Embed Size (px)
Citation preview

Basic Fluids and Electrolytes
Douglas P. Slakey

Why Listen to This?• Essential for surgeons• Based upon physiology
– Disturbances understood as pathophysiology
Most abnormalities are relatively simple, and many iatrogenic



Purpose of this Talk
To Encourage Thought
Not
Mechanical Reaction


You Have to Read!

It’s All About Balance
• Gains and Losses– Losses
• Sensible and Insensible
• Typical adult, typical day– Skin 600 ml
– Lungs 400 ml
– Kidneys 1500 ml
– Feces 100 ml
• Balance can be dramatically impacted by illness and medical care

Fluid Compartments
• Total Body Water– Relatively constant– Depends upon fat content and varies with age
• Men 60% (neonate 80%, 70 year old 45%)
• Women 50%
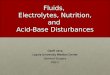
TOTAL BODY WATERTOTAL BODY WATER60% BODY WEIGHT60% BODY WEIGHT
ICF
2/3
Predominant solute
K+
ECF
1/3
Predominant solute
Na+
HH22OO

(mEq/L) Plasma IntracellularNa 140 12K 4 150Ca 5 0.0000001Mg 2 7Cl 103 3
HCO3 24 10Protein 16 40
Electrolytes

Fluid Movement
• Is a continuous process• Diffusion
– Solutes move from high to low concentration
• Osmosis– Fluid moves from low to high solute concentration.
• Active Transport– Solutes kept in high concentration compartment– Requires ATP

Movement of Water• Osmotic activity
– Most important factor– Determined by concentration of solutes
Plasma (mOsm/L)
2 X Na + Glc + BUN
18 2.8

Third Space
• Abnormal shifts of fluid into tissues
• Not readily exchangeable
• Etiologies– Tissue trauma– Burns– Sepsis

Fluid Status• Blood pressure
• Check for orthostatic changes
• Physical exam
• Invasive monitoring– Arterial line– CVP– PA catheter– Foley

Remember JVD?

Fluid Imbalances
• Must assess organ function– Renal failure– Heart failure– Respiratory failure• Excessive GI fluid losses• Burns

Volume Deficit
• Most common surgical disorder• Signs and symptoms
– CNS: sleepiness, apathy, reflexes, coma– GI: anorexia, N/V, ileus– CV: orthostatic hypotension, tachycardia with
peripheral pulses– Skin: turgor– Metabolic: temperature
Dehydration
Chronic Volume Depletion
Affects all fluid components
Solutes become concentrated
Increased osmolarity
Hct can increase 6-8 pts for 1 L deficit
Patients at risk:
Cannot respond to thirst stimuli
Diabetes insipidus
Treatment: typically low Na fluids

HypovolemiaAcute Volume Depletion
Isotonic fluid loss, from extracellular compartmentDetermine etiology
Hemorrhage, NG, fistulas, aggressive diuretic therapyThird space shifting, burns, crush injuries, ascites
Replace with blood/isotonic fluid» Appropriate monitoring
» Physical Exam» Foley (u/o > 0.5 ml/kg/min)» Hemodynamic monitoring

Fluid Replacement

Fluid Replacement
• Isotonic/physiologic– NS, LR
• Less concentrated– 0.45NS, 0.2NS– Maintenance
• Hypertonic Na

Fluid Replacement
• Plasma Expanders– For special situations– Will increase oncotic pressure– If abnormal microvasculature, will extravasate
into “third space”Then may take a long time to return to circulation

Fluid Replacement
• Maintenance– 4,2,1 “rule”
• Other losses (fistulas, NG, etc)– Can measure volume and composition!!!– Should be thoughtfully assessed and
prescribed separately if pathologic

Maintenance Fluid
• Daily Na requirement: 1 to 2 mEq/kg/day
• Daily K requirement: 0.5 to 1 mEq/kg/day
• AHA Recommended Na intake: 4 to 6 grams per day
Maintenance Fluids
To Replace Ongoing Losses,
NOT Pre-existing Deficits

