Embed Size (px)
Citation preview

BARIATRIC SURGERY
Tracy Ann Rydel, MD
August 22, 2006

CASE PRESENTATION
L.R. is a 45 yo woman with morbid obesity, 3 months s/p gastric bypass surgery.
Presented to ED with abdom pain, incr. N/V, & decr. POs x 4 days.
Emesis approx 10-15x daily = clear, frothy. Hemetemesis x 1. No bowel changes but pain with BMs in RLQ, RUQ.
ROS: chills, SOB, CP.

CASE PRESENTATION (cont’d)
• PMH: depression, HTN, Hep C, GERD, DM2, asthma
• PSH: gastric bypass 5/06
• Meds: Benaz, Atenolol, Lasix, Pravachol, Metformin, Tyco, Seroquel, Paxil, PNV’s

CASE PRESENTATION (cont’d)
PE: 39.1 142/67 120-133 18 98%RAAnxiousExpiratory wheezeRRR no murmurWell-healed abdom incision, soft, diffuse ttp.+BS, +fluid wave, no reb/guard, guiac +WBCs 12, Chem7 WNL, UA WNLCT A/P…

INDICATIONS FOR BARIATRIC SURGERY
• BMI>40• BMI>35 with high risk comorbidity*• Failed attempts at behavioral or medical rx• Motivated, psychologically stable, realistic
expectations, supportive environment• Commitment to long-term follow-up
*Cardiopulmonary conditions (sleep apnea, OHS, cardiomyopathy), DM2, DJD, body size problems that interfere with ambulation at employment

CONTRAINDICATIONS
• Untreated major depression or psychosis• Binge eating disorders• Current drug and alcohol abuse• Severe cardiac disease with prohibitive
anesthetic risks• Severe coagulopathy• Inability to comply with nutritional
requirements including life-long vitamin replacement

PREOPERATIVE REQUIREMENTS
From http://www.stanfordhospital.com/clinicsmedServices/COE/surgical/bariatricsurgery/
• You must have a stable relationship with a primary care doctor. Often we require that you be cared for continuously by one physician for one year prior to consideration of surgery. You must be willing to be followed by this physician indefinitely.
• You must be seen by a dietician and by a psychologist or psychiatrist.
• You must complete a detailed health questionnaire that we will provide.
• You must undergo at a minimum the following tests prior to surgery:– Chest Xray– EKG– Pulmonary function tests and Room Air Blood Gas– Blood tests
• Complete blood count • B12 level • Serum electrolytes, renal and liver function tests, calcium and phosphate levels, uric acid • Lipid profile (cholesterol and triglycerides) • Glucose tolerance test (unless already known to be diabetic) • Thyroid function tests
• You may be asked to undergo additional tests as well, including more elaborate testing of your heart and lungs, testing for sleep apnea, or other blood tests.

HIGH-RISK PATIENTS
Retrospective chart review by Helling TS, et al showed increased ICU/ventilatory requirements in:
--males
--BMI >60
--age >50
--underlying pulmonary comorbidity
--complications requiring re-operation

SURGICAL OPTIONS IN THE U.S.
• MALABSORPTIVE– Jejunoileal bypass– Biliopancreatic diversion (BPD)– BPD with duodenal switch
• RESTRICTIVE– Vertical Banding– Laparoscopic Adjustable Gastric Banding
• COMBINATION– Roux-en-Y Gastric Bypass

MALABSORPTIVE PROCEDURES
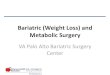
JEJUNOILEAL BYPASS:
Jejunum is transected just beyond the ligament of Trietz
VERY long blind loop remains as short portion of small bowel anastomosed just proximal to ileocecal valve
High (>50%) mortality rate from fulminant liver failure; no longer performed

from www.utdol.com: Surgical Management of Obesity. 2006.
JEJUNOILEAL BYPASS

MALABSORPTIVE PROCEDURES (cont’d)
• BILIOPANCREATIC DIVERSION:Partial gastrectomy with remainder of stomach anastomosed to ileumLong Roux limb (bypassed portion) with short common channel (food + secretions)
• BPD W/ DUODENAL SWITCH:Similar to BPD, but gastrectomy preserves pylorus, creating “gastric sleeve”

from www.utdol.com:Surgical Options for Obesity. 2006.
BPD & BPD w/ DUODENAL SWITCH

