Embed Size (px)
Citation preview
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: June 2013
1
Trainee’s Name: _________________________
Band 6 Rotational Training
Programme
Pharmacy Training Pack
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: June 2013
2
Contents Page
Page Number
1. Overview 3
2. Objectives 4-9
3. Links to competency frameworks 10
4. Background preparation 10
5. Experiential learning 10-12
6. Assessment and feedback 12-15
Appendix 1 – Details of individual rotations 16-24
Appendix 2 – Clinical Case Studies 25-31
Appendix 3 – Copies of paperwork for practice based assessments 32-44
Appendix 4 – Feedback on rotation 45
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: June 2013
3
This training pack outlines the following key aspects of the rotational training
programme for band 6 pharmacists working at Wirral University Teaching Hospitals
NHS Foundation Trust (WUTH):
In-house training provided
Details of rotations offered
Competency based assessments used during the rotations
Generic objectives for Band 6 Pharmacists to complete during their time as a
Rotational Pharmacist. Where appropriate there are rotation specific objectives
Band 6 pharmacists at WUTH will undertake a mixture of rotations, each lasting
approximately four months. Due to the time spent as a Band 6 Pharmacist in the
Trust, it is usually not possible to have completed all of the available rotations;
however, by the end of a 2-3 year period a Band 6 Pharmacist will have gained
experience in working in most of the following areas:
Aseptic services
Dispensary (both Arrowe Park and Clatterbridge sites)
Medicines Information
Cardiology
Endocrinology
Gastroenterology
St John’s hospice
Medicine for the elderly (DME)
Rehabilitation wards – e.g. stroke and neurology
Renal
Respiratory
Medical admissions
Surgical admissions
Urology
Orthopaedics
Women’s and children’s
Since this pack is aimed at the Band 6 Pharmacists’ overall development and
performance, they don’t need to have completed this training pack’s objectives
before they are able to work unsupervised on wards. However, if any of the
pharmacists involved in the training or assessment of any band 6 pharmacist have
any concerns over their competence they are to inform the Clinical Services Manager
or the Divisional Lead Pharmacist for Medicine or Surgery as appropriate.
Overview
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: June 2013
4
All band 6 pharmacists will be given a set of generic objectives (which are linked to
the departmental business plan and the Trust’s goals) as part of their individual
review (IR) process (see pages 5-9 for details). In addition, the band 6 pharmacists
are required to identify 3-6 personal objectives for each ward-based area rotation
which they will then agree with the team leader for that rotation. These objectives will
be influenced by the band 6 pharmacists’ previous experience and the common
disease states / management problems that the band 6 pharmacist is likely to
encounter during that rotation (see Appendix 1 for outlines of each ward-based
rotation). The rotations which involve working in medicines information and aseptic
services have their own training packs (which will have their own specific objectives).
Objectives
5
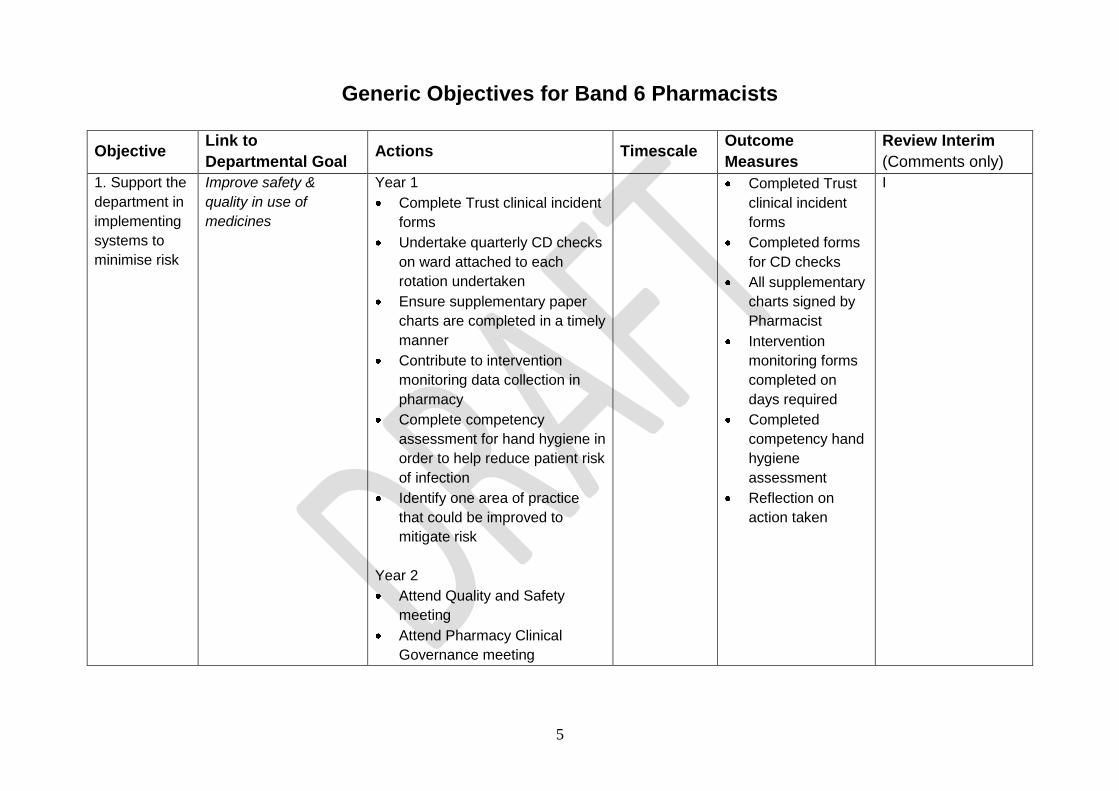
Generic Objectives for Band 6 Pharmacists
Objective Link to
Departmental Goal Actions Timescale
Outcome
Measures
Review Interim
(Comments only)
1. Support the
department in
implementing
systems to
minimise risk
Improve safety &
quality in use of
medicines
Year 1
Complete Trust clinical incident
forms
Undertake quarterly CD checks
on ward attached to each
rotation undertaken
Ensure supplementary paper
charts are completed in a timely
manner
Contribute to intervention
monitoring data collection in
pharmacy
Complete competency
assessment for hand hygiene in
order to help reduce patient risk
of infection
Identify one area of practice
that could be improved to
mitigate risk
Year 2
Attend Quality and Safety
meeting
Attend Pharmacy Clinical
Governance meeting
Completed Trust
clinical incident
forms
Completed forms
for CD checks
All supplementary
charts signed by
Pharmacist
Intervention
monitoring forms
completed on
days required
Completed
competency hand
hygiene
assessment
Reflection on
action taken
I
6
Objective Link to
Departmental Goal Actions Timescale
Outcome
Measures
Review Interim
(Comments only)
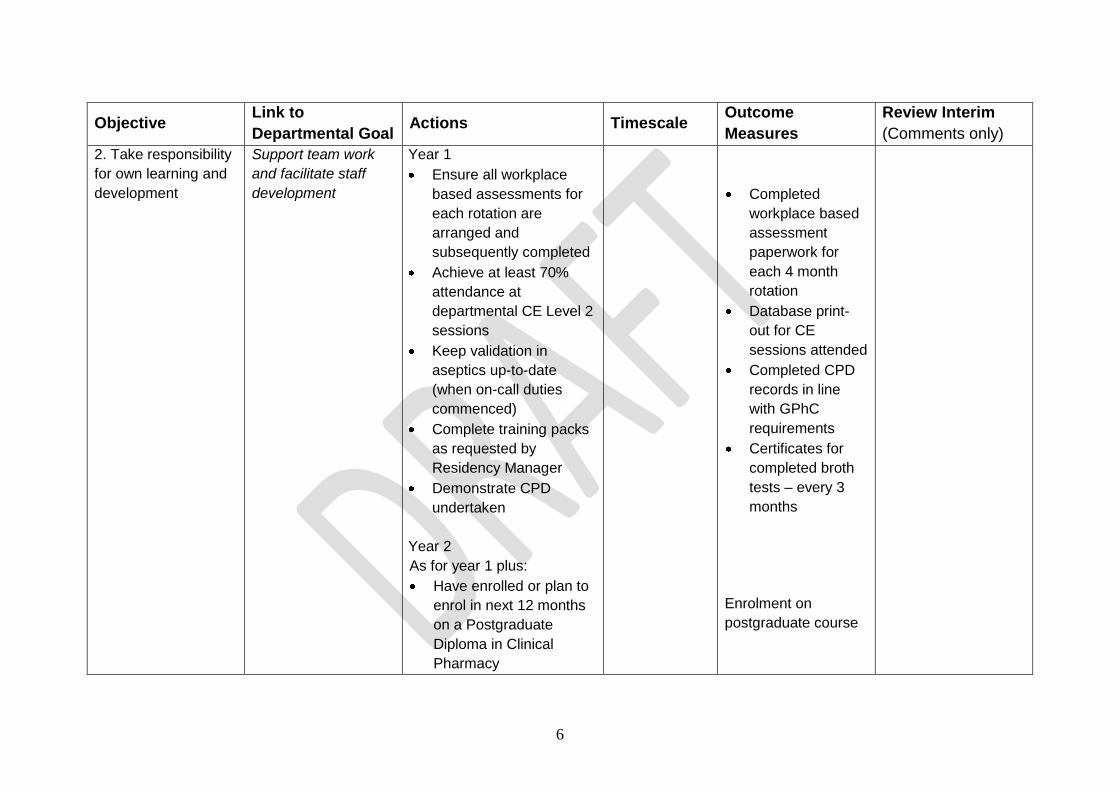
2. Take responsibility
for own learning and
development
Support team work
and facilitate staff
development
Year 1
Ensure all workplace
based assessments for
each rotation are
arranged and
subsequently completed
Achieve at least 70%
attendance at
departmental CE Level 2
sessions
Keep validation in
aseptics up-to-date
(when on-call duties
commenced)
Complete training packs
as requested by
Residency Manager
Demonstrate CPD
undertaken
Year 2
As for year 1 plus:
Have enrolled or plan to
enrol in next 12 months
on a Postgraduate
Diploma in Clinical
Pharmacy
Completed
workplace based
assessment
paperwork for
each 4 month
rotation
Database print-
out for CE
sessions attended
Completed CPD
records in line
