Embed Size (px)
Citation preview
Basic malaria microscopy
training An approach to planning and implementing training in
malaria microscopy
Omar Abdelrazig Abdalla Microbiologist – CPDC Certified Trainer
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
Opening
• Learning unit 1 Malaria, the disease
• Learning unit 2 Cleaning and storing microscope slides
• Learning unit 3 Keeping records
• Learning unit 4 Preparing blood films
• Learning unit 5 Staining with Giemsa stain
• Learning unit 6 The microscope
• Learning unit 7 Examining blood films
• Learning unit 8 Examining blood films for malaria parasites
• Learning unit 9 Routine slide examination
• Learning unit 10 Supervision in malaria microscopy
11/24/2015
Omar Abdelrazig
Learning objectives
• Adequately prepare a set number of thick and thin blood films;
• Demonstrate the correct practice and precautions for preventing transmission of
blood borne pathogens when handling blood;
• Demonstrate the correct Giemsa staining procedures for staining thick and thin
blood films for malaria microscopy;
• Demonstrate and describe the methods used to maintain microscopes in
working order;
• Demonstrate and use the correct procedures for examining stained thick and
thin blood films for malaria parasites;
• Demonstrate their ability to identify correctly the components of normal
blood;
11/24/2015
Omar Abdelrazig
Learning objectives
• Recognize and identify malaria parasites present in blood films; identify the stage(s) of plasmodia, the presence of individual species or mixed infections of Plasmodium falciparum, P. vivax, P. malariae and P.
ovale; and establish the density of malaria parasites in the film;
• Record the results of the microscopy examination on the correct form;
• inform those responsible of the findings in a timely manner;
• Demonstrate their understanding of the requirement to observe patient
confidentiality and ethical issues;
• Follow the correct procedures of the national programme, submit reports,
stores slides for audits and prepare requests for supplies, to ensure the smooth
functioning of the microscopy facility;
• Competently evaluate the gold standard test for malaria diagnosis.
11/24/2015
Omar Abdelrazig
Basic rules for the laboratory
• Do not touch, open or smell bottles, jars and containers or chemicals unless you have been instructed to do so or unless you know what you are doing and know what is in the bottle.
• Clean up when you have finished your work: • do not leave dirty glassware or slides for others to wash.
• Do not eat or drink in the laboratory: eat and drink in designated areas.
• Do not smoke.
• Use the correct precautions when handling biological specimens, chemicals and ‘sharps’, such as needles and lancets.
• Take appropriate care when handling liquids that may be corrosive or acidic or have strong fumes. Wear protective gloves when handling materials contaminated with or holding blood.
• Discard contaminated materials into the designated receptacles; if you are not sure, ask someone who will know.
• As soon as a job is finished, wash your hands with soap and water.
11/24/2015
Silent body communication
• Body languish
– Smiling
– Good gesture
– Standing
– Facing the clients
11/24/2015 Omar Abdelrazig
Nonverbal communication.
• Positive body
language
– Smiling
– Good grooming
– Erect posture
– Face to face
– Zone of comfort
Negative body languish
• looking away
• Nervous behavior
• Deep sighing
• Crossing hands
• Griming
• Masticating gum
• Yawning
11/24/2015 Omar Abdelrazig
Negative body language/distracting
behaviors.
• Rolling eyes
• Nervous behaviors
• Deep sighs
• Crossed arms,
• Wrinkled forehead
• Throwing things around
• Chewing gum
• Yawning
Omar Abdelrazig
Learning objectives the disease
• After completing training, trainees will have successfully acquired the skills and competence to:
• describe the importance of malaria as a potentially life-threatening disease, in which early, accurate diagnosis and treatment are essential for patient recovery and survival;
• describe four common clinical signs and symptoms of malaria in patients;
• record on the correct laboratory or survey forms relevant patient details for subsequent information and patient follow-up; demonstrate their ability to prepare slides for blood filming correctly;
11/24/2015
Omar Abdelrazig
Learning objectives
• describe why malaria is an important public health problem in many parts of the world;
• describe four common symptoms of malaria;
• describe why some people have malaria parasites in their blood but have no clinical symptoms;
• explain how malaria parasites produce disease in people; explain how some species of female Anopheles mosquito transmit malaria;
• explain why accurate diagnosis of malaria depends on correct microscopic identification.
11/24/2015
Omar Abdelrazig
Malaria the disease
• Importance
• Current situation
• Participants role
• Life-cycle
11/24/2015
How is malaria transmitted?
• By the bite of an infected female Anopheles mosquito.
• Shared dirty needles between drug addicts.
• Blood transfusion from an infected donor.
• Congenital: (between infected mother and uninfected baby through the placenta).
• By contaminated blood to unprotected persons – e.g. through skin abrasions.
Omar Abdelrazig 11/24/2015
Human Malaria’s
• Plasmodium falciparum -- dangerous, multi-drug resistant, causes cerebral malaria, potentially life threatening.
• P. vivax – relapses, drug resistant, causes severe anaemia, rarely causes death.
• P. malariae – untreated can last for more than 50 years, causes kidney problems.
• P. ovale – relapses, world-wide distribution but rare, often mis-identified as P. vivax.
Omar Abdelrazig 11/24/2015
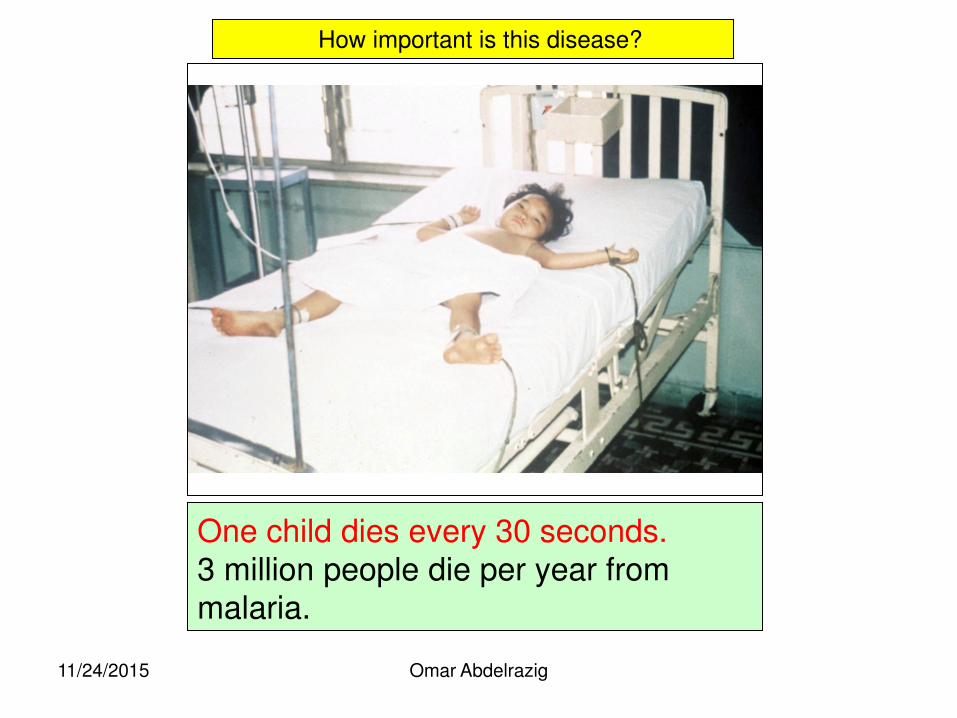
One child dies every 30 seconds. 3 million people die per year from malaria.
How important is this disease?
Omar Abdelrazig 11/24/2015
The importance of malaria
• Please remember: In the 8 hours of these lectures:
will have died from this disease or its side effects, mostly but not only in Africa,
•
Omar Abdelrazig 11/24/2015
What is the distribution of malaria?
• Global and country figures are often considered weak – there is much disagreement on their accuracy between groups.
• Pf the most serious – a potential killer. • Pv becoming more serious – difficulty with
relapses and increasing drug resistance. • Combined they are the greatest of the
disease burdens; greater than HIV/Aids, diarrhoea or ‘flu.
• TB is possibly a greater burden but is grossly under-diagnosed and under-reported.
Omar Abdelrazig 11/24/2015
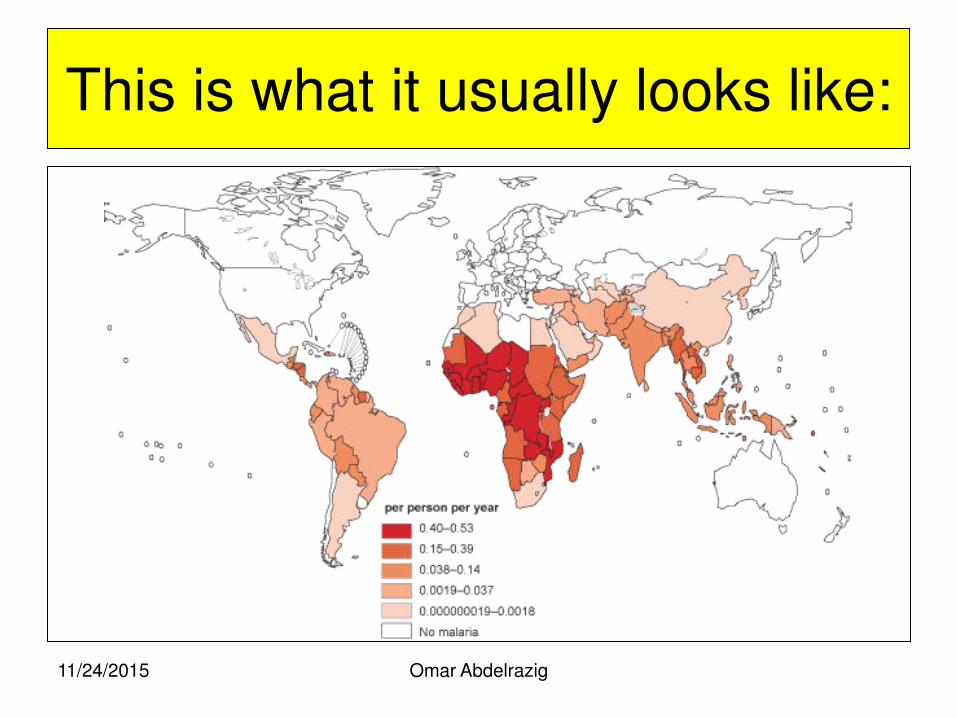
This is what it usually looks like:
Omar Abdelrazig 11/24/2015
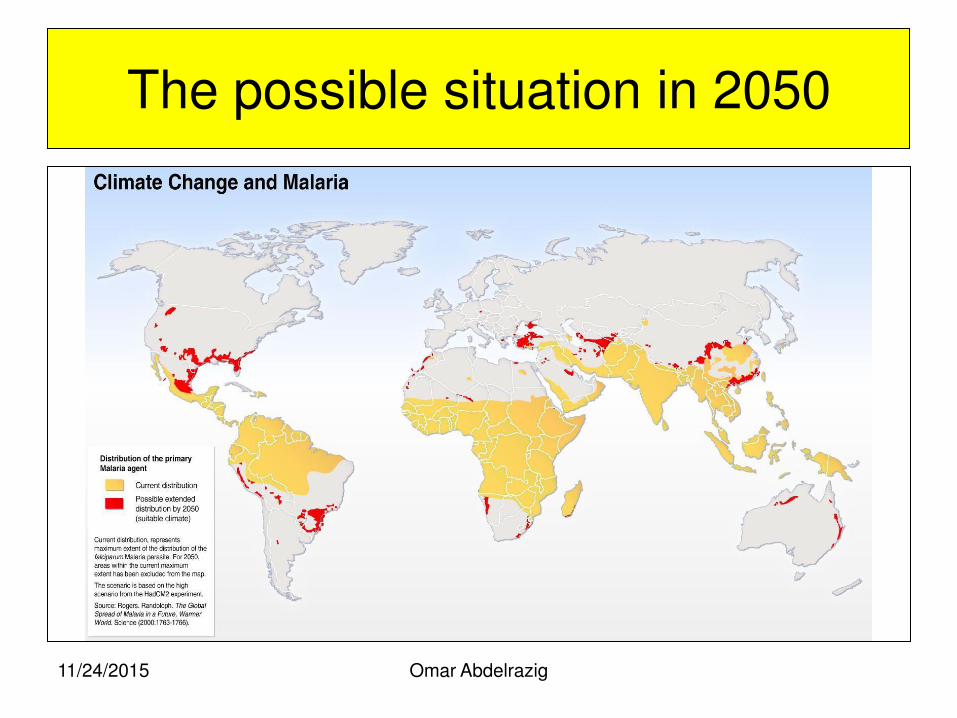
The possible situation in 2050
Omar Abdelrazig 11/24/2015
The global malaria load
• Combined there is a calculated 40% of the world’s population in 107 countries at permanent risk (80% - 90% in Africa).
• Malaria, poor education and poverty go hand in hand.
• Malaria is an opportunistic disease.
• Countries spend 1.3% of their GNP on treatment and prevention – too high for most poor nations but still not nearly enough.
• Few countries will be able to meet the GDG (UN Global Development Goals) by 2015.
Omar Abdelrazig 11/24/2015
Beware! Country’s that have no transmission do have malaria:
Example 1:
Oman has had no recorded transmission since 2007 but has about 85,000 cases per year among immigrant labour from Pakistan,
Bangladesh, Iran, India and Afghanistan.
Example 2:
Although Thailand has malaria transmission it is calculated that more than 50% of cases per year come over the border from Myanmar and
Cambodia for treatment.
Omar Abdelrazig 11/24/2015
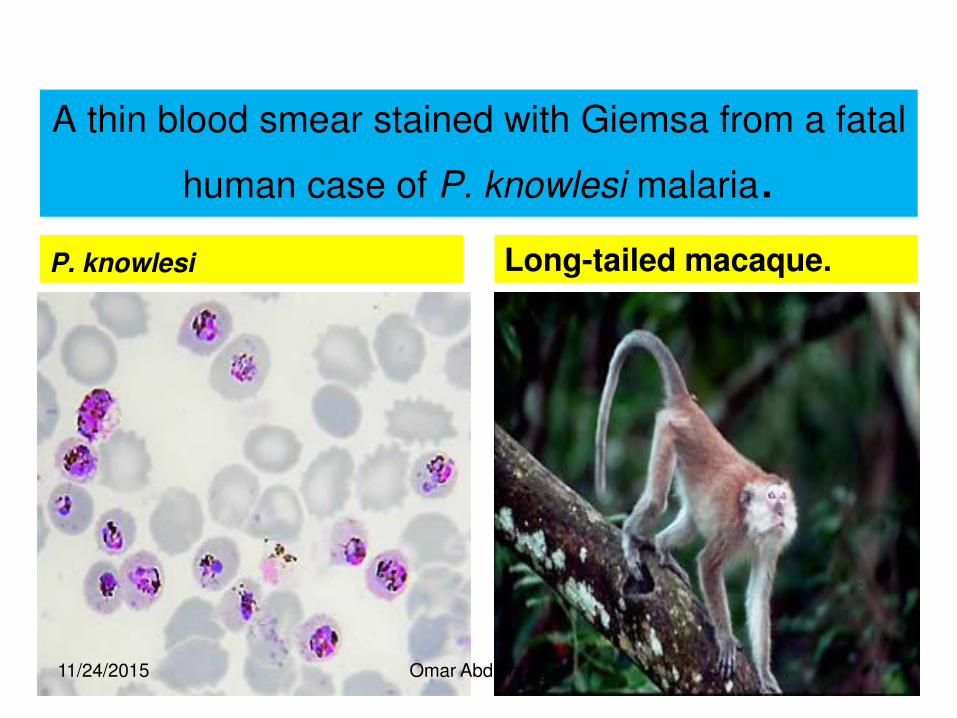
A thin blood smear stained with Giemsa from a fatal
human case of P. knowlesi malaria.
P. knowlesi Long-tailed macaque.
11/24/2015 Omar Abdelrazig
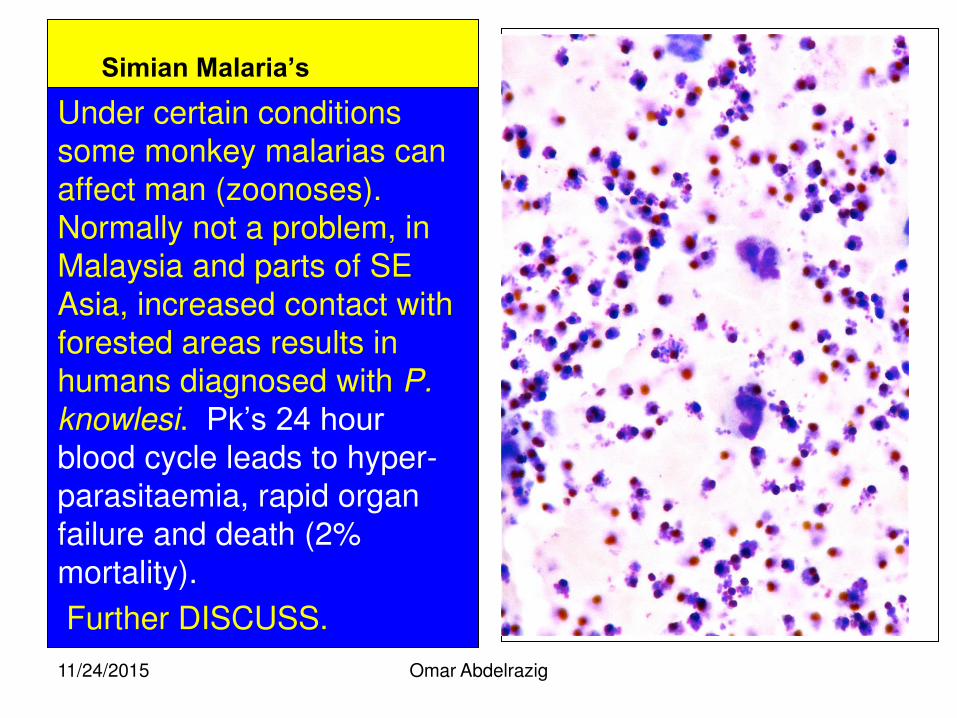
Simian Malaria’s Under certain conditions some monkey malarias can affect man (zoonoses). Normally not a problem, in Malaysia and parts of SE Asia, increased contact with forested areas results in humans diagnosed with P.
knowlesi. Pk’s 24 hour blood cycle leads to hyper-parasitaemia, rapid organ failure and death (2% mortality).
Further DISCUSS.
