Embed Size (px)
Citation preview
Barrett’s EsophagusBarrett’s Esophagus
Stuart Jon Spechler, M.D.Chief of Gastroenterology, Dallas VA Medical Center;
Professor of Medicine,Berta M. and Cecil O. Patterson Chair in Gastroenterology,
UT Southwestern Medical Center at Dallas, Texas
• A 58 year-old, obese white man has had heartburn for more than 20 years.
• He read a magazine article saying that heartburn is a risk factor for Barrett’s esophagus, which can lead to cancer of the esophagus.
• The article scared him, and he asks you what he should do.
• The article went on to say that people with heartburn should have an endoscopy to look for Barrett’s esophagus.
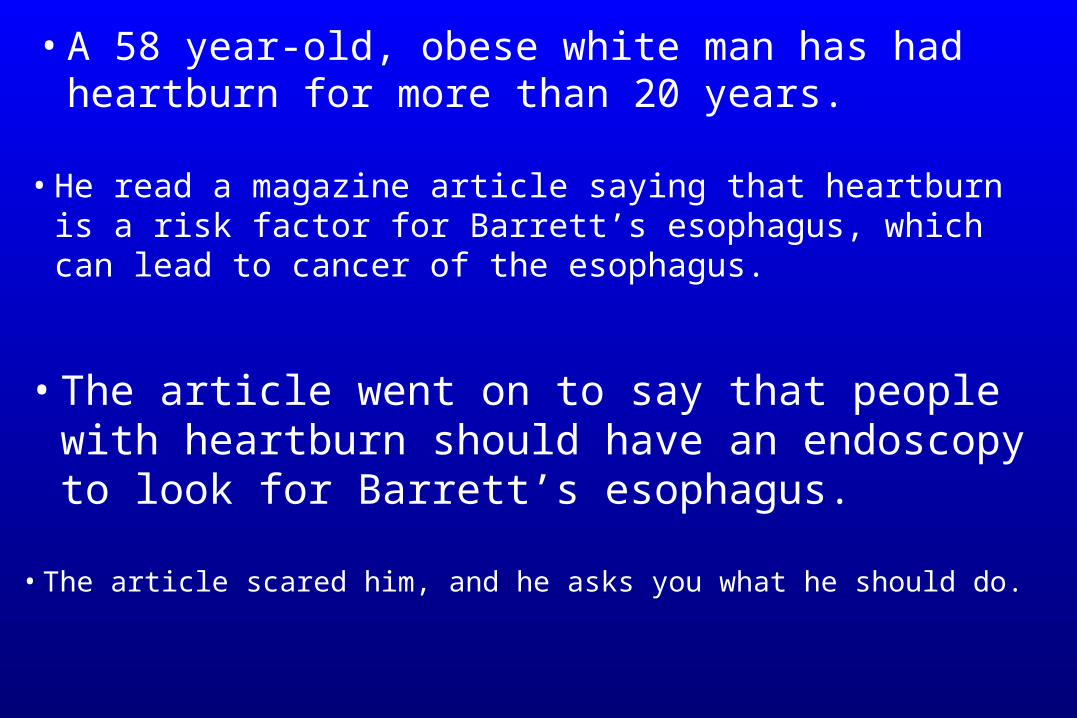
• Endoscopy reveals Barrett’s esophagus.
• Biopsy specimens show high-grade dysplasia.
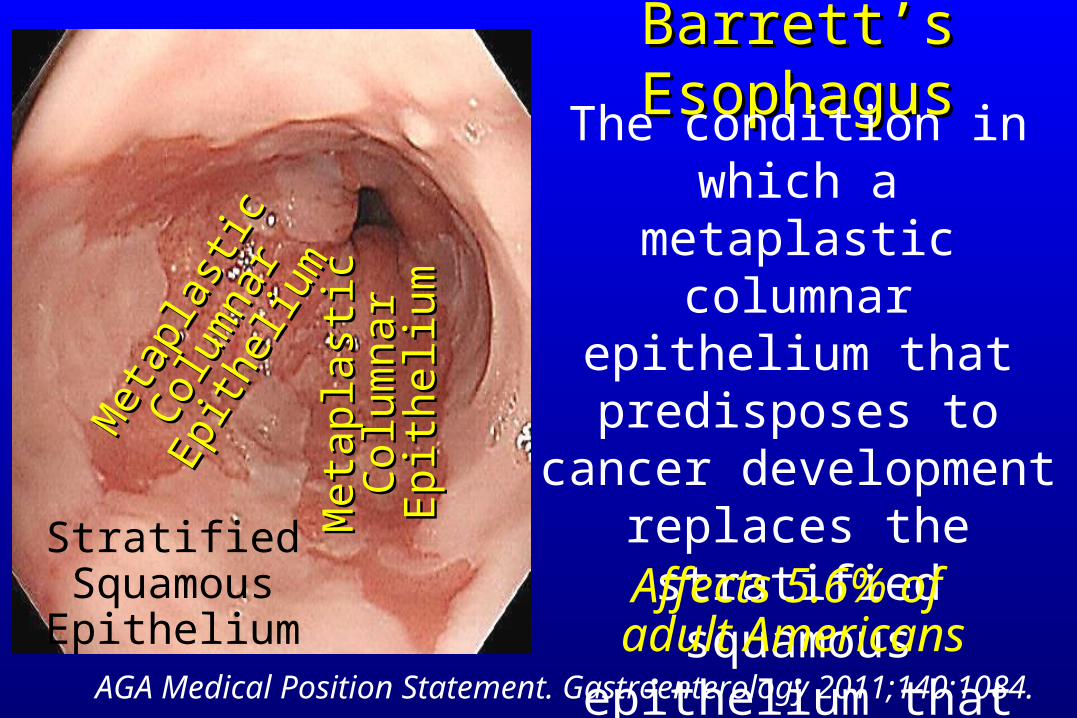
Barrett’s EsophagusBarrett’s EsophagusThe condition in which a
metaplastic columnar epithelium that predisposes
to cancer development replaces the stratified
squamous epithelium that normally lines the distal
esophagus
AGA Medical Position Statement. Gastroenterology 2011;140:1084.
StratifiedSquamousEpithelium
Met
apla
stic
Met
apla
stic
Col
umna
r
Col
umna
rEp
ithel
ium
Epith
eliu
m
Met
apla
stic
Met
apla
stic
Col
umna
rC
olum
nar
Epi
thel
ium
Epi
thel
ium
Affects 5.6% of adult Americans
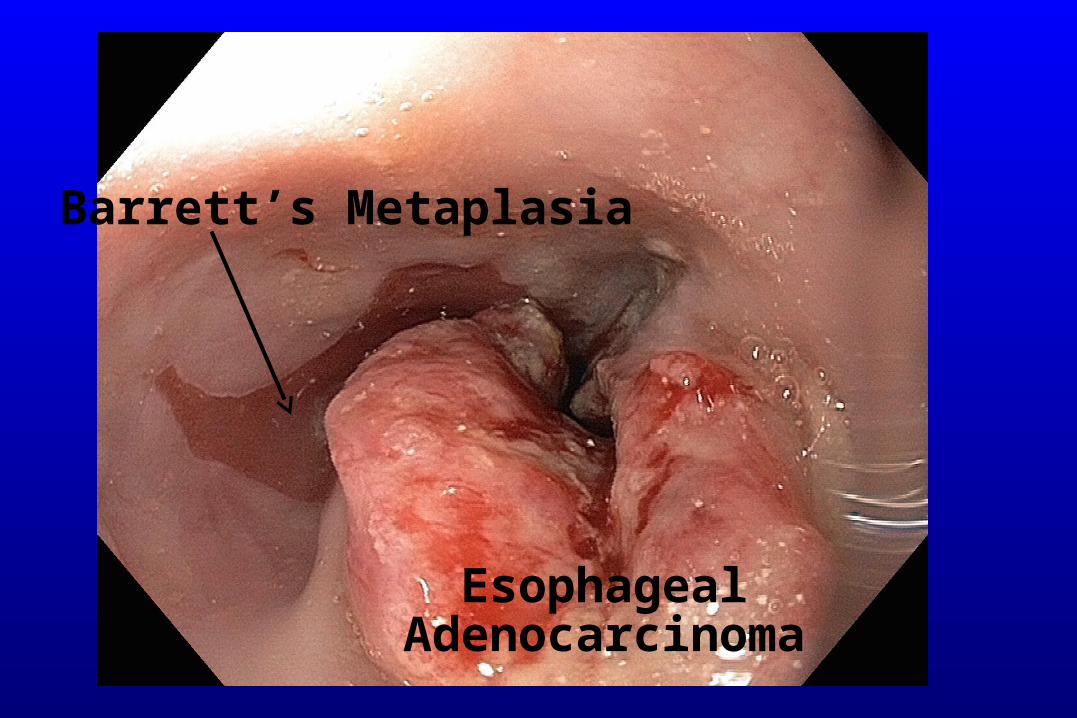
Barrett’s Metaplasia
EsophagealAdenocarcinoma
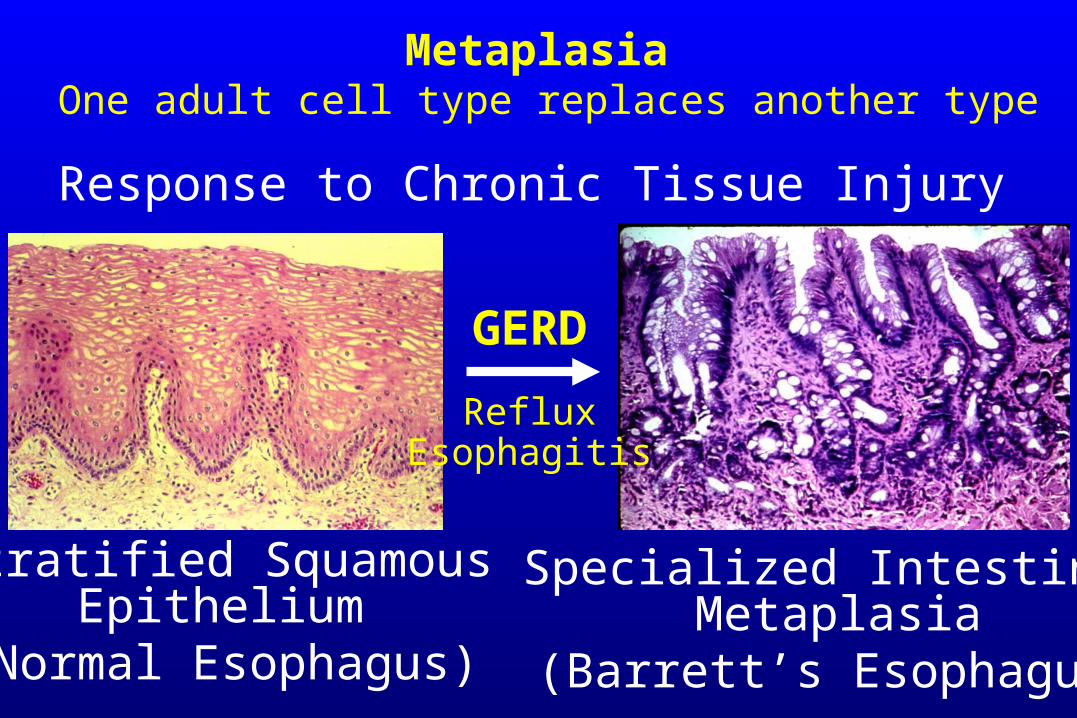
Metaplasia One adult cell type replaces another type
GERD
Stratified SquamousEpithelium
(Normal Esophagus)
Specialized IntestinalMetaplasia
(Barrett’s Esophagus)
Response to Chronic Tissue Injury
RefluxEsophagitis

GEJ(Gastro-Esophageal
Junction)
Z-Line(Squamo-Columnar
Junction)
Columnar LinedEsophagus
Adapted from Spechler. Gastroenterology 1999;117:218.