with GPhC
requirements
Certificates for
completed broth
tests – every 3
months
Enrolment on
postgraduate course
7
Objective Link to
Departmental Goal Actions Timescale
Outcome
Measures
Review Interim
(Comments only)
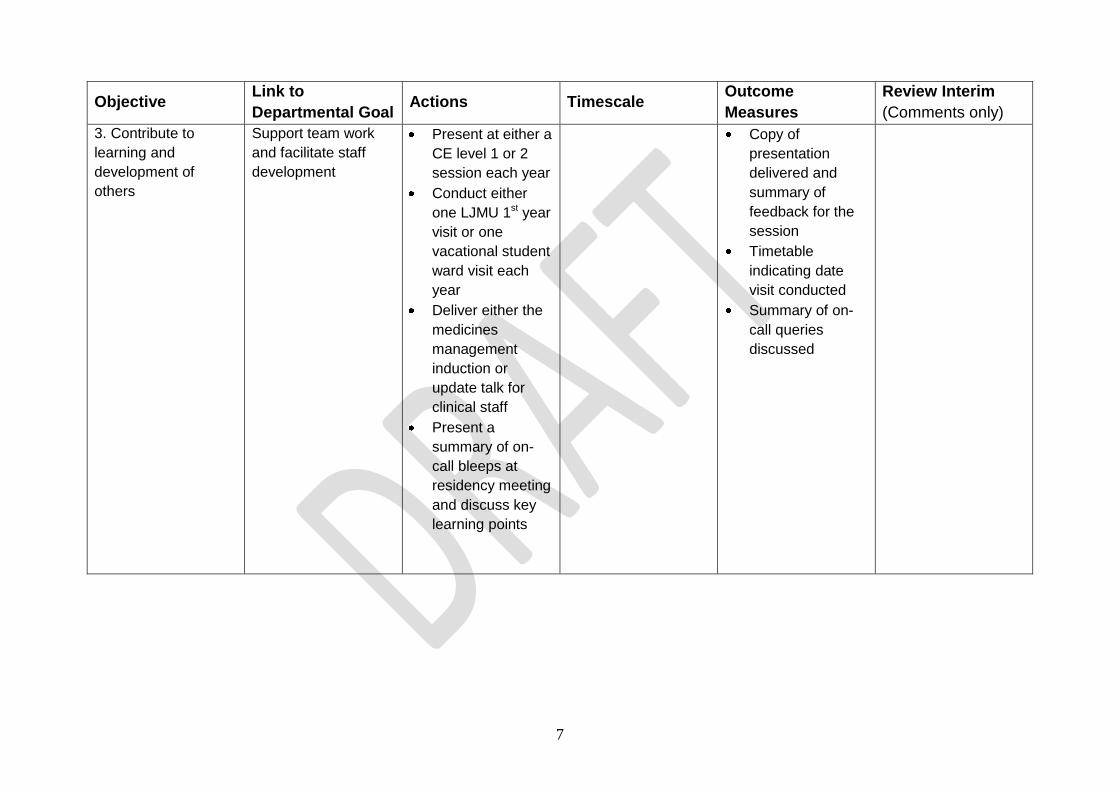
3. Contribute to
learning and
development of
others
Support team work
and facilitate staff
development
Present at either a
CE level 1 or 2
session each year
Conduct either
one LJMU 1st year
visit or one
vacational student
ward visit each
year
Deliver either the
medicines
management
induction or
update talk for
clinical staff
Present a
summary of on-
call bleeps at
residency meeting
and discuss key
learning points
Copy of
presentation
delivered and
summary of
feedback for the
session
Timetable
indicating date
visit conducted
Summary of on-
call queries
discussed
8
Objective Link to
Departmental Goal Actions Timescale
Outcome
Measures
Review Interim
(Comments only)
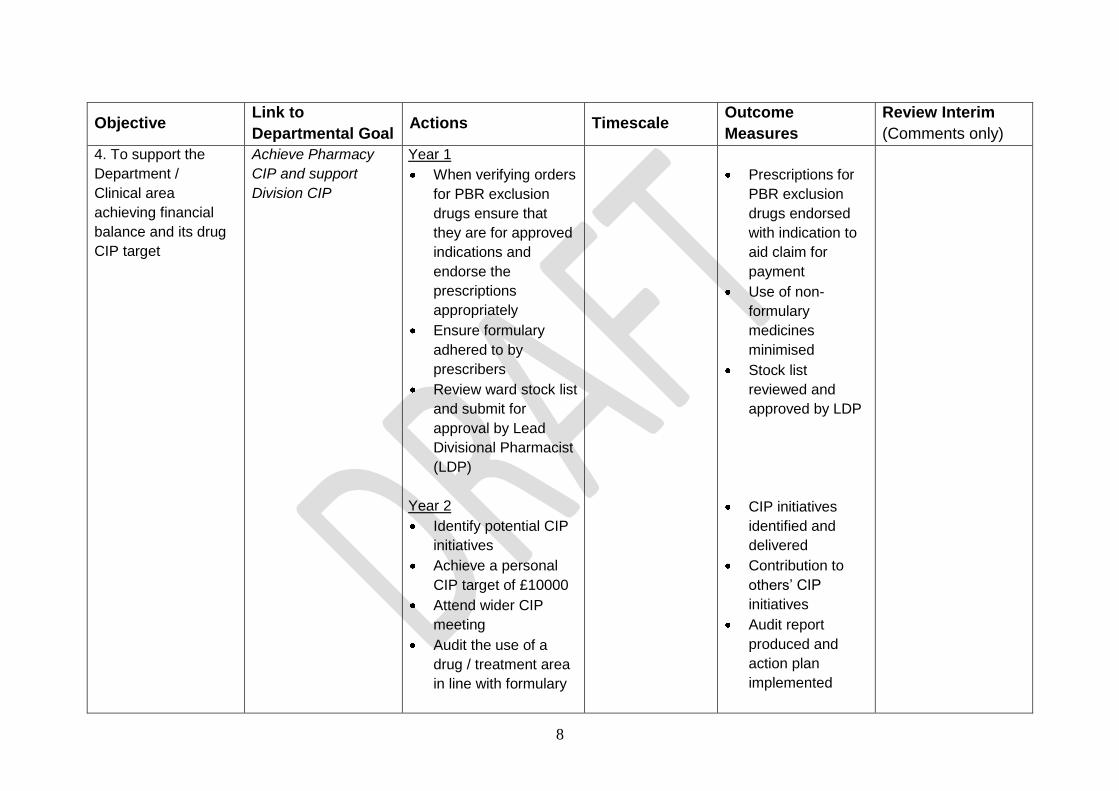
4. To support the
Department /
Clinical area
achieving financial
balance and its drug
CIP target
Achieve Pharmacy
CIP and support
Division CIP
Year 1
When verifying orders
for PBR exclusion
drugs ensure that
they are for approved
indications and
endorse the
prescriptions
appropriately
Ensure formulary
adhered to by
prescribers
Review ward stock list
and submit for
approval by Lead
Divisional Pharmacist
(LDP)
Year 2
Identify potential CIP
initiatives
Achieve a personal
CIP target of £10000
Attend wider CIP
meeting
Audit the use of a
drug / treatment area
in line with formulary
Prescriptions for
PBR exclusion
drugs endorsed
with indication to
aid claim for
payment
Use of non-
formulary
medicines
minimised
Stock list
reviewed and
approved by LDP
CIP initiatives
identified and
delivered
Contribution to
others’ CIP
initiatives
Audit report
produced and
action plan
implemented
9
Objective Link to
Departmental Goal Actions Timescale Outcome Measures
Review Interim
(Comments only)
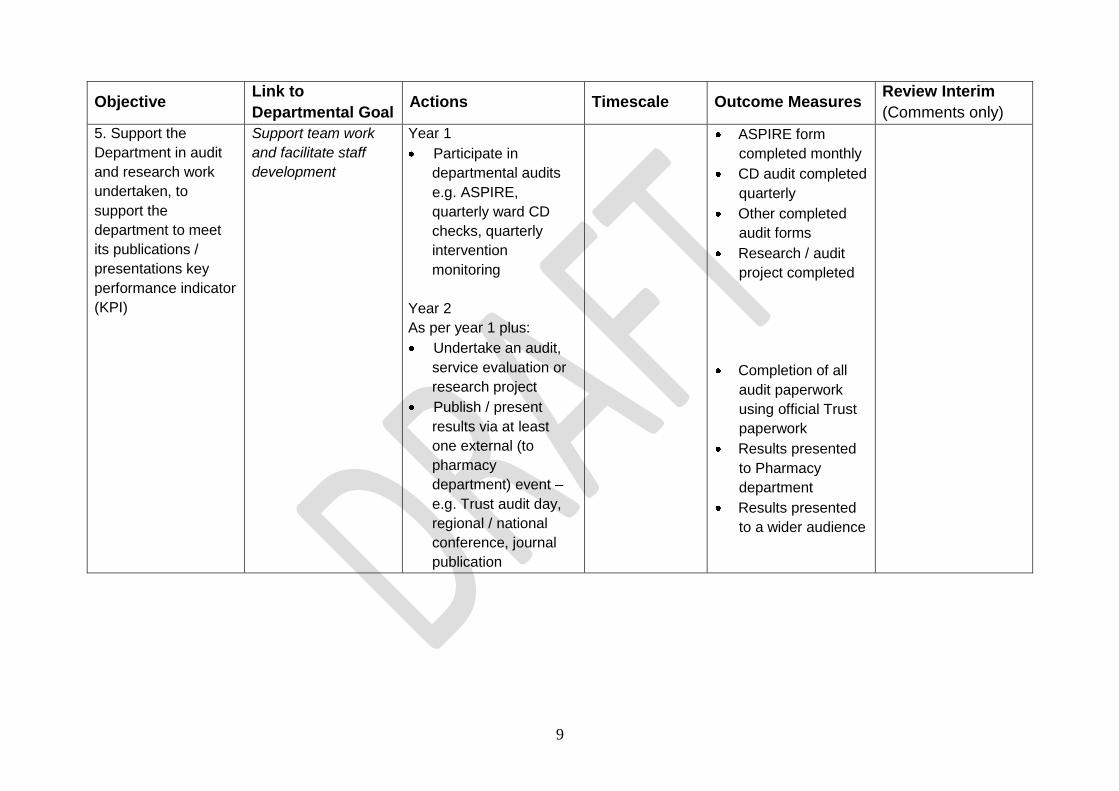
5. Support the
Department in audit
and research work
undertaken, to
support the
department to meet
its publications /
presentations key
performance indicator
(KPI)
Support team work
and facilitate staff
development
Year 1
Participate in
departmental audits
e.g. ASPIRE,
quarterly ward CD
checks, quarterly
intervention
monitoring
Year 2
As per year 1 plus:
Undertake an audit,
service evaluation or
research project
Publish / present
results via at least
one external (to
pharmacy
department) event –
e.g. Trust audit day,
regional / national
conference, journal
publication
ASPIRE form
completed monthly
CD audit completed
quarterly
Other completed
audit forms
Research / audit
project completed
Completion of all
audit paperwork
using official Trust
paperwork
Results presented
to Pharmacy
department
Results presented
to a wider audience
10
The objectives for each of the rotations are linked to the core KSF dimensions and the
competencies listed in the General Level Framework. The competency framework outlined
in this document has been adapted from the General Level Framework (GLF) developed
by the Competency Development and Evaluation Group (CoDeg) in London.
A list of recommended references will be provided for each rotation (see Appendix 1 for
details). The references listed below will be useful throughout the rotational pharmacists’
training.
1. Sexton J, Nickless G, Green C. Pharmaceutical care made easy. Pharmaceutical
Press 2006
2. Royal Pharmaceutical Society of Great Britain. Medicines Optimisation: Helping
patients to make the most of their medicines. May 2013
3. Competency Development and Evaluation Group (CoDEG). General Level Framework
– A Framework for Pharmacist Development in General Pharmacy Practice. 2nd
Edition, October 2007
4. Middleton H, O’Loan L, Varia S. Getting the most from the KSF – how to link it with
CPD. Hospital Pharmacist 2006; 13: 211-214
5. Fenn T. Your KSF development review – how to collect evidence. Hospital
Pharmacist 2007; 14:26-28
A series of case studies (see Appendix 2) have also been written for the rotational
pharmacists to attempt during the first few months of their employment. The case studies
will cover areas such as interpretation of lab tests and screening of prescriptions.
Induction
All rotational pharmacists’ will undertake an intensive induction programme to prepare
them for participation in the residency service. The programme will also include some
training packs and competency assessments to be completed before the band 6
pharmacist is able to perform certain tasks.
Continuing Education Sessions
Continuing education meetings are also held on (at least) a weekly basis during
lunchtimes. Junior pharmacists are required to attend these since they cover a variety of
key topics, including:
CPPE Learning at Lunch modules
Links to Competency Frameworks
Background Preparation
Training / Experiential Learning
11
Updates on clinical areas from specialist pharmacists
Case presentations by diploma students
Audit presentations (including those by diploma students)
Service development initiatives
There is a departmental KPI for attendance at these meetings which is reported to
pharmacy board.
