Embed Size (px)
Citation preview

Case ReportOptimal Molecular Methods in Detecting p190BCR-ABL
Fusion Variants in Hematologic Malignancies A Case Reportand Review of the Literature
Rebecca J Sonu1 Brian A Jonas2 Denis M Dwyre1
Jeffrey P Gregg1 and Hooman H Rashidi1
1Department of Pathology and Laboratory Medicine University of California Davis Medical Center Sacramento CA 95817 USA2Department of Internal Medicine Division of Hematology and Oncology University of California Davis Medical CenterSacramento CA 95817 USA
Correspondence should be addressed to Hooman H Rashidi hoomanrashidiucdmcucdavisedu
Received 20 February 2015 Revised 22 March 2015 Accepted 26 March 2015
Academic Editor Stephen Langabeer
Copyright copy 2015 Rebecca J Sonu et alThis is an open access article distributed under the Creative CommonsAttribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Patients with BCR-ABL1 positive hematologic malignancies and Philadelphia-like B-lymphoblastic leukemia (B-ALL) are potentialcandidates for targeted therapywith tyrosine kinase inhibitors (TKI) Before TKIs patients with B-ALL had amuchworse prognosisand current treatments with targeted TKI therapy have improved outcomes Thus the detection of BCR-ABL1 is crucial and a falsenegative BCR-ABL1 result may adversely affect patient care We report a case of a 76-year-old male with a new diagnosis of B-ALLwho was initially found to be BCR-ABL1 negative by quantitative polymerase chain reaction (PCR) A concurrent qualitative PCRwas performed which detected a positive BCR-ABL1 result that was confirmed by a next generation sequencing (NGS) based assayand identified as the rare fusion variant e1a3 of p190BCR-ABL Based on this result the patient was placed on dasatinib as a targetedtherapy In the era of molecular diagnostic medicine and targeted therapy it is essential to have an understanding of the limitationsof molecular assays and to follow a comprehensive diagnostic approach in order to detect common abnormalities and rare variantsIncorporating NGS methods in an algorithmic manner into the standard diagnostic PCR-based approach for BCR-ABL1 will aidin minimizing false negative results
1 Introduction
The Philadelphia chromosome (Ph) t(922)(q34q112) isconsistently seen in chronic myelogenous leukemia (CML)25 of adult B-acute lymphoblastic leukemia (B-ALL) 2ndash4of childhood B-ALL and rarely in acute myeloid leukemias[1] The Ph chromosome results from the breakpoint in theBCR gene on chromosome 22 which usually occurs in themajor breakpoint cluster region (M-bcr) between exons e12ndashe16 (also known as b1ndashb5) The breakpoints in the ABL geneon chromosome 9 occur usually at exon a2 From thesebreakpoints the resulting fusion transcripts are known ase13a2 (b2a2) and e14a2 (b3a2) [2] These fusion transcriptsare then translated into a 190-kDa protein p190BCR-ABLencoded by the fusion transcript e1a2 in theminor breakpoint
region (m-bcr) which is commonly associated with B-ALLin both adults and children The 210-kDa protein known asp210BCR-ABL is most commonly seen in CML [2] Ultimatelythese alternative chimeric BCR-ABL1 proteins produced areresponsible for the oncogenic properties of these hematologicneoplasms Additionally due to alternative splicing othertranscript variants from the major and minor breakpointregions can occur with or independently of the commonfusion transcripts described above
We report a case of a 76-year-oldmale with a new diagno-sis of B-ALL that was initially found to be BCR-ABL1 negativeby quantitative PCR A concurrent qualitative PCR was alsoperformed which was able to detect a low level positive BCR-ABL1 result which was subsequently confirmed by a nextgeneration sequencing (NGS) based assay and identified as
Hindawi Publishing CorporationCase Reports in HematologyVolume 2015 Article ID 458052 6 pageshttpdxdoiorg1011552015458052
2 Case Reports in Hematology
(a) (b)
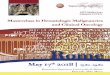
Figure 1 B-Lymphoblastic leukemia (a) Peripheral blood (Wright-Giemsa 100x) showing a circulating large sized blast (b) Bone marrowbiopsy (hematoxylinamp eosin 50x) showing fibroticmarrowwith small area of immaturemononuclear cells No areas of normal hematopoiesiswere seen
the rare BCR-ABL1 fusion variant e1a3 of p190BCR-ABL Basedon this positive result the patient was ultimately placed ondasatinib as a targeted therapy
2 Case Report
21 Clinical History and Pathology A 76-year-old man witha history of coronary artery disease chronic obstructivepulmonary disease prostate cancer in remission tobaccoand alcohol abuse and Schizoaffective disorder was admittedafter being found to have a platelet count of 10 Kmm3(normal 130ndash400Kmm3) He was significantly fatigued andhad a petechial rash After transfusion of a unit of plateletshis complete blood count showed a white blood cell count(WBC) of 71 Kmm3 (normal 45ndash11 Kmm3) hemoglobin131 gdL (normal 135ndash175 gdL) platelets of 34Kmm3 and aleukoerythroblastic peripheral blood smear showing 2 cir-culating blasts (Figure 1(a)) Computed tomography showedmild splenomegaly but no distinct lymphadenopathy wasnoted Other studies including a metabolic panel liverfunction tests coagulation panel and viral serologies werenegativeThe patient had no known previous history of CMLor peripheral blood findings suggestive of CML
A subsequent bone marrow biopsy showed a hypercellu-lar marrow (approximately 85 of total cellularity) with 95of the cellularity involved by diffuse sheets of monotonousround to slightly irregular lymphoblasts (Figure 1(b)) Thebiopsy showedmarked reticulin fibrosis Immunohistochem-ical stains performed on the core biopsy showed blasts thatwere positive for CD34 CD79a CD10 PAX-5 TdT andCD20 Flow cytometry showed that the blasts were positivefor dim CD45 CD34 CD10 CD19 CD20 (dim) HLA-DR CD79a TdT CD22 (subset) and IgM and negative formyeloperoxidase (MPO) CD13 CD33 and CD117 Over-all these findings were consistent with a B-lymphoblasticleukemia
Molecular studies for the BCR-ABL1 mutation showed alow positive qualitative PCR result for the BCR-ABL1 fusion
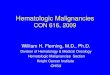
transcript (Figure 2) A repeat qualitative PCR test recon-firmed the low positive result However the quantitative PCRtesting for the BCR-ABL1 fusion transcripts (p190 and p210isoforms) yielded negative results Due to this discrepancyperipheral blood was sent for testing on the FoundationOneHeme assay (Foundation Medicine Cambridge MA) a nextgeneration sequencing (NGS) based assay Targeted RNA-seqfound 17 transcripts for the variant e1a3 p190BCR-ABL fusionDNA was sequenced to a median coverage depth of 492x Noother fusion transcripts were identified including p210BCR-ABL
or p230BCR-ABL Previous validation experiments confirmedthe sensitivity for detection of fusion events as gt99 fortumor cell fractions between 20 and 50 and 97 for tumorcell fractions of 10 High specificity was confirmed forall fusion events (PPV gt 95) [3] In addition a PTPN11V428M mutation of unclear significance was also detectedCytogenetics and FISH studies failed to yield results mainlydue to the lack of cell growth as per the outside performinginstitution T- andB-cell gene rearrangement studieswere notperformed
Due to the positive BCR-ABL1 result the patient wasstarted on induction therapy with dasatinib and steroids asper the protocol described by Foa et al [4] One monthafter starting therapy the patientrsquos counts improved (WBCcount was 87 Kmm3 with normal differential hemoglobinwas 109 gdL and platelets were 171 Kmm3) and he becametransfusion independent He tolerated the treatment well andby Day 98 of dasatinib treatment the patient continued to bein complete hematologic remission Monitoring for the BCR-ABL1 transcript will be performed with the qualitative PCRtesting and if negative with the NGS assay
3 Materials and Methods
The qualitative BCR-ABL1 RNA test was performed at theUniversity of California Davis Medical Center MolecularPathology Laboratory (Sacramento CA) The Lightcyclerassay detects theBCR-ABL1 fusion transcripts b3a2 b2a2 and
Case Reports in Hematology 3
Cycle number
0055
0050
045
0040
0035
0030
0025
0020
0015
0010
0005
0000
minus0005
0 2 4 6 8
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
42
44
46
BCR-ABL negative controlBCR-ABL positive controlPatient specimen
Fluo
resc
ence
-d(F1
)dT
Figure 2 BCR-ABL1 qualitative RT-PCR amplification curvesLightcycler amplification curves showing the cycle number of thecrossing point (CP) the point where the reactionrsquos fluorescencereaches the maximum of the second derivative of the amplificationcurve corresponding to the point where the acceleration of thefluorescence signal is at its maximum The CP is 29 cycles for thepositive control (purple) 35 cycles for the patientrsquos peripheral bloodspecimen (grey) and no amplification for the negative control (noDNA) (green) Thus the BCR-ABL1 fusion transcript was detectedfrom the patientrsquos peripheral blood