X
Specialized IntestinalMetaplasia
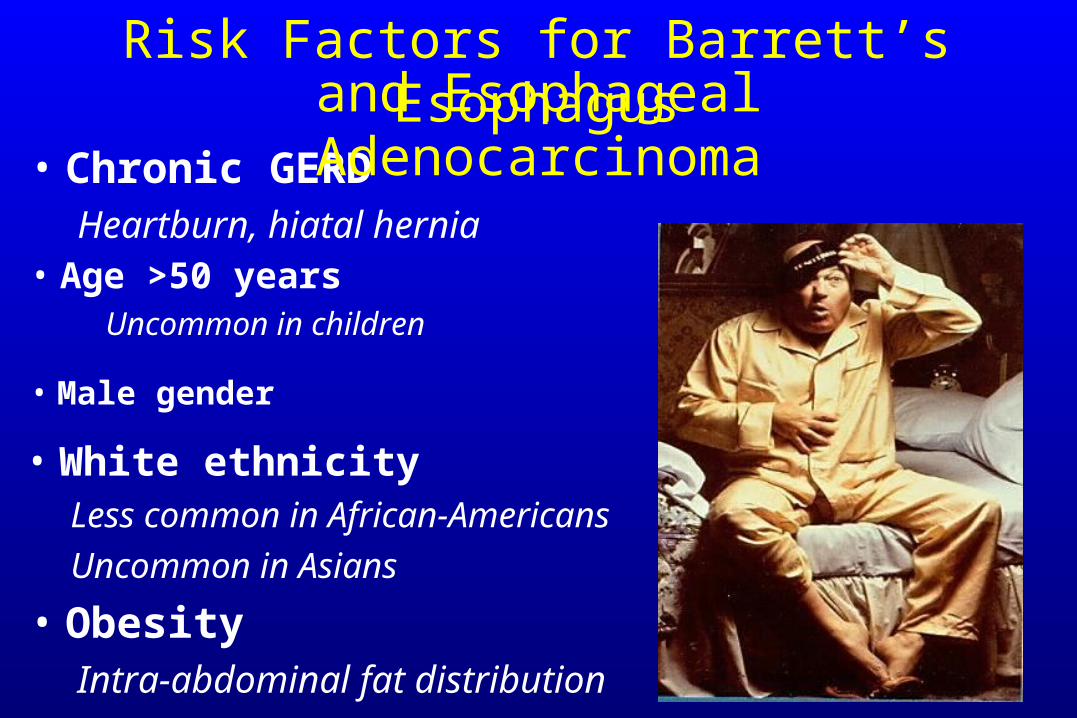
• Age >50 years Uncommon in children
Risk Factors for Barrett’s Esophagus
• Chronic GERDHeartburn, hiatal hernia
• ObesityIntra-abdominal fat distribution
• Male gender
• White ethnicityLess common in African-Americans
Uncommon in Asians
and Esophageal Adenocarcinoma
Guidelines for Endoscopy in GERD
• “Upper endoscopy is not required in the presence of typical GERD symptoms.”
• “Endoscopy is recommended in the presence of alarm symptoms and for screening of patients at high risk for complications [Barrett’s esophagus].”
ACG Guidelines. Katz. Am J Gastroenterol 2013;108:308.
ACP Guidelines. Shaheen. Ann Intern Med 2012;157:808.
• “Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting).”
• “Upper endoscopy is indicated in men and women with typical GERD symptoms that persist despite a therapeutic trial of 4 to 8 weeks of twice-daily proton pump inhibitor therapy.”

Gastroenterology 2011;140:1084.
AGA Medical Position Statement on Endoscopic Screening for Barrett’s Esophagus• We recommend against screening the general
population with GERD for Barrett’s esophagus.
• In patients with multiple risk factors associated with esophageal adenocarcinoma, we suggest screening for Barrett’s esophagus.Chronic GERD, hiatal hernia, age ≥50, male gender, white race, elevated BMI, intra-abdominal body fat distributionNorman
Barrett
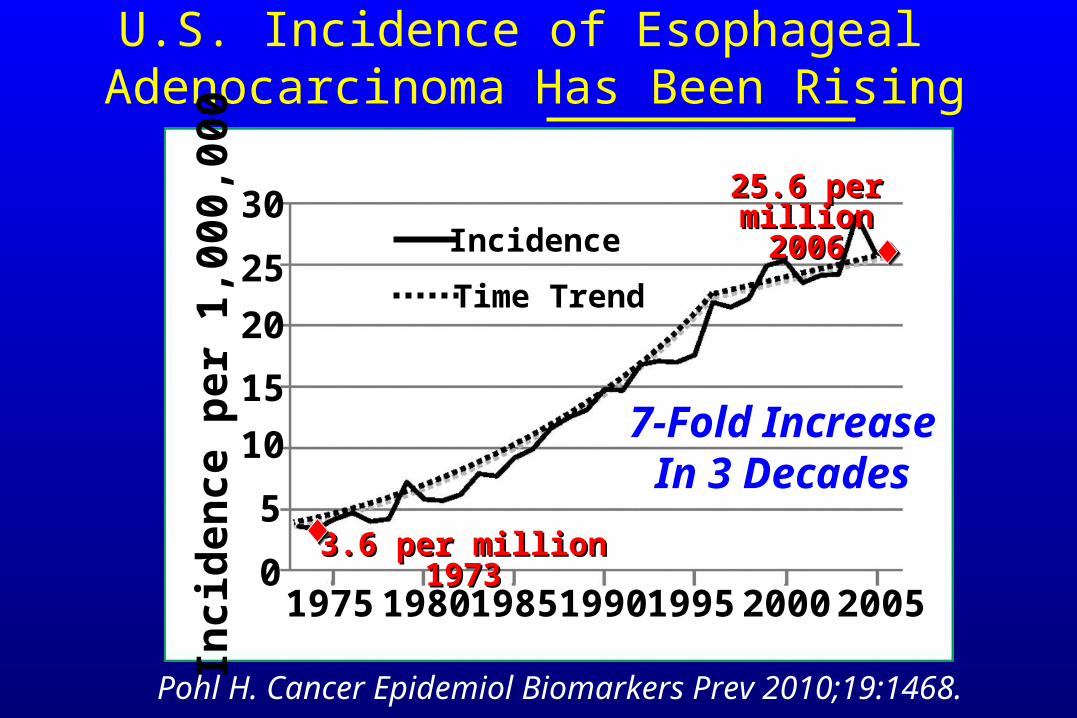
U.S. Incidence of Esophageal Adenocarcinoma Has Been Rising
1975 1980 1985 1990 1995 2000 20050
5
10
15
20
25
30In
cid
ence
per
1,0
00,0
00Incidence
Time Trend
Pohl H. Cancer Epidemiol Biomarkers Prev 2010;19:1468.