Omar Abdelrazig 11/24/2015
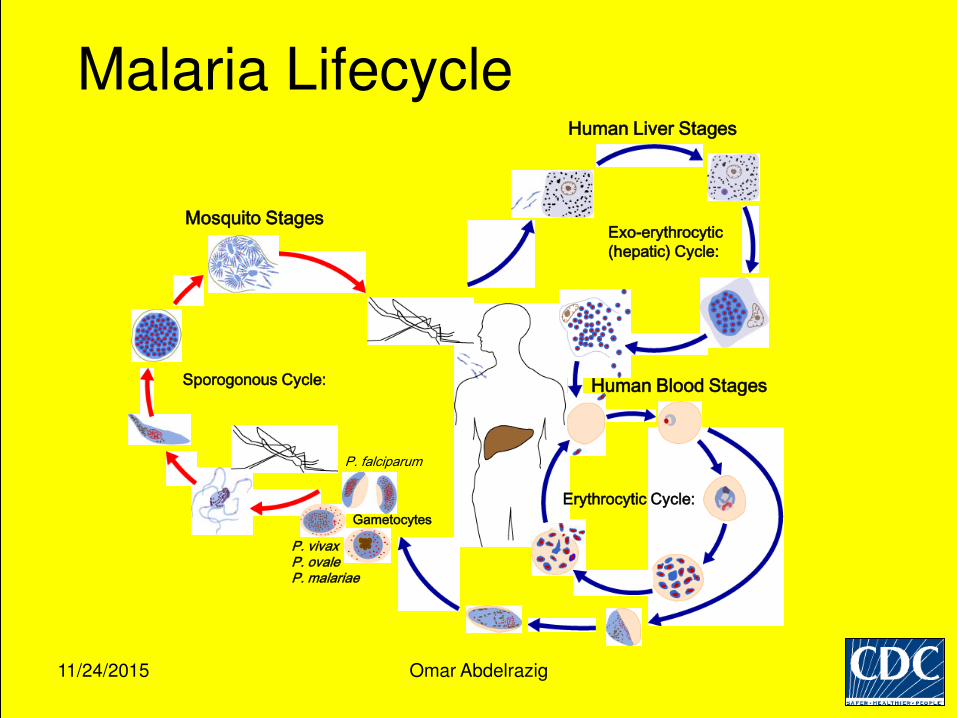
Sporogonous Cycle:
Mosquito Stages
Gametocytes
P. falciparum
P. vivax P. ovale P. malariae
Human Liver Stages
Exo-erythrocytic
(hepatic) Cycle:
Human Blood Stages
Erythrocytic Cycle:
Malaria Lifecycle
11/24/2015 Omar Abdelrazig
Signs and Symptoms:
• Fever • Chills • Headache • Body pains • Convulsions • Diarrhoea • Comatose • Cold and Flu-like
symptoms • Cough • Chest pains • More ….
Lookalikes: 1.Fevers of Unknown Origin (FUO):
2.Scrub typhus (SE Asia very common)
3.Meningitis
4.Typhoid fever
5.Flu
6.Heavy cold
7.Upset stomach
8.Cholera
9.Pneumonia
10.Dengue fever
11.More ……….
Omar Abdelrazig 11/24/2015
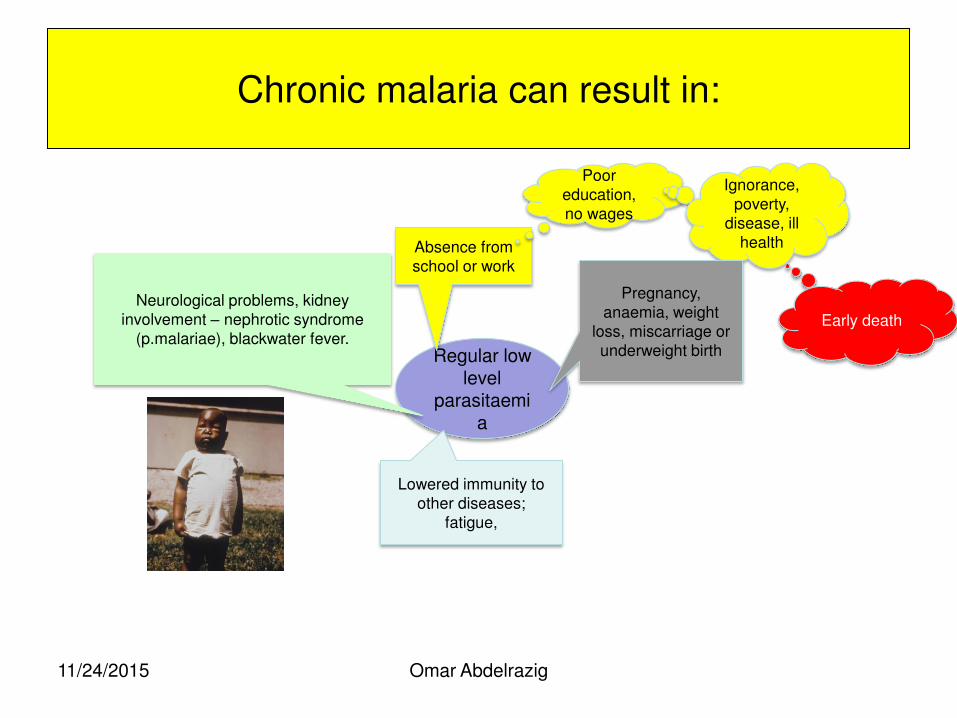
Chronic malaria can result in:
Omar Abdelrazig
Regular low level
parasitaemia
Absence from school or work
Poor education, no wages
Ignorance, poverty,
disease, ill health
Pregnancy, anaemia, weight
loss, miscarriage or underweight birth
Lowered immunity to other diseases;
fatigue,
Neurological problems, kidney involvement – nephrotic syndrome
(p.malariae), blackwater fever. Early death
11/24/2015
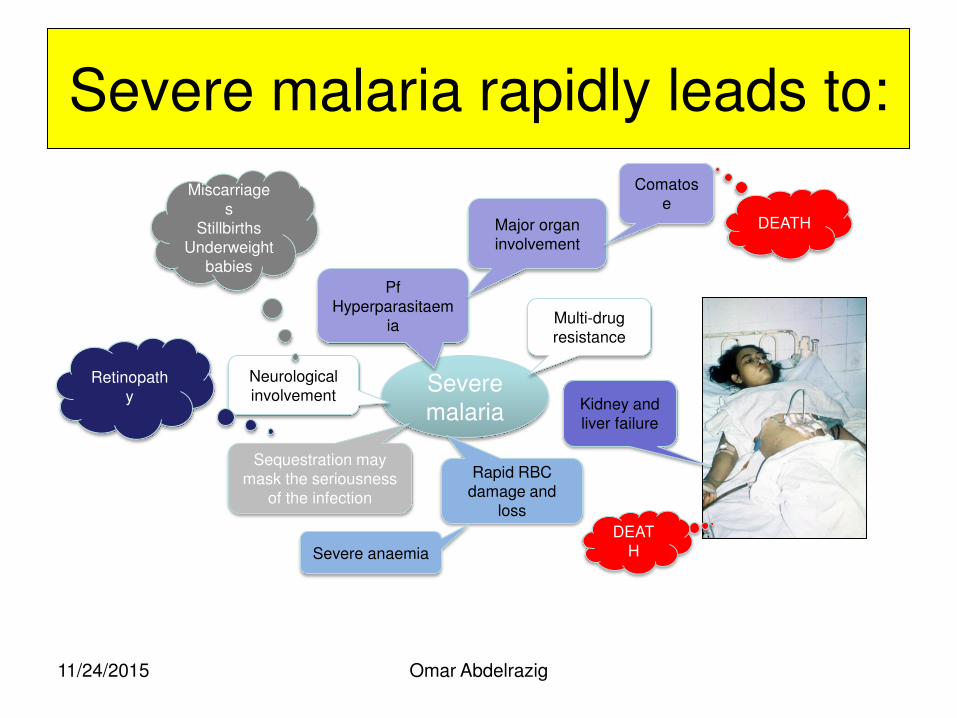
Severe malaria rapidly leads to:
Omar Abdelrazig
Severe malaria
Pf Hyperparasitaem
ia
Major organ involvement
Comatose
DEATH
Multi-drug resistance
Neurological involvement
Sequestration may mask the seriousness
of the infection
Rapid RBC damage and
loss
Severe anaemia
Kidney and liver failure
DEATH
Miscarriages
Stillbirths Underweight
babies
Retinopathy
11/24/2015
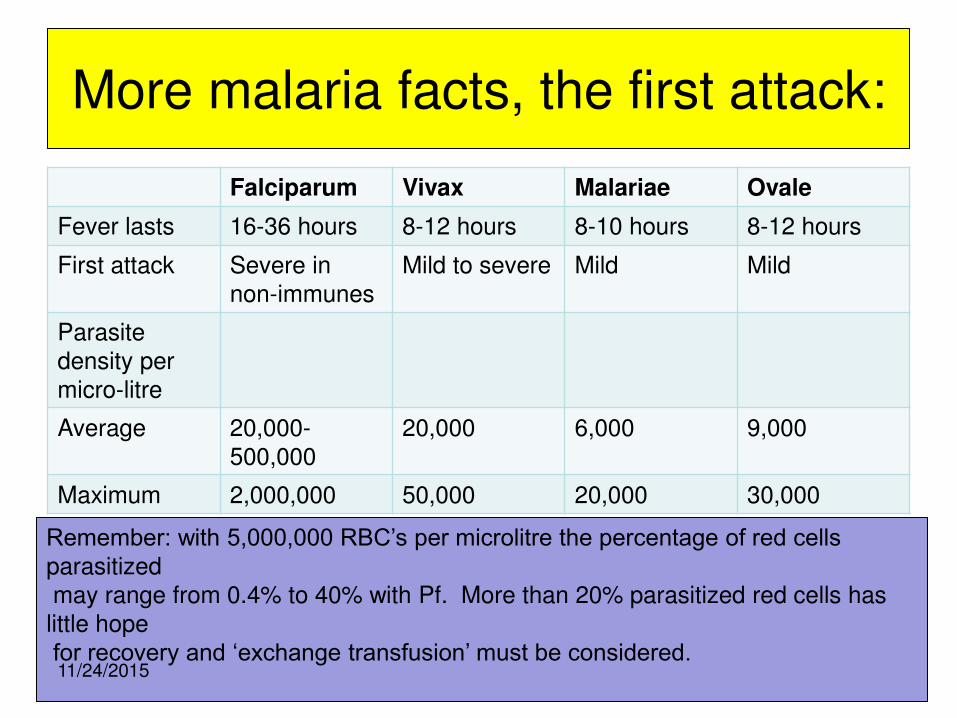
More malaria facts, the first attack:
Falciparum Vivax Malariae Ovale
Fever lasts 16-36 hours 8-12 hours 8-10 hours 8-12 hours
First attack Severe in non-immunes
Mild to severe Mild Mild
Parasite density per micro-litre
Average 20,000-500,000
20,000 6,000 9,000
Maximum 2,000,000 50,000 20,000 30,000
Omar Abdelrazig
Remember: with 5,000,000 RBC’s per microlitre the percentage of red cells parasitized may range from 0.4% to 40% with Pf. More than 20% parasitized red cells has little hope for recovery and ‘exchange transfusion’ must be considered.
11/24/2015
Omar Abdelrazig
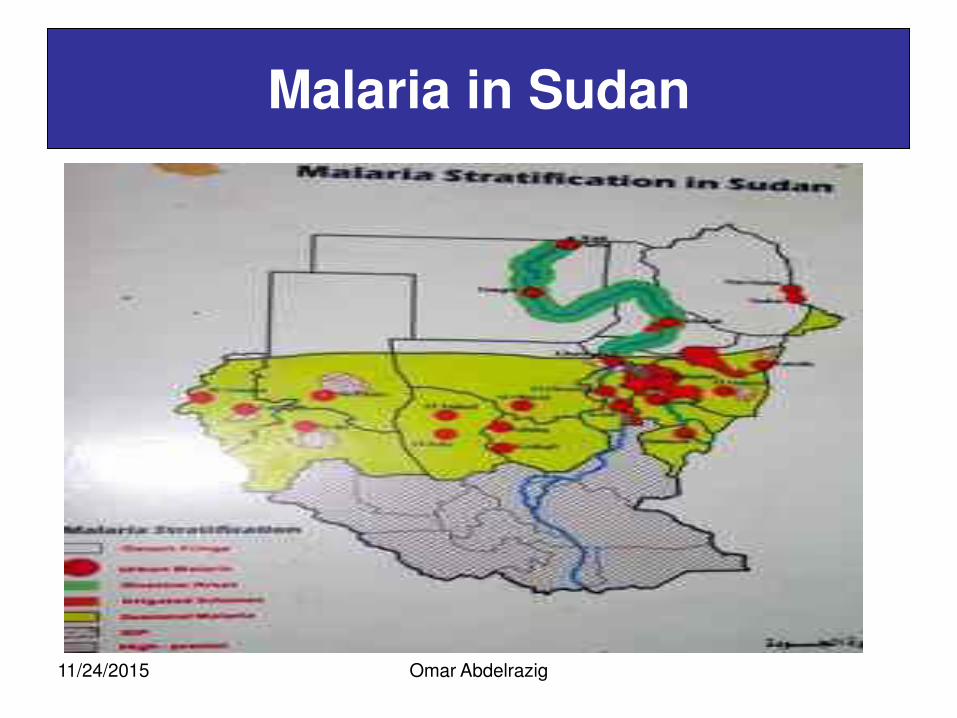
Malaria in Sudan
11/24/2015
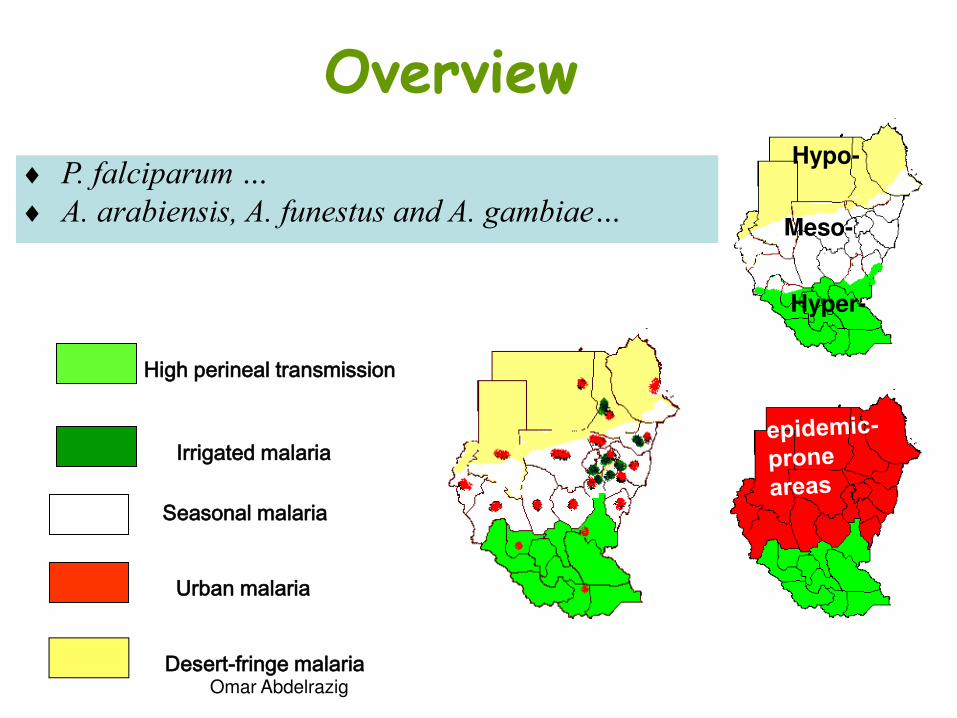
Overview
High perineal transmission
Irrigated malaria
Seasonal malaria
Urban malaria
Desert-fringe malaria
P. falciparum …
A. arabiensis, A. funestus and A. gambiae…
Hypo-
Meso-
Hyper-
Omar Abdelrazig
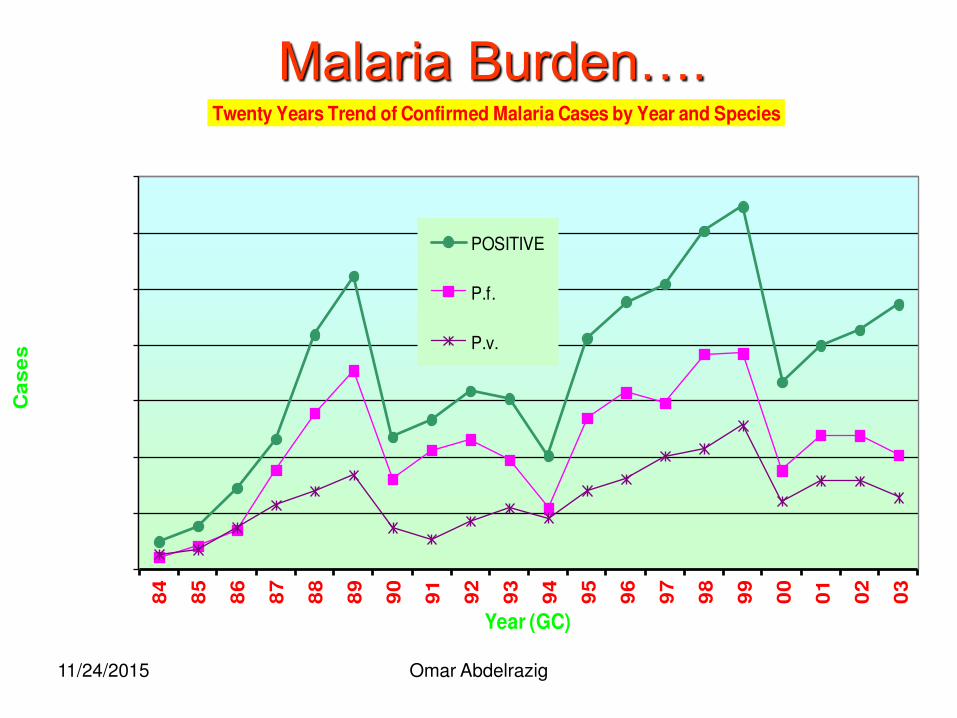
Malaria Burden….
-
100,000
200,000
300,000
400,000
500,000
600,000
700,000 8
4
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
00
01
02
03
Ca
se
s
Year (GC)
Twenty Years Trend of Confirmed Malaria Cases by Year and Species
POSITIVE
P.f.
P.v.
11/24/2015 Omar Abdelrazig
Any Questions?
Omar Abdelrazig 11/24/2015
Constrains in malaria microscopy
Following SOPs
Quality of supplies
personnel
Environment
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
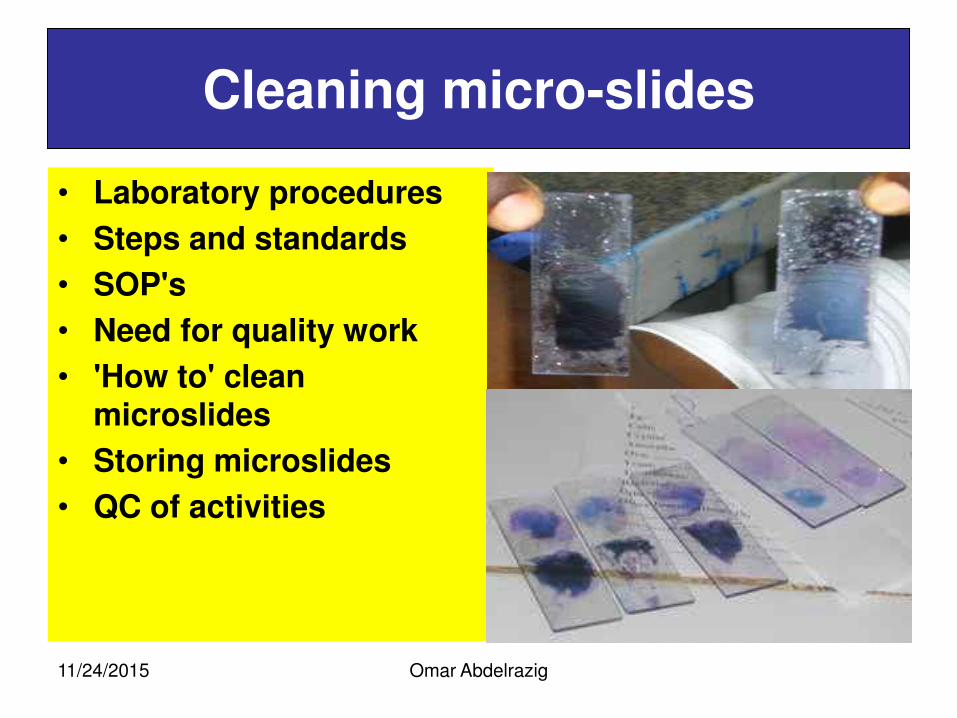
Cleaning micro-slides
• Laboratory procedures
• Steps and standards
• SOP's
• Need for quality work
• 'How to' clean microslides
• Storing microslides
• QC of activities
11/24/2015
Omar Abdelrazig
Cleaning the slides Learning objectives
• describe one standard operating procedure and explain its importance for malaria microscopy;
• select from previously used slides those suitable for making blood films and demonstrate why other slides are not suitable;
• demonstrate the two correct ways of washing, drying, wrapping and storing microscope slides for making blood films.