e1a2 which covers more than 95 of the described t(922)translocations [5] The HybProbe chemistry in the RocheLightCycler BCR-ABL1 t(922) kit was used This probe for-mat uses two labeled oligonucleotides one with a fluorescentdye at the 31015840 terminus and the other with a different dyeat the 51015840 end The probes are designed to hybridize to theBCR-ABL1 target strand such that both dyes are in closeproximity Therefore one dye acts as donor fluorophorewhereas the other (acceptor) emits light if it is positionednear the donor dye By using this probe chemistry in theLightCycler the acceptor fluorescence emission is measuredduring the annealing step when both probes hybridize to theBCR-ABL1 target strand
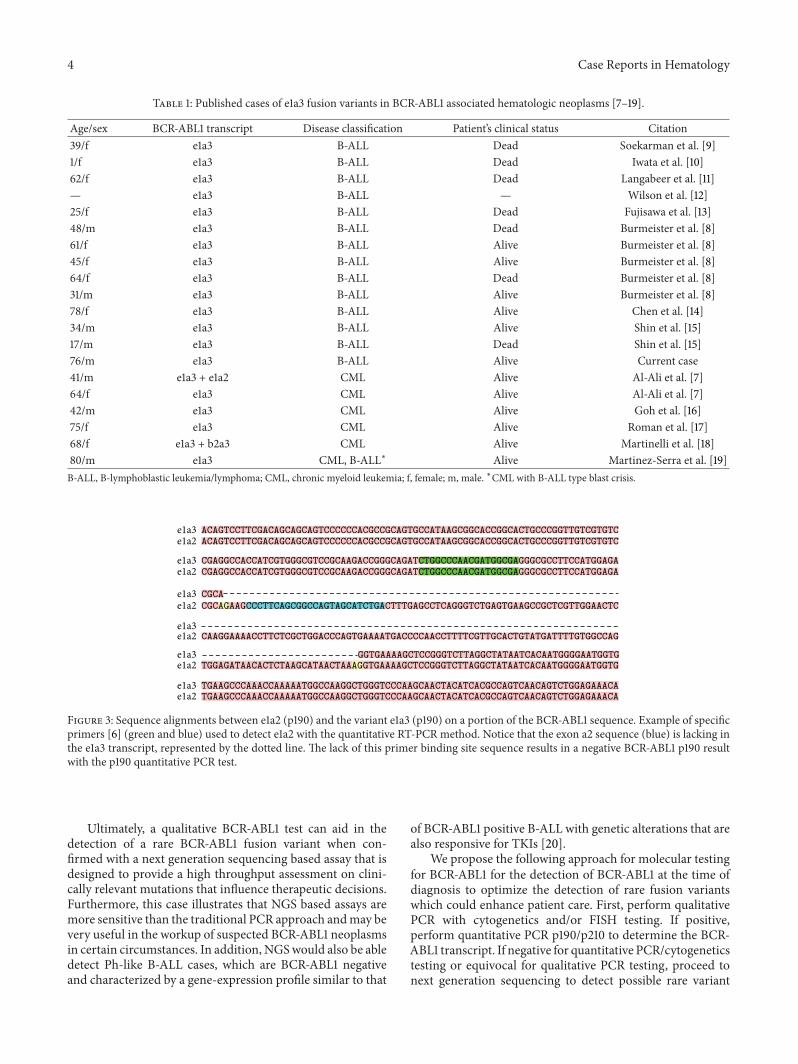
The quantitative BCR-ABL1 fusion tests were performedat ARUP Laboratories (Salt Lake City UT) utilizing reverse-transcriptase-quantitative PCR (RT-qPCR) for the detectionof BCR-ABL1 transcripts e1a2 (or p190) and e13a2 ande14a2 (or p210) Total RNA is isolated and converted tocDNA Fusion transcripts are quantitated by real time PCRamplification The primers are designed to detect the major(p210) BCR-ABL1 breakpoint including fusions between BCRexon 13 and ABL1 exon 2 (e13a2) and BCR exon 14 andABL1 exon 2 (e14a2) and the minor (p190) BCR-ABL1breakpoint with a fusion between BCR exon 1 and ABL1 exon2 (e1a2) (Figure 3) The targeted portions of the BCR-ABL1variant sequences of interest were retrieved from the NCBI(National Center for Biotechology Information) database andwere aligned using the sequence alignment tool T-COFFEEversion 1100 An example of the primer sequences that aredepicted in Figure 3 was obtained from literature [6]
FoundationOne Heme Assay (Foundation MedicineCambridge MA) uses hybridization capture applied to ge50
nanograms of extracted DNA or RNA for 405 cancer relatedgenes and select intronic regions from 31 genes (Founda-tionOne Heme DNA only 119899 = 405) targeted RNA-seq forrearrangement analysis was performed for 265 genes thatare frequently rearranged in cancer Sequencing of capturedlibraries was performed using an Illumina HiSeq 2500 toa median exon coverage depth of gt250x and resultantsequences were analyzed for base substitutions insertionsdeletions copy number alterations (focal amplifications andhomozygous deletions) and select gene fusions as previ-ously described To maximize mutation-detection accuracy(sensitivity and specificity) in impure clinical specimens thetest was previously optimized and validated to detect basesubstitutions at a ge5 mutant allele frequency (MAF) andindels with a ge10 MAF with ge99 accuracy [3]
4 Discussion
We report a 76-year-old male with a recent diagnosis ofB-ALL with the rare fusion variant e1a3 of p190BCR-ABLconfirmed by next generation sequencing The e1a3BCR-ABL1p190 variant fusion transcript lacks the ABL1exon a2 and results in a protein that lacks the N-terminaltwo-thirds of the Src homology 3 (SHE3) domain Thedomain is required for full leukemogenic potential in vivoand its absence has been proposed to be associated with amore benign clinical course [7 8] According to a literaturereview the e1a3 variant has only been reported in a few casesof B-ALL and CML (Table 1) [7ndash19] Fujisawa et al haverecognized a poor prognosis in all B-ALL cases as well asthose in CML blast phase however the clinical significanceor phenotype of this variant has yet to be determined[13] Verma et al have suggested that CML patients withBCR-ABL1p190 need to be identified as high-risk patientsand monitored closely for efficacy during TKI therapy [2]Overall the clinical significance in the detection of thisor any other variant of BCR-ABL1 is that a positive resultwill ultimately lead to a different course of managementfollow-up and treatment
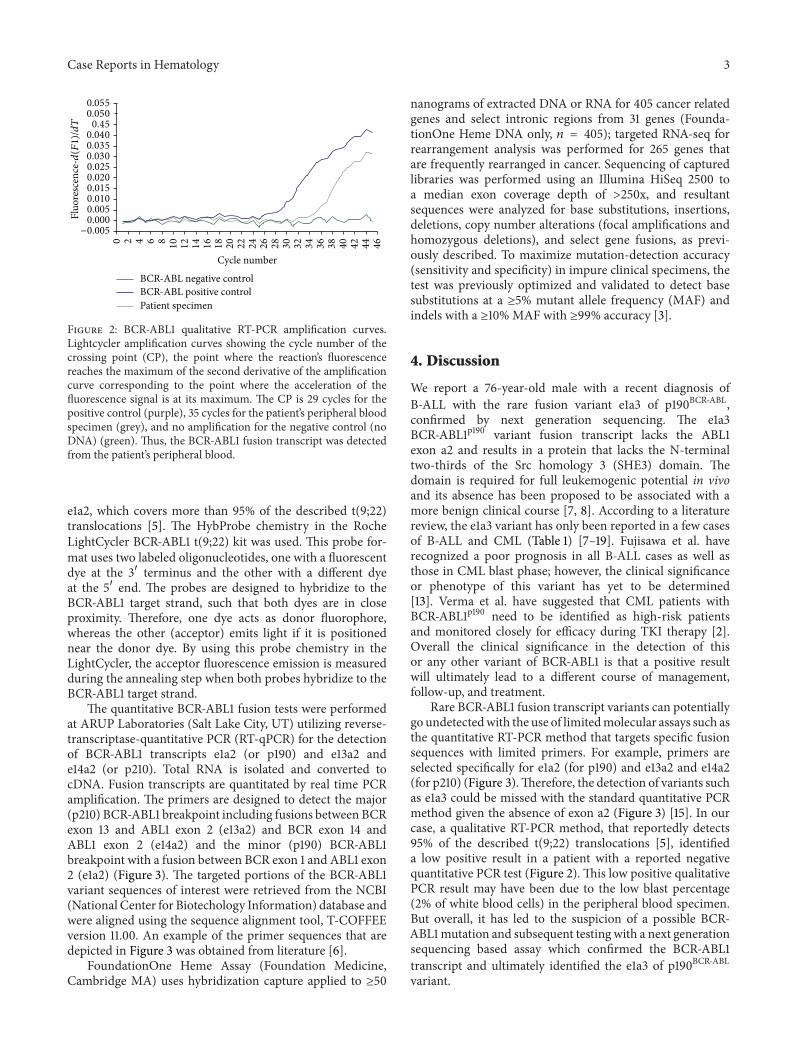
Rare BCR-ABL1 fusion transcript variants can potentiallygo undetectedwith the use of limitedmolecular assays such asthe quantitative RT-PCR method that targets specific fusionsequences with limited primers For example primers areselected specifically for e1a2 (for p190) and e13a2 and e14a2(for p210) (Figure 3)Therefore the detection of variants suchas e1a3 could be missed with the standard quantitative PCRmethod given the absence of exon a2 (Figure 3) [15] In ourcase a qualitative RT-PCR method that reportedly detects95 of the described t(922) translocations [5] identifieda low positive result in a patient with a reported negativequantitative PCR test (Figure 2) This low positive qualitativePCR result may have been due to the low blast percentage(2 of white blood cells) in the peripheral blood specimenBut overall it has led to the suspicion of a possible BCR-ABL1mutation and subsequent testing with a next generationsequencing based assay which confirmed the BCR-ABL1transcript and ultimately identified the e1a3 of p190BCR-ABLvariant
4 Case Reports in Hematology
Table 1 Published cases of e1a3 fusion variants in BCR-ABL1 associated hematologic neoplasms [7ndash19]
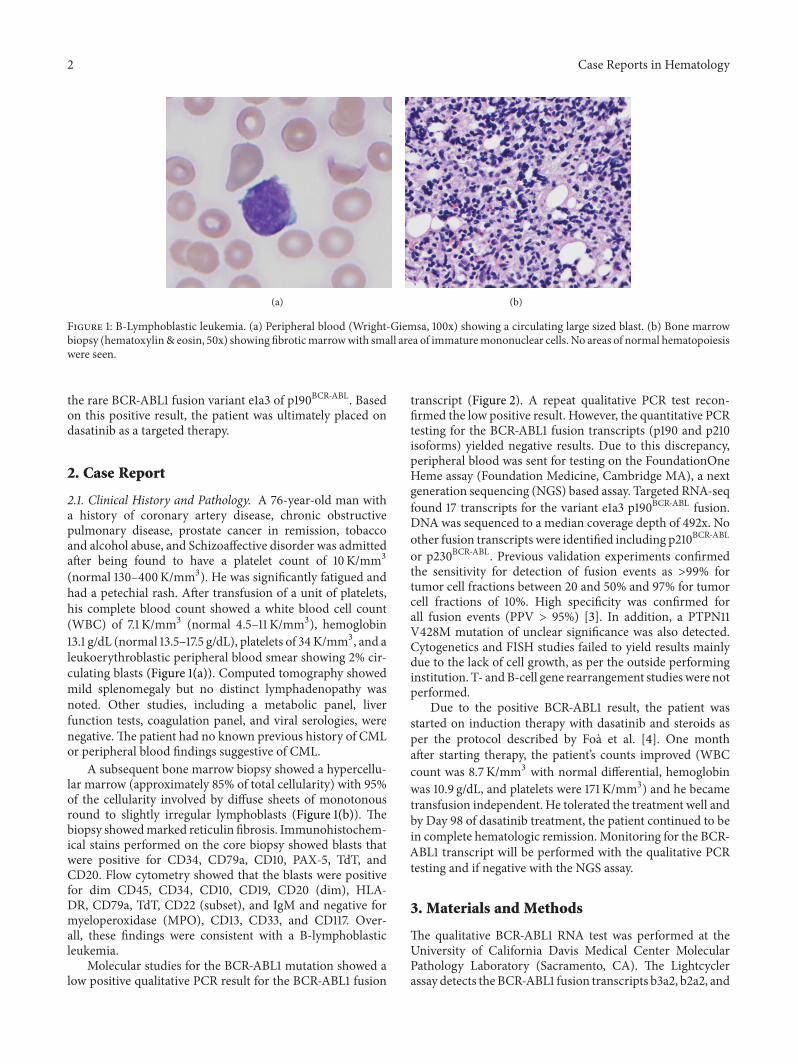
Agesex BCR-ABL1 transcript Disease classification Patientrsquos clinical status Citation39f e1a3 B-ALL Dead Soekarman et al [9]1f e1a3 B-ALL Dead Iwata et al [10]62f e1a3 B-ALL Dead Langabeer et al [11]mdash e1a3 B-ALL mdash Wilson et al [12]25f e1a3 B-ALL Dead Fujisawa et al [13]48m e1a3 B-ALL Dead Burmeister et al [8]61f e1a3 B-ALL Alive Burmeister et al [8]45f e1a3 B-ALL Alive Burmeister et al [8]64f e1a3 B-ALL Dead Burmeister et al [8]31m e1a3 B-ALL Alive Burmeister et al [8]78f e1a3 B-ALL Alive Chen et al [14]34m e1a3 B-ALL Alive Shin et al [15]17m e1a3 B-ALL Dead Shin et al [15]76m e1a3 B-ALL Alive Current case41m e1a3 + e1a2 CML Alive Al-Ali et al [7]64f e1a3 CML Alive Al-Ali et al [7]42m e1a3 CML Alive Goh et al [16]75f e1a3 CML Alive Roman et al [17]68f e1a3 + b2a3 CML Alive Martinelli et al [18]80m e1a3 CML B-ALLlowast Alive Martinez-Serra et al [19]B-ALL B-lymphoblastic leukemialymphoma CML chronic myeloid leukemia f female m male lowastCML with B-ALL type blast crisis
e1a3 ACAGTCCTTCGACAGCAGCAGTCCCCCCACGCCGCAGTGCCATAAGCGGCACCGGCACTGCCCGGTTGTCGTGTCe1a2 ACAGTCCTTCGACAGCAGCAGTCCCCCCACGCCGCAGTGCCATAAGCGGCACCGGCACTGCCCGGTTGTCGTGTC
e1a3 CGAGGCCACCATCGTGGGCGTCCGCAAGACCGGGCAGATCTGGCCCAACGATGGCGAGGGCGCCTTCCATGGAGAe1a2 CGAGGCCACCATCGTGGGCGTCCGCAAGACCGGGCAGATCTGGCCCAACGATGGCGAGGGCGCCTTCCATGGAGA
e1a3 CGCAe1a2 CGCAGAAGCCCTTCAGCGGCCAGTAGCATCTGACTTTGAGCCTCAGGGTCTGAGTGAAGCCGCTCGTTGGAACTC
e1a3e1a2 CAAGGAAAACCTTCTCGCTGGACCCAGTGAAAATGACCCCAACCTTTTCGTTGCACTGTATGATTTTGTGGCCAG
e1a3 GGTGAAAAGCTCCGGGTCTTAGGCTATAATCACAATGGGGAATGGTGe1a2 TGGAGATAACACTCTAAGCATAACTAAAGGTGAAAAGCTCCGGGTCTTAGGCTATAATCACAATGGGGAATGGTG
e1a3 TGAAGCCCAAACCAAAAATGGCCAAGGCTGGGTCCCAAGCAACTACATCACGCCAGTCAACAGTCTGGAGAAACAe1a2 TGAAGCCCAAACCAAAAATGGCCAAGGCTGGGTCCCAAGCAACTACATCACGCCAGTCAACAGTCTGGAGAAACA
Figure 3 Sequence alignments between e1a2 (p190) and the variant e1a3 (p190) on a portion of the BCR-ABL1 sequence Example of specificprimers [6] (green and blue) used to detect e1a2 with the quantitative RT-PCR method Notice that the exon a2 sequence (blue) is lacking inthe e1a3 transcript represented by the dotted line The lack of this primer binding site sequence results in a negative BCR-ABL1 p190 resultwith the p190 quantitative PCR test
Ultimately a qualitative BCR-ABL1 test can aid in thedetection of a rare BCR-ABL1 fusion variant when con-firmed with a next generation sequencing based assay that isdesigned to provide a high throughput assessment on clini-cally relevant mutations that influence therapeutic decisionsFurthermore this case illustrates that NGS based assays aremore sensitive than the traditional PCR approach andmay bevery useful in the workup of suspected BCR-ABL1 neoplasmsin certain circumstances In addition NGSwould also be abledetect Ph-like B-ALL cases which are BCR-ABL1 negativeand characterized by a gene-expression profile similar to that
of BCR-ABL1 positive B-ALL with genetic alterations that arealso responsive for TKIs [20]
We propose the following approach for molecular testingfor BCR-ABL1 for the detection of BCR-ABL1 at the time ofdiagnosis to optimize the detection of rare fusion variantswhich could enhance patient care First perform qualitativePCR with cytogenetics andor FISH testing If positiveperform quantitative PCR p190p210 to determine the BCR-ABL1 transcript If negative for quantitative PCRcytogeneticstesting or equivocal for qualitative PCR testing proceed tonext generation sequencing to detect possible rare variant
Case Reports in Hematology 5
transcripts andor Ph-like ALL disease This will allow thecapture of all clinically significant molecular mutations thatcould potentially guide therapy and management
One limitation in detecting rare variant transcripts solelyvia NGS is the inability to use standard PCR in some casesfor residual disease monitoring and follow-up ThereforeNGSmay be the only alternative for determining the presenceor absence of residual disease
5 Conclusion
In the era of molecular diagnostic medicine and a repertoireof potential targeted therapy options it is essential to have athorough understanding of the limitations of the individualmolecular assays and to follow a sound yet comprehensivediagnostic approach that would not only detect the commonabnormalities but rather be able to find the rare variants aswell Incorporating next generation sequencingmethods intoour current standard diagnostic PCR approach for BCR-ABL1andBCR-ABL1 negative Ph-like B-ALLwill aid inminimizingfalse negative results and may ultimately enhance patientcare In addition with the higher specificity of testing atthe sequencing level the rare e1a3 variant of BCR-ABL1p190may not actually be as infrequent as previously thought Theactual clinical significance of these rare variants is not yetfully understood and their role in clinical management withtargeted therapy needs to be further elucidated with the aid ofdetecting variants andmolecular profiles by newer molecularmethods such as next generation sequencing
