Embed Size (px)
Citation preview


ABSTRACT
Aims and objectives: The primary objective of the study was to evaluate and document the evidence-
based efficacy and safety of the study drug in lowering blood pressure (BP). The secondary objectives
included efficacy of the study drug in improving symptoms, quality-of-life (QOL) and biochemical
parameters including Treadmill and Doppler echocardiography.
Study design: Phase IV post-marketing/surveillance study.
Material and methods: Thirty-five subjects with Prehypertension and Hypertension (Stage 1 and
Stage 2), attending the OPDs and camps of Heart Care Foundation of India were enrolled for the
nonplacebo-controlled prospective study. The subjects were given homoeopathic combination BPA
(study drug) in liquid dosage for 12 weeks. Baseline clinical and biochemical parameters, Treadmill
test and Doppler echocardiogram were compared with the same parameters at the end of 12 weeks.
Sixteen subjects completed the study.
Results: There was a mean fall in Systolic BP (SBP) of 15.75 mmHg and mean fall in Diastolic BP (DBP)
of 10.31 mmHg without any side effects. This significant decline in BP was evident from 4th week
onwards. There was an appreciable increase in the exercise tolerance as evident by the 8.6% increase
in Metabolic equivalents (METs) and 8.2% increase in Exercise time. No significant changes were
observed in systolic or diastolic function parameters on Doppler echocardiography at three months.
There was decrease in Blood sugar from 96.5 ± 13.938 at baseline to 92.56 ±12.329 at 12 weeks (p =
0.046). Serum uric acid levels also decreased from 5.681 ± 0.8998 at baseline to 6.031 ± 0.8822 at 12
weeks (p = 0.053) suggesting a beneficial effect of the combination on insulin resistance (IR). There
were positive changes in the QOL as assessed by SF36 Questionnaire. The average Rand score
improved from 54.53 ± 21.9991 to 77.55 ± 10.493 at 12 weeks (p < 0.001). All data are presented as
Mean ± Standard deviation (SD).
Conclusion: The results of the study showed that the study drug can be safely used as monotherapy in
patients with Prehypertension or Hypertension with no complications.
1
BPA Drug in Prehypertension & Hypertension: A Pilot Study
Dr. Prachi Garg , Dr. KK Aggarwal , Dr. Sunita Gupta , Parul Takkar , Dr. Mudita Arora† ‡ ¶
* **
***
†
‡
¶
Clinical Associate, Internal Medicine, Moolchand Medcity, New DelhiSenior Consultant Cardiologist, Heart Care Foundation of India, New Delhi
Padma Shri and Dr. B.C. Roy National Awardee
Consultant Homoeopath, New Delhi
Statistician
Senior Manager, Clinical Research and Product DevelopmentBakson Drugs and Pharmaceutical Pvt. Ltd., New Delhi
Keywords: Homoeopathic combination BPA, prehypertension, hypertension

2
INTRODUCTION
AIMS AND OBJECTIVES
Hypertension is the commonest cardiovascular disorder, posing a major public health challenge to
population. The prevalence of hypertension among adults in developed countries is 25%. A similar 1
prevalence has also been observed in developing countries ranging from 10 to 20%. It has been
shown that there were 972 million people living with Hypertension worldwide in the year 2000, and it 2
is estimated that this number will escalate to more than 1.56 billion by the year 2025. Around two
thirds of those people with Hypertension worldwide were living in developing countries (639 million)
in 2000 and this number is projected to rise to three-quarters living in developing countries (1.15 3billion) by 2025. Hypertension is an important independent predictor of Cardiovascular disease
4(CVD), cerebrovascular accidents and death. The prevalence of Hypertension has been increasing in 4
India, both in rural and urban regions. The prevalence of Prehypertension in India is also increasing. 5
This implies accompanying raise in other CVD risk factors in the Indian population. In India, CVDs are
estimated to be responsible for 1.5 million deaths annually. Indeed, it is estimated that by 2020, CVDs 3will be the largest cause of mortality and morbidity in India. Trials completed within the last five years
clearly indicate that overall Cardiovascular risk is reduced by blood pressure (BP) lowering to levels
below 140/90 mmHg. Greater cardiovascular risk reduction is not seen, however, by driving BP to
levels well below 130/80 mmHg. This is true across the spectrum of cardiorenal risk with few 6
exceptions, stroke prevention possibly being one.
Antihypertensive drugs work in different ways to lower BP. Some drugs lower BP by removing extra
fluid and salt from the body (e.g. diuretics). Others lower BP by slowing down the heartbeat (e.g. b-
blockers) or by relaxing, widening or preventing the narrowing of blood vessels (e.g., angiotensin-
converting enzyme [ACE] inhibitors, calcium channel blockers [CCBs]).
A review has described the main homoeopathic medicines whose center of action includes the heart, 7
especially medicines commonly used in mother tincture form for Hypertension. The study drug is a 8-15
combination of seven drugs used for reducing high BP. They are well-known homoeopathic
medicines and help relieve associated symptoms of BP too. The drugs included are Rauwolfia
serpentina 2X (5.00% v/v), Viscum album 3X (1.00% v/v), Crataegus oxyacantha 2X (1.00% v/v), Arnica
montana 3X (0.25% v/v), Valeriana officinalis 3X (0.50% v/v), Melilotus alba 3X (0.25% v/v), Cactus
grandiflorus 3X (0.25% v/v), Excipients q.s. and Alcohol (7.00% v/v).
Primary objective: To evaluate and document the evidence-based efficacy and safety of the study
drug in lowering BP.
Secondary objectives:
u To assess the efficacy of the study drug in relieving symptoms associated with Hypertension.
u To assess the efficacy of the study drug in improving quality-of-life (QOL) in hypertensive subjects.
u To assess the improvement or changes, if any, in necessary investigations performed at the
beginning and end of study especially Lipid profile, Treadmill test and Doppler echocardiograms.

3
MATERIAL AND METHODS
Study Design
A phase IV post-marketing/surveillance study was done to delineate additional information on long-
term benefits, optimal use and any side effects after approval of the study protocol from the Ethics
Committee. The duration of the study was 15 months (October 2010 to December 2011). Subjects
with Prehypertension or Hypertension without target organ damage attending the OPD and camps of
Heart Care Foundation of India were included in the study. A total of 67 subjects were screened. There
were 32 screen failures. A total of 35 subjects were enrolled, out of whom 16 subjects completed the
study. There were 19 dropouts (lost to follow-up). Informed consent was obtained from each study
subject. The study drug was dispensed in 30 ml bottle pack duly labeled as per the Drug Authority
requirements. No placebo was used during the study. It was a nonrandomized nonblind open study.
Inclusion Criteria
u Adults of both sexes aged 25-75 years.
u Newly diagnosed or subjects with Prehypertension (diastolic BP [DBP] 80-89 mmHg and systolic
BP [SBP] 120-139 mmHg) of less than one year duration.
u Patients with stage 1 (SBP >140 and <160 and DBP >90 and <100 mmHg) and Stage 2 (SBP >160
and DBP >100 mmHg) Hypertension. All subjects were subjected to a washout period of two
weeks.
u Written informed consent for the use of the study drug as stand-alone treatment and necessary
investigations.
Exclusion Criteria
u Known Secondary Hypertension
u Body mass index (BMI) >35 kg/m2
u Pregnant and lactating women
u Poorly-controlled Hypertension and/or complications
u Target organ damage
u Diabetes
u Abnormal lab screening: Hemoglobin (Hb) <75% of lower limit, Serum Cholesterol >300 mg/dl
u Abnormal resting ECG
u Pre-existing chronic debilitating illness
u Subjects on hormonal contraceptives, Steroids or Nonsteroidal Anti-inflammatory Drugs
(NSAIDs)
Investigations
Complete blood count (CBC), Lipid profile, Fasting Blood Sugar, Serum Creatinine, Serum Uric Acid,
Serum Glutamic Pyruvic Transaminase (SGPT), Routine urinalysis, Treadmill test and Doppler

4
echocardiography were done at baseline and after 12 weeks of treatment.
Drug Dose Protocol
Each subject was given 20 drops of the study drug diluted with 30 ml water twice-daily. Patients who
were intolerant to the study drug were instructed to start with 10 drops of the study drug diluted with
30 ml water twice-daily and increase the dose gradually to 15 and then 20 drops.
Follow-up
The subjects were clinically assessed every week and their BP readings were recorded. Investigations
were done at baseline and after 12 weeks of treatment (completion of the study period).
Statistical Methods
Statistical analysis was done using the SPSS statistical package (version 17.0). Results are expressed as
Mean± standard deviation (SD). Paired test was used to compare normally distributed continuous
variables from pre- and post-intervention. BP values over time within the groups were analyzed using
repeated measures analysis of variance (ANOVA) followed by Bonferroni’s post-hoc testing; p < 0.05
was considered statistically significant.
FALL IN SYSTOLIC BP
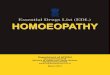
Means of SBP starting from 0 week to the 12th week were analyzed. There was statistically significant
(p < 0.001) mean fall in SBP of 15.75 mmHg at 12 weeks (95% confidence interval [CI] 9.25 to 22.25)
(Table 1 and Fig. 1). Post-hoc tests using Bonferroni correction revealed that the reduction in SBP
RESULTS
Week 0 16 146.25 9.83
Week 1 16 135.75 9.74 -7.18%
Week 2 16 138 14.17 -5.64%
Week 3 16 134.06 12.89 -8.34%
Week 4 16 131.75 9.03 -9.91%
Week 5 16 133.69 13.46 -8.59%
Week 6 16 132.63 12.92 -9.31%
Week 7 16 131.88 11.01 -9.83%
Week 8 16 131.81 10.37 -9.87%
Week 9 16 134.75 11.13 -7.86%
Week 10 16 131.44 10.84 -10.13%
Week 11 16 133.88 13.65 -8.46%
Week 12 16 130.5 11.97 -10.77%
SBPNumber of
patients Mean Standard Deviation
change from week 0 (%)
Table1. Fall in Systolic BP

5
DBPNumber of
patients Mean Standard Deviation
change from week 0 (%)
Week 0 16 95.44 7.92
Week 1 16 86.69 7.49 -9.17%
Week 2 16 85.69 10.21 -10.22%
Week 3 16 86.69 7.49 -9.17%
Week 4 16 85.06 7.64 -10.88%
Week 5 16 87.06 7.84 -8.78%
Week 6 16 84.63 10.58 -11.33%
Week 7 16 86.38 7.94 -9.49%
Week 8 16 85.38 10.06 -10.54%
Week 9 16 89.06 9.70 -6.68%
Week 10 16 85.25 6.06 -10.68%
Week 11 16 86.94 8.43 -8.91%
Week 12 16 85.13 8.76 -10.80%
values was significant from 4th week onwards.
FALL IN DIASTOLIC BP
There was statistically significant mean fall in DBP of 10.31 mmHg from 0 to 12 weeks (95% CI 5.57 to
15.05) (p < 0.001) (Table 2 and Fig. 2). Post-hoc tests using Bonferroni correction revealed that the
reduction in DBP values was again significant from the 4th week onwards.
Table2. Fall in Diastolic BP
SBP
100
110
120
130
140
150
160
0 1 2 3 4 5 6 7 8 9 10 11 12
Weeks
Mean
valu
es
Figure 1. Reduction in SBP.
SBP

6
Table 3: Increase in METs at Three Months
Baseline 14 11.54 1.82
3 months 14 12.53 2.05<0.001
METSNumber of
patients Mean Standard Deviation P Value
IMPROVEMENT IN TREADMILL PARAMETERS
There was a statistically significant improvement in Metabolic equivalents (METs) from 11.54 ± 1.82 at
baseline to 12.53 ± 2.05 at 12 weeks (p < 0.001), which amounted to an average increase of 8.6% per
patient in METs. The observed mean difference was 0.95 minutes (95% CI ?1.39 to ?0.51) (Table 3 and
Fig. 3). There was a statistically significant mean gain of exercise time of 0.82 minutes (95% CI ?1.25 to
?0.38). The gain was from 9.84 ± 1.78 minutes at baseline to 10.65 ± 1.78 minutes at 12 weeks (p =
0.001). This amounted to an average increase of 8.2%per patient in Exercise time (Table 4 & Figure 4).
METS
0
3
6
9
12
15
Baseline 3 months
Mean
valu
es
Figure 3. Increase in METs at three months.
METS
DBP
60
65
70
75
80
85
90
95
100
0 1 2 3 4 5 6 7 8 9 10 11 12
Weeks
Mean
valu
es
Figure 2. Reduction in DBP.

7
ECHO PARAMETERS
There was no statistical significant change in Echo parameters after three months of treatment.
u No significant differences were observed in the means of E/A (Ratio of Mitral E-wave velocity to
Mitral A-wave velocity) at baseline (1.15 ± 0.32) and after three months (1.10 ± 0.34) (p = 0.535).
The observed mean difference was 0.05 (95% CI ?0.11 to 0.19).
u There were no significant differences in the means of E/E’ ratio (Ratio of early mitral inflow to
early Mitral annular velocity) at baseline (9.03 ± 1.97) and after three months (9.22 ± 2.5) (p =
0.788). The observed mean difference was 0.19 (95% CI ?1.65 to 1.27).
u There was no significant difference in the means of Left ventricular (LV) end-diastolic dimension
at baseline (40 ± 4.81) and after three months (39.08 ± 4.43) (p = 0.156). The observed mean
difference was 0.93 (95% CI ?0.39 to 2.24).
u No significant differences were observed in the means of Aortic diameter (Ao) at baseline (29.86
± 3.44) and after three months (29.54 ± 3.35) (p = 0.682). The observed mean difference was 0.32
(95% CI ?1.31 to 1.95).
u There was no significant difference in the means of Left atrial (LA) diameter at baseline (28.92 ±
3.80) and after three months (28.49 ± 3.35) (p = 0.529). The observed mean difference was 0.43
Table 4 : Increase in Exercise Time at Three Months
0.001
Exercise TimeNumber of
patients Mean Standard Deviation P Value
Baseline 14 9.84 1.78
3 months 14 10.65 1.78
Exercise Time
0
2
4
6
8
10
12
14
Baseline 3 months
Mean
valu
es
Figure 4. Increase in Exercise time at three months.
EXERCISE TIME