3.6 per million 19733.6 per million 1973
25.6 per 25.6 per millionmillion
20062006
7-Fold IncreaseIn 3 Decades
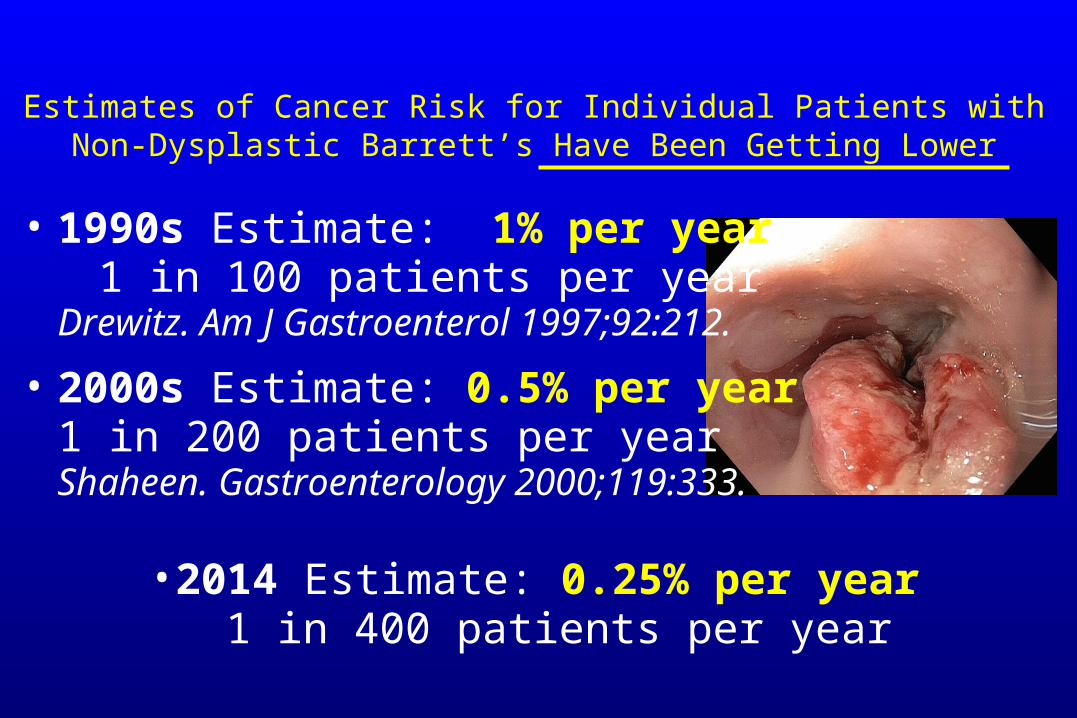
• 2000s Estimate: 0.5% per year1 in 200 patients per yearShaheen. Gastroenterology 2000;119:333.
• 1990s Estimate: 1% per year 1 in 100 patients per year
Drewitz. Am J Gastroenterol 1997;92:212.
• 2014 Estimate: 0.25% per year1 in 400 patients per year
Estimates of Cancer Risk for Individual Patients with Non-Dysplastic Barrett’s Have Been Getting Lower
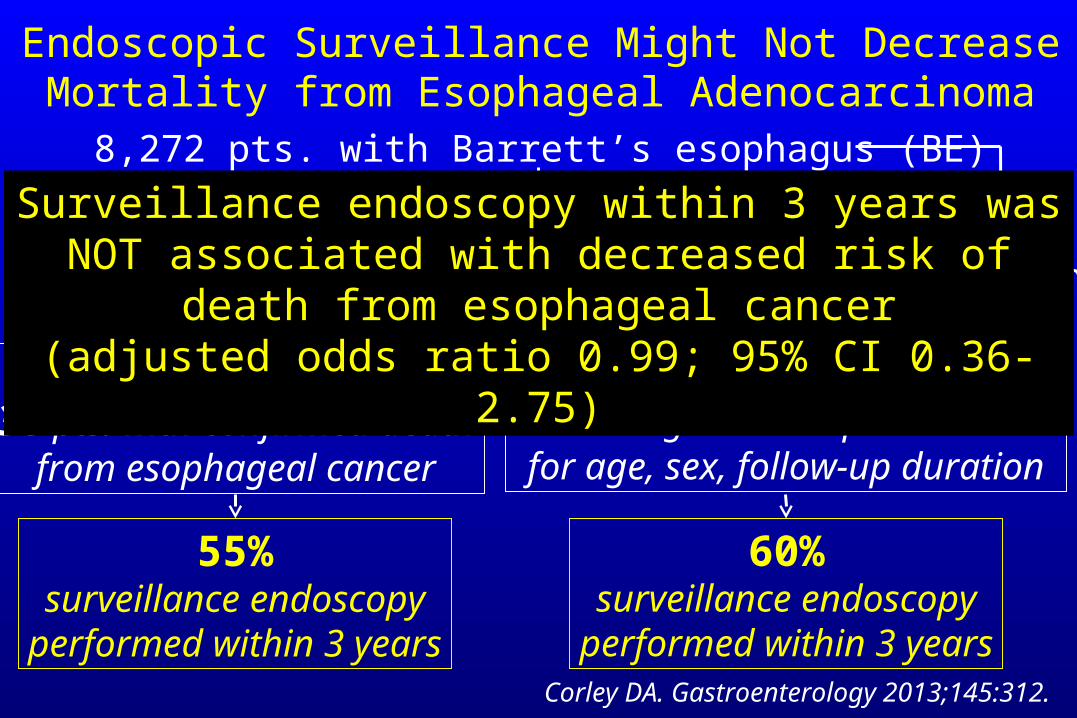
Endoscopic Surveillance Might Not Decrease Mortality from Esophageal Adenocarcinoma
Corley DA. Gastroenterology 2013;145:312.
8,272 pts. with Barrett’s esophagus (BE)
351 pts. with esophageal adenocarcinoma (EAC)
70 EAC in pts. with prior diagnosis of BE (≥6 months)
Cases38 pts. with confirmed death
from esophageal cancer
Controls101 living Barrett’s pts. matchedfor age, sex, follow-up duration
55%surveillance endoscopy
performed within 3 years
60%surveillance endoscopy
performed within 3 years
Surveillance endoscopy within 3 years was NOT associated with decreased risk of death from esophageal cancer
(adjusted odds ratio 0.99; 95% CI 0.36-2.75)
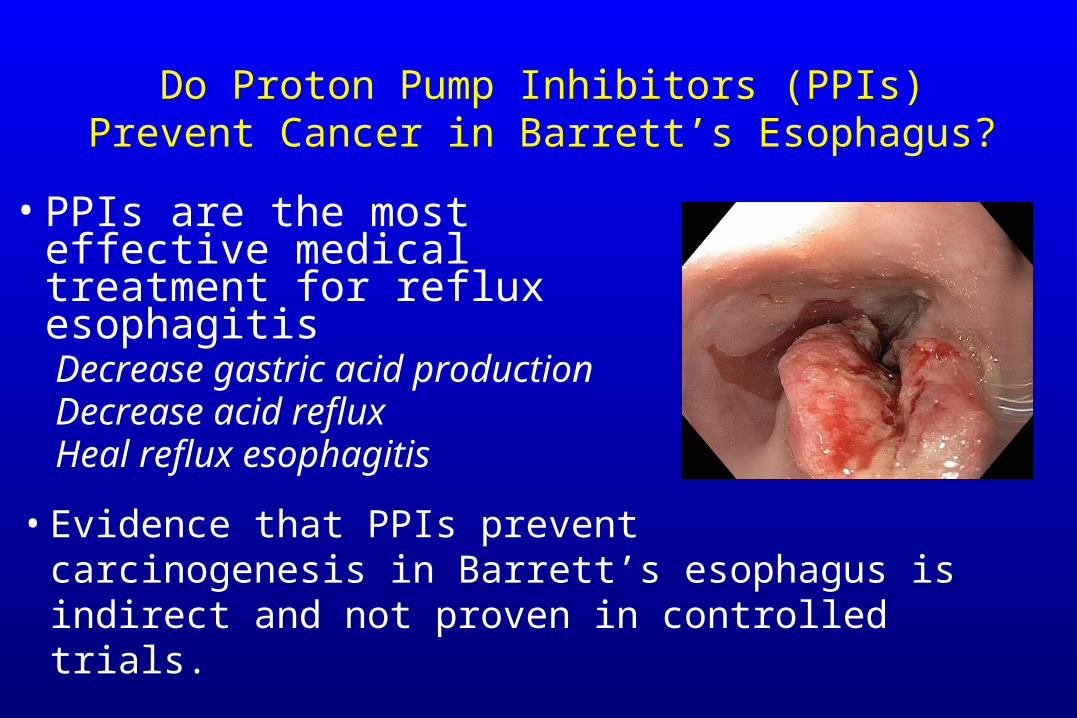
Do Proton Pump Inhibitors (PPIs) Prevent Cancer in Barrett’s Esophagus?
• Evidence that PPIs prevent carcinogenesis in Barrett’s esophagus is indirect and not proven in controlled trials.
