-
8/10/2019 Banding Versus
1/9
SCIENTIFICSECTION
Banding versus bonding of firstpermanent molars: a
multi-centrerandomized controlled trialMariyah Nazir, Tanya Walsh
and Nicky A. MandallUniversity of Manchester, UK
Susie MatthewThe Abbey Orthodontic Practice, Dalton-in-Furness,
UK
Dee FoxSt Annes Orthodontic Clinic, Lytham St Annes, UK
Objective: To assess the effectiveness of banding versus bonding
of first permanent molars during fixed appliance treatment; interms
of attachment failure, patient discomfort and post-treatment enamel
demineralization.
Design: Multi-centre randomized clinical trial.
Setting: One District General Hospital Orthodontic Department
and two Specialist Orthodontic Practices.Participants: Orthodontic
patients aged between 10 and 18 years old, randomly allocated to
either receive molar bands ( n5 40)or molar bonds ( n5 40).
Method: Bands were cemented with a conventional glass ionomer
cement and tubes were bonded with light-cured composite toall four
first permanent molar teeth for each subject. Attachments were
reviewed at each recall appointment to assess looseningor loss. The
clinical end point of the trial was the day of appliance debond.
Enamel demineralization at debond was assessedusing the modified
International Caries Assessment and Detection System (ICDAS).
Results: The first time failure rate for molar bonds was 18.4%
and 2.6% for molar bands ( P 5 0.0002). Survival
analysisdemonstrated molar bonds were more likely to fail compared
with molar bands. First permanent molars with bonded
tubesexperienced more demineralization than those with cemented
bands ( P 5 0.027). There was no statistically significant
differencein discomfort experienced by patients after banding or
bonding first permanent molars ( P . 0.05).
Conclusion: This study shows that as part of fixed appliance
therapy, American Orthodontics photoetched first permanent
molar bands cemented with 3M ESPE Ketac-Cem perform better than
American Orthodontics low profile photo-etched andmesh-based first
permanent molar tubes bonded with 3M Unitek Transbond XT in terms
of failure behaviour and molarenamel demineralization.
Key words: Molar attachment failure, molar tubes, molar bands,
randomized controlled trial, orthodontic enameldecalcification
Received 13th September 2010; accepted 19th February 2011
Introduction
The terminal attachments of xed appliances are placedon molar
teeth; most commonly the rst permanentmolars. These attachments can
take the form of acemented molar band or a bonded molar tube.
Theactive phase of xed orthodontic appliance treatmenttakes an
average of two years to complete. To reduce thelikelihood of
emergency visits, improve patient experi-ence and avoid lengthy
treatment times it is important
that these attachments have low failure rates. Indeed, it
has been suggested that Loose attachments lower morale,reduce
protability and wreak havoc with scheduling 1 andwhilst a zero per
cent attachment failure is not a realisticgoal, failure rates
should be less than 5%. 1
Prior to the advent of enamel bonding techniques, theuse of
orthodontic bands on rst permanent molar teethwas universal. Many
orthodontists continue to favourmolar bands due to beliefs
regarding lower failure ratesand reliability. 2,3 With improvements
in band design
Journal of Orthodontics , Vol. 38, 2011, 8189
Address for correspondence: Mariyah Nazir,
OrthodonticDepartment, University Dental Hospital Manchester,
HigherCambridge Street, Manchester, M15 6FH, UK.Email:
[email protected]#
2011 British Orthodontic Society DOI 10.1179/14653121141308
-
8/10/2019 Banding Versus
2/9
(micro-etching, innovative mechanical retention fea-tures)
further failure rate reductions have followed. 4,5
Simultaneously, bonded molar tubes have becomeincreasingly
popular as advances in attachment designand materials science have
led to improved survivalbehaviour. 611 Advocates of molar tubes
claim these
attachments are more efcient and convenient, allow foreasier
maintenance of oral hygiene and reduce deminer-alization. However,
there is little prospective clinicalliterature evaluating the
success of bands compared withbonds on molar teeth using
contemporary modernmaterials. 12 The majority of studies in this
eld areretrospective or non-comparative. 1315 Although
muchlaboratory based work has been conducted on molarattachment
failure behaviour, there are problematicissues with applying in
vitro ndings to the clinicalenvironment. 16 Flaws in study design
and data analysisin the eld of bond and band failure research have
beenhighlighted by others. 17
Enamel demineralization is a recognized iatrogenicrisk factor
associated with xed appliance orthodontictreatment. 18 It has been
reported that 50% of patientsundergoing xed appliance treatment
develop at least onewhite spot lesion. 19 The aesthetic and dental
health im-pact of such demineralization is recognized 20 and
manyresearchers are attempting to identify effective interven-tions
to reduce demineralization during orthodontictreatment. 21 Recent
systematic reviews have recommendedbonding and banding studies
should measure deminer-alization as a secondary outcome where
possible in orderto improve the reporting quality of clinical
trials. 22,23
The aim of this study was to assess whether there wereany
differences between rst permanent molar bandsand rst permanent
molar bonds in terms of:
