Embed Size (px)
Citation preview
7586
Saturday 18 January 1969
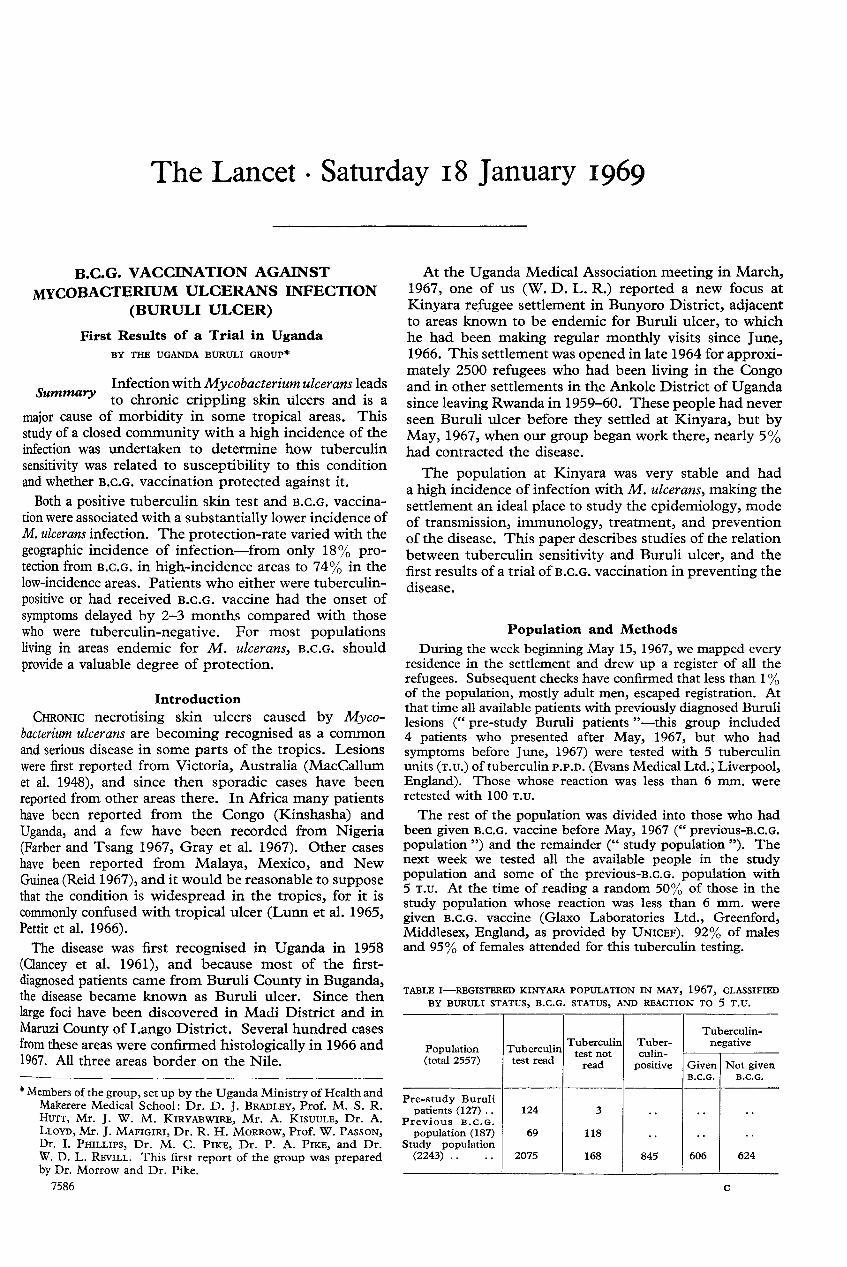
B.C.G. VACCINATION AGAINST
MYCOBACTERIUM ULCERANS INFECTION(BURULI ULCER)
First Results of a Trial in UgandaBY THE UGANDA BURULI GROUP*
Infection with Mycobacterium ulcerans leadsSummary to chronic crippling skin ulcers and is a
major cause of morbidity in some tropical areas. This
study of a closed community with a high incidence of theinfection was undertaken to determine how tuberculinsensitivity was related to susceptibility to this conditionand whether B.C.G. vaccination protected against it.Both a positive tuberculin skin test and B.C.G. vaccina-
tion were associated with a substantially lower incidence ofM. ulcerans infection. The protection-rate varied with thegeographic incidence of infection—from only 18% pro-tection from B.C.G. in high-incidence areas to 74% in thelow-incidence areas. Patients who either were tuberculin-
positive or had received B.C.G. vaccine had the onset ofsymptoms delayed by 2-3 months compared with thosewho were tuberculin-negative. For most populationsliving in areas endemic for M. ulcerans, B.C.G. shouldprovide a valuable degree of protection.
* Members of the group, set up by the Uganda Ministry of Health andMakerere Medical School: Dr. D. J. BRADLEY, Prof. M. S. R.HUTT, Mr. J. W. M. KIRYABWIRE, Mr. A. KISUULE, Dr. A.LLOYD, Mr. J. MAFIGIRI, Dr. R. H. MORROW, Prof. W. PASSON,Dr. I. PHILLIPS, Dr. M. C. PIKE, Dr. P. A. PIKE, and Dr.W. D. L. REVILL. This first report of the group was preparedby Dr. Morrow and Dr. Pike.
