Embed Size (px)
Citation preview

Balancing Evidence and Clinical Balancing Evidence and Clinical Practice in the Treatment of Practice in the Treatment of
Localized Breast CancerLocalized Breast CancerMay 5, 2006May 5, 2006
Deborah Hamolsky MS, RN : DCISDeborah Hamolsky MS, RN : DCISCarol Franc Buck Breast Care Center Carol Franc Buck Breast Care Center
UCSF Comprehensive Cancer CenterUCSF Comprehensive Cancer Center
Jane Armer PhD, RN : Jane Armer PhD, RN : LymphedemaLymphedemaUniversity of Missouri University of Missouri -- Columbia Columbia
School of NursingSchool of Nursing
DeenaDeena Dell MSN, RN, AOCN, BC : ModeratorDell MSN, RN, AOCN, BC : ModeratorDecision Tools/Session ModeratorDecision Tools/Session Moderator
Fox Chase Cancer Center Fox Chase Cancer Center

DuctalDuctal Carcinoma in Situ (DCIS): Carcinoma in Situ (DCIS): Controversies in CareControversies in Care
Confinement of malignant Confinement of malignant cells within the natural cells within the natural basement membrane of basement membrane of ductductIntraductalIntraductal, , nonnon--invasive, invasive, nonnon--infiltrating,infiltrating,stage 0 breast cancerstage 0 breast cancer
((breastcancerbreastcancer.org.org))Artist: Mary Kelso BrysonArtist: Mary Kelso Bryson

DCIS: Increasing Prevalence, DCIS: Increasing Prevalence, Earlier DetectionEarlier Detection
2005 Statistics: 2005 Statistics: DCIS 58,490 DCIS 58,490
•• 1973 DCIS 2.8% of cases1973 DCIS 2.8% of cases•• 1995 DCIS 15% of cases1995 DCIS 15% of cases•• 2005 DCIS 24% of cases2005 DCIS 24% of cases
~~20% of breast cancers20% of breast cancersdetected by mammographydetected by mammography
(NCI SEER data 2005; ACS, 2005)(NCI SEER data 2005; ACS, 2005)
Decreasing incidence of Decreasing incidence of palpable massespalpable masses
Increasing incidence of Increasing incidence of detection of DCIS with detection of DCIS with nonnon--palpable disease palpable disease
Mammographic Mammographic detection of calcificationsdetection of calcifications
Improved pathological Improved pathological detectiondetection

DCIS ControversiesDCIS Controversies
•• Surgery Surgery Lumpectomy (BCS) vs. Lumpectomy (BCS) vs. Mastectomy?Mastectomy?Sentinel Lymph Node Sentinel Lymph Node (SLN) (SLN) BxBx ??
•• Radiation therapy Radiation therapy None None whole breast (WBR)whole breast (WBR)vs. partial (PBR) vs. partial (PBR)
•• Rx recommendation Rx recommendation problems:problems:DCIS heterogeneous, no DCIS heterogeneous, no uniform gradinguniform gradingInaccuracy of size Inaccuracy of size measurement and measurement and limitations of imaginglimitations of imagingLong natural historyLong natural history(Sanders et al, 2005)(Sanders et al, 2005)Limited published clinical Limited published clinical trial datatrial data

DCIS Classification: Predicting DCIS Classification: Predicting Outcomes, Matching Treatment Outcomes, Matching Treatment
Van Nuys Prognostic Index Van Nuys Prognostic Index Tumor size Tumor size •• Nuclear grade (low, intermediate, high)Nuclear grade (low, intermediate, high)•• Margin widthMargin width•• Presence, absence of Presence, absence of comedonecrosiscomedonecrosis
USC/VNPI USC/VNPI •• Addition of age as variableAddition of age as variable
(Silverstein, Mel 2003)(Silverstein, Mel 2003)