• PPIs are the most effective medical treatment for reflux esophagitisDecrease gastric acid productionDecrease acid refluxHeal reflux esophagitis
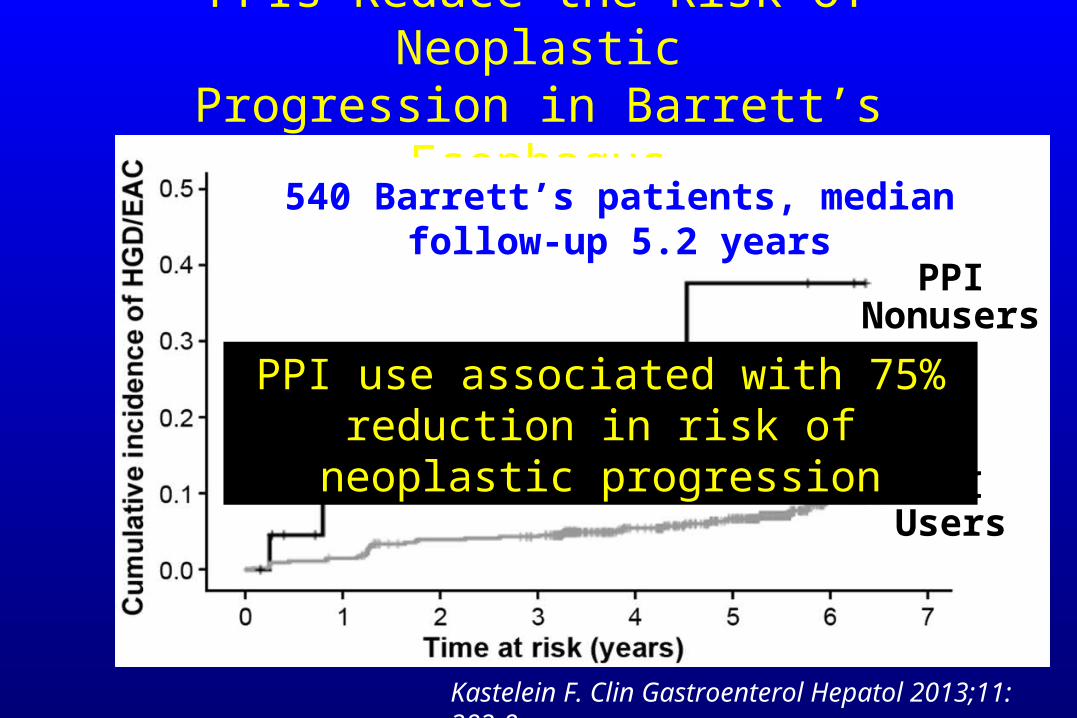
PPIs Reduce the Risk of NeoplasticProgression in Barrett’s Esophagus
PPIUsers
540 Barrett’s patients, median follow-up 5.2 years
Kastelein F. Clin Gastroenterol Hepatol 2013;11: 382-8.
PPI use associated with 75% reduction in risk of neoplastic progression
PPINonusers
Gastroenterology 2011;140:1084.
AGA Medical Position Statement on the Treatment of GERD in Barrett’s Esophagus
NormanBarrettAge 13
• GERD therapy with medication effective to treat GERD symptoms and to heal reflux esophagitis is clearly indicated.
• Antireflux surgery is not more effective than medical therapy for prevention of cancer in Barrett’s esophagus.
• We recommend against attempts to eliminate esophageal acid exposure (PPIs in doses >once daily or antireflux surgery) for cancer prevention.
Gastroenterology 2011;140:1084.
• We suggest that endoscopic surveillance [with biopsy] be performed in patients with Barrett’s esophagus.
AGA Medical Position Statement on Endoscopic Surveillance for Barrett’s Esophagus
• We suggest the following surveillance intervals:▪ No dysplasia: 3-5 years
▪ Low-grade dysplasia: 6-12 months
▪ High-grade dysplasia in the absence of eradication therapy: 3 months
NormanBarrett
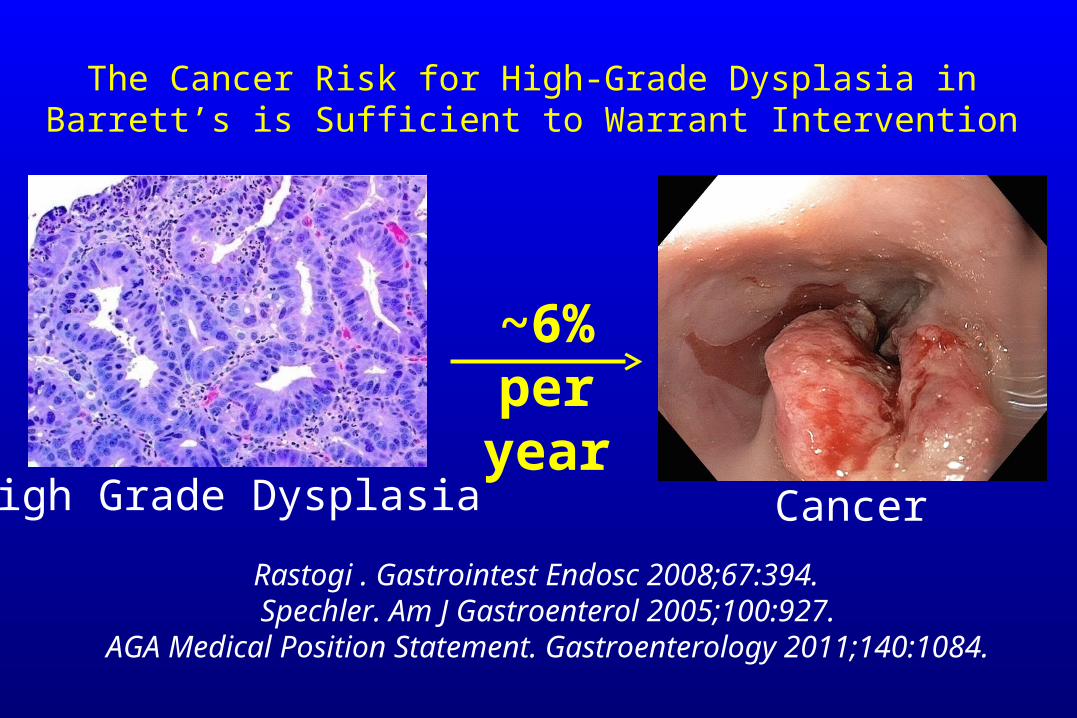
The Cancer Risk for High-Grade Dysplasia in Barrett’s is Sufficient to Warrant Intervention
Rastogi . Gastrointest Endosc 2008;67:394. Spechler. Am J Gastroenterol 2005;100:927.
AGA Medical Position Statement. Gastroenterology 2011;140:1084.
High Grade Dysplasia Cancer
~6% per year
Management Options for High-Grade Dysplasia in Barrett’s Esophagus
Intensive endoscopic surveillance (every 3 months)
Endoscopic ablation
Endoscopic mucosal resection
Esophagectomy
Gastroenterology 2011;140:1084.
• We recommend endoscopic eradication therapy rather than surveillance for treatment of
patients with confirmed high-grade dysplasia in Barrett’s
esophagus.