Introduction
CHRONic necrotising skin ulcers caused by Myco-bacterium ulcerans are becoming recognised as a commonand serious disease in some parts of the tropics. Lesionswere first reported from Victoria, Australia (MacCallumet al. 1948), and since then sporadic cases have beenreported from other areas there. In Africa many patientshave been reported from the Congo (Kinshasha) andUganda, and a few have been recorded from Nigeria(Farber and Tsang 1967, Gray et al. 1967). Other caseshave been reported from Malaya, Mexico, and NewGuinea (Reid 1967), and it would be reasonable to supposethat the condition is widespread in the tropics, for it iscommonly confused with tropical ulcer (Lunn et al. 1965,Pettit et al. 1966).The disease was first recognised in Uganda in 1958
(Clancey et al. 1961), and because most of the first-
diagnosed patients came from Buruli County in Buganda,the disease became known as Buruli ulcer. Since thenlarge foci have been discovered in Madi District and inMaruzi County of Lango District. Several hundred casesfrom these areas were confirmed histologically in 1966 and1967. All three areas border on the Nile.
At the Uganda Medical Association meeting in March,1967, one of us (W. D. L. R.) reported a new focus atKinyara refugee settlement in Bunyoro District, adjacentto areas known to be endemic for Buruli ulcer, to whichhe had been making regular monthly visits since June,1966. This settlement was opened in late 1964 for approxi-mately 2500 refugees who had been living in the Congoand in other settlements in the Ankole District of Ugandasince leaving Rwanda in 1959-60. These people had neverseen Buruli ulcer before they settled at Kinyara, but byMay, 1967, when our group began work there, nearly 5%had contracted the disease.
The population at Kinyara was very stable and hada high incidence of infection with M. ulcerans, making thesettlement an ideal place to study the epidemiology, modeof transmission, immunology, treatment, and preventionof the disease. This paper describes studies of the relationbetween tuberculin sensitivity and Buruli ulcer, and thefirst results of a trial ofB.c.G. vaccination in preventing thedisease.
Population and Methods
During the week beginning May 15, 1967, we mapped everyresidence in the settlement and drew up a register of all therefugees. Subsequent checks have confirmed that less than 1 %of the population, mostly adult men, escaped registration. Atthat time all available patients with previously diagnosed Burulilesions (" pre-study Buruli patients "-this group included4 patients who presented after May, 1967, but who hadsymptoms before June, 1967) were tested with 5 tuberculinunits (T.u.) of tuberculin P.P.D. (Evans Medical Ltd.,’ Liverpool,England). Those whose reaction was less than 6 mm. wereretested with 100 T.U.
The rest of the population was divided into those who hadbeen given B.c.G. vaccine before May, 1967 (" previous-B.c.G.population ") and the remainder (" study population "). Thenext week we tested all the available people in the studypopulation and some of the previous-B.c.G. population with5 T.u. At the time of reading a random 50% of those in thestudy population whose reaction was less than 6 mm. weregiven B.C.G. vaccine (Glaxo Laboratories Ltd., Greenford,Middlesex, England, as provided by UNICEF). 92% of malesand 95% of females attended for this tuberculin testing.
TABLE I-REGISTERED KINYARA POPULATION IN MAY, 1967, CLASSIFIEDBY BURULI STATUS, B.C.G. STATUS, AND REACTION TO 5 T.U.
112
All tuberculin testing was done by the Mantoux method(intradermal injection of 0-1 ml. of antigen), and the result wasrecorded as the transverse diameter of induration 72 hours after
injection. A reaction of 6 mm. or more was regarded as positive.Table i shows the composition of the Kinyara population basedon the tuberculin testing.
In August, 1967, we selected (by cluster sampling of families)for tuberculin retesting a random 50% of the study populationwho were tuberculin-negative. Those vaccinated were againtested with 5 T.u. and the rest with 100 T.U.
From May, 1967, to January, 1968, we held clinics every4 weeks at Kinyara for the diagnosis and treatment of Burulilesions. In February, 1968, about 80% of the refugees movedfrom Kinyara to a permanent settlement at Kyangwali, ina different area of Bunyoro, where Buruli ulcers were unknown.Since then we have held monthly clinics in both settlements.The results described here refer to the period May, 1967, toSeptember, 1968.
Clinical Procedure
Initially, in 1966, many of the patients presented withextensive and crippling ulcers, but by the time we started thestudy in May, 1967, the refugees had become aware of thecharacteristic pre-ulcerative stage and had learned to attend theclinic at the earliest sign of a lesion. Since then all suspiciouslesions have been excised completely and the biopsy specimensexamined histologically and bacteriologically (Uganda BuruliGroup 1968a).Histology
Material for histology was fixed in 10% formol saline.Sections from all lesions were examined (by M. S. R. H. andP. A. P.) after haematoxylin-eosin and Ziehl-Neelsen staining,under polarised light for foreign bodies, and after periodic-acid/Schiff and silver-methenamine staining for fungi. The
histological findings were assessed without reference to theclinical information. The specimens were classified as follows:
A. Non-reactive Buruli: extensive subcutaneous fat necrosis (withor without ulceration), with no granuloma formation. Inflammatoryresponse very slight in most. Acid-fast bacilli (A.F.B.) usuallyseen.
