Embed Size (px)
Citation preview

Basic approach to
PFT interpretation
Dr. Giulio Dominelli
BSc, MD, FRCPC
Kelowna Respiratory and Allergy Clinic

Disclosures
Received honorarium from Astra Zeneca
for education presentations

Tasked
Asked to talk about the
interpretation of
pulmonary function tests
PFT interpretation is a
HUGE area and we could
easily spend the entire
lecture on any single
component and the
controversies within
them…

In order to tackle this, I will assume a
basic understanding of the test
mechanics, measurements,
quality control and lung physiology that is used to generate
the data….
Adapted from Pulmonary Function Tests in Clinical practice. Figures 2.1

Focus
Taking the data to the bedside

Outline
The major focus
Before the data
Flow volume loops
Spirometry
Lung volumes
Diffusion
Brief overview
Muscle strength
Methacholine
CPET
Examples
Not going to cover:
ABG, Overnight oximetry or sleep studies, walk tests

Disclaimer
There are many approaches
This is the method I take when
approaching interpretation of
PFTs
Find systematic away to
approach
Follow it for each test

Before the data
Who the test is on
Ensure the demographics make sense
Alter your expectations
Who ordered the test and why
GP vs. Specialist
What is their clinical question

Before the test
Did it meet ATS standards
Acceptability and Reproducibility
Will not focus on these criteria
Special comments
Patient effort
Problems encountered
Smoking history, other clinical symptoms


Spirometric curves - qualitative
analysis
Flow-Volume Volume-Time
Adapted from Pulmonary Function Tests in Clinical practice. Figures 1.2 and 1.11

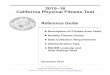
Volume-Time curve
Adequacy of the test (6 seconds)
Gives insight into pattern of disease
Obstructive vs. restrictive
http://www.nataliescasebook.com/tag/spirometry
Accessed Sep 205

Flow-Volume Curve
Ensure adequate test
Free from artefact
Insight into pattern of
disease
Obstructive or
restrictive
Screen for upper
airway obstruction
Adapted from Pulmonary Function Tests in Clinical practice. Figure 1.11

Flow-Volume Curve: Obstruction
Low peak flows
Expiratory limb is
concave or ‘scooped’
Total volume is
typically lower
Adapted from Pulmonary Function Tests in Clinical practice. Figure 1.18

Flow-Volume Curve: Restriction
Shape can vary depending on etiology
All lower volume and no concave shape
Adapted from Pulmonary Function Tests in Clinical practice. Figure 1.19
Parenchymal disease Chest Wall NMD

Flow-Volume Curve: Upper airway
obstruction
Variable: obstruction comes and goes with
maximal inspiratory or expiratory efforts
Fixed: never changes with forced efforts
Unlike lower airway disease, the
obstruction is present throughout the
expiratory cycle
Ie: not just at low lung volumes

Flow-Volume Curve: Upper airway
obstruction
Adapted from Pulmonary Function Tests in Clinical practice. Figure 1.20

Upper airway obstruction: Causes
Variable extrathoracic
Dynamic tumors or strictures, vocal cord paralysis
Variable intrathoracic
Dynamic tumors or strictures and tracheomalacia
Fixed
Non-dynamic tumors and fibrotic strictures

Looks normal by numbers
Clearly not an acceptable test

Spirometry – Quantitative analysis

Controversies
Will not address
LLN vs. fixed cut off for obstruction
Using FVC vs. VC
The absolute cut off of 0.7 is still the most
commonly used and understood
From GOLD

Obstruction
Grade the severity
This is per GOLD
Mild ≥ 80%
Moderate 50-79%
Severe 30-49%
Very severe <30%
Assess for
bronchodilator response
≥12%
and
≥200ml
Can be FVC or FEV1

Reversibility
A positive bronchodilator response is
supportive of the diagnosis of asthma
Can also been seen in COPD
False negative
Medications/Caffeine not withheld, specific
antigen, exercise induced

FEF 25-75%
It is not specific for small airway disease
It is highly variable between people and between test
Does not indicate bronchodilator response
May assist in ‘early’ or ‘borderline’ detection

Examples

Moderate obstruction
without reversibility.
Query cough due to asthma
or COPD?

Mild non-reversible
obstruction.
Consistent with COPD

Suggestive of a
restrictive disorder
Needs full PFTs

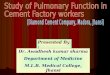
Lung volumes
Nitrogen washout, Inert gas dilution
**Plethysmography By using Boyle’s law
we can derive the lung volumes and capacities that we can not get from spirometry
TLC, RV, FRC
Adapted from Pulmonary Function Tests in Clinical practice. Figure 2.3

Lung volumes
Needed to identify
Restriction
Possible etiology
Hyperinflation
Gas trapping
Mixed disorders

Total lung capacity: TLC
Increased
COPD
Acromegaly
Athletes (swimmers)
Decreased
Restrictive ILD
Chest wall
NMD

Severity of restriction
Restriction
Mild 60-80%
Mod. 50-60%
Severe <50%
Hyperinflation
>120%
Generally don’t grade

Residual Volume
Increased – air trapping
Obstructive disorders such as COPD and
asthma
Decreased
Parenchymal restriction