11/24/2015
Omar Abdelrazig
Cleaning the slides
• The method:
• 1. Separate new slides one from the other and soak in detergent solution for 4–8 h, conveniently overnight.
• 2. After soaking, clean each slide on both sides by rubbing the two surfaces in the washing cloth or sponge between the forefinger and thumb.
• 3. Rinse the slides individually in clean water to wash off the detergent.
• 4. Drain excess water from the slides, before placing them in the jar of alcohol with the lid firmly screwed on. Keep out of direct sunlight.
• 5. When required, remove a slide and dry it thoroughly with a clean, lint-free cot- ton cloth. Always handle slides by the edges.
• 6. The slide is ready for use; it does not need wrapping.
11/24/2015
Omar Abdelrazig
Keeping records
• Record forms
• Need for accuracy
• Confidentiality
11/24/2015
Omar Abdelrazig
Record keeping :objectives
• By the end of the module participants should be able to:
• identify the correct record form(s) and register(s) for entering information on patients;
• demonstrate preparation of accurate, error-free records on the appropriate form; select the correct copy of each record form, or completed summary, for dispatch to the supervisor;
• describe examples of the possible consequences of mixing up patients’ records; and explain why a patient’s details are confidential and must not be shared with unauthorized persons.
11/24/2015
Omar Abdelrazig
Record keeping Learning objectives
• By the end you should be able to:
• follow the correct procedures of the national programme, submit reports, stores slides for audits and prepare requests for supplies, to ensure the smooth functioning of the microscopy facility;
• use the handbook as a resource to teach health workers how to make thick and thin blood films, as part of the transfer of skills and team development; and organize, following the policies and requirements of the national malaria control programme, the collaboration necessary for regular supervision of the work of the laboratory.
11/24/2015
Omar Abdelrazig
Record keeping
The record should cover:
• cover: the region, province, district or zone in which the work was
done;
• the town, village or locality in which the patient lives;
• the street and house number at which the patient can be contacted;
• the patient’s name, sex and age; the patient’s number, which may also be the blood film number;
• other details, such as symptoms, body temperature and weight;
• the results of the blood film examination, such as positive or negative for malaria parasites, species and stages seen and whether P. falciparum gametocytes were observed;
• any antimalarial treatment received before microscopy examination; and other comments, observations or instructions to the clinician
11/24/2015
What is the expected result?
1- when not writing the full name?
2 -when touching finger while sampling?
3- when using scratched un clean slides? 4 -when drying films with oven, incubator or direct
sunlight? 5- when films exposed to dust or flies . 6- when films are left to dry horizontally? ؟
7- when methanol reach the thick film? 8- when increasing Giemsa conc and lessening staining
time? 9-when fixing or staining simples while they are wet?
10- when leaving methanol open for long time? 11/24/2015 Omar Abdelrazig
What is the expected result
when using unsuitable buffer concentration? 11- 12-when filtering the stain?
13-when discarding the stain & cleaning the slide? 14-when cleaning oculars with lenses paper of oil
immersion? 15-when alternating lenses between different
microscopes? 16-when using non conforming immersion oil?
17-when using oil mixed with xylin ؟ 18-when cleaning lenses with xylin or toluene ? 19- when cleaning microscope stage with alcohol ?
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
Film preparation Learning objectives
By the end you should be able to:
• adequately prepare a set number of thick and thin blood films;
• demonstrate the correct practice and precautions for preventing transmission of blood borne pathogens when handling blood;
• demonstrate the correct Giemsa staining procedures for staining thick and thin blood films for malaria microscopy;
• demonstrate and describe the methods used to maintain microscopes in working order;
• demonstrate and use the correct procedures for examining stained thick and thin blood films for malaria parasites;
• demonstrate their ability to identify correctly the components of normal blood;
11/24/2015
Omar Abdelrazig
Preparing blood film learning objectives
By the end of this unit, you will be able to:
• explain why blood must always be regarded as potentially contaminated; name four diseases found in infected blood;
• demonstrate the normal precautions used when handling blood;
• demonstrate the action to take when blood contaminates something accidentally;
• list the materials required for making thick and thin blood films; • demonstrate the correct method for preparing a thick and a thin blood
films on the same slide, for malaria microscopy;* • demonstrate the correct way of labeling a blood films; separate thick
and thin blood films of acceptable quality from unacceptable ones, giving reasons for the selection;
• describe and identify common mistakes and faults in making thick and thin blood films and the causes.
11/24/2015
Omar Abdelrazig
Tools for specimen collection
You will need:
• protective quality latex gloves without talcum powder (two to three pairs per person per exercise);
• cleaned, wrapped slides (more than are needed);
• sterile lancets (one per patient, plus 10%);
• 70% ethanol; absorbent cotton wool;
• a sharps container;
• a slide box or tray for drying slides horizontally and protecting them from flies and dust; four or five clean, lint-free cotton cloths; record forms or a register;
• ballpoint ink-pen for the record forms or register;
• and an HB lead pencil to write on the thin film and small sharpener.
11/24/2015
Omar Abdelrazig
Precautions preparing blood films
• Wear protective gloves when taking blood samples or handling blood.
• Avoid getting blood, including dry blood from films, on your fingers or hands.
• Cover cuts or abrasions on your hands with a waterproof dressing.
• Avoid accidentally pricking yourself when handling sharp instruments that have been in contact with blood.
• Thoroughly wash your hands with soap and water as soon as you finish a job. If you get blood on your skin, quickly wipe it off with a cotton swab dampened with alcohol; then, wash the affected area with soap and water as soon as possible.
11/24/2015
Collection of Blood Smears
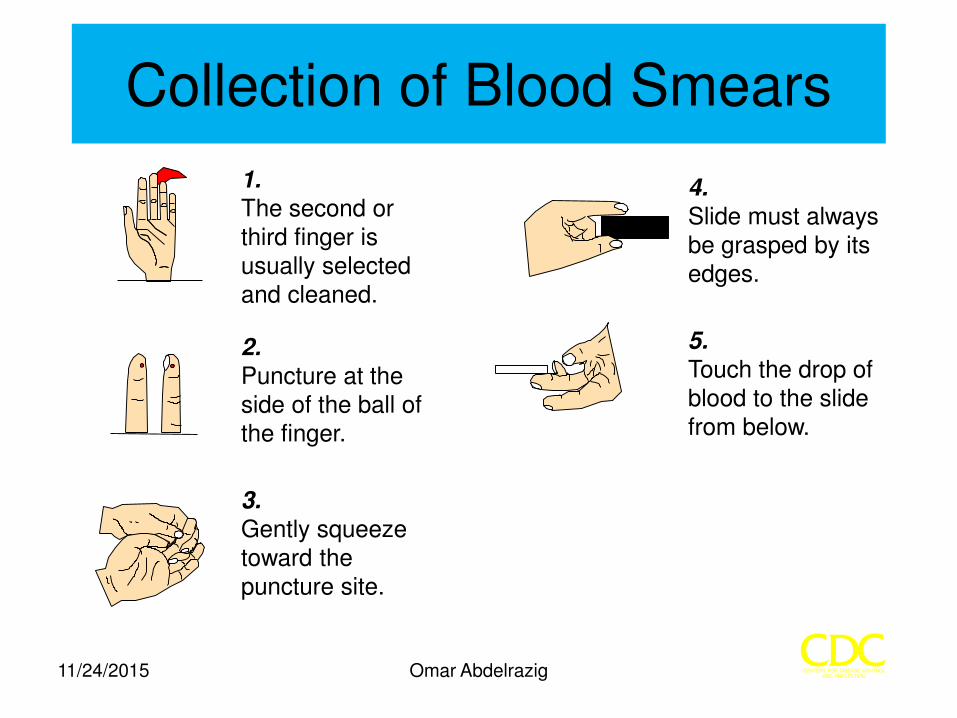
5. Touch the drop of blood to the slide from below.
4. Slide must always be grasped by its edges.
2. Puncture at the side of the ball of the finger.
3. Gently squeeze toward the puncture site.
1. The second or third finger is usually selected and cleaned.
11/24/2015 Omar Abdelrazig
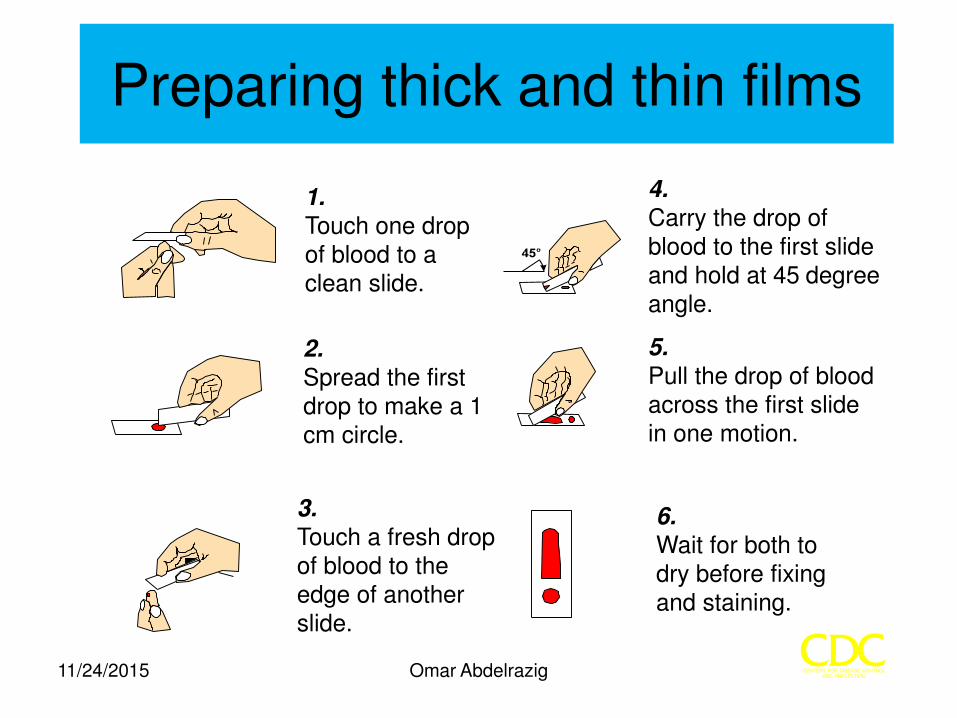
Preparing thick and thin films
1. Touch one drop of blood to a clean slide.
2. Spread the first drop to make a 1 cm circle.
3. Touch a fresh drop of blood to the edge of another slide.
6. Wait for both to dry before fixing and staining.
5. Pull the drop of blood across the first slide in one motion.
4. Carry the drop of blood to the first slide and hold at 45degree angle.
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
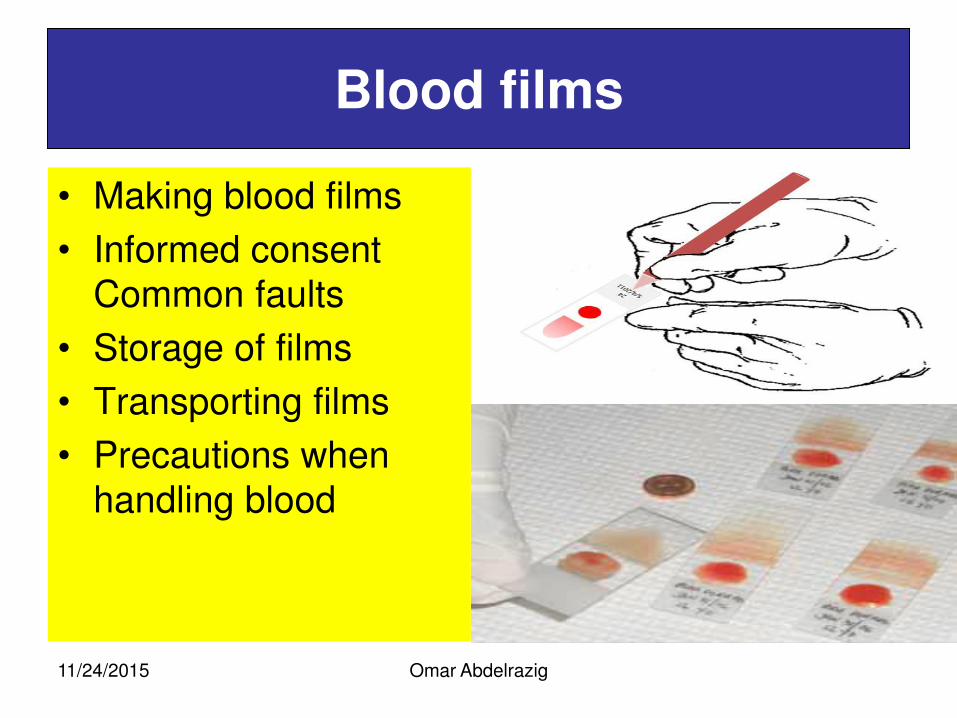
Blood films
• Making blood films
• Informed consent Common faults
• Storage of films
• Transporting films
• Precautions when
handling blood
11/24/2015
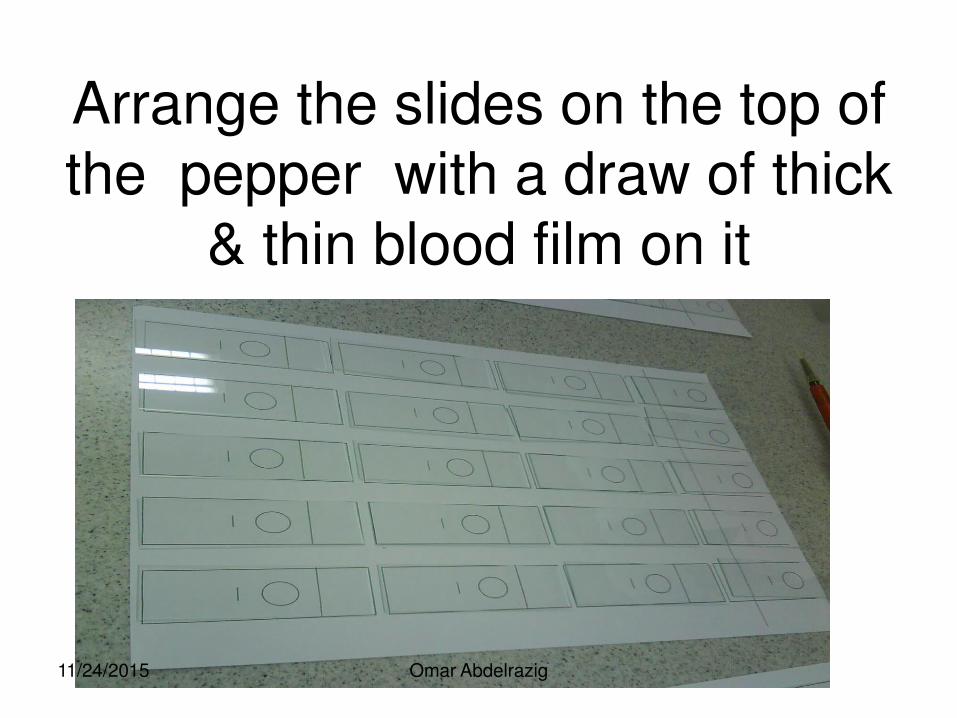
Arrange the slides on the top of the pepper with a draw of thick
& thin blood film on it
11/24/2015 Omar Abdelrazig
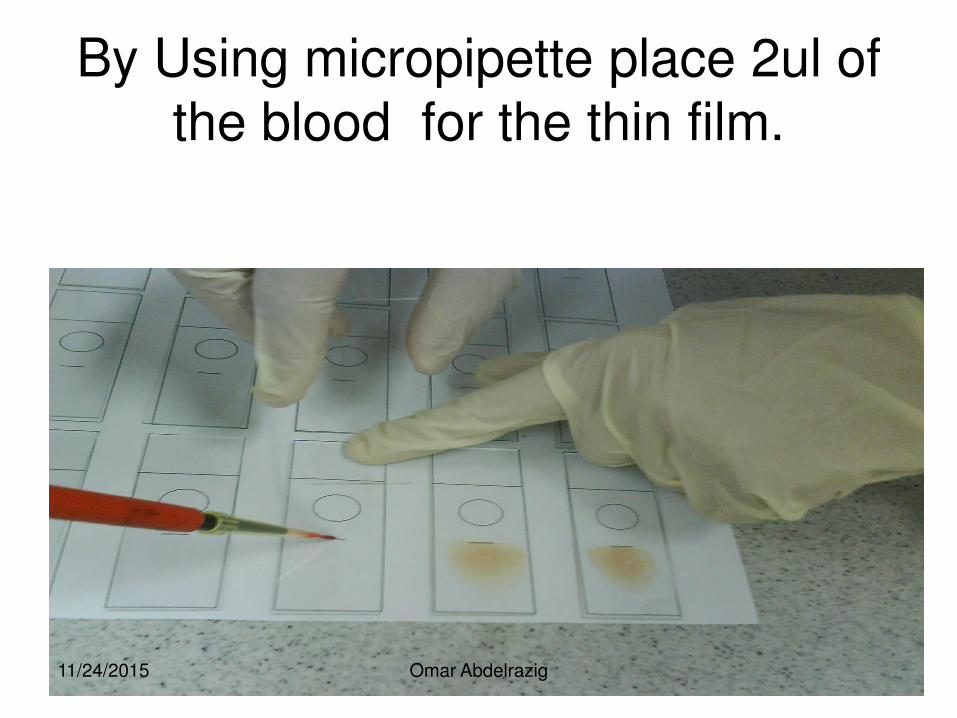
By Using micropipette place 2ul of the blood for the thin film.
