Embed Size (px)
DESCRIPTION
Keystone Island Flap for Parotid Defects
Citation preview

RECONSTRUCTIVE
Keystone Island Flap Reconstruction ofParotid Defects
Felix C. Behan, F.R.A.C.S.Cheng H. Lo, M.B.B.S.
Andrew Sizeland, Ph.D.,F.R.A.C.S.
Toan Pham, M.B.B.S.Michael Findlay, F.R.A.C.S.,
Ph.D.
Parkville, Footscray, and EastMelbourne, Victoria, Australia
Background: Skin cancers of the face and scalp have a propensity to metastasizeto the parotid group of lymph nodes. The resection of these secondary tumorsand other primary tumors in the parotid region often results in defects requiringflap reconstruction. Pectoralis major flaps are reliable and free flaps are arguablythe criterion standard. However, we have found keystone island flaps to be asimple and robust alternative, with low donor-site and patient morbidity. Theaim of this article is to share our surgical technique, experience, and outcomesof reconstructing parotid defects with keystone island flaps.Methods: The authors retrospectively reviewed 62 patients who had 63 parotiddefect reconstructions at a single institution from 2004 to 2009 (5-year period).Results: The diseases involved were squamous cell carcinoma (52 cases), mel-anoma (five cases), basal cell carcinoma (four cases), and others (two cases).Nine patients presented with a previous history of radiotherapy and 33 patientsrequired adjuvant radiotherapy. Seven patients (11 percent) suffered postop-erative complications necessitating a return to the operating room.Conclusions: Keystone island perforator-based flaps present an alternative tofree tissue transfer. From the series presented, it can be seen that reliable andreproducible results are achievable. (Plast. Reconstr. Surg. 130: 36e, 2012.)CLINICAL QUESTION/LEVEL OF EVIDENCE: Therapeutic, IV.
Reconstruction of parotid defects is commonin the field of head and neck cancer surgery.Although fewer than one-third of parotid
tumors are malignant (mucoepidermoid carci-noma being the commonest), 70 to 85 percent ofall adult salivary gland tumors occur in the parotidgland.1 In addition, Australia has the highest in-cidence of melanoma and nonmelanoma skin can-cers in the world (and the incidence is rising).2,3
Wide local excision remains the most commontreatment modality for these skin cancers.2,3 Also,squamous cell carcinoma from the frontotempo-ral scalp region has a propensity to metastasize tothe periparotid or intraparotid group of lymphnodes.1
Free tissue transfer has been the standard ofcare in the reconstruction of large head and neckdefects. However, our senior author (F.C.B.) hasused the keystone island flap with success for morethan 20 years to reconstruct defects often other-wise appropriate for microsurgical reconstruc-tion. The principles of the keystone island flap, alocoregional perforator-based island flap, werefirst detailed in 1992, and ensuing publicationsfollowed largely in the Australasian literature untilrecently.4 –7 The aim of this article is to share oursurgical technique, experience, and outcomesof reconstructing parotid defects with keystoneisland flaps. The advantages and disadvantagesof this reconstructive technique and compari-sons with alternate reconstructive options arediscussed.
PATIENTS AND METHODSStudy Design
A retrospective review of 62 patients who hadparotid defect reconstructions at a single hospital
From the Department of Plastic and Reconstructive Surgery,Royal Melbourne Hospital; the Department of Plastic andReconstructive Surgery, Western General Hospital; and theDepartment of Surgical Oncology, Peter MacCallum CancerInstitute.Received for publication October 6, 2010; accepted March10, 2011.Presented at the 79th Annual Scientific Congress of the RoyalAustralasian College of Surgeons, in Perth, Western Aus-tralia, Australia, May 4 through 7, 2010.Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3182547f55
Disclosure: The authors have no financial interestto declare in relation to the content of this article. Nooutside funding was received.
www.PRSJournal.com36e
(Western General Hospital, Melbourne, Australia)over a 5-year period (2004 to 2009) was performed.Patient information gathered from hospital re-cords included patient demographics, disease,treatment, and outcomes. These were supple-mented by records and photographs from thesenior author (F.C.B.).