DCIS and MastectomyDCIS and MastectomyRecurrence with Recurrence with mastectomy 1mastectomy 1--2%2%
Mastectomy high cure Mastectomy high cure rate; can be seen as rate; can be seen as prophylactic prophylactic –– prevents prevents invasive ca.invasive ca.
2005 Mast vs. BCS meta2005 Mast vs. BCS meta--analysis 6 trials analysis 6 trials ––mastectomy decreases mastectomy decreases recurrence, no mortality recurrence, no mortality benefit benefit ((JatoiJatoi & & ProshanProshan, 2005), 2005)
How to decide?How to decide?-- ? risk of recurrence? risk of recurrence
-- ? risk of systemic ? risk of systemic disease and mortalitydisease and mortality
-- ? surgical risks and ? surgical risks and emotional outcomes of emotional outcomes of mastectomy with, without mastectomy with, without reconstructionreconstruction
(Fisher, 1998; (Fisher, 1998; JatoiJatoi & & ProshanProshan, 2005, 2005Personal communication L. Margolis, Personal communication L. Margolis, UCSF, 2006)UCSF, 2006)
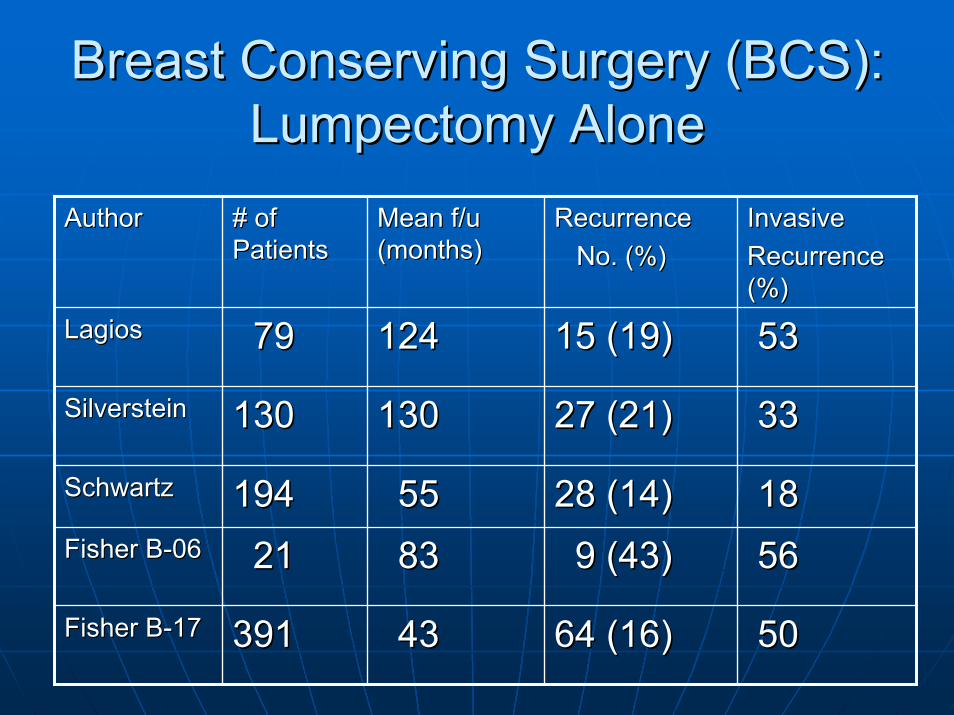
Breast Conserving Surgery (BCS):Breast Conserving Surgery (BCS):Lumpectomy AloneLumpectomy Alone
AuthorAuthor # of # of PatientsPatients
Mean f/u Mean f/u (months)(months)
RecurrenceRecurrenceNo. (%)No. (%)
InvasiveInvasiveRecurrence Recurrence (%) (%)
LagiosLagios 7979 124124 15 (19)15 (19) 5353
SilversteinSilverstein 130130 130130 27 (21)27 (21) 3333
SchwartzSchwartz 194194 5555 28 (14)28 (14) 1818Fisher BFisher B--0606 2121 8383 9 (43)9 (43) 5656
Fisher BFisher B--1717 391391 4343 64 (16)64 (16) 5050