11/24/2015 Omar Abdelrazig
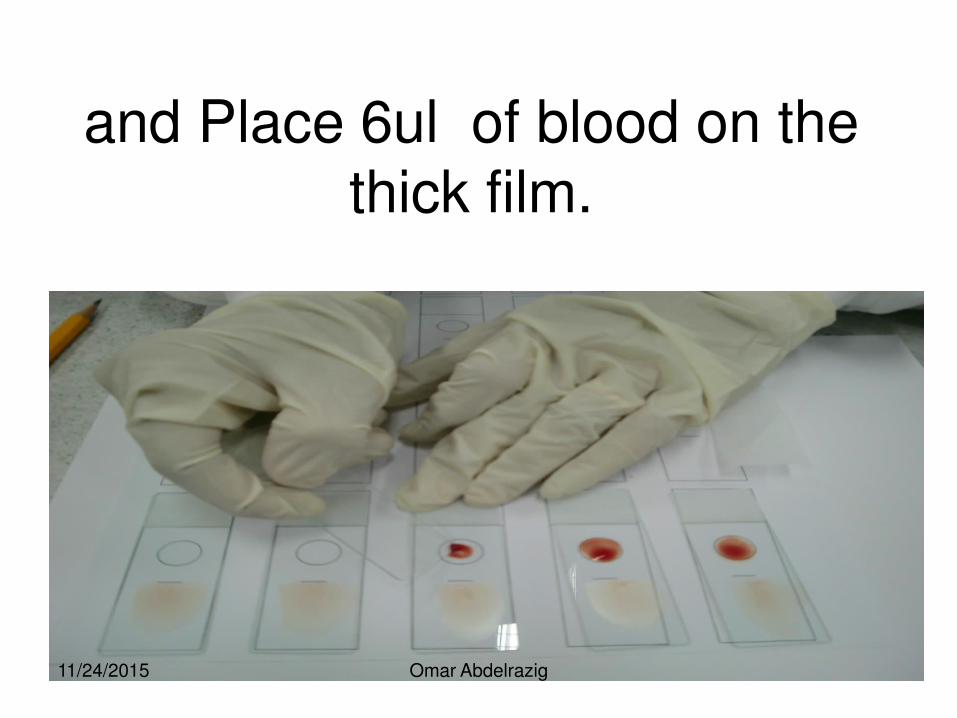
and Place 6ul of blood on the thick film.
11/24/2015 Omar Abdelrazig
prepare the slides for mounting.
11/24/2015 Omar Abdelrazig
Keep the slides of the same batch in the same slide box label it and Wright
the results .
11/24/2015 Omar Abdelrazig
• Arrange mixed slides with different species, stages and density with negative slides for training and education.
11/24/2015 Omar Abdelrazig
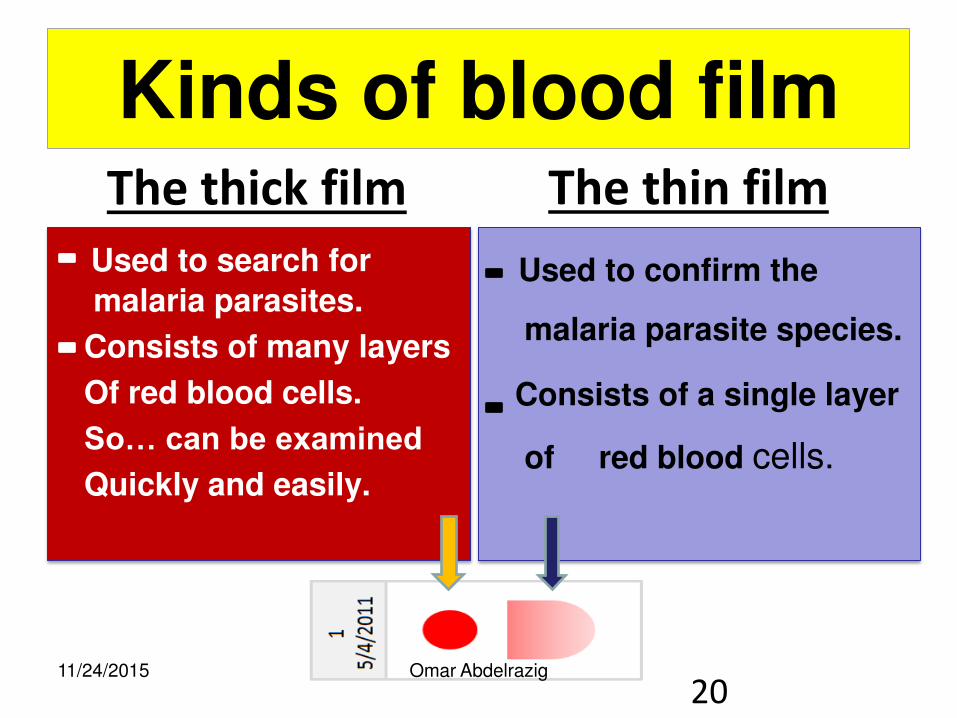
Kinds of blood film
Used to search for
malaria parasites.
Consists of many layers
Of red blood cells.
So… can be examined
Quickly and easily.
Used to confirm the
malaria parasite species.
Consists of a single layer
of red blood cells.
The thin film The thick film
20 11/24/2015 Omar Abdelrazig
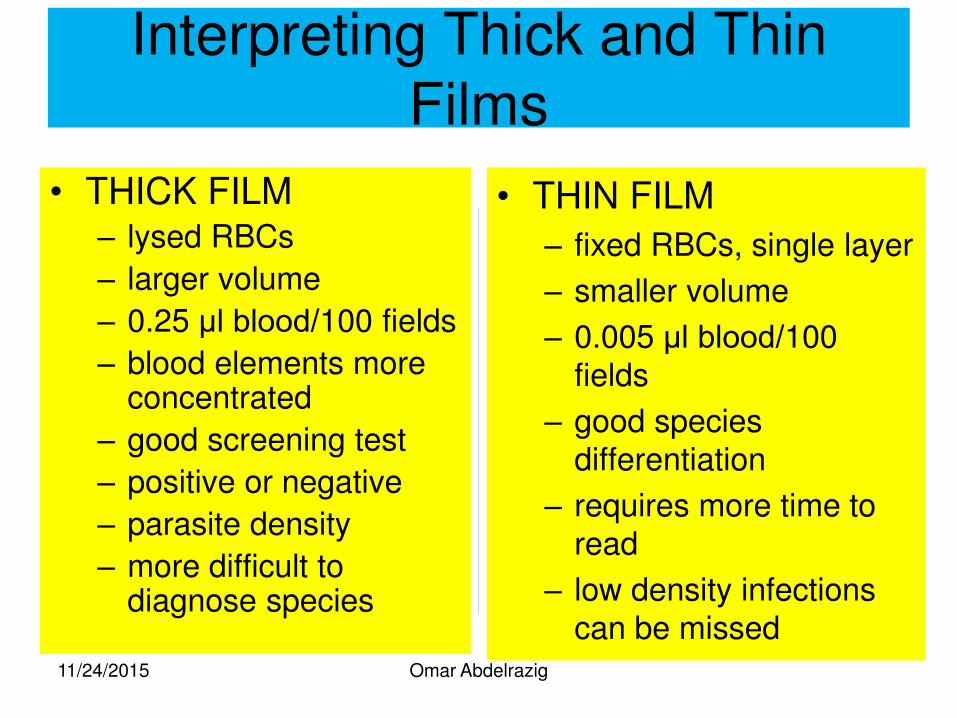
Interpreting Thick and Thin Films
• THICK FILM – lysed RBCs
– larger volume
– 0.25 μl blood/100 fields
– blood elements more concentrated
– good screening test
– positive or negative
– parasite density
– more difficult to diagnose species
• THIN FILM
– fixed RBCs, single layer
– smaller volume
– 0.005 μl blood/100 fields
– good species differentiation
– requires more time to read
– low density infections can be missed
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
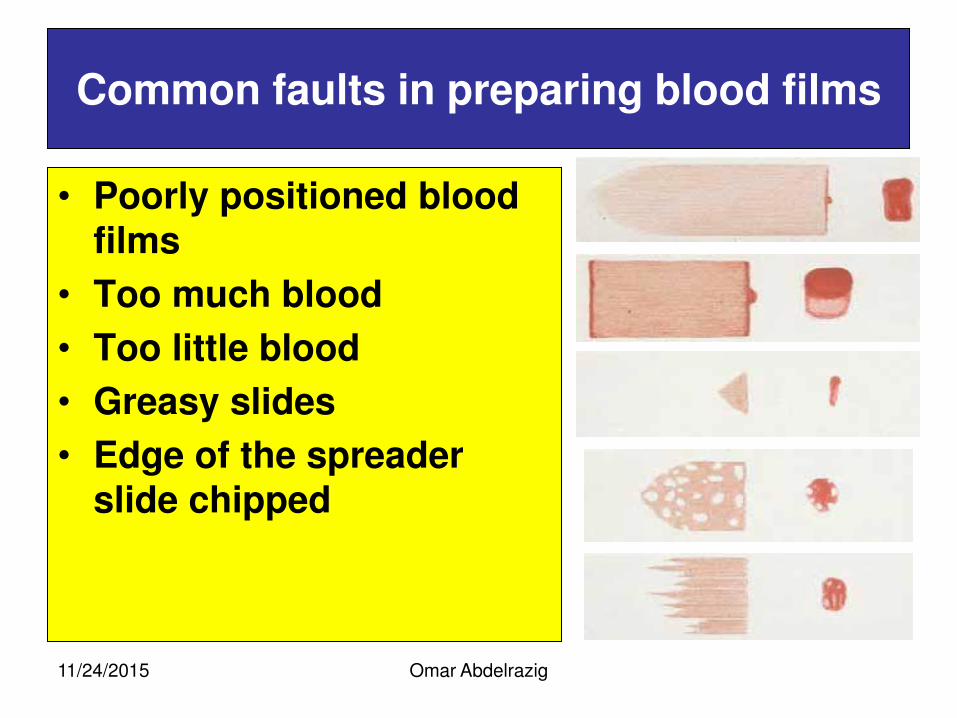
Common faults in preparing blood films
• Poorly positioned blood films
• Too much blood
• Too little blood
• Greasy slides
• Edge of the spreader slide chipped
11/24/2015
Malaria Blood Smear
• Prepare smears as soon as possible after collecting venous blood to avoid
• Changes in parasite morphology
• Staining characteristics
• Take care to avoid fixing the thick smear • Risk of fixing thick when thin is fixed with methanol
if both smears on same slide
• Let alcohol on finger dry to avoid fixing thick
• Be careful if drying with heat
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
Staining blood films
• Buffer water
• Giemsa stain
• Staining methods
• Care of equipment
11/24/2015
Omar Abdelrazig
Staining blood films
By the end of this unit, you will be able to:
• demonstrate correct operation of the analytical balance;*
• make up the buffered water used to dilute Giemsa stain;
• demonstrate correct use of the color comparator or pH meter;*
• make up the 2% correcting fluids used to adjust the pH of buffered water;
• explain why pH 7.2 buffered water is best for good Giemsa staining;
• demonstrate two correct methods of fixing thin blood films; explain when the ‘rapid’ and ‘slow’ Giemsa staining methods are used for malaria microscopy;
• demonstrate e mastery of the rapid and slow Giemsa staining methods;
• describe the correct ways of handling and storing Giemsa stain; and
• demonstrate the correct drying and storing of stained slides. 11/24/2015
Omar Abdelrazig
Buffered water
• The method:
• 1. Make sure that the pointer of the balance is set at zero by adjusting the balancing screw on the right arm.
• 2. Place a filter paper in each pan; set the balance to zero, this time by moving the gram weight along the gram scale arm.
• 3. Move the gram weight a further 0.7 g along the scale arm, ready for weighing the potassium dihydrogen phosphate.
• 4. Using a wooden spatula, place some of the KH2PO4 on the filter paper in the left-hand pan
11/24/2015
Omar Abdelrazig
Buffered water
• 5. Transfer the weighed KH2PO4 to the glass beaker, add about 150 ml of water, and stir with a clean spatula until the salt dissolves.
• 6. Place a fresh filter paper in the left-hand pan.
• 7. Reset the balance as before, but this time adjust the gram weight to 1 g for the Na2HPO4.
• 8. Using a clean, dry spatula, add the Na2HPO4 to the right-hand pan, balancing the weight as described in step 4 above.
• 9. Add the Na2HPO4 to the solution in the beaker and stir as in step 5.
• 10. When the salts have dissolved, add the solution to the conical flask and top up to the 1 liter mark with water.
11/24/2015
Buffer preparation
1buffer component :
By weighing:
) Na2HPO4 59.24 g ( + ( NaH2PO4H2O 36.38g) dissolved in 1 liter of distilled water. For daily use 10 ml of buffer is added to 990 ml of D.W.
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
2% correcting fluids
• To make up the 2% correcting fluids You will need: • an analytical balance accurate to 0.01 g or better (a two-pan trip
balance is ideal, or use an electrically operated one-pan balance);
• filter papers, 11 cm in diameter;
• two glass-stoppered bottles, each of 100 or 150 ml capacity;
• potassium dihydrogen phosphate (anhydrous) (KH2PO4)
• disodium hydrogen phosphate (anhydrous) (Na2HPO4);
• distilled or deionized water, about 200 ml; O wooden spatulas; two beakers of 250 ml capacity;
• one measuring cylinder of 100 ml capacity;
• and labels.
11/24/2015
Needed equipments
(Forceps) stop watch Measuring cylinder . Measuring flask.
latex gloves.
Cleaning gauge. Absorbent cotton. Registry log book . Lenses paper.
11/24/2015 Omar Abdelrazig
Reagents
concentrated Giemsa solution
7.2 ( Buffer .(
Ethanol 70 %
Absolute methanol. Recommended oil immersion100x
(refractive index1.52)
Distilled water. Detergent soap.
11/24/2015 Omar Abdelrazig
Giemsa Stain
Component 500 ml
Geimsa powder 3.8 gm
methanol 250 ml
glycerin 250 ml
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
The stain
• The rapid (10%) method This is the commonest method for staining 1–15 slides at a time. It is used in laboratories where a quick result to determine a patient’s malaria status is required.
The method is efficient, but more stain is used. The need for speed justifies the additional cost.
• You will need:
• Giemsa stain, decanted from the stock solution into a 25-ml bottle;
• methanol;
• 1 absorbent cotton wool;
• test tubes of 5 ml capacity;
11/24/2015
Omar Abdelrazig
Staining blood films
• distilled or deionized water buffered to pH 7.2;
• a Pasteur pipette with a rubber teat;
• a curved plastic staining tray, plate or rack;
• a slide-drying rack;
• a timing clock;
• a small electric hair-drier.
Thick blood films must be completely dry before being stained. They can be dried quickly with warm air from a small hair-drier or by careful warming over a lamp or a light bulb. Avoid overheating slides as they can ‘heat fix’ and then stain poorly.
11/24/2015
Omar Abdelrazig
Staining blood films
The method:
1. Fix the thin film by dabbing it with a pad of cotton wool dampened with methanol or by briefly dipping the film into methanol. Avoid contact between the thick film and methanol, as methanol and its vapours quickly fix the thick film, and it does not stain well.
2. Using a test tube or a small container to hold the prepared stain, make up a 10% solution of Giemsa in the buffered water by mixing three drops of Giemsa from the stock solution, using the Pasteur pipette, with 1 ml of buffered water. Each slide needs approximately 3 ml of stain to cover it.
3. Depending on whether you are using a staining tray, plate or rack, place the slides to be stained face down on the curved staining tray or face upwards on the plate or rack.
11/24/2015
Omar Abdelrazig
Staining blood films
4. Pour the stain gently under the staining tray until each slide is covered with stain, or gently pour the stain onto the slides lying face upwards on the plate or rack.
5. Stain the films for 8–10 min. Experience with the stain you are using will help you to decide the exact time needed for good staining.
6. Gently wash the stain from the slide by adding drops of clean water. Do not pour the stain directly off the slides, or the metallic-green surface scum will stick to the film, spoiling it for microscopy.
7. When the stain has been washed away, place the slides in the drying rack, film side downwards, to drain and dry. Ensure that thick films do not scrape the edge of the rack.
11/24/2015
Omar Abdelrazig
Staining blood films
• Some important things to remember with regard to the stock solution of Giemsa stain are:
• Keep the bottle tightly stoppered to avoid evaporation and oxidation of the stain by high humidity.
• Store in a dark glass bottle in a cool, dry, shady place, away from direct sunlight. For daily requirements, measure small amounts of stain into a tightly stoppered bottle (about 25 ml), so that the stock solution is less likely to be contaminated.
• Do not add water to the stock solution; even the smallest amount will cause the stain to deteriorate, making staining progressively ineffective.
• Do not shake the bottle of stain before use. Shaking re-suspends precipitates, which settle on films during staining and obscure important details during microscopy.
• Do not return unused stain to the stock bottle or to the bottle used in your daily routine. Once stain is out of the bottle, it must be used
quickly or discarded.
11/24/2015

Omar Abdelrazig
The microscope
• Binoc-light microscope
• What it can do
• Use power source
• Care of microscope
11/24/2015
Omar Abdelrazig
Learning objectives
By the end you should be able to:
• demonstrate the correct set-up and use of a binocular microscope with artificial and with natural light;
• demonstrate the correct use of the x10 paired oculars and x100 oil immersion objective;*
• operate the mechanical stage correctly; name correctly 10 component parts of the microscope;
• describe the correct way in which to maintain a microscope in good working order;
• describe two ways of storing a microscope correctly; and
• demonstrate the correct way of packing a microscope for long- distance transport.
11/24/2015
The microscope
Specifications of the microscope
• -Binocular Electrical
• - with 2 Eyepieces wide filed x 10
• - 4 objectives lens X4 , X10 , X40 , X100,
• -Voltage 230 ± 10V , 50/60 HZ. 0.25 A Fuse.
• -With blue filter
• - plastic Cover. Mechanical stage
• -lamp 6V / 20w .
11/24/2015 Omar Abdelrazig
Maintenance of microscpe
Clean the microscope
1\Cleaning the lens After each use
2\ Cleaning the body Of the microscope
daily
Cover the microscope
when not in use.
(dust & other )
Checking function 1/Checking Lens
2/ Checking Mechanical
parts
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
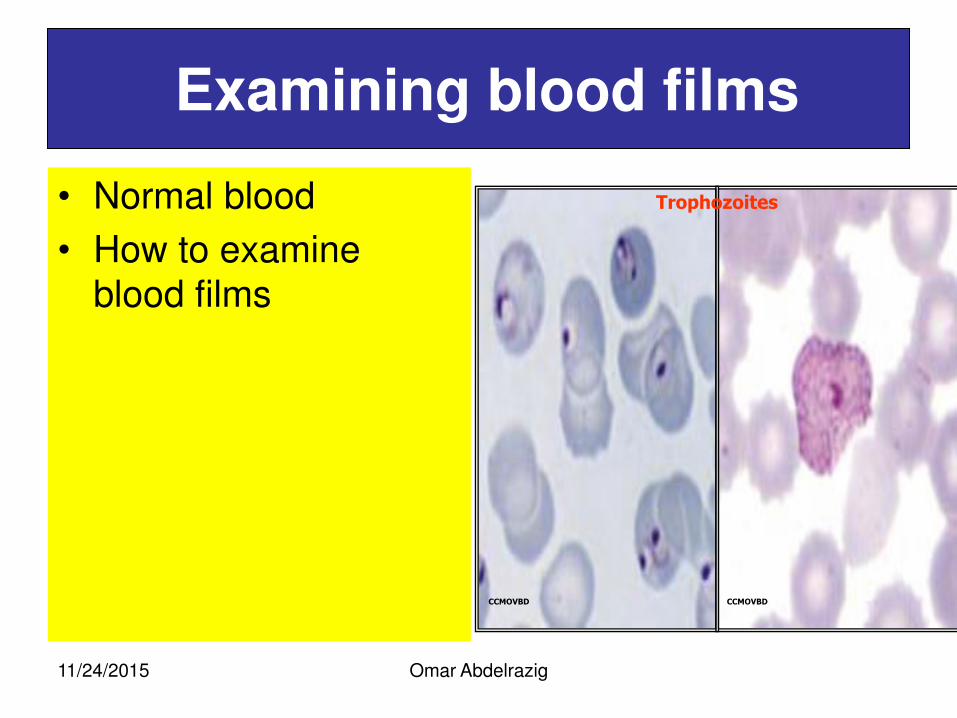
Examining blood films
• Normal blood
• How to examine blood films
CCMOVBD CCMOVBD
Trophozoites
11/24/2015
Omar Abdelrazig
Routine film exam Learning objectives
• demonstrate consistency in Giemsa malaria microscopy; demonstrate competence and consistent accuracy in identifying malaria parasites;
• demonstrate competence and consistent accuracy in differentiating between P. falciparum and P. vivax infections;
• explain why thick films are routinely used for malaria diagnosis and any exceptions to this rule;
• explain why parasite counts are made and their use;
• demonstrate consistency in counting malaria parasites in thick blood films and expressing them as parasites per microlitre of blood.
11/24/2015
Omar Abdelrazig
Examining blood film Learning objectives
• recognize and identify malaria parasites present in blood films;
• identify the stage(s) of plasmodia, the presence of individual species or mixed infections of Plasmodium falciparum, P. vivax, P. malariae and P. ovale; and establish the density of malaria parasites in the film;
• record the results of the microscopy examination on the correct form;
• inform those responsible of the findings in a timely manner;
• demonstrate their understanding of the requirement to observe patient confidentiality and ethical issues;
11/24/2015
Omar Abdelrazig
Learning objectives
• Identify the parts of a malaria parasite correctly; distinguish malaria parasites in thin and in thick films, identifying trophozoite, schizont and gametocyte stages; identify, in thin and in thick films, the four human species of malaria parasite, P. falciparum, P. vivax, P. malariae and P. ovale;
• describe and demonstrate, in thick and thin blood films, the main morphological differences between the four species of human malaria parasite;
• demonstrate common contaminants seen in blood films that are often mistaken for blood components or malaria parasites;
• recognize and name other blood parasites common to humans in your area;
• and describe ways of preventing some artifacts from contaminating blood films
11/24/2015
What does a malaria parasite look like?
• Where do you find it?
• What shape, or shapes, is it?
• What colour, or colours, is it?
• What size is it?
11/24/2015 Omar Abdelrazig
Malaria parasites are found in the red blood cells )RBC’s( of human beings:
• The RBC cycle is called the Erythrocytic cycle; it is an asexually reproductive cycle
• MP’s occupy RBC’s and grow by consuming the contents of the RBC:
- In the process malaria pigment or haematin is produced; malaria pigment does not stain but is coloured from light brown to black and can help with diagnosis
11/24/2015 Omar Abdelrazig
What are the components and colours?
With Giemsa or another Romanowsky stain the colours are:
Chromatin: RED
Cytoplasm: BLUE
Vacuole:
Sometimes present
Malaria pigment: BROWN to BLACK
Stippling: May be, usually PINK
RBC enlargement: May be
11/24/2015 Omar Abdelrazig
What shape, or shapes are they?
• MP’s can have many shapes but they all start off as a small ‘ring stage’ and progress through to ‘mature trophozoite, schizont and/or gametocyte:
• Shapes, and size, in thin films can vary from those in thick films
11/24/2015 Omar Abdelrazig
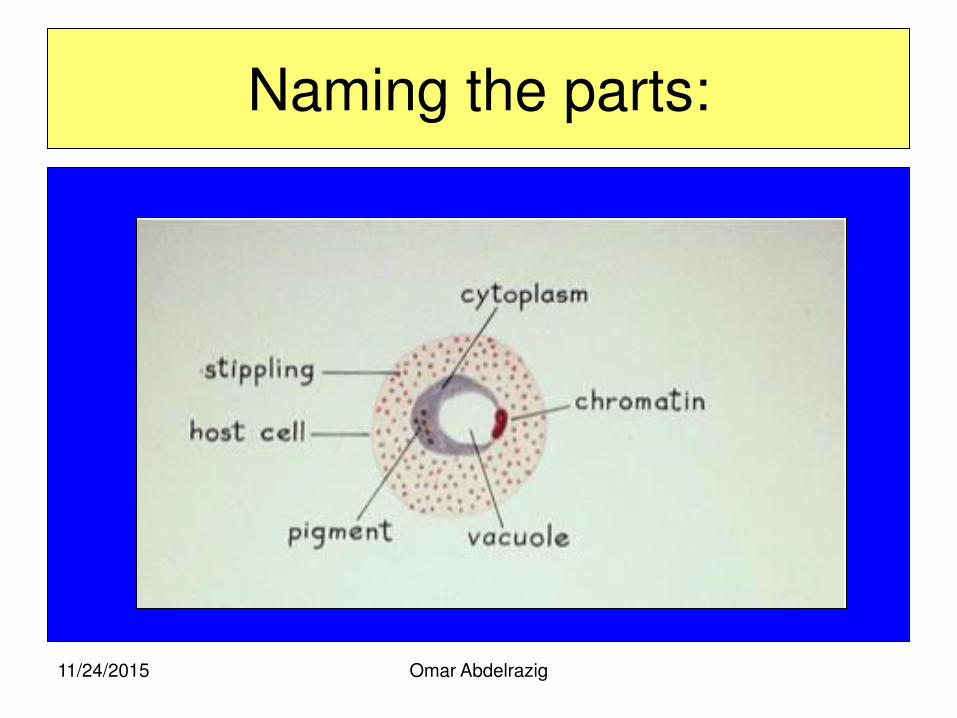
Naming the parts:
11/24/2015 Omar Abdelrazig
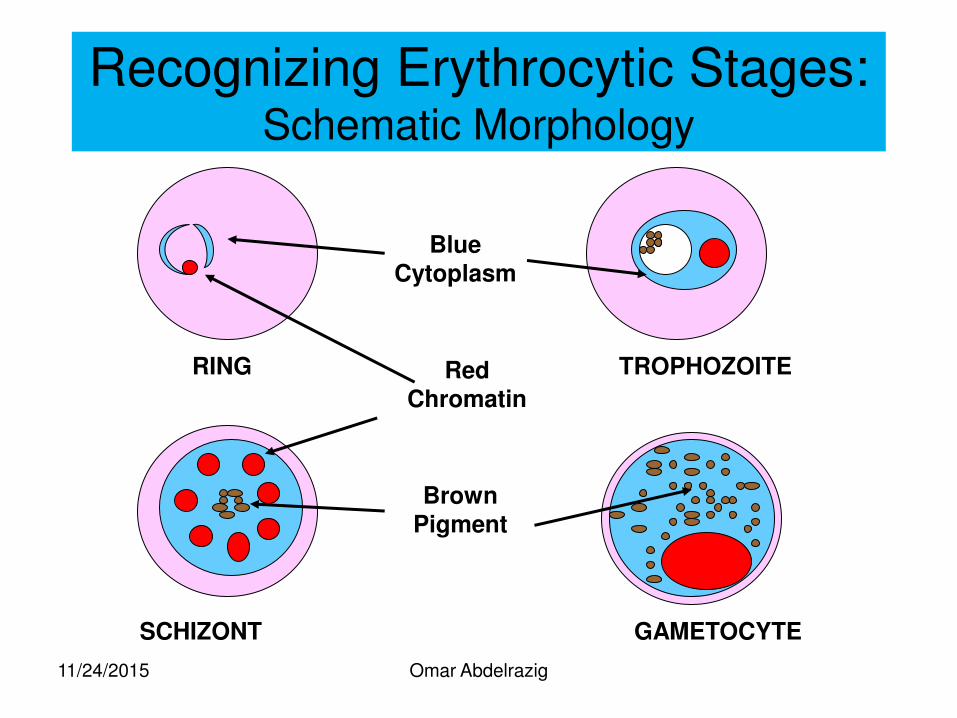
RING TROPHOZOITE
SCHIZONT GAMETOCYTE
Blue Cytoplasm
Red Chromatin
Brown Pigment
Recognizing Erythrocytic Stages: Schematic Morphology
11/24/2015 Omar Abdelrazig
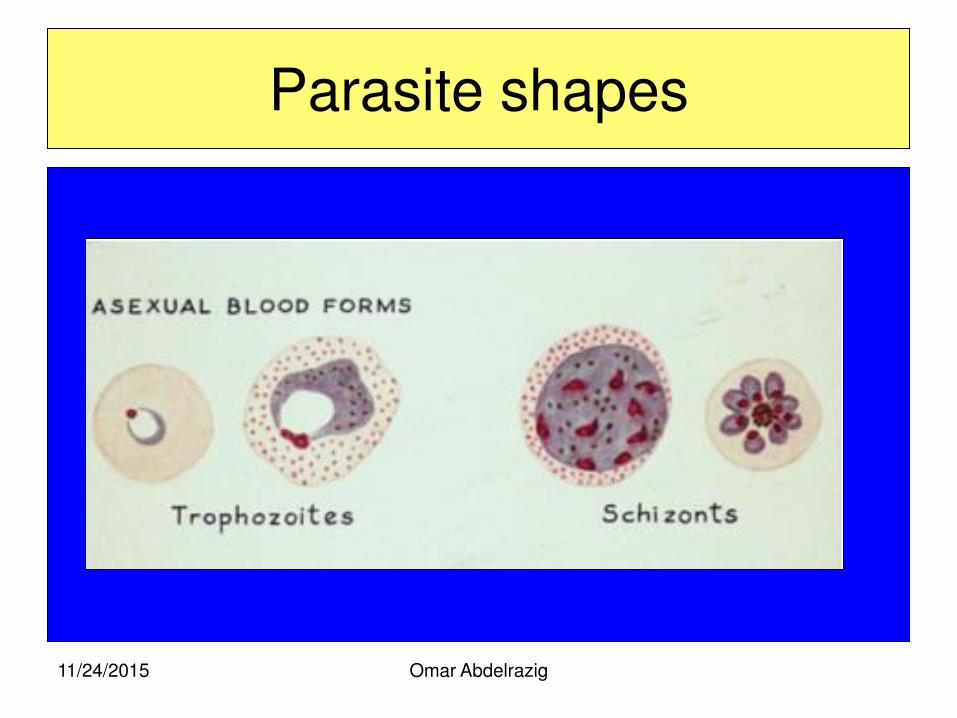
Parasite shapes
11/24/2015 Omar Abdelrazig
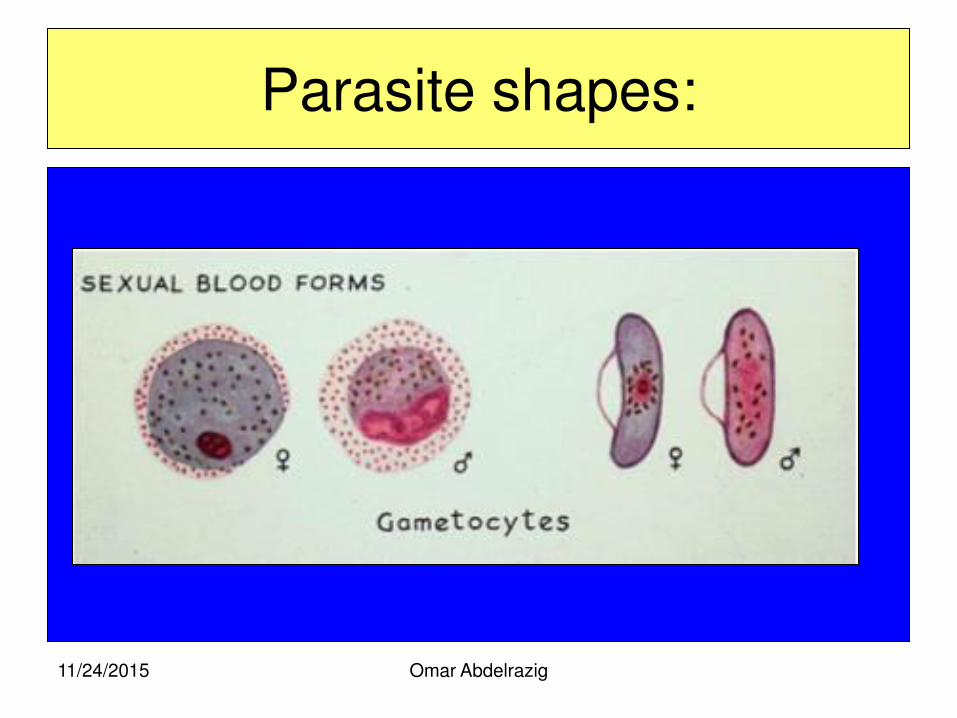
Parasite shapes:
11/24/2015 Omar Abdelrazig
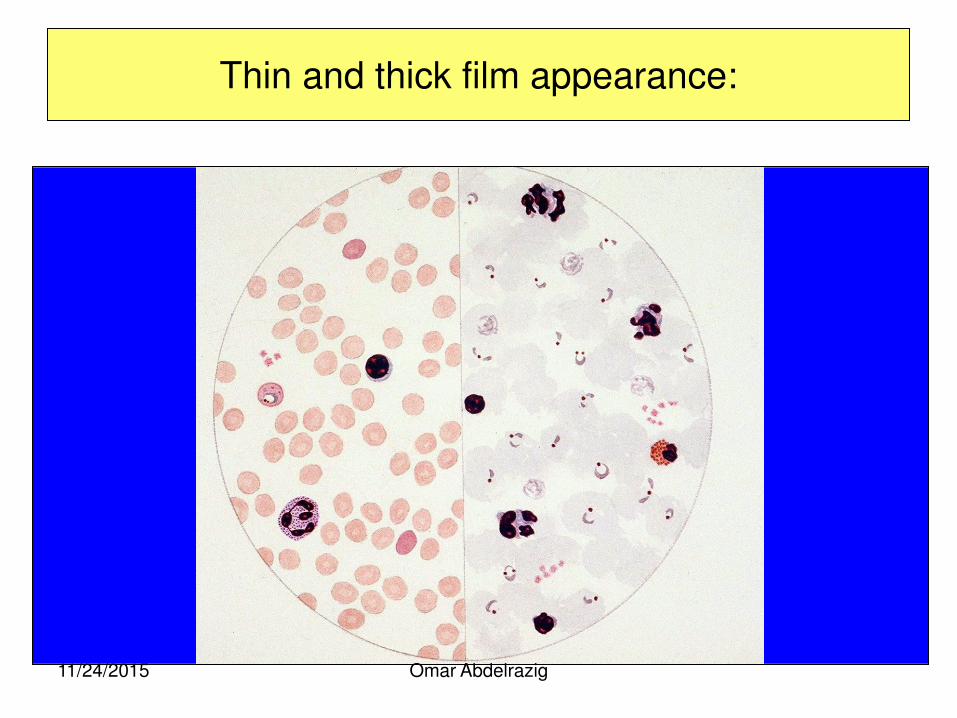
Thin and thick film appearance:
11/24/2015 Omar Abdelrazig
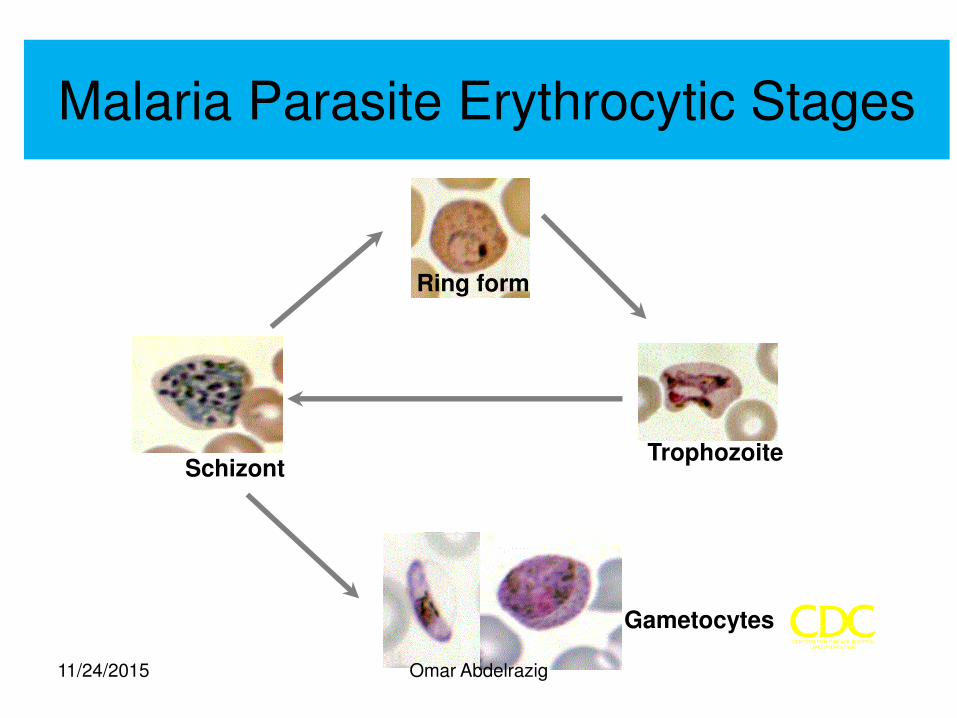
Malaria Parasite Erythrocytic Stages
Ring form
Trophozoite Schizont
Gametocytes
11/24/2015 Omar Abdelrazig
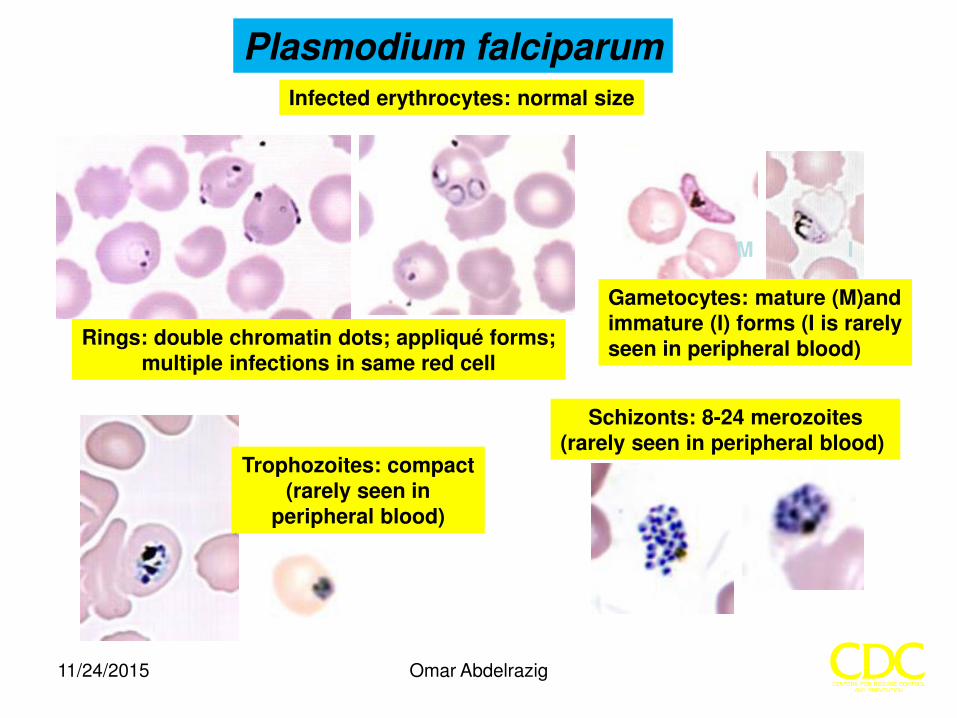
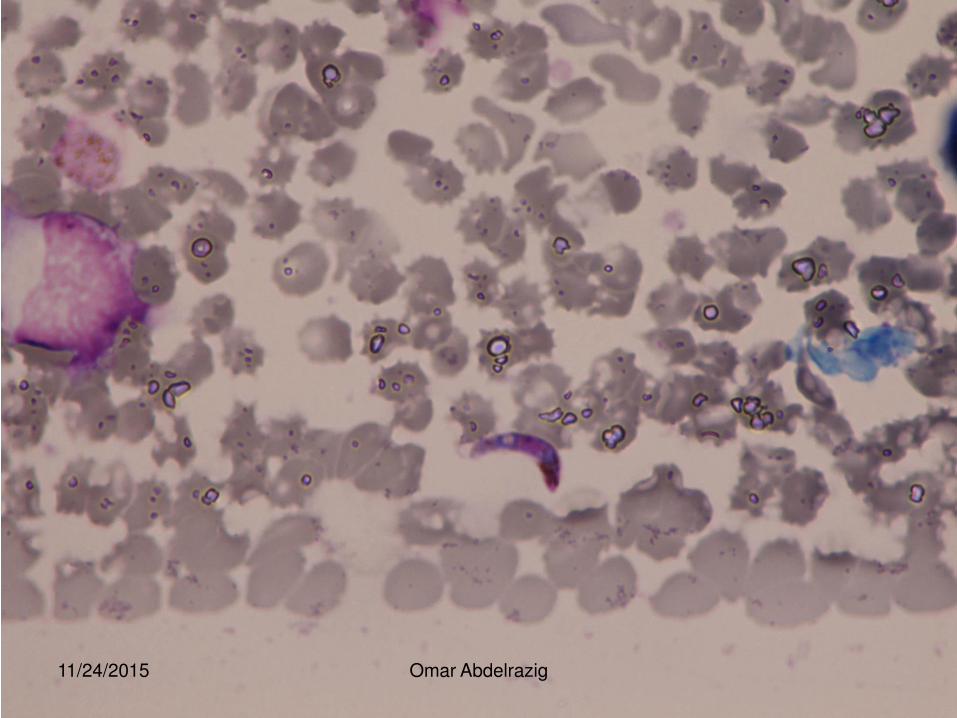
Plasmodium falciparum
Rings: double chromatin dots; appliqué forms; multiple infections in same red cell
Gametocytes: mature (M)and immature (I) forms (I is rarely seen in peripheral blood)
Trophozoites: compact (rarely seen in
peripheral blood)
Schizonts: 8-24 merozoites (rarely seen in peripheral blood)
Infected erythrocytes: normal size
M I
11/24/2015 Omar Abdelrazig
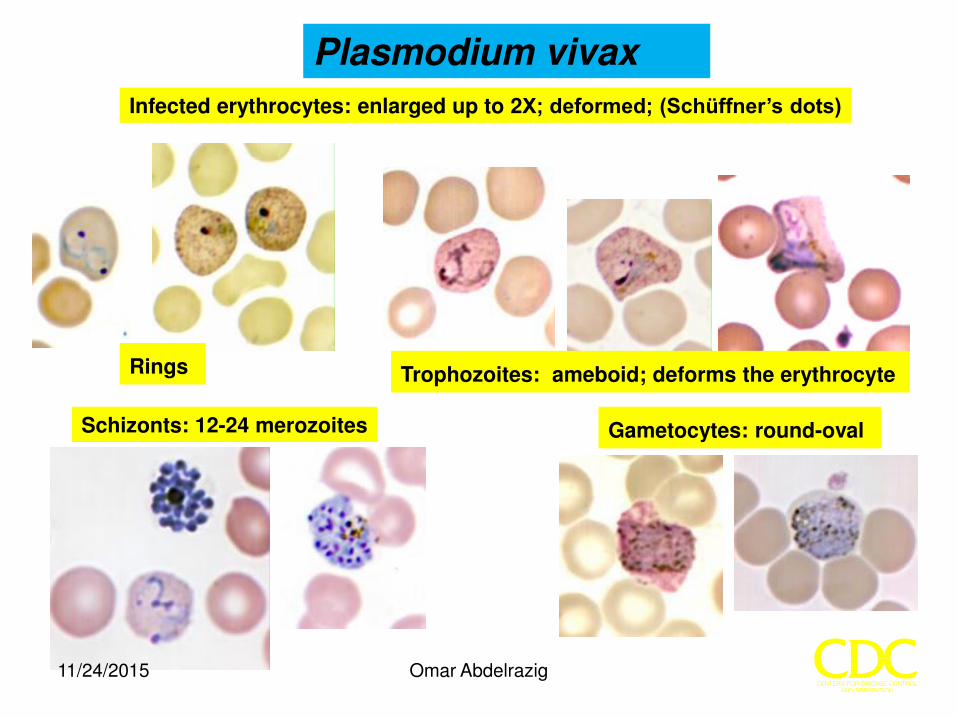
Plasmodium vivax
Trophozoites: ameboid; deforms the erythrocyte
Gametocytes: round-oval Schizonts: 12-24 merozoites
Rings
Infected erythrocytes: enlarged up to 2X; deformed; (Schüffner’s dots)
11/24/2015 Omar Abdelrazig
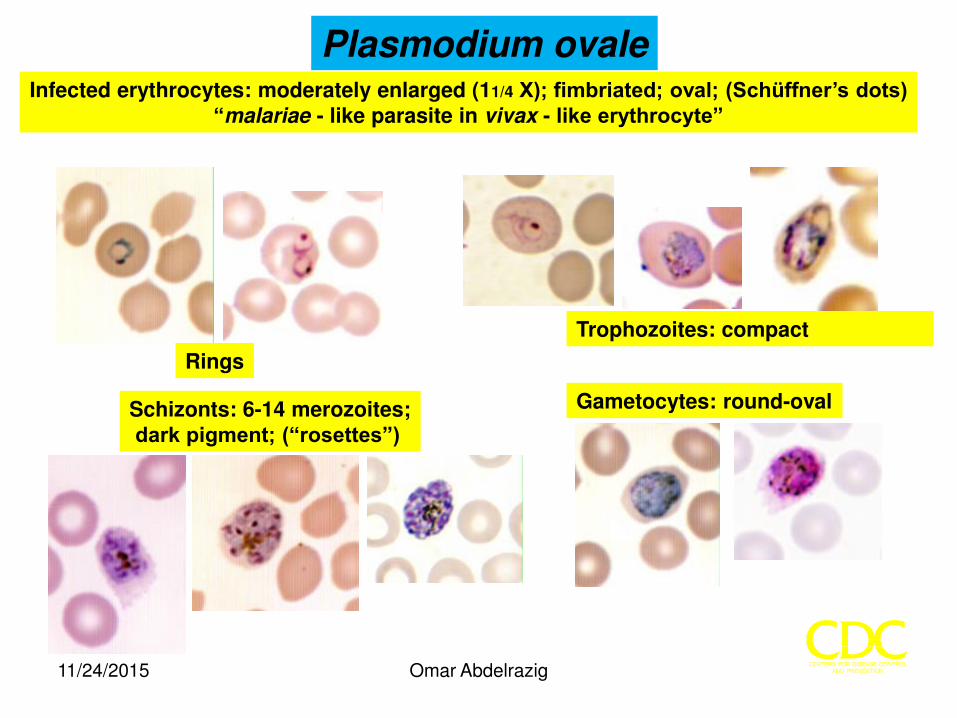
Plasmodium ovale Infected erythrocytes: moderately enlarged (11/4 X); fimbriated; oval; (Schüffner’s dots)
“malariae - like parasite in vivax - like erythrocyte”
Rings
Trophozoites: compact
Schizonts: 6-14 merozoites; dark pigment; (“rosettes”)
Gametocytes: round-oval
11/24/2015 Omar Abdelrazig
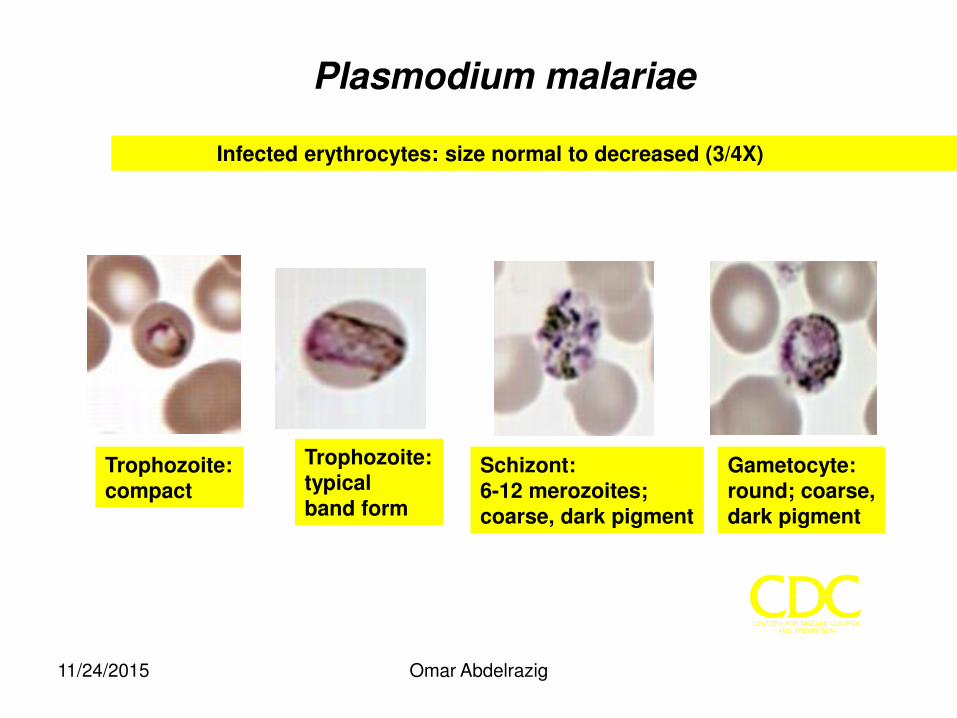
Infected erythrocytes: size normal to decreased (3/4X)
Plasmodium malariae
Trophozoite: compact
Trophozoite: typical band form
Schizont: 6-12 merozoites; coarse, dark pigment
Gametocyte: round; coarse, dark pigment
11/24/2015 Omar Abdelrazig
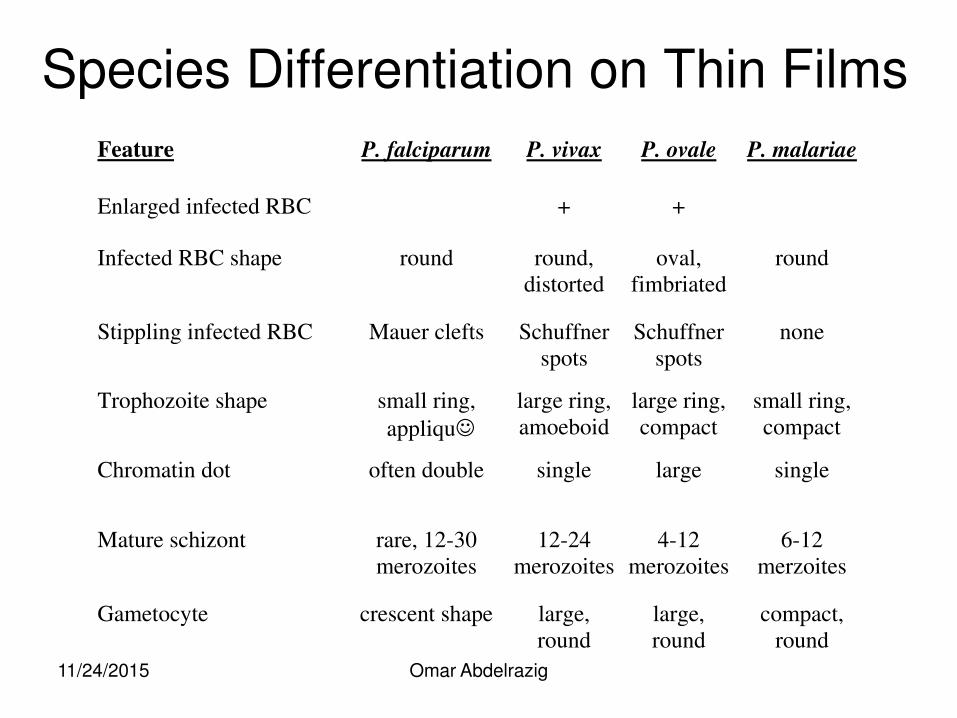
Species Differentiation on Thin Films
Feature P. falciparum P. vivax P. ovale P. malariae
Enlarged infected RBC + +
Infected RBC shape round round,
distorted
oval,
fimbriated
round
Stippling infected RBC Mauer clefts Schuffner
spots
Schuffner
spots
none
Trophozoite shape small ring,
appliqu large ring,
amoeboid
large ring,
compact
small ring,
compact
Chromatin dot often double single large single
Mature schizont rare, 12-30
merozoites
12-24
merozoites
4-12
merozoites
6-12
merzoites
Gametocyte crescent shape large,
round
large,
round
compact,
round
11/24/2015 Omar Abdelrazig
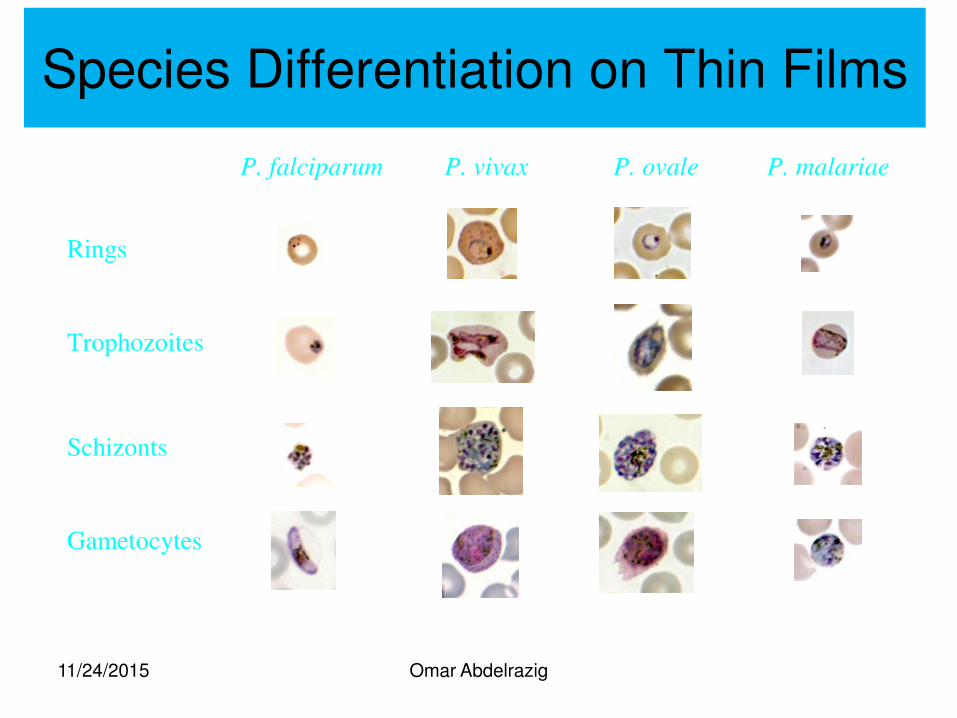
Species Differentiation on Thin Films
P. falciparum P. vivax P. ovale P. malariae
Rings
Trophozoites
Schizonts
Gametocytes
11/24/2015 Omar Abdelrazig
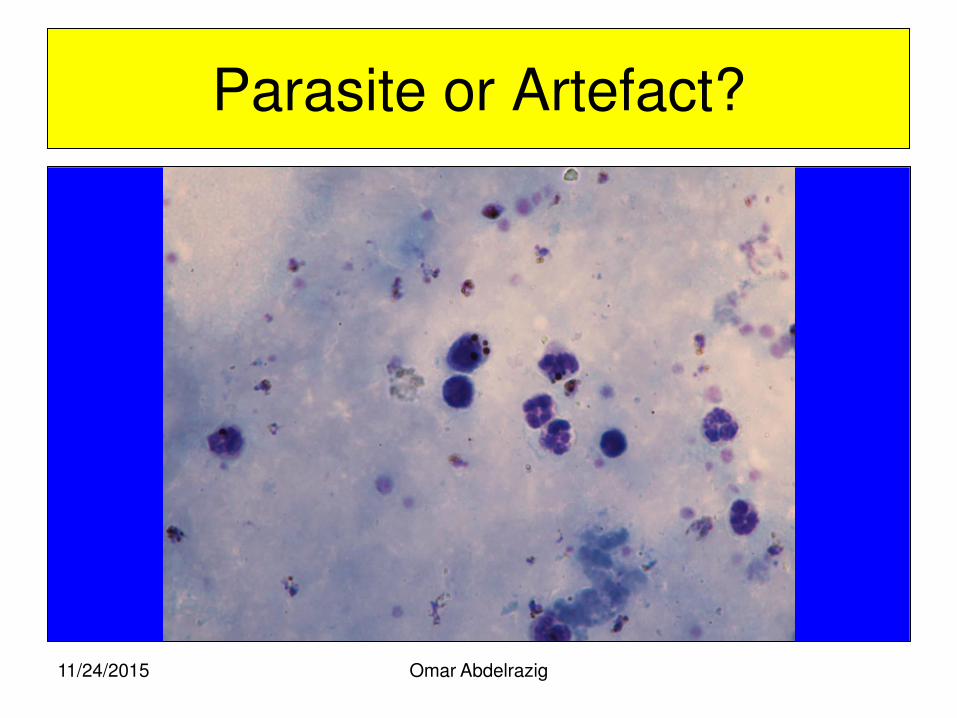
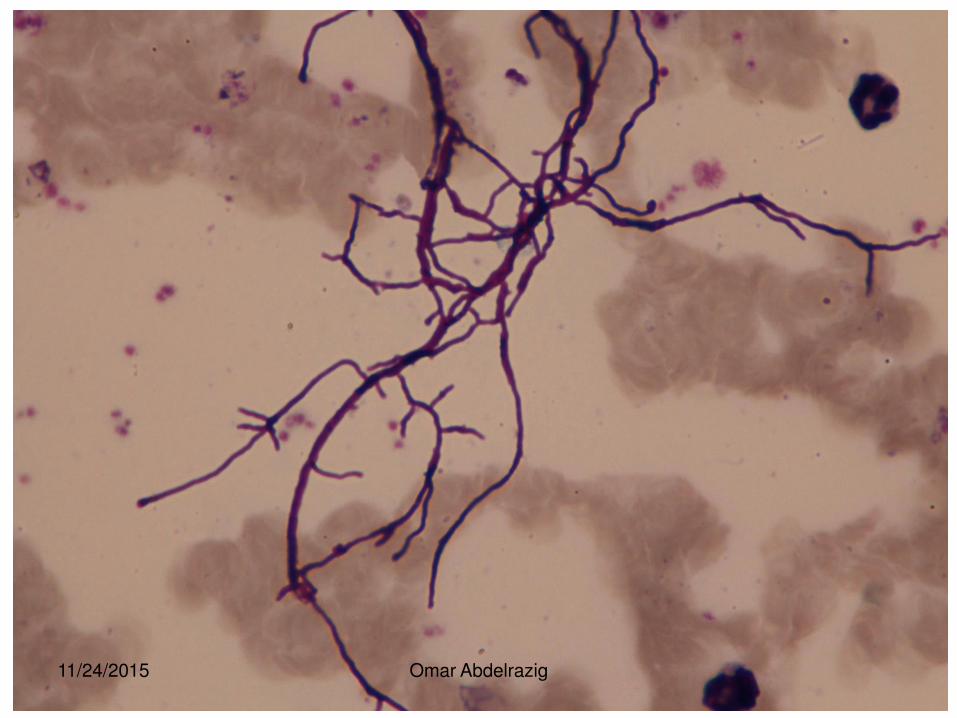
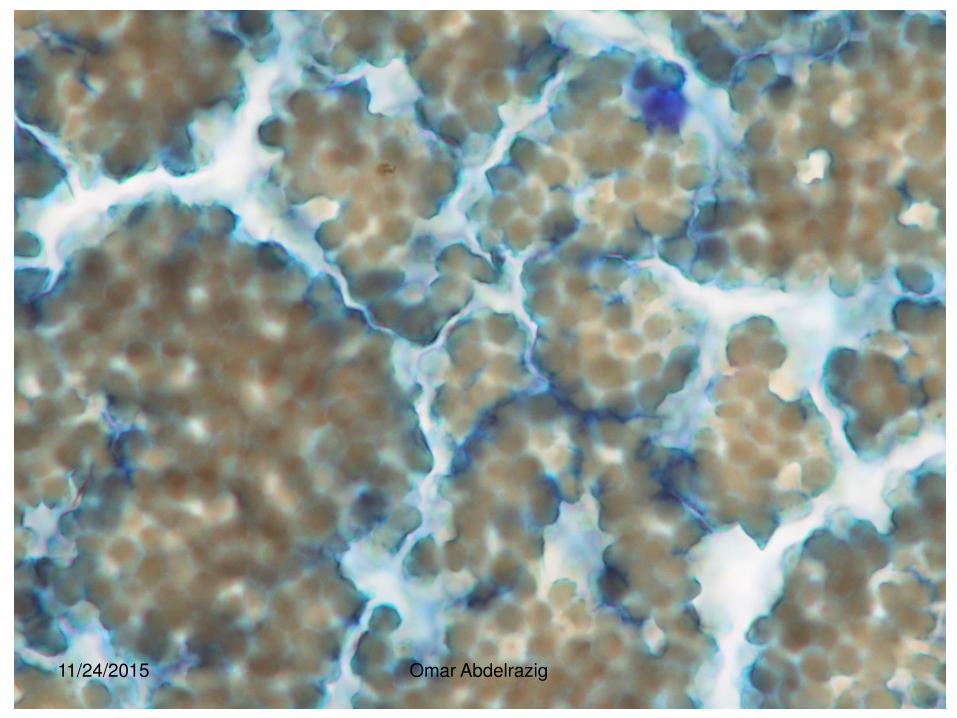
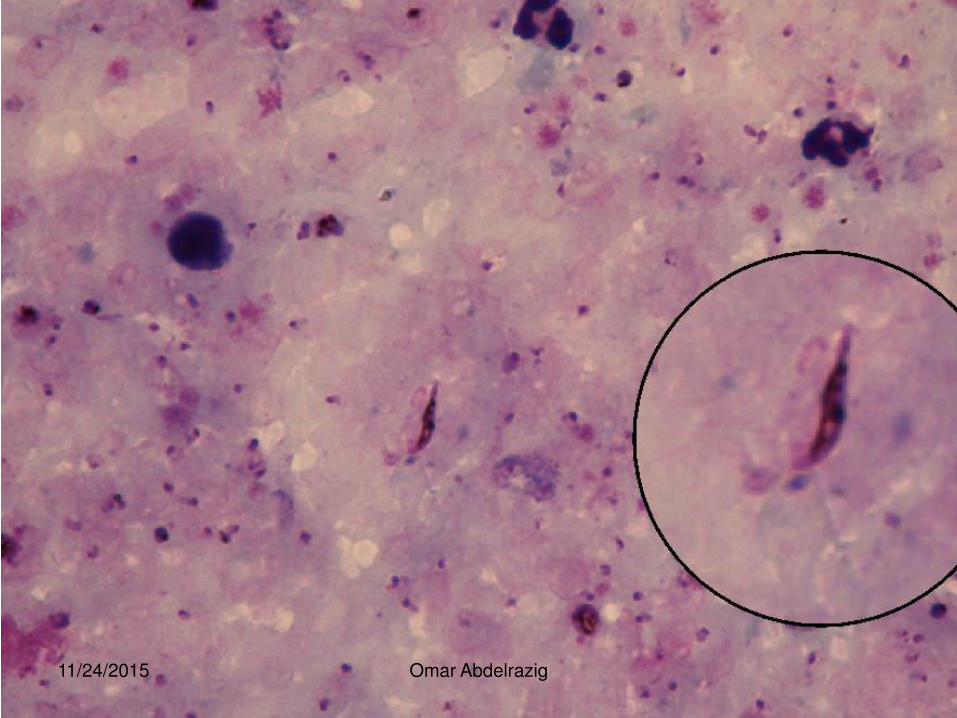
Parasite or Artefact?