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
This study was supported by Foundation Medicine Cam-bridge MA USA
References
[1] S H Swerdlow E Campo N L Harris et al World HealthOrganization Classification of Tumours of Haematopoietic andLymphoid Tissues International Agency for Research onCancer(IARC) Lyon France 4th edition 2008
[2] D Verma H M Kantarjian D Jones et al ldquoChronic myeloidleukemia (CML) with P190119861119862119877minus119860119861119871 analysis of characteristicsoutcomes and prognostic significancerdquo Blood vol 114 no 11pp 2232ndash2235 2009
[3] J He D Lipson M Nahas et al ldquoDevelopment and analyticalvalidation of a clinical next generation sequencing-based assayfor hematolymphoidmalignanciesrdquo inProceedings of the Ameri-can Association for Cancer Research Annual Meeting San DiegoCalif USA April 2014
[4] R Foa A Vitale M Vignetti et al ldquoDasatinib as first-linetreatment for adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemiardquo Blood vol 118 no 25pp 6521ndash6528 2011
[5] LightCycler t(922) Quantification Kit Instruction Manual Ver-sion 5 Roche 2013
[6] J Gabert E Beillard V H J van der Velden et al ldquoStandardiza-tion and quality control studies of lsquoreal timersquo quantitative reversetranscriptase polymerase chain reaction of fusion gene tran-scripts for residual disease detection in leukemiamdashA EuropeAgainst Cancer Programrdquo Leukemia vol 17 no 12 pp 2318ndash2357 2003
[7] H-K Al-Ali S Leiblein I Kovacs E Hennig D Niederwieserand M W N Deininger ldquoCML with an e1a3 BCR-ABL fusionrare benign and a potential diagnostic pitfallrdquo Blood vol 100no 3 pp 1092ndash1093 2002
[8] T Burmeister S Schwartz A Taubald et al ldquoAtypical BCR-ABLmRNA transcripts in adult acute lymphoblastic leukemiardquoHaematologica vol 92 no 12 pp 1699ndash1702 2007
[9] D Soekarman J van Denderen L Hoefsloot et al ldquoAnovel variant of the bcr-abl fusion product in Philadel-phia chromosome-positive acute lymphoblastic leukemiardquoLeukemia vol 4 no 6 pp 397ndash403 1990
[10] S Iwata SMizutani S Nakazawa and J-I Yata ldquoHeterogeneityof the breakpoint in the ABL gene in cases with BCRABLtranscript lacking ABL exon a2rdquo Leukemia vol 8 no 10 pp1696ndash1702 1994
[11] S E Langabeer K Haslam J Kelly M Leahy and E Van-denberghe ldquoAcute lymphoblastic leukaemia with an e1a3 BCR-ABL1 fusionrdquo Acta Haematologica vol 126 no 4 pp 214ndash2152011
[12] G A Wilson E A Vandenberghe R C Pollitt et al ldquoAreaberrant BCR-ABL transcripts more common than previouslythoughtrdquo British Journal of Haematology vol 111 no 4 pp1109ndash1111 2000
[13] S Fujisawa S Nakamura K Naito M Kobayashi and KOhnishi ldquoA variant transcript e1a3 of the minor BCR-ABLfusion gene in acute lymphoblastic leukemia case report andreview of the literaturerdquo International Journal of Hematologyvol 87 no 2 pp 184ndash188 2008
[14] Y Chen H W Wang X H Chen et al ldquoAdult acute lym-phoblastic leukemia with atypical BCR-ABL transcript e1a3 acase report and literature reviewrdquo Zhonghua Xue Ye Xue Za Zhivol 34 no 11 pp 965ndash966 2013
[15] S Y Shin J H Cho H J Kim J Jang S Lee and S Kim ldquoTwocases of acute lymphoblastic leukemia with an e1a3 BCR-ABL1fusion transcript rdquo Annals of Laboratory Medicine vol 35 no 1pp 159ndash161 2015
[16] H-G Goh J-Y Hwang S-H Kim Y-H Lee Y-L Kim andD-W Kim ldquoComprehensive analysis of BCR-ABL transcripttypes in Korean CML patients using a newly developed mul-tiplex RT-PCRrdquo Translational Research vol 148 no 5 pp 249ndash256 2006
[17] J Roman A Jimenez M Barrios J A Castillejo J Maldonadoand A Torres ldquoE1A3 as a unique naturally occurring BCR-ABLtranscript in an indolent case of chronic myeloid leukaemiardquoBritish Journal of Haematology vol 114 no 3 pp 635ndash637 2001
[18] G Martinelli M Amabile C Terragna et al ldquoConcomitantexpression of the rare E1A3 and B2A3 types of BCRABLtranscript in a chronic myeloid leukemia (CML) patientrdquoLeukemia vol 13 no 9 pp 1463ndash1464 1999
6 Case Reports in Hematology
[19] J Martinez-Serra R del Campo A Gutierrez et al ldquoChronicmyeloid leukemia with an e1a3 BCR-ABL fusion protein trans-formation to lymphoid blast crisisrdquo Biomarker Research vol 2no 14 pp 1ndash4 2014
[20] K G Roberts D Ki R C Payne-Turner et al ldquoTar-getable kinase-activating lesions in Ph-like acute lymphoblasticleukemiardquo The New England Journal of Medicine vol 371 pp1005ndash1015 2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
2 Case Reports in Hematology
(a) (b)
Figure 1 B-Lymphoblastic leukemia (a) Peripheral blood (Wright-Giemsa 100x) showing a circulating large sized blast (b) Bone marrowbiopsy (hematoxylinamp eosin 50x) showing fibroticmarrowwith small area of immaturemononuclear cells No areas of normal hematopoiesiswere seen
the rare BCR-ABL1 fusion variant e1a3 of p190BCR-ABL Basedon this positive result the patient was ultimately placed ondasatinib as a targeted therapy
2 Case Report
21 Clinical History and Pathology A 76-year-old man witha history of coronary artery disease chronic obstructivepulmonary disease prostate cancer in remission tobaccoand alcohol abuse and Schizoaffective disorder was admittedafter being found to have a platelet count of 10 Kmm3(normal 130ndash400Kmm3) He was significantly fatigued andhad a petechial rash After transfusion of a unit of plateletshis complete blood count showed a white blood cell count(WBC) of 71 Kmm3 (normal 45ndash11 Kmm3) hemoglobin131 gdL (normal 135ndash175 gdL) platelets of 34Kmm3 and aleukoerythroblastic peripheral blood smear showing 2 cir-culating blasts (Figure 1(a)) Computed tomography showedmild splenomegaly but no distinct lymphadenopathy wasnoted Other studies including a metabolic panel liverfunction tests coagulation panel and viral serologies werenegativeThe patient had no known previous history of CMLor peripheral blood findings suggestive of CML
A subsequent bone marrow biopsy showed a hypercellu-lar marrow (approximately 85 of total cellularity) with 95of the cellularity involved by diffuse sheets of monotonousround to slightly irregular lymphoblasts (Figure 1(b)) Thebiopsy showedmarked reticulin fibrosis Immunohistochem-ical stains performed on the core biopsy showed blasts thatwere positive for CD34 CD79a CD10 PAX-5 TdT andCD20 Flow cytometry showed that the blasts were positivefor dim CD45 CD34 CD10 CD19 CD20 (dim) HLA-DR CD79a TdT CD22 (subset) and IgM and negative formyeloperoxidase (MPO) CD13 CD33 and CD117 Over-all these findings were consistent with a B-lymphoblasticleukemia
Molecular studies for the BCR-ABL1 mutation showed alow positive qualitative PCR result for the BCR-ABL1 fusion
transcript (Figure 2) A repeat qualitative PCR test recon-firmed the low positive result However the quantitative PCRtesting for the BCR-ABL1 fusion transcripts (p190 and p210isoforms) yielded negative results Due to this discrepancyperipheral blood was sent for testing on the FoundationOneHeme assay (Foundation Medicine Cambridge MA) a nextgeneration sequencing (NGS) based assay Targeted RNA-seqfound 17 transcripts for the variant e1a3 p190BCR-ABL fusionDNA was sequenced to a median coverage depth of 492x Noother fusion transcripts were identified including p210BCR-ABL
or p230BCR-ABL Previous validation experiments confirmedthe sensitivity for detection of fusion events as gt99 fortumor cell fractions between 20 and 50 and 97 for tumorcell fractions of 10 High specificity was confirmed forall fusion events (PPV gt 95) [3] In addition a PTPN11V428M mutation of unclear significance was also detectedCytogenetics and FISH studies failed to yield results mainlydue to the lack of cell growth as per the outside performinginstitution T- andB-cell gene rearrangement studieswere notperformed
Due to the positive BCR-ABL1 result the patient wasstarted on induction therapy with dasatinib and steroids asper the protocol described by Foa et al [4] One monthafter starting therapy the patientrsquos counts improved (WBCcount was 87 Kmm3 with normal differential hemoglobinwas 109 gdL and platelets were 171 Kmm3) and he becametransfusion independent He tolerated the treatment well andby Day 98 of dasatinib treatment the patient continued to bein complete hematologic remission Monitoring for the BCR-ABL1 transcript will be performed with the qualitative PCRtesting and if negative with the NGS assay
3 Materials and Methods
The qualitative BCR-ABL1 RNA test was performed at theUniversity of California Davis Medical Center MolecularPathology Laboratory (Sacramento CA) The Lightcyclerassay detects theBCR-ABL1 fusion transcripts b3a2 b2a2 and
Case Reports in Hematology 3
Cycle number
0055
0050
045
0040
0035
0030
0025
0020
0015
0010
0005
0000
minus0005
0 2 4 6 8
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
42
44
46
BCR-ABL negative controlBCR-ABL positive controlPatient specimen
