Embed Size (px)
Citation preview
REPORT TO THE EMCDDAby the Reitox National Focal Point
“BELGIUM”DRUG SITUATION 2001
FINAL
REITOX


BIRN
Belgian national report on drugs 2002
Epidemiology Unit, Scientific Institute of Public Health, October 2002; Brussels (Belgium)
IPH/EPI REPORTS N° 2002 - 024Deposit number: D/2002/2505/41
BELGIAN NATIONAL REPORTON DRUGS
2002
edited bySLEIMAN Sandrine (IPH)
SARTOR Francis (IPH)
Scientific Institute of Public HealthUnit of Epidemiologyrue J. Wytsmanstraat 14B-1050 BRUSSELSTel. +32 2 642 57 82Fax +32 2 642 54 10Email: [email protected]://www.iph.fgov.be/reitox


This report was coordinated and written by the staff of the Focal Point (Kathy Colpaert,Guido Jossels, Edith Leus, Juan Pablo Protto, Francis Sartor, Sandrine Sleiman, DeniseWalckiers) and the staff of Sub-Focal Points (Fabienne Hariga, Sofie Köttgen, FredLaudens, Margarète Molnar, Delphine Pecsteen, Mark Vanderveken).
Acknowledgements
This report was made possible thanks to the contribution of many public and privateprofessionals, health professionals and social workers who participated in the datacollection despite their heavy work load. Their essential contribution is gratefullyacknowledged.
Acknowledgement is due to the Sub-Focal Points teams, ensuring the daily work of datacollection and the transmission of the information to the Focal Point.
We would like to especially thank for their very active contributions (by alphabetical order):
ADRIAENSENS G. (Steunpunt tot Bestrijding van Armoede, Bestaansonzekerheid enSociale Uitsluiting)BASTIN P. (Infor Drogues)
DAL M. (Prospective jeunesse)
DE BOE F. (Service de lutte contre la pauvreté, la précarité et l’exclusion sociale)
DE PAUW W. (Ministry of Justice)
DE WINTER Ch. (Federal Police, Drug programme)
GEIRNAERT M. (VAD)
GILLARD C. (Ministry of Justice)LEBRUN V. (Federal Police, Drug programme)
SASSE A. (IPH - HIV surveillance)
TACK E. (Ministry of Justice)
TECCO J. (Université Libre de Bruxelles)TODTS S. (Ministry of Justice)VANHYFTE C. (Federal Police, Drug programme)
VAN MAELSAEKE D. (Ministry of Finance, Customs)
WANLIN M. (FARES/VRGT)
Call for contribution and commentsEveryone interested in contributing to the next Belgian Report on Drugs can contact
the Belgian Focal Point. All comments are welcome.

EMCDDA MANAGEMENT BOARD
Willy BRUNSONDirecteur Général
Administration de la Communauté française de BelgiqueBd Léopold II, 44
B – 1080 BRUXELLESTel : 32-2/413.26.02 ; Fax : 32-2/413.26.13
e-mail : [email protected]
Claude GILLARDConseillerJuridique
Administration des Affaires pénales et criminelles
du Ministère de la JusticeBd de Waterloo, 115
B – 1000 BRUXELLES
Tel : 32-2/542.67.74 ; Fax : 32-2/538.83.75e-mail : [email protected]
EMCDDA SCIENTIFIC COMMITTEE
Joris CASSELMANKoning Leopold III laan 14
B – 3001 HEVERLEE
Tel/fax : 32-16/40.02.81e-mail : [email protected]
MINISTERS involved in health problems related to drugs (in 2001)
Mevrouw Magda ALVOETMinister van Consumentenzaken, Volksgezondheid en Leefmilieu (Minister for Health of the federal
governement)
De Heer Jos CHABERTMinister van Volksgezondheidszorg van het Brussels Hoofdstedelijk Gewest
(Minister for Health of the Region of Brussels-Capital)
Monsieur Thierry DETIENNEMinistre des Affaires Sociales et de la Santé de la Région Wallonne (Minister for Health of the Walloon
Region)
Monsieur Didier GOSUINMinistre de la Santé de la Région de Bruxelles-Capitale (Minister for Health of the Region of Brussels-Capital)
Madame Nicole MARECHALMinistre de la Santé et des Affaires Sociales de la Communauté française de Belgique
(Minister for health of the French Community of Belgium)
Herr H. NIESSENMinister der Deutschsprachigen Gemeinschafts (Minister of the German-speaking Community)
De Heer Frank VANDENBROUCKEMinister van Sociale Zaken en Pensioenen (Minister for Social Affairs of the federal governement)
Mevrouw Mieke VOGELSMinister van Welzijn, Gezondheid en Gelijke Kansen, Vlaamse Gemeenschap
(Minister for Health of the Flemish Community)

Belgian National Report on drugs 2002
Table of contents
SUMMARY 4
PART I. NATIONAL STRATEGIES : INSTITUTIONAL & LEGAL FRAMEWORKS 9
CHAPTER 1. Developments in Drug Policy and Responses 111.1. Political framework in the drug field 111.2. Legal framework 161.3. Laws implementation 171.4. Developments in public attitudes and debates 191.5. Budget and funding arrangements 21
PART II. EPIDEMIOLOGICAL SITUATION 26
CHAPTER 2. Prevalence, Patterns and Developments in drug use 282.1. Main Developments and emerging trends 282.2. Drug use in the population 292.3. Problem Drug Use 34
CHAPTER 3. Health Consequences 383.1. Drug Treatment Demand 383.2. Drug Related Mortality 383.3. Drug related infectious diseases 403.4. Other Drug Related Morbidity 46
CHAPTER 4. Social and legal Correlates and Consequences 484.1. Social problems 484.2. Drug Offences and drug related crime 484.3. Social and economic costs of drug consumption 52
CHAPTER 5. Drug Markets 535.1. Availability and supply 535.2. Seizures 535.3. Price/purity 55
CHAPTER 6. Trends per Drug 586.1. Cannabis 586.2. Synthetic drugs 586.3. Heroin opiates 596.4. Cocaine crack 596.5. Multiple use 59
CHAPTER 7. Discussion 607.1. Consistency between indicators 607.2. Methodological limitations and data quality 60
PART III. DEMAND REDUCTION INTERVENTIONS 62
CHAPTER 8. Strategies in Demand Reduction at National Level 648.1. Major strategies and activities 648.2. Approaches and new developments 65

Belgian National Report on drugs 20022
CHAPTER 9. Prevention 679.1. School programmes 67National Strategy 67Organisation and co-ordination within national structures 67Expenditures on prevention 679.2. Youth programmes outside schools 709.3. Family and childhood 719.4. Other programmes 73
CHAPTER 10. Reduction of Drug Related Harm 77Role of harm reduction within the national drug policy/strategy 77Harm reduction practice 77Range of services 77Networking between HR professionals 78Co-ordination of national policies and local practice 78Expenditures on specific harm reduction project 7810.1. Description of interventions 7910.2. Standards and evaluations 81
CHAPTER 11. Treatments 8411.1. “Drug-free” treatment and health care at national level 8411.2. Substitution and maintenance programmes 8611.3. After-care and re-integration 88
CHAPTER 12. Interventions in the criminal justice system 9012.1. Assistance to drug users in prisons 9012.2. Alternatives to prison for drug dependent offenders 9212.3. Evaluation and training 93
CHAPTER 13. Quality Assurance 9413.1. Description of new trends and developments 9413.2. Formal requirements for quality assurance 9413.3. Criteria and instruments applied in quality assurance 9413.4. Application of quality assurance procedures and results 94
PART IV. KEY ISSUES 96
CHAPTER 14. Demand reduction expenditures on drugs in 1999 9814.1. Economic Burden related to addiction in belgium 9814.2. Belgian drug policy in numbers 10114.3. References 103
CHAPTER 15. Drug and alcohol use among young people aged 12-18 10415.1. Prevalence, trends and patterns of use 10415.2. Health and social consequences 10615.3. Demand and harm reduction responses 10715.4. Methodological information 107
CHAPTER 16. Social Exclusion and reintegration 10816.1. Definitions and concepts 10816.2. Drug use patterns and consequences observed among socially excludedpopulation. 10916.3. Relationship between social exclusion and drug use 11016.4. Political Issues and Reintegration programmes 11116.5. Methodological information 112

Belgian National Report on drugs 2002 3
REFERENCES 116Bibliography 118Data Bases -Websites 129
ANNEXES 132Annex 1 : Drug Monitoring Sytem and Sources of Information 134Annex 2 : List of tables 141Annex 3 : List of Figures 142Annex 3 : List of Figures 142Annex 4 : List of abbreviations 143Annex 5 : Index 145

Belgian National Report on drugs 20024
Belgian National Report on Drugs 2002
SUMMARY
ÿ NATIONAL STRATEGY: A GLOBAL APPROACH
The Belgian legislation does not distinguish the applied penalties neither according to thetypes of drugs (so called “hard” or “soft” drugs), nor to the quantities of the seized drugs.Only the concepts of possession, group use and trafficking are considered and areapplied by the judicial authorities according to criteria applicable to each individual case.In 1997, the Parliament and the Council of Ministers adopted the conclusions of a workinggroup on the drug problem: the law enforcement on drugs was consequently adaptedspecifying e.a. that the penal justice must be an ‘Ultimum remedium” in case of seriouspublic nuisance. In January 2001, the Belgian Federal government issued a policy noteaiming to modify the narcotic law of 1921. The note includes the following points ofaction, aiming to control the illicit market/consumption of drugs :
- a global and integrated approach based on the creation of a Drug Cell / Inter-ministerial Conference on Drug Policy. Clear agreements should be anticipated inthe field of justice-assistance,
- support of evaluation, epidemiology and research in the field of illicit drug,- enhancement of prevention, with particular attention to youth,- development of a more integrated legal framework for health care, harm reduction
and reintegration,- in the field of repression, priorities will be given to the struggle against the illegal
production and the trade of raw materials, against synthetic drugs and against thecocaine and heroin trade and to the social nuisance. Prosecutions in the case ofsimple consumption have to constitute an ultimate stage in the framework of theintervention by judicial authorities. The narcotic law of 1921 will be modified inorder to make a distinction between cannabis and other illegal drugs. Furthermore,the qualification “use of illicit drugs in a group” will be eliminated from the NarcoticDrug Act and the possession of cannabis for personal use or in a quantity suchthat one can suppose that it is not intended to the sale, will no longer continue tobe prosecuted.
This note is currently under examination at the Belgian Senate. The new Narcotic law willonly concern adults since special youth courts are competent for offences committed byyouths.
A financial framework to support the municipalities with a high criminality rate wascreated. Some of those municipalities have set up projects aiming at drug treatment andprevention.
In the Federate Entities a growing effort is made to get a global prevention: the focus ismainly health and welfare oriented. Several evolutions are clear: development of a policyplan, increasing education and expertise of prevention workers, improved co-ordination ofprevention activities from a health perspective, further development of local crimeprevention initiatives with focus on drug prevention, enlarged provision in training,community approach. Many organisations and municipalities have developed prevention

Belgian National Report on drugs 2002 5
and/or care and cure activities in different fields: social services, workplaces, youthorganisations, schools, peer groups, harm reduction, leisure time.A executing Decree issued on 13rd February 2001 provides amongst other rules, aregulation for scientific research in general and research with medical / sensitive data inthe framework of the ‘Privacy Act’. A Royal Decree issued on 19th July 2001 authorizesthe use of cannabis to carry out clinical trials for some therapeutic indications.
ÿ KEY ACTORS
The Belgian political structures require a coordination of the different departmentsinvolved in the drug issue. The Health Policy Drug Cell, created in 2001 elaborates anintegrated health policy concerning drugs, and a coordination structure 'Cellule Drogue /Drug cell' is still pending.
There are a lot of key actors on the one hand at federal level: the Ministry of Justice, theMinistry of Foreign Affairs, the Ministry of Internal Affairs, the Ministry of Social Affairs andPublic Health, and the Ministry of Finances, and on the other hand at federate levels : thecommunities and regional governments (Flemish, French and German-speakingCommunities, Brussels-Capital Region).The Belgian Focal Point, located at the Scientific Institute of Public Health, is the Belgianrepresentative in the REITOX1 network settled down by the EMCDDA. The BIRN (BelgianInformation Reitox Network) was created in 1995 and links the National Focal Point withthe 4 Sub-Focal Points: ASL (Arbeitsgemeinschaft für Suchtvorbeugung undLebensbewältigung) for the German-speaking Community, CTB-ODB (ConcertationToxicomanies Bruxelles - Overleg Druggebruik Brussel) for the Brussels-Capital Region,EUROTOX for the French Community, VAD (Vereniging voor Alcohol en andere Drugproblemen) for the Flemish Community.
ÿ EPIDEMIOLOGICAL SITUATION
Drug use among the school population appears to be the best documented. Schoolsurveys are regularly conducted both in the Flemish and French Communities within theframework of the repeated WHO HBSC cross-sectional survey. At present, trends in druguse can be made over the last decade both in the Flemish and French Communities.Other school surveys are also conducted independently of the HBSC surveys in differentareas of the country.
Data on the lifetime and recent use of cannabis among adults living in the FrenchCommunity has been collected as part of a continuous monitoring of health behaviourcarried out from April 1996 to March 2001. A short module designed to estimate thelifetime and last month prevalence of cannabis and XTC/amphetamines use wasintroduced in the 2001 edition of the national Health Interview Survey.
In the National Report, the TDI data were usually presented separately for each federateentity (Communities or Region) but could actually not be pooled to provide national figuresbecause these data are not comparable between the different federate entities.
1 REITOX : Réseau Européen d'Information sur les drogues et TOXicomanies / European network linking
EMCDDA and National Focal Points for the exchange of information on drugs and drug addictions.

Belgian National Report on drugs 20026
The prevalence of problematic drug use in Belgium can presently only be estimatedusing the prevalence of HIV among problematic drug users and data related to drug usersfrom the national HIV/AIDS register. The lifetime prevalence of injecting drug use in 1995and in 1997 was estimated in this way. On the other hand, a feasibility study has beencarried out in Charleroi in 2001-2002 in order to obtain local information on the prevalenceof the problematic drug use through the “capture-recapture” method.
The National Institute of Statistics provides data on drug-related deaths, which complywith the EMCDDA guidelines. Unfortunately, these data are out dated owing to thecomplexity of the administrative structure of the country. On the other hand, the number ofoverdoses registered by special registries (forensic or police) appears to be unreliable.
The different monitoring systems collecting TDI data provide some self-reportedinformation on the HIV, hepatitis B and C status among treated drug users. Moreaccurate estimates of the prevalence of HIV, hepatitis B and C among treated drug userscan be derived from the measurements of biological markers carried out by two Flemishtreatment centres.
In conclusion, the global description of the situation and trends in drug consumption anddrug related problems remain incomplete. Therefore, it is urgent to make an importanteffort in order to improve the collection of reliable standardized data. The comparability ofthe data collected by the federate entities should be improved in order to make meaningfulcomparisons between the different parts of the country and to produce valid figures atnational level.
In the present national report no treatment demand indicator data will be presented sincethe National Focal Point did not receive on time the required data except for the Germanspeaking Community.
An early warning system on drugs is being developed. A network of toxicologicallaboratories for substance analyses set up. Work on establishing a second network forthe collection of socio-cultural information, and a third network of clinical laboratories,which carry out analyses on human samples is in progress. The aim is to provide timelyand regular results not only on new drugs but also on all kinds of illegal substancescirculating. The Belgian system is integrated in the European Joint Action on NewSynthetic Drugs.
SOME RESULTS…
In school and youth population, the lifetime, last year and last month prevalence ofcannabis use persists in its rising trend. The lifetime prevalence of XTC use shows erraticannual fluctuations, although it seems that it has decreased somewhat between 1998 and2000.
According to the results of the French Community survey in general adult population, asignificant increasing trend is shown in the lifetime prevalence of cannabis use from 13%in 1996 to 22% in 2000. The last week prevalence of cannabis use among the 18-49years is around 3% in 2000.

Belgian National Report on drugs 2002 7
A study based on 1997 data estimated the prevalence of intravenous users among the 15-64 years old to be to 0.35-0.42%.
The prevalence of IDU among HIV cases remains relatively stable since 1998: around 5%. In 2000, the proportion of self-reported HIV-seropositivity among IVDUs demandingtreatment was around 2-3 %. The prevalence of HBV infection amounts to 20-25 % andseems stable since 1998. Based on biological testing, around 40% of IDU’s patientshave antibodies against hepatitis C.
Regarding social and legal correlates, drug possession and personal use infringementsrepresent 73% of all infringements related to narcotics in 2000. Cannabis is the mostcommonly involved drug of all drug related arrests.Globally, the number of drug seizures has increased in the nineties. The highest numberof seizures of cannabis and XTC was recorded in 2000.
ÿ DEMAND REDUCTION
A lot of interventions were set up but still often without any planned evaluation. InBelgium, the culture of evaluation is not developed in this field. However, all projectsfunded by the French Community have an evaluation component. A collaborative projectwas initiated at European level (EMCDDA) : EDDRA (Exchange on Drug DemandReduction Actions) is a project aiming to develop a data base presenting an inventory ofprevention and harm reduction projects conducted in Europe and focusing on theirevaluative component.
ÿ KEY ISSUES
A snowball survey, among drug users, has showed that the last month prevalence ofcannabis and XTC use among youngsters and adults are quite comparable. However,differences appear in prevalence for other substances.An exploratory survey about issues of new synthetic drugs has been conducted in 2000.Its main aim was to investigate the emergence of a problematic consumption of newsynthetic drugs. It shows that the frequency of problems linked to consumption of XTCamong youngsters is similar to the one reported by adults.
Regarding social exclusion and reintegration, an inter-governmental conference (CIG) hasbeen set up. Constituted by 6 working groups, the CIG gathers all the governments of thecountry. The fight against social exclusion is a responsibility of both Federate and FederalGovernments, each one of those having with their own specific responsibilities. One ofthese groups, “Commission of Social Affairs” is responsible for the Belgian National ActionPlans against poverty and social exclusion (NAPs/incl).
ÿ PRIORITIES FOR THE FUTURE
An important effort is urgent in order to obtain standardized epidemiological data. Thedevelopment of a high quality information system is essential in order to enlarge theknowledge on the nature, the extent and the change in drug use in term of prevalence,

Belgian National Report on drugs 20028
incidence, mortality, morbidity, social consequences, but also about attitudes andbehaviours. Qualitative and quantitative information is necessary.From a public health point of view, reliable epidemiological information on the prevalenceof drug use in the different groups of the population, on the patterns of use, on thedemand reduction initiatives, on their specific targets and on their outcomes will permitbetter determining the objectives, priority interventions and target groups and to correctlyassess their impact. Moreover, standardized information will provide the possibility tocompare the situation in different areas, to compare the outcomes of different types ofintervention and to identify the most-efficient programmes.As there are many interventions as well in prevention as in care activities, there arenumerous sources of information for the data collection. A strategy for the data collectionshould be defined. Co-ordination should be implemented and a minimal harmonised dataset should be collected.