In addition to the aforementioned programme, there are the following additional sessions
organised for band 6 pharmacists during the first few months of their employment:
Medication history taking
Basic guide to laboratory tests
Introduction to microbiology
Antibiotic therapeutic drug monitoring
Problem solving exercises in medicine
Problem solving exercises in surgery
Problem solving in critical care
Organisation of Rotations
Rotational pharmacists will also “learn by doing” during their rotations. To facilitate this
experiential learning, each rotation will include:
General overview of the rotation. The team leader for the rotation (or designated
deputy in their absence) will give a general overview of the rotation (ideally on day 1),
including:
o A general introduction to the ward /area including details of personnel (e.g.
consultants, specialist nurses) working in that area
o References including any SOPs that must be read
Workplace-based assessments (WBAs). The WBAs are formative in nature (i.e.
don’t have a mark attached to them) and are used to assess competence and provide
feedback to aid personal development. It is the responsibility of the Band 6 Pharmacist
to arrange dates for the various assessments with the relevant personnel. Further
details of the WBAs listed below can be found on pages 12 - .
o Mini clinical evaluation exercise (mini–CEX). This will be conducted by the
Lead Pharmacist for Education and Training
o General ward visit. This will be conducted by the Lead Pharmacist for
Education and Training
o Case Based Discussion (CBD). This will be conducted by the Team Leader
(or nominated deputy) for the rotation
o Record of In-service Training Assessment (RITA). This will be conducted by
the Team Leader (or nominated deputy) for the rotation
Meetings with team leader for the rotation or Lead Pharmacist Education and
training. Additional ward visits / meetings at other times during the rotation may also
be arranged and this is encouraged. The format of such meetings will depend on both
12
the rotation and Activities undertaken during each ward visit should be documented in
the activities diary (see Appendix ).
WBAs are used during the rotations to both assess the band 6 pharmacist’s level of
competence and as a development tool through identifying learning needs. The practice
based assessments used are:
Mini-Clinical Evaluation Exercise (Mini-CEX)
General Ward Visit Summary
Case Based Discussion (CBD)
Record of In-service Training Assessment (RITA)
Copies of the paperwork for these WBAs can be found in Appendix 3. When judging the
complexity of the cases used for the Mini-CEXs and CBDs, consider:
Whether the patient has multiple co-morbidities?
Whether the patient subject to polypharmacy?
Whether the patient has altered drug handling?
Whether the patient is prescribed unusual (e.g. unlicensed) medicines?
Videos demonstrating these assessment tools, which have been produced by the Joint
Programmes Board, are available at: http://www.jpbsoutheast.org/assessment-tools/jpb-
assessment-tools-dvd/
Mini-Clinical Evaluation Exercise (Mini-CEX)
The Mini-CEX involves observation and assessment of the band 6 pharmacist in their day-
to-day practice. It will be used to assess their performance against the GLF competencies
of delivery of patient care and problem solving. The Mini-CEX is intended as a 15-20
minute snapshot of a pharmacist / patient or pharmacist / doctor or even pharmacist /
patient / doctor interaction. Whilst the mini-CEX is designed to be used in the ward
environment assessing the band 6 pharmacist prospectively providing pharmaceutical care
for new patients on their wards, it may also be conducted in the dispensary or during a
rotation in medicines information (by observing them dealing with a telephone query).
Each mini-CEX should represent a different clinical problem which will depend on the
rotation being undertaken. The suggested process for conducting a Mini-CEX is:
The band 6 pharmacist and assessor will agree the time and date of the assessment
The band 6 pharmacist will identify up to THREE patients that are new to them in
advance of the ward visit and tell assessor the name and location of these patients
The assessor will then select ONE of these patients for the Mini-CEX
The assessor will be looking at the band 6 pharmacist’s ability to prospectively deliver
pharmaceutical care for the patient selected (from the initial consultation with the
Assessment
13
patient and information retrieval from the case notes, to problem identification and
resolution if feasible)
The assessor should position themselves carefully (to avoid being intrusive)
During the Mini-CEX, the assessor should question the junior pharmacist at appropriate
times to ascertain how they are prioritising problems identified. However, interjections
and interruptions should be kept to a minimum. Whilst clinical knowledge is assessed
to some degree during a Mini-CEX, the band 6 pharmacist should not be subjected to
intensive questioning by the assessor
Once the assessment is over, the assessor should complete the feedback form in the
absence of the band 6 pharmacist. The assessor and the band 6 pharmacist should
meet to discuss the results (ideally within an hour of the observation) and identify
agreed strengths, areas for development and an action plan following each encounter.
The action plan should include objectives for the next accompanied ward visit or
assessment.
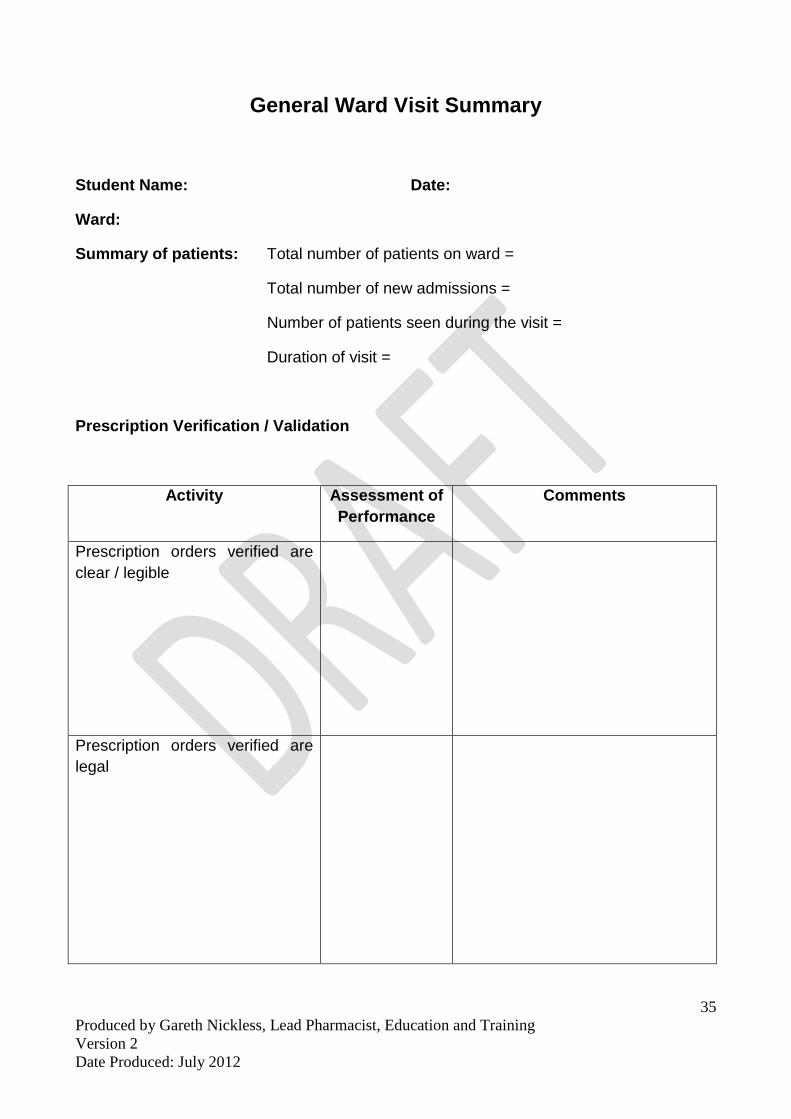
General Ward Visit Summary The principle behind this ward visit is to gain a better overview of how a band 6 pharmacist
is coping with their workload at ward level and assess some of the competencies that are
not included in the Mini-CEX and CBD proformas. The assessor’s role will be mainly
observational with questioning of the band 6 pharmacist tailored to evaluating their
approach on the ward rather than assessing clinical knowledge.
The activities will be observed for a number of patients seen during the ward visit and the
tutor will form an overall impression of how the student performed for each activity. No
mark is attached to this visit, but the following rating scale will be used to assess overall
performance:
Rarely: 0-24%
Sometimes: 25-50%
Usually: 51-84%
Consistently: 85-100%
Not applicable / unable to observe on this occasion
It is envisaged that a visit will last approximately an hour to allow observations for several
patients. Practicalities of the visit:
The assessor will select patients for review at random
For each patient seen the assessor will ask the band 6 pharmacist to provide a brief
overview of the patient’s priority problems and any input they have had
For each patient seen the assessor will review the prescription chart (or electronic
equivalent) to determine:
o The number of items verified
o Whether the items verified are clear, legal and safe
o Appropriate endorsements to the prescription order have been made in line with
departmental policy / standards
14
For items prescribed > 24hours ago that have not been verified, the band 6 pharmacist
will be questioned to ascertain the possible reason(s) for this
The band 6 pharmacist will be asked whether there are any issues for follow up to
determine how they prioritise tasks / manage workload
Where the band 6 pharmacist has had input (including medicines reconciliation and
counseling) or offered advice, the assessor will review the patient’s case notes to
determine whether the documentation of their actions complies with departmental
policy
Case Based Discussions (CBD)
Case based discussions are designed to assess clinical decision-making and the
application or use of pharmaceutical knowledge in the care of the band 6 pharmacist’s own
patients. In essence, it involves a senior pharmacist questioning the band 6 pharmacist
about the care they have provided for a patient, allowing the senior pharmacist to explore
the band 6 pharmacist’s understanding of specific issues (from pharmacology and
pathophysiology to monitoring and counselling). It also enables the discussion of the
ethical and legal framework of practice (when appropriate), and in all instances, it allows
the band 6 pharmacist to discuss why they acted as they did.
Each CBD should represent a different clinical problem which will depend on the rotation
being undertaken. The suggested process for conducting a CBD is:
The band 6 pharmacist will select three case records from patients they have recently
been caring for (week to be penciled in diary at start of rotation, exact date/time to be
confirmed at least 1 week prior to assessment).
The designated senior pharmacist will select one of these for the case-based
discussion session. The assessment will preferably be undertaken at ward level, with
follow-up discussion in pharmacy if required.
The discussion should focus around the 5 question areas listed on the form in
Appendix 3.
The whole assessment should take no longer than 30 minutes including feedback
and completion of the assessment form.
Immediate feedback will be provided after each encounter by the designated senior
pharmacist.
In order to maximise the educational impact of using CBD the band 6 pharmacist and
designated senior pharmacist will need to identify agreed strengths, areas for
development and an action plan for each encounter. The band 6 pharmacist is
expected to follow-up on any action plan agreed.
Record of In-service Training Assessment (RITA)
The RITA will be undertaken by the designated senior pharmacist towards the end of each
four month rotation and should take approximately 30-45 minutes to complete. It is a
15
formal meeting between the band 6 pharmacist and the designated senior pharmacist and
allows for a review of the band 6 pharmacist’s progress, highlighting:
Achievements during the rotation (including progress with objectives)
Areas to concentrate on during future rotations
Problems or difficulties the band 6 pharmacist may be experiencing
Portfolios
Each new member of staff is issued with a portfolio on behalf of the Trust’s Learning and
Development directorate. The evidence contained in this portfolio should be used during
the individual review process, to demonstrate achievement of the GLF competencies and
included in the portfolios for the Liverpool John Moores University Postgraduate Diploma
in Clinical Pharmacy.