1. Failure rate;2. Enamel demineralization (at debond);3.
Patient discomfort at first recall.
The null hypothesis tested was that there is no
differencebetween rst permanent molar bands and rst perma-nent
molar bonds in terms of failure rate during xedappliance treatment,
patient discomfort at rst recall orenamel demineralization at
debond.
Subjects andmethods
Ethical approval was obtained from the NHS Multi-Centre Research
Ethics Committee. All eligible patientswere given written
information describing the trial, withthe opportunity to ask
further questions. Writtenconsent was taken from patients recruited
to the trial.The recruitment period extended from July 2005 to
July
2007 and patients were followed until the end of treatment
(appliance debond).
The study sample was taken from consecutive patientsattending
three centres for xed appliance treatment:
N The Abbey Orthodontic Practice (Dalton-in-Furness)
05/MRE05/27;
N St Annes Orthodontic Clinic (Lytham St Annes) 05/MRE05/27;
N Tameside General Hospital Orthodontic
Department(Ashton-under-Lyne) 05/MRE05/27.
An a priori sample size calculation determined that asample size
for each group of 38 would be sufcient todetect a failure rate
difference of 30% (odds ratio of 6.00)between the molar bands group
(with a predicted failurerate of 10%) 24 and a molar bond group
(with a predictedfailure rate of 40%) using a two group continuity
correctedchi-square test with a 0.05 two-sided signicance level
andpower of 80%. A 40% bond failure was based on clinicalopinion as
there was no supporting literature. A totalsample size of 76
patients was required and to allow fordropouts, the decision was
made to recruit 80 patients.
The appliances were placed by one operator at eachcentre.
Inclusion criteria
N Patients aged between 10 and 18 years old;N Patient starting
orthodontic treatment with upper and
lower fixed appliances (pre-adjusted edgewise);N Patient and
parent informed and written consent.
Exclusion criteria
N Lack of consent;N Absence of or planned extraction of first
permanent
molars;N First permanent molars with evidence of deminerali-
zation or hypoplastic enamel;N Occlusion likely to debond bonded
attachments;N Patients requiring orthognathic surgery;N Occlusions
that require extra-oral or intra-oral
anchorage reinforcement (headgear, palatal arch,lingual arch) or
precluded the use of bonds, e.g. useof a quad-helix appliance.
Random allocation and concealment
Randomization was carried out using random numbertables; even
numbers were assigned to the molar bandgroup and odd numbers to the
molar bond group. Arestricted randomization method in blocks of 10
was
82 Nazir et al. Scientific Section JO June 2011
-
8/10/2019 Banding Versus
3/9
employed to ensure equal numbers of patients wereallocated to
each of the treatment groups. The randomallocation sequence was
generated by one clinician.Participants were enrolled by individual
operators at eachsite. The allocations were concealed in envelopes
markedwith each subjects identication number and held in acentral
place to which the operators did not have access.The operator and
patient remained blind to the attachment
type until after the consent and registration procedures.In line
with recent recommendations 21,23 a parallel
method rather than a split-mouth study design wasemployed to
reduce any bias that may be introduced bycross-over effects.
Therefore if a patient was allocated tothe bonding group for
example, molar bonds wereplaced on all four rst permanent
molars.