Lumpectomy and Lumpectomy and xRTxRT
AuthorAuthor # of # of PatientsPatients
Mean f/u Mean f/u monthsmonths
Recurrence # Recurrence # (%)(%)
Invasive Invasive Recurrence %Recurrence %
SilversteinSilverstein 185185 9090 10 (18)10 (18) 5353SolinSolin 274274 102102 42 (15)42 (15) 5555ForquetForquet 153153 108108 25 (16)25 (16) 7272Fisher BFisher B--0606 2727 8383 2 (7)2 (7) 5050Fisher BFisher B--1717 399399 4343 28 (7)28 (7) 2929

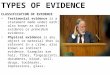
Focal All Linear Ductal All Regional, MultiregionalHeterogeneous
SegmentalClumped
Regional, Multiregional Clumped
Homogenous All (Laura Esserman UCSF, 2004)
Magnetic Resonance Imaging GroupingGeographic Distribution / Enhancement Pattern
n = 8 n = 5 n = 14
Small, ER+Small, ER+↑↑ Ki67, Ki67, ↑↑ gradegrade
↓↓ CD68, CD68, ↓↓ comedocomedoER+ER+
↓↓ CD68, CD68, ↓↓ comedocomedo
n = 11 n = 8 n = 3
ERER--↑↑ Ki67, Ki67, ↑↑ gradegrade
↑↑ Ki67, Ki67, ↑↑ gradegrade↑↑ CD68, CD68, ↑↑ comedocomedo
Large, ERLarge, ER--
↑↑ Ki67, Ki67, ↑↑ gradegrade↑↑ CD68, CD68, ↑↑ comedocomedo