Minimum Portfolio Evidence Requirements
Completed clinical checking test
Completed accuracy checking test
Completed kinetics competency log
Certificate of completed broth test every 3 months since date of commencing on-call
duties
Mini-CEXs – minimum of two at Foundation gateway, three for subsequent annual IRs
General ward visit summary - minimum of two at Foundation gateway, three for
subsequent annual IRs
Case based discussions – minimum of two at Foundation gateway, three for
subsequent annual IRs
RITAs - 2 at Foundation gateway, 3 for subsequent annual IRs
Quarterly CDs check forms – one for each rotation (containing ward commitments)
completed
Interventions log
Incident forms x 10
E&T database printout of CE sessions attended and delivered
CPD records using GPhC format x 9
Certificates of completion for:
1. E-BMJ Packs
1. Starting patients on anticoagulants – how to do it
2. Maintaining patients on anticoagulants – how to do it
3. Injectable medicines
2. NHS diabetes e-learning – The safe use of insulin
3. Information governance training (completed every 12 months)
4. Safeguarding children (completed every 3 years)
16
Respiratory Rotation
Overview
This rotation will involve provision of a ward pharmacy service to ward 38. Ward 38 has
38 beds organised as follows:
12 Lung Support Unit (LSU) beds
1 sleep study room – often empty. When patients undertake a sleep study they arrive
in the evening and leave the next morning. No TTH is produced for these patients
7 side rooms
18 “general” beds divided between 4 bays
Therapeutic Problems
By the end of this rotation you should have encountered patients with the following
conditions:
o Asthma
o COPD
o Community acquired pneumonia
o Hospital acquired pneumonia
o Bronchiectasis
o Pleural effusions
o Pulmonary emboli
o Type 2 respiratory failure
Depending on the patients admitted to the ward, you may also gain experience in the
management of:
Tuberculosis
Environmental mycobacterium infections
Pulmonary fibrosis
Directed Reading
BTS asthma guidelines (current edition)
NICE COPD guidelines
BTS CAP guidelines
Respiratory section of medicines guide
Respiratory section of antimicrobial formulary
Appendix 1 – Details of Individual Rotations
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
17
Medicine for the Elderly (DME) rotation
Overview
This rotation will involve provision of a ward pharmacy service to a selection of DME wards
which are organised as follows:
Ward 20 – 20 rehab and 10 acute medical beds
Ward 21 – 31 bed acute male ward
Ward 22 – 12 bed OPSS unit (older persons short-stay ward), 2 side rooms used
for OPRA clinic (outpatients) 16 mixed male and female acute beds.
Ward 23 – 12 acute stroke beds and 17 step down beds.
Ward 24 – 30 bed acute female ward
Ward 26 – 12 acute DME beds (rest of ward is endocrine)
Ward 36 – Rehabilitation ward
Therapeutic Problems
DME patients are likely to have multiple comorbidities and multiple pharmaceutical
problems. By the end of this rotation you are likely to have encountered patients with the
following conditions:
Community acquired pneumonia
Hospital acquired pneumonia
Dementia
Falls
Stroke
Parkinson’s disease
Renal impairment
Heart failure
Acute coronary syndrome
Atrial fibrillation
GI bleeds
Diabetes
Leg ulcers and other skin conditions
COPD
Nil by mouth patients
Polypharmacy
Compliance issues
Directed Reading
The reading used will depend on the patients seen; there are a variety of conditions that
will be covered in DME. All rotational pharmacists should read:
Respiratory section of antimicrobial formulary
WUTH Dementia Care guideline
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
18
NICE Clinical Guideline – Falls
WUTH Falls Pharmaceutical Care standard
Parkinson’s Disease – Clinical Features and Diagnosis. Clinical Pharmacist. December
2011
Parkinson’s Disease – Management. Clinical Pharmacist. December 2011
WUTH Parkinson’s guideline
WUTH ACS and AF pathways
NICE bites – Heart failure
WUTH Compliance aid guidelines
“Time is Brain” – WUTH stroke pathway
Formulary / NICE guidance for other conditions.
If covering ward 23, must read:
Stroke classification and diagnosis. Clinical Pharmacist. 2011; 3: 200-202.
Stroke acute management. Clinical Pharmacist. 2011; 3: 205-208.
Stroke long-term management. Clinical Pharmacist. 2011; 3: 209-212.
NICE TA 122. Alteplase for the treatment of acute ischaemic stroke.
NICE TA 210 – Clopidogrel and modified release dipyridamole for the prevention of
occlusive vascular events.
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
19
Renal rotation
Overview
This rotation will involve provision of a ward pharmacy service to the renal directorate.
The renal directorate is set out as follows:
10 acute inpatient renal beds APH
Haemodialysis unit APH (3 bays of 6 beds and 1 side room)
Haemodialysis unit CGH
There are approximately 80 patients having haemodialysis on the haemodialysis unit at
APH. These consist of outpatients who regularly dialyse at APH, and inpatients who have
been admitted acutely unwell. These inpatients usually:
Have established ESRF and are dialysis dependent and may normally dialyse at
another dialysis unit but are currently admitted at APH with an acute illness.
Have had deterioration in renal function and have been newly initiated on
haemodialysis as an inpatient.
Therapeutic Problems
By the end of this rotation you should have encountered patients with the following
conditions:
AKI of various causality
CKD3-5
ESRF requiring haemodialysis
Secondary hyperparathyroidism
Anaemia associated with CKD
Depending on the patients admitted at time of admission, you may also gain experience in
the management of:
Renal transplant
ESRF requiring peritoneal dialysis
Vasculitis and SLE
Activities
Ward Round
Patient reviews with lead pharmacist
Ward based assessments
Shadow renal MDT colleagues – To be arranged by rotating pharmacist if rota
allows

Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
20
Directed Reading
Shaw S, Coleman A, Selby N. Acute kidney injury: diagnosis, staging and
prevention. Clinical Pharmacist 2012; 4:98.
Shaw S, Morlidge C, Ashley A. Acute kidney injury: management. Clinical
Pharmacist 2012; 4:103.
CPPE Renal Focal Point. Access at: http://www.cppe.ac.uk
Brown C, Prescribing principles for patients with chronic kidney disease. Pharmacy
in Practice 2008; 18(1):23-27. Available at: http://www.pharmacyinpractice.com
Wood S, Calculating GFR is crucial when determining drug dosage requirements in
reduced renal function. Pharmacy in Practice 2008; 18(1):19-22. Available at:
http://www.pharmacyinpractice.com
Brown C, Pharmacological management of chronic kidney disease and its
complications. Pharmacy in Practice 2009; 19(1):22-30. Available at:
http://www.pharmacyinpractice.com
Levy J, Pusey C, Singh, A. Fast Facts: Renal Disorders Health Press Ltd; 2006.
http://lib.myilibrary.com/ProductDetail.aspx?id=81430 [accessed 09/04/13]
O'Callaghan, C. The Renal System at a Glance 3rd Edition
Wiley-Blackwell; 2009. http://lib.myilibrary.com/ProductDetail.aspx?id=237096
[accessed 09/04/13]
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
21
Cardiology Rotation
Overview
This rotation will involve provision of a ward pharmacy service to a selection of cardiology
wards which are organised as follows:
Ward 32 – General cardiology ward
Ward 33 – Beds 1-10 and 23-29 Heart failure unit
HAC – Heart Assessment Centre – located beds 11-22 on ward 33.
CCU – Coronary Care Unit
Cardiology Day Suite – Located next to the catheter lab on the 3rd floor
Therapeutic Problems
Cardiology patients are likely to have multiple comorbidities and multiple pharmaceutical
problems. By the end of this rotation you are likely to have encountered patients with the
following cardiac conditions:
o Acute Coronary Syndrome
o Heart failure
o Atrial fibrillation (acute and chronic)
o Complex arrhythmias
o Bradycardia
o Ischaemic heart disease
o Endocarditis
o Resistant hypertension
Directed Reading
The reading used will depend on the patients seen; there are a variety of conditions that
will be covered in cardiology. All rotational pharmacists should read:
General
Cardiology section of the medicines Guide which will cover local Wirral guidelines:
Chest Pain Pathway (including ticagrelor and fondaparinux prescribing guidelines)
Atrial Fibrillation Pathway
Heart Failure Guidelines
Hypertension
Hypercholesterolemia
New Oral Anticoagulant Prescribing guideline for stroke prevention in AF
Additional Reading
Hypertension
o Hypertension: Clinical management of primary hypertension in adults CG127
Published August 2011
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
22
Heart Failure
o Sani M. Heart failure – Clinical Features and Diagnosis. Clinical Pharmacist
2009; 1: 113-119
o Williams H. Heart failure – Management. Clinical Pharmacist 2009; 1: 120-125
o Management of chronic heart failure in adults in primary and secondary care.
Nice Clinical Guideline 108 Aug 2010.
o ESC Guidelines for the diagnosis and treatment of acute and chronic heart
failure 2012
o NICE Technical Appraisal for Ivabradine for treating chronic heart failure
Myocardial Infarction
o Worrall A. Acute Coronary Syndromes – Assessment and Interventions. Hospital
Pharmacist 2007; 14: 285-292
o Fletcher G, Worrall A. Acute Coronary Syndromes – Pharmacological
Treatment. Hospital Pharmacist 2007; 14: 295-299
o MI: Secondary prevention. Nice Clinical Guideline No48 2007
o Hyperglycaemia in acute coronary syndromes: Management of hyperglycaemia
in acute coronary syndromes Nice Clinical Guideline 130 October 2011.
o NICE Technical Appraisal for ticagrelor in acute coronary syndrome
Atrial Fibrillation
o The Management of Atrial Fibrillation. NICE Clinical Guideline No 36 2006
o NICE Technical Appraisals for dabigatran, apixaban and rivaroxaban for stroke
prevention in atrial fibrillation.
Endocarditis
o Guidelines for the diagnosis and antibiotic treatment of endocarditis in adults: a
report of the Working Party of the British Society for Antimicrobial Chemotherapy
2012 – available at britishinfection.org
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
23
Haematology Rotation
Overview
This rotation will involve provision of a ward pharmacy service to ward 30 and the
Haematology Day Ward. Ward 30 has 22 single rooms used for the following specialities:
Haematology
Endocrinology
General Medicine
Rheumatology
The number of patients admitted for each speciality is not fixed and may change week-by-
week.
Therapeutic Problems
By the end of this rotation you should have encountered patients with the following
conditions:
Lymphoma
Myeloma
Leukaemia
Depending on the patients admitted to the ward, you may also gain experience in the
management of:
Complications of Chemotherapy / Oncological Emergencies
o Neutropenic Sepsis
o Chemotherapy induced Nausea and Vomiting
o Chemotherapy induced diarrhoea
o Superior Vena Cava Obstruction
o Spinal Cord Compression
o Tumour Lysis Syndrome
Idiopathic Thrombocytopenic Purpura
Activities
Ward Round
Patient reviews with lead pharmacist
Ward based assessments
Complete competency assessment to clinically verify SACT prescriptions
Shadow haematology MDT colleagues – to be arranged by rotating pharmacist if rota
allows
Directed Reading
ABC of Clinical Haematology (book available in Pharmacy)
BOPA E-Learning Website
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
24
Surgical Rotation
Overview
This rotation will involve provision of pharmaceutical care to patients admitted to the
surgical wards, namely:
SAU – surgical admissions
Ward 10, 11 (+ Trauma) and 12 – orthopaedics
Ward 14 - urology
Ward 16 – special surgery
Ward 17 – colorectal
Ward 18 - vascular
Therapeutic Problems
By the end of this rotation you should have encountered patients with the following
management problems:
Thromboprophylaxis
Prevention of surgical site infection
Medicines requiring discontinuation in the peri-operative period
Post-operative pain
Post-operative nausea and vomiting
Post-operative constipation
Recommended Reading
1. NICE-venous thromboembolism, reducing the risk.
2. WUTH Antimicrobial Formulary – surgery section
3. WUTH Clinical Guidance - Pain management
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
25
These case studies aim to develop some of the core skills and knowledge required for the provision of pharmaceutical care to patients and provides on-going education as a bridge to starting a clinical diploma. It consists of some small case studies and prescription reviews to be completed by the rotational pharmacist and discussed with their line manager. 1. Laboratory tests For each patient described in this section:
Comment briefly on the blood results (high, low, normal)
Give a possible explanation for the changes observed
Patient 1 Male, aged 52 years old PC Lethargy and weight gain PMH Bipolar Disorder IHD DH Priadel 600mg ON Atenolol 50mg OD Aspirin 75mg OD Simvastatin 40mg ON Blds U&Es (NAD)
TSH 22.3 (0.5-5.5)
Patient 2 Female, aged 72 years PMH Heart failure DH Bumetanide 3mg om, 2mg at lunchtime
Metolazone 5mg om Spironolactone 50mg om UE K+ 6.4mmol/L
Na + 121mmol/L Creatinine 214 micromoles/L Urea 38.3mmol/L
Patient 3 Male 59 years old PC Jaundice and abdominal swelling SH Drinks 3 litres of strong cider per day U&Es Na = 129 mmol/L
Bili 45 µmol/L Gamma GT 200 IU/L ALP 178 IU/L ALT 34 IU/L
Appendix 2 – Clinical Case Studies
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
26
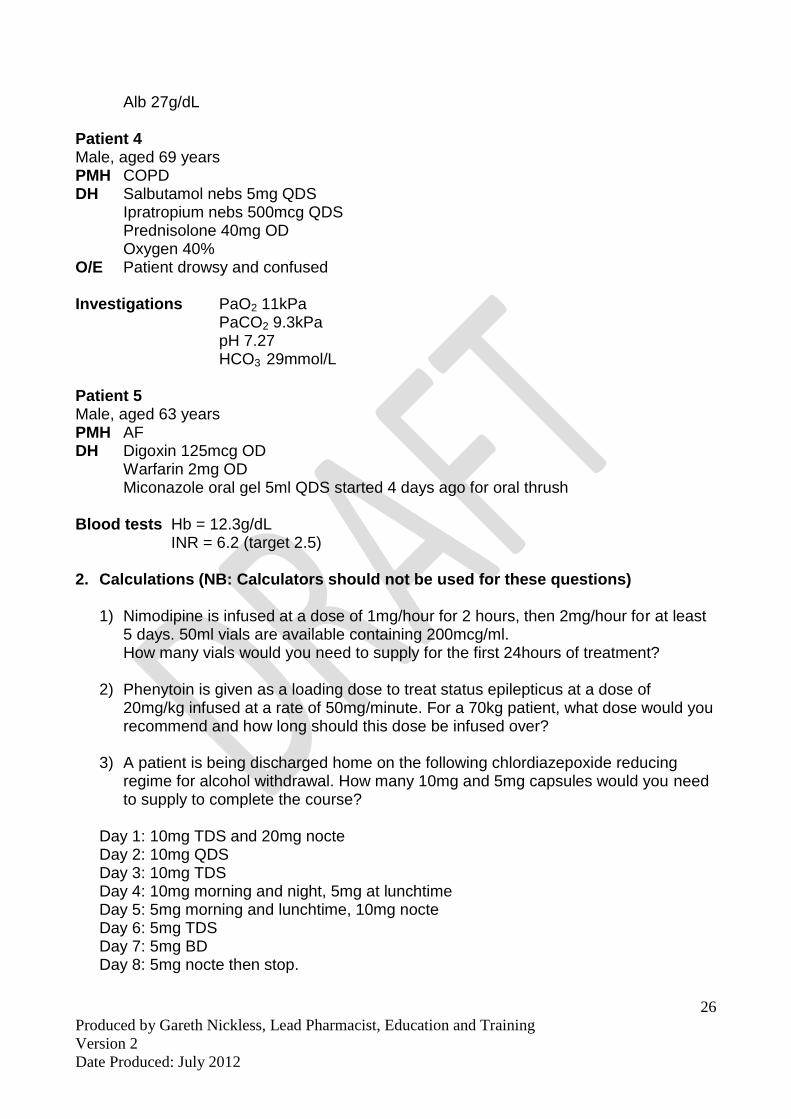
Alb 27g/dL Patient 4 Male, aged 69 years PMH COPD DH Salbutamol nebs 5mg QDS Ipratropium nebs 500mcg QDS Prednisolone 40mg OD Oxygen 40% O/E Patient drowsy and confused Investigations PaO2 11kPa PaCO2 9.3kPa pH 7.27 HCO3 29mmol/L Patient 5 Male, aged 63 years PMH AF DH Digoxin 125mcg OD Warfarin 2mg OD Miconazole oral gel 5ml QDS started 4 days ago for oral thrush Blood tests Hb = 12.3g/dL INR = 6.2 (target 2.5) 2. Calculations (NB: Calculators should not be used for these questions)
1) Nimodipine is infused at a dose of 1mg/hour for 2 hours, then 2mg/hour for at least 5 days. 50ml vials are available containing 200mcg/ml. How many vials would you need to supply for the first 24hours of treatment?
2) Phenytoin is given as a loading dose to treat status epilepticus at a dose of 20mg/kg infused at a rate of 50mg/minute. For a 70kg patient, what dose would you recommend and how long should this dose be infused over?
3) A patient is being discharged home on the following chlordiazepoxide reducing regime for alcohol withdrawal. How many 10mg and 5mg capsules would you need to supply to complete the course?
Day 1: 10mg TDS and 20mg nocte Day 2: 10mg QDS Day 3: 10mg TDS Day 4: 10mg morning and night, 5mg at lunchtime Day 5: 5mg morning and lunchtime, 10mg nocte Day 6: 5mg TDS Day 7: 5mg BD Day 8: 5mg nocte then stop.
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
27
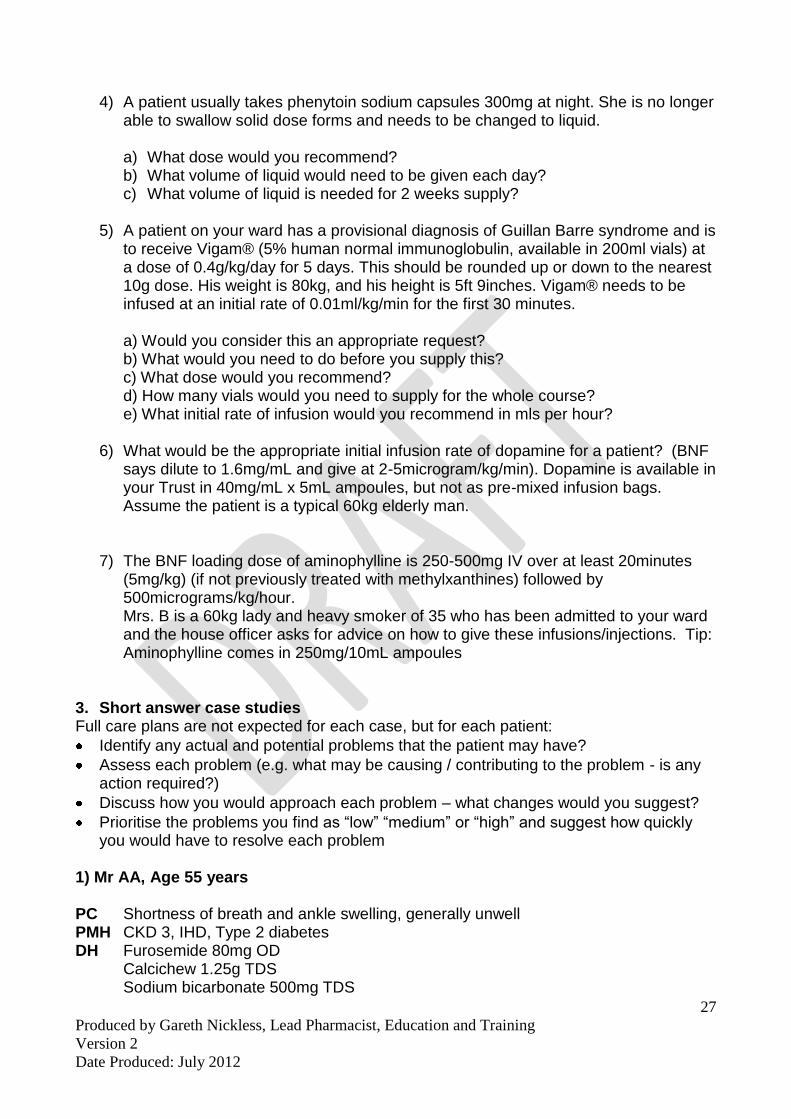
4) A patient usually takes phenytoin sodium capsules 300mg at night. She is no longer able to swallow solid dose forms and needs to be changed to liquid.
a) What dose would you recommend? b) What volume of liquid would need to be given each day? c) What volume of liquid is needed for 2 weeks supply?
5) A patient on your ward has a provisional diagnosis of Guillan Barre syndrome and is
to receive Vigam® (5% human normal immunoglobulin, available in 200ml vials) at a dose of 0.4g/kg/day for 5 days. This should be rounded up or down to the nearest 10g dose. His weight is 80kg, and his height is 5ft 9inches. Vigam® needs to be infused at an initial rate of 0.01ml/kg/min for the first 30 minutes.
a) Would you consider this an appropriate request? b) What would you need to do before you supply this? c) What dose would you recommend? d) How many vials would you need to supply for the whole course? e) What initial rate of infusion would you recommend in mls per hour?
6) What would be the appropriate initial infusion rate of dopamine for a patient? (BNF
says dilute to 1.6mg/mL and give at 2-5microgram/kg/min). Dopamine is available in your Trust in 40mg/mL x 5mL ampoules, but not as pre-mixed infusion bags. Assume the patient is a typical 60kg elderly man.
7) The BNF loading dose of aminophylline is 250-500mg IV over at least 20minutes (5mg/kg) (if not previously treated with methylxanthines) followed by 500micrograms/kg/hour. Mrs. B is a 60kg lady and heavy smoker of 35 who has been admitted to your ward and the house officer asks for advice on how to give these infusions/injections. Tip: Aminophylline comes in 250mg/10mL ampoules
3. Short answer case studies Full care plans are not expected for each case, but for each patient:
Identify any actual and potential problems that the patient may have?
Assess each problem (e.g. what may be causing / contributing to the problem - is any action required?)
Discuss how you would approach each problem – what changes would you suggest?