PART I. National Strategies : Institutional & Legal Frameworks
Synthesis by PECSTEEN Delphine
on basis of contribution ofDE RUYVER Brice


Belgian National Report on drugs 2002
CHAPTER 1. Developments in Drug Policy and Responses
1.1. POLITICAL FRAMEWORK IN THE DRUG FIELD
1.1.a Objectives and priorities of the national drug policy
On Friday 19 January 2001 the Belgian Federal Government proposed a new policynote, a proposal to modify the law of 1921 (Narcotic Drug Act)2.Since then, this note is under examination at the Belgian Senate. Key points of this newpolicy are detailed hereafter.
1.1.b New initiatives and major changes in political approach
In this section two levels are presented:- the federal level,- the federate levels: Flemish, French, German Communities and the Brussels Region.
ÿ Federal level® Policy note of the federal government on the drug problems (2001)
The Federal Drug Policy Note wants a reply to most urgent problems concerningconsumption and dependence of drugs. The note covers both illegal and legal drugs(alcohol, tobacco, some medicines). In addition, the objective of this note is to put intopractice some of the recommendations of the drug parliamentary policy working group.
Between a strictly repressive approach and, at the opposite, a full tolerance policy, theparliamentary working group opted for a policy of normalisation. The main objectives are:less drug, less physical and psycho-social damages, less social nuisances. To achievethese objectives the policy priorities were redefined: prevention and reduction of drug use,decrease of the number of new drug users, protection of the community and its memberswho are facing the drug phenomenon and its consequences, provision of care to drugusers and readiness to guarantee them a better life despite their drug use.
Like most European countries, Belgium was so far adopting a kind of tolerance policytowards cannabis, but this has led to differences in judicial consequences. The FederalDrug Policy Note respects all the international treaties adhered to by Belgium. Because ofthese treaties the selling of cannabis remains prohibited.
Royal decrees and directives should implement the Federal Drug Policy Note of January2001.
2 See point 1.3.b

PART 1National Strategies
Belgian National Report on drugs 200212
The note includes several points of action, aiming to control the illicit market/consumptionof drugs. The new national policy is based on 3 pillars: (i) prevention of drugconsumption; (ii) harm reduction, assistance, and re-integration; (iii) repression.
1. A GLOBAL AND INTEGRATED APPROACH
• Drug Cell / Inter-ministerial Conferenceon Drug Policy : the ‘Drug Cell’ will becomposed of representatives of thedifferent levels of power (Federal State,Communities and Regions) and chaired bya drug co-ordinator. The Drug Cell willsupport and will counsel authorities as wellas the inter-ministerial Conference onDrug Policy. It will also act as a nationalco-ordinator at the European level. TheHealth Policy Drug Cell, created in 2001,as part of the Drug Cell, elaborates anintegrated health policy concerning drugs.• Justice - Assistance : clearagreements- Agreements related to the professionalsecrecy, to the respect of treatmentprogrammes and to the status ofassistants in the framework of securitycontracts, prevention contracts and otherdrug-related contracts and alternativejudicial measures;- Agreements related to crisis centres;- Designation of judicial ‘case-managers’in each ‘house of justice’;- Better delimitation of prevention tasksbetween police services and the psycho-medico-social sector in the framework ofsecurity contracts.
2. EV A L U A T I O N , EPIDEMIOLOGY AND
RESEARCH
The national Focal Point gathers andanalyses data on the consumption ofdrugs in Belgium, examine and comparethe effects of the different measures. TheNFP will also continue the development ofan ‘Early Warning System’ in order torapidly detect the introduction of newsubstances in the drug market. Evaluationof treatment methods, health careinstitutions, care circuits and preventiontechniques will be carried out.
3. PREVENTION
The Communities have autonomouscompetence and should continue theirefforts concerning prevention. A number ofrelatively concrete actions regardingpsychoactive medicines, driving underdrug influence and the policy regardingtobacco and alcohol are included in thenote though.
Particular attention will be granted toyouths in order to avoid their contact withillegal and legal drugs at an increasinglyyounger age and to teach them to handlethese substances in a responsiblemanner.
4. HEALTH CARE, HARM REDUCTION AND
REINTEGRATION
Taking into account local needs, a moreintegrated legal framework will bedeveloped to make health care possiblefor drug addicts through local carenetworks, of which mental health carecentres can be a part. Special attentionwill go to youths, psychiatric patients withdrug problems (dual diagnosis), foreignerpopulations as well as crisis care centres.Legal substitution treatments will beorganised and an evaluation will beconducted on the basis of clinical trials onthe medical prescription of heroine.The various sources of funding will bebetter co-ordinated as well.

PART 1National Strategies
Belgian National Report on drugs 2002 13
5. REPRESSION
The struggle against the trade of drugshas to go together with measures aimingto reduce the demand of drugs andhence a policy oriented to limitation ofpersonal drug consumption. Authoritieswill pay particular attention to derivedcriminality and to social nuisance.Prosecutions in the case of simpleconsumption have to constitute anultimate stage in the framework of theintervention by judicial authorities. If adrug user is put in detention, he has tohave access to the therapeutic andmedical assistance.• Penal Policy and trade of drugsThe Minister of Justice will establish adirective on the trade of drugs. Prioritiesare among others the struggle againstthe illegal production and the trade ofraw materials, against synthetic drugsand the cocaine and heroin trade.• Penal reaction to the consumption ofdrugsThe law of 1921 on drugs will beadapted: in order to make a distinctionbetween cannabis and other illegaldrugs. Furthermore, the qualification“use of illicit drugs in a group” will beeliminated from the Narcotic Drug Act.The possession of cannabis for personaluse or in a quantity such that one cansuppose that it is not intended to thesale, will no longer be prosecuted.Please note that these changes onlyapply to adults; the policy regardingyouths remains unchanged.
‘Hard’ drugs remain prohibited.• Fixing of the sanctionThe measure of probation will be appliedmore largely. The therapeutic advice will belegally recognized (i.e. assistance workersgive advice on whether accompaniment isindicated).• Penitentiary drug policy Measures will be established to counter theintroduction of drugs in prison. Theapproach will be oriented to theaccompaniment of the drug user,substitution treatments will be organizedand the consumer will be able to call anassistance of quality, possibly throughexternal services, during its detention.
The modalities regarding the distinctionbetween cannabis and other illicit drugs,and the investigation and prosecution policystill have to be outlined in Royal Decrees.
® Federal political note related to mental health care (2001)
The Minister of Public Health has proposed a vision of a new, more integratedorganization of mental health care, oriented to the future.Points of action are : the patient as starting point (demand of care and participation,reorganization in function of target groups: care, platforms of dialogue for mental healthcare, plug in by first line health cares and by general hospital, reform of care), specificitiesof target groups (youths, adults, elderly, drug addicts, handicapped presenting seriousbehaviour problems) and quality health care (research and recording of data, training).
PART 1National Strategies
Belgian National Report on drugs 200214
® Security and Society Contracts
The council of Ministers has reached on 21st December 2001, an agreement on the futureof the Security and Society Contracts. The Permanent Secretariat for Prevention Policy(PSPP), department of the Ministry of Interior, is in charge of elaborating, co-ordinatingcrime prevention policy. These contracts will be reconducted for a 2 years programme(2002-2003) and will be renamed “Security and Prevention Contracts”.
Municipalities, which benefit of these contracts have been selected on the basis of 3criteria :
- More than 60,000 inhabitants,- High criminality rates,- Low socio –economical level.
Prevention of drug use and treatment of drug users are thematic areas of these contracts.More details on these contracts are given in Part III Demand Reduction.
ÿ Federate levels® Drug Policy in the Flemish Community
The point of view of the Flemish Government concerning drug problems stresses thepromotion of health and well being, the prevention of drug problems, harm reduction andtreatment facilities for different target groups. It promotes co-operation between federaland community governments to develop a global approach.
In the Flemish Community, there is a global approach for prevention and to a much lesserextent for treatment (as treatment is mainly financed by the federal government). TheFlemish government has organised its policy through a covenant that is signed betweenthe government and the co-ordinating agency VAD. A policy plan was developed in which8 areas of work were defined to implement a Flemish drug policy 1999-2001. The plancontains different actions in each area of work, with indicators for measuring its realisation(evaluation).The main areas of work are: information and sensibilisation, consultancy, training andsupport, development of new concepts and data collection and research.The provincial networks also have a covenant with the Flemish government in which theirareas of work are defined to strengthen the Flemish drug policy (the areas are in the fieldof co-ordination, implementation of concepts and data collection).
Political agreements have led to the implementation of needle exchange programmes in2001.
The global prevention policy is implemented through the different sectors in society(education, youth work, workplace, adult education, health and welfare sector, leisuresector, …). Key people within these sectors are identified and training and consultancy isset up to empower them to develop a prevention policy in their setting.Drug prevention workers act at the regional and local levels.
In some regions, the treatment sector has organised itself in the area of crisis interventionby setting up an experimental, voluntary ‘crisis network’.

PART 1National Strategies
Belgian National Report on drugs 2002 15
® Drug Policy in the French Community
The Ministry of Health of the French community is responsible for health promotionincluding prevention projects. It defines health promotion according to the Ottawaconvention. In its five-year Health Promotion Programme (1998-2003), the FrenchCommunity has identified six priority health problems: infectious diseases (HIV,immunisation and tuberculosis), cardio-vascular diseases, cancers, addictions, mentalhealth problems and accidents.In terms of target population, priority is given to the socially excluded population, and toschoolchildren.The following strategies to deal with addiction have been proposed:
a) To fight the anxiety and activism often associated with the issue of drugs and topromote public awareness and training programmes for adults.
b) To promote debates between young people and adults around drug issues in thescope of general education, placed within a wider context of questioning themeaning of life and our choices in life, at a critical period in the psychosocialdevelopment of adolescents.
c) Instead of focusing on drugs themselves, prevention should focus on attitudes,behaviour and perceptions of young people.
d) To look towards a global perception of addiction, not restricted just to illegal drugs.e) To also choose strategies aimed at reducing the risks of using legal or illegal drug.f) Finally, it is absolutely essential that prevention issues be addressed in a manner
that respects human rights, democracy and a law-based society.
Under the AIDS prevention programme, intravenous drug users are identified as one ofthe target population.
® Drug Policy in the German-speaking Community
In the coalition agreement of the government of the German Speaking Community,prevention has been set as the primary step in the drug sphere. According to thegovernment of the German Community, the proximity to the border of Germany, theNetherlands and Luxembourg demands collaborations across borders. A forum to permitinternational exchange is the „Mondorfgroup“. Representatives from the Saarland, MoselleRheinland-Pfalz, Luxembourg, the German Speaking Community of Belgium and thedepartment in France cooperate in this team. The German Speaking Community putsemphasis on a more active communication between local working people in the drugsphere. People being responsible for prevention and therapy/aftercare should be inpermanent dialogue.
® Drug Policy in the Brussels-Capital Region
The Brussels Drugs Programme, emphasizing demand reduction, brings together thoseinvolved in the drug field , and co-ordinates regional health actors' projects or initiativeswith other sectors (lawyers, Justice Department, Public Prosecutor's office, federal andlocal Police forces). Among the eleven issues dealt with by the programme, two focus onexternal collaborations (with the various authorities in Belgium and with internationalcollaborators).It should be noted that funding for Brussels-based drug-related health programmes canoriginate from six different sources.

PART 1National Strategies
Belgian National Report on drugs 200216
From April 1st, 2001, a new structure has been set up. The 11-issues programme as wellas the overall aims are kept unchanged. Five working groups (for five target populations)are going to report regularly for providing policymakers with up-to-date information.Main responsibility deals with information, networking, data collection, expertise andreporting.It also favours co-operation between governments to improve a comprehensive approachto the drugs problem.
1.1.c Coordination policies
The Health Policy Drug Cell has been set up as mentioned in the Federal Drug PolicyNote. But a coordination structure 'Cellule Drogue / Drug cell' is still pending (see Action 1of the federal note: a global and integrated approach).
1.2. LEGAL FRAMEWORK
1.2.a Major changes in law and regulations existent and/or planned in the field ofdrug demand, supply, precursors and drugs related money laundering
In 2001 change occurred in the confidentiality of data :
The ‘Privacy Act’ of 8 December 1992 and the Royal Decrees pertaining to this lawguarantee individual privacy rights. An adaptation of the Belgian law to the 1995 EuropeanDirective was made in 1998. The adapted Law and its Decree (13 February 2001) provideamongst other rules, a regulation for scientific research in general and research withmedical / sensitive data. The current legislation includes the possibility to use personaldata for another purpose than initially foreseen, such as for scientific research purposes.The Decree distinguishes procedures to follow when using anonymous data – encodedpersonal or non-encoded personal data.
In the framework of the Policy note of the Federal government on drug issue, a project isfinanced by the Ministry of Health to formulate guidelines about the cooperation betweenjustice and assistance.
1.2.b Legal framework in the demand reduction field: prevention, treatment andharm reduction
1.2.b.1 Royal Decree on the medical use of cannabis (2001)
This Royal Decree authorizes the use of cannabis to carry out clinical trials for sometherapeutic indications such as nausea and uneasiness linked to chemotherapy andradiotherapy, glaucoma, multiple sclerosis and syndromes linked to AIDS and chronicpains. Treatments using cannabis can only be prescribed by physicians engaged in auniversity hospital or a hospital legally recognized for the treatment of the above-mentioned therapeutic conditions.Clinical trials are submitted on certain conditions and must be reviewed and accepted byan ad-hoc ethical committee. The prescription should be made by a physician attached to

PART 1National Strategies
Belgian National Report on drugs 2002 17
a university hospital or to a recognized hospital for the treatment of therapeutic conditionsor by a reference centre for pain control.
1.2.b.2 Legal basis for substitution treatments
The Federal Drug Policy Note of January 2001 mentions that legal substitution treatmentswill be organized.
A follow-up to the 'Consensus Conference on methadone substitution treatment(Committee on Addiction of the Hygiene High Council, Health Council - ministry of SocialAffairs, Public Health and Environment, published in 1994) has been organised. Between1997 and 1999, about one hundred experts discussed the state of art of methadonesubstitution treatment in the light of recent developments in Belgium. Therapeuticefficiency of methadone has been reassessed.
The limited and minor changes in the 'Consensus Conference' document underline itsvery high acceptance/adoption by all actors in the field of drug addiction therapy.Reductions of heroin use, of IV use, of the spread of the HIV virus and of the mortalityrelated to opiates use, are the major results generally attested by all Belgian practitionersthrough their professional experience. Recommendations have been issued to strengthenthe development of this therapeutic orientation in the interest of the patient, his/hersurroundings and the community in general.
1.2.c Other
Decree of the French Community on doping (27 march 2001).
The French community adopted a decree related to Health promotion in sport, to theinterdiction of doping and its prevention. A French-speaking health promotion commissionis created. The community disposes now of an instrument and a policy integrating thestruggle against doping in the perspective of health promotion in sport.
1.3. LAWS IMPLEMENTATION
1.3.a Implementation of law
Despite several directives from the Board of Prosecutors General (1993,1998) an uniformdrug prosecution policy could not be implemented. Efforts and/or agreements made in2001 in this field had little impact on the situation.
1.3.b Prosecution policy, priorities and objectives in relation to drug addicts,occasional users, drug related crime
The future prosecution policy, as presented in the Policy note of the Federal Governmenton drug issue (2001), would be based on a policy of normalisation focusing on thefollowing priorities :

PART 1National Strategies
Belgian National Report on drugs 200218
- The criminal intervention towards drug users will always be the “ultimum remedium”.Drug use should never be a reason for a criminal approach, except in cases of specificrisk situations, such as driving under the influence of drugs or social nuisance.- The criminal intervention will take into account the individual situation of the drug user.When problematic drug users come into contact with the criminal justice system, publicprosecutors will endeavour to direct them towards treatment facilities. The problematicdrug user can refuse the offer of a referral to a treatment facility; however, doing someans that the public prosecutor can always decide to prosecute or offer another modalityof settling the drug offence.- Drug addiction is not accepted as justification for criminal offences.
To further enhance a uniform investigation and prosecution policy, one or morespecialised magistrates will be appointed to handle drug files. One magistrate from thepublic prosecutors office, the so-called “reference drug magistrate” will have the finalresponsibility for the handling of the drug problem files within each legal district. Thismagistrate will follow up with the other magistrates when drug cases are involved toensure a uniform drug policy within the legal district. (Policy note of the federalGovernment on the drug issue, p. 64).In the future directive a distinction will be made between three categories of drugoffences (Policy note of the federal Government on the drug issue, Annex 2, The criminalreaction towards drug use, p.5-10):
Category 1: the import, production, transport, possession of a small amount of illicitdrugs for personal use
An official report will be written by the police in the case of :- a limited possession of illegal drugs, other than cannabis, for personal use (as a
rule, the use of illicit drugs, other than cannabis, is seen as problematic at theinvestigation level);
- a problematic cannabis use.In both cases, the magistrate will decide upon the use of therapeutic advice and referral toa treatment facility. The public prosecutor will determined the criminal response when theproblematic cannabis use or other risk situations. The range of responses includes thewarning, the transaction, the probation, the mediation and the prosecution.
Category 2: the import, production, transport, possession of an amount of illicit drugsthat surmounts the qualification of “possession for personal use” (category 1) and / orthat is committed in the framework of aggravating circumstances that are stipulatedunder the Belgian Narcotic Drug Act of 24 February 1921 (e.g. use in the presence ofminors)
The police normally make an official report. The investigation policy is primarily aimed atnuisance situations, risk situations and large-scale dealers.At the prosecution level a distinction is made between drug related crime to sustainpersonal use and drug related crime committed solely for the purpose of profit seeking.In the first case, the reaction of the public prosecutor depends upon the presence ofproblematic drug use or the severity of the offences. In the case of problematic use, thereferral to a treatment facility is aimed. In the case of serious drug related offences, theusers will be prosecuted.In the case of profit seeking, or in the case of aggravating circumstances under theBelgian Narcotic Drug Act of 24 February 1921, the user will also be prosecuted.