Partial Breast Irradiation (PBI)Partial Breast Irradiation (PBI)
Techniques:Techniques:Brachytherapy Brachytherapy
-- multimulti--cathetercatheter-- balloon catheterballoon catheter-- mammositemammosite-- intraoperativeintraoperative RT with RT with linear accelerator or low linear accelerator or low energy xenergy x--raysrays-- 3D conformal RT3D conformal RT
(Rogers, 2004)(Rogers, 2004)
DCIS DCIS multicentricitymulticentricity& recurrence& recurrence6 studies: 24% of 374 pts. 6 studies: 24% of 374 pts.
(Margolis, L. , UCSF, personal (Margolis, L. , UCSF, personal communication 2006)communication 2006)
Not all pts. eligible for Not all pts. eligible for xRTxRT receive it (pt. choice, receive it (pt. choice, access)access)
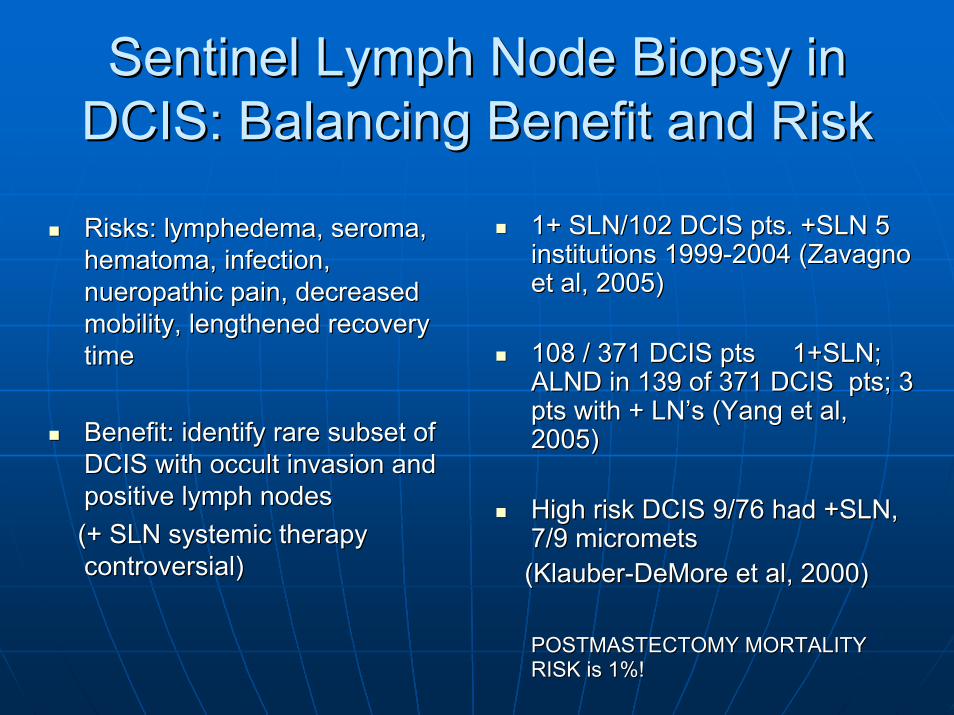
Sentinel Lymph Node Biopsy in Sentinel Lymph Node Biopsy in DCIS: Balancing Benefit and RiskDCIS: Balancing Benefit and Risk
Risks: lymphedema, Risks: lymphedema, seromaseroma, , hematomahematoma, infection, , infection, nueropathicnueropathic pain, decreased pain, decreased mobility, lengthened recovery mobility, lengthened recovery timetime
Benefit: identify rare subset of Benefit: identify rare subset of DCIS with occult invasion and DCIS with occult invasion and positive lymph nodes positive lymph nodes (+ SLN systemic therapy (+ SLN systemic therapy controversial)controversial)
1+ SLN/102 DCIS pts. +SLN 5 1+ SLN/102 DCIS pts. +SLN 5 institutions 1999institutions 1999--2004 (2004 (ZavagnoZavagnoet al, 2005)et al, 2005)
108 / 371 DCIS pts 1+SLN; 108 / 371 DCIS pts 1+SLN; ALND in 139 of 371 DCIS pts; 3 ALND in 139 of 371 DCIS pts; 3 pts with + pts with + LN’sLN’s (Yang et al, (Yang et al, 2005)2005)
High risk DCIS 9/76 had +SLN, High risk DCIS 9/76 had +SLN, 7/9 7/9 micrometsmicromets((KlauberKlauber--DeMoreDeMore et al, 2000)et al, 2000)
POSTMASTECTOMY MORTALITY POSTMASTECTOMY MORTALITY RISK is 1%!RISK is 1%!

Conclusions: Surgery and Whole Conclusions: Surgery and Whole Breast Irradiation (WBR) Breast Irradiation (WBR)
•• Low grade, nonLow grade, non--comedocomedo, , <2.5cm tumor, detected by <2.5cm tumor, detected by ▬▬►▬▬► OBSERVEOBSERVEmammogram, negative marginsmammogram, negative margins
•• High grade, High grade, comedocomedo necrosis,necrosis,>2.5cm tumor, palpable tumor, >2.5cm tumor, palpable tumor, ▬▬►▬▬► RADIATION RADIATION Negative margins, post excision Negative margins, post excision AFTER EXCISIONAFTER EXCISIONMammogramsMammograms
•• Positive margins after excisionPositive margins after excision ▬▬►▬▬► MASTECTOMYMASTECTOMYDiffuse Diffuse microcalcificationsmicrocalcifications
(NSABP B(NSABP B--06,B06,B--17, EORTC 10853, JCRT17, EORTC 10853, JCRT--Harvard, ECOG ES914, Harvard, ECOG ES914, NCCN Practice Guidelines v.2.2006 )NCCN Practice Guidelines v.2.2006 )

