Embed Size (px)
Citation preview
Behavioral and Pharmacological Treatments for Smokers with Depression
Richard A. Brown, Ph.D.
Brown Medical SchoolButler Hospital, Providence, R.I.
Supported by grants from the National Institute on Drug Abuse (DA 08511 and DA 017332)
Cigarette Smoking and Depression
• Smoking and depression frequently co-occur in community and clinical samples:– Smokers exhibit higher rates of MDD and depressive sx– Lifetime MDD associated with increased smoking
prevalence in both men and women– Lifetime MDD higher among treated smokers (22-61%)
compared to general population (~17%)
Treatment of Smokers with Depressive Vulnerabilities:
Early Findings I
• Glassman and colleagues (1988), in a clinical trial of clonidine, found that 61% of sample (n=71) had past MDD– These past MDD smokers had significantly lower
abstinence rates than their non-past MDD counterparts
• Subsequent analyses of these data (Covey et al., 1990) for only placebo subjects revealed that past MDD smokers experienced greater depressed mood and concentration difficulties during nicotine withdrawal than non-past MDD smokers
Treatment of Smokers with Depressive Vulnerabilities:
Early Findings II
• Hall and colleagues (1990) found that 46% of their treatment sample (n=65) had past MDD
• These past MDD smokers had significantly higher scores on measures of anxiety, anger and depression than non-past MDD smokers– One week after quit date, past MDD subjects showed greater
increases in anger, confusion and depression than non-past MDD subjects
– Positive history of MDD predicted relapse to smoking for married subjects at six-month follow-up

Summary of Early Findings
• Early findings relating depression and smoking suggested that:– Smokers with past MDD constitute a significant
proportion of those who present for smoking cessation– Smokers with past MDD are less successful at smoking
cessation, due largely to increased depressed mood and depressive symptoms while attempting to quit
Later Findings of Past MDD and Smoking Outcomes
• Since Glassman et al (1988), results of studies examining the effects of lifetime MDD on smoking cessation have been decidedly mixed
• While some studies have found that past MDD to be associated with poorer smoking outcome in general (Glassman et al., 1993) and in women (Hall et al., 1998), other studies have not found an association between past MDD and smoking outcome (Hall et al., 1994; Ginsberg et al., 1995)

Past MDD and Elevated Depressive Symptoms
• Interestingly, past MDD smokers engaged in cessation have been shown to have elevated depressive symptoms compared to non-past MDD smokers (Keuthen et al., 2000; Niaura et al., 1999)
• Nonetheless, in both studies, positive history of MDD was not predictive of smoking cessation failure
Results of Meta-analysis
• A recent meta-analysis by Hitsman et al. (2003) revealed that, contrary to expectations, there were no overall differences in rates of smoking cessation between smokers who were positive and those who were negative for history of MDD
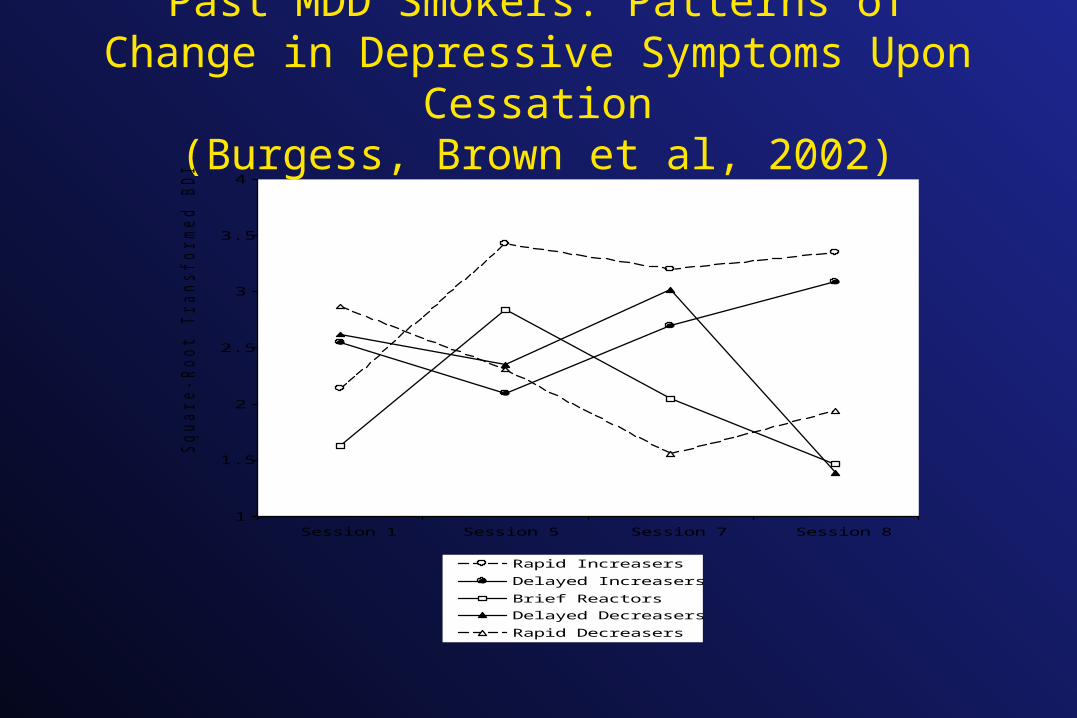
Past MDD Smokers: Patterns of Change in Depressive Symptoms Upon Cessation
(Burgess, Brown et al, 2002)
1
1.5
2
2.5
3
3.5
4
Session 1 Session 5 Session 7 Session 8
Sq
ua
re
-R
oo
t T
ra
nsfo
rm
ed
BD
I S
co
re
Rapid Increasers
Delayed Increasers
Brief Reactors
Delayed Decreasers
Rapid Decreasers
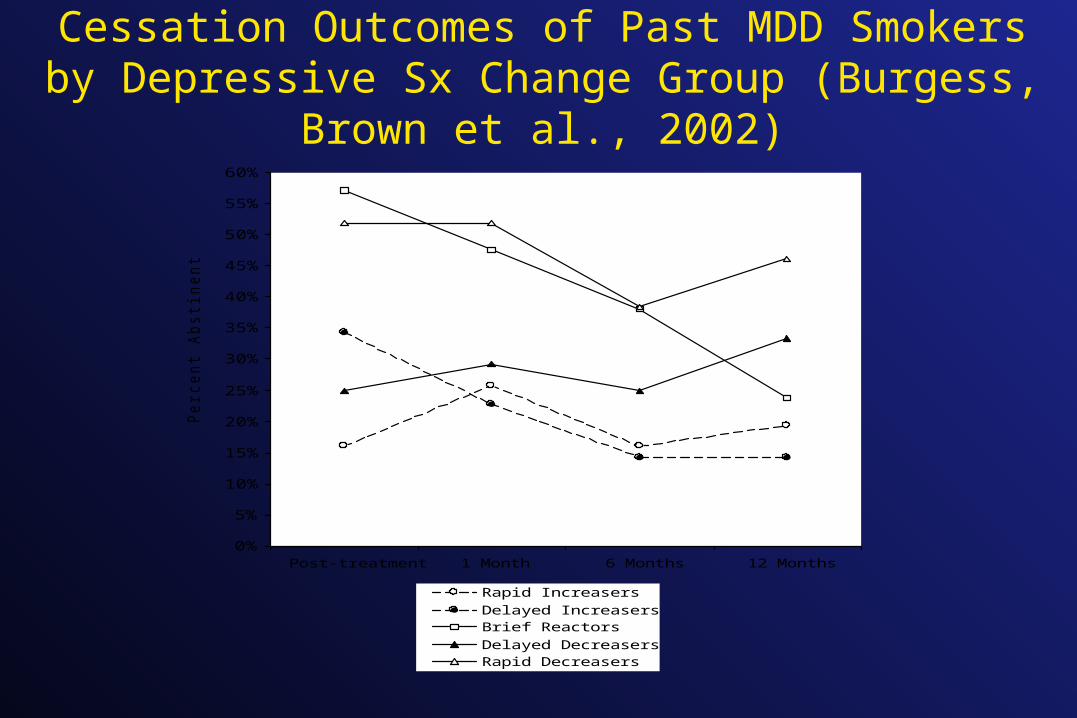
Cessation Outcomes of Past MDD Smokers by Depressive Sx Change Group (Burgess, Brown et al., 2002)
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
55%
60%
Post-treatment 1 Month 6 Months 12 Months
Pe
rce
nt A
bstin
en
t
Rapid IncreasersDelayed IncreasersBrief ReactorsDelayed DecreasersRapid Decreasers
Past MDD Smokers: Patterns of Change in Depressive Symptoms
• 40 % of past MDD smokers (n = 179) showed increasing depressive symptoms upon quitting
• 47% had a pattern of decreasing depressive symptoms upon quitting
• Increasing depressive symptoms were associated with recurrent (rather than single episode) past MDD and younger age of first MDD onset
Utility of Mood Coping Skills
The acquisition of skills for coping with depression and negative moods may be helpful for past MDD smokers to: • Prevent the onset of depressive symptoms upon
cessation from smoking, and
• Modify or improve their affect in potential negative
affect situations, which are the most common
precipitants of relapse
Findings from Treatment Outcome Studies: CBT Mood Management
• Three studies by Hall and colleagues have yielded mixed results
• In an initial study (Hall et al., 1994) in which subjects received nicotine gum, past MDD smokers in a 10-session mood management treatment achieved higher continuous abstinence than those in a standard 5-session treatment
• However, failure to equate for contact time limits the interpretation of the results
Hall and colleagues - Study 2
• In a second study using nicotine gum and placebo, Hall and colleagues (1996) equated for contact time (both interventions were 10 sessions) using a health education control that expanded the 5 session treatment used in the previous study
• Contrary to earlier findings, the mood management condition did not outperform the control among past MDD subjects
Hall and colleagues - Study 3
• Finally, Hall and colleagues (1998) completed a third study incorporating nortriptyline and placebo. In this study, the mood management condition again had greater contact time than the control (10 vs. 5 sessions).
• As in the first study, mood management was more effective in smokers with past MDD, but not for smokers without past MDD

Conclusions from the Mood Management Outcome Studies of Hall and Colleagues
• The results of these three studies suggest that smokers with past MDD benefit from more intensive behavioral treatment
• However, these results do not demonstrate the specific effects of mood management treatment with this subpopulation
Efficacy of CBT Depression Skills Treatment in Past MDD Smokers
• We compared the efficacy of standard smoking cessation treatment (ST) with that of ST combined with CBT for depression (CBT-D) in 179 smokers with past MDD (Brown et al., 2001)
• We utilized a sample of past MDD smokers in order to have adequate power to test main effects of treatment in this subpopulation
ST vs. CBT-D in Past MDD Smokers
• Subjects were 179 smokers with past MDD• Both treatment conditions provided eight, two-hour
sessions and were equated for participant and therapist contact time
• Smoking status was assessed and biochemically verified (CO and cotinine) at posttreatment, 1 month, 6 months and 12 months
• Completion rates at f/us were 95%, 91% and 92% respectively
Standard Treatment Components
• Self-monitoring of smoking behavior
• Self-management
• Nicotine fading
• Relapse prevention
• Social support

CBT-D Treatment Components
• Included all components of ST treatment, plus:• Daily mood rating• Increasing pleasant activities• Increasing positive - decreasing negative thoughts• ABC technique (also known as RET)• Social skills/assertiveness• Maintaining gains
Brown et al. (2001): Findings I
• Contrary to prediction, CBT-D did not produce significantly higher abstinence rates compared to ST in this sample of past MDD smokers
• This may have been, in part, because these past MDD smokers fared relatively well in nonpharmacologic standard treatment at 12 months (24.7% abstinence). This compared to 32.5% abstinence among those receiving CBT-D
Brown et al. (2001): Findings II
• However, in secondary analyses, past MDD smokers with recurrent MDD and who were heavy smokers (> 25 cigs/day) did significantly better with CBT-D than ST
• Recurrent MDD - 28.0% vs. 16.7% (p = .02) • Heavy smokers - 30.4% vs. 15.2% (p = .02)
Brown et al. (2001): Findings III
• In hierarchical GEE analysis, smokers with recurrent MDD were 2.30 (95% CI = 1.05-5.03) times more likely to abstain across follow-ups if they received CBT-D rather than ST
• Heavy smokers (> 25 cigarettes/day) were 2.62 (95% CI = 1.18-5.83) more likely to abstain across follow-up if they received CBT-D rather than ST

Smoking Outcomes by Depressive History
Availability of CBT-D Treatment Materials
• Brown, R.A. (2003). Comorbidity treatment: Skills training for coping with depression and negative moods. In Abrams, D.B., Niaura, R. S., Brown, R.A., Emmons, K.M., Goldstein, M.G., & Monti, P.M. (Eds.). The tobacco dependence treatment handbook: A guide to best practices. New York: Guilford Press
Single Episode (Past) vs. Recurrent MDD
• Findings from Brown et al. (2001) suggest that lifetime MDD, in and of itself, may not be a sufficiently robust predictor of poor prognosis in smoking cessation
• Findings of Covey et al. (1997) support the notion that any risk conveyed by past MDD may be attributable to those with recurrent rather than single episode past MDD
Recurrent MDD as Risk Factor - I
• Extrapolating from their data, the abstinence rates in Covey et al. (1997) were 29.3%, 31.3% and 13.4% respectively, among smokers with no history of MDD, one prior episode of MDD, and recurrent past episodes of MDD
Recurrent MDD as Risk Factor - II
• Subsequent analyses of pooled data from the three studies by Hall and colleagues support the finding that poor prognosis for smoking cessation treatment outcome is not conveyed in the main by a history of MDD, rather by a history of recurrent MDD (Hall et al., 2001)
• While there were no differences in outcomes for individuals with no or single episodes of MDD, smokers with recurrent MDD who received mood management were 2.43 times more likely to be abstinent at 12-month follow-up compared to recurrent MDD smokers in the control conditions

Revised Conclusions• The association between history of MDD and smoking
cessation failure is equivocal, at best. Rather, risk for cessation failure may be conveyed by recurrent, rather than single past episode MDD.
• Past MDD smokers are not a homogeneous group who experience an increase in depressive symptoms upon quitting smoking. Fewer than 50% of past MDD smokers may experience increased depressive symptoms upon quitting.
• Cognitive-behavioral mood management as a smoking cessation treatment may benefit smokers with recurrent past episodes of MDD.
Current Depressive Symptoms and Smoking Cessation Failure
• Accumulating evidence suggests that a more proximal indication of depression, current level of depressive symptoms, is reliably associated with smoking cessation failure
• Results from the National Health and Nutrition Examination Survey (NHANES) and the NHANES Follow-up Study are particularly impressive

NHANES Study Findings
• Cross-sectional analysis showed that, as the depressive symptoms [as assessed by the CES-D ] increased, the prevalence of smokers increased whereas the quit ratio decreased (Anda et al., 1990).
• Prospective analysis showed that depressed smokers (>16 on CES-D) were 40% less likely than nondepressed smokers to have quit after nine years.
• The results were independent of the effects of amount smoked, age, gender, and education. The results command attention because the sample was both large and representative of the US population.
Cessation Sample Findings of Effects of Depressive Symptoms on Cessation Failure• Results from smoking cessation samples support the
conclusion that risk for smoking cessation failure is conveyed by current level of depressive symptoms – Rausch et al. (1990)– Kinnunen et al. (1996)– Blondal et al. (1999)– Ludman et al. (2000)– Hanna et al. (1994)– Zuckerman et al. (1989)– Niaura et al. (2001)
Use of Antidepressants in Smoking Cessation
• Several drugs marketed as antidepressants have demonstrated efficacy for smoking cessation:– Sustained release bupropion (Zyban)– Nortriptyline– Fluoxetine
Fluoxetine in Smokers with Elevated Depressive Symptoms
• In contrast to bupropion and nortriptyline, fluoxetine has demonstrated only modest evidence of overall efficacy for smoking cessation (Niaura et al., 2002), but has been shown to provide specific smoking cessation benefits in smokers with elevated depressive symptoms.

Fluoxetine “Helps some cigarette smokers more than others”
• Hitsman et al. (1999) - randomized, double-blind, placebo-controlled trial of 253 adult smokers assigned to either fluoxetine or placebo for smoking cessation
• Four baseline risk factors were examined:
– High depressive sx
– High nicotine dependence
– Concern about weight gain
– Low self-efficacy
• Only one risk variable, high depressive symptoms, interacted with fluoxetine treatment in any of the analyses
Hitsman et al. (1999) Findings I
• In intention to treat analyses, a significant interaction of fluoxetine treatment and depressive symptoms was found, but only at 1 week after quit date. No main effects or interactions of any variables with fluoxetine treatment were evident at 1-, 3-, and 6-month follow-ups.
• However, in analyses examining treatment compliant participants, high depressive symptoms remained the only risk variable to evidence significant interactions with fluoxetine treatment, which were evident at the longer term, 1- and 3-month follow-ups. Follow-up data beyond 3-months was not available for treatment compliant participants.
Hitsman et al. (1999) Findings II
• These data suggest that some benefit may be realized by all high depressive symptom smokers treated with fluoxetine for smoking cessation, but that greater benefit is likely to accrue for those high depressive symptom smokers who are compliant and complete treatment.
Further Evidence for Fluoxetine
• Blondal et al. (1999) conducted a randomized, double-blind, placebo- controlled trial of nicotine inhaler and fluoxetine vs. nicotine inhaler and placebo in 100 adult smokers.
• The study found no overall advantage for either condition on smoking cessation outcomes, although confidence intervals were wide.
• However, the inhaler-fluoxetine group demonstrated increased abstinence rates among smokers with high baseline depressive symptoms (on the Beck Depression Inventory; BDI) compared to high BDI smokers in the inhaler-placebo condition.
Blondal et al. Findings
• High-BDI smokers in the inhaler-fluoxetine condition had 19% abstinence at one year follow-up compared to 7% among high-BDI smokers in the inhaler-placebo condition.
• The authors suggest that, in light of the fact that one-third of their study sample was high on depressive symptoms (BDI > 10), a study of sufficient power testing the efficacy of fluoxetine with this subgroup of smokers is warranted.

Evidence for Zyban in Past MDD Smokers
• Smith et al. (2003) examined the efficacy of bupropion sustained release (SR) and the nicotine patch for smoking cessation in subgroups of smokers at possible risk for relapse, from previously published clinical trial (n = 893) with four treatment conditions:– Placebo tablet + placebo patch– Placebo tablet + 21 mg/24-hr nicotine patch– 300 mg bupropion SR + placebo patch– 300 mg bupropion SR + 21 mg/24-hr nicotine patch
• In comparison to placebo tablet, bupropion SR approximately tripled 1-year non-smoking rates among women and previously depressed individuals
Conclusions about Antidepressants
• While bupropion and nortriptyline have demonstrated greater overall efficacy for smoking cessation, fluoxetine has been shown to provide specific smoking cessation benefits in smokers with elevated depressive symptoms.
• The strongest demonstration of this effect of fluoxetine in elevated depressive symptom smokers has been in combination with nicotine replacement therapy.
• There is also evidence of specific smoking cessation benefits for past MDD smokers with bupropion SR.
Summary I• Early findings suggested that lifetime MDD smokers
were more likely to experience increased depressive symptoms upon quitting smoking, and to fail at smoking cessation
• More recent findings suggest that this risk may be conveyed by having recurrent MDD rather than single past episode MDD
• The combination of CBT-D mood management skills and standard smoking cessation treatment appears to be efficacious for smokers with recurrent MDD

Summary II
• High levels of depressive symptoms may be the most reliable indicator of smoking cessation failure
• While bupropion and nortriptyline have demonstrated greater overall efficacy for smoking cessation, fluoxetine has been shown to provide specific smoking cessation benefits in smokers with elevated depressive symptoms, especially in combination with nicotine replacement therapy
• There is also evidence of specific smoking cessation benefits for past MDD smokers with bupropion SR





























