Embed Size (px)
Citation preview

Base di evidenza relativa al trattamento dietetico dell’IRC in fase sostitutiva -
emodialisi
Giorgio Bedogni
www.giorgiobedogni.it 1
Base di evidenza relativa al trattamentodietetico dell'IRC in fase sostitutiva -
emodialisi
Giorgio Bedogni
www.giorgiobedogniit

Argomenti
• La malnutrizione protido-energetica in emodialisi
• La “reverse epidemiology” in emodialisi
www.giorgiobedogni.it 2
Argomenti
• L a malnutrizione protido-energetica in emodialisi
• L a "reverse epidemiology" in emodialisi
www.giorgiobedogniit 2

Altri argomenti
• Saranno affrontati in dettaglio da F Pasticci e AL Fantuzzi
www.giorgiobedogni.it 3
Altri argomenti
• Saranno affrontati in dettaglio da F Pasticci e ALFantuzzi
www.giorgiobedogniit 3

Programma
• La malnutrizione protido-energetica in emodialisi
• La “reverse epidemiology”
www.giorgiobedogni.it 4
Programma
• L a malnutrizione protido-energetica in emodialisi
• L a "reverse epidemiology"
www.giorgiobedogniit 4

Malnutrizione e dialisi
• La malnutrizione protido-energetica (PEM, protein energy malnutrition) è comune nei pazienti emodializzati (sino al 40%)
• (Solito problema del confronto di stime ottenute con metodi differenti) http://www.kidney.org/professionals/kdoqi/guidelines_updates/nut_a02.html
www.giorgiobedogni.it 5
Malnutrizione e dialisi
• L a malnutrizione protido-energetica (PEM, proteinenergy malnutrition) è comune nei pazienti emodializzati(sino al 40%)
• (Solito problema del confronto di stime ottenute conmetodi differenti)
http://wwwkidneyorg/professionals/kdoqi/guidelines updates/nut_a02.html
www.giorgiobedogniit

Malnutrizione e dialisi
• I pazienti con PEM hanno una mortalità aumentata http://www.kidney.org/professionals/kdoqi/guidelines_updates/nut_a02.html
• (Persiste il problema del confronto di indicatori differenti)
• Sorprendentemente, non sono state effettuate rassegne
sistematiche se non per l’albumina e la proteina C-reattiva e soltanto piuttosto recentemente (2010)
www.giorgiobedogni.it 6
Malnutrizione e dialisi
• I pazienti con PEM hanno una modalità aumentata
http://wwwkidneyorg/professionals/kdogi/guidelines updates/nut a02.html
• (Persiste il problema del confronto di indicatori differenti)
• Sorprendentemente, non sono state effettuate rassegnesistematiche se non per l'albumina e la proteina O-reattiva e soltanto piuttosto recentemente (2010)
www.giorgiobedogniit 6

Proteine sieriche e mortalità
www.giorgiobedogni.it 7
ELSEV1ER
Proteine sieriche e mortalità
Nutrition 26 (2010) 10-32
Review a r t i *
NUTRITION
www.nutritionjml.com
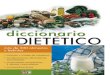
Relationship between serum protein and mortality in adults on long-termhemodialysis: Exhaustive review and meta-analysis
Marietjie Herselman, Ph.D.", Nazeema Esau, 13.Sc. Dieteficsa, Jeanne-Marie Kruger, M.Nutr.a,Demetre Labadarios, M.B., Ch.13., Ph.D.b, and M. Rafique Moosa, M.D.'
aDivision of HUM1111 Nutrition, Stellenbosch University and Tvgerberg Academie. Hospital, Tygerberg, Sondi AfricabKnowledge Systems., Human Sci ences Research Council and Tygerberg Academie Hospital, Tygerberg, South Africa
'Department of Medicine, Stellenbosch University and Tygerberg Acuti emie Hospital, Tygerberg, Sondi Africa
Manuscript received Fehmary 25, 2009; accepted July 30, 2009.
www.giorgiobedogniit 7