Fluo
resc
ence
-d(F1
)dT
Figure 2 BCR-ABL1 qualitative RT-PCR amplification curvesLightcycler amplification curves showing the cycle number of thecrossing point (CP) the point where the reactionrsquos fluorescencereaches the maximum of the second derivative of the amplificationcurve corresponding to the point where the acceleration of thefluorescence signal is at its maximum The CP is 29 cycles for thepositive control (purple) 35 cycles for the patientrsquos peripheral bloodspecimen (grey) and no amplification for the negative control (noDNA) (green) Thus the BCR-ABL1 fusion transcript was detectedfrom the patientrsquos peripheral blood
e1a2 which covers more than 95 of the described t(922)translocations [5] The HybProbe chemistry in the RocheLightCycler BCR-ABL1 t(922) kit was used This probe for-mat uses two labeled oligonucleotides one with a fluorescentdye at the 31015840 terminus and the other with a different dyeat the 51015840 end The probes are designed to hybridize to theBCR-ABL1 target strand such that both dyes are in closeproximity Therefore one dye acts as donor fluorophorewhereas the other (acceptor) emits light if it is positionednear the donor dye By using this probe chemistry in theLightCycler the acceptor fluorescence emission is measuredduring the annealing step when both probes hybridize to theBCR-ABL1 target strand
The quantitative BCR-ABL1 fusion tests were performedat ARUP Laboratories (Salt Lake City UT) utilizing reverse-transcriptase-quantitative PCR (RT-qPCR) for the detectionof BCR-ABL1 transcripts e1a2 (or p190) and e13a2 ande14a2 (or p210) Total RNA is isolated and converted tocDNA Fusion transcripts are quantitated by real time PCRamplification The primers are designed to detect the major(p210) BCR-ABL1 breakpoint including fusions between BCRexon 13 and ABL1 exon 2 (e13a2) and BCR exon 14 andABL1 exon 2 (e14a2) and the minor (p190) BCR-ABL1breakpoint with a fusion between BCR exon 1 and ABL1 exon2 (e1a2) (Figure 3) The targeted portions of the BCR-ABL1variant sequences of interest were retrieved from the NCBI(National Center for Biotechology Information) database andwere aligned using the sequence alignment tool T-COFFEEversion 1100 An example of the primer sequences that aredepicted in Figure 3 was obtained from literature [6]
FoundationOne Heme Assay (Foundation MedicineCambridge MA) uses hybridization capture applied to ge50
nanograms of extracted DNA or RNA for 405 cancer relatedgenes and select intronic regions from 31 genes (Founda-tionOne Heme DNA only 119899 = 405) targeted RNA-seq forrearrangement analysis was performed for 265 genes thatare frequently rearranged in cancer Sequencing of capturedlibraries was performed using an Illumina HiSeq 2500 toa median exon coverage depth of gt250x and resultantsequences were analyzed for base substitutions insertionsdeletions copy number alterations (focal amplifications andhomozygous deletions) and select gene fusions as previ-ously described To maximize mutation-detection accuracy(sensitivity and specificity) in impure clinical specimens thetest was previously optimized and validated to detect basesubstitutions at a ge5 mutant allele frequency (MAF) andindels with a ge10 MAF with ge99 accuracy [3]
4 Discussion
We report a 76-year-old male with a recent diagnosis ofB-ALL with the rare fusion variant e1a3 of p190BCR-ABLconfirmed by next generation sequencing The e1a3BCR-ABL1p190 variant fusion transcript lacks the ABL1exon a2 and results in a protein that lacks the N-terminaltwo-thirds of the Src homology 3 (SHE3) domain Thedomain is required for full leukemogenic potential in vivoand its absence has been proposed to be associated with amore benign clinical course [7 8] According to a literaturereview the e1a3 variant has only been reported in a few casesof B-ALL and CML (Table 1) [7ndash19] Fujisawa et al haverecognized a poor prognosis in all B-ALL cases as well asthose in CML blast phase however the clinical significanceor phenotype of this variant has yet to be determined[13] Verma et al have suggested that CML patients withBCR-ABL1p190 need to be identified as high-risk patientsand monitored closely for efficacy during TKI therapy [2]Overall the clinical significance in the detection of thisor any other variant of BCR-ABL1 is that a positive resultwill ultimately lead to a different course of managementfollow-up and treatment
Rare BCR-ABL1 fusion transcript variants can potentiallygo undetectedwith the use of limitedmolecular assays such asthe quantitative RT-PCR method that targets specific fusionsequences with limited primers For example primers areselected specifically for e1a2 (for p190) and e13a2 and e14a2(for p210) (Figure 3)Therefore the detection of variants suchas e1a3 could be missed with the standard quantitative PCRmethod given the absence of exon a2 (Figure 3) [15] In ourcase a qualitative RT-PCR method that reportedly detects95 of the described t(922) translocations [5] identifieda low positive result in a patient with a reported negativequantitative PCR test (Figure 2) This low positive qualitativePCR result may have been due to the low blast percentage(2 of white blood cells) in the peripheral blood specimenBut overall it has led to the suspicion of a possible BCR-ABL1mutation and subsequent testing with a next generationsequencing based assay which confirmed the BCR-ABL1transcript and ultimately identified the e1a3 of p190BCR-ABLvariant
4 Case Reports in Hematology
Table 1 Published cases of e1a3 fusion variants in BCR-ABL1 associated hematologic neoplasms [7ndash19]
Agesex BCR-ABL1 transcript Disease classification Patientrsquos clinical status Citation39f e1a3 B-ALL Dead Soekarman et al [9]1f e1a3 B-ALL Dead Iwata et al [10]62f e1a3 B-ALL Dead Langabeer et al [11]mdash e1a3 B-ALL mdash Wilson et al [12]25f e1a3 B-ALL Dead Fujisawa et al [13]48m e1a3 B-ALL Dead Burmeister et al [8]61f e1a3 B-ALL Alive Burmeister et al [8]45f e1a3 B-ALL Alive Burmeister et al [8]64f e1a3 B-ALL Dead Burmeister et al [8]31m e1a3 B-ALL Alive Burmeister et al [8]78f e1a3 B-ALL Alive Chen et al [14]34m e1a3 B-ALL Alive Shin et al [15]17m e1a3 B-ALL Dead Shin et al [15]76m e1a3 B-ALL Alive Current case41m e1a3 + e1a2 CML Alive Al-Ali et al [7]64f e1a3 CML Alive Al-Ali et al [7]42m e1a3 CML Alive Goh et al [16]75f e1a3 CML Alive Roman et al [17]68f e1a3 + b2a3 CML Alive Martinelli et al [18]80m e1a3 CML B-ALLlowast Alive Martinez-Serra et al [19]B-ALL B-lymphoblastic leukemialymphoma CML chronic myeloid leukemia f female m male lowastCML with B-ALL type blast crisis
e1a3 ACAGTCCTTCGACAGCAGCAGTCCCCCCACGCCGCAGTGCCATAAGCGGCACCGGCACTGCCCGGTTGTCGTGTCe1a2 ACAGTCCTTCGACAGCAGCAGTCCCCCCACGCCGCAGTGCCATAAGCGGCACCGGCACTGCCCGGTTGTCGTGTC
e1a3 CGAGGCCACCATCGTGGGCGTCCGCAAGACCGGGCAGATCTGGCCCAACGATGGCGAGGGCGCCTTCCATGGAGAe1a2 CGAGGCCACCATCGTGGGCGTCCGCAAGACCGGGCAGATCTGGCCCAACGATGGCGAGGGCGCCTTCCATGGAGA
e1a3 CGCAe1a2 CGCAGAAGCCCTTCAGCGGCCAGTAGCATCTGACTTTGAGCCTCAGGGTCTGAGTGAAGCCGCTCGTTGGAACTC
e1a3e1a2 CAAGGAAAACCTTCTCGCTGGACCCAGTGAAAATGACCCCAACCTTTTCGTTGCACTGTATGATTTTGTGGCCAG
e1a3 GGTGAAAAGCTCCGGGTCTTAGGCTATAATCACAATGGGGAATGGTGe1a2 TGGAGATAACACTCTAAGCATAACTAAAGGTGAAAAGCTCCGGGTCTTAGGCTATAATCACAATGGGGAATGGTG
e1a3 TGAAGCCCAAACCAAAAATGGCCAAGGCTGGGTCCCAAGCAACTACATCACGCCAGTCAACAGTCTGGAGAAACAe1a2 TGAAGCCCAAACCAAAAATGGCCAAGGCTGGGTCCCAAGCAACTACATCACGCCAGTCAACAGTCTGGAGAAACA
Figure 3 Sequence alignments between e1a2 (p190) and the variant e1a3 (p190) on a portion of the BCR-ABL1 sequence Example of specificprimers [6] (green and blue) used to detect e1a2 with the quantitative RT-PCR method Notice that the exon a2 sequence (blue) is lacking inthe e1a3 transcript represented by the dotted line The lack of this primer binding site sequence results in a negative BCR-ABL1 p190 resultwith the p190 quantitative PCR test
Ultimately a qualitative BCR-ABL1 test can aid in thedetection of a rare BCR-ABL1 fusion variant when con-firmed with a next generation sequencing based assay that isdesigned to provide a high throughput assessment on clini-cally relevant mutations that influence therapeutic decisionsFurthermore this case illustrates that NGS based assays aremore sensitive than the traditional PCR approach andmay bevery useful in the workup of suspected BCR-ABL1 neoplasmsin certain circumstances In addition NGSwould also be abledetect Ph-like B-ALL cases which are BCR-ABL1 negativeand characterized by a gene-expression profile similar to that
of BCR-ABL1 positive B-ALL with genetic alterations that arealso responsive for TKIs [20]
We propose the following approach for molecular testingfor BCR-ABL1 for the detection of BCR-ABL1 at the time ofdiagnosis to optimize the detection of rare fusion variantswhich could enhance patient care First perform qualitativePCR with cytogenetics andor FISH testing If positiveperform quantitative PCR p190p210 to determine the BCR-ABL1 transcript If negative for quantitative PCRcytogeneticstesting or equivocal for qualitative PCR testing proceed tonext generation sequencing to detect possible rare variant
Case Reports in Hematology 5
transcripts andor Ph-like ALL disease This will allow thecapture of all clinically significant molecular mutations thatcould potentially guide therapy and management