Clinical sequence
A standardized procedure was followed for each patientas
follows:
N
Consent and registration;N A letter was sent to the patients GDP
to inform them
of their participation in the study;N Baseline variables
recorded including patient age,
gender, intervention group and malocclusion type;N Patients
allocated to receive bands had separators placed
for 1 week followed by cementation of AmericanOrthodontics H
(Sheboygan, WI, USA) photo-etchedmolar bands with 3M ESPE Ketac-Cem
H (St. Paul,
MN, USA) mixed according to the manufacturersinstructions;
N Where patients were allocated to the bonding group,molars were
isolated with cotton wool rolls andsuction; Kerr H (Orange County,
CA, USA) 37%phosphoric acid enamel etchant was applied to thebuccal
surfaces for 30 s. The teeth were then washedwith water from a
three-in-one tip for at least 15 sbefore drying. 3M Unitek
Transbond XT primer andlight cured composite were used to bond
AmericanOrthodontics low profile molar tubes with photo-etched mesh
bases to the molar teeth;
N The remainder of the upper and lower fixed appliances(Roth
prescription) was then placed in the usual way andeach clinician
followed their routine orthodontic treat-ment mechanics. Distal-end
cutters were not used in themouth as this was likely to debond
bonded attachments;
N All patients were instructed to avoid hard, sticky or
sweetfoods. They were requested to use a 0.05% sodiumfluoride
mouthwash daily for the duration of their
treatment.
Stopping criteria
In line with routine clinical practice the followingstopping
rules and subsequent appliance removal wereapplied:
N Repeated failure to attend appointments;
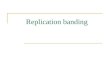
N Sound tooth surface: Code 0; N First visual change in enamel
upon drying (when seen wet there is no evidence of any change):
Code 1;N Distinct visual change in enamel when viewed wet: Code 2;
N Localized shallow enamel breakdown due to caries with no visible
dentine:Code 3; N Localized deeper enamel breakdown due to caries
with no visible dentine:Code 4; N Distinct cavity with visible
dentine: Code 5
Figure 1 International Caries Detection and Assessment System
(ICDAS) criteria
JO June 2011 Scientific Section Banding and bonding molars: a
multi-centre RCT 83
-
8/10/2019 Banding Versus
4/9
N Repeated breakages or general lack of co-operation;N Poor oral
hygiene;N Presence or development of clinically significant
demineralization, root resorption and/or caries;N
Patient/parental request to stop treatment for any reason.
Clinical outcome measures
The primary outcome measure was molar band or molarbond failure.
At review appointments, outright bond or
cement failure resulting in frank loss of the attachmentor
attachment loosening due to partial bond or cementfailure, were
both recorded as failure. When a failureepisode occurred the same
type of attachment wasreplaced to allow further analysis of failure
behaviour.
Post-treatment demineralization was assessed at debondby direct
visual examination. 19,2528 Conventionally,clinical assessment of
enamel demineralization related toorthodontic treatment has been
evaluated by the absence/presence of white spot lesions. 19,27,29
With time, the
Figure 2 Trial prole for comparison of rst permanent molar bands
and bonds
84 Nazir et al. Scientific Section JO June 2011
-
8/10/2019 Banding Versus
5/9
majority of such white spot lesions improve 30 and are notalways
indicative of true demineralization. 31 Moreextensive enamel
lesions are of greater concern as thereis less potential for
remineralization. There is a lack of consistency among the
contemporary demineralizationcriteria systems which limits the
comparability of
measured outcomes. The International Caries Detectionand
Assessment System (ICDAS) criteria have beendeveloped by an
international team of caries researchersto produce one standard
system for caries detection andassessment histological evaluation
of extracted teeth hasdemonstrated that as ICDAS codes increase in
severity,there is an increased likelihood of demineralization. 32
Themodied ICDAS was used at the chairside to record theextent of
enamel demineralization on the buccal surfacesof the rst permanent
molars at debond (Figure 1). Inaddition to being practical, the
system has been proven tohave content, correlational and
discriminatory validity. 33
Patient based outcomes
Patient discomfort was measured on a 7 point Likertscale at the
rst review appointment after attachmentplacement, where 1 5 no
discomfort and 7 5 extremediscomfort. This was a requirement of the
local ethicscommittee, as they were concerned that one or
othertreatment may signicantly increase patient discomfort.
