Embed Size (px)
Citation preview

Behavioral Decompensation in Behavioral Decompensation in Alzheimer’s DiseaseAlzheimer’s Disease
A Systematic and Multimodal A Systematic and Multimodal Approach to Patient ManagementApproach to Patient Management

Case StudyCase Study
► 81 y/o veteran longtime smoker w/ COPD, dx AD x 2 81 y/o veteran longtime smoker w/ COPD, dx AD x 2
yrs, recently dx w/ “inoperable” lung CA sent from NH yrs, recently dx w/ “inoperable” lung CA sent from NH
for control of combative behavior and hospice for control of combative behavior and hospice
consultation; pt lost 20# over past month, anorexic, consultation; pt lost 20# over past month, anorexic,
largely unresponsive.largely unresponsive.
► Rx includes 1,500mg divalproex, risperidone 0.5mg Rx includes 1,500mg divalproex, risperidone 0.5mg
qAM, 1mg qHS, recent addition of haloperidol 0.5mg IM qAM, 1mg qHS, recent addition of haloperidol 0.5mg IM
TID to allow for care administration…TID to allow for care administration…

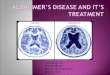
Peak Frequency ofPeak Frequency ofBehavioral Symptoms as AD ProgressesBehavioral Symptoms as AD Progresses
Jost BC, Grossberg GT. J Am Geriatr Soc. 1996; 44:1078-1081
Months Before/After Diagnosis
-40 -30 -20 -10 0 10 20 30
Fre
qu
en
cy (
% o
f P
atie
nts
) 100
80
60
40
20
0
Agitation
DiurnalRhythm
Irritability
WanderingAggression
HallucinationsMood
ChangeSociallyUnacc.
DelusionsSexually Inappropriate
AccusatorySuicidalIdeation
Paranoia
Depression
Anxiety
SocialWithdrawal

““DOCTOR, WE’VE GOT A PROBLEM...”DOCTOR, WE’VE GOT A PROBLEM...”
IT’S OVER!IT’S OVER!

Keys To Evaluation Of BehavioralKeys To Evaluation Of BehavioralProblems In DementiaProblems In Dementia
IIdentify the problem behavior dentify the problem behavior (WHAT)(WHAT)
TTiming / frequency of the behavior iming / frequency of the behavior (WHEN)(WHEN)
SSurroundings / environment urroundings / environment (WHERE)(WHERE)
OOthers involved? thers involved? (WITH WHOM)(WITH WHOM)
VVery troubling / dangerous?ery troubling / dangerous?
EEvaluation: physical & cognitive statusvaluation: physical & cognitive status
RRecommendationsecommendations
IIdentify the problem behavior dentify the problem behavior (WHAT)(WHAT)
TTiming / frequency of the behavior iming / frequency of the behavior (WHEN)(WHEN)
SSurroundings / environment urroundings / environment (WHERE)(WHERE)
OOthers involved? thers involved? (WITH WHOM)(WITH WHOM)
VVery troubling / dangerous?ery troubling / dangerous?
EEvaluation: physical & cognitive statusvaluation: physical & cognitive status
RRecommendationsecommendations
Gray KF. Clin Geriatr Med. 2004(Feb);20(1):69-82

The Delicate Balance of ClinicalThe Delicate Balance of ClinicalDecision-makingDecision-making
RISKSRISKSBENEFITSBENEFITS

Behavioral and Psychological Behavioral and Psychological Symptoms in Dementia: BPSDSymptoms in Dementia: BPSD
► General descriptive term for heterogeneous General descriptive term for heterogeneous group of non-cognitive symptoms & behaviors group of non-cognitive symptoms & behaviors occurring in dementiaoccurring in dementia
► Symptom Clusters within BPSD include:Symptom Clusters within BPSD include: Depressive 20% - 40%Depressive 20% - 40% Psychotic 30% - 40%Psychotic 30% - 40% Agitation/aggressive 50% - 80%Agitation/aggressive 50% - 80%
B. A. Lawlor. J.Clin.Psychiatry 65 Suppl 11:5-10, 2004

Criteria Criteria forfor Depression Depression ofof Alzheimer’s DiseaseAlzheimer’s Disease
A. (Need 3 or more over 2 wks...)►Depressed mood and/orDepressed mood and/or►Decreased positive affect or pleasureDecreased positive affect or pleasure
● Appetite disruptionAppetite disruption● Sleep disruptionSleep disruption● Psychomotor retardation / agitationPsychomotor retardation / agitation● IrritabilityIrritability● Fatigue or loss of energyFatigue or loss of energy● Worthlessness, hopelessness, guiltWorthlessness, hopelessness, guilt● Thoughts of death or suicidal ideationThoughts of death or suicidal ideation
B. B. All criteria met for dx of ADAll criteria met for dx of AD
C. Sx cause clinically significant distress or disruption C. Sx cause clinically significant distress or disruption in fxnin fxn
J. T. Olin, et al. Am.J.Geriatr.Psych 10(2):125-128, 2002P. B. Rosenberg, et al. Int.J.Geriatr.Psychiatry 20 (2):119-127, 2005

TREAT Depression ofTREAT Depression ofAlzheimer’s Disease!Alzheimer’s Disease!
BENEFITSBENEFITS
RISKSRISKS
► Rx Mood, anxiety► Rx Sleep?► Rx agitation?

AAN Practice Parameters 2001AAN Practice Parameters 2001Guideline-Reaffirmed 10/18/2003Guideline-Reaffirmed 10/18/2003
AAN practice parameters support the use AAN practice parameters support the use
of first-line nonpharmacologic strategies of first-line nonpharmacologic strategies
for agitation, especially when identifiable for agitation, especially when identifiable
causes such as pain or environmental causes such as pain or environmental
triggers are responsibletriggers are responsible
Doody RS, Stevens JC, Beck C, et al. Neurology. 2001(May 8);56(9):1154-1166

Principles ofPrinciples ofNonpharmacologic ManagementNonpharmacologic Management
► SafetySafety Control risk: physical, financial, drivingControl risk: physical, financial, driving
► SerenitySerenity Manage affects: avoid overt frustration and Manage affects: avoid overt frustration and
angeranger► StructureStructure
Increase organization: maintain schedules, Increase organization: maintain schedules, facilitate good habitsfacilitate good habits
► SanitySanity Reduce caregiver strain: seek social support, Reduce caregiver strain: seek social support,
use respite services use respite services
Gray KF. Clin Geriatr Med. 2004(Feb);20(1):69-82

► Educational programs should be offered to family Educational programs should be offered to family caregivers to improve caregiver satisfaction and to caregivers to improve caregiver satisfaction and to delay the time to NH placement (Guideline).delay the time to NH placement (Guideline).
► Staff of long-term care facilities should also be Staff of long-term care facilities should also be educated about AD to minimize the unnecessary use of educated about AD to minimize the unnecessary use of antipsychotic medications (Guideline).antipsychotic medications (Guideline).
► Behavior modification, scheduled toileting, and Behavior modification, scheduled toileting, and prompted voiding reduce urinary incontinence prompted voiding reduce urinary incontinence (Standard).(Standard).
► Functional independence can be increased by graded Functional independence can be increased by graded assistance, skills practice, and positive reinforcement assistance, skills practice, and positive reinforcement (Guideline). (Guideline).
R. S. Doody, et al. Neurology 56 (9):1154-1166, 2001
AAN Practice Parameters 2001AAN Practice Parameters 2001Guideline-Reaffirmed 10/18/2003Guideline-Reaffirmed 10/18/2003

Medication Considerations Medication Considerations ForFor
Non-urgent/Emergent “Agitation”Non-urgent/Emergent “Agitation”
BENEFITSBENEFITS
RISKSRISKS
CholinesteraseCholinesteraseInhibitorsInhibitors
andandMemantineMemantine

NPI Scores Following Treatment with NPI Scores Following Treatment with Different ChEIsDifferent ChEIs
–3
–2
–1
0
1
2
3
Mea
n c
han
ge
fro
m b
asel
ine
N = 106 N = 106N = 103
N = 103
N = 98
Imp
rove
men
t
Pla
ceb
o
24 m
g/d
ay
Pla
ceb
o
10 m
g/d
Op
en-l
abel
3–12
mg
/d
MMSE = 14.4 MMSE = 11.8 MMSE 12 MMSE = 9.2 MMSE = 10.8NPI-121 NPI-122 NPI-103 NPI-124 NPI-125
Nursing Community/ Community Nursing Nursing home assisted living home home
1Tariot et al., 2001; 2Feldman et al., 2001; 3Wilkinson et al., 2002; 4Cummings et al., 2000; 5Bullock et al., 2001; Cummings, et al., 2004
Pla
ceb
o
10 m
g/d
N = 125 N = 119
Baseline
N = 113
Op
en-l
abel
3–12
mg
/d
GalantamineAricept Rivastigmine
Mean Change Per Item After ~ 6 Months in Five StudiesMean Change Per Item After ~ 6 Months in Five StudiesMean Change Per Item After ~ 6 Months in Five StudiesMean Change Per Item After ~ 6 Months in Five Studies

Impact of Galantamine on Behavioral Impact of Galantamine on Behavioral SymptomsSymptoms
Efficacy measureEfficacy measure Galantamine Galantamine (N = 1,327)(N = 1,327)
Placebo Placebo (N = 686)(N = 686) PP
Individual NPI domain scoresIndividual NPI domain scores
DelusionsDelusions -0.04 (2.43)-0.04 (2.43) 0.19 (2.23)0.19 (2.23) 0.100.10
HallucinationsHallucinations -0.02 (1.58)-0.02 (1.58) 0.07 (1.24)0.07 (1.24) 0.0680.068
Agitation/aggressionAgitation/aggression 0.10 (2.64)0.10 (2.64) 0.27 (2.30)**0.27 (2.30)** 0.050*0.050*
Depression/dysphoriaDepression/dysphoria 0.11 (2.40)0.11 (2.40) 0.13 (2.26)0.13 (2.26) 0.970.97
AnxietyAnxiety -0.05 (2.66)-0.05 (2.66) 0.19 (2.48)0.19 (2.48) 0.044*0.044*
Elation/euphoria 0.01 (0.96) 0.00 (1.02) 0.86
Apathy/indifference -0.22 (3.25)** -0.13 (3.21) 0.28
DisinhibitionDisinhibition 0.00 (1.61)0.00 (1.61) 0.09 (1.33)0.09 (1.33) 0.020*0.020*
Irritability/labilityIrritability/lability 0.12 (2.60)0.12 (2.60) 0.20 (2.36)*0.20 (2.36)* 0.710.71
Aberrant motor behaviorAberrant motor behavior -0.15 (2.96)-0.15 (2.96) 0.12 (2.91)0.12 (2.91) 0.050*0.050*
a Effect size: difference in mean change scores (galantamine minus placebo) divided by the pooled within-group SD (Cohens’s ).*p <.05 for between-group comparisons (Val Elteren test, df: 1).** <.05 for within-group comparisons (Wilcoxon signed-rank tests).
N. Herrmann, et al. Am.J.Geriatr.Psychiatry 13 (6):527-534, 2005

Memantine in Moderate to SevereMemantine in Moderate to SevereAD Study: Impact on Behavior - NPIAD Study: Impact on Behavior - NPI
At End PointAt End Point
► There was no statistically significant difference There was no statistically significant difference between the 2 groups for total NPI scoresbetween the 2 groups for total NPI scores
► There was a statistically significant difference There was a statistically significant difference between the treatment groupsbetween the treatment groupsin favor of memantine in the following domainsin favor of memantine in the following domains
Delusions Delusions P = .0386* P = .0386*
Agitation/aggressionAgitation/aggression P = .0083*4 P = .0083*4
*LOCF analysis. Sources: Reisberg B, et al. N Engl J Med. 2003;348:1333-1341. Data on file, Forest Laboratories, Inc.

*
Memantine + Donepezil in Moderate toMemantine + Donepezil in Moderate toSevere AD Study: Impact on BehaviorSevere AD Study: Impact on Behavior
*
P=.002 P=.001
Mea
n C
han
ge
Fro
m B
asel
ine
NPI BGP-Care
Wo
rsenin
gIm
pro
vemen
tMemantine + Donepezil Treatment Associated With
Superior Outcomes in Key AD Domains
*LOCF analysis. Bars indicate 95% confidence intervals. Source: Tariot P, et al. JAMA. 2004;291:317-324.
-1.5-1.0-0.50.00.51.01.52.02.53.03.54.04.55.0
Memantine+Donepezil Placebo+Donepezil

AAN Practice Parameters 2001AAN Practice Parameters 2001(Reaffirmed 10-18-03)(Reaffirmed 10-18-03)
► Treat agitation, psychosis and Treat agitation, psychosis and depressiondepression The patient's paranoia, suspiciousness, The patient's paranoia, suspiciousness,
combativeness or resistance to maintaining combativeness or resistance to maintaining personal hygiene can seem overwhelming to personal hygiene can seem overwhelming to families and caregivers and significantly families and caregivers and significantly impact quality of life. Evidence indicates that impact quality of life. Evidence indicates that several strategies can decrease problem several strategies can decrease problem behaviors. behaviors. If environmental manipulation failsIf environmental manipulation fails to eliminate agitation or psychosis, use to eliminate agitation or psychosis, use antipsychoticsantipsychotics……
R. S. Doody, et al. Neurology 56 (9):1154-1166, 2001 Full guidelines available at www.aan.com

Diagnostic Criteria forDiagnostic Criteria forPsychosis of ADPsychosis of AD
► Diagnosis of Alzheimer’s dementiaDiagnosis of Alzheimer’s dementia
► Exclusion of schizophrenia or other causes of Exclusion of schizophrenia or other causes of psychotic symptomspsychotic symptoms
► Hallucinations and/or delusionsHallucinations and/or delusions
Late-onsetLate-onset
Present intermittently for Present intermittently for 1 month1 month
Disruptive to patient functioningDisruptive to patient functioning
► Associated agitation, negative symptoms, and Associated agitation, negative symptoms, and depressiondepression
► Disturbances do not correlate exclusively with deliriumDisturbances do not correlate exclusively with delirium
D. V. Jeste and S. I. Finkel. Am.J.Geriatr.Psychiatry 8 (1):29-34, 2000
L. S. Schneider, et al. Am.J.Geriatr.Psychiatry 11 (4):414-425, 2003

ANTIPSYCHOTIC USE ANTIPSYCHOTIC USE FOR “AGITATION”FOR “AGITATION”
RISKS ?RISKS ?
BENEFITS ?BENEFITS ?
► Persistent DANGER Persistent DANGER to self or others?to self or others?
► Behaviors impair Behaviors impair function?function?
C. Ballard and J. Cream. Int.Psychogeriatr. 17 (1):4-12, 2005

The Delicate Balance of ClinicalThe Delicate Balance of ClinicalDecision-makingDecision-making
RISKSRISKSBENEFITSBENEFITS

Antipsychotic DocumentationAntipsychotic Documentation
► Severity of symptomsSeverity of symptoms
► Danger to patient and othersDanger to patient and others
► Lack of response to alternative approachesLack of response to alternative approaches
► Awareness of risks of treatmentAwareness of risks of treatment
► Judgment that potential benefits outweigh risksJudgment that potential benefits outweigh risks Previous benefit?Previous benefit? Previous tolerability?Previous tolerability?
► Discussion with familyDiscussion with family
► Monitoring planMonitoring plan
► Plan for dose reduction when stablePlan for dose reduction when stable

Atypical Antipsychotic Treatment for Psychosis & Atypical Antipsychotic Treatment for Psychosis & Dangerous Behavioral Dyscontrol in Dementia:Dangerous Behavioral Dyscontrol in Dementia:
► Olanzapine 2.5 – 10 mg, oral “loading” pts in Olanzapine 2.5 – 10 mg, oral “loading” pts in
urgent settings [15-20 mg 1st 24 hr]; IM*urgent settings [15-20 mg 1st 24 hr]; IM*
► Risperidone 0.5 – 2 mg, caution w/ doses > 1 mgRisperidone 0.5 – 2 mg, caution w/ doses > 1 mg‡‡
► Quetiapine 25-150 mg, especially w/ Quetiapine 25-150 mg, especially w/
parkinsonism, Lewy Body Dementiaparkinsonism, Lewy Body Dementia††
► Aripiprazole 5-10 mg, non-urgent useAripiprazole 5-10 mg, non-urgent use§§
► Ziprasidone 20-60 mg BID, emerging option; IMZiprasidone 20-60 mg BID, emerging option; IM¶¶
*J. S. Street et al. Arch Gen Psychiatry. 2000;57(10):968-976; and R. W. Baker et al. J Clin Psychopharmacol. 2003;23(4):342-348; ‡I. R. Katz et al. J Clin Psychiatry. 1999;60(2):107-115 and P. P. de Deyn et al. Clin Neurol Neurosurg. 2005; †P. N. Tariot and M. S. Ismail. J Clin Psychiatry. 2002;63 suppl 13:21-26; §De Deyn et al. AAGP 16th Annual Meeting, 2003; ¶A. Berkowitz. J Psychiatric Practice. 2003;9(6) 469-473

Efficacy Efficacy andand Adverse Effects Adverse Effects ofof Atypical Atypical Antipsychotics Antipsychotics forfor Dementia: Dementia:
Meta-analysis Meta-analysis ofof Randomized, Placebo-controlled Trials Randomized, Placebo-controlled Trials
► Efficacy on rating scales was observed by meta-Efficacy on rating scales was observed by meta-analysis for aripiprazole and risperidone, but not for analysis for aripiprazole and risperidone, but not for olanzapineolanzapine
► There were smaller effects for less severe dementia, There were smaller effects for less severe dementia, outpatients, and patients selected for psychosisoutpatients, and patients selected for psychosis
► Approx 1/3 dropped out w/o overall differences Approx 1/3 dropped out w/o overall differences between Rx & placebobetween Rx & placebo
► Adverse events mainly somnolence & UTI or Adverse events mainly somnolence & UTI or incontinence across Rx, and EPS or abnormal gait incontinence across Rx, and EPS or abnormal gait with risperidone or olanzapinewith risperidone or olanzapine
L. S. Schneider, et al. Am.J Geriatr.Psychiatry 14 (3):191-210, 2006

Efficacy Efficacy andand Adverse Effects Adverse Effects ofof Atypical Atypical
Antipsychotics Antipsychotics forfor Dementia: Dementia: (con’t)(con’t) Meta-analysis Meta-analysis ofof Randomized, Placebo-controlled Trials Randomized, Placebo-controlled Trials
► Cognitive test scores worsened with drugsCognitive test scores worsened with drugs
► There was no evidence for increased injury, falls, There was no evidence for increased injury, falls, or syncopeor syncope
► Significant risk for cerebrovascular events, Significant risk for cerebrovascular events, especially with risperidoneespecially with risperidone
► Increased risk for death overall was reported Increased risk for death overall was reported elsewhereelsewhere
► The modest efficacy and uncertain response The modest efficacy and uncertain response
rates combined with the risks detailed here rates combined with the risks detailed here
suggest that antipsychotics should be used with suggest that antipsychotics should be used with
more deliberate considerationmore deliberate considerationL. S. Schneider, et al. Am.J Geriatr.Psychiatry 14 (3):191-210, 2006

Antipsychotic EquivalenciesAntipsychotic EquivalenciesBased On D2 Receptor Occupancy & Expert Based On D2 Receptor Occupancy & Expert
Consensus GuidelinesConsensus Guidelines
► Quetiapine Quetiapine = 300-400 mg= 300-400 mg
► Chlorpromazine Chlorpromazine = 100 mg= 100 mg
► Ziprasidone Ziprasidone »» 80 mg 80 mg
► AripiprazoleAripiprazole = 10 mg= 10 mg
► LoxapineLoxapine = 15 mg= 15 mg
► Olanzapine Olanzapine = 10 mg= 10 mg
► Risperidone Risperidone = 2.5 mg= 2.5 mg
► Haloperidol Haloperidol = 2 mg= 2 mg
Kane et al. J Clin Psychiatry. 2003;64 (suppl 12):5-19;Kapur et al. Am J Psychiatry. 2001;158(3):360-369Schotte et al. Psychopharmacology (Berl).1996;124 (1-2):57-73

Non-neuroleptic OptionsNon-neuroleptic OptionsFor “Agitation” ??For “Agitation” ??
““BENEFITS”BENEFITS”
RISKSRISKS
LIMITED PROOF OF EFFICACY
K. M. Sink, et al. JAMA 293 (5):596-608, 2005

Alternative RxAlternative Rx FORFOR “Agitation”“Agitation”
► SSRI REDUCE IRRITABILITY: non-psychotic pts, SSRI REDUCE IRRITABILITY: non-psychotic pts,
psychosis?psychosis?
► TRAZODONE (25-50 mg BID-TID) during day, qHSTRAZODONE (25-50 mg BID-TID) during day, qHS
► BUSPIRONE (10-60 mg/day): may take 2-4 wksBUSPIRONE (10-60 mg/day): may take 2-4 wks
► DIVALPROEX, CARBAMAZEPINE, GABAPENTINDIVALPROEX, CARBAMAZEPINE, GABAPENTIN
► ADJUNCTIVE BENZODIAZEPINESADJUNCTIVE BENZODIAZEPINES
► HORMONES for SEXUAL AGGRESSION: HORMONES for SEXUAL AGGRESSION:
(medroxyprogesterone acetate 150 mg IM q4wks)(medroxyprogesterone acetate 150 mg IM q4wks)
Gray KF. Clin Geriatr Med. 2004(Feb);20(1):69-82

Behavioral Decompensation in ADBehavioral Decompensation in AD
► Medications do not work aloneMedications do not work alone
► Fewer expectations late in dayFewer expectations late in day
► Distract with tasks or foodDistract with tasks or food
► Remind and assist; don’t take over!Remind and assist; don’t take over!
► Be willing to compromiseBe willing to compromise
► Back off and let patient relax; redirect Back off and let patient relax; redirect as appropriateas appropriate
► ““They can’t resist if you don’t insist”They can’t resist if you don’t insist”
Last Words for CaregiversLast Words for Caregivers