www.giorgiobedogni.it 8
irralevant and duplicataabstract. apicluded
(Pg = 1550)
Excluded (N = 235) •No adiustme-t(or zonfoundors (51)
Insufficiant monellitv data ce PEM risk facbors (105)Fun papars noi available 115)
Noi restriczad lo HD (23)No rnortality outcpme (20)
Childran included (10)Review Depor (6)
Duplicabon (5)
Studies excluded (N .= 131)•insufficient reortality cala un risk laCtUrS (07)
Noi limitad h e m o d i a l y s e (47)Children included (15)
Deedair (15)Roview piacer (2)
Acute ronal (aduna included 11)No acpustment for confounding factors (1)
StageTitles and abstracts undergoing liberai screening
for relevancy (MEM(N = 2005)
Stage 2Potentially relevant Nies and abstracts undergoingindependent screening for inclusimi in the review
(MIRM. NE. MH)(N = 445)
Stage 3Data extraction and further screening of fui) papers
(MH. NE. MAK)(N1 = 210)
Stud . excludad frum rnata-analysisdue :o incompleto statstical data c ,
radequate number of studia., bui stili •included in systamatic review
(N = 41)
Stage 4Studies undergoing quality
assessment and included in final review(MH. JMK)
(N = 79)
Stage 5Studies included in meta-analysis
(N = 38)
www.giorgiobedogni.it 8

Albumina e mortalità
www.giorgiobedogni.it 9
Table 3Subgroup analysis for serum albumin (HR with 95% CI)
Groups (no. of studies) HR 95% CI Difference between subgmups (P)
Lower limit Upper limit
AH studies combined (n - 33) 0.7355 0.6775 0.7984All-cause mortality (n = 25) 0.7038 0.6367 0.7781 0.0014Cardioyascular mortality (n = 8) 0.8726 0.7909 0.9628
All-cause mortality only (n = 25)*Prospective (n = 16) 0.7803 0.7141 0.8526 0.0748Retmspective (n = 9) 0.6759 0.5680 0.8044Lower-quality study (n = 12) 0.6553 0.5330 0.8057 0.0678Higher-quality study (n = I I ) 0.7774 0.7123 0.8485Adjusted for infiarnmation (n=10) 0.7790 0.6886 0.8811 0.0406Not adjusted far infiammation (n = 13) 0.6595 0.5729 0.7593Duration 0-3 y (n =14) 0.6403 0.5418 0.7566 0.0116Duration >3 y (n =11) 0.8070 0.7233 0.9005Patients <60 y (n = 12) 0.6013 0.5019 0.7204 0.0012Patients >60 y (n = 11) 0.8328 0.7468 0.9287Sample size <225 (n = 13) 0.8102 0.7206 0.8909 0.0236Sample size >225 (n = 12) 0.6702 0.5821 0.7716Not adjusted far KVV (n = 17) 0.6767 0.5895 0.7769 0.0027Adjusted for K IN (n = 4) 0.8651 0.7798 0.9597Not adjusted for comorbidity (n = 3) 0.4721 0.2440 0.9134 0.1144Adjusted for comorbidity (n = 18) 0.7120 0.6367 0.7960
Albumina e mortalità
www.giorgiobedogniit
CI, conlidence interval; HR, hazard ratio; KtN, adequacy of dialysisExcluding studies reporting un cardloyascular mortality and studies with incomplete data un subgroup categories.
9

Proteina C-reattiva e mortalità
• Pooled results for C-reactive protein showed a weak but significant direct relation with all-cause mortality (HR 1.0322, 95% CI 1.0151–1.0496), but there was not a significant relation between C-reactive protein and cardiovascular mortality (HR 1.0172, 95% CI 0.9726-1.0639).
www.giorgiobedogni.it 10
Proteina C-reattiva e mortalità
• Pooled results for C-reactive protein showed a weak butsignificant direct relation with all-cause mortality (HR1.0322, 95% CI 1.0151-1.0496), but there was not asignificant relation between C-reactive protein andcardiovascular mortality (HR 1.0172, 95% CI0.9726-1.0639).
www.giorgiobedogniit lo

Malnutrizione e infiammazione
• Protein-energy malnutrition (PEM) and inflammation are common and usually concurrent in maintenance dialysis patients. Many factors that appear to lead to these 2 conditions overlap, as do assessment tools and such criteria for detecting them as hypoalbuminemia. Kalantar-Zadeh K. Am J Kidney Dis. 2003;42:864.
www.giorgiobedogni.it 11
Malnutrizione e infiammazione
• Protein-energy mainutrition (PEM) and inflammation arecommon and usually concurrent in maintenance dialysispatients. Many factors that appear to lead to these 2conditions overiap, as do assessment tools and suchcriteria for detecting them as hypoalbuminemia.
Kalantar-Zadeh K. Am J Kidney Dis. 2003;42:864.
www.giorgiobedogniit