AGA Medical Position Statement on the Management of Barrett’s Esophagus
NormanBarrett
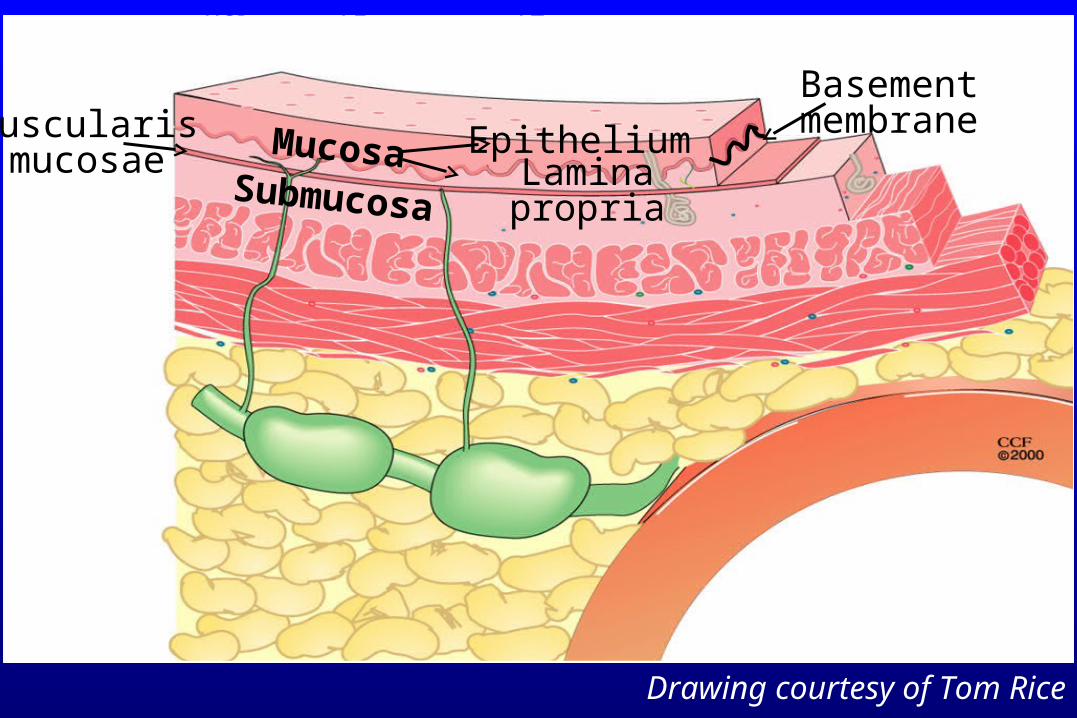
Drawing courtesy of Tom Rice
HGD T2T1
MucosaSubmucosa
Muscularismucosae
BasementmembraneEpithelium
Lamina propria
Drawing courtesy of Tom Rice
T1
T2T3 T4
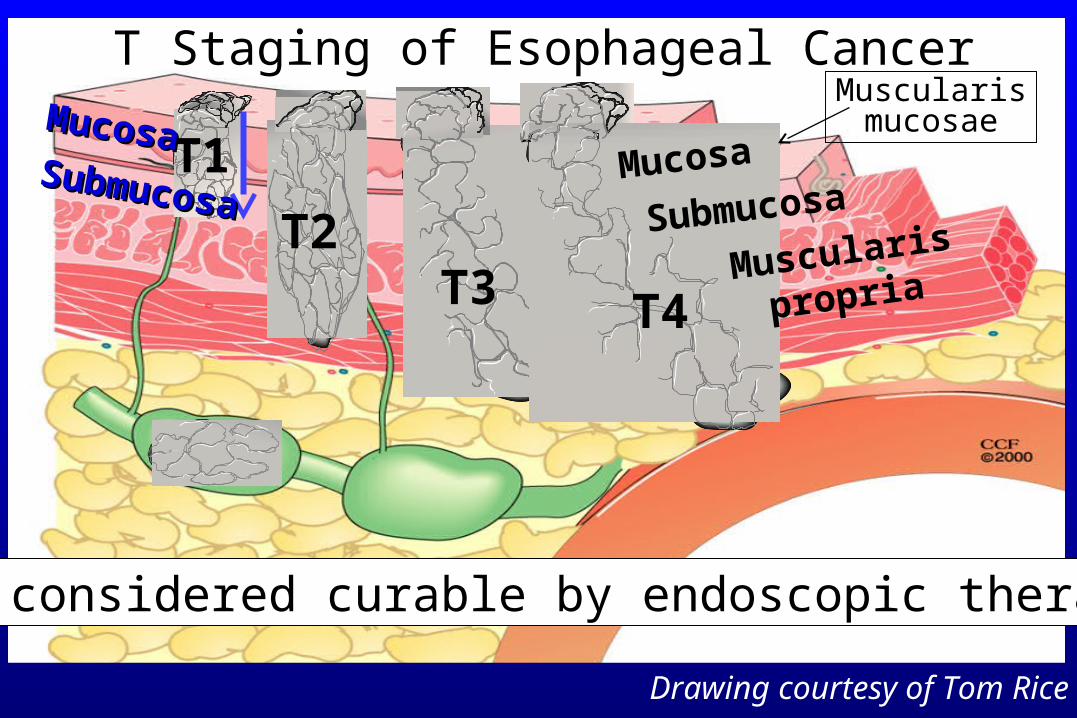
T Staging of Esophageal Cancer
None considered curable by endoscopic therapy.
Mucosa
SubmucosaSubmucosaSubmucosa
MucosaMucosaMuscularismucosae
Muscularis
propria
Drawing courtesy of Tom Rice
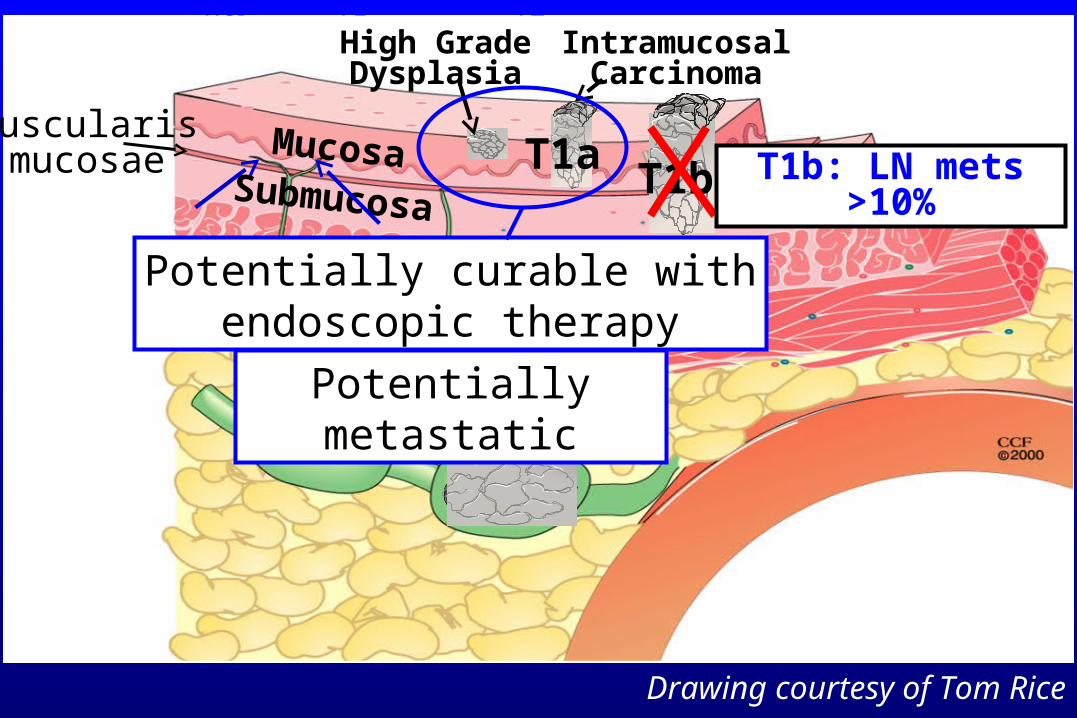
HGD T2T1
MucosaSubmucosa
IntramucosalCarcinoma
T1a
High GradeDysplasia
T1b
Potentially curable withendoscopic therapy
Muscularismucosae T1b: LN mets >10%
Potentially metastatic
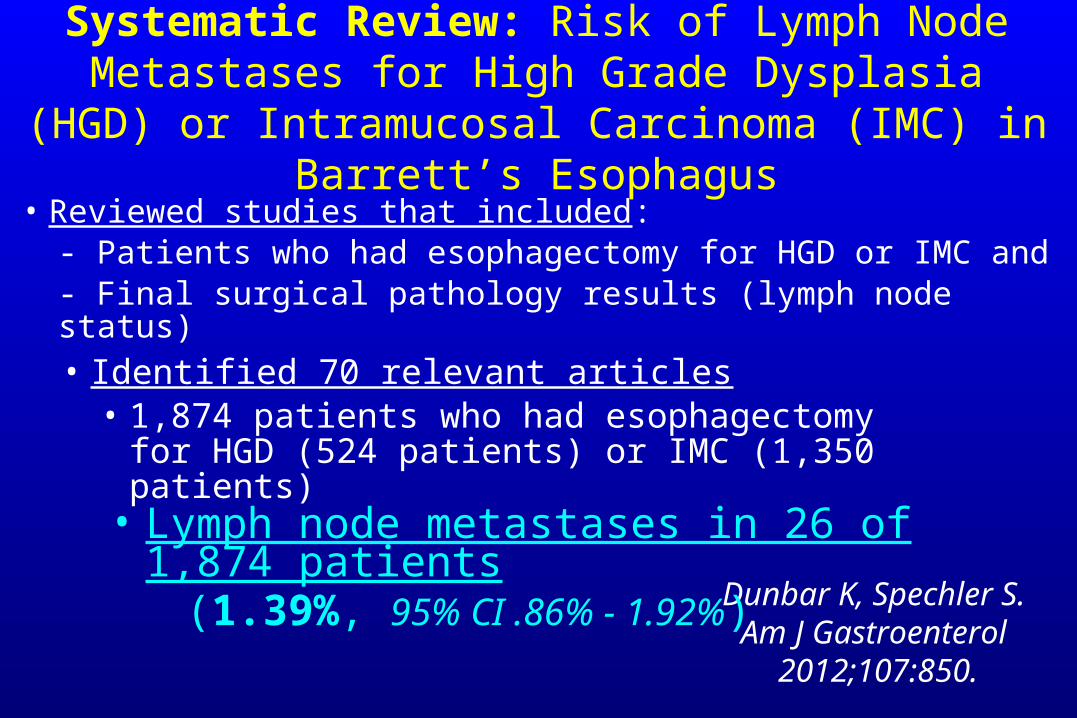
Systematic Review: Risk of Lymph Node Metastases for High Grade Dysplasia (HGD) or Intramucosal Carcinoma
(IMC) in Barrett’s Esophagus
Dunbar K, Spechler S. Am J Gastroenterol
2012;107:850.