PART 1National Strategies
Belgian National Report on drugs 2002 19
Category 3 : Drug related crimes, other than those outlined in categories 1 and 2
The drug related crimes include acquisitive crimes of a severe nature (armed robbery,street robbery), expressive crimes of a severe nature (violence, heavy threats, hostage)and consensual crimes of a severe nature (membership of criminal organisations involvedin drug production, drug trade, dealing on a large scale).
The investigation policy will give priority to this category of offences. The police willmention the problematic use of the involved person in the official report.
At the prosecution level, the severity of the offences and the presence of problematic druguse will be taken into account. As far as possible the premises of the protection of thesociety (the severity of the offence) and an individualised and early therapeuticintervention (problematic use) are to be reconciled.In the case of serious drug related crimes, combined with problematic drug use, a referralto the treatment services is possible, although only if the public prosecutor determines thatthe severity of the offence does not impede with an individualised response; otherwise theoffender will be prosecuted.
It is important to note that most of the terms, such as “small amount”, “limited possession”,still have to be clearly defined.
1.4. DEVELOPMENTS IN PUBLIC ATTITUDES AND DEBATES
1.4.a Public perception of the drug issues: main results from surveys
The survey on “Belgians and drugs” (Patesson and Steinberg, 2000) gives someinformation on the public opinion regarding prevention3. The results of this survey showedthat according to the public the main actors of prevention should be the school system(60%), followed by parents (50%), media (36%) and medical doctors (19%).84% respondents regard the responsibility of young people as the most efficient methodfor prevention. Also considered effective are police interventions against dealers,information on risks in schools, control and repression in schools and leisure locations.
Free access to cannabis is regarded as an effective prevention by 47% of Flemishspeaking respondents and by 30% of the French speaking ones. Finally forced treatmentis perceived as efficient for prevention by 56% of the Flemish-speaking participants andby 44% of the French speaking ones.
1.4.b Orientations of the main public debates by civil society, national Parliament,organisations, NGO’s
Misunderstandings of the Federal Drug Policy Note were the source of ambiguous signalslaunched towards the general public. This leads to a great deal of confusion amongyoungsters and parents. Most youngsters, wrongly, now think that cannabis has beenlegalised.
3 A sample of 1013 persons aged between 18 and 55 years selected according to quotas sampling.
PART 1National Strategies
Belgian National Report on drugs 200220
In co-operation with the Flemish Ministers of Education and Health, a circular letter wascomposed to be sent to all secondary schools in Flanders, in which the proposed changesin the legislation are explained and in which schools are given suggestions to stick to theirdrug policy on the one hand, but to use the public debate about cannabis on the otherhand, to discuss with students about drugs in general and cannabis in particular.
1.4.c Media presentation and imaging drug use
The Federal Drug Policy Note on drugs had a large media coverage. Cannabis was thetopic of several debates on television, the theme of a multiplicity of local conferences andalso the subject of internet forum.
Launch of the information campaign "Better understand the new policy of theFederal governement" (May 2001)4
The 24-page brochure presents in the form of frequently asked questions : the basis of thepolicy of the Federal Government concerning drugs, proposals in prevention andassistance, aspects linked to the penal right as for the usage (new regulation for thecannabis, problematical consumption, social nuisances) and the struggle of thegovernment against the trade of drugs.
Campaigns in the Flemish CommunityVAD prepared a state of the art concerning cannabis on the basis of the literature and theexperiences of the prevention and treatment sector. This document is distributed in thesector and is available on the website.
A recent development in Flanders is the public confession made on television and in thepress by well-known personalities of their usage of soft drugs. More and more itemsappear in newspapers on drug issues and debates on drug use are not infrequent ontelevision.
VAD adapted the ‘TV-spot’ that was developed for the European drug prevention week of1998. The main message remained: ‘talking is the first step’. The TV-spot was scheduledon prime time television during the month of December 2000 and repeated in January2001 once the Federal Drug Policy Note was made public.
VAD developed some new information materials (posters, brochures) on cannabis andadapted existing materials. All available information and prevention materials werebrought together in a leaflet that was distributed largely to a variety of key persons in thedifferent areas (education, youth work, local prevention workers, …) and through thewaiting rooms of general practitioners.
Launch of the consciousness-raising brochure on prevention in the FrenchCommunityThe brochure “Drogues assuétudes: quelle prévention” edited by the French Minister ofEducation and Health in collaboration with a NGO presents an overview of the
4 http://www.minsoc.fgov.be/press_releases/fr/aelvoet/2001/2001_05_29_brochure _campagne_drogues.pdf).

PART 1National Strategies
Belgian National Report on drugs 2002 21
intervention philosophy of the services involved in drug prevention in the FrenchCommunity.
1.5. BUDGET AND FUNDING ARRANGEMENTS
1.5.a Funding directly related to drug issues
First of all, the complexity of the Belgian administrative structure does not permit to havean overview of the global national budget in relation to drug issues. A project “TheBelgian drug policy in numbers” is currently funded by the Federal Office for Scientific,Technical and Cultural Affairs (SSTC/DWTC). The aim of this study is “to make asignificant contribution by identifying all agencies involved in drugs policy and estimatingthe cost price of the various aspects of the policy being pursued”5. Three steps constitutethe research:
- Identification of the actors involved in the implementation of drug policy,- Cost of the various components of the policy being pursued,- Population reached among drug users.
Results of the survey are expected to be published in 2003.
Secondly, different problems regarding the quality of available financial data arise from thefact that funded projects are not always only focused on illegal drugs: indeed some ofthem are dedicated to tobacco prevention, alcohol or AIDS. Moreover, sometimes, someprojects focusing first on drugs addiction become more general.
In the Key Issue related to drugs expenditures, an overview of the budget is presented.
In order to prevent people from taking drugs and to ensure that people (with drugproblems or likely to develop serious drug problems) receive appropriate help and advice,the Federal Government has decided to provide an additional annual budget of € 12.4Million (for 2002 and onwards). This funding is mainly allocated to :
- € 135 000 Drug Cell- € 1 396 000 Evaluation and Research- € 2 271 000 Prevention- € 7 086 000 Treatment- € 1 082 000 Repression
1.5.b Drugs direct funding at national level
According to the previous comments, some sources of financing are presented. Thisinformation is not exhaustive.
Federal Level
Social and health careIn 2001, the Ministry of Social Affairs (through Social Security) had a provisional budgetfor treatment centres (under agreement) amounting to € 27 917 768. This budget does
5 For a summary of the project please refer to the following web site : http://www.belspo.be

PART 1National Strategies
Belgian National Report on drugs 200222
not include the participation of the Ministry of Internal Affairs, partly financing theMASS/MSOC (ambulatory centres), through Security and Society Contracts6.
Security and Society ContractsIn 2001, the budget for the Drugs Plans of the Security and Society Contracts, distributedbetween 26 cities, amounted to € 6 127 169 including the contribution to the MASS/MSOC.
Communities and Regions
In addition to the federal financing, drugs demand reduction activities are also supportedby the Communities.The 2001 annual budget is for:
Flemish Community: € 2 618 722French Community: € 1 250 000German Community: € 279 767 53Walloon Region: € 1 25 MoMixed Community Commission of the Region of Brussels Capital: € 247 184French-speaking Community Commission of Region of Brussels Capital: € 2 843 000(according to the decree 1995)Flemish-speaking Community Commission of Region of Brussels Capital: € 139 068 27
1.5.c Results from specific national survey
See chapter 14.
6 INAMI/RIZIV (2001), La rééducation fonctionnelle des toxicomanes de 1980 à 1999. Bruxelles.

PART 1National Strategies
Belgian National Report on drugs 2002 23
Legislation References
- Policy note of the federal government on the drugproblemsNote politique du Gouvernement Fédéral relative à laproblématique de la drogueFederale Beleidsnota Drugs19/01/2001http://www.minsoc.fgov.be
- Report of the drug parliamentary policy working groupRapport 5 juin 1997Chambre des Représentants de BelgiqueRapport fait au nom du Groupe de travail chargéd’étudier la problématique de la drogue (1062/1-2-3-96/97).Verslag 5 juni 1997Belgische Kamer van VolksvertegenwoordigersVerslag namens de werkgroep belast met hetbestuderen van de drugproblematiek (1062/1-2-3-96/97).http://www.dekamer.be/cgi-bin/docs49.bat?l=n&dir=1062
- Policy note related to mental health careNote de politique relative aux soins de santé mentaleBeleidsnota Voor Geestelijke Gezondheidszorghttp://www.minsoc.fgov.be/
- Security and Prevention ContractsContrats de securité et de PréventionVeiligheids- en PreventiecontractenCouncil of ministers 21 December 2001http://faits.fgov.be/
- Confidentiality of dataA.R. portant à execution de la loi du 8/12/1992 relative àla protection de la vie privée à l’égard des traitements dedonnées à caractère personnel.K.B. ter uitvoering van de wet va 8/12/1992 totbescherming van de persoonlijke levensfeer tenopzichte van de verwerking van persoonsgegevens.Moniteur Belge/Belgisch Staatsblad,13 February 2001.http://194.7.188.126/justice/index_fr.htm
- Royal Decree on the medical use ofcannabisA.R. 4 juillet 2001 déterminant lesconditions pour la délivrance desmédicaments contenant un ou destétrahydrocannabinol(s)K.B. 4 juli 2001 tot bepaling van devoorwaarden voor het afleveren vangeneesmiddelen die één of meertetrahydrocannabinolen bevatten.Moniteur Belge/Belgisch Staatsblad, 19July 2001.http://www.just.fgov.be
- Rapport de suivi de la conférence deConsensus sur la méthadone :Evaluation des recommendationsformulées en 1994 et propositionscomplémentaires.Follow-up van de conferentie over demethadone consensus : Evaluatie vande aanbevelingen geformuleerd in 1994en aanvullende voorstellen.November 2000.http://www.health.fgov.be/CSH_HGR/
- Board of General Prosecutors1994 and 1998.Ministre de la Justice et le Collège deProcureurs généraux, La directive du 8mai 1998 relative à la politique depoursuite en matière de détention et devente au détail de stupéfiants illégaux.Minister van Justitie en het College vanProcureurs-generaal,Gemeenschappelijke richtlijn over hetvervolgingsbeleid inzake bezit endetailhandel van illegale verdovendemiddelen, 08 mei 1998.
- Decree of the French Community ondopingDécr. Comm. Fr. 8 mars 2001 relatif àla promotion de la santé dans lapratique du sport, à l'interdiction dudopage et à sa prévention enCommunauté française.Decr. Fr. Gem. 8 maart 2001betreffende de promotie van degezondheid bij de sportbeoefening, hetdopingverbod en de preventie ervan inde Franse Gemeenschap, MoniteurBelge/Belgisch Staatsblad, 27 march2001, 10033-10039.http://www.just.fgov.be

PART 1National Strategies
Belgian National Report on drugs 200224


PART II. Epidemiological Situation
Coordinated and written by SLEIMAN Sandrine
With the active contribution of
COLPAERT Kathy, JOSSELS Guido, KÖTTGEN Sofie, LAUDENS Fred, LEUS Edith,MOLNAR Margarète, PECSTEEN Delphine, PROTTO Juan, SARTOR Francis,
VANDERVEKEN Mark

Belgian National Report on drugs 2002
CHAPTER 2. Prevalence, Patterns and Developments in drug use
This year this part of the report is rather short. In one hand, older information, studiesalready presented in previous reports are not repeated. In the other hand, as a number ofinstitutions faced with difficulties in data collection and then in updating their databases,very few new results could be presented. In addition, comparison between the differentsources of information (federate entities) has to be done with caution because of thevarious and non-standardized methods of data collection.
2.1. MAIN DEVELOPMENTS AND EMERGING TRENDS
The trends observed in the last year have been the same trends for several years:growing popularity of cannabis and XTC use among youngsters. Focusing on the mostrecent trend, the lifetime prevalence and the last-month prevalence increase, both forboys and for girls in all age groups.
Males use more frequently drugs than females and use increases with age. Problemsrelated to the use of heroin and cocaine are the most common reasons for the demand oftreatment. The ‘typical user’ starts at a young age (younger than 18, or even youngerthan 15 years old). Poly-addiction has become very common.
An increase of demands for treatment of problematic cannabis use, is usually observed incentres of mental health care. Indeed, most cannabis problematic users have easieraccess to advice and treatment in these centres than in ‘specialised’ addiction centresclassically more oriented to opiates users. Nevertheless, some of the specialised centres,are more accessible to problematic cannabis users.
HIV-seroprevalence among drug users remains low in Belgium. In contrast, studies showhigh prevalences of hepatitis B and C, which are not decreasing throughout the years.Given its evolution to chronicity and cancer, hepatitis seems to become the main publichealth consequence of intravenous drug use.
The set-up of low threshold centres offers an additional possibility to access to treatmentincluding methadone substitution and to extend risk reduction interventions.

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 29
2.2. DRUG USE IN THE POPULATION
2.2.a General adult population
In Belgium, up to now, no national representative study on the use of drugs in the generaladult population has been completed. However, in the 2001 edition of the national HealthInterview Survey (HIS), some drugs questions were introduced. These questions arerelated to lifetime and last month prevalence of cannabis and XTC amphetamines use.The questionnaire is self-administrated and focused on people aged 15-64 years. Resultsare presently analysed and will be published in the next annual report.
In the French Community, from April 1996 to March 2001, a continuous monitoring of thehealth behaviour has been conducted in four areas, representative of this Community’shouseholds (Piette and De Smet 2001). The survey is using a computer assistedtelephone interview method with random dialling of the household and random selectionof one adult. The participation rate is 68%.
The access to cannabis and to cocaine as well as the consumption of cannabis (at leastonce and during the last 7 days) was also investigated. More interviewed people thinkthey could access nearby their houses to cannabis (65%) than to cocaine (see alsochapter 5).About 20 % of adults interviewed in 2000 stated to have used cannabis at least once andthe prevalence decreases with age (Table 1). Males reported cannabis experience morethan females. These differences remain significant after standardization respectively forsex, education and area, and for age, education and area.
Table 1 : Lifetime prevalence rate (%) of cannabis use among the adult population, FrenchCommunity, 1996-2000
Period 18-49 Years* 18-34 years* 35-44 years*N Total M F Total M F Total
1996-97 976 12.8(10.8-14.8)**
24.9 11.0 17.8(14.6-21.1)**
12.7 8.7 10.5(7.3-13.8)**
1998-99 1108 20.8(18.3-22.8)**
35.3 17.0 26.1(22.5-29.7)**
23.4 10.1 16.3(13.0-19.6)**
2000 694 22.2(19.2-25.2) **
39.1 22.8 30.9(25.7-36) **
23.1 8.2 15.0(10.8-19.3)**
*: adjusted rates for age, sex (for the total figure), education and area;
**: 95% confidence interval.
According to the results of the French Community survey, a significant increasing trend isshown in the lifetime prevalence of cannabis use from 13% (1996) to 22% (2000). But ithas been noticed that the prevalence of the last 7 days among the 18-49 years represents3%. This last week prevalence is similar to the last month prevalence.
PART 2 Epidemiological Situation
Belgian National Report on drugs 200230
2.2.b School and youth population
This section aims to present the various studies carried out on the consumption of drugsin the school population.Studies on school and youth population are presented through 3 sub-sections:
- HBSC7 studies,- Flemish Community study by VAD,- Local studies.
2.2.b.1 Health Behavior School-aged Children studies : National Information
In Belgium two studies are conducted based on the international protocol HBSC.
The University of Ghent (UG) is responsible for the HBSC study in the FlemishCommunity. The study is repeated on a regular basis (1990-2000). As from 1998 allstudents of secondary schools were interviewed.The University of Brussels (ULB) is responsible for the HBSC study in the FrenchCommunity, since 1986. Results are standardized for age, sex and type of education.
The prevalence of drug use is higher in males than in females (Table 2; Maes andVereecken 1999; Kinable 1999). The results of the surveys carried out by the University ofGhent suggest that in the age group 15-16 years, the lifetime prevalence of :
- cannabis use increased from 15 % to 21 % over the period 1994-2000,- XTC use decreased from 4,1 to 2,6 % during the same period. However, this
decrease may only be apparent since the definition of XTC changed in 2000 : insurveys conducted before 2000, the XTC category includes both XTC and speed,
- amphetamines and solvents use shows no particular trend.
Moreover, the lifetime prevalence in the age group 17-18 years :- increased from 23.1 % to 39 % for cannabis use over the period 1994-2000,- XTC use increased from 6.3 to 8 % during the same period,- amphetamines use shows an increase (4.3 and 8.2 % in 1994 and 2000
respectively), and- solvent use decreased from 5.5 to 4.6%.
In the French Community, an increase of the consumption of all substances is seen forboth age groups and more especially for cannabis. Lifetime prevalence of XTC seems toincrease much more in the older age class.
7 The Health Behavior School-aged Children (HBSC) survey is a research project that aims to gain new insight into, andincrease our understanding of health behaviors, lifestyles and their context in young people in different countries andcultural settings. The study also aims at increasing the understanding of young people’s health including how they perceivehealth itself. HBSC started in 1982, initiated by researchers from Finland, Norway and England. Shortly afterwards it wasadopted by the World Health Organization (Regional Office for Europe) as a WHO collaborative study. There are currently35 HBSC member countries and regions. The surveys are carried out in schools among 11, 13 and 15-year-old pupils. Astandardized questionnaire is used. The recommended sample size is 1500 students per age group in each country. Eachcountry can, if it wishes it, add additional questions. It is the case in Belgium where the two responsible teams add a module“drugs”. The Belgian samples are representative of the various networks and types of teaching as well as sex.