One limitation in detecting rare variant transcripts solelyvia NGS is the inability to use standard PCR in some casesfor residual disease monitoring and follow-up ThereforeNGSmay be the only alternative for determining the presenceor absence of residual disease
5 Conclusion
In the era of molecular diagnostic medicine and a repertoireof potential targeted therapy options it is essential to have athorough understanding of the limitations of the individualmolecular assays and to follow a sound yet comprehensivediagnostic approach that would not only detect the commonabnormalities but rather be able to find the rare variants aswell Incorporating next generation sequencingmethods intoour current standard diagnostic PCR approach for BCR-ABL1andBCR-ABL1 negative Ph-like B-ALLwill aid inminimizingfalse negative results and may ultimately enhance patientcare In addition with the higher specificity of testing atthe sequencing level the rare e1a3 variant of BCR-ABL1p190may not actually be as infrequent as previously thought Theactual clinical significance of these rare variants is not yetfully understood and their role in clinical management withtargeted therapy needs to be further elucidated with the aid ofdetecting variants andmolecular profiles by newer molecularmethods such as next generation sequencing
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
This study was supported by Foundation Medicine Cam-bridge MA USA
References
[1] S H Swerdlow E Campo N L Harris et al World HealthOrganization Classification of Tumours of Haematopoietic andLymphoid Tissues International Agency for Research onCancer(IARC) Lyon France 4th edition 2008
[2] D Verma H M Kantarjian D Jones et al ldquoChronic myeloidleukemia (CML) with P190119861119862119877minus119860119861119871 analysis of characteristicsoutcomes and prognostic significancerdquo Blood vol 114 no 11pp 2232ndash2235 2009
[3] J He D Lipson M Nahas et al ldquoDevelopment and analyticalvalidation of a clinical next generation sequencing-based assayfor hematolymphoidmalignanciesrdquo inProceedings of the Ameri-can Association for Cancer Research Annual Meeting San DiegoCalif USA April 2014
[4] R Foa A Vitale M Vignetti et al ldquoDasatinib as first-linetreatment for adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemiardquo Blood vol 118 no 25pp 6521ndash6528 2011
[5] LightCycler t(922) Quantification Kit Instruction Manual Ver-sion 5 Roche 2013
[6] J Gabert E Beillard V H J van der Velden et al ldquoStandardiza-tion and quality control studies of lsquoreal timersquo quantitative reversetranscriptase polymerase chain reaction of fusion gene tran-scripts for residual disease detection in leukemiamdashA EuropeAgainst Cancer Programrdquo Leukemia vol 17 no 12 pp 2318ndash2357 2003
[7] H-K Al-Ali S Leiblein I Kovacs E Hennig D Niederwieserand M W N Deininger ldquoCML with an e1a3 BCR-ABL fusionrare benign and a potential diagnostic pitfallrdquo Blood vol 100no 3 pp 1092ndash1093 2002
[8] T Burmeister S Schwartz A Taubald et al ldquoAtypical BCR-ABLmRNA transcripts in adult acute lymphoblastic leukemiardquoHaematologica vol 92 no 12 pp 1699ndash1702 2007
[9] D Soekarman J van Denderen L Hoefsloot et al ldquoAnovel variant of the bcr-abl fusion product in Philadel-phia chromosome-positive acute lymphoblastic leukemiardquoLeukemia vol 4 no 6 pp 397ndash403 1990
[10] S Iwata SMizutani S Nakazawa and J-I Yata ldquoHeterogeneityof the breakpoint in the ABL gene in cases with BCRABLtranscript lacking ABL exon a2rdquo Leukemia vol 8 no 10 pp1696ndash1702 1994
[11] S E Langabeer K Haslam J Kelly M Leahy and E Van-denberghe ldquoAcute lymphoblastic leukaemia with an e1a3 BCR-ABL1 fusionrdquo Acta Haematologica vol 126 no 4 pp 214ndash2152011
[12] G A Wilson E A Vandenberghe R C Pollitt et al ldquoAreaberrant BCR-ABL transcripts more common than previouslythoughtrdquo British Journal of Haematology vol 111 no 4 pp1109ndash1111 2000
[13] S Fujisawa S Nakamura K Naito M Kobayashi and KOhnishi ldquoA variant transcript e1a3 of the minor BCR-ABLfusion gene in acute lymphoblastic leukemia case report andreview of the literaturerdquo International Journal of Hematologyvol 87 no 2 pp 184ndash188 2008
[14] Y Chen H W Wang X H Chen et al ldquoAdult acute lym-phoblastic leukemia with atypical BCR-ABL transcript e1a3 acase report and literature reviewrdquo Zhonghua Xue Ye Xue Za Zhivol 34 no 11 pp 965ndash966 2013
[15] S Y Shin J H Cho H J Kim J Jang S Lee and S Kim ldquoTwocases of acute lymphoblastic leukemia with an e1a3 BCR-ABL1fusion transcript rdquo Annals of Laboratory Medicine vol 35 no 1pp 159ndash161 2015
[16] H-G Goh J-Y Hwang S-H Kim Y-H Lee Y-L Kim andD-W Kim ldquoComprehensive analysis of BCR-ABL transcripttypes in Korean CML patients using a newly developed mul-tiplex RT-PCRrdquo Translational Research vol 148 no 5 pp 249ndash256 2006
[17] J Roman A Jimenez M Barrios J A Castillejo J Maldonadoand A Torres ldquoE1A3 as a unique naturally occurring BCR-ABLtranscript in an indolent case of chronic myeloid leukaemiardquoBritish Journal of Haematology vol 114 no 3 pp 635ndash637 2001
[18] G Martinelli M Amabile C Terragna et al ldquoConcomitantexpression of the rare E1A3 and B2A3 types of BCRABLtranscript in a chronic myeloid leukemia (CML) patientrdquoLeukemia vol 13 no 9 pp 1463ndash1464 1999
6 Case Reports in Hematology
[19] J Martinez-Serra R del Campo A Gutierrez et al ldquoChronicmyeloid leukemia with an e1a3 BCR-ABL fusion protein trans-formation to lymphoid blast crisisrdquo Biomarker Research vol 2no 14 pp 1ndash4 2014
[20] K G Roberts D Ki R C Payne-Turner et al ldquoTar-getable kinase-activating lesions in Ph-like acute lymphoblasticleukemiardquo The New England Journal of Medicine vol 371 pp1005ndash1015 2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Case Reports in Hematology 3
Cycle number
0055
0050
045
0040
0035
0030
0025
0020
0015
0010
0005
0000
minus0005
0 2 4 6 8
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
42
44
46
BCR-ABL negative controlBCR-ABL positive controlPatient specimen
Fluo
resc
ence
-d(F1
)dT
Figure 2 BCR-ABL1 qualitative RT-PCR amplification curvesLightcycler amplification curves showing the cycle number of thecrossing point (CP) the point where the reactionrsquos fluorescencereaches the maximum of the second derivative of the amplificationcurve corresponding to the point where the acceleration of thefluorescence signal is at its maximum The CP is 29 cycles for thepositive control (purple) 35 cycles for the patientrsquos peripheral bloodspecimen (grey) and no amplification for the negative control (noDNA) (green) Thus the BCR-ABL1 fusion transcript was detectedfrom the patientrsquos peripheral blood
e1a2 which covers more than 95 of the described t(922)translocations [5] The HybProbe chemistry in the RocheLightCycler BCR-ABL1 t(922) kit was used This probe for-mat uses two labeled oligonucleotides one with a fluorescentdye at the 31015840 terminus and the other with a different dyeat the 51015840 end The probes are designed to hybridize to theBCR-ABL1 target strand such that both dyes are in closeproximity Therefore one dye acts as donor fluorophorewhereas the other (acceptor) emits light if it is positionednear the donor dye By using this probe chemistry in theLightCycler the acceptor fluorescence emission is measuredduring the annealing step when both probes hybridize to theBCR-ABL1 target strand
The quantitative BCR-ABL1 fusion tests were performedat ARUP Laboratories (Salt Lake City UT) utilizing reverse-transcriptase-quantitative PCR (RT-qPCR) for the detectionof BCR-ABL1 transcripts e1a2 (or p190) and e13a2 ande14a2 (or p210) Total RNA is isolated and converted tocDNA Fusion transcripts are quantitated by real time PCRamplification The primers are designed to detect the major(p210) BCR-ABL1 breakpoint including fusions between BCRexon 13 and ABL1 exon 2 (e13a2) and BCR exon 14 andABL1 exon 2 (e14a2) and the minor (p190) BCR-ABL1breakpoint with a fusion between BCR exon 1 and ABL1 exon2 (e1a2) (Figure 3) The targeted portions of the BCR-ABL1variant sequences of interest were retrieved from the NCBI(National Center for Biotechology Information) database andwere aligned using the sequence alignment tool T-COFFEEversion 1100 An example of the primer sequences that aredepicted in Figure 3 was obtained from literature [6]
FoundationOne Heme Assay (Foundation MedicineCambridge MA) uses hybridization capture applied to ge50
nanograms of extracted DNA or RNA for 405 cancer relatedgenes and select intronic regions from 31 genes (Founda-tionOne Heme DNA only 119899 = 405) targeted RNA-seq forrearrangement analysis was performed for 265 genes thatare frequently rearranged in cancer Sequencing of capturedlibraries was performed using an Illumina HiSeq 2500 toa median exon coverage depth of gt250x and resultantsequences were analyzed for base substitutions insertionsdeletions copy number alterations (focal amplifications andhomozygous deletions) and select gene fusions as previ-ously described To maximize mutation-detection accuracy(sensitivity and specificity) in impure clinical specimens thetest was previously optimized and validated to detect basesubstitutions at a ge5 mutant allele frequency (MAF) andindels with a ge10 MAF with ge99 accuracy [3]
4 Discussion