Surgical TechniqueThe principles and technique of keystone is-
land flap have been published previously, and asummary of the pertinent points are presentedhere.4,5,8 In 2003, a classification system was devel-oped for keystone island flaps,5 as follows:
Type I: standard flap design without division ofdeep fascia.
Type II: deep fascia on the convex aspect of theflap is divided to enhance mobilization. Fur-ther subcategorization (type IIa) secondary de-fect is closed primarily and (type IIb) second-ary defect is closed with a split skin graft.
Type III: double keystone flaps are designed tofacilitate closure, one on either side of thedefect.
Type IV: up to two-thirds of the flap is under-mined. Flap mobilization is maximized.
The keystone island flap is usually a curvilineartrapezoidal design but, for parotid defects, theexact shape of the keystone island flap is less im-
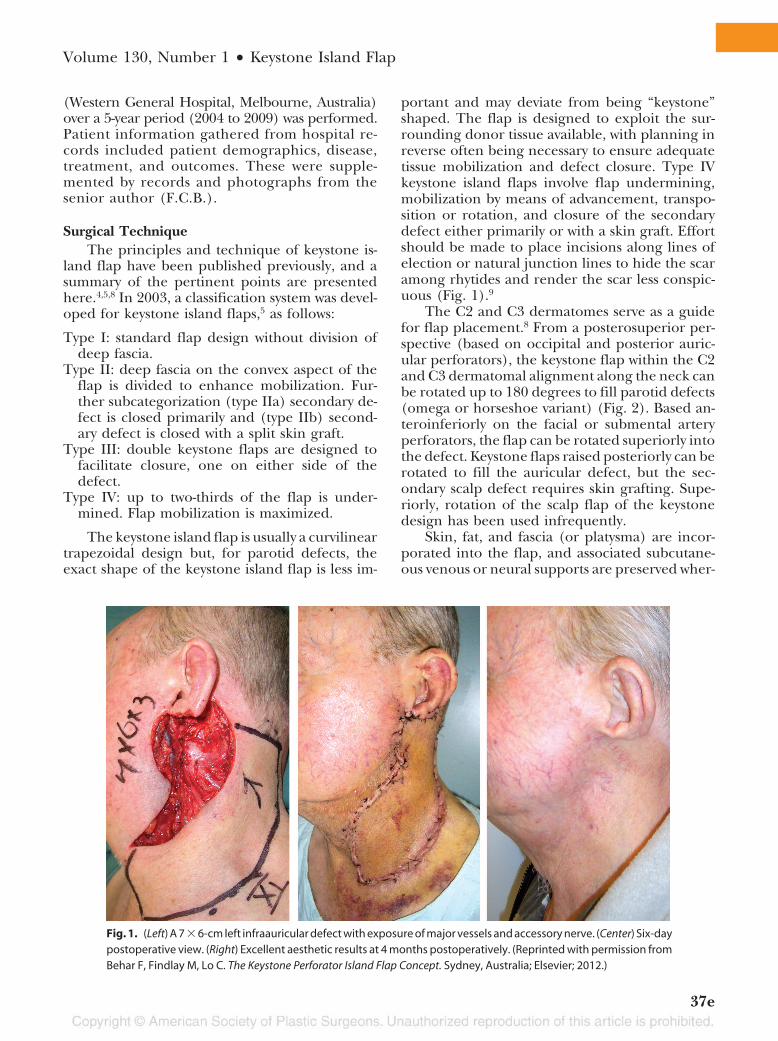
portant and may deviate from being “keystone”shaped. The flap is designed to exploit the sur-rounding donor tissue available, with planning inreverse often being necessary to ensure adequatetissue mobilization and defect closure. Type IVkeystone island flaps involve flap undermining,mobilization by means of advancement, transpo-sition or rotation, and closure of the secondarydefect either primarily or with a skin graft. Effortshould be made to place incisions along lines ofelection or natural junction lines to hide the scaramong rhytides and render the scar less conspic-uous (Fig. 1).9
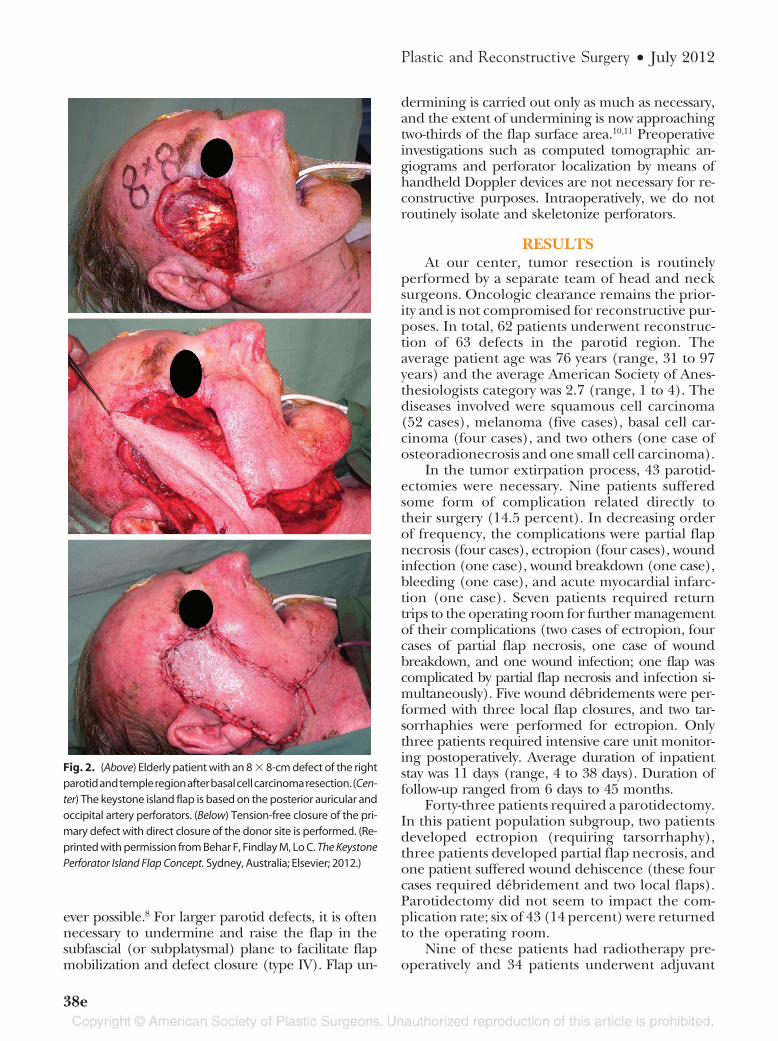
The C2 and C3 dermatomes serve as a guidefor flap placement.8 From a posterosuperior per-spective (based on occipital and posterior auric-ular perforators), the keystone flap within the C2and C3 dermatomal alignment along the neck canbe rotated up to 180 degrees to fill parotid defects(omega or horseshoe variant) (Fig. 2). Based an-teroinferiorly on the facial or submental arteryperforators, the flap can be rotated superiorly intothe defect. Keystone flaps raised posteriorly can berotated to fill the auricular defect, but the sec-ondary scalp defect requires skin grafting. Supe-riorly, rotation of the scalp flap of the keystonedesign has been used infrequently.
Skin, fat, and fascia (or platysma) are incor-porated into the flap, and associated subcutane-ous venous or neural supports are preserved wher-
Fig. 1. (Left) A 7 � 6-cm left infraauricular defect with exposure of major vessels and accessory nerve. (Center) Six-daypostoperative view. (Right) Excellent aesthetic results at 4 months postoperatively. (Reprinted with permission fromBehar F, Findlay M, Lo C. The Keystone Perforator Island Flap Concept. Sydney, Australia; Elsevier; 2012.)
Volume 130, Number 1 • Keystone Island Flap
37e
ever possible.8 For larger parotid defects, it is oftennecessary to undermine and raise the flap in thesubfascial (or subplatysmal) plane to facilitate flapmobilization and defect closure (type IV). Flap un-
dermining is carried out only as much as necessary,and the extent of undermining is now approachingtwo-thirds of the flap surface area.10,11 Preoperativeinvestigations such as computed tomographic an-giograms and perforator localization by means ofhandheld Doppler devices are not necessary for re-constructive purposes. Intraoperatively, we do notroutinely isolate and skeletonize perforators.
RESULTSAt our center, tumor resection is routinely
performed by a separate team of head and necksurgeons. Oncologic clearance remains the prior-ity and is not compromised for reconstructive pur-poses. In total, 62 patients underwent reconstruc-tion of 63 defects in the parotid region. Theaverage patient age was 76 years (range, 31 to 97years) and the average American Society of Anes-thesiologists category was 2.7 (range, 1 to 4). Thediseases involved were squamous cell carcinoma(52 cases), melanoma (five cases), basal cell car-cinoma (four cases), and two others (one case ofosteoradionecrosis and one small cell carcinoma).
In the tumor extirpation process, 43 parotid-ectomies were necessary. Nine patients sufferedsome form of complication related directly totheir surgery (14.5 percent). In decreasing orderof frequency, the complications were partial flapnecrosis (four cases), ectropion (four cases), woundinfection (one case), wound breakdown (one case),bleeding (one case), and acute myocardial infarc-tion (one case). Seven patients required returntrips to the operating room for further managementof their complications (two cases of ectropion, fourcases of partial flap necrosis, one case of woundbreakdown, and one wound infection; one flap wascomplicated by partial flap necrosis and infection si-multaneously). Five wound debridements were per-formed with three local flap closures, and two tar-sorrhaphies were performed for ectropion. Onlythree patients required intensive care unit monitor-ing postoperatively. Average duration of inpatientstay was 11 days (range, 4 to 38 days). Duration offollow-up ranged from 6 days to 45 months.
Forty-three patients required a parotidectomy.In this patient population subgroup, two patientsdeveloped ectropion (requiring tarsorrhaphy),three patients developed partial flap necrosis, andone patient suffered wound dehiscence (these fourcases required debridement and two local flaps).Parotidectomy did not seem to impact the com-plication rate; six of 43 (14 percent) were returnedto the operating room.
Nine of these patients had radiotherapy pre-operatively and 34 patients underwent adjuvant
Fig. 2. (Above) Elderly patient with an 8 � 8-cm defect of the rightparotidandtempleregionafterbasalcellcarcinomaresection.(Cen-ter) The keystone island flap is based on the posterior auricular andoccipital artery perforators. (Below) Tension-free closure of the pri-mary defect with direct closure of the donor site is performed. (Re-printed with permission from Behar F, Findlay M, Lo C. The KeystonePerforator Island Flap Concept. Sydney, Australia; Elsevier; 2012.)
Plastic and Reconstructive Surgery • July 2012
38e

radiotherapy after keystone island flap reconstruc-tion. The nine patients who had preoperative ra-diotherapy did not have a higher complicationrate. Only one of nine patients (11 percent) hada complication (ectropion) requiring surgery.There were no partial or total flap losses in thispatient group. Because of the retrospective natureof this article, the dimensions of defects were notrecorded in every patient. However, these ninepatients who had preoperative radiotherapy hadan average defect size of 36 cm2, which appearedsimilar in size to the nonirradiated defects.
DISCUSSIONIn 1973, the senior author (F.C.B.) introduced
the term “angiotome” to refer to any area of in-tegument supplied by an axial vessel.12 It was pro-posed that each angiotome may be safely raised asa flap, or extended by random communications orlinkage vessels with an adjacent angiotome.12 Thesenior author (F.C.B.) went on to publish his ex-perience with the keystone island flap concept(keystone design perforator island flap) in 1992and 2003,4,5 a reconstructive technique developedand based on the angiotome concept.
Keystone island flaps (perforator based) anddermal pedicled platysma flaps both incorporateskin, subcutaneous tissue, and the underlying plat-ysma. Since platysma flaps were first introducedapproximately 30 years ago,13 several variationshave been described to provide coverage of neck,chin, cheek, lips, and the oral cavity. These in-clude the standard or superiorly based platysmaflap (submental artery, a branch of the facialartery),14 the distally or inferiorly based flap (trans-verse cervical or superficial cervical arteries)14,15
(Fig. 3), and the transverse platysma flap (occipitaland posterior auricular arteries).16,17 Szudek andTaylor performed a systematic review of 16 caseseries and 190 patients with platysma flaps, reveal-ing a total complication rate of 37 percent.18 Ac-cording to their review, complication rates be-tween 10 and 40 percent have been reported.18
Whereas platysma flaps were regarded as unre-liable,18 our current series of keystone island flapscompared rather favorably, with a total complica-tion rate of 14.5 percent despite 63 percent (43 of62) of the patients having had radiotherapy intheir multimodality tumor management. Preop-erative radiotherapy is not a contraindication forkeystone island flaps. In fact, the robust nature ofkeystone island flaps, even in irradiated fields af-fected by obliterative endarteritis and chronicischemia, has been previously demonstrated andpublished.6 In our experience, complication rates
were acceptably low and compared favorably withthose of other reconstructive techniques.6
A direct comparison may be made between thekeystone island flap and the transverse platysmaflap because they may be similarly oriented in the
Fig. 3. (Above) A patient with a 13 � 7-cm right infraauriculardefect after parotidectomy and neck dissection for squamouscell carcinoma. (Center) A double keystone flap (type III) is mobi-lized to close the defect. (Below) Direct closure of the donor sitewith a drain in situ is shown. (Reprinted with permission fromBehar F, Findlay M, Lo C. The Keystone Perforator Island Flap Con-cept. Sydney, Australia; Elsevier; 2012.)
Volume 130, Number 1 • Keystone Island Flap
39e
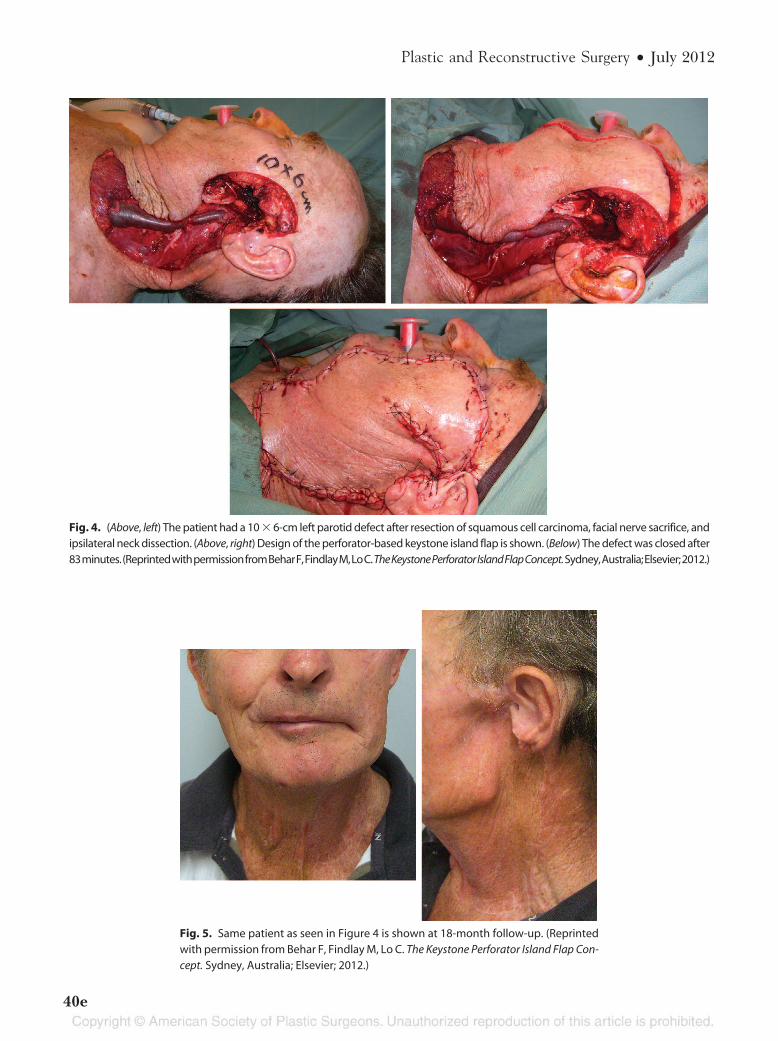