Prioritise the problems you find as “low” “medium” or “high” and suggest how quickly you would have to resolve each problem
1) Mr AA, Age 55 years PC Shortness of breath and ankle swelling, generally unwell PMH CKD 3, IHD, Type 2 diabetes DH Furosemide 80mg OD Calcichew 1.25g TDS Sodium bicarbonate 500mg TDS
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
28
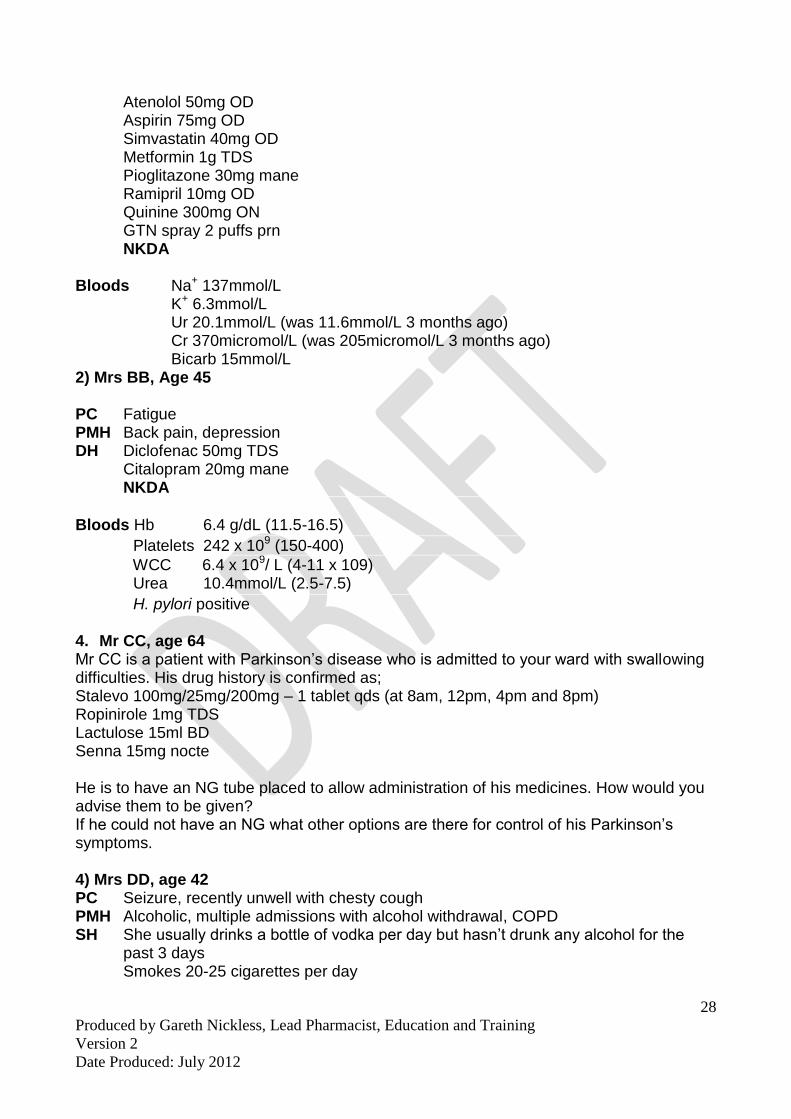
Atenolol 50mg OD Aspirin 75mg OD Simvastatin 40mg OD Metformin 1g TDS Pioglitazone 30mg mane Ramipril 10mg OD Quinine 300mg ON GTN spray 2 puffs prn
NKDA Bloods Na+ 137mmol/L
K+ 6.3mmol/L Ur 20.1mmol/L (was 11.6mmol/L 3 months ago) Cr 370micromol/L (was 205micromol/L 3 months ago) Bicarb 15mmol/L
2) Mrs BB, Age 45 PC Fatigue PMH Back pain, depression DH Diclofenac 50mg TDS Citalopram 20mg mane NKDA
Bloods Hb 6.4 g/dL (11.5-16.5)
Platelets 242 x 109 (150-400)
WCC 6.4 x 109/ L (4-11 x 109) Urea 10.4mmol/L (2.5-7.5)
H. pylori positive 4. Mr CC, age 64 Mr CC is a patient with Parkinson’s disease who is admitted to your ward with swallowing difficulties. His drug history is confirmed as; Stalevo 100mg/25mg/200mg – 1 tablet qds (at 8am, 12pm, 4pm and 8pm) Ropinirole 1mg TDS Lactulose 15ml BD Senna 15mg nocte He is to have an NG tube placed to allow administration of his medicines. How would you advise them to be given? If he could not have an NG what other options are there for control of his Parkinson’s symptoms. 4) Mrs DD, age 42 PC Seizure, recently unwell with chesty cough PMH Alcoholic, multiple admissions with alcohol withdrawal, COPD SH She usually drinks a bottle of vodka per day but hasn’t drunk any alcohol for the
past 3 days Smokes 20-25 cigarettes per day
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
29
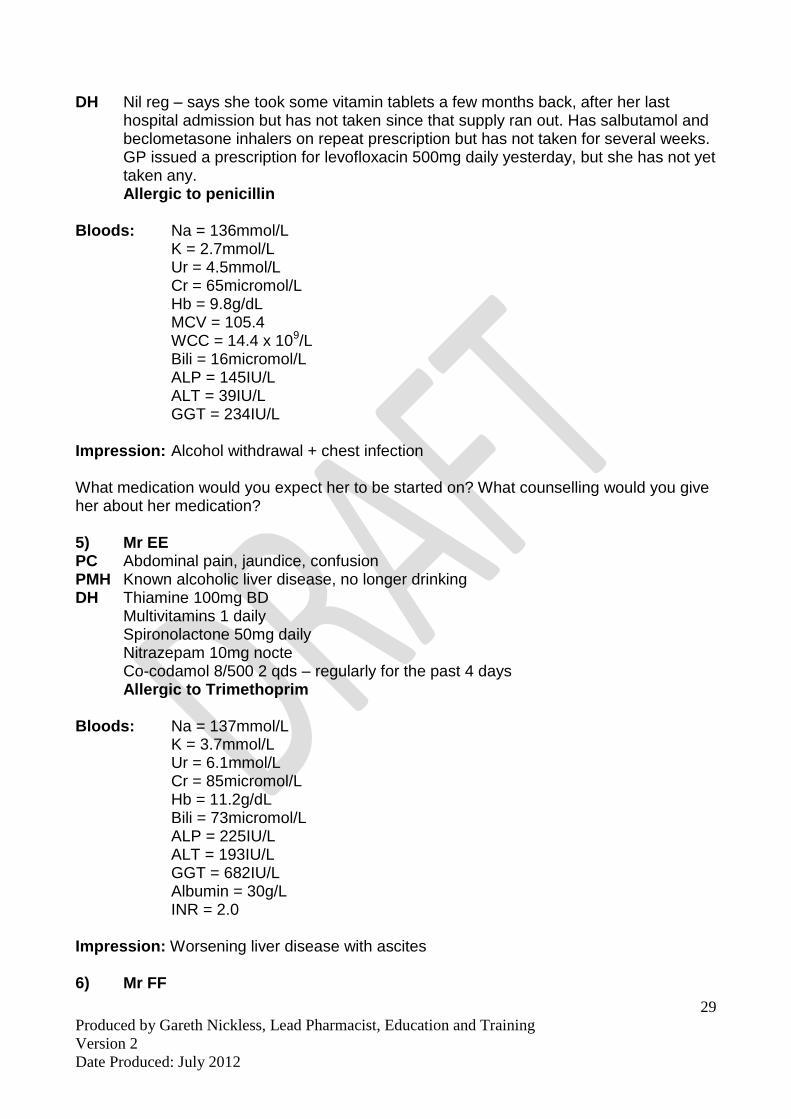
DH Nil reg – says she took some vitamin tablets a few months back, after her last hospital admission but has not taken since that supply ran out. Has salbutamol and beclometasone inhalers on repeat prescription but has not taken for several weeks.
GP issued a prescription for levofloxacin 500mg daily yesterday, but she has not yet taken any. Allergic to penicillin
Bloods: Na = 136mmol/L
K = 2.7mmol/L Ur = 4.5mmol/L Cr = 65micromol/L Hb = 9.8g/dL MCV = 105.4 WCC = 14.4 x 109/L Bili = 16micromol/L ALP = 145IU/L ALT = 39IU/L GGT = 234IU/L
Impression: Alcohol withdrawal + chest infection What medication would you expect her to be started on? What counselling would you give her about her medication? 5) Mr EE PC Abdominal pain, jaundice, confusion PMH Known alcoholic liver disease, no longer drinking DH Thiamine 100mg BD Multivitamins 1 daily Spironolactone 50mg daily Nitrazepam 10mg nocte Co-codamol 8/500 2 qds – regularly for the past 4 days
Allergic to Trimethoprim Bloods: Na = 137mmol/L
K = 3.7mmol/L Ur = 6.1mmol/L Cr = 85micromol/L Hb = 11.2g/dL Bili = 73micromol/L ALP = 225IU/L ALT = 193IU/L GGT = 682IU/L Albumin = 30g/L INR = 2.0
Impression: Worsening liver disease with ascites 6) Mr FF
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
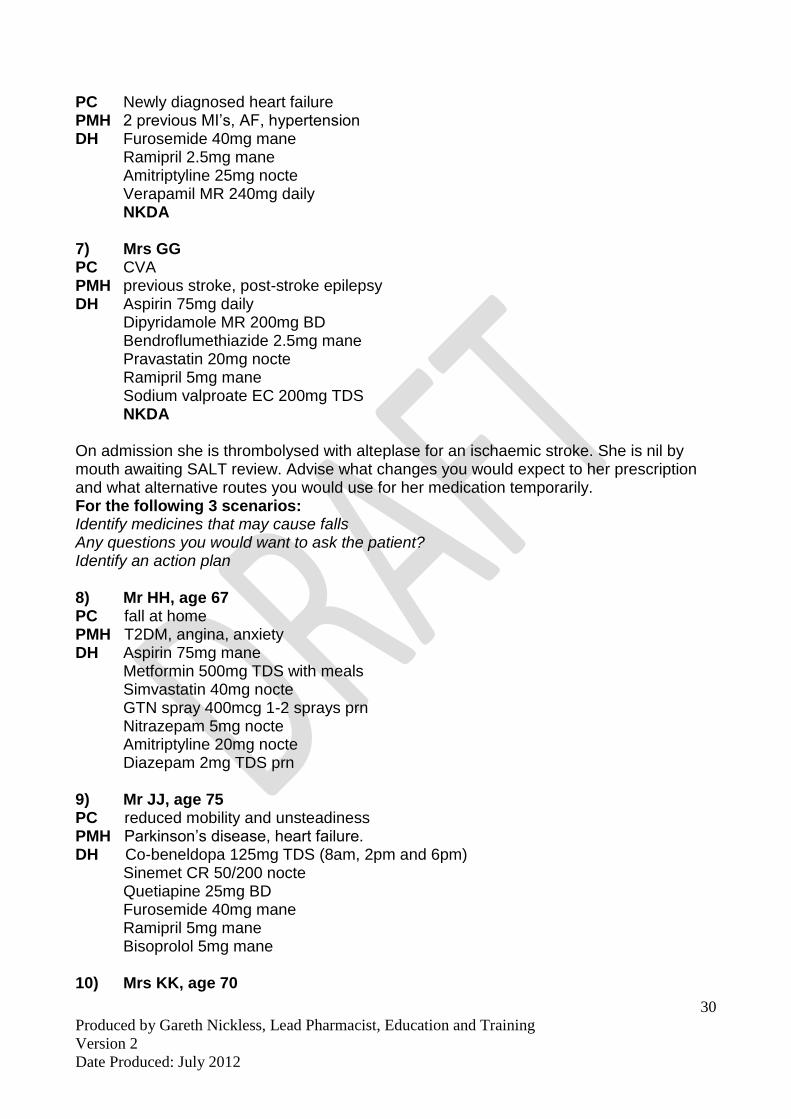
30
PC Newly diagnosed heart failure PMH 2 previous MI’s, AF, hypertension DH Furosemide 40mg mane Ramipril 2.5mg mane Amitriptyline 25mg nocte Verapamil MR 240mg daily NKDA
7) Mrs GG PC CVA PMH previous stroke, post-stroke epilepsy DH Aspirin 75mg daily Dipyridamole MR 200mg BD Bendroflumethiazide 2.5mg mane Pravastatin 20mg nocte Ramipril 5mg mane Sodium valproate EC 200mg TDS NKDA On admission she is thrombolysed with alteplase for an ischaemic stroke. She is nil by mouth awaiting SALT review. Advise what changes you would expect to her prescription and what alternative routes you would use for her medication temporarily. For the following 3 scenarios: Identify medicines that may cause falls Any questions you would want to ask the patient? Identify an action plan 8) Mr HH, age 67 PC fall at home PMH T2DM, angina, anxiety DH Aspirin 75mg mane
Metformin 500mg TDS with meals Simvastatin 40mg nocte GTN spray 400mcg 1-2 sprays prn Nitrazepam 5mg nocte Amitriptyline 20mg nocte Diazepam 2mg TDS prn
9) Mr JJ, age 75 PC reduced mobility and unsteadiness PMH Parkinson’s disease, heart failure. DH Co-beneldopa 125mg TDS (8am, 2pm and 6pm)
Sinemet CR 50/200 nocte Quetiapine 25mg BD Furosemide 40mg mane Ramipril 5mg mane Bisoprolol 5mg mane
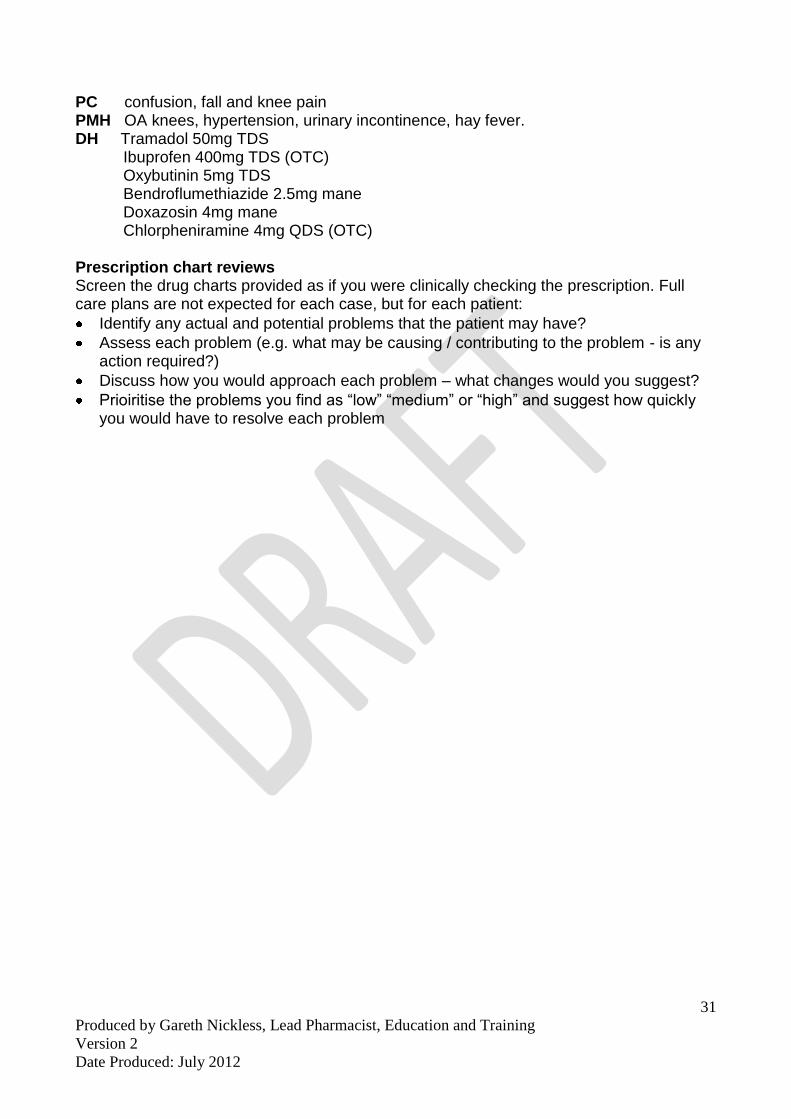
10) Mrs KK, age 70
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
31
PC confusion, fall and knee pain PMH OA knees, hypertension, urinary incontinence, hay fever. DH Tramadol 50mg TDS
Ibuprofen 400mg TDS (OTC) Oxybutinin 5mg TDS Bendroflumethiazide 2.5mg mane Doxazosin 4mg mane Chlorpheniramine 4mg QDS (OTC)
Prescription chart reviews Screen the drug charts provided as if you were clinically checking the prescription. Full care plans are not expected for each case, but for each patient:
Identify any actual and potential problems that the patient may have?