B. Reactive Buruli: epithelioid and giant-cell granulomas of thetuberculoid type present in subcutaneous fat, with minimum necrosis.A.F.B. seen in very small numbers.
C. Reactive lesion, presumed Buruli: as B, but no A.F.B. seen.D. Miscellaneous lesions involving subcutaneous fat: not Buruli.
The histology of a non-reactive Buruli lesion is characteristicand is not seen in any other condition (Dodge 1964). Althoughcategories B and C are identical histologically, the presence ofA.F.B. in B makes this category virtually diagnostic, whereasC is consistent with a Buruli lesion but is not diagnostic.
BacteriologySince February, 1968, most lesions have been examined
bacteriologically by inoculation of a concentrate of the specimeninto Lowenstein-Jensen medium and into a mouse’s foot-pad(Clancey 1964). M. ulcerans was identified as an A.F.B. whichgrew after incubation for 8-12 weeks at 33°C but not at 37°Cand which produced a characteristic foot-pad lesion.
Diagnostic CriteriaOf the 127 pre-study Buruli patients, the lesions in 76 were
histologically proven, while in the remaining 51 the diagnosisrested solely on clinical grounds (all diagnoses made byW. D. L. R.). Since May, 1967, we have, with one exception,accepted the diagnosis of a Buruli lesion only when this hasbeen confirmed histologically.
Results
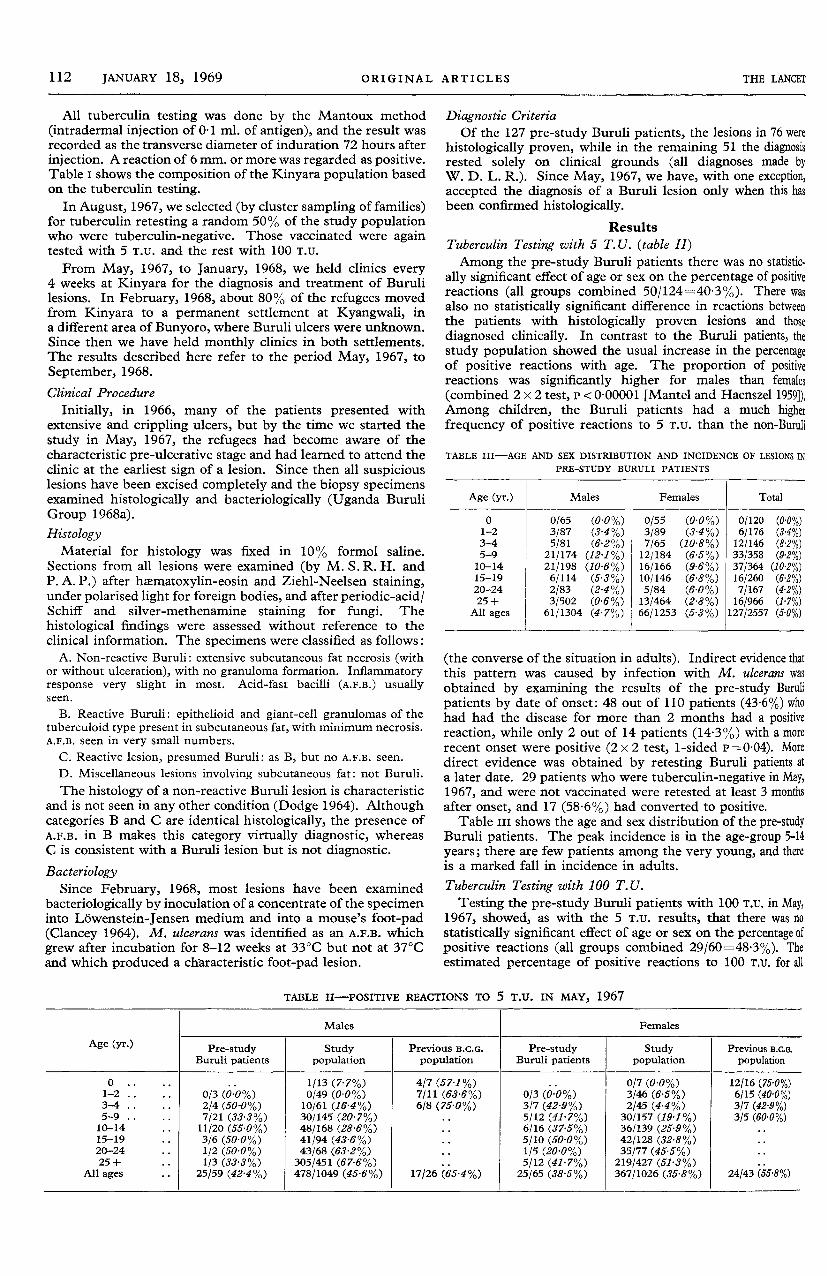
Tuberculin Testing with 5 T. U. (table II)Among the pre-study Buruli patients there was no statistic.
ally significant effect of age or sex on the percentage of positivereactions (all groups combined 50/124=40’3%). There wasalso no statistically significant difference in reactions betweenthe patients with histologically proven lesions and thosediagnosed clinically. In contrast to the Buruli patients, thestudy population showed the usual increase in the percentageof positive reactions with age. The proportion of positivereactions was significantly higher for males than females(combined 2 x 2 test, P < 0.00001 [Mantel and Haenszel 1959]),Among children, the Buruli patients had a much higherfrequency of positive reactions to 5 T.u. than the non-Buruli
TABLE III-AGE AND SEX DISTRIBUTION AND INCIDENCE OF LESIONS IN
PRE-STUDY BURULI PATIENTS
(the converse of the situation in adults). Indirect evidence thatthis pattern was caused by infection with M. ulcerans wasobtained by examining the results of the pre-study Burulipatients by date of onset: 48 out of 110 patients (43-6%) whohad had the disease for more than 2 months had a positivereaction, while only 2 out of 14 patients (14-3%) with a morerecent onset were positive (2 x 2 test, 1-sided P=0-04). Moredirect evidence was obtained by retesting Buruli patients ata later date. 29 patients who were tuberculin-negative in May,1967, and were not vaccinated were retested at least 3 monthsafter onset, and 17 (58-6%) had converted to positive.
Table ill shows the age and sex distribution of the pre-studyBuruli patients. The peak incidence is in the age-group 5-14years; there are few patients among the very young, and thereis a marked fall in incidence in adults.
Tuberculin Testing with 100 T.U.Testing the pre-study Buruli patients with 100 T.u. in May,
1967, showed, as with the 5 T.u. results, that there was nostatistically significant effect of age or sex on the percentage ofpositive reactions (all groups combined 29/60=48-3%). Theestimated percentage of positive reactions to 100 T.u. for all
TABLE II-POSITIVE REACTIONS TO 5 T.U. IN MAY, 1967
113
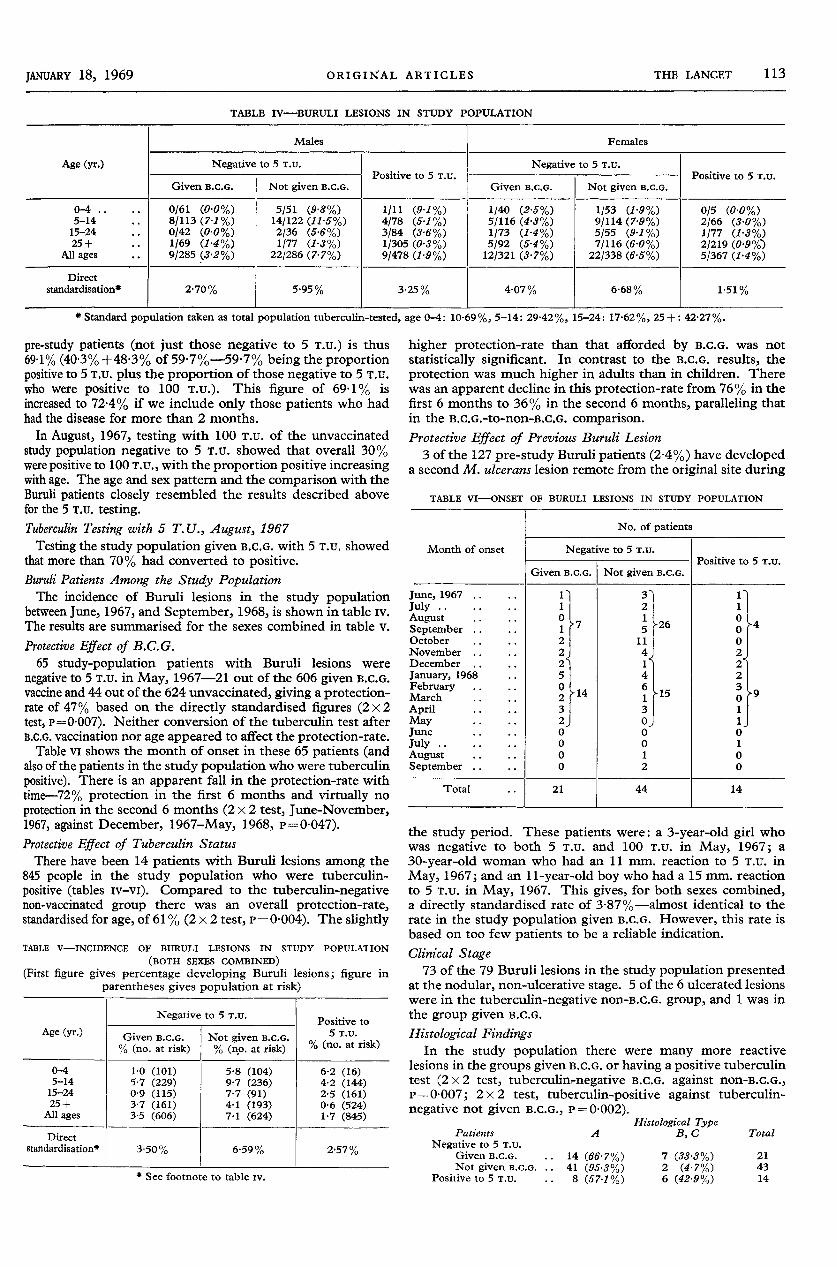
TABLE IV-BURULI LESIONS IN STUDY POPULATION
*Standard population taken as total population tuberculin-tested, age 0-4: 10-69%, 5-14: 29-42%, 15-24: 17-62%, 25+: 42-27%.pre-study patients (not just those negative to 5 T.u.) is thus
69-1% (403% +48’3% of 597%-597% being the proportionpositive to 5 T.U. plus the proportion of those negative to 5 T.u.who were positive to 100 T.U.). This figure of 69-1% isincreased to 72-4% if we include only those patients who hadhad the disease for more than 2 months.
In August, 1967, testing with 100 T.u. of the unvaccinatedstudy population negative to 5 T.u. showed that overall 30%were positive to 100 T.u., with the proportion positive increasingwith age. The age and sex pattern and the comparison with theBuruli patients closely resembled the results described abovefor the 5 T.U. testing.Tuberculin Testing with 5 T.U., August, 1967Testing the study population given B.c.G. with 5 T.u. showed
that more than 70% had converted to positive.Buruli Patients Among the Study PopulationThe incidence of Buruli lesions in the study population
between June, 1967, and September, 1968, is shown in table iv.The results are summarised for the sexes combined in table v.
Protective Effect of B.C.G.65 study-population patients with Buruli lesions were
negative to 5 T.U. in May, 1967-21 out of the 606 given B.C.G.vaccine and 44 out of the 624 unvaccinated, giving a protection-rate of 47% based on the directly standardised figures (2 x 2test, p= 0-007). Neither conversion of the tuberculin test afterB.C.G. vaccination nor age appeared to affect the protection-rate.Table vi shows the month of onset in these 65 patients (and
also of the patients in the study population who were tuberculinpositive). There is an apparent fall in the protection-rate withtime-72 % protection in the first 6 months and virtually noprotection in the second 6 months (2 x 2 test, June-November,1967, against December, 1967-May, 1968, p= 0-047).Protective Effect of Tuberculin StatusThere have been 14 patients with Buruli lesions among the
845 people in the study population who were tuberculin-positive (tables iv-vi). Compared to the tuberculin-negativenon-vaccinated group there was an overall protection-rate,standardised for age, of 61 % (2 x 2 test, P = 0-004). The slightly
TABLE V-INCIDENCE OF BURULI LESIONS IN STUDY POPULATION
(BOTH SEXES COMBINED)(First figure gives percentage developing Buruli lesions; figure in
parentheses gives population at risk)
* See footnote to table iv.
higher protection-rate than that afforded by B.C.G. was notstatistically significant. In contrast to the B.C.G. results, theprotection was much higher in adults than in children. Therewas an apparent decline in this protection-rate from 76% in thefirst 6 months to 36% in the second 6 months, paralleling thatin the B.C.G.-to-non-B.C.G. comparison.Protective Effect of Previous Buruli Lesion
3 of the 127 pre-study Buruli patients (2-4%) have developeda second M. ulcerans lesion remote from the original site during
TABLE VI-ONSET OF BURULI LESIONS IN STUDY POPULATION
the study period. These patients were: a 3-year-old girl whowas negative to both 5 T.u. and 100 T.U. in May, 1967; a30-year-old woman who had an 11 nun. reaction to 5 T.u. inMay, 1967; and an 11-year-old boy who had a 15 mm. reactionto 5 T.u. in May, 1967. This gives, for both sexes combined,a directly standardised rate of 3-87%-almost identical to therate in the study population given B.C.G. However, this rate isbased on too few patients to be a reliable indication.Clinical Stage
73 of the 79 Buruli lesions in the study population presentedat the nodular, non-ulcerative stage. 5 of the 6 ulcerated lesionswere in the tuberculin-negative non-B.C.G. group, and 1 was inthe group given B.c.G.
Histological FindingsIn the study population there were many more reactive
lesions in the groups given B.c.G. or having a positive tuberculintest (2 x 2 test, tuberculin-negative B.C.G. against non-B.C.G.,p==0007, 2 x 2 test, tuberculin-positive against tuberculin-negative not given B.c.G., P=0.002).
114
The difference between the group given B.C.G. and the tuber-culin-positive group is not statistically significant. There wasno relation between the histological findings and the timebetween onset and excisional biopsy. In the 3 pre-study Burulipatients who had a second lesion the histology of the secondlesion was in each case of the non-reactive type.
Bacteriological FindingsThe isolation-rates of M. ulcerans from lesions of different
histological types were as follows:
The bacilli may be unevenly distributed in the lesion:organisms were frequently isolated from lesions showing noA.F.B. histologically and were not isolated from some lesionswhich had abundant A.F.B. histologically. No other Myco-bacterium species were isolated.
Relation of Protection to Geographical VariationThe Kinyara settlement was divided into 14 geographical
sectors for administrative purposes (Uganda Buruli Group1968b). In 3 sectors more than 5% of the population wasinfected with M. ulcerans during the study period (combined43 out of 270=5-97%). The other 11 sectors had an averageof 2-78% of their populations infected (51 out of 1837). In the3 high-incidence sectors B.C.G. gave a protection-rate of only18 % (see table vn), whereas in the low-incidence sectors it gavea protection-rate of 74% (2x2 test, 1-sided P=003). Thisnegative association between incidence of infection and
protection from B.c.G. is paralleled by the results on thenumbers of patients who were tuberculin-positive (table vn).
TABLE VII-BURULI LESIONS IN STUDY POPULATION BY SECTOR
INCIDENCE
After direct standardisation.
In the three high-incidence sectors the tuberculin-positiveprotection-rate was 40%, compared with 70% in the low-incidence sectors.
Discussion
M. ulcerans has a considerable antigenic overlap withM. tuberculosis and with B.C.G. Evidence for this includesthe high frequency of tuberculin sensitivity among theBuruli patients, independent of age and sex, in contrast tothe non-Buruli population, and the conversion to positivetuberculin tests in patients developing Buruli lesions.Furthermore, the population that was tuberculin-positivein May, 1967, was partially protected from Buruli lesions.The most important finding is that s.c.. also conferssubstantial protection against Buruli lesions.
In man, B.C.G. protects for many years against tuber-culosis (Medical Research Council 1963), and the sameappears to be true of tuberculoid leprosy (Brown et al.
1968). It was, therefore, surprising that its efficacy inpreventing Buruli lesions appeared to wane dramaticallyafter only 6 months. (The B.C.G. used was the standardGlaxo vaccine; tuberculin retesting showed that it was
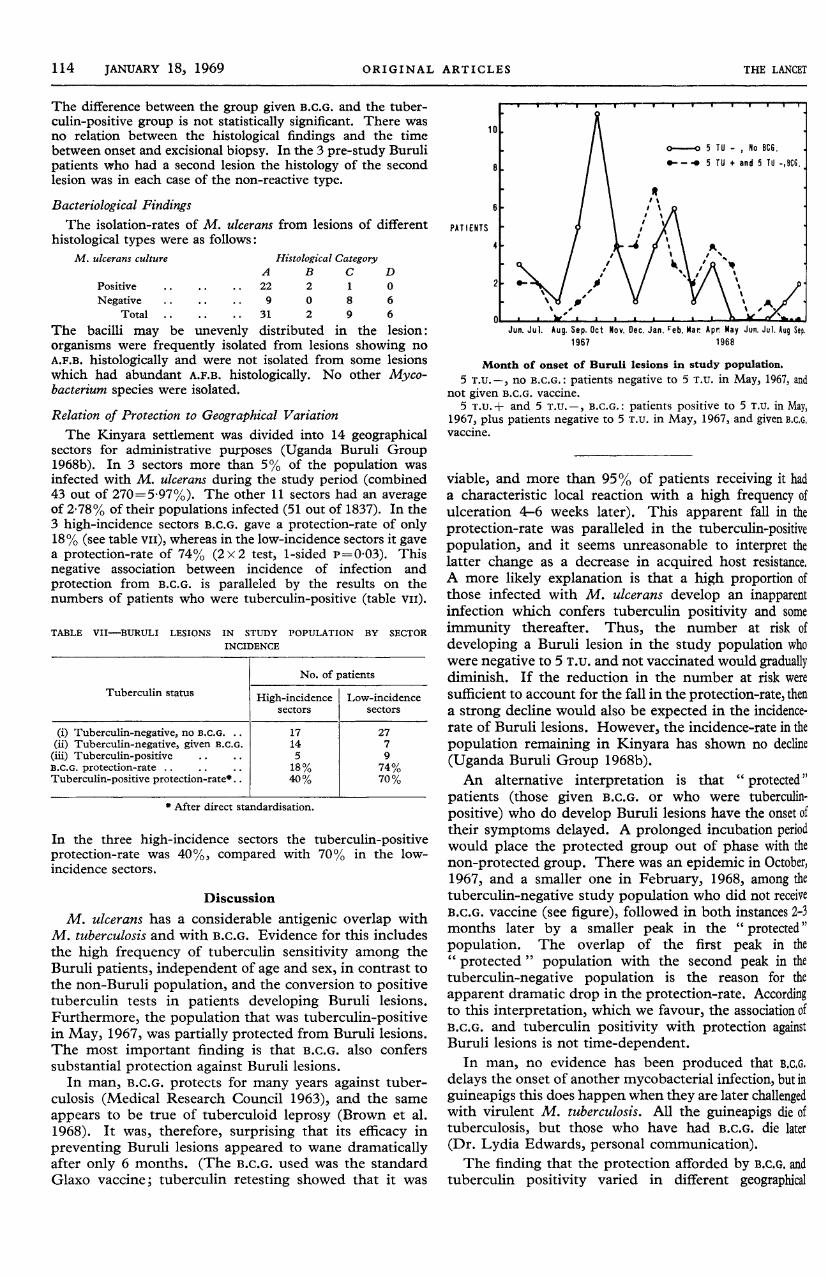
Month of onset of Buruli lesions in study population.5 T.U. -, no B.c.G.: patients negative to 5 T.u. in May, 1967, and
not given B.C.G. vaccine.5 T.U.+ and 5 T.u.-, B.C.G.: patients positive to 5 T.U. in May,
1967, plus patients negative to 5 T.u. in May, 1967, and given B.C.G.vaccine.
viable, and more than 95% of patients receiving it hada characteristic local reaction with a high frequency ofulceration 4-6 weeks later). This apparent fall in theprotection-rate was paralleled in the tuberculin-positivepopulation, and it seems unreasonable to interpret thelatter change as a decrease in acquired host resistance.A more likely explanation is that a high proportion ofthose infected with M. ulcerans develop an inapparentinfection which confers tuberculin positivity and someimmunity thereafter. Thus, the number at risk ofdeveloping a Buruli lesion in the study population whowere negative to 5 T.U. and not vaccinated would graduallydiminish. If the reduction in the number at risk weresufficient to account for the fall in the protection-rate, thena strong decline would also be expected in the incidence-rate of Buruli lesions. However, the incidence-rate in thepopulation remaining in Kinyara has shown no decline(Uganda Buruli Group 1968b).An alternative interpretation is that " protected"
patients (those given B.C.G. or who were tuberculin-
positive) who do develop Buruli lesions have the onset oftheir symptoms delayed. A prolonged incubation periodwould place the protected group out of phase with thenon-protected group. There was an epidemic in October,1967, and a smaller one in February, 1968, among thetuberculin-negative study population who did not receiveB.C.G. vaccine (see figure), followed in both instances 2-3months later by a smaller peak in the " protected"
"
population. The overlap of the first peak in the" protected " population with the second peak in thetuberculin-negative population is the reason for the
apparent dramatic drop in the protection-rate. Accordingto this interpretation, which we favour, the association ofB.C.G. and tuberculin positivity with protection againstBuruli lesions is not time-dependent.
In man, no evidence has been produced that B.C.G.
delays the onset of another mycobacterial infection, but inguineapigs this does happen when they are later challengedwith virulent M. tuberculosis. All the guineapigs die oftuberculosis, but those who have had B.C.G. die later(Dr. Lydia Edwards, personal communication).The finding that the protection afforded by B.c.G. and
tuberculin positivity varied in different geographical

115
sectors of the camp according to the incidence of Burulilesions is of both practical and theoretical importance.The incidence of Buruli lesions in some sectors was so
high that it must represent almost a maximum infection-rate. We know of no other reports of such a highfrequency, and it seems likely that the 74% protection-ratethat applies in the lower-incidence sectors is the one thatmore closely represents the value of B.c.G. to most
populations exposed to M. ulcerans.In terms of an explanation for the varying protection
with varying incidence, it is likely that where the incidenceis greater, the inocula are larger or more frequent, thusoverwhelming host immunity. This phenomenon hasbeen observed by Fenner (1957) in mice. He found thatB.C.G. gave complete protection against a low-challengeinoculum of M. ulcerans but a much reduced protectionagainst a large inoculum. This hypothesis cannot
be directly tested until the mode of transmission isknown.
A much larger proportion of the preulcerative lesionsin the " protected " population showed evidence of hostresponse, as indicated by a reactive histological picture.Just as most primary tuberculous lesions regress whenhost immunity develops, at least some Buruli nodules mayregress if not excised. Quite possibly the reactive pre-ulcerative lesions would have a greater tendency to regressspontaneously: had the criterion for surgical interventionbeen ulceration, we would have had to excise fewer lesionsbut would have observed a greater difference between the" protected " and " non-protected
"
populations. Thispossibility is supported by the fact that 5 of the 6 patientswho presented with ulcerated lesions since June, 1967,were in the " non-protected " population.For most populations exposed to M. ulcerans, B.c.G.
vaccination would probably be of great value, and in factmay very closely parallel the protection afforded by B.c.G.against tuberculosis and tuberculoid leprosy.We should like to thank the refugees who took part in this study;
their trust and cooperation were a continuous encouragement. Weshould like to thank the doctors in Masindi and Hoima Hospitals fortheir help, Prof. R. Blowers and Dr. I. Sutherland for advice, andMr. R. Fernandes and Mr. P. Nickson for technical assistance.
Special acknowledgement is due to the Uganda Ministry of Cultureand Community Development and to the United Nations HighCommission for Refugees for permission to work in the settle-ments.
This study was made possible by a generous grant from the Well-come Trust. Mr. Kiryabwire was in receipt of a Makerere UniversityCollege Research Grant for a period at the start of the study. Dr.M. C. Pike was on attachment from the Medical Research Council’sStatistical Research Unit.
Requests for reprints should be sent to Dr. R. H. Morrow,Makerere University College Medical School, P.O. Box 7072,Kampala, Uganda.
REFERENCES
Brown, J. A. K., Stone, M. M., Sutherland, I. (1968) Br. med. J. i, 24.Clancey, J. K. (1964) J. Path. Bact. 88, 175.- Dodge, O. G., Lunn, H. F., Oduori, M. L. (1961) Lancet, ii, 951.
Dodge, O. G. (1964) J. Path. Bact. 88, 167.Farber, E. R., Tsang, A. (1967) Archs Surg., Chicago, 95, 297.Fenner, F. (1957) Am. Rev. Tuberc. pulm. Dis. 76, 76.Gray, H. H., Kingma, S., Kok, S. H. (1967) Trans. R. Soc. trop. Med. Hyg.
61, 712.Lunn, H. F., Connor, D. H., Wilks, N. E., Barnley, G. R., Kamunvi, F.,
Clancey, J. K., Bee, J. D. A. (1965) E. Afr. med. J. 42, 275.MacCallum, P., Tolhurst, J. C., Buckle, G., Sissons, H. A. (1948) J. Path.
Bact. 60, 93.Mantel, N., Haenszel, W. (1959) J. natn Cancer Inst. 22, 719.Medical Research Council (1963) Br. med. J. i, 973.Pettit, J. H. S., Marchette, N. J., Rees, R. J. W. (1966) Br. J. Derm. 78,
187.
Reid, I. S. (1967) Med. J. Aust. i, 427.Uganda Buruli Group (1968a) Unpublished.- (1968b) Unpublished.
EXCESSIVE URINARY EXCRETION OF
CERTAIN PORPHYRINOGENIC STEROIDS IN
HUMAN ACUTE INTERMITTENT PORPHYRIA
A. GOLDBERG M. R. MOORE A. D. BEATTIE
OF THE M.R.C. GROUP IN IRON AND PORPHYRIN METABOLISM, ANDDEPARTMENT OF MEDICINE, WESTERN INFIRMARY, GLASGOW
P. E. HALL J. MCCALLUM J. K. GRANTOF THE UNIVERSITY DEPARTMENT OF STEROID BIOCHEMISTRY,
ROYAL INFIRMARY, GLASGOW
Summary Individual urinary 17-oxosteroid excretionwas measured by gas-liquid chromato-
graphy in 6 patients with acute intermittent porphyria.There were significant elevations of ætiocholanolone
glucuronide in 2 patients, of dehydroepiandrosteroneglucuronide and sulphate in 2 patients, and of epiandro-sterone sulphate in 3 patients. Of the 4 patients whoshowed these abnormalities, 2 were in relapse, and 2 hadhad severe attacks 8 months and 21/2 years before theinvestigation. The 2 patients with a normal pattern of17-oxosteroid excretion in urine had been in remission for15 years and 41/2 years. In the light of these results, freedehydroepiandrosterone or its sulphate were injectedintraperitoneally into rats every 24 hours, and causedsignificant elevations of hepatic &dgr;-aminolævulic acid
synthetase, reaching maximal levels at about 72 hours.This enzyme is the rate-limiting enzyme of hæm bio-
synthesis and is strikingly increased in the liver in humanand experimentally-induced acute porphyria. An endo-genous factor has thus been found in some patients withacute porphyria which may explain certain clinical
associations, such as the age of onset after puberty, and theoccurrence of attacks not attributable to exogenous factors.
Introduction
ACUTE intermittent porphyria, an inborn error of
metabolism, is the most important of the porphyriadiseases in the U.K. It is usually diagnosed by thedetection in the urine of excessive quantities of the hsemprecursors, 8-aminolsevulic acid (A.L.A.), and porpho-bilinogen (P.B.G.). It has also been established thatpatients have in their livers a striking increase of theenzyme 8-aminolxvulic acid synthetase (A.L.A. synthetase).The gastrointestinal and neuropsychiatric clinical mani-festations of this disease have one main characteristic-
intermittency. The cause of these intermittent attacks hasbeen partly ascribed to the administration of drugs, suchas barbiturates, alcohol, or certain steroids of the typecontained in contraceptive pills, or a diet very low incarbohydrate and protein, but in many cases there is noevidence for any of these factors. It has been suspectedthat certain endogenous factors, possibly of a hormonalnature, may be responsible for the initiation of attacks.This view was promoted and strengthened by certainstriking clinical associations. The onset of the diseaseseldom occurs before the age of puberty, and in a series of50 patients the youngest was a girl of 11 years. There isa female predominance (3 females to 2 males), and themain age of onset is in the third decade in women and inthe fourth decade in men. The disease rarely occurs aftermiddle age. Out of 31 women the attack was associated in7 with the menstrual period, and in 6 others there wasamenorrheca; in 6 women attacks were associated withpregnancy, 3 in its first few weeks, and 3 just after itstermination (Goldberg 1959).