Embed Size (px)
Citation preview

Behavioral Health Integration: Whole Person Care Conference
January 27, 2017
Kathy Bradley, MD, MPHSenior Investigator Group Health Research Institute
Affiliate Professor Medicine &Health Services,
University of Washington
Research Associate VA Puget Sound HSR&D1

2
My Background
Primary care general internist
VA Women’s Health – 1995-2000
Population-based alcohol screening in VA
VA mental health integration (2002-2011)
3 models: Co-located, collaborative
care, behavioral health lab
Group Heath Behavioral Health
Integration (2014- present)
Research: collaborative care for alcohol
and opioid use disorders (2010 - present)

3
Outline?
1. What is Behavioral Health Integration?
2. Evidence
3. Group Heath lessons learned
4. Road Map : how to get there:
Understanding current situation
People
Systems

What is Behavioral Health
Integration?
4

Behavioral Health Integration?
5

6
What is Behavioral Health Integration?
Three types of integration…
Primary care (PC) teams offering
behavioral health (BH) services
BH teams offering PC
PC teams and BH teams caring for
patients together: coordination
http://www/Breecollaborative.org
http://www.hca.wa.gov/about-hca/healthier-washington/medicaid-
transformation

What is Behavioral Health Integration?
7
PC

What is Behavioral Health Integration?
8
BH
PC
What is Behavioral Health Integration?
9
BH
PC

Medical HomeAdvanced Primary Care

Elements of the Medical Home
Care Goals and Plan
Medication management
Self-management support
Preventive Care
Monitoring
Care management
Care Coordination

EvidenceBH care in PC settings
12

Depression and Suicide
13

14
Evidence - Depression
Depression Screening
Recommended by USPSTF
Adolescent & adults
Brief screen - PHQ-2
Siu JAMA 2016http://www.healthdisparities.net/hdc/hdcsearch/isysquery/8
d60cd76-98e9-47b4-b0a0-755dc6ddb7ef/9/doc/

15
Evidence - Depression
Depression measurement-based care
Depression assessment: PHQ-9
10-14 – optional
15-19 medications or therapy
20+ medication and therapy
Monitor
Goal decrease by 50%
Katon NEJM 2010; Unutzer JAMA 2006
http://aims.uw.eduhttp://psychnews.psychiatryonline.org/doi/full/10.1176/appi.pn.2016.9a11

16
Evidence - Depression
Collaborative Care
Care manager, coordination
Self management support
Measurement based care
Track patients supported by registry
Check-in 1-2 weeks re: side effects
Monitor response
Improves outcomes
Reimbursed by CMS: ~ 159$ per
patient per month??Katon NEJM 2010; Unutzer JAMA 2006
http://aims.uw.eduhttp://psychnews.psychiatryonline.org/doi/full/10.1176/appi.pn.2016.9a11

Evidence - DepressionCollaborative Care Management
Unutzer Am J Managed Care 2008

18
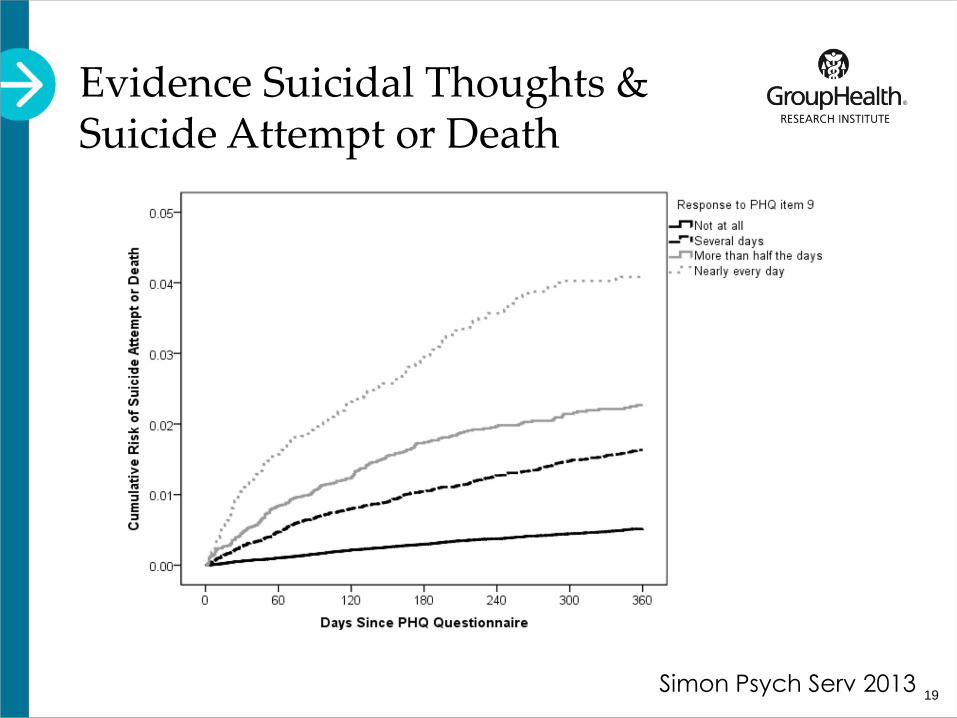
Evidence - Depression
Suicide risk assessment
PHQ-9 depression screen
In the past 2 weeks how often…
Question #9: …thoughts that you
would be better off dead, or of hurting
yourself in some way
“More than half the days” (2-3 points)
19
Evidence Suicidal Thoughts & Suicide Attempt or Death
Simon Psych Serv 2013
20
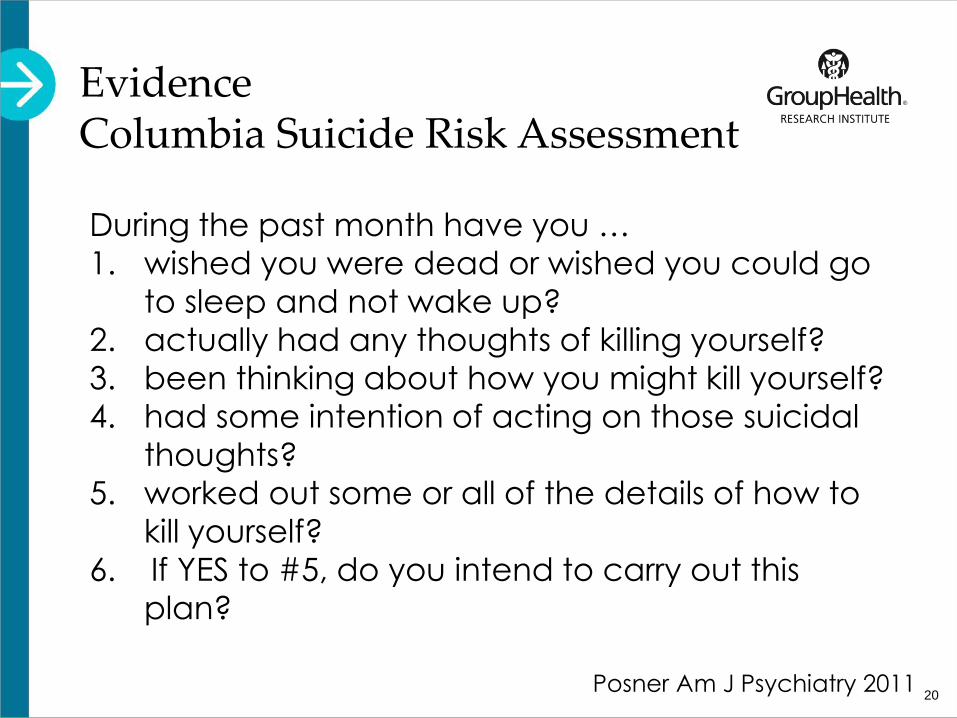
EvidenceColumbia Suicide Risk Assessment
During the past month have you …
1. wished you were dead or wished you could go
to sleep and not wake up?
2. actually had any thoughts of killing yourself?
3. been thinking about how you might kill yourself?
4. had some intention of acting on those suicidal
thoughts?
5. worked out some or all of the details of how to
kill yourself?
6. If YES to #5, do you intend to carry out this
plan?
Posner Am J Psychiatry 2011

21
EvidenceColumbia Suicide Risk Assessment
During the past month have you …
1. wished you were dead or wished you could go
to sleep and not wake up?
2. actually had any thoughts of killing yourself?
3. been thinking about how you might kill yourself?
4. had some intention of acting on those suicidal
thoughts?
5. worked out some or all of the details of how to
kill yourself?
6. If YES to #5, do you intend to carry out this
plan?
Posner Am J Psychiatry 2011

Story #1Uncontrolled diabetes in an
older woman:
22

Story #1Uncontrolled diabetes in an
older woman:
23
Out of control diabetes
HA1C 14.1
Non-adherent; not engaged in self care
No history of mental health conditions
Behavioral Health Integration:
24
PHQ-9 score 24
PHQ-9 Question #9: 2
Suicide Risk Assessment: 5
Did not “look depressed”

Substance Use and Addiction
25

26
Evidence – Substance UsePreventive Alcohol Screening
Substance Use - Prevention
Alcohol screening and brief preventive
counseling (USPSTF)
3rd highest prevention priority
Screens: AUDIT-C or single item
Advice re recommended limits and link
drinking to health
Jonas Ann Intern Med 2012; Moyer Ann Intern Med 2013
Solberg Am J Prev Med 2008
Fleming JAMA 1997, Alcohol Clin Exper Res 2002

Evidence – Substance UsePreventive Alcohol Screening
Outcomes
Decreased ED & hospital use
Savings 1st year: $522/patient
Savings 4 years: for each $1 spent on SBI:
$4.30 saved on inpatient & ED
$39.00 saved from societal perspective
Fleming, JAMA, 1997; Fleming 2000;
Fleming, ACER, 2002; Mundt 2006
27

28
Evidence – Substance Use
Substance Use Disorder Medications
Alcohol use disorders (AUDs):
Naltrexone,
Acamprosate,
Disulfiram
Opioid Use Disorders (OUDs):
Buprenorphine
Injectable naltrexone
Jonas JAMA 2014; Bradley & Kivlahan JAMA 2014
Mattick Cochrane Reviews 2008 and 2009

29
Evidence – Substance Use
Substance Use care management
Medications for AUD vs referral to
treatment
5 fold increased engagement
Decreased heavy drinking
Jonas JAMA 2014; Bradley & Kivlahan JAMA 2014
Oslin JGIM 2014

Alcohol Care Management vsReferral to Treatment
0
10
20
30
40
50
60
Perc
en
t d
ays o
f h
eavy d
rin
kin
g
Alcohol CareManagement
Specialty Addictioncare
Oslin JGIM 2014; Combine Manual

31
Evidence – Substance Use
Substance Use care management
Medications for AUD
Medications for OUDs
Access: 100-125 patients/RN
67% retention at 12 months
PCPs: most satisfying patients
Jonas JAMA 2014; Bradley & Kivlahan JAMA 2014
Alford Arch Intern Med 2011; Korthuis Ann Intern Med 2016

Why Medication Treatment of OUDs is Critical
Long-term OUD treatment with medications,
compared to non-medication treatment
improves outcomes including
Marked improvements in quality of life
Decreases relapse
Increased survival
Decreases acute care (ED & hospital)
Often decreases total health care costs
Lo-Ciganic Addiction 2015, Murphy Pharmaco economics, 2016
Clark Health Affairs 201132

Story #2Uncontrolled diabetes in
older man
33

Story #2Uncontrolled diabetes in
older man
34
Previous lower extremity amputation
Diabetes out of control
Foot ulcer
RN seeing weekly

Story #2Uncontrolled diabetes and
foot ulcer in older man
35
AUDIT-C score 10
Symptoms alcohol use disorder: 6
Pint of vodka a day +
Wanted help

How to Get from Here to There?
36

How to Get from Here to There?
Example: Group Heath’s Behavioral Health
Integration
37

38
Goals
Screening & assessment – routine
All patients, every year
Prevention
Treatment
Depression
Substance use disorders
Monitoring – measurement-based care
Severity at baseline & over time

Example Group Heath
39
Screen
Assess
Shared decision
making & treatment
Monitor and
Adapt

40
Strategies
Leadership support – BH Service
Evidence-based care
Design with front line staff
Simple systems
EHR support
Local implementation team & champions
Supported by coach (weekly)
Social workers trained in outreach and
engagement for addiction first

Barriers
41

Barriers… Time

Barriers… Lack of Buy-in
“No Thursday is out.
How about never—is never good for you?”

Barriers… Attitudes
You
Want
Me
To
Do
What
????

45
Lack of
“Shared
Meaning”
Barriers… Inadequate Communication

46
Friday afternoon “disasters”
Suicidal patients
“Detox”
Barriers…

What Helps?
47

What Helps? Teamwork



What Helps? Taking Time and Talking

Tell and Use Stories

What Helps?Pick a Goal; Take the Leap

What Helps? Trial and Error

Solve for worst case scenarios first56
What Helps? Resilience

Roadmap
57

Step 1Environmental Scan

59
Road Map – Step 1
1. Environmental scan:
Assess current state of care system
Who: all stakeholders
What: ideally visit each others worlds,
ask about care organization, observe
and listen
Identify gaps in quality of care
Summarize findings
Bring results to stakeholder meetings

60
Road Map – Step 2
2. People - identify team
All stakeholders
Why you are there
All voices heard
Take turns leading meeting
61
Road Map – Step 3
3. Pick a goal to start on …
Screening & assessment – routine?
Treatment – add substance use disorders?
Monitoring – measurement-based care?

62
Road Map – Step 3
3. Pick a goal to start on …
Screening & assessment – routine?
Treatment – add substance use disorders?
Monitoring – measurement-based care?
Crisis management
Suicidal patients
Patients wanting “detox”

63
Road Map – Step 4
4. Quality Improvement systems
Regular meetings
Change goal
Pilot test, adapt, repeat
Measure progress
Make meetings effective
Healthier Washington medicaid transformation project toolkit draft
for public comment January 2017

64
SummaryBehavioral Health Integration
Change in way we think about PC & BH
Strong evidence
Apply medical home concepts
One step at a time
Its possible!

Thank You!
65

Questions & Discussion
Acknowledgements
CHOICE Trial -– NIAAA- R01 AA018702
SPARC Trial – AHRQ – R18HS023173
3:30 Project – GH Partnership for Innovation
Options Study – NIAAA – R21 AA023037
Mentoring Award – NIAAA – K24AA022128
Clinical Trials Network – NIDA – 5UG1DA040314
Health Systems Node
Screening for marijuana and drugs
PROUD Trial Phase 1
Group Health Behavioral Health Service
GH Development Fund – Mike Evans video
Resources
http://www/Breecollaborative.org
Youtube: https://youtu.be/tbKbq2IytC4
Healthier Washington medicaid transformation
project toolkit draft for public comment January
2017
Thursdays at noon: Webinar - UW psychiatry
case reviews for primary care