Maintenance Fluids
D5 0.45NS + 20 mEq KCl/L at 125 ml/H


How much Sodium is Enough???
» NS» 0.9% = 9 grams Na per liter
» 0.45 NS = 4.5 grams per liter» 125 ml/hour = 3000 ml in 24 hours» 3 liters X 4.5 grams Na = 13.5 GRAMS Na!
(If 0.2 NS: 3 liters X 2 grams Na = 6 grams Na)

Assessment of Disorders of Volume
and Electrolytes• Effects are variable and complex
• Simplified treatment algorithms cannot address the variable and complex nature of these disorders
• Acid - Base balance is integral with these disorders

Hyponatremia• Na loss
– True loss of Na– Dilutional (water excess)– Inadequate Na intake
• Classified by extracellular volume– Hyovolemic (hyponatremia)
• Diuretics, renal, NG, burns
– Isotonic (hyponatremia)• Liver failure, heart failure, excessive hypotonic IVF
– Hypervolemic (hyponatremia)• Glucocorticoid deficiency, hypothyroidism

Na Volume
Check Ur Na
< 10 mmol/L
VomitingDiarrhea3rd spaceHepatorenal
Adrenal InsufficiencyDiureticsSalt-Wasting SyndromeSIADH
> 20 mmol/L

SIADH• Causes
– Cancers (pancreas, oat cell)– CNS (trauma, stroke)– Pulmonary (tumors, asthma, COPD)– Surgical stress– Medications
• Anticonvulsants, antineoplastics, antipsychotics, sedatives (morphine)

SIADHToo much ADH
Affects renal tubule permeability
Increases water retention (ECF volume) Increased plasma volume, dilutional hyponatremia,
decreases aldosterone, increased GFR
Increased Na excretion (Ur Na >40mEq/L)
Fluid shifts into cellsSymptoms: thirst, dyspnea, vomiting, abdominal cramps,
confusion, lethargy

SIADH Treatment
• Fluid restriction– Will not responded to fluid challenge
(distinguishes from pre-renal cause)
• Possibly diuretics


Hypovolemia and Metabolic Abnormality
• Acidosis– May result from decreased perfusion
• Alkalosis– Complex physiologic response to more chronic
volume depletion

Paradoxical Aciduria
Na
Cl
Na
H
K
Loop of Henle
HypochloremicHypovolemia

Hypernatremia
Relatively too little H2O
– Free water loss (burns, fever)– Diabetes insipidus (head trauma, surgery,
infections, neoplasm)• Dilute urine
– Nephrogenic DI• Kidney cannot respond to ADH

Hypernatremia
• Hypovolemic– GI loss, osmotic diuresis– Increased Na load (usually iatrogenic)
[0.6 X wt (kg)] X [Serum Na/140 - 1]
Free water deficit:

Hypernatremia Volume Replacement
• Example:
• Na 153, 75 kg person
• (0.6 X 75) X [(153/140) - 1]
• 45 X [1.093 -1]
• 45 X 0.093 = 4.2 Liters

Potassium
• 98% intracellular• 20 to 40 mEq/L of urine
– Kidneys cannot retain K
• Dietary sources– Chocolate, dried fruits, nuts– Fruits: oranges, bananas, apricots– Meats– Potatoes, mushrooms, tomatoes, carrots

Potassium and Ph
• Acidosis– Extracellular H+ increases, moves intracellular
forcing K+ extracellular
• Alkalosis– Intracellular H+ decreases, to keep intracellular
fluid neutral, K+ moves into cells

Hyperkalemia
• Associated medications– ACE inhibitors, beta-blockers, antibiotics,
chemotherapy, NSAIDS, spironolactone
• Treatment– Mild: dietary restriction, assess medications– Moderate: Kayexalate
• Do NOT use sorbitol enema in renal failure patients

Hyperkalemia
• Emergency (> 6 mEq/l)
• Treatment– Monitor ECG, VS– Calcium gluconate IV– Insulin and glucose IV– Kayexalate, Lasix + IVF, dialysis



![Thomas]. Slakey. Slakey intellectual virtues, there is the completely non-rational part, the source of the vegetative processes of nutrition and growth common not only to human beings](https://img.pdfslide.net/doc/110x75/5ac2898c7f8b9a357e8e0f8f/thomas-slakey-slakey-intellectual-virtues-there-is-the-completely-non-rational.jpg)