RESTRICTIVE PROCEDURES
INTRAGASTRIC BALLOON:
Deflated balloon inserted into stomach antrum then filled with 400-600 ml saline
Not available in US; widely used in Brazil and Europe
Limited long-term efficacy—transient weight loss

from www.obezitecerrahisi.com
INTRAGASTRIC BALLOON

RESTRICTIVE PROCEDURES (cont’d)
VERTICAL BANDING:
“Stomach stapling”
Small upper portion of stomach partitioned and stapled, reinforced with mesh
Possible for staples to erode, cause ulcers; largely replaced by LAGB

from American Family Physician, 2006, 73(8): 1405.
VERTICAL BANDING

RESTRICTIVE PROCEDURES (cont’d)
LAPAROSCOPIC ADJUSTABLE GASTRIC BANDING (LABG):
Prosthetic band (ring-shaped) laparoscopically placed around entrance to stomach
Band connected via tubing to port placed in subQ tissue; tightness of band adjusted by injecting saline into the band thereby reducing its diameter

from American Family Physician, 2006, 73(8): 1405.
LAP ADJUSTABLE BANDING

MALABSORPTIVE + RESTRICTIVE
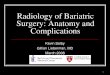
ROUX-EN-Y GASTRIC BYPASS:Small proximal gastric pouch divided and separated from
rest of stomach; food passes through thisLarger portion receives no food but secretion of gastric
acid, pepsin, intrinsic factor continuesShort proximal (biliopancreatic) limb, the Y-loop, transports
secretions from pancreas, liver, gastric remnantLonger distal portion, the Roux limb, anastomosed to small
pouch and receives its foodY-loop and Roux limb connected distally to feed into
jejunum; most digestion in this common channel

from American Family Physician, 2006, 73(8): 1404.
ROUX-EN-Y GASTRIC BYPASS

BARIATRIC SURGERY NOS
GASTRIC PACING
The next surgical miracle? Not so much.
Problems with electrodes limiting this method.
Potential to alter gastric motility/emptying, altering sensation of “fullness”
Check back in another 8-10 years….

POST-OP COMPLICATIONS
• Phase I: one to six weeks
• Phase II: seven to twelve weeks
• Phase III: thirteen wks to 12 months
Overall operative mortality = 1%

POST-OP COMPLICATIONS: PHASE I
Medical:
-pulmonary embolism
(1%)
-myocardial infarction
-respiratory failure
-pneumonia
-urinary tract infection
Surgical:
-anastomotic leak
(2-3%)
-postop bleeding
-bowel perforation
-bowel obstruction
-wound infections

POST-OP COMPLICATIONS PHASE II
RESTRICTIVE:-staple line disruption or
band erosion-stomal stenosis-pouch/esophageal
dilatation-port failure-GERD/ulcers-infection (foreign body)
ROUX-EN-Y:-gastric remnant
distention perf-stomal stenosis-wound infection-cholelithiasis-ventral hernia-incisional hernia

POST-OP COMPLICATIONS PHASE III
-GERD/esophagitis/gastritis
-small bowel obstruction
-staple/band erosion
-dehydration due to severe constipation or freq vomiting

POST-OP DIETARY PLAN
• Immediately postop for 24 hrs: Water and sugar-free clear liquids (30 mL q2 while awake).
• One day to two weeks postop: High protein liquid diet (ex: Boost HP, Ensure Plus, Carnation Instant Breakfast). – Patients should generally consume 30 to 60 mL q2
while awake, and the liquid diet should be supplemented with add’l water and sugar-free clear liquids to maintain adequate fluid intake.

POST-OP DIETARY PLAN (cont’d)
Two to four weeks postop: Pureed diet (eg, yogurt, soups, cottage cheese, eggs, protein shakes, soft vegetables).
• Focus on sources of protein, ingesting 1 to 1.5 g of protein per kg ideal body weight (approx 75 g protein/d).
• Eat about 3 oz four to six times daily and drink water and sugar-free clear liquids.
• Eat slowly (no more than 1 oz every 10 minutes), stop eating if feeling full, do not consume food and beverages at the same time (drink beverages 30 minutes before or 60 minutes after eating).
• Vomiting frequently occurs if food is ingested too quickly or if too much food is eaten.

POST-OP DIETARY PLAN (cont’d)
Four to six weeks postoperatively: Transition diet (ex: sliced deli meats, cheeses, salads, chili, fruits) in addition to the pureed diet.
• Careful chewing is essential during the transition diet. Try different foods one at a time in small quantities (one bite) during this phase. If the trial of the new food is tolerated it can be added to the list of transition foods.
• The stomach pouch begins to tolerate larger quantities of food during this phase, and eating frequency can be decreased to three small meals per day with two to three snacks.

POST-OP DIETARY PLAN (cont’d)
• After six weeks: Solid food phase – Solid foods should be encouraged at each meal. If
portion sizes remain small, two snacks should be added to the diet to prevent rapid weight loss.
– As the patient transitions from a liquid diet to solid food, there are often food intolerances associated with vomiting. Foods that commonly cause intolerance include:
-Red meats -Bread-Corn -Fruits with Seeds-Rice -High fat foods

LONG-TERM CONSEQUENCES
Nutritional deficiencies• Anemia: Fe-def v. megaloblastic [B12, folate]• Wernicke encephalopathy (ophthalmoplegia,
nystagmus, ataxia) [B1=thiamine]• Secondary hyperparathyroidism [Ca2+, Vit D]• Osteopenia [Ca2+, Vit D]• Alopecia [Zn]• Coagulopathy [Vit K]

LONG-TERM CONSEQUENCES (cont’d)
• Dumping syndrome– Cholinergic response to undigested carbs in jejunum– N/V, diarrhea, tachy, salivation, dizziness
• -Cholelithiasis– Rapid weight loss increases lipogenicity of bile,
increasing stone formation– Lap chole often performed at time of RYGB

LONG-TERM CONSEQUENCES
• Depression-extreme wt loss physiologically causes lethargy, sadness; body is in “starvation mode”-coping with inability to enjoy food as previously-possible rejection from partner, friends
• Plastic surgery-high risk for panniculitis post bariatric surgery-panniculectomy recommended but often not covered by insurance; up to 15 kg excess skin typically removed

NUTRITIONAL SUPPLEMENTATION
• Vit B12: 1000mcg IM q 6 months for life or 1000mcg SL qwk.
• MVI with trace minerals (eg, Centrum Silver). May require a liquid vitamin preparation because pills are not tolerated by the stomach pouch.
• Vit D: MVI supplement should contain 800 IU of vitamin D; if it contains only 400 IU of vitamin D, take additional 400 IU daily either as a separate supplement or by taking a second MVI.
• Calcium: 1200 to 1500 mg qd. Calcium citrate better absorbed than calcium carbonate after RYGB.
• FeSO4: if at risk for iron deficiency,take 325 mg/d prophylactically. If development of iron deficiency anemia, take 640 mg/d. Iron absorption is improved when iron is administered along with vitamin C.
• Thiamine 50mg daily if persistent vomiting or inadequate nutrient intake.

SUCCESS RATES
Swedish Obese Subjects Study• Severely obese (BMI>34 male, >38 female)• 4047 pts followed to 2 yrs,1703 pts to 10 yrs• Wt loss 23.4% in surgical grp, 1.9% control at 10
years• Resolution of diabetes, hypertriglyceridemia, low
HDL, hyperuricemia• No detectable effect on HTN or
hypercholesterolemia

PRIMARY CARE FOLLOW-UP
• Q3 months in first year– CBC, glucose, creatinine
• Q6 months in first year– LFT, Fe, ferritin, TIBC, B12, folate, calcium,
PTH
• Annually forever– All of the above

PRIMARY CARE FOLLOW-UP (cont’d)
• Psychosocial acceptance
• Monitor DM, HTN meds; may be able to wean quickly
• Monitor cardiopulmonary status: may have decreased needs, especially in patients with OSA

SPECIAL CONSIDERATIONS
• CHILDREN AND ADOLESCENTS– Extremely limited data re: safety, efficacy– Markedly increased risk of complications from
nutritional deficits– Possible higher yield in life-years preserved
• PREGNANCY– Pregnancy contraindicated within 18 mo of surgery– High-risk OB necessitated due to nutritional
deficiencies– Extremely high risk for neural tube defects– Marked increase in fertility with weight loss post-op

CASE PRESENTATION: CONCLUSION
CT abdomen/pelvis:
• Thickened transverse, ascending, & descending colonic wall, fat stranding
• Retroperitoneal ascites
• Diverticulosis
• GB distention, CBD dilatation w/o GB thickening or stones

CASE PRESENTATION: CONCLUSION
Patient frustrated with prolonged ED workup and stay; refused admission. Signed AMA papers.
Agreed to take PO Metronidazole and Ciprofloxacin and go to PMD appt next day.
PMD contacted following day, patient no-showed to appointment.
To be continued??

REFERENCESBoan J. Management of patients after bariatric surgery. www.uptodate.com. 2006.Davis MM, et al. National trends in bariatric surgery, 1996-2002. Archives of Surgery. 2006. 141:
71-4.Goldfeder LB et al. Fatal complications of bariatric surgery. Obesity Surgery. 2006. 16: 1050-6.Helling TS, et al. Determinants of the need for intensive care and prolonged mechanical ventilation in
patients undergoing bariatric surgery. Obesity Surgery. 2004. 14(8): 1036-41.Inge TH, et al. A critical appraisal of evidence supporting a bariatric surgical approach to weight
management for adolescents. The Journal of Pediatrics. 2005, Jul. 10-19.Sanchez VM, et al. Complications of bariatric surgery. www.uptodate.com. 2006.Sanchez VM, et al. Surgical management of morbid obesity. www.uptodate.com. 2006.Sjorstrom L, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery.
New England Journal of Medicine. 2004. 351(26): 2683-93.Still CD. Management of morbid obesity: before and after surgery: the team approach to
management. Journal of Family Practice. 2005. Suppl:S18-25.Ukleja A, Stone RL. Medical and gastroenterologic management of the post-bariatric surgery patient.
The Journal of Clinical Gastroenterology. 2004. 38(4): 312-21.Villagra VG. A primer on bariatric surgery: Treatment of last resort for morbid obesity. Supplement to
Disease Management. 2004: 7(1): S-23-30.Virji A & Murr MM. Caring for patients after bariatric surgery. American Family Physician. 2006.
73(8): 1403-8.Xanthakos SA, Inge TH. Nutritional consequences of bariatric surgery. Current Opinion in Clinical
Nutrition and Metabolic Care. 2006. 9: 489-96.