We report a 76-year-old male with a recent diagnosis ofB-ALL with the rare fusion variant e1a3 of p190BCR-ABLconfirmed by next generation sequencing The e1a3BCR-ABL1p190 variant fusion transcript lacks the ABL1exon a2 and results in a protein that lacks the N-terminaltwo-thirds of the Src homology 3 (SHE3) domain Thedomain is required for full leukemogenic potential in vivoand its absence has been proposed to be associated with amore benign clinical course [7 8] According to a literaturereview the e1a3 variant has only been reported in a few casesof B-ALL and CML (Table 1) [7ndash19] Fujisawa et al haverecognized a poor prognosis in all B-ALL cases as well asthose in CML blast phase however the clinical significanceor phenotype of this variant has yet to be determined[13] Verma et al have suggested that CML patients withBCR-ABL1p190 need to be identified as high-risk patientsand monitored closely for efficacy during TKI therapy [2]Overall the clinical significance in the detection of thisor any other variant of BCR-ABL1 is that a positive resultwill ultimately lead to a different course of managementfollow-up and treatment
Rare BCR-ABL1 fusion transcript variants can potentiallygo undetectedwith the use of limitedmolecular assays such asthe quantitative RT-PCR method that targets specific fusionsequences with limited primers For example primers areselected specifically for e1a2 (for p190) and e13a2 and e14a2(for p210) (Figure 3)Therefore the detection of variants suchas e1a3 could be missed with the standard quantitative PCRmethod given the absence of exon a2 (Figure 3) [15] In ourcase a qualitative RT-PCR method that reportedly detects95 of the described t(922) translocations [5] identifieda low positive result in a patient with a reported negativequantitative PCR test (Figure 2) This low positive qualitativePCR result may have been due to the low blast percentage(2 of white blood cells) in the peripheral blood specimenBut overall it has led to the suspicion of a possible BCR-ABL1mutation and subsequent testing with a next generationsequencing based assay which confirmed the BCR-ABL1transcript and ultimately identified the e1a3 of p190BCR-ABLvariant
4 Case Reports in Hematology
Table 1 Published cases of e1a3 fusion variants in BCR-ABL1 associated hematologic neoplasms [7ndash19]
Agesex BCR-ABL1 transcript Disease classification Patientrsquos clinical status Citation39f e1a3 B-ALL Dead Soekarman et al [9]1f e1a3 B-ALL Dead Iwata et al [10]62f e1a3 B-ALL Dead Langabeer et al [11]mdash e1a3 B-ALL mdash Wilson et al [12]25f e1a3 B-ALL Dead Fujisawa et al [13]48m e1a3 B-ALL Dead Burmeister et al [8]61f e1a3 B-ALL Alive Burmeister et al [8]45f e1a3 B-ALL Alive Burmeister et al [8]64f e1a3 B-ALL Dead Burmeister et al [8]31m e1a3 B-ALL Alive Burmeister et al [8]78f e1a3 B-ALL Alive Chen et al [14]34m e1a3 B-ALL Alive Shin et al [15]17m e1a3 B-ALL Dead Shin et al [15]76m e1a3 B-ALL Alive Current case41m e1a3 + e1a2 CML Alive Al-Ali et al [7]64f e1a3 CML Alive Al-Ali et al [7]42m e1a3 CML Alive Goh et al [16]75f e1a3 CML Alive Roman et al [17]68f e1a3 + b2a3 CML Alive Martinelli et al [18]80m e1a3 CML B-ALLlowast Alive Martinez-Serra et al [19]B-ALL B-lymphoblastic leukemialymphoma CML chronic myeloid leukemia f female m male lowastCML with B-ALL type blast crisis
e1a3 ACAGTCCTTCGACAGCAGCAGTCCCCCCACGCCGCAGTGCCATAAGCGGCACCGGCACTGCCCGGTTGTCGTGTCe1a2 ACAGTCCTTCGACAGCAGCAGTCCCCCCACGCCGCAGTGCCATAAGCGGCACCGGCACTGCCCGGTTGTCGTGTC
e1a3 CGAGGCCACCATCGTGGGCGTCCGCAAGACCGGGCAGATCTGGCCCAACGATGGCGAGGGCGCCTTCCATGGAGAe1a2 CGAGGCCACCATCGTGGGCGTCCGCAAGACCGGGCAGATCTGGCCCAACGATGGCGAGGGCGCCTTCCATGGAGA
e1a3 CGCAe1a2 CGCAGAAGCCCTTCAGCGGCCAGTAGCATCTGACTTTGAGCCTCAGGGTCTGAGTGAAGCCGCTCGTTGGAACTC
e1a3e1a2 CAAGGAAAACCTTCTCGCTGGACCCAGTGAAAATGACCCCAACCTTTTCGTTGCACTGTATGATTTTGTGGCCAG
e1a3 GGTGAAAAGCTCCGGGTCTTAGGCTATAATCACAATGGGGAATGGTGe1a2 TGGAGATAACACTCTAAGCATAACTAAAGGTGAAAAGCTCCGGGTCTTAGGCTATAATCACAATGGGGAATGGTG
e1a3 TGAAGCCCAAACCAAAAATGGCCAAGGCTGGGTCCCAAGCAACTACATCACGCCAGTCAACAGTCTGGAGAAACAe1a2 TGAAGCCCAAACCAAAAATGGCCAAGGCTGGGTCCCAAGCAACTACATCACGCCAGTCAACAGTCTGGAGAAACA
Figure 3 Sequence alignments between e1a2 (p190) and the variant e1a3 (p190) on a portion of the BCR-ABL1 sequence Example of specificprimers [6] (green and blue) used to detect e1a2 with the quantitative RT-PCR method Notice that the exon a2 sequence (blue) is lacking inthe e1a3 transcript represented by the dotted line The lack of this primer binding site sequence results in a negative BCR-ABL1 p190 resultwith the p190 quantitative PCR test
Ultimately a qualitative BCR-ABL1 test can aid in thedetection of a rare BCR-ABL1 fusion variant when con-firmed with a next generation sequencing based assay that isdesigned to provide a high throughput assessment on clini-cally relevant mutations that influence therapeutic decisionsFurthermore this case illustrates that NGS based assays aremore sensitive than the traditional PCR approach andmay bevery useful in the workup of suspected BCR-ABL1 neoplasmsin certain circumstances In addition NGSwould also be abledetect Ph-like B-ALL cases which are BCR-ABL1 negativeand characterized by a gene-expression profile similar to that
of BCR-ABL1 positive B-ALL with genetic alterations that arealso responsive for TKIs [20]
We propose the following approach for molecular testingfor BCR-ABL1 for the detection of BCR-ABL1 at the time ofdiagnosis to optimize the detection of rare fusion variantswhich could enhance patient care First perform qualitativePCR with cytogenetics andor FISH testing If positiveperform quantitative PCR p190p210 to determine the BCR-ABL1 transcript If negative for quantitative PCRcytogeneticstesting or equivocal for qualitative PCR testing proceed tonext generation sequencing to detect possible rare variant
Case Reports in Hematology 5
transcripts andor Ph-like ALL disease This will allow thecapture of all clinically significant molecular mutations thatcould potentially guide therapy and management
One limitation in detecting rare variant transcripts solelyvia NGS is the inability to use standard PCR in some casesfor residual disease monitoring and follow-up ThereforeNGSmay be the only alternative for determining the presenceor absence of residual disease
5 Conclusion
In the era of molecular diagnostic medicine and a repertoireof potential targeted therapy options it is essential to have athorough understanding of the limitations of the individualmolecular assays and to follow a sound yet comprehensivediagnostic approach that would not only detect the commonabnormalities but rather be able to find the rare variants aswell Incorporating next generation sequencingmethods intoour current standard diagnostic PCR approach for BCR-ABL1andBCR-ABL1 negative Ph-like B-ALLwill aid inminimizingfalse negative results and may ultimately enhance patientcare In addition with the higher specificity of testing atthe sequencing level the rare e1a3 variant of BCR-ABL1p190may not actually be as infrequent as previously thought Theactual clinical significance of these rare variants is not yetfully understood and their role in clinical management withtargeted therapy needs to be further elucidated with the aid ofdetecting variants andmolecular profiles by newer molecularmethods such as next generation sequencing
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
This study was supported by Foundation Medicine Cam-bridge MA USA
References
[1] S H Swerdlow E Campo N L Harris et al World HealthOrganization Classification of Tumours of Haematopoietic andLymphoid Tissues International Agency for Research onCancer(IARC) Lyon France 4th edition 2008
[2] D Verma H M Kantarjian D Jones et al ldquoChronic myeloidleukemia (CML) with P190119861119862119877minus119860119861119871 analysis of characteristicsoutcomes and prognostic significancerdquo Blood vol 114 no 11pp 2232ndash2235 2009
[3] J He D Lipson M Nahas et al ldquoDevelopment and analyticalvalidation of a clinical next generation sequencing-based assayfor hematolymphoidmalignanciesrdquo inProceedings of the Ameri-can Association for Cancer Research Annual Meeting San DiegoCalif USA April 2014
[4] R Foa A Vitale M Vignetti et al ldquoDasatinib as first-linetreatment for adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemiardquo Blood vol 118 no 25pp 6521ndash6528 2011
[5] LightCycler t(922) Quantification Kit Instruction Manual Ver-sion 5 Roche 2013
[6] J Gabert E Beillard V H J van der Velden et al ldquoStandardiza-tion and quality control studies of lsquoreal timersquo quantitative reversetranscriptase polymerase chain reaction of fusion gene tran-scripts for residual disease detection in leukemiamdashA EuropeAgainst Cancer Programrdquo Leukemia vol 17 no 12 pp 2318ndash2357 2003
[7] H-K Al-Ali S Leiblein I Kovacs E Hennig D Niederwieserand M W N Deininger ldquoCML with an e1a3 BCR-ABL fusionrare benign and a potential diagnostic pitfallrdquo Blood vol 100no 3 pp 1092ndash1093 2002
[8] T Burmeister S Schwartz A Taubald et al ldquoAtypical BCR-ABLmRNA transcripts in adult acute lymphoblastic leukemiardquoHaematologica vol 92 no 12 pp 1699ndash1702 2007
[9] D Soekarman J van Denderen L Hoefsloot et al ldquoAnovel variant of the bcr-abl fusion product in Philadel-phia chromosome-positive acute lymphoblastic leukemiardquoLeukemia vol 4 no 6 pp 397ndash403 1990