Malnutrizione e infiammazione
• PEM in dialysis patients has been suggested to be secondary to inflammation; however, the evidence is not conclusive, and an equicausal status or even opposite causal direction is possible. Hence, malnutrition-inflammation complex syndrome (MICS) is an appropriate term. Kalantar-Zadeh K. Am J Kidney Dis. 2003;42:864.
www.giorgiobedogni.it 12
Malnutrizione e infiammazione
• PEM in dialysis patients has been suggested to besecondary to inflammation; however, the evidence is notconclusive, and an equicausal status or even oppositecausai direction is possible. Hence, malnutrition-inflammation complex syndrome (MICS) is anappropriate temi
Kalantar-Zadeh K. Am J Kidney Dis. 2003;42:864.
www.giorgiobedogniit 12

Malnutrizione e infiammazione
• Because MICS leads to a low body mass index, hypocholesterolemia, hypocreatininemia, and hypohomocysteinemia, a “reverse epidemiology” of cardiovascular risks can occur in dialysis patients. Kalantar-Zadeh K. Am J Kidney Dis. 2003;42:864.
www.giorgiobedogni.it 13
Malnutrizione e infiammazione
• Because MICS leads to a low bodv mass index,hypocholesterolemia, hvpocreatininemia, andhypohomocvsteinemia, a "reverse epidemiology" ofcardiovascular risks can occur in dialysis patients.
Kalantar-Zadeh K. Am J Kidney Dis. 2003;42:864.
www.giorgiobedogniit 13

Cause di PEM
• Anorexia**– Uraemic*toxicity*– Impaired*gastric*emptying*– In5lammation*with/without*co;morbid*
conditions**• Emotional*and/or*psychological*disorders*• Dietary*restrictions*
– Prescribed*restrictions:*low;potassium,*low;phosphorous*regimens*
– Social*constraints:*poverty,*inadequate*dietary*support*
– Physical*incapacity:*inability*to*acquire*or*prepare*food*to*eat*
• Nutrient*losses*during*dialysis*– Loss*through*haemodialysis*membrane*into*
dialysate*– Adherence*to*haemodialysis*membrane*or*
tubing*– Loss*into*peritoneal*dialysate*
• Hypercatabolism*caused*by*co;morbid*illness*
– Cardiovascular*disease**– Diabetic*complications*– Infection*and/or*sepsis**– Other*co;morbid*conditions**
• Hypercatabolism*associated*with*dialysis*treatment*
– Negative*protein*balance*– Negative*energy*balance*
• Endocrine*disorders*of*uraemia*– Resistance*to*insulin*– Resistance*to*growth*hormone*and/or*
insulin;growth*factor;1*– Increased*serum*level*of/or*sensitivity*to*
glucagon*– Hyperparathyroidism*
• * Other*endocrine*disorders*– Acidaemia*with*metabolic*acidosis*
*may*be*associated*with*in5lammation**
www.giorgiobedogni.it 14
Pasticci*F*et*al.*Journal*of*Renal*Care*2012;38:50.*
• A n o r e x i a *Uraemic toxicityImpaired gastric emptyingInfiammation with/without co-morbidconditions*
• E m o t i o n a l and/or psychological disorders• D i e t a r y restrictions
— Prescr ibed restrictions: low-potassium,low-phosphorous regimensSocial constraints: poverty, inadeguatedietary support
- Phys ica l incapacity: inability to acquire orprepare food to eat
• N u t r i e n t losses during dialysis— L o s s through haemodialysis membrane into
dialysateAdherence to haemodialysis membrane ortubing
- L o s s into peritoneal dialysate
Cause di PEM
Pasticci F et al. journal of Renal Care 2012;38:50.
www.giorgiobedogni.it
Hypercatabolism caused by co-morbidillness
Cardlovascular disease*Diabetic complicationsInfection and/or sepsis*Other co-morbid conditions*
Hypercatabolism associated with dialysistreatment
— Negat ive protein balance— Negat ive energy balance
Endocrine disorders of uraemiaResistance to insulinResistance to growth hormone and/orinsulin-growth factor-1Increased serum level of/or sensitivity toglucagonHyperparathyroidism
Other endocrine disorders— Ac idaemia with metabolic acidosis
*may be associated with infiammation
14