• Reviewed studies that included:- Patients who had esophagectomy for HGD or IMC and- Final surgical pathology results (lymph node status)• Identified 70 relevant articles
• 1,874 patients who had esophagectomy for HGD (524 patients) or IMC (1,350 patients)
• Lymph node metastases in 26 of 1,874 patients (1.39%, 95% CI .86% - 1.92%)
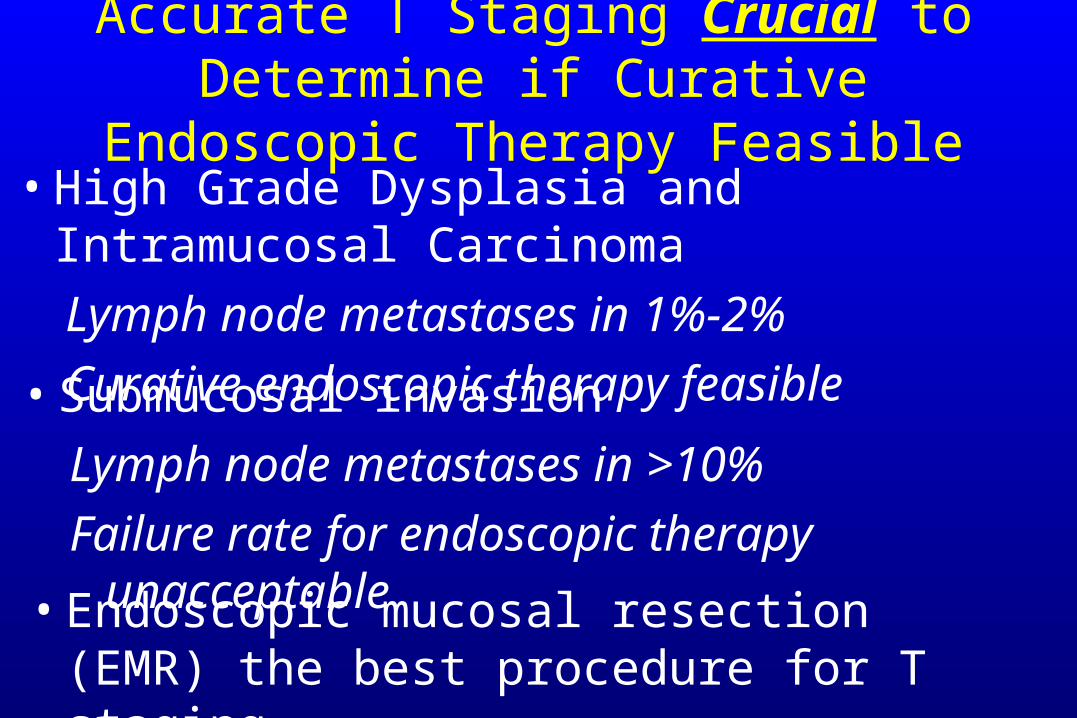
Accurate T Staging Crucial to Determine if Curative Endoscopic Therapy Feasible
• High Grade Dysplasia and Intramucosal Carcinoma
Lymph node metastases in 1%-2%
Curative endoscopic therapy feasible• Submucosal invasion
Lymph node metastases in >10%
Failure rate for endoscopic therapy unacceptable
• Endoscopic mucosal resection (EMR) the best procedure for T staging
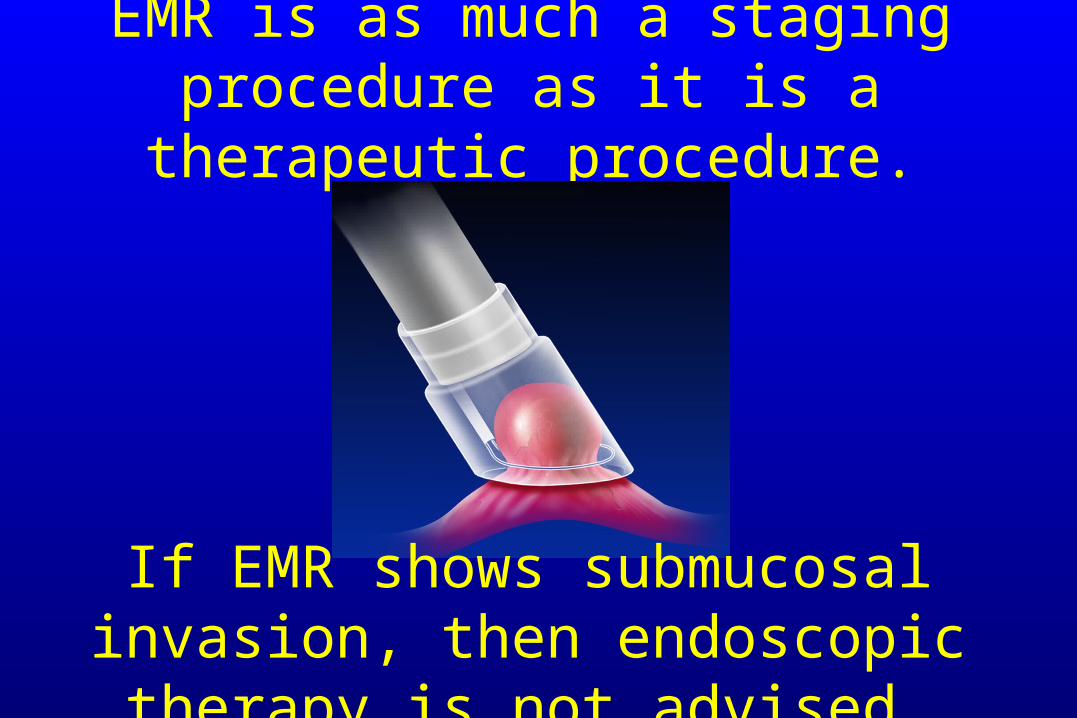
EMR is as much a staging procedure as it is a therapeutic procedure.
If EMR shows submucosal invasion, then endoscopic therapy is not advised.
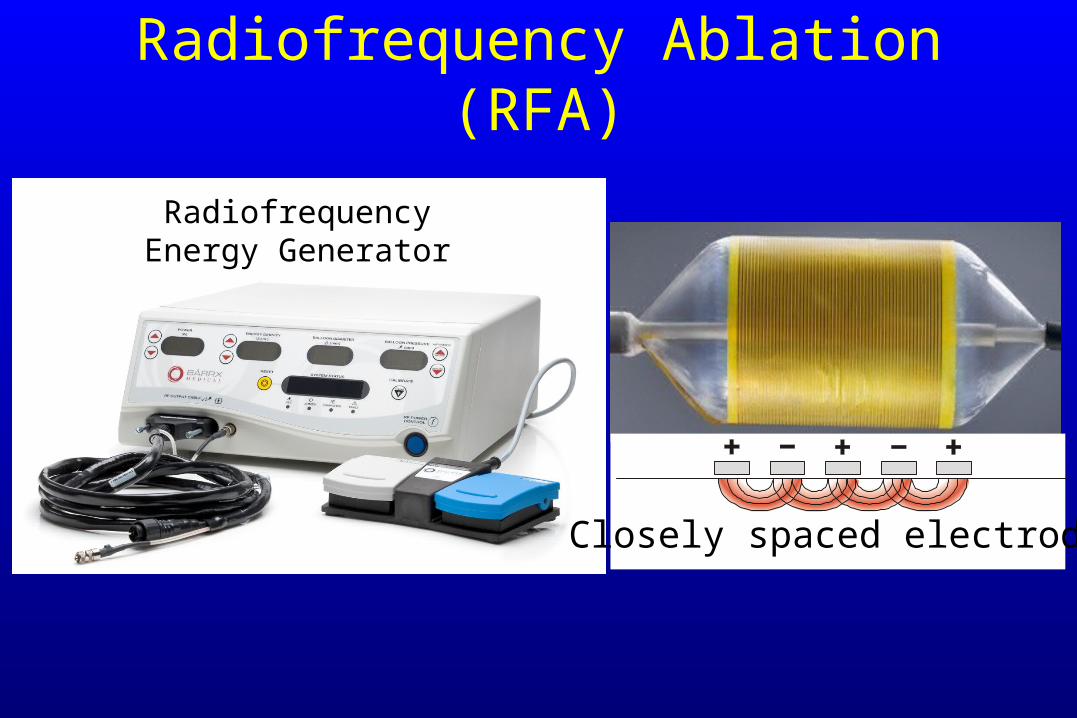
Radiofrequency Ablation (RFA)
RadiofrequencyEnergy Generator
Closely spaced electrodes
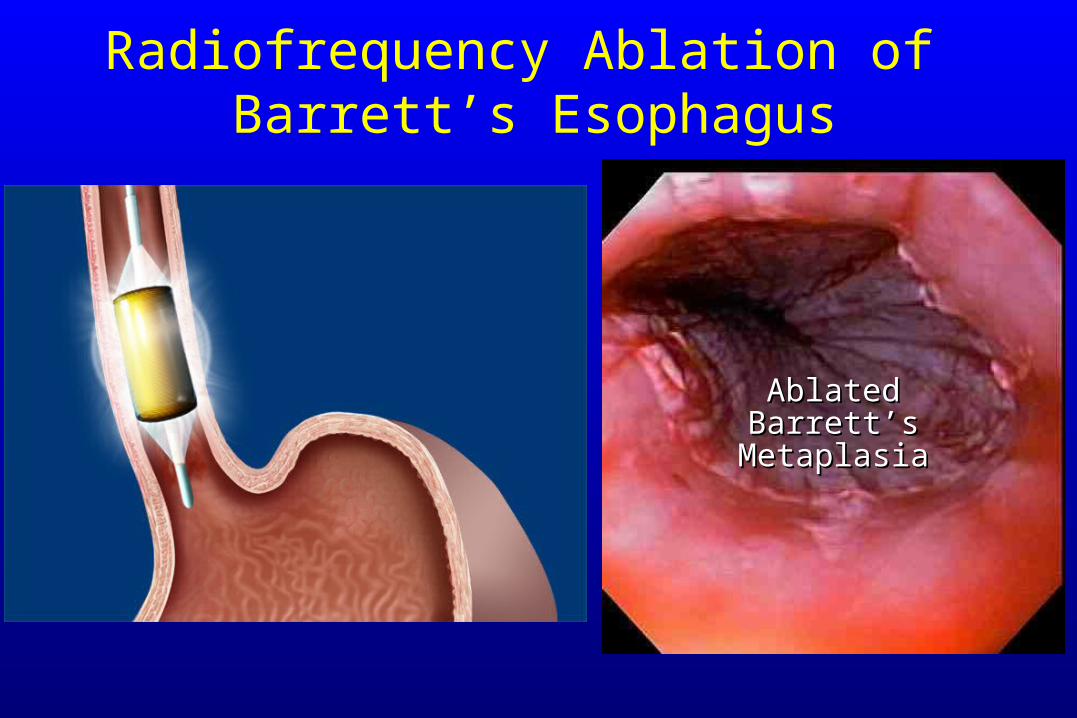
Radiofrequency Ablation of Barrett’s Esophagus
AblatedAblatedBarrett’sBarrett’s
MetaplasiaMetaplasia
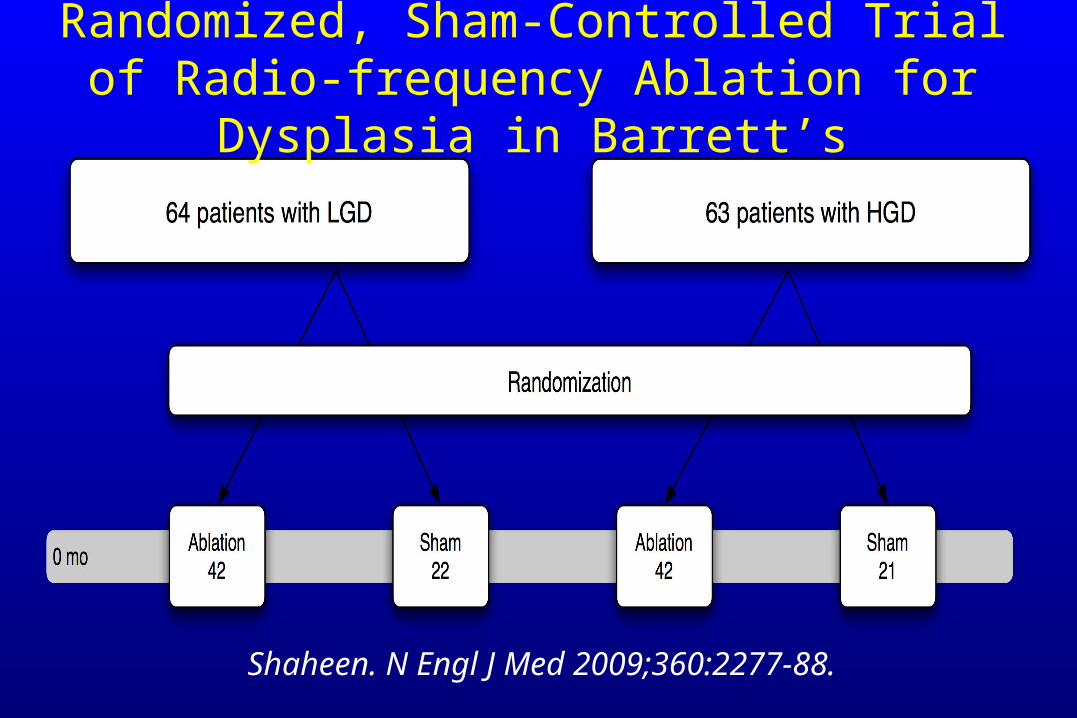
Shaheen. N Engl J Med 2009;360:2277-88.
Randomized, Sham-Controlled Trial of Radio-frequency Ablation for Dysplasia in Barrett’s
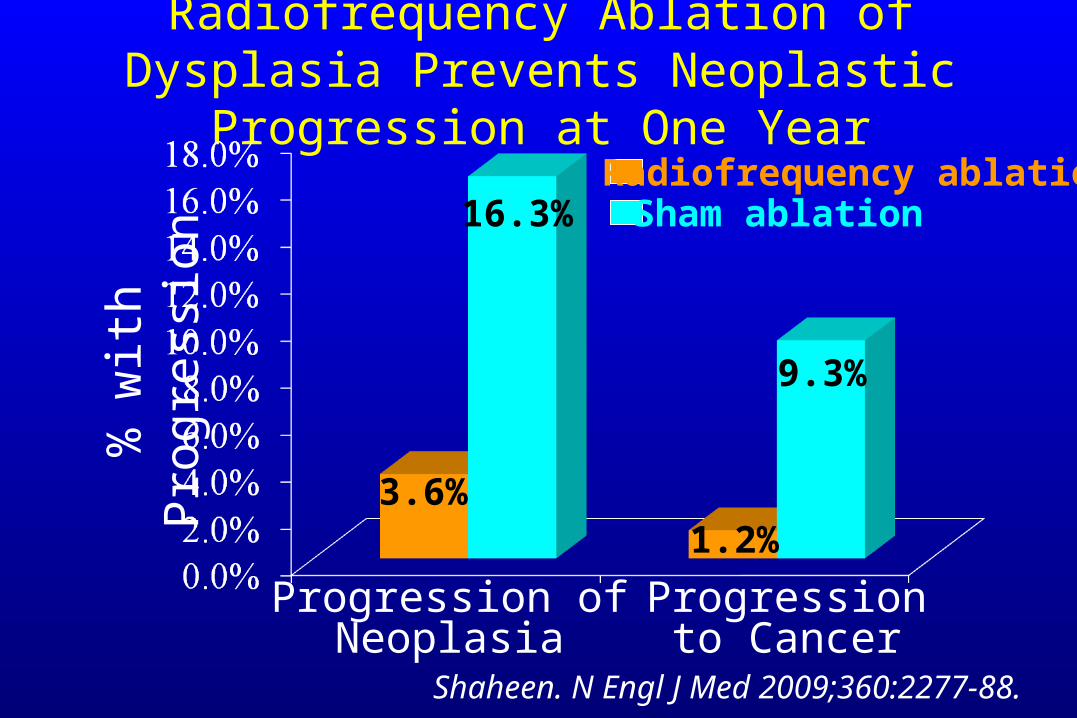
Radiofrequency Ablation of Dysplasia Prevents Neoplastic Progression at One Year
% w
ith
Pro
gres
sion
Progression ofNeoplasia
Progressionto Cancer
Radiofrequency ablationSham ablation
3.6%
16.3%
1.2%
9.3%
Shaheen. N Engl J Med 2009;360:2277-88.
Complications of Radiofrequency Ablation in 84 Patients
5 esophageal strictures (6%)
1 UGI Bleed (1%)
2 hospitalizations for chest pain (2%)
Shaheen. N Engl J Med 2009;360:2277-88.

Endoscopic Therapy for Mucosal NeoplasiaIn Barrett’s Esophagus 2014
• EMR of mucosal irregularities for staging and therapy
• Ablate the remaining Barrett’s metaplasia to minimize metachronous neoplasia
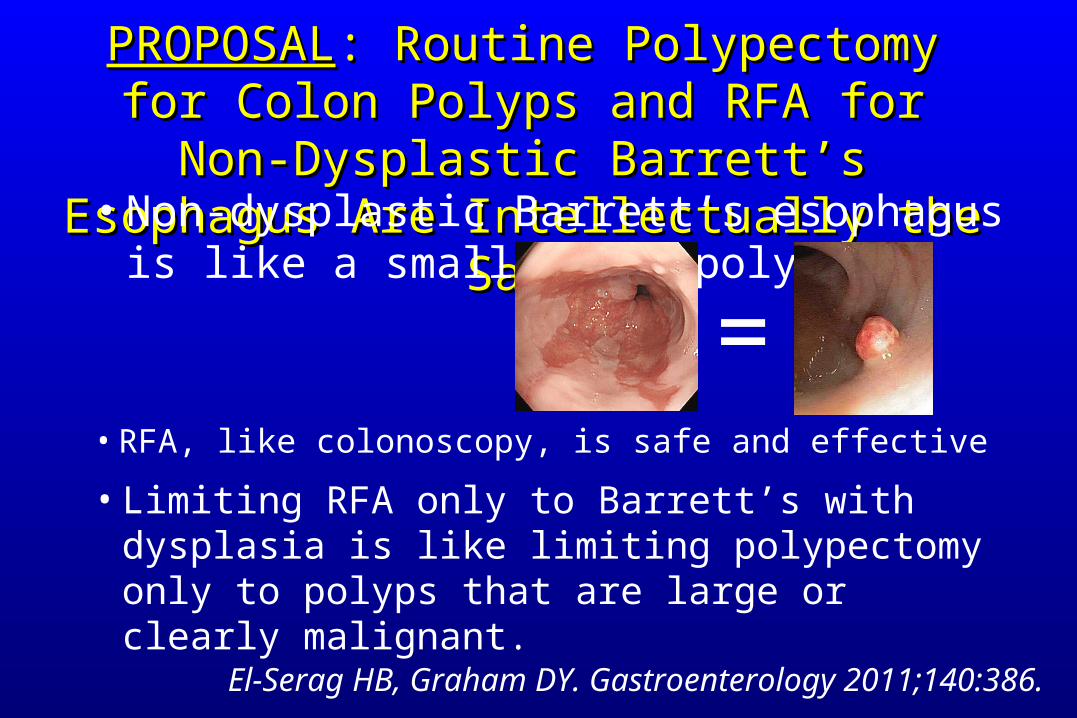
PROPOSALPROPOSAL: Routine Polypectomy for Colon : Routine Polypectomy for Colon Polyps and RFA for Non-Dysplastic Barrett’s Polyps and RFA for Non-Dysplastic Barrett’s
Esophagus Are Intellectually the SameEsophagus Are Intellectually the Same
El-Serag HB, Graham DY. Gastroenterology 2011;140:386.
• RFA, like colonoscopy, is safe and effective
• Non-dysplastic Barrett’s esophagus is like a small colon polyp
• Limiting RFA only to Barrett’s with dysplasia is like limiting polypectomy only to polyps that are large or clearly malignant.
=
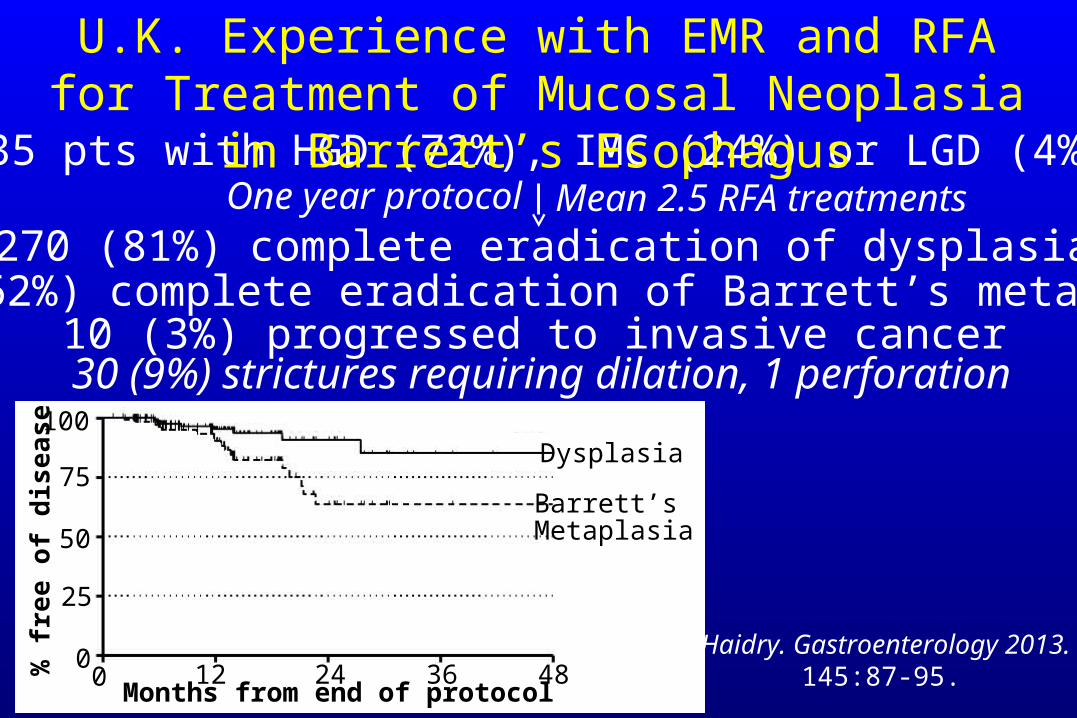
335 pts with HGD (72%), IMC (24%) or LGD (4%)
270 (81%) complete eradication of dysplasiaMean 2.5 RFA treatments
Haidry. Gastroenterology 2013. 145:87-95.
U.K. Experience with EMR and RFA for Treatment of Mucosal Neoplasia in Barrett’s Esophagus
208 (62%) complete eradication of Barrett’s metaplasia10 (3%) progressed to invasive cancer
30 (9%) strictures requiring dilation, 1 perforation
One year protocol
120 24 36 48Months from end of protocol
% f
ree
of d
isea
se
25
50
75
100
0
Dysplasia
Barrett’sMetaplasia
RFA for Non-Dysplastic Barrett’s Esophagus?• Generally requires several endoscopies for
complete eradication• Complication rate low, but not trivial• Substantial rate of recurrence of metaplasia
• Efficacy in preventing cancer not established
• Does not obviate surveillance
• Frequency and importance of subsquamous intestinal metaplasia not clear
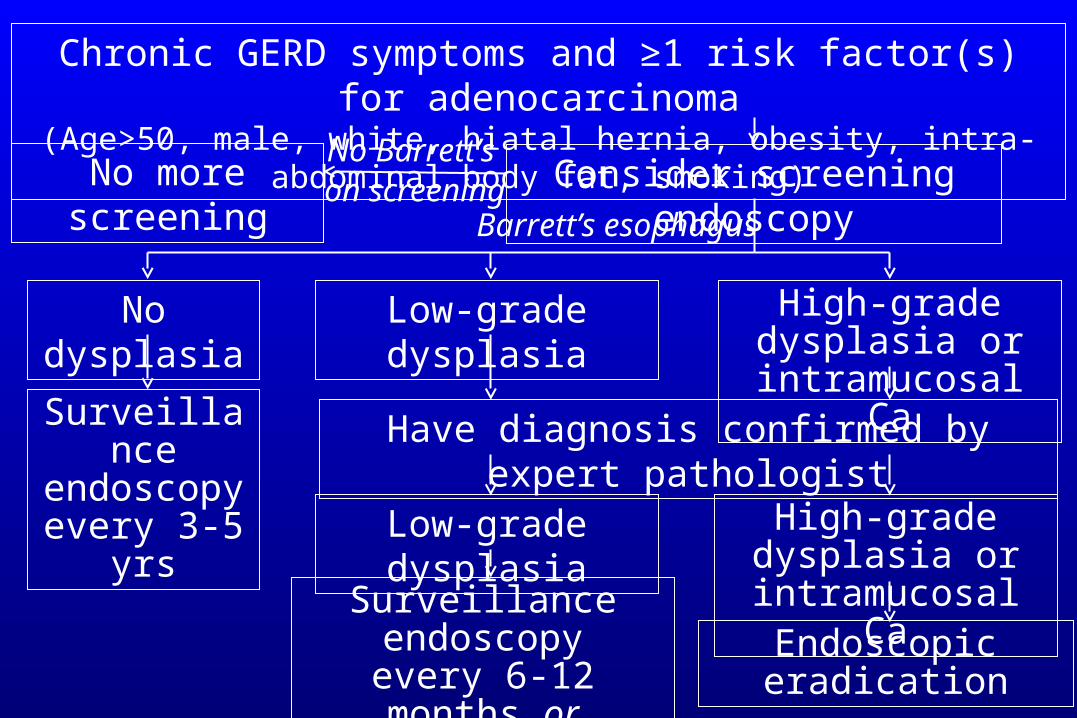
Chronic GERD symptoms and ≥1 risk factor(s) for adenocarcinoma(Age>50, male, white, hiatal hernia, obesity, intra-abdominal body fat, smoking)
Consider screening endoscopyNo more screeningNo Barrett’s
No dysplasia Low-grade dysplasia High-grade dysplasia or intramucosal Ca
Have diagnosis confirmed by expert pathologist
Low-grade dysplasia High-grade dysplasia or intramucosal Ca
Surveillanceendoscopy
every 3-5 yrs
Endoscopic eradicationSurveillance endoscopyevery 6-12 months or
endoscopic eradication
on screeningBarrett’s esophagus
AGA Medical Position Statement on the Management of Barrett’s Esophagus
Gastroenterology 2011;140:1084.
• Endoscopic eradication therapy is not suggested for the general population of patients with Barrett’s esophagus in the absence of dysplasia.
• RFA should be a therapeutic option for select individuals with non-dysplastic Barrett’s esophagus who are judged to be at increased risk for progression to HGD or cancer.
Specific criteria that identify this population have not been fully defined.Norman
Barrett
• Knowledge is knowing a tomato is a fruit.
• Wisdom is knowing not to put it in a fruit salad.

![Barrett’s esophagus and new therapeutic modalitiesThe prevalence of Barrett’s esophagus in the adult population is 0.4–1.6% [1,3,12,13]. Assum-ing a US adult population in 2007](https://img.pdfslide.net/doc/110x75/5f4d5b4d6dfbad3c763bb443/barrettas-esophagus-and-new-therapeutic-modalities-the-prevalence-of-barrettas.jpg)