[10] S Iwata SMizutani S Nakazawa and J-I Yata ldquoHeterogeneityof the breakpoint in the ABL gene in cases with BCRABLtranscript lacking ABL exon a2rdquo Leukemia vol 8 no 10 pp1696ndash1702 1994
[11] S E Langabeer K Haslam J Kelly M Leahy and E Van-denberghe ldquoAcute lymphoblastic leukaemia with an e1a3 BCR-ABL1 fusionrdquo Acta Haematologica vol 126 no 4 pp 214ndash2152011
[12] G A Wilson E A Vandenberghe R C Pollitt et al ldquoAreaberrant BCR-ABL transcripts more common than previouslythoughtrdquo British Journal of Haematology vol 111 no 4 pp1109ndash1111 2000
[13] S Fujisawa S Nakamura K Naito M Kobayashi and KOhnishi ldquoA variant transcript e1a3 of the minor BCR-ABLfusion gene in acute lymphoblastic leukemia case report andreview of the literaturerdquo International Journal of Hematologyvol 87 no 2 pp 184ndash188 2008
[14] Y Chen H W Wang X H Chen et al ldquoAdult acute lym-phoblastic leukemia with atypical BCR-ABL transcript e1a3 acase report and literature reviewrdquo Zhonghua Xue Ye Xue Za Zhivol 34 no 11 pp 965ndash966 2013
[15] S Y Shin J H Cho H J Kim J Jang S Lee and S Kim ldquoTwocases of acute lymphoblastic leukemia with an e1a3 BCR-ABL1fusion transcript rdquo Annals of Laboratory Medicine vol 35 no 1pp 159ndash161 2015
[16] H-G Goh J-Y Hwang S-H Kim Y-H Lee Y-L Kim andD-W Kim ldquoComprehensive analysis of BCR-ABL transcripttypes in Korean CML patients using a newly developed mul-tiplex RT-PCRrdquo Translational Research vol 148 no 5 pp 249ndash256 2006
[17] J Roman A Jimenez M Barrios J A Castillejo J Maldonadoand A Torres ldquoE1A3 as a unique naturally occurring BCR-ABLtranscript in an indolent case of chronic myeloid leukaemiardquoBritish Journal of Haematology vol 114 no 3 pp 635ndash637 2001
[18] G Martinelli M Amabile C Terragna et al ldquoConcomitantexpression of the rare E1A3 and B2A3 types of BCRABLtranscript in a chronic myeloid leukemia (CML) patientrdquoLeukemia vol 13 no 9 pp 1463ndash1464 1999
6 Case Reports in Hematology
[19] J Martinez-Serra R del Campo A Gutierrez et al ldquoChronicmyeloid leukemia with an e1a3 BCR-ABL fusion protein trans-formation to lymphoid blast crisisrdquo Biomarker Research vol 2no 14 pp 1ndash4 2014
[20] K G Roberts D Ki R C Payne-Turner et al ldquoTar-getable kinase-activating lesions in Ph-like acute lymphoblasticleukemiardquo The New England Journal of Medicine vol 371 pp1005ndash1015 2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
4 Case Reports in Hematology
Table 1 Published cases of e1a3 fusion variants in BCR-ABL1 associated hematologic neoplasms [7ndash19]
Agesex BCR-ABL1 transcript Disease classification Patientrsquos clinical status Citation39f e1a3 B-ALL Dead Soekarman et al [9]1f e1a3 B-ALL Dead Iwata et al [10]62f e1a3 B-ALL Dead Langabeer et al [11]mdash e1a3 B-ALL mdash Wilson et al [12]25f e1a3 B-ALL Dead Fujisawa et al [13]48m e1a3 B-ALL Dead Burmeister et al [8]61f e1a3 B-ALL Alive Burmeister et al [8]45f e1a3 B-ALL Alive Burmeister et al [8]64f e1a3 B-ALL Dead Burmeister et al [8]31m e1a3 B-ALL Alive Burmeister et al [8]78f e1a3 B-ALL Alive Chen et al [14]34m e1a3 B-ALL Alive Shin et al [15]17m e1a3 B-ALL Dead Shin et al [15]76m e1a3 B-ALL Alive Current case41m e1a3 + e1a2 CML Alive Al-Ali et al [7]64f e1a3 CML Alive Al-Ali et al [7]42m e1a3 CML Alive Goh et al [16]75f e1a3 CML Alive Roman et al [17]68f e1a3 + b2a3 CML Alive Martinelli et al [18]80m e1a3 CML B-ALLlowast Alive Martinez-Serra et al [19]B-ALL B-lymphoblastic leukemialymphoma CML chronic myeloid leukemia f female m male lowastCML with B-ALL type blast crisis
e1a3 ACAGTCCTTCGACAGCAGCAGTCCCCCCACGCCGCAGTGCCATAAGCGGCACCGGCACTGCCCGGTTGTCGTGTCe1a2 ACAGTCCTTCGACAGCAGCAGTCCCCCCACGCCGCAGTGCCATAAGCGGCACCGGCACTGCCCGGTTGTCGTGTC
e1a3 CGAGGCCACCATCGTGGGCGTCCGCAAGACCGGGCAGATCTGGCCCAACGATGGCGAGGGCGCCTTCCATGGAGAe1a2 CGAGGCCACCATCGTGGGCGTCCGCAAGACCGGGCAGATCTGGCCCAACGATGGCGAGGGCGCCTTCCATGGAGA
e1a3 CGCAe1a2 CGCAGAAGCCCTTCAGCGGCCAGTAGCATCTGACTTTGAGCCTCAGGGTCTGAGTGAAGCCGCTCGTTGGAACTC
e1a3e1a2 CAAGGAAAACCTTCTCGCTGGACCCAGTGAAAATGACCCCAACCTTTTCGTTGCACTGTATGATTTTGTGGCCAG
e1a3 GGTGAAAAGCTCCGGGTCTTAGGCTATAATCACAATGGGGAATGGTGe1a2 TGGAGATAACACTCTAAGCATAACTAAAGGTGAAAAGCTCCGGGTCTTAGGCTATAATCACAATGGGGAATGGTG
e1a3 TGAAGCCCAAACCAAAAATGGCCAAGGCTGGGTCCCAAGCAACTACATCACGCCAGTCAACAGTCTGGAGAAACAe1a2 TGAAGCCCAAACCAAAAATGGCCAAGGCTGGGTCCCAAGCAACTACATCACGCCAGTCAACAGTCTGGAGAAACA
Figure 3 Sequence alignments between e1a2 (p190) and the variant e1a3 (p190) on a portion of the BCR-ABL1 sequence Example of specificprimers [6] (green and blue) used to detect e1a2 with the quantitative RT-PCR method Notice that the exon a2 sequence (blue) is lacking inthe e1a3 transcript represented by the dotted line The lack of this primer binding site sequence results in a negative BCR-ABL1 p190 resultwith the p190 quantitative PCR test
Ultimately a qualitative BCR-ABL1 test can aid in thedetection of a rare BCR-ABL1 fusion variant when con-firmed with a next generation sequencing based assay that isdesigned to provide a high throughput assessment on clini-cally relevant mutations that influence therapeutic decisionsFurthermore this case illustrates that NGS based assays aremore sensitive than the traditional PCR approach andmay bevery useful in the workup of suspected BCR-ABL1 neoplasmsin certain circumstances In addition NGSwould also be abledetect Ph-like B-ALL cases which are BCR-ABL1 negativeand characterized by a gene-expression profile similar to that
of BCR-ABL1 positive B-ALL with genetic alterations that arealso responsive for TKIs [20]
We propose the following approach for molecular testingfor BCR-ABL1 for the detection of BCR-ABL1 at the time ofdiagnosis to optimize the detection of rare fusion variantswhich could enhance patient care First perform qualitativePCR with cytogenetics andor FISH testing If positiveperform quantitative PCR p190p210 to determine the BCR-ABL1 transcript If negative for quantitative PCRcytogeneticstesting or equivocal for qualitative PCR testing proceed tonext generation sequencing to detect possible rare variant
Case Reports in Hematology 5
transcripts andor Ph-like ALL disease This will allow thecapture of all clinically significant molecular mutations thatcould potentially guide therapy and management
One limitation in detecting rare variant transcripts solelyvia NGS is the inability to use standard PCR in some casesfor residual disease monitoring and follow-up ThereforeNGSmay be the only alternative for determining the presenceor absence of residual disease
5 Conclusion
In the era of molecular diagnostic medicine and a repertoireof potential targeted therapy options it is essential to have athorough understanding of the limitations of the individualmolecular assays and to follow a sound yet comprehensivediagnostic approach that would not only detect the commonabnormalities but rather be able to find the rare variants aswell Incorporating next generation sequencingmethods intoour current standard diagnostic PCR approach for BCR-ABL1andBCR-ABL1 negative Ph-like B-ALLwill aid inminimizingfalse negative results and may ultimately enhance patientcare In addition with the higher specificity of testing atthe sequencing level the rare e1a3 variant of BCR-ABL1p190may not actually be as infrequent as previously thought Theactual clinical significance of these rare variants is not yetfully understood and their role in clinical management withtargeted therapy needs to be further elucidated with the aid ofdetecting variants andmolecular profiles by newer molecularmethods such as next generation sequencing
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
This study was supported by Foundation Medicine Cam-bridge MA USA
References
[1] S H Swerdlow E Campo N L Harris et al World HealthOrganization Classification of Tumours of Haematopoietic andLymphoid Tissues International Agency for Research onCancer(IARC) Lyon France 4th edition 2008
[2] D Verma H M Kantarjian D Jones et al ldquoChronic myeloidleukemia (CML) with P190119861119862119877minus119860119861119871 analysis of characteristicsoutcomes and prognostic significancerdquo Blood vol 114 no 11pp 2232ndash2235 2009
[3] J He D Lipson M Nahas et al ldquoDevelopment and analyticalvalidation of a clinical next generation sequencing-based assayfor hematolymphoidmalignanciesrdquo inProceedings of the Ameri-can Association for Cancer Research Annual Meeting San DiegoCalif USA April 2014
[4] R Foa A Vitale M Vignetti et al ldquoDasatinib as first-linetreatment for adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemiardquo Blood vol 118 no 25pp 6521ndash6528 2011
[5] LightCycler t(922) Quantification Kit Instruction Manual Ver-sion 5 Roche 2013
[6] J Gabert E Beillard V H J van der Velden et al ldquoStandardiza-tion and quality control studies of lsquoreal timersquo quantitative reversetranscriptase polymerase chain reaction of fusion gene tran-scripts for residual disease detection in leukemiamdashA EuropeAgainst Cancer Programrdquo Leukemia vol 17 no 12 pp 2318ndash2357 2003
[7] H-K Al-Ali S Leiblein I Kovacs E Hennig D Niederwieserand M W N Deininger ldquoCML with an e1a3 BCR-ABL fusionrare benign and a potential diagnostic pitfallrdquo Blood vol 100no 3 pp 1092ndash1093 2002