Conclusions: Partial Breast Conclusions: Partial Breast Irradiation (PBI) Irradiation (PBI)
1. Preference that patients be 1. Preference that patients be enrolled on protocol; continued enrolled on protocol; continued insufficient evidenceinsufficient evidence
2. Adequate surgeon training for 2. Adequate surgeon training for technique utilization in intratechnique utilization in intra--operative (IORT), balloon operative (IORT), balloon catheter, bead or seed catheter, bead or seed implants, shortened implants, shortened (accelerated) courses of (accelerated) courses of external beamexternal beam
3. Selection Criteria (off trial)3. Selection Criteria (off trial)Age Age >50>50IDC or DCISIDC or DCISTotal tumor size Total tumor size ≤≤2cm2cmNegative margins of at least Negative margins of at least 2mm2mmSLN / ALND negativeSLN / ALND negative
(The American Society of Breast (The American Society of Breast Surgeons, 2003; NCCN Practice Surgeons, 2003; NCCN Practice Guidelines v.2.2006)Guidelines v.2.2006)

Conclusions: Criteria to Include Conclusions: Criteria to Include Sentinel Lymph Node (SLN) BiopsySentinel Lymph Node (SLN) Biopsy
Biopsy SLN with mastectomy (cannot technically do Biopsy SLN with mastectomy (cannot technically do later if occult invasive disease)later if occult invasive disease)Not generally recommended for DCIS with breast Not generally recommended for DCIS with breast conserving surgery unless DCIS conserving surgery unless DCIS >5cm or >5cm or microinvasionmicroinvasion (controversial)(controversial)Insufficient data to include SLN for specific Insufficient data to include SLN for specific biological markers (grade, histology)biological markers (grade, histology)
(ASCO Guidelines, 2005, (ASCO Guidelines, 2005, PendasPendas et al, 2004; et al, 2004; JakubJakub et al, 2004, et al, 2004, NCCN Guidelines, 2006)NCCN Guidelines, 2006)

Future Directions and New Future Directions and New Questions in DCIS TreatmentQuestions in DCIS Treatment
Will surgical treatment Will surgical treatment always be necessary? always be necessary?
The role of adjuvant, The role of adjuvant, neoadjuvantneoadjuvant, therapy, therapy
Ongoing data collection Ongoing data collection re SLN, radiation therapyre SLN, radiation therapy
Role of MRI in DCISRole of MRI in DCIS
Prevention Prevention
NeoadjuvantNeoadjuvant Therapy Therapy hormone (hormone (LetrozoleLetrozole) ) statinstatin trials (trials (FulvestrantFulvestrant))
NSABP BNSABP B--35 35 AnastrozoleAnastrozole v. v. TamoxifenTamoxifen
RTOG 9804 RTOG 9804 xRTxRT v. no v. no xRTxRT for low risk for low risk DCIS DCIS
NSABP BNSABP B--9 9 WBI v. PBRWBI v. PBR(NSABP 2006, UCSF Trials (NSABP 2006, UCSF Trials Program, 2006)Program, 2006)

DCISDCIS
Define Disease SubtypeDefine Disease SubtypeAnd PredispositionAnd Predisposition
(Laura (Laura EssermanEsserman MD UCSF, 2004)MD UCSF, 2004)
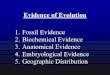
Disease-free survival (months)
Cum
ulativeProp
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 10 20 30 40 50 60 70
P = 0.0003
CR n=20
PR n=104
MR n=30
NC n=8
PD n=3
Tailor Tailor TreatmentTreatment
Biopsies in the Future Should Define Biopsies in the Future Should Define Disease Type, Treatment and Disease Type, Treatment and
Prevention ApproachPrevention Approach

DCIS and the Art of Supporting DCIS and the Art of Supporting Informed Patient DecisionsInformed Patient Decisions
Diagnosis, grade, extent Diagnosis, grade, extent of disease, ageof disease, ageDCIS treatment choices DCIS treatment choices •• Recurrence riskRecurrence risk•• Chance of invasive Chance of invasive
cancercancer•• Chance of cancer in Chance of cancer in
contralateralcontralateral breastbreast
Patient PreferencePatient PreferenceHow important isHow important is•• Keeping your breast?Keeping your breast?•• Minimizing chance of Minimizing chance of
having to deal with having to deal with breast cancer?breast cancer?
•• Avoiding radiation?Avoiding radiation?