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 31
* The definition of XTC in 2000 is not the same as preceding years’. Before 2000 the item XTC contained speed. In 2000XTC does not contain speed.
It appears that the lifetime prevalence is higher in the French Community than in theFlemish Community except for solvents (table 2), however the comparability of thesesamples have not been checked. The lifetime prevalence of drug consumption amongboys is always higher than among girls (up to 10 % for cannabis).
Overall, the lifetime prevalence of drug use in the 17-18-years age group shows the sametrends as in the 15-16-years group.
Flemish Community
From 1994 to 2000, cannabis is the only drug with an increased last month prevalence.The second most frequently reported drug is XTC.
Table 2 : Lifetime prevalence (%) of drug use among the school population aged 15-18 years for Flemish and French Communities, 1994-2000
HBSC UG HBSC ULB
1994 1996 1998 2000 1994 1998
N 10.414 4.771 12.088 7.072 15.347 12.987Cannabis15-16 Males 20 17.9 22.2 25 18.1 29.1
Females 10 11.6 15.4 16.3 13.3 23.9Total 14.9 14.6 18.9 20.7 15.4 26.2
17-18 Males 32.1 37.1 42.7 44.7 29.5 48.9Females 14.2 23 30.7 33.8 18.5 37.7
Total 23.1 29.9 36.7 39 23.3 42.4XTC
15-16 Males 5 5.8 6.6 3.2 4.7 5.5Females 3 2.7 3.3 1.9 3.5 4.7
Total 4.1 4.2 5 2.6 4.1 5.117-18 Males 8.9 11.4 13.2 10.1* 7.4 13.6
Females 3.7 4.3 8 6.1* 4.0 8.5
Total 6.3 7.7 10.6 8* 5.5 10.7
Amphetamines15-16 Males 3 2.7 4.2 4.1 2.5 5.4
Females 2 1.7 2.3 2.6 1.1 4.5Total 2.6 2.2 3.3 3.3 1.7 4.9
17-18 Males 6.5 6.1 7.2 10.2* 2.9 11.3Females 2.1 2.5 4.3 6.4* 1.8 6.7
Total 4.3 4.2 5.7 8.2* 2.2 8.6Solvents15-16 Males 4 3.4 5 5 2.4 5.4
Females 2 1 2.7 2.2 2.8 3.8Total 3.3 2.1 3.8 3.6 2.6 4.5
17-18 Males 8.0 8.7 9.3 5.7 3.2 6.2Females 2.1 3.1 5.4 3.6 2.1 3.1
Total 5.5 5.8 7.3 4.6 2.6 4.4

PART 2 Epidemiological Situation
Belgian National Report on drugs 200232
The last month prevalence is higher among boys than girls for all substances (table 3),although a rise is observed for all genders. This is the case for the age group 15-16 as forthe age group 17-18 years (Maes and Vereecken 1999).
Table 3 : Last month prevalence (%) of drug consumption among students, FlemishCommunity schools, 2000
Aged 15-16 Aged 17-18
Drug Boys(n = 719)
Girls(n = 870)
Boys(n = 603)
Girls(n = 78)
Cannabis 15.1 8.5 25.4 15.0XTC 1.5 1.1 5.0 2.9Sniff, volatile inhalants 2.2 1.4 3.4 2.5
Amphetamines 1.8 0.9 3.3 2.3LSD 1.7 0.5 1.3 1.2
Cocaine 0.5 0.3 1.0 1.0Heroin 0.3 0.0 0.2 0.4
For example, the frequency of cannabis use during the last month is higher among boysthan girls (Maes and Vereecken 1999), but rises throughout the years among bothgenders.Nevertheless, for the girls the frequency of consumption of cannabis has doubled between1994 and 2000 (Table 4).
Table 4 : Frequency (%) of cannabis use during the last month; Flemish Communityschools, 1994-2000
1994 1996 1998 2000
1-2times
3 times ormore
1-2times
3 times ormore
1-2times
3 times ormore
1-2times
3 times ormore
Boys 7.9 7.8 9.4 11.2 11.4 14.3 11.7 13.7
Girls 3.6 2.0 5.2 3.7 6.9 7.0 7.6 7.3
French Community
From 1988 to 1998, the lifetime prevalence of drug use among young people aged 13-17years rises steadily from 8 % to 21.7%.Same comment is available for the last month prevalence (from 1% to 12.6%).

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 33
0
5
10
15
20
25
1988 1990 1992 1994 1998
%
At least once Last month
Figure 1 : Proportion of young people aged 13-17 years having used a drug at least onceand during the last month, French Community secondary schools 1988-1998 (Piette et al.1997)
2.2.b.2 Community Study : VAD Survey
Since 1999, VAD conducts a large study in the Flemish Community schools. This studyuses its own protocol and covers representatively all types of schools.During the last year, 15.5 % of the students have used an illegal drug. This correspondsto 19.4 % of boys and 11.7 % of the girls. 10% of all students declared to use less thanonce a week and 5.5% used them more often .
2.2.b.3 Local surveys
Some local surveys in different parts of the country (repeated or punctual surveys) haveglobally shown the same results as presented in the previous sections.
Studies carried out in 2001 :
® VUB Area (Brussels & Flemish Brabant)Method : questionnairesN = 2150Number of Schools = 23 + 5 departments/faculties of post-secondary education schoolsClass age = 12-22 yearsIn 1994, start of Brussels Flemish schools study.
In 1998, Brussels study and follow-up of 450 students till 2003.In 2001, start of the study in Flemish Brabant + follow-up.
® “GGDs” of Limburg and ASL. Area : Region of Aachen, German speaking community ofBelgium and the province Limburg in The Netherlands.
Method : questionnairesN = ± 1400 in German speaking Community of Belgium, ± 17000 in region of Aachen and ± 21000in LimburgNumber of Schools = 126Class age = ± 12 – 16 (classes 2 and 4 of secondary education)

PART 2 Epidemiological Situation
Belgian National Report on drugs 200234
On the “GGDs” and ASL survey, results are not yet available to report the majorfindings.
® ULB. Area :Brussels (French)Method : questionnairesN = 1200Class age = 11-18 yearsIn 2001, the survey was held in 4th degree secondary classrooms.
In conclusion :
Even if one should be careful in interpreting the quantitative data of drug consumption byyoung people, based on the data obtained by means of self-administered questionnaires,the results of the above mentioned studies globally indicate that in 1994-2001 :
- The prevalence of cannabis use persists in its rising trend (for lifetime, last yearand last month use),
- XTC use seems to have decreased in 2000, but this trend could be related to thechange of definition of XTC;
- Overall, the lifetime prevalence of drug use seems to rise for all age groups as wellas for both genders.
2.3. PROBLEM DRUG USE
2.3.a National prevalence estimate of intravenous drug users
The feasibility in Belgium of different methods has been assessed in the framework of theEMCDDA project on problematic drug use prevalence (Sartor and Walckiers 2001). It hasbeen shown that only one method could presently be used. This method is based on theuse of HIV/AIDS data as well as an estimate of the prevalence of HIV among IDUs. Morespecifically, the number of IDUs was derived from the number of alive HIV persons, theprevalence rate of IDU among HIV patients and the prevalence rate of HIV seropositivityamong IDUs (Table 5).
Table 5 : Lifetime prevalence of injecting drug use in the population aged 15-64years, in 1995 and 1997
1995 1997 1997
Alive HIV cases 6,734 7,819 7,819
p(IDU/HIV) (%) 8.73 8.00 8.00p(HIV/IDU) (%) 3.0 1 2.7 2 2.2 3
Prevalent IDU cases 19,600 23,200 28,400Prevalence rate (%) 0.29 0.35 0.42
1 HIV+ : self-reported in 1995; 2 HIV+ : self-reported in 1997; 3 HIV+ : blood test in 1997

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 35
2.3.b Regional prevalence estimate of opiate users
Local prevalence of opiates use in the French Community was estimated using thecapture-recapture method (Ledoux et al. 1999). The prevalence rates were calculated forthe 15-54 years group (Table 6). These results have however to be interpreted withcaution because the underlying assumptions required to apply the method are obviouslynot met (lack of mutual independence of the two samples, and probability of selection intoa sample/list for each individual probably not equal).
Table 6 : Number and prevalence of opiate users in the FrenchCommunity, 1993-1994
Area Population15-54 years
(01/01/1995)
Number ofopiate users
Prevalence rate /1000
Brussels 523,664 6,769 10,9Wallonia 1,811,515 7,841 4,3
FrenchCommunity
2,335,179 14,610 6,3
The feasibility of a capture-recapture study is currently carried out in Charleroi and resultswill be presented in the next report.
2.3.c Risk behaviour and trends
ÿ Injecting use (Charleroi)
More than 50% of the heroin users in treatment in the region of Charleroi (Wallonia) overthe period 1995-1999 have injected at least once; since 2000 the proportion of everinjecting heroin users has decreased (Depaepe 2002). Regarding cocaine users, figuresturn around 30% since 2000 (table 7). For 2001, around 30 % heroin and cocaine usersare currently injecting.
Table 7 : Percentage of injecting users in Charleroi, 1995-2001 (sample sizebetween brackets)
Drug Ever injecting Current injecting
1995 1996 1997 1998 1999 2000 2001 1999 2000 2001
Heroin 53(554)
55(481)
50(531)
56(588)
53(660)
41(571)
44.4(172)
17 20 35
Cocaine 37(286)
31(320)
37(350)
43(465)
41(547)
34(533)
33(101)
11 21 33.3
Medicines 1.2(163)
1.3(233)
1.8(226)
5.4 (93)
2.6(230)
1.2(453)
- - - -
ÿ Snowball survey (French Community)
Snowball surveys were carried out yearly since 1996 : drug use, its pattern and someknowledge and attitudes were investigated (Hariga F., personal communication). The

PART 2 Epidemiological Situation
Belgian National Report on drugs 200236
users have been interviewed in different regions (Brussels, Charleroi, Liège, Namur,Verviers and Wavre) but these regions may vary each year.Owing to large inter-annual variations, there is no clear pattern in the proportion of current(last 6 months) IDU among drug users (table 8). Clustering may also be a non-negligiblesource of bias. There is however a declining trend in the proportion of IDUs sharingsyringes. Sharing other parts of injection equipment, such as spoon, cotton, water,happen more frequently. For example in 1999 and 2000 respectively, 66 % and 61 % ofcurrent IDUs reported sharing syringes.
Table 8 : Percentage of lifetime and current* IDUs and sharingsyringes among current IDUs, French Community, 1993-2001
1996 1997 1998 1999 2000 2001
Number of users 1,294 1,395 1,243 928 574 1051
Mean age (years) 27 28 28 28 29 29,5
Males (%) 66 69 67 70 70 65
Lifetime IDUs/drugusers (%)
68 74 65 68 60 -
Current IDUs/drugusers (%)
53 56 43 52 40 46
Sharing/IDUs (%) 60 59 53 52 43 44
* injection during the last 6 months
In 2001, the current use of cocaine was reported by 62 % of the sample; 55 % of thesecocaine users are intravenous users (table 9). This percentage is significantly higher thanin 2000.
Table 9 : Percentage of current* IDUs according to drug used, FrenchCommunity, 1999-2001
Current use Current injecting
Drug 1999 2000 2001 1999 2000 2001
Heroin 81 69 69 54 (755)** 50 (397) 56 (416)
Cocaine 69 64 62 58 (644) 46 (367) 55 (362)
Amphetamines
23 30 28 19 (211) 19 (171) 21 (62)
Methadone 28 36 27 12 (208) 16 (208) 25 (65)
*injection during the last 6 months
**sample size into brackets
ÿ Injecting and Poly-drug use at a Rock Festival (French Community)
Information on these behaviours should be considered as an indication of the prevalenceof these behaviours among some selected groups of drug users. Indeed, there is aselection bias and a clustering effect.A survey on drug use is repeatedly conducted during a Rock Festival in the camp where50,000 spectators live during the festival (Hariga, Personal Communication).

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 37
In 2001, the intravenous drug users represented 5 % of users (table 10). The proportionof IDUs is lower than the preceding years (25 % in 1996 and 13 % in 1997 and 1998).
Table 10 : Percentage of IDUs, Rock festival, French Community, 1996-2001
1996 1997 1998 1999 2000 2001
Number ofinterviews
123 167 157 686 479 454
Current druguse
87 96 88 88 83 87
IDUs / users 25 13 13 4 4 5
The lower percentage of IDUs observed since 1999 compared to the previous years canbe explained by two reasons. First, the population has changed as the musicalprogramme changed from a mainly rock oriented festival to a more “house” festival.Secondly, in 1999 and 2000, the survey was carried out in the whole festival, not onlyaround the stands and not in the camping only.
In 2000, 435 spectators were interviewed : 83% stated to use at least one illicit drug, 30%of respondents used exclusively one drug (Table 11).In 2001, 35.5% of drug users stated to use 3 drugs or more and about one five reported touse only one drug.
Table 11 : Proportion of poly-drug use, Rock festival, French Community, 1996-2001
1996 1997 1998 1999 2000 2001
Number interviews 123 167 157 686 435 454Only 1 drug (%) 47 40 25 33 30 223 drugs or more (%) 32 45 36 36 40 35.5Total : at least 1 illicitdrug (%)
87 93 88 88 83 93
There is no major difference in the pattern of consumption observed in 2001 compared tothe two previous years.

Belgian National Report on drugs 2002
CHAPTER 3. Health Consequences
3.1. DRUG TREATMENT DEMAND
In Belgium the organisation of the Treatment Demand data collection process is beingmanaged by the four Sub-Focal Points: ASL for the German-speaking Community;CTB/ODB for Brussels Capital Region; EUROTOX for the French Community and VAD forthe Flemish Community. Each of them has its own registration system. Gradually thesesystems are expected to move towards each other and towards the Treatment DemandProtocol. These four Sub-Focal Points subsequently send the data in an aggregatedformat to the National Focal Point.
In the present national report no TDI data will be presented since :- the National Focal Point did not receive the required data from all sub Focal Points
for various reasons,- No information is available regarding the quality of epidemiological data collected
in the framework of the key indicator TDI. The coverage of the registrationsystems, among other things, is not documented at all. Therefore the NFP couldnot go through a formal quality control mechanism of the TDI data sent to theEMCDDA. In the National Report, the TDI data were usually presented separatelyfor each federate entity (Communities or Region) but could actually not be pooledto provide national figures because these data are not comparable between thedifferent federate entities.
3.2. DRUG RELATED MORTALITY
3.2.a General population mortality register
According to the EMCDDA guidelines, three definitions (“selections”) are possible fordrug-related deaths. These definitions are the restrictive “selection A”, the broad “selectionB”, and finally the all-inclusive “selection C”.Selection A comprises psychosis, drug dependence, nondependent drug abuse, oraccidental poisoning, due to opiates, cannabis, cocaine, stimulants, or hallucinogens.Selection B contains everything from selection A, with the addition of suicide andundetermined poisoning. And selection C contains all the items listed under selection Aand B, with psychopharmaceutical drugs added (EMCDDA, 2002).
The figure 2 presents the number of drug-related deaths in Belgium according to thedifferent selections

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 39
0
50
100
150
200
250
300
1991 1992 1993 1994 1995 1996
Year
Dru
g-R
elat
ed D
eath
s
SelectionC
SelectionB
SelectionA
Figure 2 : Number of drug-related deaths according to the EMCDDA selections A, B and C,Belgium, 1991-1996
The rise in drug-related deaths between 1991 and 1993 (selections A and B have nearlydoubled) should be interpreted with care, for another important trend is observed (table12): it seems that from 1991 to 1993 there is also an increase in the number of cases withcertificates mentioning psychoactive substances involved in the drug-related death.Therefore, one could say that the number of drug-related deaths are possibly influencedby an increase in the completeness of death certification over the period 1991-1993.
Table 12 : Proportion of drug-related deaths* with certificates mentioning involvement ofpsychoactive substances (%), Belgium, 1991-1996
Substance mentioned on certificate 1991 1992 1993 1994 1995 1996
Cases with involvement of psychoactivesubstances mentioned on death certificate
40.1 50.8 58.7 55.6 59.6 59.2
Opiate + any other psychoactive substance 31.7 29.7 46.3 48.3 52.6 49.6
Any psychoactive substance without opiates 68.3 70.3 53.7 51.7 47.4 50.4
* Based on the National definition, i.e. all 55 DRD-codes presented in the EMCDDA guidelines.
3.2.b Overdoses registered by police services
Although last year data was presented from a police register monitoring overdoses, it hasnow become clear that the register’s coverage and representativeness aren’t very good.For this reason, and because of its unsystematic way of registration, we have decided notto use these data anymore.

PART 2 Epidemiological Situation
Belgian National Report on drugs 200240
3.3. DRUG RELATED INFECTIOUS DISEASES
3.3.a HIV/AIDS
3.3.a.1 Injecting drug use among HIV/AIDS patients
In Belgium, diagnosed seropositive HIV persons and AIDS cases are registered in twointegrated databases at the Scientific Institute of Public Health in Brussels8.From the beginning of the epidemic till December 2001, 13800 HIV infected patients havebeen registered. Among these, 2922 have reached the clinical stage of AIDS (Sasse2002). The number of HIV infected people is much greater among males than amongfemales. Since 1997 an increasing trend in the number of new diagnosed cases of HIVinfection is observed.
Information on the risk factor status is globally available for 60 % of cases.The proportion of IDU among HIV cases (cases of HIV with intravenous drug use as riskfactor) decreased from 1986, reaching 3.4% in 1995 and then remain relatively stable(figure 3).
Infection via intravenous drug use was higher among young people, but it becomescomparable during the last recent years to that observed among older people. Amonginfected people aged between 15 and 24 years, the number of new cases stating IDU isquite low, respectively 4 cases in 2000 and 2 cases in 2001. This declining trend will haveto be confirmed in the long run.Since 1995 the trend of IDU among HIV cases seems to vary in a similar way amongmales and females (figure 4).
8Approximately 600,000 blood samples are yearly screened for HIV antibodies with the ELISA assay,
excluding testing related to blood donations. Seven reference laboratories are recognised by the Ministry ofPublic Health to confirm the results of these positive ELISA tests. Since they are the only laboratoriessubsidised for this confirmation, their reporting on new positive HIV individuals gives the number of newlydiagnosed seropositives in the country. Data on age, sex, nationality, residence, and possible route oftransmission are collected through a standardised form sent by these laboratories to the physician of eachnew HIV patient. On the other hand, the newly diagnosed AIDS cases are notified in an independent way byclinicians on a standardised form. They are validated by a Commission of experts referring to the definition ofthe Centres for Diseases Control, adopted by the European Centre for the Epidemiological Surveillance ofAIDS. This Commission guarantees data confidentiality. A follow-up survey is conducted each year to collectdata on last consultation and possible death of reported AIDS cases. Since a common code is used to recordeach case, whether HIV-positive or AIDS, it is possible to avoid multiple counting and also to link the twodatabases.