[8] T Burmeister S Schwartz A Taubald et al ldquoAtypical BCR-ABLmRNA transcripts in adult acute lymphoblastic leukemiardquoHaematologica vol 92 no 12 pp 1699ndash1702 2007
[9] D Soekarman J van Denderen L Hoefsloot et al ldquoAnovel variant of the bcr-abl fusion product in Philadel-phia chromosome-positive acute lymphoblastic leukemiardquoLeukemia vol 4 no 6 pp 397ndash403 1990
[10] S Iwata SMizutani S Nakazawa and J-I Yata ldquoHeterogeneityof the breakpoint in the ABL gene in cases with BCRABLtranscript lacking ABL exon a2rdquo Leukemia vol 8 no 10 pp1696ndash1702 1994
[11] S E Langabeer K Haslam J Kelly M Leahy and E Van-denberghe ldquoAcute lymphoblastic leukaemia with an e1a3 BCR-ABL1 fusionrdquo Acta Haematologica vol 126 no 4 pp 214ndash2152011
[12] G A Wilson E A Vandenberghe R C Pollitt et al ldquoAreaberrant BCR-ABL transcripts more common than previouslythoughtrdquo British Journal of Haematology vol 111 no 4 pp1109ndash1111 2000
[13] S Fujisawa S Nakamura K Naito M Kobayashi and KOhnishi ldquoA variant transcript e1a3 of the minor BCR-ABLfusion gene in acute lymphoblastic leukemia case report andreview of the literaturerdquo International Journal of Hematologyvol 87 no 2 pp 184ndash188 2008
[14] Y Chen H W Wang X H Chen et al ldquoAdult acute lym-phoblastic leukemia with atypical BCR-ABL transcript e1a3 acase report and literature reviewrdquo Zhonghua Xue Ye Xue Za Zhivol 34 no 11 pp 965ndash966 2013
[15] S Y Shin J H Cho H J Kim J Jang S Lee and S Kim ldquoTwocases of acute lymphoblastic leukemia with an e1a3 BCR-ABL1fusion transcript rdquo Annals of Laboratory Medicine vol 35 no 1pp 159ndash161 2015
[16] H-G Goh J-Y Hwang S-H Kim Y-H Lee Y-L Kim andD-W Kim ldquoComprehensive analysis of BCR-ABL transcripttypes in Korean CML patients using a newly developed mul-tiplex RT-PCRrdquo Translational Research vol 148 no 5 pp 249ndash256 2006
[17] J Roman A Jimenez M Barrios J A Castillejo J Maldonadoand A Torres ldquoE1A3 as a unique naturally occurring BCR-ABLtranscript in an indolent case of chronic myeloid leukaemiardquoBritish Journal of Haematology vol 114 no 3 pp 635ndash637 2001
[18] G Martinelli M Amabile C Terragna et al ldquoConcomitantexpression of the rare E1A3 and B2A3 types of BCRABLtranscript in a chronic myeloid leukemia (CML) patientrdquoLeukemia vol 13 no 9 pp 1463ndash1464 1999
6 Case Reports in Hematology
[19] J Martinez-Serra R del Campo A Gutierrez et al ldquoChronicmyeloid leukemia with an e1a3 BCR-ABL fusion protein trans-formation to lymphoid blast crisisrdquo Biomarker Research vol 2no 14 pp 1ndash4 2014
[20] K G Roberts D Ki R C Payne-Turner et al ldquoTar-getable kinase-activating lesions in Ph-like acute lymphoblasticleukemiardquo The New England Journal of Medicine vol 371 pp1005ndash1015 2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Hematology 5
transcripts andor Ph-like ALL disease This will allow thecapture of all clinically significant molecular mutations thatcould potentially guide therapy and management
One limitation in detecting rare variant transcripts solelyvia NGS is the inability to use standard PCR in some casesfor residual disease monitoring and follow-up ThereforeNGSmay be the only alternative for determining the presenceor absence of residual disease
5 Conclusion
In the era of molecular diagnostic medicine and a repertoireof potential targeted therapy options it is essential to have athorough understanding of the limitations of the individualmolecular assays and to follow a sound yet comprehensivediagnostic approach that would not only detect the commonabnormalities but rather be able to find the rare variants aswell Incorporating next generation sequencingmethods intoour current standard diagnostic PCR approach for BCR-ABL1andBCR-ABL1 negative Ph-like B-ALLwill aid inminimizingfalse negative results and may ultimately enhance patientcare In addition with the higher specificity of testing atthe sequencing level the rare e1a3 variant of BCR-ABL1p190may not actually be as infrequent as previously thought Theactual clinical significance of these rare variants is not yetfully understood and their role in clinical management withtargeted therapy needs to be further elucidated with the aid ofdetecting variants andmolecular profiles by newer molecularmethods such as next generation sequencing
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
This study was supported by Foundation Medicine Cam-bridge MA USA
References
[1] S H Swerdlow E Campo N L Harris et al World HealthOrganization Classification of Tumours of Haematopoietic andLymphoid Tissues International Agency for Research onCancer(IARC) Lyon France 4th edition 2008
[2] D Verma H M Kantarjian D Jones et al ldquoChronic myeloidleukemia (CML) with P190119861119862119877minus119860119861119871 analysis of characteristicsoutcomes and prognostic significancerdquo Blood vol 114 no 11pp 2232ndash2235 2009
[3] J He D Lipson M Nahas et al ldquoDevelopment and analyticalvalidation of a clinical next generation sequencing-based assayfor hematolymphoidmalignanciesrdquo inProceedings of the Ameri-can Association for Cancer Research Annual Meeting San DiegoCalif USA April 2014
[4] R Foa A Vitale M Vignetti et al ldquoDasatinib as first-linetreatment for adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemiardquo Blood vol 118 no 25pp 6521ndash6528 2011
[5] LightCycler t(922) Quantification Kit Instruction Manual Ver-sion 5 Roche 2013
[6] J Gabert E Beillard V H J van der Velden et al ldquoStandardiza-tion and quality control studies of lsquoreal timersquo quantitative reversetranscriptase polymerase chain reaction of fusion gene tran-scripts for residual disease detection in leukemiamdashA EuropeAgainst Cancer Programrdquo Leukemia vol 17 no 12 pp 2318ndash2357 2003
[7] H-K Al-Ali S Leiblein I Kovacs E Hennig D Niederwieserand M W N Deininger ldquoCML with an e1a3 BCR-ABL fusionrare benign and a potential diagnostic pitfallrdquo Blood vol 100no 3 pp 1092ndash1093 2002
[8] T Burmeister S Schwartz A Taubald et al ldquoAtypical BCR-ABLmRNA transcripts in adult acute lymphoblastic leukemiardquoHaematologica vol 92 no 12 pp 1699ndash1702 2007
[9] D Soekarman J van Denderen L Hoefsloot et al ldquoAnovel variant of the bcr-abl fusion product in Philadel-phia chromosome-positive acute lymphoblastic leukemiardquoLeukemia vol 4 no 6 pp 397ndash403 1990
[10] S Iwata SMizutani S Nakazawa and J-I Yata ldquoHeterogeneityof the breakpoint in the ABL gene in cases with BCRABLtranscript lacking ABL exon a2rdquo Leukemia vol 8 no 10 pp1696ndash1702 1994
[11] S E Langabeer K Haslam J Kelly M Leahy and E Van-denberghe ldquoAcute lymphoblastic leukaemia with an e1a3 BCR-ABL1 fusionrdquo Acta Haematologica vol 126 no 4 pp 214ndash2152011
[12] G A Wilson E A Vandenberghe R C Pollitt et al ldquoAreaberrant BCR-ABL transcripts more common than previouslythoughtrdquo British Journal of Haematology vol 111 no 4 pp1109ndash1111 2000
[13] S Fujisawa S Nakamura K Naito M Kobayashi and KOhnishi ldquoA variant transcript e1a3 of the minor BCR-ABLfusion gene in acute lymphoblastic leukemia case report andreview of the literaturerdquo International Journal of Hematologyvol 87 no 2 pp 184ndash188 2008
[14] Y Chen H W Wang X H Chen et al ldquoAdult acute lym-phoblastic leukemia with atypical BCR-ABL transcript e1a3 acase report and literature reviewrdquo Zhonghua Xue Ye Xue Za Zhivol 34 no 11 pp 965ndash966 2013
[15] S Y Shin J H Cho H J Kim J Jang S Lee and S Kim ldquoTwocases of acute lymphoblastic leukemia with an e1a3 BCR-ABL1fusion transcript rdquo Annals of Laboratory Medicine vol 35 no 1pp 159ndash161 2015
[16] H-G Goh J-Y Hwang S-H Kim Y-H Lee Y-L Kim andD-W Kim ldquoComprehensive analysis of BCR-ABL transcripttypes in Korean CML patients using a newly developed mul-tiplex RT-PCRrdquo Translational Research vol 148 no 5 pp 249ndash256 2006
[17] J Roman A Jimenez M Barrios J A Castillejo J Maldonadoand A Torres ldquoE1A3 as a unique naturally occurring BCR-ABLtranscript in an indolent case of chronic myeloid leukaemiardquoBritish Journal of Haematology vol 114 no 3 pp 635ndash637 2001
[18] G Martinelli M Amabile C Terragna et al ldquoConcomitantexpression of the rare E1A3 and B2A3 types of BCRABLtranscript in a chronic myeloid leukemia (CML) patientrdquoLeukemia vol 13 no 9 pp 1463ndash1464 1999
6 Case Reports in Hematology
[19] J Martinez-Serra R del Campo A Gutierrez et al ldquoChronicmyeloid leukemia with an e1a3 BCR-ABL fusion protein trans-formation to lymphoid blast crisisrdquo Biomarker Research vol 2no 14 pp 1ndash4 2014
[20] K G Roberts D Ki R C Payne-Turner et al ldquoTar-getable kinase-activating lesions in Ph-like acute lymphoblasticleukemiardquo The New England Journal of Medicine vol 371 pp1005ndash1015 2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Case Reports in Hematology
[19] J Martinez-Serra R del Campo A Gutierrez et al ldquoChronicmyeloid leukemia with an e1a3 BCR-ABL fusion protein trans-formation to lymphoid blast crisisrdquo Biomarker Research vol 2no 14 pp 1ndash4 2014
[20] K G Roberts D Ki R C Payne-Turner et al ldquoTar-getable kinase-activating lesions in Ph-like acute lymphoblasticleukemiardquo The New England Journal of Medicine vol 371 pp1005ndash1015 2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom