: moderate
Ketorolac: high / Strong
*new on updated Beers

38
Analgesia Organ System or Therapeutic
Category or Drug
Rationale
Recommendation
Quality/ Strength
Skeletal Muscle Relaxants
Most muscle relaxants are poorly tolerated by older adults because of the anticholinergic adverse effects, sedation, risk of fracture; effectiveness at dosages tolerated by older adults is questionable.
Avoid
Moderate/ Strong
carisoprodol chlorzoxazone cyclobenzaprine metaxaolone methocarbamol orphenadrine
*new on updated Beers

39
Controversial
Vitamins and Supplements
Although dietary supplements are commonly taken to prevent chronic disease, the long-term health consequences of many compounds are unknown.
Is Your MVI Killing You?
The Iowa Women’s Health Study – Use of vitamin and mineral supplements was
examined in relation to total mortality in older women enrolled in the Iowa Women’s Health Study from 1986 - 2008.
– A total of 38,772 women (mean age 61.6) were included in this analysis over 19 years.
Mursu J, Robien K, et al. Dietary Supplements and Mortality Rate in Older Women: The Iowa Women’s Health Study. Arch Intern Med 2011;171:1625-1633

40
Results in the Iowa’s Women’s Health Study
In multivariable adjusted proportional hazards regression models, the use of multivitamins were associated with increased risk of total mortality when compared with corresponding nonuse. – total absolute risk increase 2.4% – vitamin B6 (pyridoxine) 4.1% – folic acid 5.9% – iron 3.9% – magnesium 3.6% – zinc 3.0% – copper 18.0%
Mursu J, Robien K, et al. Dietary Supplements and Mortality Rate in Older Women: The Iowa Women’s Health Study. Arch Intern Med 2011;171:1625-1633
Summary and Recommendations
The possibility of an adverse drug event should always be thought of when evaluating a complaint in the elderly when on multiple mediations i.e. any new symptom should be considered drug-related until proven otherwise.
Pharmacokinetics and pharmacodynamics lead to changes in plasma drug concentrations and increased drug sensitivity.
Recognize that adverse drug events (ADEs) result in as much as four
times as many hospitalizations in the elderly compared with younger, adults. – prescribing cascades, drug-drug interactions, and inappropriate drug doses are some
of the important causes of preventable ADEs.
KNOW the medications to “re-consider” or avoid in elderly adults and for those patients that are on these medications, attempt SLOW downtitrations
Thank You