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 41
0
5
10
15
20
25
30
35
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
%
HIV with IVDU : all ages HIV with IVDU : 15-24 yr
Figure 3 : Percentage of IDUs among new HIV-cases from 1986 to 2001 in Belgium (all agesand 15-24 years)
0
5
10
15
20
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
%
HIV with IVDU : males HIV with IVDU : females
Figure 4 : Percentage of IDUs among new -cases from 1986 to 2000 in Belgium, according tosex
3.3.a.2 HIV sero-positivity among drug users
In 2001, results of the snowball survey (already described in 2.3.c), 1051 drug users wereinterviewed, the mean age is 29,5 years. Current injectors (during the last 6 months)represent 46%. The mean age for first injection was 19 years (range :10-32). Amongthese injectors, 266 reported to have been tested for HIV seropositivity and for 12 of them
PART 2 Epidemiological Situation
Belgian National Report on drugs 200242
reported to be HIV positive yielding a self reported prevalence rate of 4.5% (Hariga F.,personal communication).
3.3.a.3 HIV sero-positivity among treated patients
In the French community, information on the infectious status of clients is collectedthrough the CCAD/EUROTOX monitoring system. The information is based on self-reporting. In the Flemish part of the country, biological data on infectious status areprovided by “De Sleutel” which is an organisation bringing together several ambulatoryand residential treatment centres in Flanders. Biological testing for HIV, hepatitis B and Cis performed only for the clients seeing a doctor. Criteria for seeing a doctor are not linkedto the type and/or the way of product-use, but all clients getting substitution and/or othermedication do see a doctor.
A declining trend since 1994 is observed both in the Flemish and French part of thecountry (table 13).
Table 13 : Percentage of self-reported HIV-seropositivity among IDUs asking fortreatment in centres of the French and Flemish Communities, 1993-2000
Year 1993 1994 1995 1996 1997 1998 1999 2000
French Community
Number of treatmentdemands from IDUs
654 607 550 666 620 505 697 412
Number of self reportedIDUs
296 270 255 314 294 255 217 128
% HIV + (self reported) 6,1 7,4 3,1 1,3 2,7 2,7 2,3 3,1
Flemish Community
Number of treatmentdemands from IDUs
236 75 352 303
Number of tested IDUs 120 56 186 161
% HIV+ (tested) 0,8 5,4 0,5 1,2
A seroprevalence study was made on patients seen at the outpatient clinic “Free Clinic” inAntwerp between January 1 and June 30, 2001. In this 6-month period 477 individualsvisited the clinic, 337 (71 %) of them were male and 140 (30 %) were female (Matheï C.,personal communication). The age distribution in this population varied between 25 and58 years. The mean age was 35 years. 70 % individuals reported to have used drugs byintravenous way at least once in their live.HIV seroprevalence data are available for 336 out of the 477 patients (70 %). Seventeenindividuals (5.1 %) were anti-HIV positive. Fifteen of them were intravenous drug users;this means a seroprevalence of 5.9 % (table 14).

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 43
Table 14 : Sero-prevalence of HIV in an outpatientclinic, Antwerp, 2001
IDU Anti-HIV+
YesNo
5.9 % (254)2.4 % ( 82)
Total 5.1 % (336)sample size into brackets
3.3.a.4 HIV sero-positivity among prisoners
Different studies were carried out in different prisons about the HIV status, but drug useand administration route are normally not known. The most recent results come from astudy in the prison of Lantin (Wallonia), where serological testing is performed on requestof either prisoners or doctors. In 2000, 7 of the 740 tested prisoners (0.95 %) werediagnosed HIV-positive. In 2001, 6 on the 573 tested prisoners were diagnosed HIV-positive (1.05%) (Service de santé de l’administration des établissements pénitentiairepersonal communication).
3.3.b Hepatitis B and C
In Belgium, IDU seems to be the first cause of HCV contamination at this time (Delwaideet al. 1997). The other sources of transmission, such as transfusion of blood and itsderivates, mother-child exchanges, sexual and family contamination and medical care areless frequent.In Belgium, current hepatitis C prevalence in the general population is estimated to bearound 1 % (Beutels et al. 1997).
3.3.b.1 HBV- and HCV sero-positivity among treated patients
Although based on different methods, respectively self-reporting in the French communityand biological diagnosis (anti-HBc) from a sample of ambulatory and residential centres inFlanders (“De Sleutel”), prevalence rates are quite similar for HBV, around 20-25 % (table15). They don't show any particular trend over the last 3 years.
The prevalence of self-reported HBV infection in surveyed lifetime IDUs registered in themonitoring system of the French community increases with age (table 15). The sametrend is observed from the sample of ambulatory and residential treatment centres from“De Sleutel” (De Sleutel 2000;table 15).
Data on prevalence of HBsAg (first biological marker of the viral infection detectable inserum) are available from “De Sleutel” : they show an increase from 0 % (0/116) in 1997to 7.4 % (14/190) in 1999 but a decrease to 2.6 % in 2000 (4/154). One should becautious in interpreting these data because biological testing is performed only for theclients seeing a doctor and there are no guidelines with criteria specifying the patients tobe tested.

PART 2 Epidemiological Situation
Belgian National Report on drugs 200244
Among lifetime IDUs, i.e. IDUs having injected at least once, hepatitis C appears to bemore prevalent than hepatitis B (tables 15 and 16). Between 1997 and 1999, around halfof the lifetime IDUs registered through the monitoring system of the French Community,having declared having been tested reported they were found positive for hepatitis C(table 16). Between 1997 and 2000, around 40 % of tested lifetime IDUs patients of “DeSleutel” have antibodies against hepatitis C.
In 1999, in the French Community, 20/229 IDUs reporting having been tested for hepatitis(9 %) stated being both HBV- and HCV- positive.
Table 15 : Percentage of hepatitis B infected among IDUs asking for treatment, incentres of the French and Flemish Communities, 1997-2000
HBV 1997 1998 1999 2000
French Community
Number of treatment demands from IDUs 620 505 697 412
Number of IDUs tested (self-reported) 115 240 195 127Number of hepatitis B + (self-reported) 27 57 39 20
% hepatitis+ of total IDUs 23 24 20 16
% infected in males 21 22 27 16% infected in females 28 29 19 15% infected in age <25 14 18 10 7
% infected in age 25-34 25 22 21 16% infected in age >34 33 35 26 22
% infected in opiate using IDUs 23 24 21 16% infected in IDUs not using opiates 25 18 17 15
Flemish Community
Number of treatment demands from IDUs 236 75 352 303
Number of IDUs tested 73 54 155 123Number of hepatitis B +(anti-HBc+) 15 13 37 27
% hepatitis+ of total IDUs 21 24 24 22
% infected in males 23 23 28 22
% infected in females 8 33 7 20
% infected in age <25 11 7 12 8
% infected in age 25-34 27 21 26 26
% infected in age >34 57 50 44 42
The prevalence of HCV infection in tested IDUs (having injected at least once) registeredby the CCAD/EUROTOX system (self-reported status; Hariga F., Eurotox, personalcommunication) increases also with age but to a smaller extend than for hepatitis B; theincrease is more important in de “De Sleutel” data (De Sleutel 2000) (HCV Ab+; table 16).

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 45
Table 17 gives the results of a serologic study carried out among patients attending anoutpatient clinic in Antwerp between January 1 and June 30, 2001. Details on this studyhave already been presented in the section 3.3.a.3. Hepatitis B and C status is known for328 (69 %) individuals (Matheï C., personal communication). The prevalence of anti-HBcwas 43 % among the intravenous drug users compared to 20 % among the non-intravenous drug users. The prevalence of anti-HCV within the group of intravenous drugusers was 80 % compared to 17 % in the group of non-intravenous drug users.
Table 17 : Sero-prevalence (%) of HBV and HCV in anoutpatient clinic, Antwerp, 2001
IDU Anti-HBc+ Anti-HCV+
YesNo
43 (249)20 ( 79)
80 (252)17 ( 76)
Total 38 (328) 65 (328)sample size into brackets
3.3.b.2 HBV- and HCV sero-positivity among prisoners
In the prison of Lantin (Wallonia), in 1999, respectively 8% (51/664 prisoners) and 28%(191/677) were diagnosed respectively HBV- (HBsAg) and HCV-positive. In 2000, 4%(27/708) were positive for HBsAg and 25% (184/741) tested prisoners were HCVpositive. In 2001, 5,4% (31/576) were positive for HbsAg and 27.7% (167/603) HCV
Table 16 : Percentage of hepatitis C infected among IDU asking for treatment, incentres of the French and Flemish Communities,1997-2000
HCV 1997 1998 1999 2000
French Community
Number of treatment demands from IDUs 620 505 697 412
Number of IDUs self-reported 115 240 195 127
Number of hepatitis C + self-reported 54 124 100 66
% hepatitis+ of total IDUs 47 52 51 52
% infected in males 46 49 49 52
% infected in females 48 60 57 52
% infected in age <25 41 47 32 27
% infected in age 25-34 46 49 57 54
% infected in age >34 67 58 54 57
% infected in opiate using IDUs 44 53 56 48
% infected in IDUs not using opiates 62 39 59 63
Flemish Community
Number of treatment demands from IDUs 236 75 352 303
Number of IDUs tested 114 56 195 164
Number of hepatitis C + (biological testing) 45 26 74 59
% hepatitis+ of total IDUs 40 46 38 36
% infected in males 40 40 39 34
% infected in females 39 100 30 47
% infected in age <25 25 21 14 16
% infected in age 25-34 53 52 51 45
% infected in age >34 77 62 63 60

PART 2 Epidemiological Situation
Belgian National Report on drugs 200246
positive (Service de santé de l’administration des établissements pénitentiaire personalcommunication).
3.3.c Tuberculosis
In Belgium, 1,321 new cases with tuberculosis were registered in 2001 (incidence rate :12.9/100,000 inhabitants, Fares/VRGT 2002). Risk factors were recorded: drug addictionwas stated for 7 cases in Brussels and for 6 cases in Wallonia, representing in both area2% of new tuberculosis cases.
3.4. OTHER DRUG RELATED MORBIDITY
3.4.a Non-fatal drug emergencies
No information gathered.
3.4.b Psychiatric co-morbidity
No information gathered.
3.4.c Drugs and driving
From August 1999 until September 2000, a number of drivers have been tested, a part ofthem in the framework of the European Rosita-study (more information: www.rosita.org).Most of the drivers were tested during roadside controls in the neighbourhood of bigdiscotheques and after-clubs. About 500 drivers have been tested positive for drugscontrolled by the law of 16/03/99 (amphetamines, methamphetamines, cocaine, heroinand tetrahydroxycannabinol). One hundred thirty-three among these were detectedduring the Rosita-study. About 40 % of them (N = 55) were under influence of more thanone drug (table 18). Not mentioned are alcohol, medication or other illegal drugs.
Table 18 : Number of drivers andnumber of substances for which theywere tested positive in the Rosita-study,1999-2000
Number ofdrugs
N %
1 78 592 41 313 12 94 2 1
Some of these drugs are unspecified. There are no exact data on the combinations ofdrugs found, but there are data on the frequency of a drug (table 19).

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 47
Table 19 : Frequency of occurrence of the substancescontrolled by the law of 16/03/99 in the samples tested positiveduring the Rosita-study
Number of drugs N %Cannabis 95 50Amphetamines and methamphetamines 60 32Cocaine 24 13Opiates 9 1

Belgian National Report on drugs 2002
CHAPTER 4. Social and legal Correlates and Consequences
4.1. SOCIAL PROBLEMS
In previous reports, information on social problems was presented according to the TDIdata collection. For the same reasons as explained in section 3.1, TDI data are notpresented. Nevertheless, see chapter 16 for related matters.
4.2. DRUG OFFENCES AND DRUG RELATED CRIME
The Belgian General Police Support Service (SGAP/APSD) collects data from all policeservices in Belgium, specifically the municipality polices (mainly oriented to the localtrafficking), the judicial police and the gendarmerie/Rijkswacht (local, national andinternational trafficking) and the customs (national and international trafficking).
Two sources of information are used. Police's reports sent by units of Judicial Police,'Gendarmerie/Rijkswacht 9' and municipality polices to the Court are the first one. From1994 to 1997, six variables were available: identification number of the report,identification of the involved unit, type of infringement, tentative or not, location and time ofthe infringement. From 1998 onwards, the covered variables will be expanded (a.o. thetype of drug will be available).The second source is the 'unique form' (formulaire uniforme/eenvormig formulier) that arealso transmitted by Customs and Accises (Taxes) when a seizure is performed. The aimof this form was initially to stimulate the exchange of operational information between thedifferent police units. Although it is estimated that these forms are not systematically used(used for around 50% of infringements), interesting information is included as type andquantity of seized drugs.
A large re-organisation of the forces of police was initiated in 1998: a unique police forceresulting from the merging of the Judicial Police, the 'Gendarmerie/Rijkswacht' and themunicipality polices will be constituted. Simultaneously the development andimprovement of a unique database used directly by all services of police for theregistration of their repressive activities is in progress.
The interpretation of the national criminal statistics on the seizure of narcotics calls forsome explanation. The statistical data on the seizure of narcotics is based exclusively onthe positive results of searches or investigations but by no means reflects the number ofinfringements committed in this field. On the other hand, these figures do not provide anyinformation on the severity of the infringement, nor on the importance of the seizure.Since 1993, a distinction was made for the first time between the use and the trafficking ofnarcotics. The term use is applied to narcotics seized from a person who had them in hispossession but only for personal consumption. The term trafficking is applied to all
9 The reports of the Gendarmerie/Rijkswacht units are also centralised at BCR/CBO (Bureau Central de
Recherche - Programme Drogue / Centraal Bureau voor Opsporing – Programma Drugs / Centralinvestigation office – Drug programme). Some units of the municipality police also report to this central'Gendarmerie/Rijkswacht' office. Data are kept in a database called POLIS. Data are related to theinfringements (type, location, date). Drugs classified according categories (cannabis, opiates, LSD,…) arementioned in most of cases. For the identification of the substance, the Becton-Dickinson test as well asthe experience of the policeman are used. Following information is available: involved person, vehicleused, modus operandi, tools used. There is no information on the seizure or not of substances neither ontheir weight.
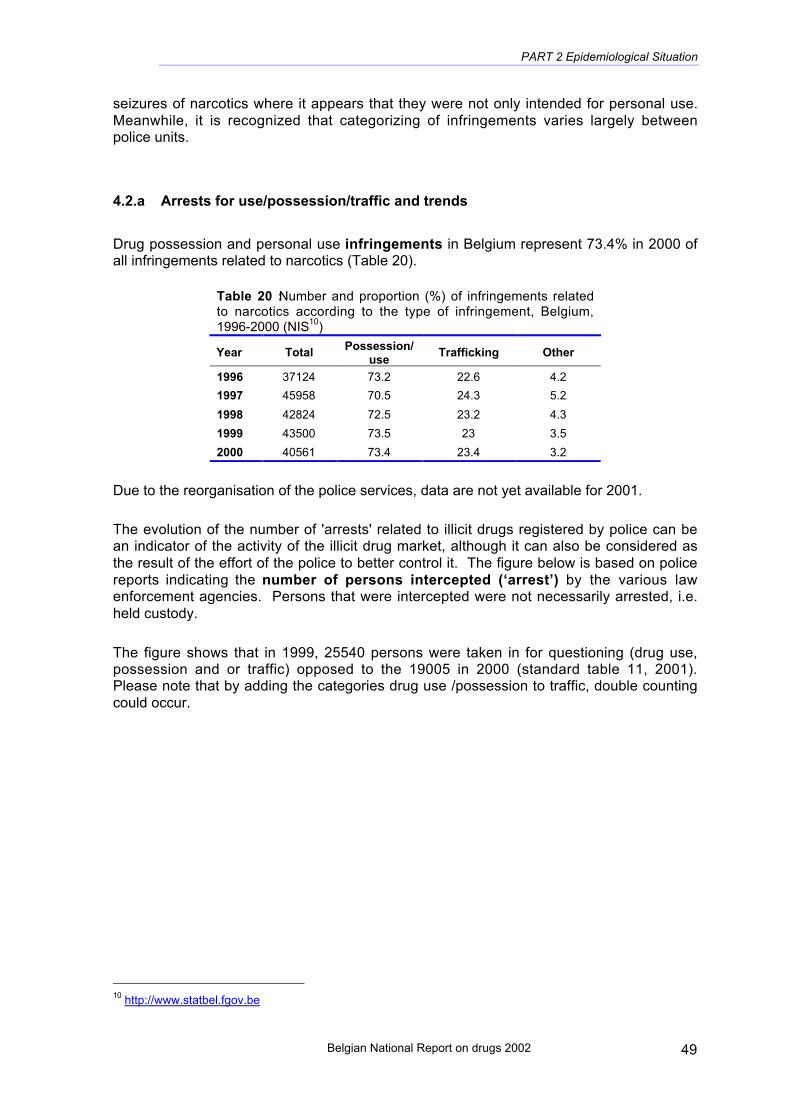
PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 49
seizures of narcotics where it appears that they were not only intended for personal use.Meanwhile, it is recognized that categorizing of infringements varies largely betweenpolice units.
4.2.a Arrests for use/possession/traffic and trends
Drug possession and personal use infringements in Belgium represent 73.4% in 2000 ofall infringements related to narcotics (Table 20).
Table 20 : Number and proportion (%) of infringements relatedto narcotics according to the type of infringement, Belgium,1996-2000 (NIS10)
Year Total Possession/use
Trafficking Other
1996 37124 73.2 22.6 4.2
1997 45958 70.5 24.3 5.2
1998 42824 72.5 23.2 4.3
1999 43500 73.5 23 3.5
2000 40561 73.4 23.4 3.2
Due to the reorganisation of the police services, data are not yet available for 2001.
The evolution of the number of 'arrests' related to illicit drugs registered by police can bean indicator of the activity of the illicit drug market, although it can also be considered asthe result of the effort of the police to better control it. The figure below is based on policereports indicating the number of persons intercepted (‘arrest’) by the various lawenforcement agencies. Persons that were intercepted were not necessarily arrested, i.e.held custody.
The figure shows that in 1999, 25540 persons were taken in for questioning (drug use,possession and or traffic) opposed to the 19005 in 2000 (standard table 11, 2001).Please note that by adding the categories drug use /possession to traffic, double countingcould occur.
10 http://www.statbel.fgov.be
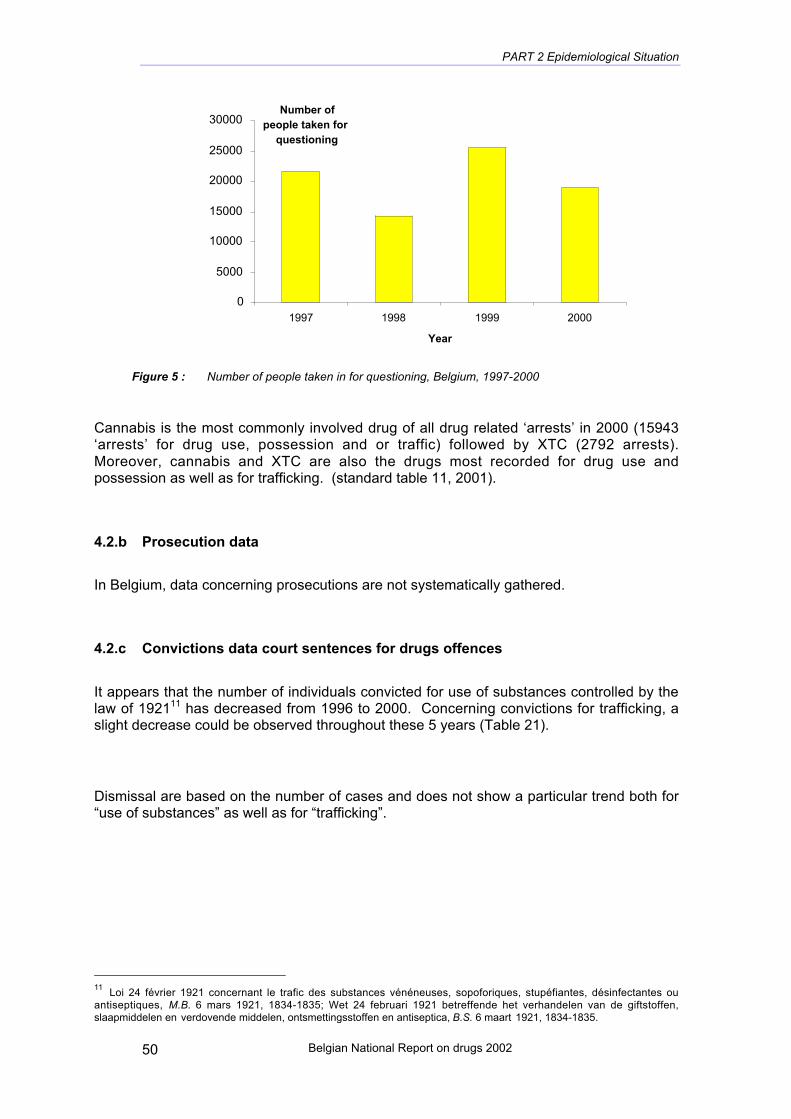
PART 2 Epidemiological Situation
Belgian National Report on drugs 200250
0
5000
10000
15000
20000
25000
30000
1997 1998 1999 2000
Year
Number of people taken for
questioning
Figure 5 : Number of people taken in for questioning, Belgium, 1997-2000
Cannabis is the most commonly involved drug of all drug related ‘arrests’ in 2000 (15943‘arrests’ for drug use, possession and or traffic) followed by XTC (2792 arrests).Moreover, cannabis and XTC are also the drugs most recorded for drug use andpossession as well as for trafficking. (standard table 11, 2001).
4.2.b Prosecution data
In Belgium, data concerning prosecutions are not systematically gathered.
4.2.c Convictions data court sentences for drugs offences
It appears that the number of individuals convicted for use of substances controlled by thelaw of 192111 has decreased from 1996 to 2000. Concerning convictions for trafficking, aslight decrease could be observed throughout these 5 years (Table 21).
Dismissal are based on the number of cases and does not show a particular trend both for“use of substances” as well as for “trafficking”.
11 Loi 24 février 1921 concernant le trafic des substances vénéneuses, sopoforiques, stupéfiantes, désinfectantes ouantiseptiques, M.B. 6 mars 1921, 1834-1835; Wet 24 februari 1921 betreffende het verhandelen van de giftstoffen,slaapmiddelen en verdovende middelen, ontsmettingsstoffen en antiseptica, B.S. 6 maart 1921, 1834-1835.
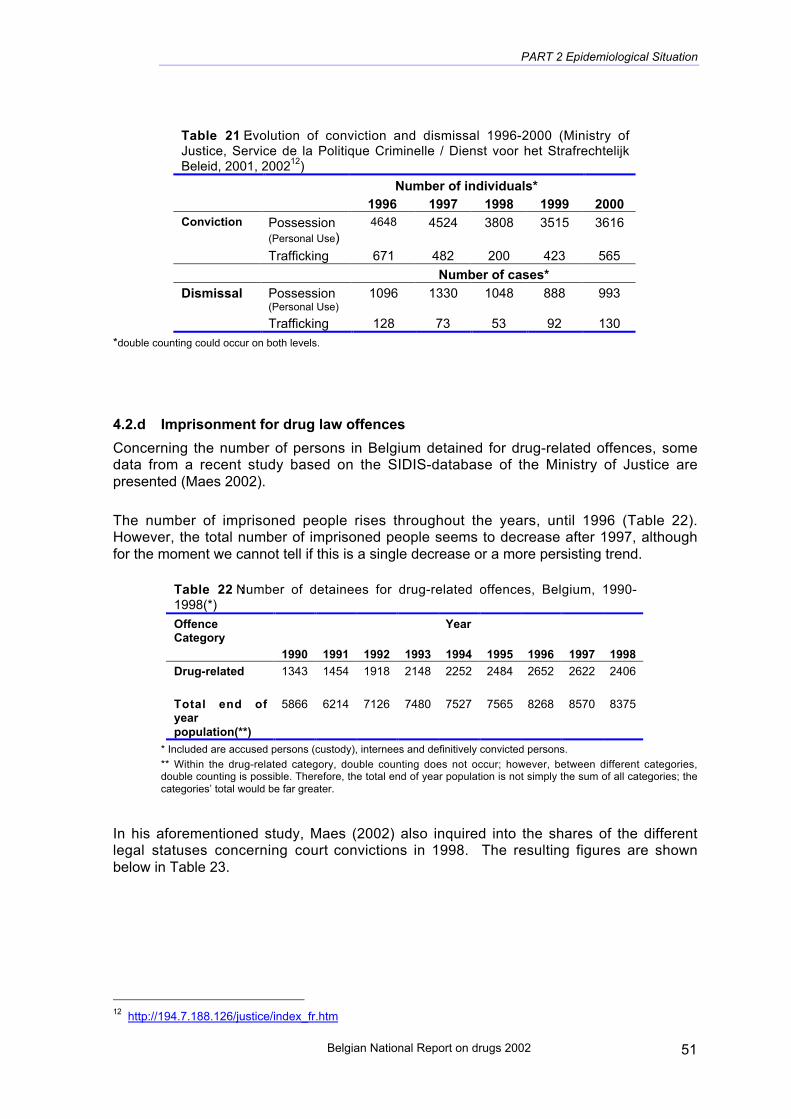
PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 51
Table 21 : Evolution of conviction and dismissal 1996-2000 (Ministry ofJustice, Service de la Politique Criminelle / Dienst voor het StrafrechtelijkBeleid, 2001, 200212)
Number of individuals*1996 1997 1998 1999 2000
Conviction Possession(Personal Use)
4648 4524 3808 3515 3616
Trafficking 671 482 200 423 565
Number of cases*
Dismissal Possession(Personal Use)
1096 1330 1048 888 993
Trafficking 128 73 53 92 130
*double counting could occur on both levels.
4.2.d Imprisonment for drug law offences
Concerning the number of persons in Belgium detained for drug-related offences, somedata from a recent study based on the SIDIS-database of the Ministry of Justice arepresented (Maes 2002).
The number of imprisoned people rises throughout the years, until 1996 (Table 22).However, the total number of imprisoned people seems to decrease after 1997, althoughfor the moment we cannot tell if this is a single decrease or a more persisting trend.
Table 22 : Number of detainees for drug-related offences, Belgium, 1990-1998(*)
OffenceCategory
Year
1990 1991 1992 1993 1994 1995 1996 1997 1998
Drug-related 1343 1454 1918 2148 2252 2484 2652 2622 2406
Total end ofyearpopulation(**)
5866 6214 7126 7480 7527 7565 8268 8570 8375
* Included are accused persons (custody), internees and definitively convicted persons.
** Within the drug-related category, double counting does not occur; however, between different categories,double counting is possible. Therefore, the total end of year population is not simply the sum of all categories; thecategories’ total would be far greater.
In his aforementioned study, Maes (2002) also inquired into the shares of the differentlegal statuses concerning court convictions in 1998. The resulting figures are shownbelow in Table 23.
12 http://194.7.188.126/justice/index_fr.htm