Valutazione dello stato protido-energetico
www.giorgiobedogni.it 15
http://www.kidney.org/professionals/kdoqi/guidelines_updates/nut_a02.html
Valutazione dello stato protido-energetico
Category
I. Measurements that should beperformed routinely in alipatients
Measures that can be usefulto confirm or extend the dataobtained from the measures inCategory I
III. Clinically useful measures,which, if low, might suggestthe need for a more rigorousexamination of protein-energy nutritional status
Measure
Predialysis or stabilized serumalbumin
% of usual postdialysis bodyweight, body mass indexa andinterdialytic weight gainaof standard (NHANES li) bodyweight
Subjective global assessmentDietary interview and/or diarynPNA (nPCR)Predialysis or stabilized serum
prealbumin (transthyretin)Skinfold thicknessMidarm muscle area,
circumference, or diameterDual energy x-ray
absorptiometryPredialysis or stabilized serum—Creatinine—Urea nitrogen—CholesterolCreatinine index
http://www.kidneyorg/professionalsikdogiiguidelines_updatesinut_a02.html
www.giorgiobedogniit
Minimum Frequencyof Measurement
Monthly
Monthly
Every 4 months
Every 6 monthsEvery 6 monthsMonthlyAs needed
As neededAs needed
As needed
As neededAs neededAs needed
15

Introito proteico raccomandato
• “Surprisingly few studies have assessed the dietary protein requirements for these patients. Moreover, there is not a single randomized controlled trial in which patients undergoing MHD were randomly assigned to different levels of DPI and the effect on morbidity and mortality was examined”
Kopple JD et al. Nutritional management of renal disease. Lippincott Williams & Wilkins; 2004, p. 440.
www.giorgiobedogni.it 16
Introito proteico raccomandato
• "Surprisingly few studies have assessed the dietaryprotein requirements for these patients. Moreover, thereis not a single randomized controlled trial in whichpatients undergoing MHD were randomly assigned todifferent levels of DPI and the effect on morbidity andmodality was examined"
Kopple JD et al. Nutritional management of renal disease.Lippincott Williams & Wilkins; 2004, p. 440.
www.giorgiobedogniit 16

Introito proteico raccomandato
www.giorgiobedogni.it 17
Pasticci*F*et*al.*Journal*of*Renal*Care*2012;38:50.*
Introito proteico raccomandatoHaemodialysis Peritoneal dialysis
DOQI 1 . 2 gAg IBW/day501)/0 HBV
ESPEN 1 . 2 gAg IBW/daySCW/p3 HBV
EBPG A t least 1.1 g/kg IBW/dayBalanced intake of high qualityanimai protein and vegetable
• p r o t e i n sourceEDTNNERCA 1.1-1.2 g/kg IBW/day
k501)/0 HBV
1.2-1.3 g/kg IBW/day50% HBV
g/kg IBW/day_50% HBV
Greater intake if peritonitis
1.0-1.2 g/kg IBW/day1.5 g/kg IBW/day if peritonitis_50%HBV
Table 3: Suggested protein intake for the dialysis patient.DOQI = Disease Outcomes Quality Initiative; ESPEN = EuropeanSociety for Parenteral and Enteral Nutrition; EBPG = EuropeanBest Practice Guidelines; EDTNNERCA = European Dialysis andTransplant Nurses Association/European Renal Care Association;IBW = ideai body weight; HBV = high biological value. Adaptedfrom: NKF 2000 (DOQI); Toigo et al. (2000) (ESPEN); EDTNNERCA2002; Fouque et al. (2007) (EPBG).
Pasticci F et al. journal of Renal Care 2012;38:50.
www.giorgiobedogni.it 17

Malnutrizione e infiammazione
• Because MICS leads to a low body mass index, hypocholesterolemia, hypocreatininemia, and hypohomocysteinemia, a “reverse epidemiology” of cardiovascular risks can occur in dialysis patients. Kalantar-Zadeh K. Am J Kidney Dis. 2003;42:864.
www.giorgiobedogni.it 18
Malnutrizione e infiammazione
• Because MICS leads to a low bodv mass index,hypocholesterolemia, hvpocreatininemia, andhypohomocvsteinemia, a "reverse epidemiology" ofcardiovascular risks can occur in dialysis patients.
Kalantar-Zadeh K. Am J Kidney Dis. 2003;42:864.
www.giorgiobedogniit 18

Programma
• La malnutrizione protido-energetica in emodialisi
• La “reverse epidemiology”
www.giorgiobedogni.it 19
Programma
• L a malnutrizione protido-energetica in emodialisi
• L a "reverse epidemiology"
www.giorgiobedogniit 19

“Reverse epidemiology”
www.giorgiobedogni.it 20
CARDIOVASCULAR AND SURVIVAL PARADOXES IN DIALYSIS PATIENTS
What is So Bad about Reverse Epidemiology Anyway?
Kamyar Kalantar-Zadeh
"Reverse epidemiology"
Harold Simmons Center for Kidney Diseose Research and Epidemiology. Division of Nephrology andHypertension, Los Angeles Biomedical Research Center at Harbor-UCLA, Torrance and UCLA David GeffenSchool of Medicine, Los Angeles, California
Seminars in Dialysis—Vol 20, No 6 (November-December)2007 pp. 593-601DOI: 10.1111/j.1525-139X2007.00360.x
www.giorgiobedogni.it 20

“Reverse epidemiology”
www.giorgiobedogni.it 21
1_8-
• 1.6-
w 1 4--o •"5
1.2-•_
0.6-
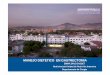
BMI associated death risk:Generai population versus hemodialysis patients
—a— General PopulationHemodialysis
"Reverse epidemiology"
BMI (kgim2)
0.49 h 9 t i , 9 9 t hN•tb. 9.9. 9 etb. 1,5 9,57 3 ‘ • s t •
< o ' e t : < f f ( D ' q 3 C 2 i 1 , 9 5 0 5 3 n i g2 : 1 1 9 -
>30
www.giorgiobedogniit
FIG. I. Crossing curves o f the Obesity Paradox: Dialysispatients vs. the generai population. Comparison between theimpacts o f body mass index (8M1) on ali cause mortaiity in thegenerai population a ) versus in maintenance hemodialysis popu-lation (À). The generai population data are adopted from Calleet ai., NEJM 1999, 341:1097 1105 (combined men and women.healthy, nonsmoker) (108). The hemodialysis data are adoptedfrom Leavey et al., Neph Dialysis Transpiant 2001. 16:2386 94(combined US and EuroN data) (109). *Note that each popula-tion has a different follow-up Nriod: 14 years for the generaipopulation vs. 4 years for hemodialysis patients. **BM1 stratifi-cations are different in two populations: X-axis is based on theoriginai graph of the generai population, and the originai hemo-dialysis 8M1 subgroup ranges are printed additionally along thehemodialysis curve. [adapted, with pennission, from Kalantar-Zadeh et al. (15)].
21

“Reverse epidemiology”
• Most recently there have even been emerging longitudinal studies showing that gaining body weight and total fat are associated with improved survival overtime.
• These apparently counterintuitive observations have been collectively referred to as ‘‘reverse epidemiology’’, ‘‘risk factor paradox’’ such as ‘‘obesity paradox’’, and ‘‘altered risk factor pattern’’.
www.giorgiobedogni.it 22
"Reverse epidemiology"
• Most recently there have even been emerginglongitudinal studies showing that gaining body weightand total fat are associated with improved survivalovedime.
• These apparently counterintuitive observations havebeen collectively referred to as "reverse epidemiology","risk factor paradox" such as "obesity paradox", and"altered risk factor pattern".
www.giorgiobedogniit

“Reverse epidemiology”
• As over two-thirds of dialysis patients are already dead within 5 years of commencing dialysis treatment, the long-term effects of conventional risk factors on future mortality is essentially irrelevant.
www.giorgiobedogni.it 23
"Reverse epidemiology"
• A s over two-thirds of dialysis patients are aiready deadwithin 5 years of commencing dialysis treatment, thelong-term effects of conventional risk factors on futuremodality is essentially irrelevant.
www.giorgiobedogniit

“Reverse epidemiology”
• What we consider ‘‘reverse’’ epidemiology, i.e., the stronger impact of undernutrition and short-term death, may indeed be the ‘‘natural’’ epidemiology of mankind.
www.giorgiobedogni.it 24
"Reverse epidemiology"
• What we consider "reverse" epidemiology, i.e., thestronger impact of undernutrition and shod-term death,may indeed be the "natural" epidemiology of mankind.
www.giorgiobedogniit

“Reverse epidemiology”
www.giorgiobedogni.it 25
"Reverse epidemiology"
TABLE 2. Possible pathophysiologie mechanisms leading tosurvival advantages of obesity in dialysis patients
Pathophysiologic mechanisms of Obesity Paradox
Time differential of competitive risk factors: overnutrition vs.undernutrition (71)
Dominant role of wasting in chronic disease states (77)Irrelevancy of risk factors of long-term mortality (68)Selected genotype resulting from survival selection over the CKDprogression (107)
Role of the visceral compartment as the source of uremic toxin(55)
Containment/storage of uremic toxins in fat tissue (24)Salutary anti-inflammatory cytokines related to fat, includingadiponectins (113)
Tumor necrosis factor alpha receptors (47)Endotoxin-lipoprotein hypothesis (49)Stability of hemodynamic status in obese patientsi (45)Neurohormonal alterations in obesity (46)Alteration of conventional risk factors in uremic milieuProtecting role of fat storage during hardship episodes in thehistory of mankind (69)
www.giorgiobedogniit 25

“Reverse epidemiology”
www.giorgiobedogni.it 26
• As physicians and scientists with professional integrity committed to the ‘‘cause-no-harm’’ motto, we should feel uneasy by the readiness with which the Liu et al. dismiss the paradoxical associations as mere confounding without biological plausibility and replace them with the more speculative concept that cholesterol should be lowered in all dialysis patients no matter what.
"Reverse epidemiology"
• A s physicians and scientists with professional integritycommitted to the "cause-no-harm" motto, we should feeluneasy by the readiness with which the Liu et al. dismissthe paradoxical associations as mere confoundingwithout biological plausibility and replace them with themore speculative con cept that cholesterol should belowered in all dialysis patients no matter what.
www.giorgiobedogniit 26

Statine, colesterolo ed emodialisi
www.giorgiobedogni.it 27
Statine, colesterolo ed emodialisi
HMG CoA reductase inhibitors (statins) for dialysis patients
Sankar D Navaneethant*, Sagar UNigwekar2, \l'ad° Perkovic3, David WJohnson4, Jonathan C Craig5, Giovanni FMStrippoli6
Editoria! Group: Cochrane Renal GroupPublished Offline: 8 JUL 2009
Assessed as up-to-date: 20 JUL 2008
D01: 10.1002/14651858,CD004289,pub4
www.giorgiobedogniit 27

Statine, colesterolo ed emodialisi
• Compared with placebo, statin use was associated with a significantly lower end of treatment average total cholesterol (14 studies, 1823 patients; MD -42.61 mg/dL, 95% CI -53.38 to -31.84), LDL cholesterol (13 studies, 1801 patients; MD -43.06 mg/dL, 95% CI -53.78 to -32.35) and triglycerides (14 studies, 1823 patients: MD -24.01 mg/dL, 95% CI -47.29 to -0.72).
www.giorgiobedogni.it 28
Statine, colesterolo ed emodialisi
• Compared with placebo, statin use was associated witha significantly lower end of treatment average totalcholesterol (14 studies, 1823 patients; MD -42.61 mg/dL,95% Ci -53.38 to -31.84), LIDL cholesterol (13 studies,1801 patients; MD -43.06 mq/dL, 95% Ci -53.78 to-32.35) and triglycerides (14 studies, 1823 patients: MD-24.01 mg/dL, 95% Ci -47.29 to -0.72).
www.giorgiobedogniit 28

Statine, mortalità ed emodialisi
• Compared to placebo, statins did not decrease all-cause mortality (10 studies, 1884 patients; RR 0.95, 95% CI 0.86 to 1.06) or cardiovascular mortality (9 studies, 1839 patients: RR 0.96, 95% CI 0.65 to 1.40).
• There was a lower incidence of nonfatal cardiovascular events with statins compared to placebo in haemodialysis patients (1 study, 1255 patients; RR 0.86, 95% CI 0.74 to 0.99).
www.giorgiobedogni.it 29
Statine, mortalità ed emodialisi
• Compared to placebo, statins did not decrease all-causemortality (10 studies, 1884 patients; RR 0.95, 95% Ci0.86 to 1.06) or cardiovascular mortality (9 studies, 1839patients: RR 0.96, 95% Ci 0.65 to 1.40).
• There was a lower incide nce of nonfatal cardiovascularevents with statins compared to placebo inhaemodialysis patients (l study, 1255 patients; RR 0.86,95% Ci 0.74 to 0.99).
www.giorgiobedogniit 29

Grazie
www.giorgiobedogni.it 30
Grazie
www.giorgiobedogniit 30