RV/TLC ratio
Restriction
Parenchymal Normal as symmetrical decrease
Extra-parenchymal Increased as typically no change in RV
Obstruction
I generally do not look at it, but usually increased

FRC – insight into lung compliance
Increased
Increases slightly with age
Emphysema Due to loss of elastic
recoil
Decreased
Lung fibrosis
Obese Low ERV
Supine

Bring it together: Disease patterns
Differentiate obstructive subtypes
While both asthma and COPD may have gas
trapping and a high RV/TLC
Asthma should not have hyperinflation
Confirm restriction suspected on
spirometry
Can have low VC due to gas trapping

Disease patterns
Differentiate restrictive subtypes
Parenchymal restriction Low TLC, RV, but normal RV/TLC
Extra-parenchymal restriction Low TLC, but normal RV and high RV/TLC
Especially NMD where RV may be very high due to expiratory muscle weakness
Identify mixed
Low ratio on spirometry, but low TLC RV can be variable

DLCO
Diffusing capacity of
the lungs for carbon
monoxide measures
the ability of the lungs
to transfer gas from
inhaled air to the red
blood cells in
pulmonary capillaries

Grading severity
>75% normal
60-75% mild
40-60 moderate
<40% severe

DLCO
Decreased
Need to consider the
ddx in the context of
the rest of the PFT
Obstruction
Restriction
Isolated DLCO
Increased
Pulmonary
hemorrhage
Polycythemia
Increased pulmonary
blood flow
Mueller, exercise,
pregnancy, supine
position, left to right
shunt

Differential diagnosis
Obstruction Isolated Restriction
Emphysema Anemia ILD
Bronchiolitis CO Pneumonitis
Obstructive ILD
LAM/Sarcoid
Pulmonary
vasculature
NMD
Early ILD Chest wall

DLCO adjustment
Hemoglobin
Polycythemia or anemia can alter the DLCO
Non-linear relationship
CO
Active smokers can effect the measurement
and can use ABG to adjust
Alveolar volume

DLCO adjustment - VA
Most labs report a DLCO that is corrected for the measured lung volume (DLCO/VA)
The concept comes from normal subjects who inhaled a submaximal volume
However, routine use of the DLCO/VA is not recommended The correction is not linear and does not give insight
in to the reason for low VA Incomplete alveolar expansion, diffuse versus localized loss
of alveolar units, and poor alveolar mixing
I only use it to consider extraparenchymal restriction

Examples

Scooped flow volume
Very long expiratory phase

Severe non-reversible obstruction, gas trapping, mild gas
exchange……..bronchiectasis/ACOS?


Ddx isolated DLCO


Mixed obstructive / restrictive
Severe gas exchange
Likely not just simple COPD


Severe obstruction, hyperinflated, gas trapping, severe
gas exchange


The supplemental tests
Muscle strength
Methacholine

Muscle strength
MIP and MEP
Useful in monitoring
known NMD
In those with
restriction or
dyspnea NYD
Can be seen before
clinical weakness

Muscle strength
Low MIP, normal MEP
Diaphragmatic paralysis
Low MEP, normal MIP
Spinal cord injury below C5
Low MIP can also be seen in gas trapping
Diaphragm at a mechanic disadvantage
MEP <40 predicts ineffective cough

Muscle strength
Supine and upright FVC
Drop in FVC of <10% in normal
Drop of >30% suggests bilateral
diaphragmatic paralysis

Mild-moderate restriction and borderline gas exchange that
overcorrects for Va
?Extra-parenchymal restriction, specifically NMD


Bronchial Challenge test
Used to help in diagnosing or excluding asthma
by provoking bronchoconstriction by controlled
external stimuli
Most commonly methacholine used (M-agonist)

Test and severity
Adapted from Pulmonary Function Tests in Clinical practice. Figure 4.1

Interpretation
A negative methacholine test is very useful
in ruling out asthma
Very high negative predictive value
False negative: medication and specific Ag
A positive methacholine does not equal
asthma
Must be taken in clinical context

False positive methacholine
Allergic rhinitis without asthma
Smokers/COPD
CHF
Bronchiectasis / CF
Sarcoid
Recent URTI


A quick word on CPET
Adapted from Pulmonary Function Tests in Clinical practice. Figure 9.2

CPET
An underutilized tool
Determine exercise capacity Exercise prescription, disability
Identify the cause of exercise impairment Dyspnea NYD
Select therapy and response Thoracic surgery and response to PH Rx
Diagnose exercise induced asthma

Reference material
Pulmonary function tests in clinical practice
Dr Altalag, Road and Wilcox
Springer 2009
Interpretative strategies for the lung function tests
Pellegrino et al.
Eu. Respir. J. 2005

Special thanks
To all the RTs at KGH
Especially the PFT department where all my
examples came from

Questions or some more examples

Certainly looks like asthma
Patient reports previous smoking history

Mild reversible obstruction with gas trapping
Normal diffusion
Consistent with asthma and not COPD


Not diagnostic of asthma
Certainly severe obstruction, high FRC, borderline diffusion
Asthma, COPD, ACOS


Not obstructive (post bronchodilator)
Moderate restriction
Severe diffusion, probably PHTN and restriction


Very severe obstruction, hyperinflation, gas trapping and
diffusion
Severe COPD