PART 2 Epidemiological Situation
Belgian National Report on drugs 200252
Table 23 : End of year population (%) for drug-related offences perlegal status, Belgium,1998
OffenceCategory
Accusation(custody)
Internment Final Conviction (*)
£ 5years
+ 5years
Total(Convicted)
Drug-related 19.2 1.9 44.1 33.9 78.0
* Persons in prison as a replacing sentence are not included
4.2.e Other drug-related crime
Specific information on theft, violence and other drug related criminality was not gathered.
4.3. SOCIAL AND ECONOMIC COSTS OF DRUG CONSUMPTION
4.3.a Studies and estimates of health care costs, other social costs
See chapters 1 & 14.
4.3.b Estimates of total consumption/demand/expenditure on drugs
No information gathered.

Belgian National Report on drugs 2002
CHAPTER 5. Drug Markets
5.1. AVAILABILITY AND SUPPLY
5.1.a Availability and access to different drugs, trends
The continuous monitoring of the health behavior in the French Community (1996-99)reports that two thirds of adults aged 18-49 years believe possible to get cannabis and45% cocaine near to their house (Piette and De Smet 2000).
In the qualitative study ‘Youngsters in Brussels’, 22 teenagers of Brussels (14 boys, 8girls, 13-18 year old) were interviewed in July 1997 (Kohn and Piette 1997). They statedthat cannabis is available everywhere: from friends, in The Netherlands, during festivals,in youngster-house, at school.
5.1.b Sources of supply and trafficking patterns
Information on supply and trafficking patterns is collected for the Belgian Questionnairerequested for the UNDCP annual report.
The final destination of a large part of the seizures, involving residents in Belgium, is oftenEuropean countries and more precisely, UK, The Netherlands and France.
• Heroin would mainly come from the Balkans’ road.
• It appears that importations of cocaine (from Latin America) in Belgium are performedby those who export XTC from Belgium to Latin America.
• Marihuana seems to be produced in the Netherlands (90%) and 80 % of haschishcome from Morocco.
• XTC 20% of XTC in Belgium come from The Netherlands and the other 80% would beproduced in Belgium. XTC is then exported to US (30%), UK (20%) and othersEuropean countries.
5.2. SEIZURES
The trends over the period 1985-2000 as far as the number of seizures of cannabis,heroin, cocaine and XTC/amphetamines are concerned cannot be easily specifiedbecause data on seizures are not available for the years 1996 and 1997.
Data on the seized quantities for these drugs are however available for the last decade.The quantities of seized cannabis have regularly increased from 9,504 kg in 1992 to106,690 kg in 1996 (Figure 6). They decreased considerably during the period 1997 to2000 to reach the levels observed during the period 1990-1991 (less than 20,000 kg).The quantities of seized heroin have greatly fluctuated from year to year without a clear

PART 2 Epidemiological Situation
Belgian National Report on drugs 200254
pattern; the highest quantity of heroin being seized in 1990 (291 kg). The quantities ofseized cocaine exhibit an erratic increasing trend. First, there was an exponentialincrease from 1985 to 1993, followed by a sharp decline during the period 1994-96. Asudden rise occurred in 1997 when the highest seized quantities (3,321 kg) wereobserved. Finally, a significant decrease took place during the period 1998-2000. Thequantities of XTC/amphetamines pills seized appeared to increase in an exponential wayfrom 1990: for instance, the quantities of amphetamines and XTC seized in 2000 (morethan 800,000 pills) almost double in comparison to the quantities seized in 1999 (about490,000 pills, Figure 6).
In addition, the number of seizures and the seized quantities were not correlated forcannabis and heroin whereas a strong correlation exists between the number of seizuresand the seized quantity for cocaine and XTC/amphetamines.
1985 1990 1995 2000
0
30
60
90
120
Cannabis (quantity seized x 1000 kg)
1985 1990 1995 2000
0.0
0.1
0.2
0.3
Heroin (quantity seized x 1000 kg)
1985 1990 1995 2000
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Cocaine : quantity seized x 1000 kg
1985 1990 1995 2000
0
250
500
750
1000
XT
C : quantity seized x 1000 pills
Figure 6 : Quantities of products seized, 1985-2000, Belgium.

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 55
Large yearly variations exist in the quantities seized in Belgium. They could be the resultof the collaboration between countries in the fight against traffickers : indeed the currentpolicy/strategy when a traffic is discovered, consists in postponing the intervention (arrestof the traffickers and seizure of the drugs) and to follow the travel in order to be moreefficient by discovering the organization of the distribution, the partners in crime, etc… Sosuch data on quantities will be better interpreted at larger (European) level.
5.3. PRICE/PURITY
Table 24 : Mean price in Euros at street level of some illegal substances : Belgium, 1996-2001
DRUG 1996 1997 1998 1999 2000 2001
Cannabis resin(per gram)
8.1(3.7-12.4)*
3.1(2.5-3.7)
7.4 8.1(6.2-9.9)
5.6(5.0-6.2)
7.3(3.7-12.5)
Cannabis leaves(per gram)
5.0(2.5-7.4)
3.7(2.5-5.0)
6.5 5.6(3.7-7.4)
4.2(3.4-5.0)
7.9(3.7-12.5)
Heroin brown(per gram)
37.2 22.3(19.8-24.5)
21.1 39.7(19.8-59.5)
26.8(18.8-34.7)
30.7
(12.5-50)
Cocaine powder(per gram)
49.6(37.2-62.0)
55.8(49.6-61.2)
58.9 55.8(37.2-74.4)
60.1(45.9-74.4)
53.4
(42.2-64.6)
Amphetaminespowder(per tablet)
- - - 7.9(6.0-9.9)
5.0(3.7-6.2)
11.9(9.4-14.4)
'Ecstasy'(per tablet)
12.4 6.5 8.7 7.2(4.5-9.9)
7.3(5.7-8.9)
6.3(3.7-13.1)
LSD(per dose)
6.2(5.0-7.4)
6.8(5.0-8.7)
6.9 - 3.1(2.5-3.7)
8.7
(7.4-9.9)
* Minimum and maximum price are given in parenthesis.No figures on crack trafficking are available (very minimal consumption)
For 2001, data on 718 analyses performed by 9 laboratories were collected in theframework of the EWS (see annex 1 for more information). It concerns analyses of seized
Table 25 : Mean purity at street level of some illegal substances, Belgium, 2000-2001
2000 (1) 2001 (1)
DRUG Number ofanalyses
Mean(Minimum-maximum)
Number ofanalyses
Mean(Minimum-maximum)
Cannabis resin (2) 10 7.1(0.9-18.1)
11 13.6
(0.9-26.9)
Cannabis leaves :’nederwiet’
30 10.4(0.8-21.9)
8 6(0.15-16.7)
Heroin brown 29 30.6(4-62)
Heroin white
2210
21.9(2-65)
64.7(15.9-95)
- -
Cocaine 199 68.6(8-99.3)
80 63
(19-100)
Amphetamines 65 9.8(0.2-49.6)
31 22.4
(2-54.1)(1) : the percentages are not weighted because the exact amount of sample on which the analysis was doneis not known,(2) : % HTC content.

PART 2 Epidemiological Situation
Belgian National Report on drugs 200256
products. Some data are not included in the abovementioned number, such asincomplete data, data of traces of drugs found in cars and data of products found inclandestine laboratories for they do not represent the drugs circulating at users’ level.
In 565 analysed samples (80 %), one “controlled” substance of the same category (i.e. asubstance listed in the UN 1971 Convention on Psychotropic Substances) was found,sometimes combined with an adulterant (e.g. caffeine) or a diluent (e.g. sugar). In somecases (N = 39; 5 %), controlled substances of different types were found in combination inone analysed sample. In 15 % of the cases (N = 114), the analysed sample does notcontain any substance controlled under the UN Schedules. Note that this class does notcoincide with the category ‘other’. The category other also comprises substances that arescheduled, such as hormones and psychiatric medicines.To determine the distribution of each of the individual substances, the frequency ofoccurrence of every substance is considered. Thus, samples that contained more thanone substance were counted for each substance. The distribution for 2001 is shown intogether with the distribution for 2000 (Table 26). It is important to note that thesepercentages reveal nothing about the amounts of the seized drugs; they give only anindication of the frequency wherewith a specific drug was found in the samples receivedby the laboratories.
Table 26 : Distribution of substances in samples of drugs seized in 2000 and 2001
2000 2001N % N %
Amphetamines 132 11.2 83 10.8Cannabis 132 11.2 91 11.9Cocaine 228 19.4 100 13.1GHB 37 3.2 23 3.0Hallucinogens 9 0.8 5 0.7Opiates 79 6.7 82 10.7Ringsubstitutedamphetamines
336 28.6 225 29.4
Other 221 18.8 156 20.4
Total 1174 100 765 100
Just as in 2000, the ringsubstituted amphetamines are the most represented category in2001. Only the category cocaine represented a significantly bigger share (P < 0.001) in2000 than in 2001. The proportion of opiates on the other hand is higher (P < 0. 01) in2001 than in 2000. For the other categories, the percentages in 2001 are comparable tothose in 2000.
About 45 % (N = 324) of the samples analysed in 2001 contain controlled substances ofsynthetic origin, namely amphetamines, ringsubstituted amphetamines, GHB and somehallucinogens. This percentage is the same as the percentage found in 2000 (N = 491).Table 27 compares the distribution of the synthetic drugs analysed in 2000 and 2001.Sometimes a sample is composed of a combination of an amphetamine and aringsubstituted amphetamine (N = 9). In some cases (N = 8), two types of ringsubstitutedamphetamines were found in one sample. This explains why the total amount of syntheticsubstances is different from the sum of the numbers of amphetamines (N = 83),ringsubstituted amphetamines (N = 225), GHB (N = 23) and the synthetic hallucinogens(N = 2).

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 57
Table 27 : Distribution of synthetic drugs in samples of drugs seized in 2000and 2001
2000 2001
Substances N % N %
Ringsubstituted AmphetaminesMDMA 311 59.1 217 63.6_-PEA, piperonal, safrol, formyl-MDMA, PMK* 13 2.5 5 1.5MDE (or MDEA) 9 1.7 4 1.2MDA 14 2.7 3 0.92C-B (BDMPEA) 0 0 3 0.9PMA 0 0 1 0.34-MTA 3 0.6 0 0DOB 2 0.4 0 0AmphetaminesAmphetamine/ methamphetamine 132 25.1 82 24.0BMK** 0 0 1 0.3GHB 37 7.0 23 6.7LSD 4 0,8 2 0.6Ketamine 1 0.2 0 0
Total 526 100 341 100* Precursors or impurities of ring-substituted amphetamines (PMK= 3,4- methylenedioxyphenyl-2-propanone)
** Precursor of amphetamine (benzylmethylketone or phenylacetone)
The ringsubstituted amphetamine MDMA (better known as XTC) is the most representedsynthetic drug (63.6 %) in 2001. Other ringsubstituted amphetamines are: MDE (1.2 %),MDA (0.9 %), 2C-B (0.9 %) and PMA (0.3 %). In 1.5 % of the cases, a precursor orimpurity of a ringsubstituted amphetamine was found alone.

Belgian National Report on drugs 2002
CHAPTER 6. Trends per Drug
6.1. CANNABIS
Available information suggests the following facts:
- the use of cannabis in adult and secondary school population is increasing overthe 1990’s;
- one adult out of five (18-49 years old) in the French Community experiencedcannabis at least once (corresponding to the European mean figure);
- the lifetime prevalences of cannabis use among young people aged 15-16 years isregularly increasing from 15 to 21 %; over the period 1994 - 2000;
- the proportion of patients starting treatment reporting cannabis use as the cause oftheir main problems is increasing;
- cannabis is the cause of 70% of the cases in which people are taken in forquestioning (stable);
- the number of seizures considerably fluctuates from year to year;- the retail price is relatively stable;- most of adults stated that they could get cannabis quite easily near to their home.
6.2. SYNTHETIC DRUGS
Available information suggests the following facts:
- the estimate of lifetime prevalence of XTC use in adult is out-dated : a very low,lifetime prevalence, less than 1%, was found in 1994 in the Flemish Community;
- from 15-16 years of age onwards, XTC (and other club drugs) are the secondproduct most used (after cannabis);
- at the age of 15-16 years, a slightly increasing proportion of students (reaching 4%in VAD 2000 surveys - respectively 3.6 % in boys and 6.7 % in girls -) experiencedXTC;
- among XTC users less than half used XTC during the last month; however, theproportion of ‘regular’ users among XTC users increases : respectively 34-36-45 %in 1994, 96 and 98;
- the proportion of patients starting treatment and reporting XTC as their mainproblematic drug does not seem to increase; in centres participating to the FlemishVAD monitoring system, XTC and stimulants users (not including cocaine)represent 20.2% of clients in 1999 but only 15% in Brussels CTB-ODB (includingcocaine) and around 3% in CCAD/EUROTOX system (such discrepancies seemsto be attributable to differences in the coverage of the different type of treatmentcentres);
- XTC is the cause of a varying proportion the cases in which people are taken in forquestioning;
- the number of seizures increased during recent years;- the retail price is declining reaching the mean price of 6.3 Euro for a tablet in 2001;- no information on accessibility in adults is available.
PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 59
6.3. HEROIN OPIATES
Available information suggests the following facts:
- the estimate of lifetime prevalence of opiates and heroin use in adult generalpopulation is out-dated : a very low lifetime prevalence, less than 0.1%, was foundin 1994 in the Flemish Community;
- at the age of 15-16 years, a low proportion of students experienced heroin use:less than 1% (stable) in Flemish surveys but 1.5% in the French Community(HBSC survey);
- the proportion of patients starting treatment of heroin/opiates addiction as thecause of their main problems seems decreasing over the period 1993-1999;
- injection behaviour among heroin users starting treatment is quite stable (incontrast to the global trend in treatment centres due to the relative increase ofpeople treated for non-injectable drug);
- heroin/opiates are the cause of a varying proportion of the cases in which peopleare taken in for questioning;
- the number of seizures decreased during recent years;- the retail price has been stable since 1995;- no information on accessibility in adults is available.
6.4. COCAINE CRACK
Available information suggests the following facts:
- the estimate of lifetime prevalence of cocaine use in adult general population isoutdated: a very low lifetime prevalence, 0,5%, was found in 1994 in the FlemishCommunity;
- at the age of 15-16 years, a low proportion of students experienced heroin use:less than 2% in Flemish surveys and 1.4% in the French Community (HBSCsurvey);
- the proportion of patients starting treatment when cocaine is reported as the causeof the main problems seems increasing;
- injection behaviour among cocaine users starting treatment seems slightlyincreasing (in contrast to the global decreasing trend in treatment centres due tothe relative increase of people treated for non-injectable drug) and varies betweenmonitoring systems (remaining lower to heroin injecting behaviour though almostequal in French Community reporting systems).
- the number of seizures seems decreasing during recent years;
6.5. MULTIPLE USE
No new information available.

Belgian National Report on drugs 2002
CHAPTER 7. Discussion
7.1. CONSISTENCY BETWEEN INDICATORS
There is consistency between trends of some indicators : for example, increasingcannabis use among youngsters and also among adults, consistency between the variousschool surveys, high level of HCV among IDUs reported by all studies. Neverthelessreliability of most data remains relatively poor and should be improved in order to takedecisions on a more solid basis.
7.2. METHODOLOGICAL LIMITATIONS AND DATA QUALITY
Drug use among the school population appears to be the best documented. In generalthe quality of the data collected in school surveys is thought to be rather satisfactory. Mostof these surveys are conducted by or in close co-operation with experienced researchinstitutions or universities, repeating regularly the survey with the same methodology andthe same tools. In some cases the data have been validated by other researches. Schoolsurveys are conducted both in the Flemish and French Communities within the frameworkof the repeated WHO HBSC cross-sectional survey. At present, trends in drug use can bemade over the last decade both in the Flemish and French Communities. Other schoolsurveys are also conducted independently of the HBSC surveys in different areas of thecountry. Since these surveys are not standardized, it is difficult to compare their results.On the other hand, the implementation of these local surveys makes uneasy to carry outthe large standardised HBSC surveys : indeed some schools do not agree to participate inthe HBSC survey because of a recent participation in a local school survey. The majorityof studies conducted in schools are self-report surveys, using a paper-basedquestionnaire to be filled in during school time. No cohort research has been carried out.
Data on the lifetime and recent use of cannabis among adults living in the FrenchCommunity has been collected as part of a continuous monitoring of health behaviourcarried out from April 1996 to March 2001. Reliability of the collected data can however bequestioned since the survey was based on a computer assisted telephone interviewmethod with random dialling of the household and random selection of one adult, on onehand, and the response rate was low, on the other hand. A short module designed toestimate the lifetime and last month prevalence of cannabis and XTC/amphetamines usewas introduced in the 2001 edition of the national Health Interview Survey. Thequestionnaire is self-administrated and focuses on people aged 15-64 years. Results arecurrently analysed and will be published in the next annual report.
No information is available regarding the quality of epidemiological data collected in theframework of the key indicator TDI. The NFP has no full access to the data on thetreatment demand indicator provided by the different monitoring systems. The coverage ofthe registration systems, among other things, is not documented at all. Therefore the NFPcould not go through a formal quality control mechanism of the TDI data sent to theEMCDDA. In the National Report, the TDI data were usually presented separately foreach federate entity (Communities or Region) but could actually not be pooled to providenational figures because these data are not comparable between the different federate

PART 2 Epidemiological Situation
Belgian National Report on drugs 2002 61
entities. The feasibility to implement a national programme designed to set up a qualitycontrol mechanism will be investigated during next year.
The possibilities to estimate the prevalence of problematic drug use in Belgium havebeen investigated. The results of this study show that only one method could directly beapplied in Belgium. This method consists in using estimates of the prevalence of HIVamong problematic drug users and data related to drug users from the national HIV/AIDSregister which is though to make an exhaustive census of all HIV seropositive personsand all AIDS cases. The lifetime prevalence of injecting drug use in 1995 and in 1997 wasestimated in this way. The low prevalence of HIV among problematic drug users appearsto be the main factor influencing the reliability of the estimates. On the other hand, afeasibility study has been carried out in Charleroi in 2001-2002 in order to obtain localinformation on the prevalence of the problematic drug use through the “capture-recapture”method. The data collected during this survey are currently analysed. The possibility toimplement such approach in the other major Belgian cities will be considered.
The National Institute of Statistics provides data on drug-related deaths, which complywith the EMCDDA guidelines. Unfortunately, these data are out dated owing to thecomplexity of the administrative structure of the country. On the other hand, the number ofoverdoses registered by special registries (forensic or police) appears to be unreliable.
The different monitoring systems collecting TDI data provide some information on the HIV,hepatitis B and C status among treated drug users. Two factors may play a role inlimiting the confidence level of the estimated prevalence rate of infectious diseases: self-reporting of the infectious status and the very low response rate. However, more accurateestimates of the prevalence of HIV, hepatitis B and C among treated drug users can bederived from the measurements of biological markers carried out by two Flemishtreatment centres. It appears that prevalence estimated through self-reported data gives arough idea of the prevalence of infectious diseases estimated though biological testing.
Also insight on of new trends in drug (ab)use is important. In general more research isneeded on the social context of drug use, aiming at mechanisms of drug abuse,dependence, etc…
In conclusion, the global description of the situation and trends in drug consumption anddrug related problems remain incomplete. Therefore, it is urgent to make an importanteffort in order to improve the collection of reliable standardized data. The comparability ofthe data collected by the federate entities should be improved in order to make meaningfulcomparisons between the different parts of the country and to produce valid figures atnational level.

PART III. Demand Reduction Interventions
KÖTTGEN S.LAUDENS F.PECSTEEN D.TODTS S.VANDERVEKEN M.


CHAPTER 8. Strategies in Demand Reduction at National Level
8.1. MAJOR STRATEGIES AND ACTIVITIES
The main national strategies focus on health (for more information please refer to Part 1).However, at the federal level, there are a number of demand reduction projects from acrime prevention perspective (Ministry of Internal Affairs). The projects are given to localcommunes with higher than average crime statistics. After a recent evaluation of theseprojects, criteria for funding were revised taking into account socio-economic data such asnumber of inhabitants, resources of the commune in addition to criminality. The projectscover prevention and outreach. Some projects have set up their own structure at the locallevel and try to fill a gap in prevention or treatment facilities. Other projects are integratedin existing health centres. Up to now, the projects operated with annual contracts and willbe reconducted till 200313.In seven out of the 10 provinces of Belgium, a medical social low threshold centre(MSOC-MASS) is set up to deal with problematic drug users. The centres are located inthe major city of the province and provide treatment, counselling, outreach. The centresare financed partly through the social security system or by the Security and SocialContracts.The federal ministry of Social Affairs provides the financing for a number of TherapeuticCommunities, Crisis Centres and Day Centres, which were set up in the seventies and
13 For more information see website : http://vspp.fgov.be/f/cpsf.htm
Federal Level
Federal Ministry of SocialAffairs, Public Health and
Environment
Federal Ministry of InternalAffairs
Security and (Society)Prevention Contracts
Communities and Regions
Prevention (harm reduction)Treatment
Rehabilitation
Treatment

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 65
have expanded their capacities substantially in recent years. They are recognized on anindividual basis.
Communities and Regions, dealing with prevention and treatment are detailed in the nextsection.
8.2. APPROACHES AND NEW DEVELOPMENTS
8.2.a New and innovative approaches
In the federal drug policy paper, the concept of ‘treatment networks' is proposed asorganizational frame for the treatment of people with drug problems at a regional and/orprovincial level. The policy paper provides the set up of LCD (Local Co-ordination groupsDrugs) in which case management, and the development of circuits of care are promoted.The ‘Overlegplatforms Geestelijke Gezondheidszorg’ is the initiators of these LCD.
8.2.b Socio-cultural developments relevant to demand reduction
Drug use among young people is still on the rise. Drug use has become part of the youthculture of different groups of young people. They experiment with various (legal andillegal) drugs (poly drug use). Many sectors in society have come to realize that drug useamong young people exists and there is a growing motivation to deal with it.
Common key elements are more and more taken into account for preventioninterventions. First, young people experience real life problems during the criticaladolescent period: relational and psychological problems, such as the difficulty of gettingalong with their parents. The quality of relationships and the importance of dialoguebetween young people and adults are advocated by the majority as an essentialpreventive measure. It is crucial that young people get greater autonomy and individualresponsibility, which would allow them to deal with the very considerable role of peerpressure in experience, learning and therefore in dealing with the risk factors due toexposure. No moral approach is being used, yet each individual should be equipped tomake responsible choices.
With the emergence of HIV infection, AIDS and hepatitis, risk reduction new strategieshave been developed: needles exchange, treatment with substitution substances, anddistribution of condoms... The activities are a.o. undertaken within the security contractsof the Ministry of the Internal Affairs with local authorities.
8.2.c Developments in public opinion
No new study in 2001.
8.2.d New research findings
- Exploratory research of alcohol- and drug prevention in services for sociallydisadvantaged youth. Else De Donder, Johan Rosiers en Els vandenberghe. VAD (2001).The objective of the research is to find clues for new prevention strategies. After literacystudy an exploratory round was organised with key figures in youth services andresearchers. Five youth services were selected for further in-depth interviews. In total 22youngsters and 7 youth workers were interviewed.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200266
Even if the research population is not marked by an extensive drug use, drugs are a vastpart of their lives. All of them know drug users in their surrounding. The youthorganisations have an important preventive role, in general as well as drug specific. Thepositive interactions within these settings improve the self-image and the strong cohesionbetween youngsters and youth workers leads to care-taking relationships.Most of the youth services have an elementary drug policy, mostly based on houseregulations. Regulations have to be understandable and recognisable for the youngsters.The first premise demands an open communication, the second a participation of theyoung in the creation of the rules. The subject of drug use should be 'debatable' at alltimes. Group activities on the subject should certainly reflect the social world of the targetgroup. The survey revealed also some potential pitfalls in working on (drug) preventionwith socially disadvantaged youth.
- Recherche ethno-epidemiologique sur la consommation d’ecstasy et de “nouvellesdrogues” en Communauté francaise. Gilles Hacourt. Eurotox (2002).This research has been realised in March 2000 until October 2001. In total 364 personswere interviewed between 14 and 36 years old, non drug users, drug users,experimenters, selected in different settings (festivals, universities, mega-dancing’s…).The main aim of this research is a better knowledge of the phenomenon of synthetic drugconsumption in order to allow the development of politics and actions of harm reductionand prevention in accordance with the reality of the field.The survey shows that new synthetic drug users are not necessarily youngsters, sociallyintegrated, follower of techno music and mega-dancing’s. XTC concerns a more largepopulation. In majority (70%), the main motivation of people consuming XTC is theresearch of pleasure. Globally, the users report they try to control their consumption. Forexample, they pay attention to the context, to their psychological state. Most of theminquire as far as the information is estimated objective, without judgement and nonmoralistic. However, this “deliberate” consumption does not hinder they take risks. 40%declare having conducted under influence. 25% had sexual relationship withoutprotection. In generally, the users don’t consider themselves drug addicts. What concernsthe price, a pill is not so expensive anymore (20 Euro in 1989, nowadays 3 Euro).
8.2.e Specific events during the reporting year
- Policy note of the federal government on drug problems was issued on 19th January2001.
- VAD organised a conference on Alcohol (November 22th 2001). The study day provideda diverse program and zoomed in on the latest policy developments and researchfindings. The afternoon workshops included topics as: a total ban on alcohol use duringdriving, alcohol publicity, and the role of the GP in detecting problematic alcohol use. Theconference was closed with a presentation of the Dutch policy on alcohol followed by adiscussion with Flemish and federal policymakers.
- Cannapistes: “cannabis: maintenant que c’est ‘légal’: quelles nouvelles à Bruxelles14?”(13 novembre 2001): A prospecting day concerning the use of cannabis and theprevention, curative and socio-economical dispositions that should be implementedinsofar as this is legally accepted.
14 www.users.skynet.be/cannapistes