Statistical data analysis
The data were checked for normality and to allowmeaningful
comparisons with previous studies, only rsttime failures were
analyzed. Subsequent failures wereevaluated, but not included in
the survival analysis.
Where molar bonds were replaced with bands (repeatedfailures,
anchorage requirements) an intention-to-treatanalysis was applied
and all patients were analyzedaccording to the group to which they
had been originallyrandomized.
To assess ICDAS reliability, 27 images were assessedand
re-assessed a week apart by all operators. Theresults were then
analyzed using a weighted kappastatistic.
Clustering of data within patients was accounted forby
appropriate statistical analysis: the cluster adjustedchi-square
test was used to analyze attachment failure atthe tooth level. The
Mann-Whitney U test was used to
compare median levels of patient discomfort betweenthe two
treatment groups and to analyze demineraliza-tion data. Survival
analysis was used to estimate therelative risk of failure from the
point of attachmentplacement until the end-point of the study,
usingSTATA statistical software version 9.0.
Results
A CONSORT diagram illustrating the ow of patientsthrough each
stage of the trial is shown (Figure 2).Baseline demographic and
clinical characteristics arepresented in Table 1.
Agreement and repeatability
All operators showed at least 95% intra-rater agreementwith the
gold standard ICDAS scores, demonstratinghigh levels of agreement.
Additionally, weighted kappascores for intra-rater reliability
between initial testing
Table 1 Distribution of patient characteristics at baseline for
each
treatment group.
Molar bands group Molar bonds group
Patient variables n (%) n (%)
Total 38 (50.0) 38 (50.0)GenderMale 16 (42.1%) 14 (36.8%)Female
22 (57.9%) 24 (66.7%)Age1012 12 (31.6%) 12 (31.6%)1315 24 (63.2%)
20 (52.6%)1618 2 (5.3%) 6 (15.7%)
MalocclusionClass I 8 (21.1%) 13 (34.2%)Class II/I 22 (57.9%) 16
(42.1%)Class II/II 5 (13.2%) 6 (15.8%)Class III 3 (7.9%) 3
(7.9%)CentreAbbey 12 (31.6%) 11 (28.9%)St Annes 9 (23.7%) 11
(28.9%)TGH 17 (44.7%) 16 (42.1%)
Table 2 Cluster adjusted chi-square test to compare first
timefailures between molar bands and bonds
Failure at tooth level
Failures No failures Totaln (%) n (%) n (%)
Bands 4 (2.6) 148 (97.4) 152 (100)Bonds 28 (18.4) 124 (81.6) 152
(100)
Inter-cluster correlation 5 0.0860.ICC 95% confidence intervals
5 [0.000, 0.0192].Pooled adjustment chi-square statistic 5 14.295
and P 5 0.0002.Group adjustment chi-square statistic 5 14.295 and P
5 0.0002.
JO June 2011 Scientific Section Banding and bonding molars: a
multi-centre RCT 85
-
8/10/2019 Banding Versus
6/9
and one week re-testing ranged from 0.95 to 0.96
(SE0.19200.1924), demonstrating good repeatability.
Failure outcomes
There was a total of 32 (10.5%) rst time attachment
failures and these occurred in 23 (60.5%) patients.
Theproportion of rst time attachment failures was greaterfor molar
bonds (18.4%, n5 28) than for molar bands(2.6%, n5 4). This nding
was statistically signicant(P 5 0.002) using the cluster adjusted
chi-squared test(group adjustment) (Table 2). Patients who had
molarband failures only experienced one failure episode ( n5
4;10.5%), whereas multiple attachment failure episodeswere more
common in the molar bonds group ( n5 10;26.3%). Analysis using the
chi-square test showed nostatistically signicant differences in the
number of patients experiencing attachment failures between
trialcentres ( P 5 0.27); age groups ( P 5 0.90); genders(P 5
0.665) or between upper and lower arches ( P 5 0.453).
Discomfort outcomes
There was no statistically signicant difference in thediscomfort
levels recorded at rst review followingattachment placement between
the molar band andmolar bond groups in terms of upper arch ( P 5
0.754) orlower arch ( P 5 0.583) discomfort (Table 3).