8
(95% CI ?0.98 to 1.83).
u There were no significant differences in the means of LV septum at baseline (9.78 ± 1.29) and
after three months (9.77 ± 1.17) (p = 0.969). The observed mean difference was 0.01 (95% CI
?0.69 to 0.72).
u There was no significant difference in the means of posterior wall thickness at baseline (9.78 ±
1.29) and after three months (9.77 ± 1.17) (p = 0.969). The observed mean difference was 0.01
(95% CI ?0.69 to 0.72).
BIOCHEMISTRY
u There was no significant difference in the means from baseline to the end of the study for Hb
(14.406 ± 1.3463 at baseline and 14.106 ± 1.3102 at 12 weeks [p = 0.193]);
u There was no significant difference in the means from baseline to the end of the study for
Erythrocyte sedimentation rate (ESR) (15.69 ± 13.553 at baseline and 16.25 ± 8.497 at 12 weeks
[p = 0.847]);
u There was no significant difference in the means from baseline to the end of the study for Serum
Creatinine (0.888 ± 0.1854 at baseline and 0.85 ± 0.1838 at 12 weeks [p = 0.315]);
u There was no significant difference in the means from baseline to the end of the study for SGPT
(51.38 ± 40.516 at baseline and 44.63 ± 19.677 at 12 weeks [p = 0.534]);
u There was no significant difference in the means from baseline to the end of the study for Total
cholesterol (183.88 ± 39.16 at baseline and 194.25 ±35.21 at 12 weeks [p = 0.191]);
u There was no significant difference in the means from baseline to the end of the study for Low-
density lipoprotein (LDL) cholesterol (122.56 ± 36.30 at baseline and 127.20 ± 29.25 at 12 weeks
[p = 0.476]);
u There was no significant difference in the means from baseline to the end of the study for VLDL
cholesterol (25.66 ± 8 at baseline and 28.48 ± 10.59 at 12 weeks [p = 0.209]);
u There was no significant difference in the means from baseline to the end of the study for High-
density lipoprotein (HDL) cholesterol (42.38 ± 9.14 at baseline and 41.38 ± 8 at 12 weeks [p =
0.403]);
u There was no significant difference in the means from baseline to the end of the study for
Triglycerides (128.31 ± 40.01 at baseline and 142.31 ± 53.15 at 12 weeks [p = 0.213]).
u Blood sugar decreased at three months (96.5 ± 13.938 at baseline and 92.56 ± 12.329 at 12 weeks
[p = 0.046]). A similar decrease was seen in the Serum uric acid levels (5.681 ± 0.8998 at baseline
and 6.031 ± 0.8822 at 12 weeks [p = 0.053]). Both these changes suggested a beneficial effect on
the Insulin resistance (IR).
u There was no change in BMI (28.62 ± 5.69 at baseline and 28.32 ± 5.83 at 12 weeks [p = 0.160]).

9
CHANGES IN QUALITY OF LIFE (QOL)16
Change in QOL was assessed by SF36 Questionnaire and each subject was scored before and after
completion of study. The average Rand score improved from 54.53 ± 21.9991 at baseline to 77.55 ±
10.493 at 12 weeks (p < 0.001).
No serious adverse events were reported during the entire course of the study.
17In a review of short-term studies on Antihypertensives including CCBs, Diuretics, ACE inhibitors, a
blockers, b-blockers, Angiotensin II receptor blockers, the change in SBP and DBP was a negative value
ranging from –2 to even –12 points, which is comparable to that observed in the current study with
mean fall in SBP of 15.75 mmHg and mean fall in DBP of 10.31 mmHg without any side effects
observed during the entire study duration. The change however was observed for over a period of 12
weeks with a statistically significant fall observed from 4th week onwards, so the study drug can be
safely used for Prehypertension, Stage 1 Hypertension and for Stage 2 excluding hypertensive
emergencies and urgencies. There were appreciable increase in METs by 8.6% and exercise time by
8.2%, though no change was observed in Echo parameters as duration of observation was just 12
weeks during which a change in Echo is not expected as the trends go in other such studies.
The results of the study showed that the study drug can safely be used as monotherapy in patients
with Prehypertension or Hypertension without complications. This is only a preliminary study and
more data needs to be collected for further collaboration. A prolonged study for a period of at least six
months to one year is needed for an in-depth analysis of the medicine.
The study product BPA (Bee Pee Aid) was supplied by Bakson Drugs and Pharmaceuticals Pvt. Ltd.
It was an independent study and not influenced by any market forces.
SAFETY EVALUATION
DISCUSSION
CONCLUSION
ACKNOWLEDGMENT
DISCLAIMER
Figure 5. Changes in QOL
Total Rand Score
0
20
40
60
80
100
Baseline Final
Me
an
va
lue
s
TOTAL RAND SCORE

10
REFERENCES
u Kokiwar PR, Gupta SS, Durge PM. Prevalence of hypertension in a rural community of Central India. JAPI
2012;60:26-9.1.
u Chockalingam A, Campbell NR, Fodor JG. Worldwide epidemic of hypertension. Can J Cardiol
2006;22(7):553-5.
u Bansal SK, Saxena V, Kandpal SD, Gray WK, Walker RW, Goel D. The prevalence of hypertension and
hypertension risk factors in a rural Indian community: A prospective door-to-door study. J Cardiovasc Dis
Res 2012;3(2): 117-23.
u Yadav S, Boddula R, Genitta G, Bhatia V, Bansal B, Kongara S, et al. Prevalence & risk factors of
prehypertension & hypertension in an affluent north Indian population. Indian J Med Res 2008;128(6):712-
20.
u Asmathulla S, Rajagovindan D, Sathyapriya V, Pai BK. Prevalence of prehypertension and its relationship to
cardiovascular disease risk factors in Puducherry. Indian J Physiol Pharmacol 2011;55(4):343-50.
u Cunnane RT, Bakris GL. Hypertensive goals in patients with coronary artery disease. Curr Cardiol Rep 2012
Aug 14. [Epub ahead of print]
u Holland L. Cardiovascular medicines. British Homeopathic Journal 1994;83(4):223-9.
u Circosta C, De Pasquale R, Samperi S, Pino A, Occhiuto F. Biological and analytical characterization of two
extracts from Valeriana officinalis. J Ethnopharmacol 2007;112(2):361-7.
u Mojiminiyi FB, Owolabi ME, Igbokwe UV, Ajagbonna OP. The vasorelaxant effect of Viscum album leaf
extract is mediated by calcium-dependent mechanism. Niger J Physiol Sci 2008;23(1-2):115-20.
u Shamon SD, Perez MI. Blood pressure lowering efficacy of reserpine for primary hypertension. Cochrane
Database Syst Rev 2009;(4):CD007655.
u Miller AL. Botanical influences on cardiovascular disease. Altern Med Rev 1998;3(6):422-31.
u Jones AO. Cactus grandiflorus in some forms of heart disease. Br Med J 1890;1(1515):70-1.
Norred CL, Zamudio S, Palmer SK. Use of complementary and alternative medicines by surgical patients.
AANA J 2000;68(1):13-8.
u Robin Murphy. Rauwolfia serpentina, Viscum album, Crataegus, Arnica montana, Valeriana, Melilotus alba,
Cactus grandiflorus. In: Lotus Materia Medica. 2nd edition, (revised), 2009:p.172-6, 307-11, 556-9, 1117-
20, 1465-7,1855-8.
u William Boericke. Rauwolfia serpentina, Viscum album, Crataegus, Arnica montana, Valeriana, Melilotus
alba, Cactus grandiflorus. In: Pocket Manual of Homeopathic Materia Medica and Repertory. 9th edition
2005:p.76-9, 137-9, 237-8, 427-8, 664-5, 677-8, 1072.
u Bulpitt CJ, Fletcher AE. The measurement of quality of life in hypertensive patients: a practical approach. Br
J Clin Pharmacol 1990;30(3):353-64.
u Effective Health Care. Bulletin on the effectiveness of health service interventions for decision makers.
Effectiveness of antihypertensive drugs in black people. 2004:8(4).


![[Insert title of report] - assets.publishing.service.gov.uk · Cosmetics Aromatherapy ... as traditional herbal medicines or as homoeopathic medicines have to meet statutory standards](https://img.pdfslide.net/doc/110x75/5b25b81e7f8b9a5b4d8b4634/insert-title-of-report-cosmetics-aromatherapy-as-traditional-herbal.jpg)