Assess each problem (e.g. what may be causing / contributing to the problem - is any action required?)
Discuss how you would approach each problem – what changes would you suggest?
Prioiritise the problems you find as “low” “medium” or “high” and suggest how quickly you would have to resolve each problem

Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
32
Appendix 3 – Copies of Paperwork for Practice
Based Assessments
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
33
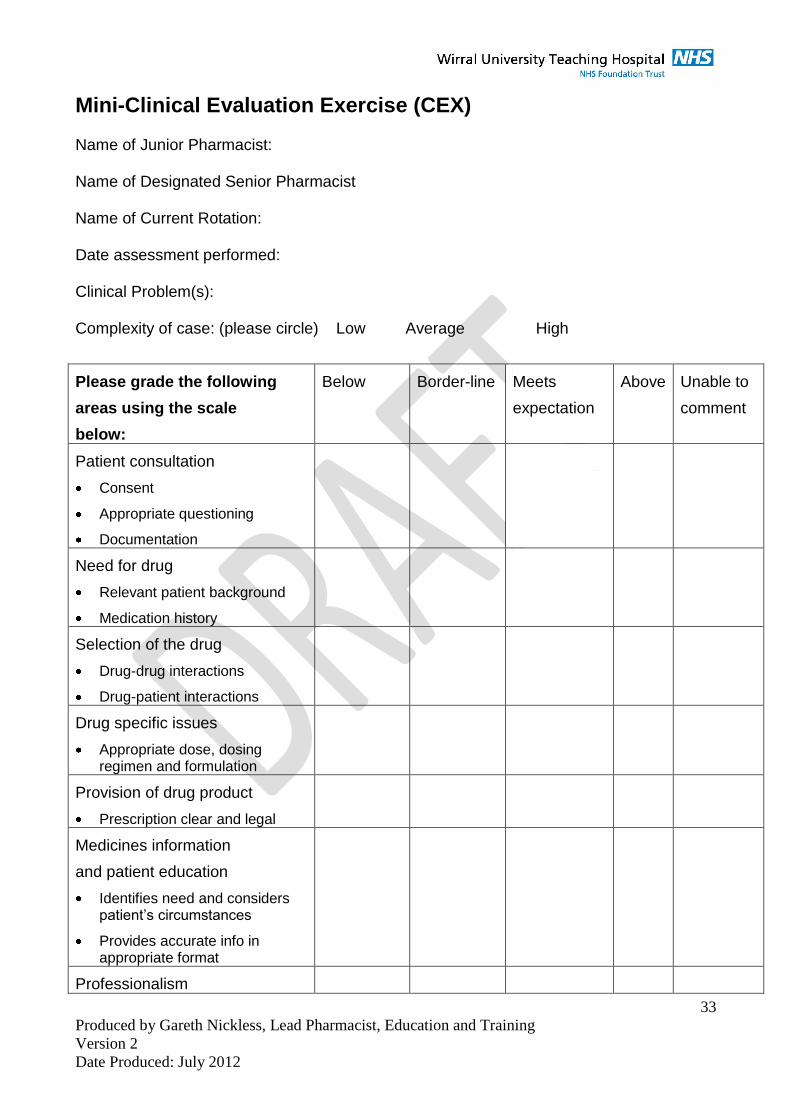
Mini-Clinical Evaluation Exercise (CEX) Name of Junior Pharmacist: Name of Designated Senior Pharmacist Name of Current Rotation: Date assessment performed: Clinical Problem(s): Complexity of case: (please circle) Low Average High
Please grade the following
areas using the scale
below:
Below Border-line Meets
expectation
Above Unable to
comment
Patient consultation
Consent
Appropriate questioning
Documentation
Need for drug
Relevant patient background
Medication history
Selection of the drug
Drug-drug interactions
Drug-patient interactions
Drug specific issues
Appropriate dose, dosing regimen and formulation
Provision of drug product
Prescription clear and legal
Medicines information
and patient education
Identifies need and considers patient’s circumstances
Provides accurate info in appropriate format
Professionalism
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
34
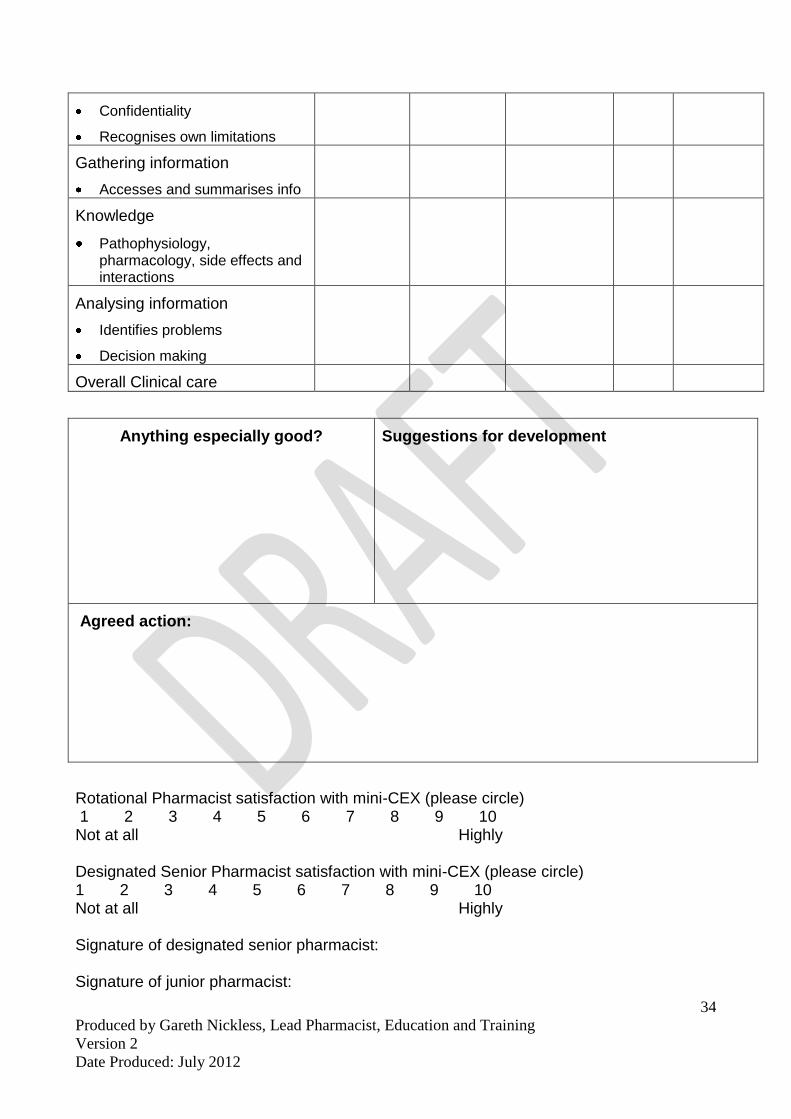
Confidentiality
Recognises own limitations
Gathering information
Accesses and summarises info
Knowledge
Pathophysiology, pharmacology, side effects and interactions
Analysing information
Identifies problems
Decision making
Overall Clinical care
Anything especially good?