Demineralization outcomes
Analysis at the patient level demonstrated that 44 (60%)patients
developed some degree of demineralization(ICDAS code 1 and above).
Sixteen (36%) bandedpatients experienced demineralization compared
with 28(64%) bonded patients ( P 5 0.038) (Table 4). However,the
majority of patients with demineralization onlydeveloped ICDAS code
1 lesions (rst visual change inenamel upon drying when seen wet
there was noevidence of any change: n5 30; 68%). No patients
developed frank carious lesions (ICDAS codes 3, 4and 5).
Analysis at the tooth level demonstrated 98 (33%) rstpermanent
molars developed some degree of deminer-alization (ICDAS code 1 and
above). Thirty-six (24%)banded molars developed demineralization
compared
with 62 (43%) bonded molars demineralization(P 5 0.027) (Table
5). The majority of teeth affected bydemineralization had ICDAS
code 1 lesions n5 78 (80%),the remaining teeth had ICDAS code 2
lesions. No teethdeveloped frank carious lesions (ICDAS codes 3, 4
and 5).
Survival analysis
The mean total treatment time was 19 months. Theshortest course
of xed appliance treatment was9 months and the longest course was 3
years and1 month. The minimum time to attachment failure was8 days
and the maximum time was 310 days (10 months
and 10 days). The assumption of the Cox proportionalhazard was
met (i.e. the hazard ratio is constant;P 5 0.888). Survival
functions for the two attachmenttypes are illustrated by the Cox
proportional hazardssurvival analysis (Figure 3). This demonstrates
molarbonds were more likely to fail during xed appliancetreatment.
The relative risk of failure for eitherattachment is low at any
time point as demonstratedby the high survival function values on
the y-axis.Although the hazard ratio was positive and thus,
theprognosis worse for the molar bonds group, the ndingsshould be
interpreted with caution as there were only asmall number of
failures ( n5 36) despite a large numberof observations ( n5 304).
In survival analysis, it is thenumber of failures which gives power
to the test and inthis study that number was small.
Discussion
The main nding of this study was that during xedorthodontic
appliance treatment bonds placed on rstpermanent molars are more
likely to fail than bands.The relatively low attachment failure
rates reported mayTable 3 Mann-Whitney U test to compare molar
bands and bonds
in terms of arch discomfort.
n MedianMaximumpain score
Minimumpain score
UpperArch
Band 38 2 4 1Bond 38 2 6 1
z52 0.313, P 5 0.754LowerArch
Band 38 2 5 1Bond 38 2 6 1
z52 0.549, P 5 0.583
Table 4 Mann-Whitney U test to compare molar bands and bondsin
terms of ICDAS score (patient level).
n Median
MaximumICDASscore
MinimumICDASscore
Band 38 0 2 0Bond 36 1 2 0
z52 2.078, P 5 0.038.
86 Nazir et al. Scientific Section JO June 2011
-
8/10/2019 Banding Versus
7/9
be due the application of stringent inclusion andexclusion
criteria, the use of systematic standardizedclinical techniques or
as a result of improvements inattachment design.
Strengths of the study
This was a real world study evaluating the effectivenessof
banding and bonding rst permanent molars as partof xed appliance
treatment. Conducting an effective-ness study allows data to be
generalized with regard tothe rest of the orthodontic population
where the sameattachments and adhesives are used. All patients
werefollowed until the end of treatment as recommended byCochrane
systematic reviews of banding and bondingstudies. It has been
reported that the majority of attachment failures occur within the
rst 6 months of treatment. 34 The current study demonstrated all
failuresoccurred within 13 months of commencing
treatment.Attachment failure rates do increase with time 11,12
andreporting of failure rates early in treatment mayunderestimate
true failure rates. Each patient wasrandomly allocated to either
molar bands or molarbonds at the outset of treatment. Other workers
haveused split-mouth studies when investigating attachmentfailures.
The split mouth design allows patients to act astheir own control,
which reduces variability; however
disadvantages of this methodology are possible cross-over
effects and one adhesive or cement contaminatingthe other materials
performance. This may confoundthe results and limit the robustness
of any ndings.
Weaknesses of the study
Considering a number of patients in the study experi-enced
multiple bond failures we were unable to elicit anypredictor
variables that could help identify vulnerablepatients at the start
of treatment. Multivariate sub-group analysis was not planned at
the outset, whichmeans that the study may have been
insufcientlypowered to detect any failure predictors that did
exist.Other workers have demonstrated the inuence of
age,malocclusion and socio-economic background on thenumber of
attachment failures. 12,15,24
Context and implications for clinical practice
Failure outcomes. The molar band failure rate in thisstudy
(2.6%) compares favourably with the ndings of other workers. 2,3
Additionally, the molar bond failurerate (18.4%) was lower than
that reported by othercomparative prospective 12 and retrospective
studies. 14
This 16% difference in failure rates would suggest bandsare a
more reliable rst permanent molar attachmentthan bonds during xed
appliance treatment. A numberof patients experienced numerous molar
bond failures;this was not always on the same rst permanent
molar.We may have a cohort of patients who have a predilectionfor
appliance wrecking and in such circumstances it may
be prudent to revert to bands on all molar teeth as soon assuch
wrecking behaviour is observed.
Demineralization
It has been reported that almost 50% 19 of individualsundergoing
xed appliance treatment develop enameldemineralization. In this
study, 60% of patients and 33%of molar teeth developed enamel
demineralization.However, the majority of lesions (80%) were
limited toICDAS code 1. No patients experienced frank
enamelbreakdown. Although the majority of enamel lesions
willremineralize with low dose uoride therapy 21 they can
compromise aesthetics, particularly where anterior teethare
affected. Appropriate and careful selection of patientswith good
oral hygiene habits from the outset shouldallow for minimal
demineralization experience. The lowerdemineralization codes
observed in the molar band groupcompared with the molar bond group
may be due to theuse of glass-ionomer banding cement, with its
resultantbenecial local uoride releasing properties. 7,35 However,a
recent systematic review investigating the effectiveness
Figure 3 Survival functions for molar bands and bonds
(Coxproportional hazards regression)
Table 5 Mann-Whitney U test to compare molar bands and bondsin
terms of ICDAS score (tooth level).
n Median
MaximumICDASscore
MinimumICDASscore
Band 152 0 2 0Bond 154 1 2 0
z52 3.757, P 5 0.027.
JO June 2011 Scientific Section Banding and bonding molars: a
multi-centre RCT 87
-
8/10/2019 Banding Versus
8/9
of orthodontic banding adhesives concluded there was alack of
suitable evidence to allow specic recommenda-tions regarding the
use of any one material overanother. 23 Studies comparing glass
ionomer cement withcomposite resin for bonding have demonstrated
reducedrates of enamel demineralization 26,27 however; this has
been at the expense of increased attachment failurerates.
17,36,37 Benson et al. 21 in their systematic reviewconcluded the
current level of evidence demonstratingglass ionomer based
adhesives for bracket bonding maybe more effective at preventing
enamel demineralizationthan conventional composite resins is weak.
Factorsother than cement/adhesive composition may
affectdemineralization experience and site of lesions; such
asuoride supplementation in the form of mouthwashesand varnishes as
well the role of the right-handed or left-handed dominance when
tooth brushing.
Patient discomfort
This study is the rst to report patient-based outcomesassociated
with placement of rst permanent molarattachments. It would be
tempting to postulate bandingwould be more uncomfortable for
patients as theattachment physically surrounds the entire tooth
surfaceand placement can involve trauma to the gingivae;however, no
differences were demonstrated betweenbands and bonds, low levels of
discomfort were reportedand patients tolerated both types of
attachment well.
Conclusions
N First permanent molars bonded with 3M UnitekTransbond XT have
a higher failure rate than firstpermanent molar bands cemented with
3M ESPEKetac-Cem.
N Bonded first permanent molars demonstrated higherlevels of
post-treatment demineralization than bandedfirst permanent
molars.
N No differences in discomfort were experienced bypatients when
banding or bonding first permanentmolars as part of fixed appliance
treatment.
ContributorsNicky Mandall was responsible for the study
concept,ethical approval, data interpretation, critical revisionand
nal approval of the article. Mariyah Nazir wasresponsible for study
design, administration, recruit-ment and treatment, drafting,
critical revision and nalapproval of the article. Dee Fox was
responsible forrecruitment, treatment, data entry, organization
and
accommodation for examiner training and reliabilityexercises.
Susie Matthew was responsible for recruit-ment, treatment and data
entry. Tanya Walsh wasresponsible for statistical analysis, data
interpretation,critical revision and nal approval of the
article.Mariyah Nazir is the guarantor.
References
1. Bennett RK. Loose brackets: minor inconvenience or
profitvacuum? Ormco Clinical Impressions 2001; 10 : 2228.
2. Gillgrass TJ, Benington PC, Millett DT, Newell J, GilmourWH.
Modified composite or conventional glass ionomer forband
cementation? A comparative clinical trial. Am J Orthod Dentofacial
Orthop 2001; 120 : 4953.
3. Clark JR, Ireland AJ, Sherriff M. An in vivo and ex vivostudy
to evaluate the use of a glass polyphosphonate cementin orthodontic
banding. Eur J Orthod 2003; 25 : 31923.
4. Millett DT, Duff S, Morrison L, Cummings A, GilmourWH. In
vitro comparison of orthodontic band cements. AmJ Orthod
Dentofacial Orthop 2003; 123 : 1520.
5. Hodges SJ, Gilthorpe MS, Hunt NP. The effect of micro-etching
on the retention of orthodontic molar bands: aclinical trial. Eur J
Orthod 2001; 23 : 9197.
6. Fricker JP. A new self-curing resin-modified
glass-ionomercement for the direct bonding of orthodontic brackets
invivo. Am J Orthod Dentofacial Orthop 1998; 113 : 38486.
7. Gaworski M, Weinstein M, Borislow AJ, Braitman
LE.Demineralisation and bond failure: a comparison of a
glassionomer and a composite resin bonding system in vivo. AmJ
Orthod Dentofacial Orthop 1999; 116 : 51821.
8. Kula K, Schreiner R, Brown J, Glaros A. Clinical bond
failure of pre-coated and operator-coated orthodonticbrackets.
Orthod Craniofac Res 2002; 5 : 16165.
9. Sharma-SayalSK,Rossouw PE, Kulkarni GV,Titley KC.Theinfluence
of orthodontic bracket base design on shear bondstrength. Am J
Orthod Dentofacial Orthop 2003; 124 : 7482.
10. Aljubouri YD, Millett DT, Gilmour WH. Six and twelvemonths
evaluation of a self-etching primer versus two-stageetch and prime
for orthodontic bonding: a randomizedclinical trial. Eur J Orthod
2004; 26 : 56571.
11. Manning N, Chadwick SM, Plunkett D, Macfarlane TV.
Arandomized clinical trial comparing one-step and
two-steporthodontic bonding systems. J Orthod 2006; 33 : 27683.
12. Banks P, MacFarlane TV. Bonded versus banded first
permanent molar attachments: a randomized clinical trial. J
Orthod 2007; 32 : 12836.
13. Millett DT, Hallgren A, Fornell AC, Robertson M. Bondedmolar
tubes: a retrospective evaluation of clinical perfor-mance. Am J
Orthod Dentofacial Orthop 1999; 115 : 667 74.
14. Millett DT, Letters S, Roger E, Cummings A, Love J.Bonded
molar tubes an in vitro evaluation. Angle Orthod 2001; 71 :
38085.
88 Nazir et al. Scientific Section JO June 2011
-
8/10/2019 Banding Versus
9/9
15. Pandis N, Christensen L, Eliades T. Long-term
clinicalfailure rate of molar tubes bonded with a
self-etchingprimer. Angle Orthod 2005; 75 : 100002.
16. Eliades T, Brantley WA. The inappropriateness of
conven-tional orthodontic bond strength assessment protocols. EurJ
Orthod 2000; 22 : 1323.
17. Miller JR, Mancl L, Arbuckle G, Baldwin J, Phillips RW.
Athree-year clinical trial using a glass ionomer cement for
thebonding of orthodontic brackets. Angle Orthod 1996; 66
:30912.
18. Ellis PE, Benson PE. Potential hazards of
orthodontictreatment what your patient should know. Dent
Update2002; 29 : 49296.
19. Gorelick L, Geiger AM, Gwinnett AJ. Incidence of whitespot
formation after bonding and banding. Am J Orthod Dentofacial Orthop
1982; 81 : 9398.
20. Geiger AM, Gorelick L, Gwinnett AJ, Benson BJ. Reducingwhite
spot lesions in orthodontic populations with fluoriderinsing. Am J
Orthod Dentofacial Orthop 1992; 101 : 40307.
21. Benson PE, Shah AA, Millett DT, Dyer F, Parkin N, VineRS.
Fluorides, orthodontics and demineralization: a sys-tematic review.
J Orthod 2005; 32 : 10214.
22. Mandall NA, Hickmann J, Macfarlane TV, Mattick CR,Millett
DT, Worthington D. Adhesives for fixed orthodon-tic brackets.
Cochrane Database Syst Rev 2003; (2):CD002282.
23. Millett DT, Glenny AM, Mattick CR, Hickmann J,Mandall NA.
Adhesives for fixed orthodontic bands.Cochrane Database Syst Rev
2007; (2): CD004485.
24. Millett DT, Gordon PH. The performance of first
molarorthodontic bands cemented with glass ionomer cement
Aretrospective analysis. Br J Orthod 1992; 19 : 21520.
25. Twetman S, McWilliam JS, Hallgren A, Oliveby A.
Cariostatic effect of glass ionomer retained
orthodonticappliances: an in vivo study. Swed Dent J 1997; 21 :
16975.
26. Marcusson A, Norevall LI, Persson M. White spotreduction
when using glass ionomer cement for bondingin orthodontics: a
longitudinal and comparative study. EurJ Orthod 1997; 19 :
23342.
27. Chung CK, Millett DT, Creanor SL, Gilmour WH, FoyeRH.
Fluoride release and cariostatic ability of a compomer
and a resin-modified glass ionomer cement used fororthodontic
bonding. J Dent 1998; 26 : 53338.
28. Millett DT, McCluskey LA, McAuley F, Creanor SL,Newell J,
Love J. A comparative clinical trial of acompomer and a resin
adhesive for orthodontic bonding.Angle Orthod 2000; 70 : 23340.
29. Ghiz MA, Ngan P, Kao E, Martin C, Gunel E. Effects of
sealant and self-etching primer on enamel demineralisation.Part II:
an in-vivo study. Am J Orthod Dentofacial Orthop2009; 135 :
20613.
30. Millett DT, Nunn JH, Welbury RR, Gordon PH.Demineralisation
in relation to brackets bonded with glassionomer cement or a resin
adhesive. Angle Orthod 1999; 69 :6570.
31. Kanthathas K, Wilmott DR, Benson PE. Differentiation of
developmental and post-orthodontic white spot lesionsusing image
analysis. Eur J Orthod 2005; 27 : 16772.
32. Pitts N. ICDAS an international system for cariesdetection
and assessment being developed to facilitate cariesepidemiology,
research and appropriate clinical manage-ment. Community Dent
Health 2004; 21 : 19398.
33. Ismail A, Sohn W, Tellez M, et al . The International
CariesDetection and Assessment System (ICDAS): an integratedsystem
for measuring dental caries. Community Dent Oral Epidemiol 2007; 35
: 17078.
34. Hegarty DJ, Macfarlane TV. In Vivo bracket
retentioncomparison of a resin-modified glass ionomer cement and
aresin-based bracket adhesive system after a year. Am J Orthod
Dentofacial Orthop 2002; 121 : 496501.
35. Pascotto RC, Navarro MF, Capelozza-Filho L, Cury JA. Invivo
effect of a resin-modified glass ionomer cement onenamel
demineralization around orthodontic brackets. AmJ Orthod
Dentofacial Orthop 2004; 125 : 3641.
36. Miguel JA, Almeida MA, Chevitarese O. Clinical compar-ison
between a glass ionomer cement and a composite fordirect bonding of
orthodontic brackets. Am J Orthod Dentofacial Orthop 1995; 107 :
48487.
37. Norevall LI, Marcusson A, Persson M. A clinical evalua-tion
of a glass ionomer cement as an orthodontic bondingadhesive
compared with an acrylic resin. Eur J Orthod 1996;18 : 37384.
JO June 2011 Scientific Section Banding and bonding molars: a
multi-centre RCT 89