Fig. 4. (Above, left) The patient had a 10 � 6-cm left parotid defect after resection of squamous cell carcinoma, facial nerve sacrifice, andipsilateral neck dissection. (Above, right) Design of the perforator-based keystone island flap is shown. (Below) The defect was closed after83minutes.(ReprintedwithpermissionfromBeharF,FindlayM,LoC.TheKeystonePerforatorIslandFlapConcept.Sydney,Australia;Elsevier;2012.)
Fig. 5. Same patient as seen in Figure 4 is shown at 18-month follow-up. (Reprintedwith permission from Behar F, Findlay M, Lo C. The Keystone Perforator Island Flap Con-cept. Sydney, Australia; Elsevier; 2012.)
Plastic and Reconstructive Surgery • July 2012
40e

neck. In 1997, Ariyan reported seven cases oftransverse platysma flap and stated that the skinpaddle may be outlined across the midline of theneck.16 In 2003, two further cases were published,with the additional comment that the usable por-tion of the skin paddle does not extend beyondthe midline.17 There appeared to be concernsabout crossing the midline and, unfortunately, theillustrations published did not include frontalviews showing the distal tip of donor site. It is notuncommon for keystone island flaps to cross thesagittal midline, incorporating at least two andpossibly more than four vascular territories. Withno cases of total flap loss and a partial flap necrosisrate of 6 percent (four of 63), we hypothesize thatthe perforator-based island flap design augmentsvascular hemodynamics and flap survival.4,6
The use of keystone island flaps for parotid re-construction is subject to defect characteristics (e.g.,type of tissue loss, location, size) and the availabilityof adjacent donor tissue. As with any other locore-gional reconstructive technique, locoregional skinavailability is a prerequisite. Redundant skin in theelderly is certainly an advantage. The youngest pa-tient in our series was aged 31 years, with melanomaand a defect size of 6 � 4 cm. Patient assessment andpatient selection is key, and the reconstructive ap-proach for every patient must be individualized.
Neck dissections and previous radiotherapy ne-cessitate careful flap design but are certainly notcontraindications (Figs. 4 and 5). In contrast, thekeystone island flap is a reproducible, single-stagereconstructive option that is relatively easy and quick(Figs. 4 and 5) to perform without microsurgicalskills or equipment. Donor-site morbidity is minimal(often direct closure). Keystone island flaps providethin and pliable locoregional tissue and a good colormatch to the skin of the parotid region, and areoften preferred over microvascular transfers.
CONCLUSIONSThe reconstruction of parotid defects after re-
section of primary parotid tumors or secondarymetastases can be challenging. Keystone islandflaps present a single-stage reconstructive optionthat is relatively easy to perform without the needfor microvascular tissue transfer. From the seriespresented, it can be seen that reliable and repro-ducible results are achievable.
Cheng H. Lo, M.B.B.S.Department of Plastic and Reconstructive Surgery
Royal Melbourne HospitalGrattan Street
Parkville, Victoria 3050, [email protected]
PATIENT CONSENT
Written consent was obtained for use of the patientimages in Figure 2.
REFERENCES1. Saadeh PB, Delacure MD. Head and neck cancer and salivary
gland tumors. In: Thorne CH, Beasley RW, Aston SJ, BartlettSP, Gurtner GS, Spear SL, eds. Grabb & Smith’s Plastic Surgery.6th ed. Philadelphia: Wolters Kluwer/Lippincott Williams &Wilkins; 2007:333–346.
2. Cancer Council Australia and Australian Cancer Network.Basal Cell Carcinoma, Squamous Cell Carcinoma (and RelatedLesions): A Guide to Clinical Management in Australia. Sydney,New South Wales, Australia: Cancer Council Australia andAustralian Cancer Network; 2008.
3. Australian Cancer Network Melanoma Guidelines RevisionWorking Party. Clinical Practice Guidelines for the Managementof Melanoma in Australia and New Zealand. Wellington, NewZealand: Cancer Council Australia and Australian CancerNetwork, Sydney and New Zealand Guidelines Group; 2008.
4. Behan FC. The fasciocutaneous island flap: An extension ofthe angiotome concept. ANZ J Surg. 1992;62:874–886.
5. Behan FC. The keystone design perforator island flap inreconstructive surgery. ANZ J Surg. 2003;73:112–120.
6. Behan FC, Sizeland A, Porcedu S, Somia N, Wilson J. Key-stone island flap: An alternative reconstructive option to freeflaps in irradiated tissue. ANZ J Surg. 2006;76:407–413.
7. Behan FC, Sizeland A. Reiteration of core principles of thekeystone island flap. ANZ J Surg. 2006;76:1127–1134.
8. Behan FC, Sizeland A, Gilmour F, Hui A, Seel M, Lo CH. Useof the keystone island flap for advanced head and neckcancer in the elderly: A principle of amelioration. J PlastReconstr Aesthet Surg. 2010;63:739–745.
9. McGregor AD, McGregor IA. Fundamental Techniques of PlasticSurgery and Their Surgical Applications. 10th ed. New York:Churchill Livingstone; 2000.
10. Behan FC, Lo CH. Principles and misconceptions regardingthe keystone island flap. Ann Surg Oncol. 2009;16:1722–1723.
11. Behan FC, Lo CH, Shayan R. Perforator territory of thekeystone flap: Use of the dermatomal roadmap. J Plast Re-constr Aesthet Surg. 2009;62:551–553.
12. Behan FC, Wilson I. The vascular basis of laterally basedforehead island flaps, and their clinical applications. PlastReconstr J (European section, Madrid) 1973;24
13. Futrell JW, Johns ME, Edgerton MT, Cantrell RW, Fitz-HughGS. Platysma myocutaneous flap for intraoral reconstruc-tion. Am J Surg. 1978;136:504–507.
14. Mathes SJ, Nahai F. Reconstructive Surgery: Principles, Anatomy& Technique. New York: Churchill Livingstone; 1997.
15. Coleman JJ III, Jurkiewicz MJ, Nahai F, Mathes SJ. The plat-ysma musculocutaneous flap: Experience with 24 cases. PlastReconstr Surg. 1983;72:315–321.
16. Ariyan S. The transverse platysma myocutaneous flap for headand neck reconstruction. Plast Reconstr Surg. 1997;99:340–347.
17. Ariyan S. The transverse platysma myocutaneous flap forhead and neck reconstruction: An update. Plast Reconstr Surg.2003;111:378–380.
18. Szudek J, Taylor SM. Systematic review of the platysma myo-cutaneous flap for head and neck reconstruction. Arch Oto-laryngol Head Neck Surg. 2007;133:655–661.
Volume 130, Number 1 • Keystone Island Flap
41e