11/24/2015 Omar Abdelrazig
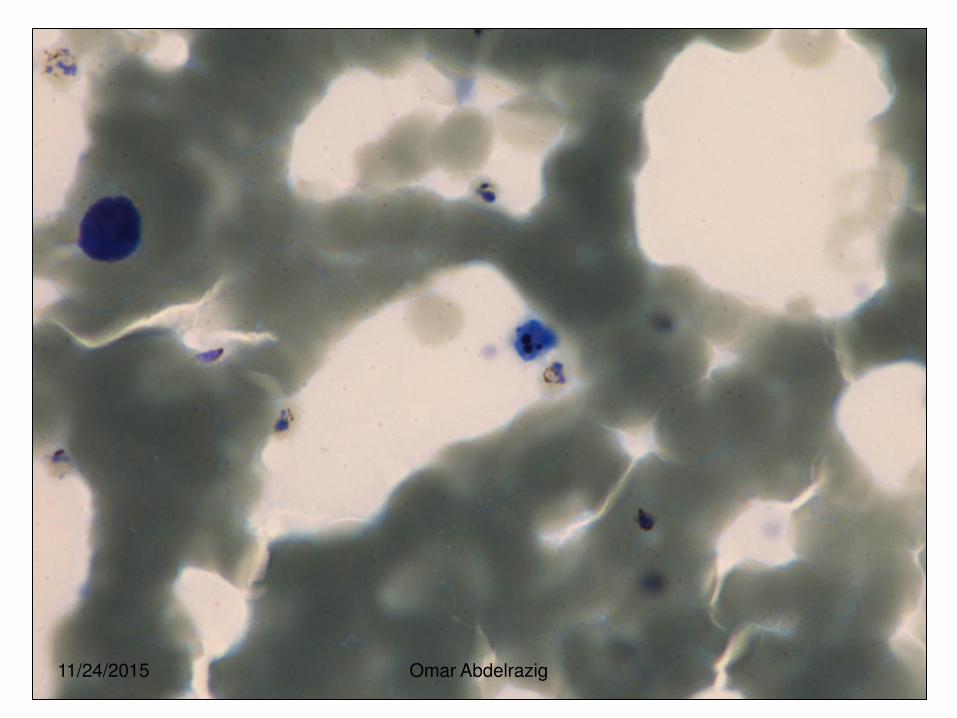
11/24/2015 Omar Abdelrazig
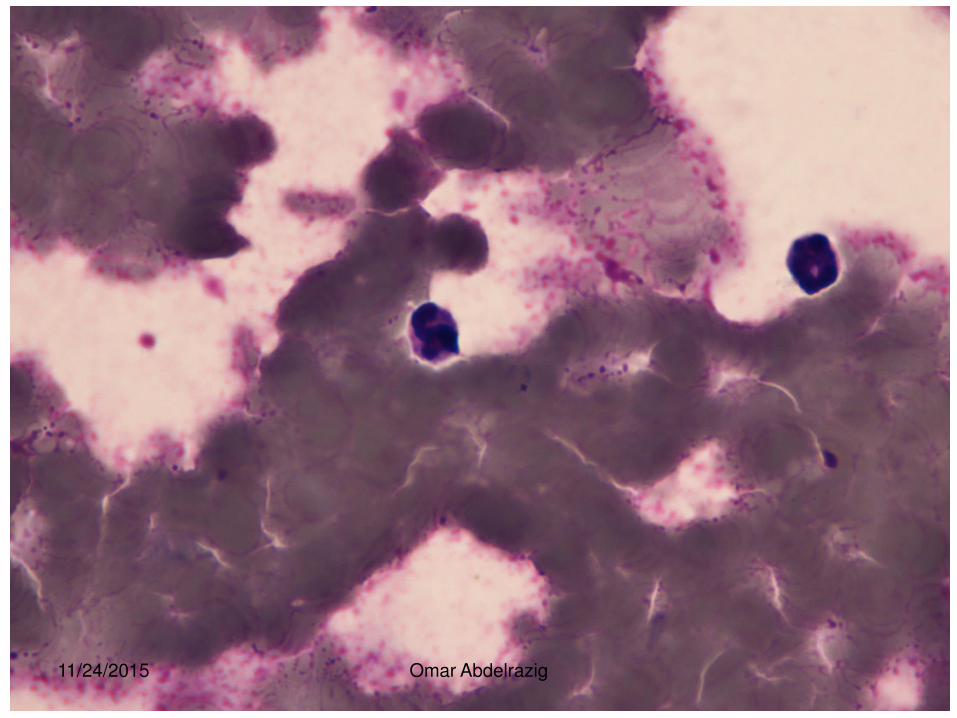
11/24/2015 Omar Abdelrazig
11/24/2015 Omar Abdelrazig
11/24/2015 Omar Abdelrazig
11/24/2015 Omar Abdelrazig
11/24/2015 Omar Abdelrazig

11/24/2015 Omar Abdelrazig
Omar Abdelrazig
Routine film examination
• Thick films
• Thin films
• Parasite counts and densities
11/24/2015
Omar Abdelrazig
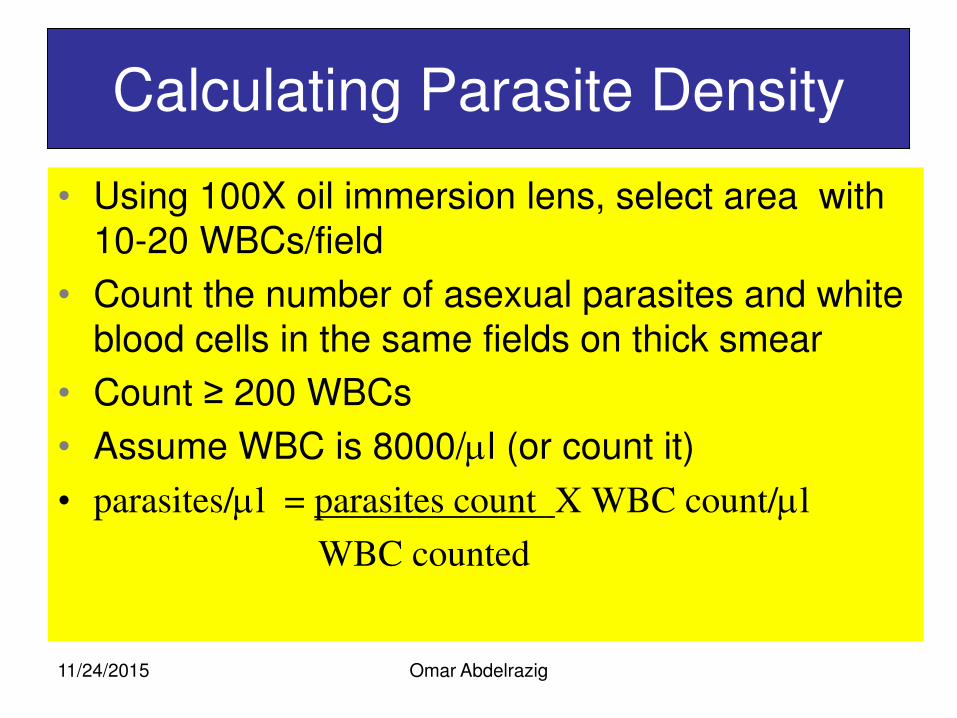
Calculating Parasite Density
• Using 100X oil immersion lens, select area with 10-20 WBCs/field
• Count the number of asexual parasites and white blood cells in the same fields on thick smear
• Count ≥ 200 WBCs
• Assume WBC is 8000/l (or count it)
• parasites/l = parasites count X WBC count/l
WBC counted
11/24/2015
Omar Abdelrazig
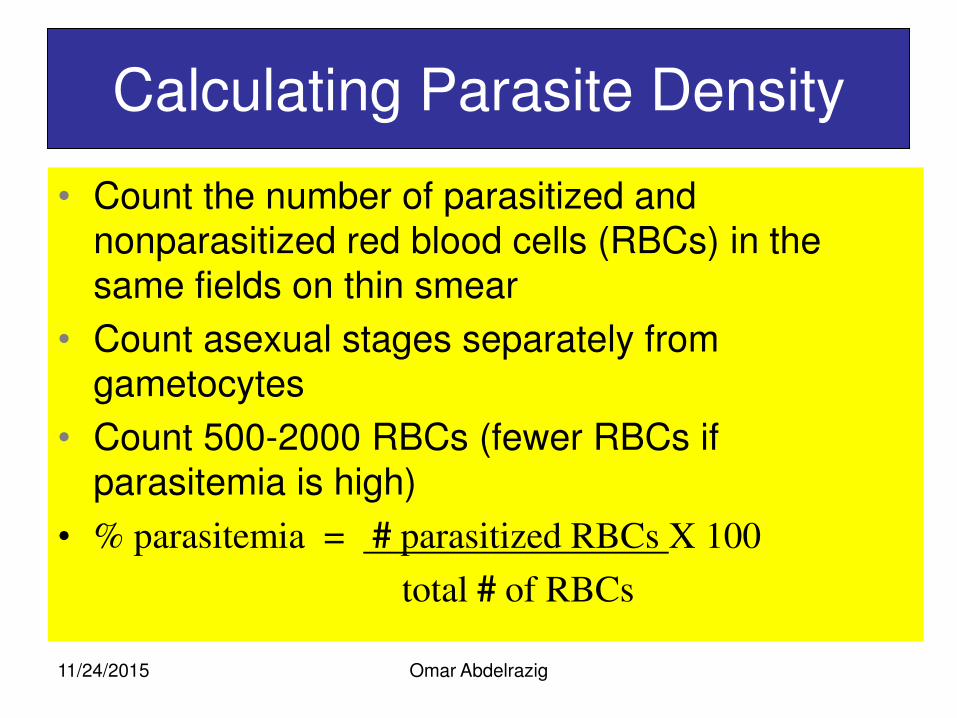
Calculating Parasite Density
• Count the number of parasitized and nonparasitized red blood cells (RBCs) in the same fields on thin smear
• Count asexual stages separately from gametocytes
• Count 500-2000 RBCs (fewer RBCs if
parasitemia is high)
• % parasitemia = # parasitized RBCs X 100
total # of RBCs
11/24/2015
Omar Abdelrazig
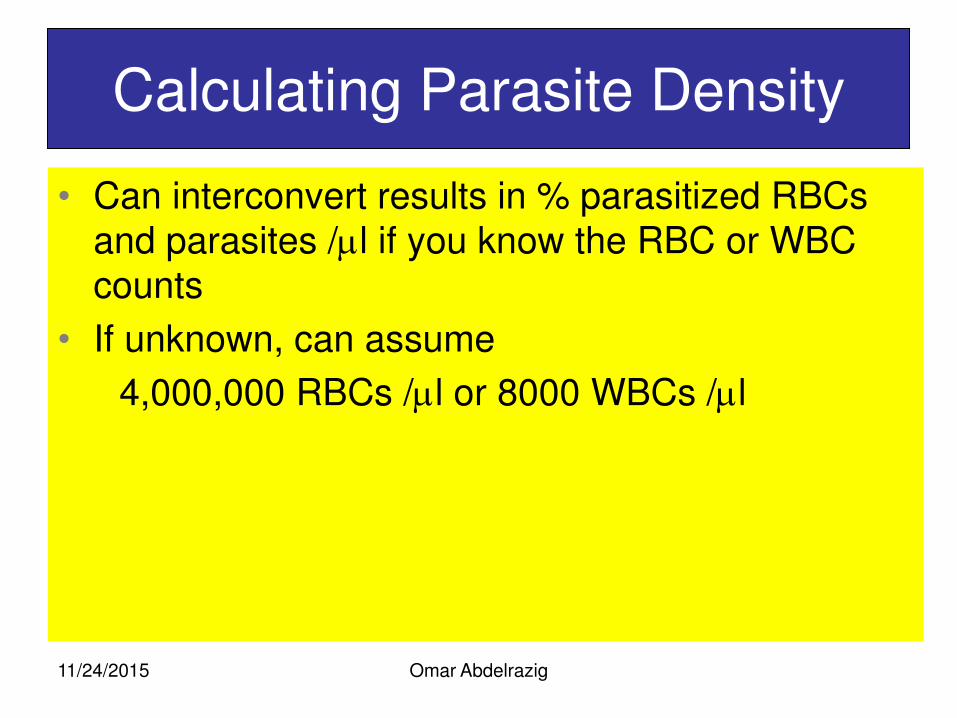
Calculating Parasite Density
• Can interconvert results in % parasitized RBCs and parasites /l if you know the RBC or WBC counts
• If unknown, can assume
4,000,000 RBCs /l or 8000 WBCs /l
11/24/2015
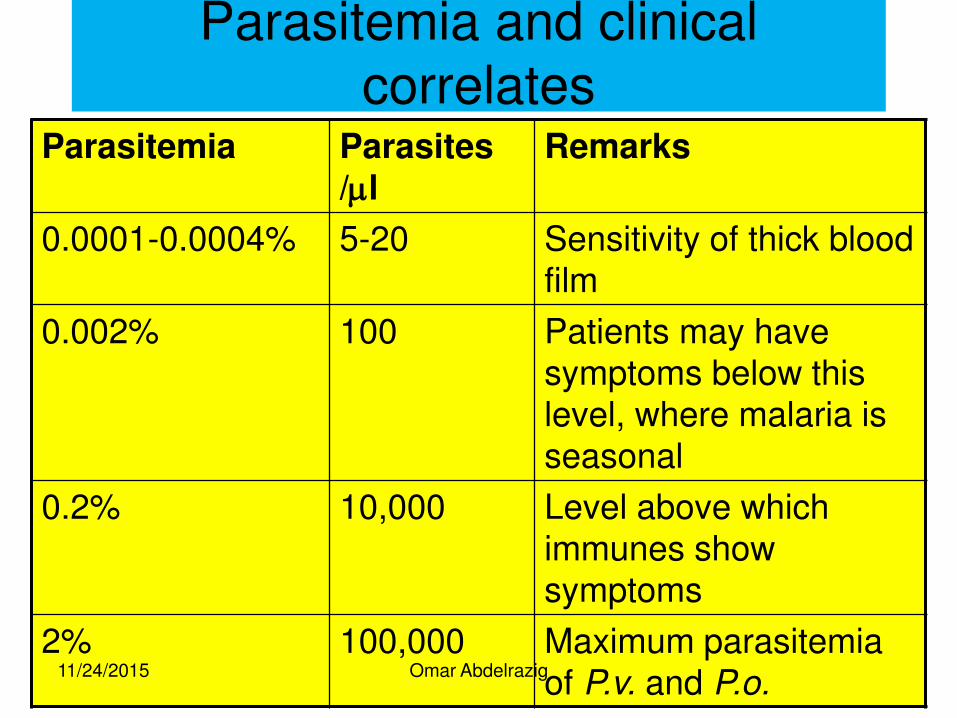
Parasitemia and clinical correlates
Parasitemia Parasites /l
Remarks
0.0001-0.0004% 5-20 Sensitivity of thick blood film
0.002% 100 Patients may have symptoms below this level, where malaria is seasonal
0.2% 10,000 Level above which immunes show symptoms
2% 100,000 Maximum parasitemia of P.v. and P.o.