Suggestions for development
Agreed action:
Rotational Pharmacist satisfaction with mini-CEX (please circle) 1 2 3 4 5 6 7 8 9 10 Not at all Highly Designated Senior Pharmacist satisfaction with mini-CEX (please circle) 1 2 3 4 5 6 7 8 9 10 Not at all Highly Signature of designated senior pharmacist: Signature of junior pharmacist:
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
35
General Ward Visit Summary
Student Name: Date:
Ward:
Summary of patients: Total number of patients on ward =
Total number of new admissions =
Number of patients seen during the visit =
Duration of visit =
Prescription Verification / Validation
Activity Assessment of
Performance
Comments
Prescription orders verified are
clear / legible
Prescription orders verified are
legal
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
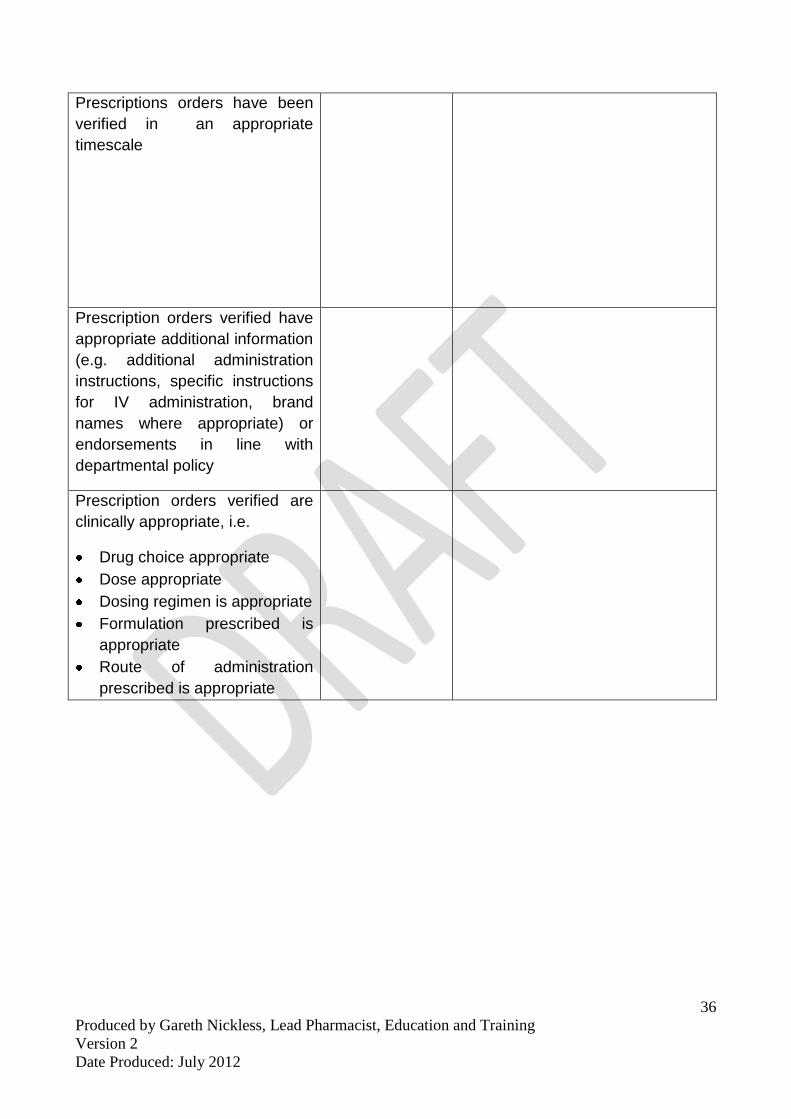
36
Prescriptions orders have been
verified in an appropriate
timescale
Prescription orders verified have
appropriate additional information
(e.g. additional administration
instructions, specific instructions
for IV administration, brand
names where appropriate) or
endorsements in line with
departmental policy
Prescription orders verified are
clinically appropriate, i.e.
Drug choice appropriate
Dose appropriate
Dosing regimen is appropriate
Formulation prescribed is
appropriate
Route of administration
prescribed is appropriate
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
37
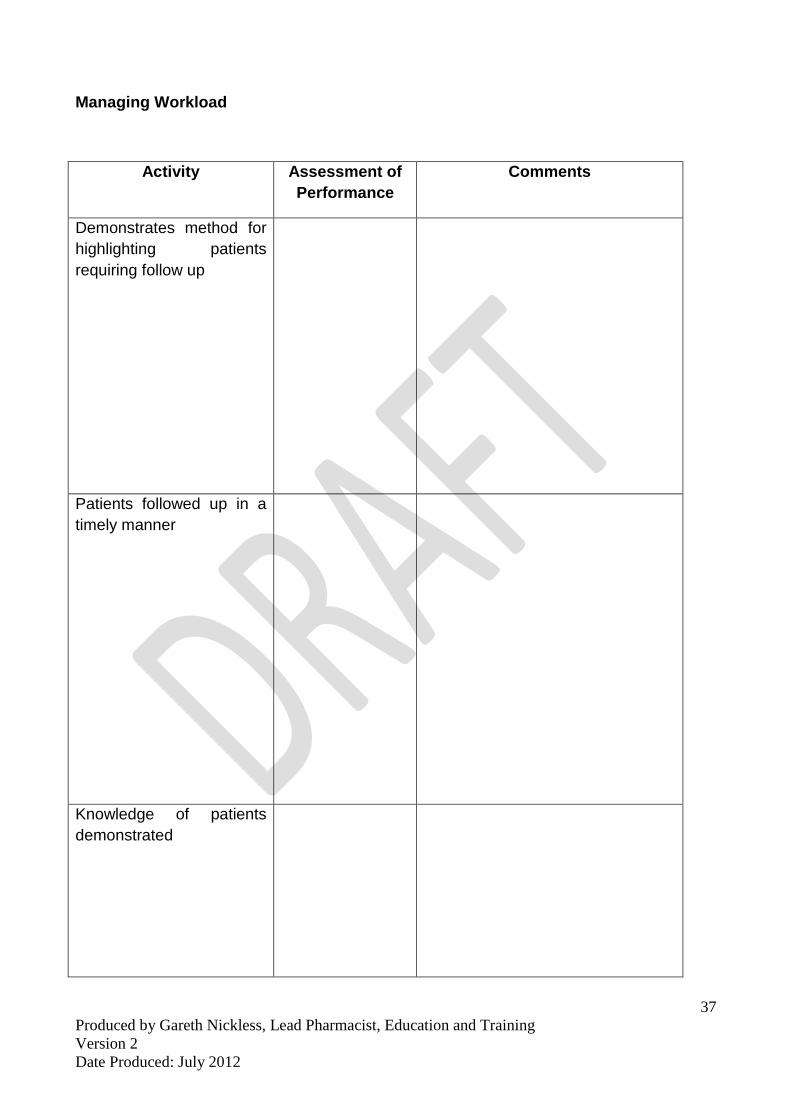
Managing Workload
Activity Assessment of
Performance
Comments
Demonstrates method for
highlighting patients
requiring follow up
Patients followed up in a
timely manner
Knowledge of patients
demonstrated

Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
38
Demonstrates method for
prioritising workload
appropriately
Enlists the help of
colleagues where
appropriate (e.g.
delegation of tasks to the
ward based technician)
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
39
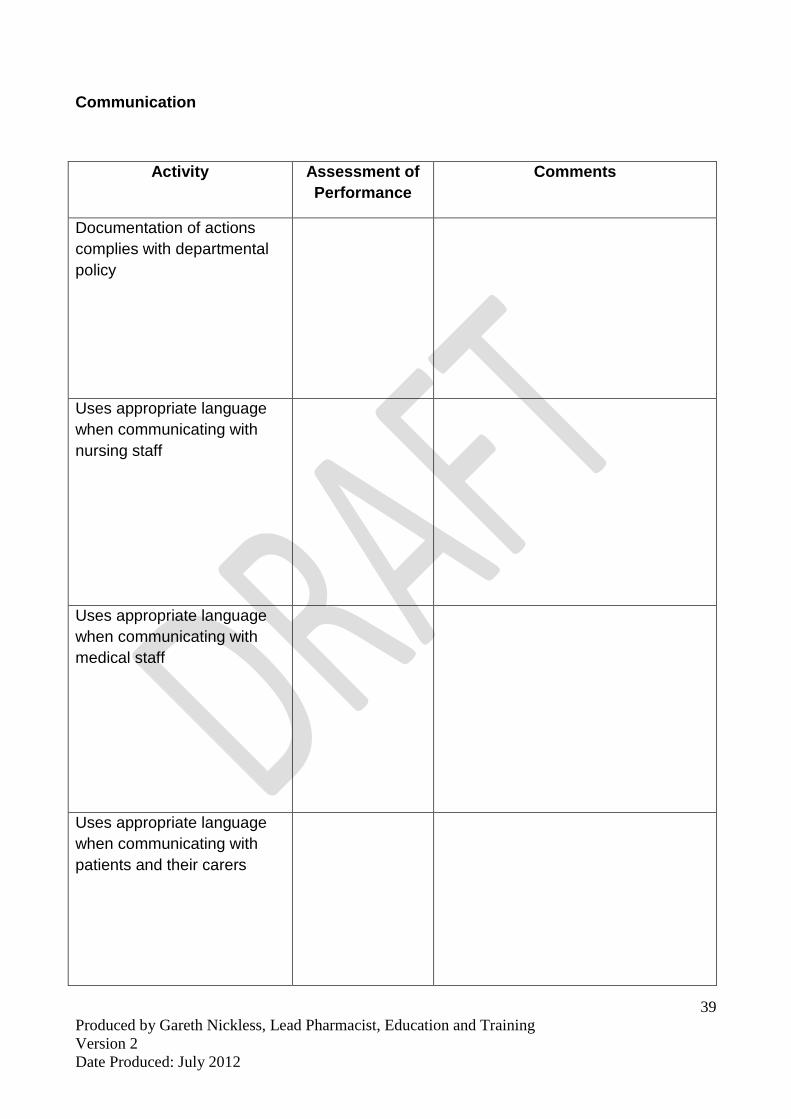
Communication
Activity Assessment of
Performance
Comments
Documentation of actions
complies with departmental
policy
Uses appropriate language
when communicating with
nursing staff
Uses appropriate language
when communicating with
medical staff
Uses appropriate language
when communicating with
patients and their carers
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
40
Overall Comments Relating to the Visit:
Actions Required:
Tutor Signature:
Student Signature:
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
41
Case-based Discussion (CbD) Junior Pharmacist name: Name of Designated Senior Pharmacist: Name of Rotation / Therapeutic Area Covered: Date of Assessment: Complexity of case: (please circle) Low Average High
Please grade the following Areas:
Below Border-line Meets expectation
Above Unable to comment
Pharmaceutical needs Assessment
Identifies the patient’s problems
Prioritises the patient’s problems
Treatment recommendations:
Refers to EBM, local & national guidelines
Knowledge of pathophysiology, pharmacology and therapeutics
Follow up/ Monitoring
Discusses rationale for monitoring
Demonstrates practical on-going and appropriate monitoring
Discusses how patient was managed in conjunction with the wider healthcare team
Professionalism
Timely and succinct
Ethical approach
Recognises own limitations
Considers interface issues
Overall Clinical judgement
Discuss own judgement, synthesis, caring and effectiveness for patient
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
42
Anything especially good?
Suggestions for development
Agreed action:
Rotational Pharmacist’s satisfaction with CBD (please circle) 1 2 3 4 5 6 7 8 9 10 Not at all Highly Assessor’s satisfaction with CBD (please circle) 1 2 3 4 5 6 7 8 9 10 Not at all Highly Signature of designated senior pharmacist: Signature of junior pharmacist:
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
43
Record of In-service Training Assessment (RITA) Name of Junior Pharmacist: Name of Designated Senior Pharmacist: Name of Current Rotation: Date of Review: Period covered: from …………………….to…………………. Please provide a brief description of experience / activities undertaken, since the last review (if applicable): Documentation taken into account during the review: 1. 2. 3. 4. 5. Please describe progress made with the departmental objectives and highlight particular strengths of the band 6 pharmacist
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
44
Please identify any areas of particular weaknesses/difficulties/perceived problems or areas that need further work and give details of the proposed action plan Overall Tutor comments:
Signature Band 6 Pharmacist comments:
Signature
Produced by Gareth Nickless, Lead Pharmacist, Education and Training
Version 2
Date Produced: July 2012
45
Name of Rotation: _______________________________________ 1. The objectives were made clear to me at the start of the rotation (1 = strongly
disagree, 5 = strongly agree) 1 2 3 4 5 2. A list of relevant references was provided (1 = strongly disagree, 5 = strongly
agree): 1 2 3 4 5 3. Please indicate how many meetings (including ward visits) you had during the
rotation:
_____________________________________ 4. Please provide any other information relating to the organisation of the rotation
that you think would be useful for future rotations
Appendix 4 – Feedback on Rotation





