11/24/2015 Omar Abdelrazig
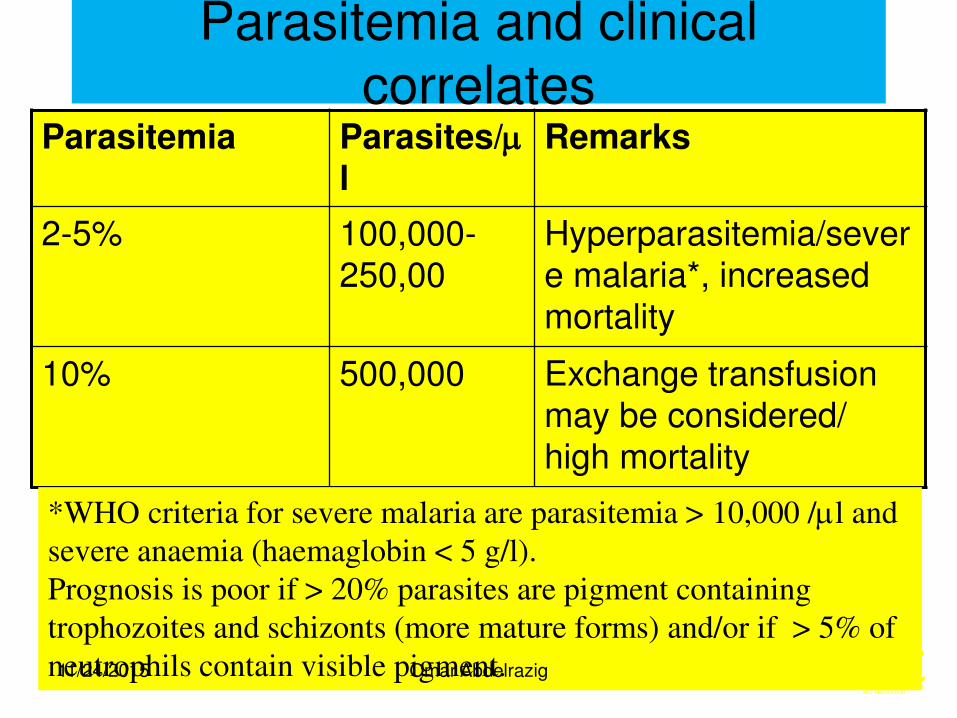
Parasitemia and clinical correlates
Parasitemia Parasites/l
Remarks
2-5% 100,000-250,00
Hyperparasitemia/severe malaria*, increased mortality
10% 500,000 Exchange transfusion may be considered/ high mortality
*WHO criteria for severe malaria are parasitemia > 10,000 /l and
severe anaemia (haemaglobin < 5 g/l).
Prognosis is poor if > 20% parasites are pigment containing
trophozoites and schizonts (more mature forms) and/or if > 5% of
neutrophils contain visible pigment. 11/24/2015 Omar Abdelrazig
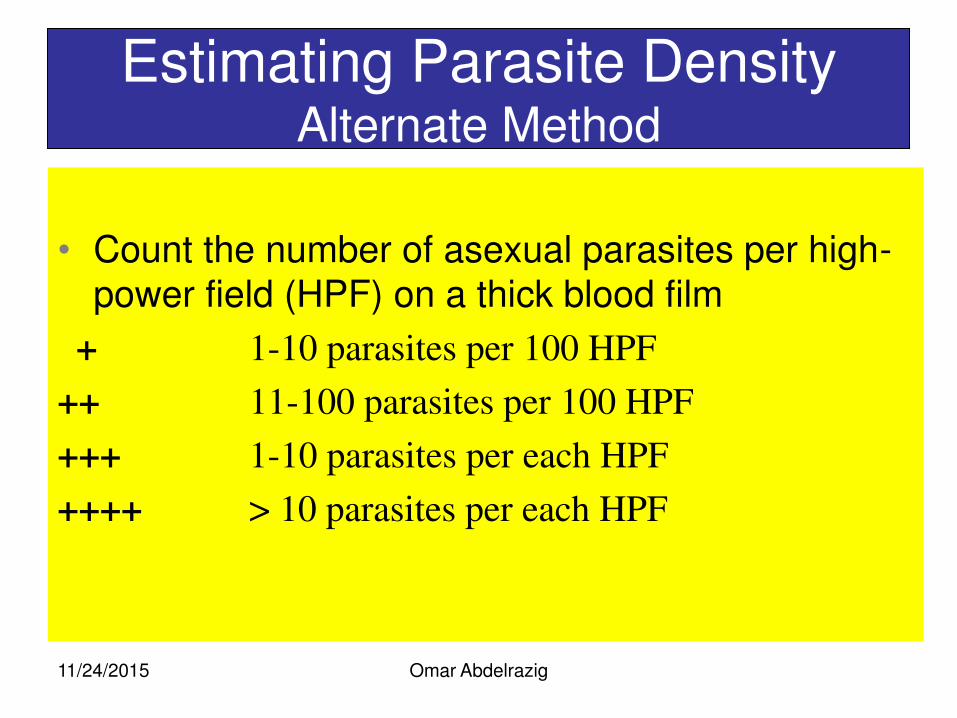
Omar Abdelrazig
Estimating Parasite Density Alternate Method
• Count the number of asexual parasites per high-power field (HPF) on a thick blood film
+ 1-10 parasites per 100 HPF
++ 11-100 parasites per 100 HPF
+++ 1-10 parasites per each HPF
++++ > 10 parasites per each HPF
11/24/2015
Omar Abdelrazig
Calculating Parasite Density
• Can interconvert results in % parasitized RBCs and parasites /l if you know the RBC or WBC counts
• If unknown, can assume
4,000,000 RBCs /l or 8000 WBCs /l
11/24/2015
Omar Abdelrazig
Calculating Parasite Density
• Can interconvert results in % parasitized RBCs and parasites /l if you know the RBC or WBC counts
• If unknown, can assume
4,000,000 RBCs /l or 8000 WBCs /l
11/24/2015
Omar Abdelrazig
The gold standard diagnostic test learning objective
By the of this unit participant should be able to :
• Identify different tests used in diagnosis of malaria.
• Evaluate which test could be the gold standard one.
11/24/2015
Malaria Diagnosis
• Clinical Diagnosis
• Malaria Blood Smear
• Fluorescent microscopy
• Antigen Detection
• Serology
• Polymerase Chain Reaction
11/24/2015 Omar Abdelrazig
Clinical Diagnosis
• Hyperendemic and holoendemic areas
• Laboratory resources not needed
• Fever or history of fever
• Sensitivity ranges from poor to high
• Often has poor specificity and predictive values
• Overlap with other syndromes
11/24/2015 Omar Abdelrazig
Malaria Blood Smear
• Remains the gold standard for diagnosis • Giemsa stain
• distinguishes between species and life cycle stages
• parasitemia is quantifiable
• Threshold of detection • thin film: 100 parasites/l
• thick film: 5 -20 parasites/l
• Requirements: equipment, training, reagents, supervision
• Simple, inexpensive yet labor-intensive
• Accuracy depends on laboratorian skill
11/24/2015 Omar Abdelrazig
Interpreting Thick and Thin Films
• THICK FILM – lysed RBCs
– larger volume
– 0.25 μl blood/100 fields
– blood elements more concentrated
– good screening test
– positive or negative
– parasite density
– more difficult to diagnose species
• THIN FILM
– fixed RBCs, single layer
– smaller volume
– 0.005 μl blood/100 fields
– good species differentiation
– requires more time to read
– low density infections can be missed
11/24/2015 Omar Abdelrazig
Malaria Blood Smear
• Prepare smears as soon as possible after collecting venous blood to avoid
• Changes in parasite morphology
• Staining characteristics
• Take care to avoid fixing the thick smear • Risk of fixing thick when thin is fixed with methanol if
both smears on same slide
• Let alcohol on finger dry to avoid fixing thick
• Be careful if drying with heat
11/24/2015 Omar Abdelrazig
Fluorescent Microscopy
• Modification of light microscopy
• Fluorescent dyes detect RNA and DNA that is contained in parasites
• Nucleic material not normally in mature RBCs
• Kawamoto technique – Stain thin film with acridine orange (AO)
– Requires special equipment – fluorescent microscope
– Staining itself is cheap
– Sensitivities around 90%
11/24/2015 Omar Abdelrazig
Quantitative Buffy Coat (QBC ®)
• Fluorescent microscopy after centrifugation
• AO-coated capillary is filled with 50-100 µl blood
• Parasites concentrate below the granulocyte layer in tube
• May be slightly more sensitive than light microscopy but some reports of 55-84%
11/24/2015 Omar Abdelrazig
Quantitative Buffy Coat (QBC ®)
• Useful for screening large numbers of samples
• Quick, saves time
• Requires centrifuge, special stains
• 3 main disadvantages – Species identification and quantification
difficult
– High cost of capillaries and equipment
– Can’t store capillaries for later reference
11/24/2015 Omar Abdelrazig
Malaria Serology – antibody detection
• Immunologic assays to detect host response
• Antibodies to asexual parasites appear some days after invasion of RBCs and may persist for months
• Positive test indicates past infection
• Not useful for treatment decisions
11/24/2015 Omar Abdelrazig
Malaria Serology – antibody detection
• Valuable epidemiologic tool in some settings
• Useful for – Identifying infective donor in transfusion-transmitted
malaria
– Investigating congenital malaria, esp. if mom’s smear is negative
– Diagnosing, or ruling out, tropical splenomegaly syndrome
– Retrospective confirmation of empirically-treated non-immunes
11/24/2015 Omar Abdelrazig
Malaria Antigen Detection • Immunologic assays to detect specific
antigens
• Commercial kits now available as immunochromatographic rapid diagnostic tests (RDTs), used with blood
• P. falciparum histidine-rich protein 2 (PfHRP-2)
• parasite LDH (pLDH)
• Monoclonal and polyclonal antibodies used in antigen (Ag) capture test
• Species- and pan-specific Ab
• Cannot detect mixed infections
• Cross reactivity with rheumatoid factor reportedly corrected
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
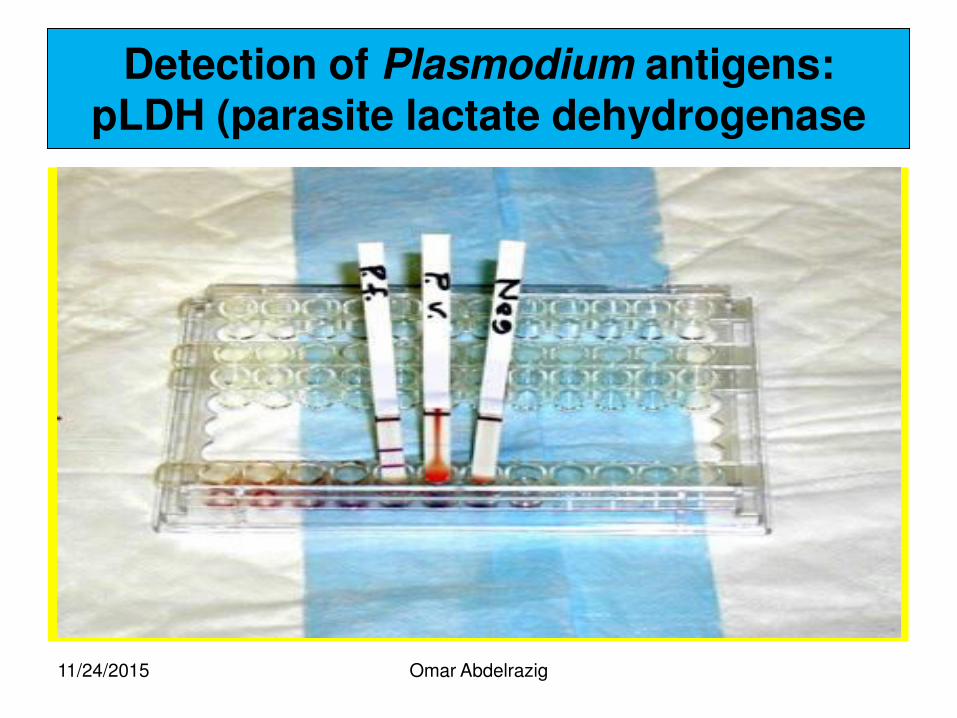
Detection of Plasmodium antigens: pLDH (parasite lactate dehydrogenase
11/24/2015
Omar Abdelrazig
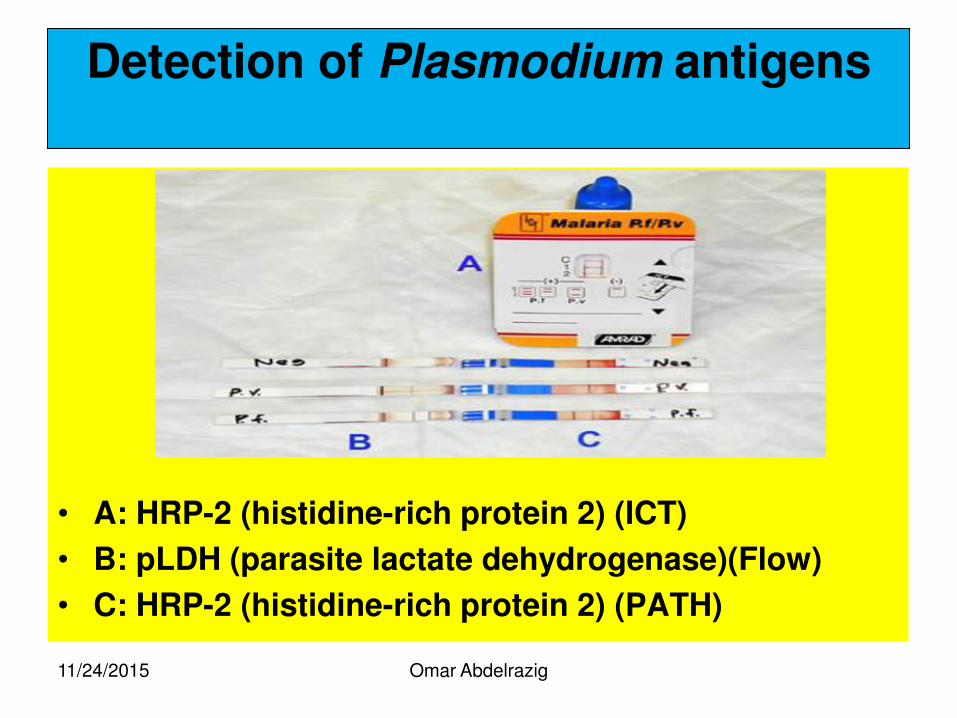
Detection of Plasmodium antigens
• A: HRP-2 (histidine-rich protein 2) (ICT)
• B: pLDH (parasite lactate dehydrogenase)(Flow)
• C: HRP-2 (histidine-rich protein 2) (PATH)
11/24/2015
Polymerase Chain Reaction (PCR)
• Threshold of detection at CDC – 0.1 parasite/µl if whole blood in tube
– 2 parasites/µl if using filter paper
• Definitive species-specific diagnosis now possible
• Can identify mutations – try to correlate to drug resistance
• Parasitemia not quantifiable
• May have use in epidemiologic studies
• Requires specialized equipment, reagents, and training
11/24/2015 Omar Abdelrazig
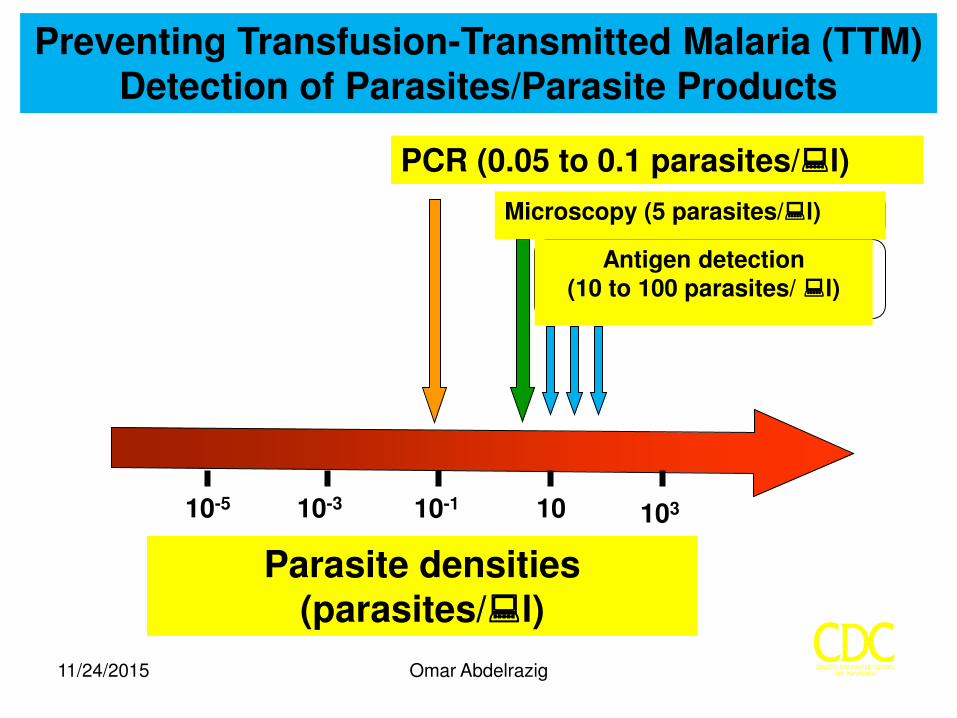
Preventing Transfusion-Transmitted Malaria (TTM) Detection of Parasites/Parasite Products
Parasite densities (parasites/l)
103 10 10-1 10-3 10-5
PCR (0.05 to 0.1 parasites/l)
Microscopy (5 parasites/l)
Antigen detection (10 to 100 parasites/ l)
11/24/2015 Omar Abdelrazig
Omar Abdelrazig
References
• Basic malaria microscopy, learners guide. WHO.
• Centre for disease control & prevention. U.S.A.
• John Storey, WHO consultant.
• Laboratories Administration, MOH. Sudan.
• Omar Abdelrazig, MOH. Sudan.
11/24/2015
Omar Abdelrazig
Questions?
Questions and disscussion .
11/24/2015