CHAPTER 9. Prevention
9.1. SCHOOL PROGRAMMES
NATIONAL STRATEGY
Prevention is not a responsibility of the federal government, but of the communitygovernments (see more details chapter 1).
ORGANISATION AND CO-ORDINATION WITHIN NATIONAL STRUCTURES
For the three communities, the strategies are based on:
- long term perspective,- global integrated approach,- data collection (Ginger data base for the Flemish Community ),- adult “multiplicator”,- no differences between sub-areas.
In the French Community, there is no official co-ordination structure (however, co-ordination exists at local level). In the Flemish and German Communities, VAD and ASL,work respectively as official co-ordination structures.
EXPENDITURES ON PREVENTION
Please refer to Key Issue 14.
9.1.a Specificities of policies
The drug policy at school consists of three levels: ‘plan’, ‘education’ and ‘intervention’. Theplan determines the boundaries of what is acceptable in the school. (For the FrenchCommunity, Hazette15 and for the Flemish Community ‘Drugbeleid op School16’ forsecondary schools and 'basic principles for drug prevention17 for primary schools).
It is important -among other things to start prevention programmes as soon as possible.The approach in kindergarten and primary schools is integrated within the framework ofhealth education and health promotion (in a wide sense: violence, communication, socialrelations, risks, etc.)Secondary education is based on the same framework, but is also characterized by moredrug specific activities and teaching packages. To motivate and facilitate healthybehaviour, repetition is necessary. In the part ‘intervention’, attention is given to theformation of networks around the school - including school, parents, school health service,
15 www.agers.cfwb.be/org/circulaires/16_05_02.pdf16 Set ‘Drugbeleid op School’: Discussietekst, Draaiboek, Begeleidersmap. Brussel, VAD, 1993.17 Basisprincipes voor (drug)preventie in de basisschool. Brussel, VAD, 1999.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200268
prevention workers, social workers - and to the training of teachers in early interventionmethods and referral.A drug policy at school should be set up by all partners involved in the school setting:students, teachers, principal, other school personnel, parents (associations), school healthservice.Training is offered to all these parties to make them able to deal with the different aspectsof a drug policy at school that is put in operation.The involvement of students (and parents) in a drug policy at school is not very easy. Inthe Flemish Community and particularly, to stimulate students’ involvement, aquestionnaire was developed to collect information on pupils’ attitudes towards drugs,their current drug use and their opinions about the drug policy of the school. The resultsmay stimulate the communication between parents, teachers, pupils, etc.The evaluation of this questionnaire confirmed the importance of the involvement of allparties (school health service, prevention workers, parents,...).Overall, it is very important that the drug policy at school is a continuous process in whichthe different aspects of the policy receive permanent attention, in continuouscommunication between the different partners.
9.1.b Models of school interventions
In the French Community, interventions in schools are managed by specialisedassociations or by internal services of the schools. The specialised associations offer twomain training types: adult “multiplicator” training and training to the youngsters.
As mentioned before, the programs are integrated within the framework of healthpromotion and are not only limited to drugs prevention.
There are two models of interventions in schools in the Flemish Community:
1. School advisory services give free and multidisciplinary support to teachers, parentsand schools. These services are active in four domains: preventive healthcare (healthpromotion of which drug prevention is one aspect), learning and studying, study careerand psychological & social functioning. Advisory services negotiate policy agreementswith schools to determine the responsibilities of both schools and advisory services inthese four domains.
2. Specialised healthcare organisations offer a broad range of interventions from training,education & support (for pupils, teachers and parents) to ready-made didactical packagesand educational projects. These packages and projects are often grounded in differentprevention models.
9.1.c Prevention programmes available in the country
See standard table19 and the context information.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 69
9.1.d Evaluation studies and results
French CommunityAll health promotion projects funded by the French Community must have an evaluationbuilt in the project. In addition, the French Community is funding two departments inuniversities (Promes in ULB and Ceres in ULG) to provide technical support and advisethe promoters of the projects.However, most evaluations are process evaluation and internal evaluations. Funding forimpact evaluation is most limited.
- CERES (2000).This is a qualitative evaluation done in 56 secondary schools of the French Community.The aims of this study were to evaluate the implementation processes of preventionprojects in schools. More precisely, the relations between schools, external drugsprevention services and cities were explored. Positive aspects and difficulties of projects’implementation in schools were also investigated.
Flemish Community- Andries, C., Lambrecht, C. (2000).Procesevaluatie pilootproject “naar een gezondheidsbeleid in Brusselse scholen”The project about “health education” (gezondheidsvoorlichting en – opvoeding) was a pilotproject, an evaluation study was set up to list encountered problems and importantfactors, and make recommendations for similar future projects.Outcomes :
- Timespan too short (+overall bad timing),- Overall strong motivation (in spite of regular frustrations),- Little support and “theory – practice-translations”,- Missing participation of pupils, parents and school management,- Recommended use of more students counsellors.
- VAD & University of Ghent (2001)Evaluation study of drug policy in secondary schools In Flanders.In 1999 VAD launched a survey of students at secondary schools about the drug policy atschool. The questionnaire contains questions about drug use, motivations, perception ofdrug policy on school… The main goal is helping schools to evaluate their drug policy.The survey also stimulates the communication about drugs and drug prevention betweenparents, students and teachers. Between January 1999 and June 2001 one third of allFlemish secondary schools (n=374) participated in the survey on the drug policy at school.To evaluate the follow up of the students survey by participating schools, VAD and thefaculty of educational sciences of the University of Ghent interviewed key persons in 220secondary schools in Flanders. Almost _ of the schools discussed the results of theirstudent survey with the teachers. Only 37.7% of the schools arranged feedback on theresults for students and 39.5% did the same for parents.
The results are discussed with the students on the student board or through classdiscussion, parents get the results presented at the parent board or at an informationevening, and to inform teachers, results were communicated in the staff meeting.Especially in the communication process to students and parents, schools appeal topersons or services outside the school setting (CLB, prevention worker, police, …). Inmany schools the school survey resulted in the start or an optimisation of the drug policy.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200270
9.1.e Research projects
- Kohn, L., Piette, D., Université Libre de BruxellesStudy of cannabis consumption amongst adolescents for the development of a policy anda programme of prevention: analysis of existing data, preliminary qualitative approach andprospective quantitative survey with follow up of 2 years.For some results, please refer to standard table 2d.
9.2. YOUTH PROGRAMMES OUTSIDE SCHOOLS
9.2.a Definitions used
Youth programmes addressed to young people, take place for example in youthorganisations, youth movements (different scouts federations, Patro’s,…) youth houses,sports clubs and young people’s services.
9.2.b Types and characteristics of intervention with youth outside schools
Flemish CommunityThe VAD launched two new, parallel projects for the sports sector in cooperation with theBelgian Football Association and the Flemish Sports Federation. The VAD is developingdidactic materials for prevention workers and mediators in the sports sector. In 2002-2003these two projects will be continued with information sessions for coaches andpolicymakers. The aims are to explain the role of sports and sport clubs in prevention andreflect on the issue of implementing a drug prevention policy in the sport club. In the sameperiod as the information sessions VAD will hold a poster campaign in sport clubs tosensitise the club members, parents and supporters for the alcohol an drug issue.
French CommunityA number of structures are organizing outreach activities, as sport, cultural andrecreational activities. These activities are set up locally. For example: en 2001, a theatreworkshop (“Chuut, suivez-moi!”) was created in a public school to sensitize youth to drugproblems (AMO le Cercle).
Futurofoot is a five years action plan launched in cooperation with the Football federation.This plan includes 6 actions (training programme for coaches, training for youngsters,organisation of championships, promotion of football to youngsters,…) Social actionsrelated to some phenomena’s such as violence, drugs, …are also carried out. In thisframework, the federation collaborates for the project “no to drugs” with NGO’s specialisedin prevention.
German-speaking-CommunityConducted by the German-speaking-Community and in co-operation with further regionalinstitutions a BIG-POINT-Day on the subject of “sports and recreational activities” hasbeen carried out. The people’s participation was by around 1,000 persons. On this eventthe ASL had an information stand on the topic of “drugs and drug-abuse”.
PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 71
9.2.c Statistics and evaluation results
No information available.
9.2.d Specific training for professionals and peers in this field
There is not specific training in this field.
9.3. FAMILY AND CHILDHOOD
9.3.a Definitions used
Prevention must be interpreted in a wide sense. I.e. interventions towards all parents non-restricted to parents using drugs and/or their children. It has to be taken in the sense ofdeveloping “life skills.”
9.3.b Types and characteristics of intervention with family and childhood
French CommunityDe facto, no activities are undertaken regarding drug prevention toward first childhood.The first early interventions among children at this level are organized by the “Office de laNaissance et de l’Enfance” (O.N.E). The medical-social workers (TMS) give assistance toparents on healthy living.
Besides this, various types of treatment programmes include this issue “drug addictparents” as part of their programme. These programmes want to provide assistance todrug addicted mothers, and improve the relationships mother-child as well as the livingconditions for the children (Kangourou project).
German-speaking CommunityFor several years the ASL offers education-trainings for interested parents. In this projectthe parents are used to multiply the training’s contents by wide spreading it on their part.The ASL cares for several groups of people who bring up their children alone and itarranges activities and holiday-trips with these groups.
Flemish Community'Hole in the fence18' is a prevention programme aimed at children in early childhood. Pre-school children listen to a story about the adventures of a bunch of vegetables. Throughout the story the children learn about the importance of life skills. Teachers or parents cantell the story and the word 'drug' is not mentioned in the story.
18 Het gat in de haag', De Sleutel
PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200272
9.3.c Research projects and evaluation results
Flemish Community- In the autumn of 2000 VAD ordered a preliminary investigation into education supportprograms for addicted parents with young children (Derluyn, Vanderplasschen &Broekaert 2000). An inventory has been made of all the different models of educationsupport programs for this target group. The study of literature showed us that a lot ofsocial services are involved in the support and care of addicted parents with youngchildren. As a result of this, a lot of different visions and methods are used witch leads to alack of harmony in the approach of the target group.As a follow-up of this preliminary investigation VAD ordered in 2001 two pilot projects.The objective of those two projects was to develop and to implement one or more modelsof education support; one in an ambulant and the other in a residential setting.The Kiem, project TIPI (Derluyn, Calle, et.al. 2002), worked out an inpatient program whilethe MSOC Genk (de Bruijn, Smits 2002) shaped up an outpatient program.Both projects resulted in a manual. In both manuals education support for individuals asfor groups are described. Both the backgrounds of the programs as well as theimplementation and the evaluation are exhaustive described, so they can be used aspractical instruments. Beside the intrinsic aspects, a lot of attention goes to the concreteimplementation and the structural adaptation of the social services.
French Community- Families and risk behaviours among the young people(Jamoulle P., Panuzi-Roger N.)
Topic areas :- Social building of risk behaviours and addictions (difficulties of socialisation for
young people living in precarious and marginalized neighbourhoods, crisis ofmeaning within families, crisis of the schools, amplification of judicial risks)
- Trans-generation weaving of risk behaviours and addictions- The springs for resilience processes- Tracks for prevention and access to services
Methodology :Field survey among families and relatives of young people who have developed itinerariesof risks (addictions, violence, illegal activities, anorexia /bulimia, auto-mutilation, suicidesattempts ….)Three methodological approaches:
- Observation and immersion in living places of the families and relatives- Biographic or ethnographic interviews- Survey within two vulnerable neighbourhoods
Constant implications of professionals and decision makers in the research process.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 73
9.4. OTHER PROGRAMMES
9.4.a Description of the following interventions
ÿ Peer-to-peer approachesNo information available.
ÿ Telephone help-lines (Infor-Drogues 2002, Druglijn-VAD 2002)“INFOR-DROGUES” and “DRUGLIJN” are respectively the drug helplines for the Frenchand Flemish Communities.As shown in the table below, the two services faced up to an increase of calls. Around60% of callers are females.Cannabis is the product in both communities for which questions are the most answered.On the qualitative level, the lack of clearness and the confusion created by the lastpolitical and juridical measures concerning the cannabis explains the high rate of callsfrom users and relatives about this substance. In association with this Druglijn alsonoticed a large increase in calls concerning legal information.
Table 28 : Telephone help-lines 2000-2001
Infor-Drogues Druglijn2000 2001 2000 2001
Number of calls 5226 6041 5818 6442 % Males % Females
--
4060
3664
3763
Involved substances fordrug-related calls (%)CannabisCocaineXTC (mdma)HeroineAlcoholPsychoactive medicinesMethadoneLSDAmphetamine
40,810,410,39,66,54,64,54,23,2
37,710,910,69,47,54,84,84
4,1
38101351971215
4210106
19711
12
Through these calls at Infor drogues,10.382 demands were registered (2000: 10.427; -0,4%) concerning : information 36 %; demands of prevention activity 3 %; advicedemands 27 %; demands of listening 3 %; help demands 23 %; demand of people for thecounselling service 3 %; no explicit demand 5 %.The callers: 18 % of the callers are users, 37 % are relatives (82 % are members of thefamily), 12 % are professionals, 7 % are students, 22 % “other” persons and 4 %unknown.
In 2001 the DrugLijn received 6442 effective calls (compared to 5818 calls in 2000).Six out of ten calls concern demands for information related to specific substances. In halfof these information calls people ask questions about effects and risks.76 % of the callers have emotional problems. More than one third of these are parent-child problems and one fifth concern emotional problems because of own use. In 56% ofthe calls people ask for concrete prevention or treatment possibilities.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200274
26 % of the callers are users or ex-users, 49 % are relatives (of which the majority areparents) and 18 % of the calls originate from a professional. Finally 7 % are just interestedbut do not actually consume.
The following table shows the repartition of callers by class age. It is noticed with caution(because of the high percentage of unknown data), that there is a difference between thetwo help lines according to the distribution by age categories.
Table 29 : Percentage by age of callers, 2001
Class age Infor-Drogues%
Druglijn%
Under 18 3.2 5.218-25 10 12.326-35 17.8 10.136-50 2.9 17.750 and older 4.2 5.6Unknown 43 49.1
ÿ Community programmesFrench CommunityIn 2001, projects were continued without changes ( eg. Projet Lama).
Flemish CommunityThe concept of a global alcohol and drug policy for local communities was developedduring the European Drug Prevention Week ’98. At that time, the project ‘A local alcoholand drug policy. Join in!’ was launched. With this project, we aim to call on all local keypersons (f.i. youthleaders, supervisors in the workplace, owner of hotel and cateringbusiness,…) to join in a local alcohol and drug policy and to support them in this. Wedeveloped a series of publications for the facilitators and partners in a local alcohol anddrug policy and for other interested field workers.To keep the concept of a local alcohol and drug policy alive, the manual ‘To less trouble.Manual tackling drug inconvenience’ was added in 2001 to the publications. The manualaddresses to prevention workers, local policy makers, welfare workers and social workers.
ÿ Drugs use at the workplaceThere is a growing interest in other drug problems (illicit drugs and medication). More andmore public enterprises are willing to develop such policies.Alcohol problems represent major struggles.
French Community- BrusselsContinuity of previous programmes and adaptation to new problems.
Flemish CommunityPrevention programmes include the development of a policy and early interventionprogrammes. Local and regional prevention workers are more and more implied in thedevelopment of an alcohol and other drugs related policy, due to the increasing demandfor consultation and guidance. VAD, the Flemish co-ordinating organisation, organisestraining sessions and intervision for these people. This should enable them to provide a

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 75
better service to these local consultation demands. Training programmes (for companydoctors, nurses, social workers and supervisors) are available in Flanders.
ÿ Welfare sectorSeveral years ago VAD launched two training programmes for the welfare sector (centravoor algemeen welzijnswerk en OCMW). Each programme consists of three parts:1.Introduction in alcohol- en drugproblems2. An alcohol and drugpolicy in a welfare centre3.Motivational interviewingAs the years before teams can apply for these training programmes. Trainers are theregional prevention workers.
ÿ Mass media campaignsIn november 2001 VAD launched the Bedrogen Campaign.The main aims of the campaign were to sensitise and to inform . The campaign had tostimulate the information seeking behaviour of young people on recreational drug use andon the risks involved for themselves as well as for others. We tried to reach 15 to 25 yearolds with a strong interest in dance music and its liftstyle. We focused on those who didnot (already) use party drugs but who possible felt attracted to these drugs as well as onthe occasional dance drug user who still stand open for sensitising messages. Thecampaign passed information on party drugs themselves, as well as basic harm reductionadvice.On a second level the campaign was een attempt to reach responsibles and mediators inthe nightlife industry (club owners, organisers of events and media).
In 2001 ASL’s specialized library has been extended and the books have been listed by acompatible system with other regional libraries. About 800 books, videos and newspapersin the prevention field are available there.
The Belgian Road Safety Institute (IBSR/BIVV) organises (since already several years) aprevention campaign “BOB” (against driving under alcohol effects), which is very popular.In 2001, this concept has been implemented in other European countries in the frameworkof the campaign “Euro-Bob”, financed by the European Commission. In addition, IBSRlaunched specific drugs prevention campaigns (“Rouler drogué, c’est parti pour unmauvais trip”).
ÿ Internet- VAD launched in 2001 its first of four consecutive alcohol sensibilisation campaigns.The target group for the 2001 campaign were youngsters age 12 to 16. The campaignwas build around a website19. The website simulated a virtual cool world with four comiccharacters. The chosen character guided the surfer through the website. BetweenOctober and December 2001 the website reported approximately 20.000 visitors.The use of Internet aiming at the promotion, dissemination or information sharing is verylow.- Prospective Jeunesse (Brussels): Updating and restructuring of their internet sitehttp://www.prospective-jeunesse.be. Research projects and evaluation results.
19 www.acoolworld.be

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200276
9.4.b Research projects and evaluation results
No Information available.
9.4.c Specific training
The Scientific Society of French speaking Pharmacists has organized in 2001 a trainingrelated to addictions divided in 4 topics: substances, social and psychological aspects,prevention and treatment20.
20 http://www.sspf.be/assuetude.htm

CHAPTER 10. Reduction of Drug Related Harm
ROLE OF HARM REDUCTION WITHIN THE NATIONAL DRUG POLICY/STRATEGY
In 1995, the federal government formulated an action plan for illegal drugs, based on ahealth perspective and on the harm reduction philosophy. In the French Community,needle exchange programmes are implemented since 1994. In July 2000 in Flanders, thenecessary legislative adaptations were made and in 2001 syringe exchange programmeswere officially implemented. So far, in Belgium, no legal framework for methadonesubstitution exists. Methadone is, however, being prescribed throughout Belgium, throughconsensus reached amongst partners concerned (1987 and updated in 2000). In theFlemish region, most methadone (maintenance) programmes are being provided by lowthreshold drug services. In smaller towns and rural areas, if existing at all, methadone isbeing prescribed by GPs under the supervision of drug services. In certain urban areasthe demand outweighs the availability of methadone (maintenance) programmes.In the French Community, access to methadone is provided by a broad range of services(low threshold services, GPs, outpatients specialised units, mental health facilities).
HARM REDUCTION PRACTICE
In the French Community harm reduction project are generally run by NGOs and some bythe cities under the “security contracts” funded by the Ministry of Interior.
The main objectives are to increase the health awareness, to give them a range ofalternatives to high-risk behaviour and to reinforce risk-reduction measures. Allprogrammes are “peers” prevention projects.
Targets:- Harm reduction activities targeting injecting drug users (Aids, hepatitis and
similar risks)- Harm reduction activities in dance scene targeting young drug users in
festivals, music events, rave and dancing- Harm reduction projects targeting specifically drug users in prison
Main objectives and targets are also valid for the Flemish Community (except target in thedance scene).
Specific training for professionals on harm reduction is implemented in Brussels and theWalloon Region.
RANGE OF SERVICES
Interventions of reduction of drug related harm take mainly place in low threshold services(outreach work, …). In Flanders, BAD is, as a users organisation also active in harmreduction.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200278
NETWORKING BETWEEN HR PROFESSIONALS
Through the whole country, different institutions are mobilised for the Early WarningSystem. For more detailed information on the EWS in Belgium refer to the Annex 1.
German CommunityThe ASL networked in 2001 twenty-nine institutions or persons for an Early WarningSystem ( EWS ) to inform them in synthetic drugs.All secondary schools, regional fire departments, the police, interested doctors andpharmacists as well as the hospitals are receiver of these mostly from Germany cominginformation.
Flemish and French CommunityThe plat-form BOM (Brussels overlegplatform voor middelengebruik) - Modus Vivendi -Free clinic focuses only on Brussels and works on the theme of needle exchange.
French Community- Sub-group “Needle exchange” of Réseau liégeois,- Super prison: theme drugs/prison,- Super Boule de Neige: animator Boule de Neige (Charleroi, Liège, Bruxelles, Namur),- Group “pilotage stérifix Bruxelles et super seringues”: theme accessibility of sterileinjection material in Brussels,- Harm reduction workshop,- Local plat-form (Brabant wallon, St-Gilles): theme drug addiction,- Harm reduction “breakfast”: all professionals of harm reduction of Brussels FrenchCommunity and EU,- Euro Boule de neige.
Flemish CommunityThe new syringe exchange programme is centrally coordinated to assure the same kind ofservice to all injecting drug users in Flanders. Personnel for the programme is attached tolow threshold services in every province21. Actors participating in these programmes aredrug services, pharmacists and outreach workers.
CO-ORDINATION OF NATIONAL POLICIES AND LOCAL PRACTICE
Discussions are held on this topic in the Drug Health Cell.
EXPENDITURES ON SPECIFIC HARM REDUCTION PROJECT
For this point, refer to Key Issue 14.
21 Syringe exchange programmes coordinated by VAD and Free Clinic Antwerp. Provincial coordination by the
so-called MSCOC's (low treshold services)
PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 79
10.1. DESCRIPTION OF INTERVENTIONS
10.1.a Outreach work in recreational settings (definitions and delivery of services)
French CommunityHarm reduction in music festivals, techno clubs and free parties. These activities arespread and according to the specificity of the event can include the following services:
• Diffusion of information:Targeting young people during Information stands. All programmes are peers preventionprojects. Activities during the event include diffusion of information on drugs, onprevention of sexual risks, distribution of condoms (lubricants), information on localavailable services, prevention of dehydration and bad trips. Through questionnaires,information on drug use and attitudes are collected from participants. “Peers” are trained(and paid!) and selected according to the musical program of the event (house, hip hop,etc.).
• Pill testing:On site pill testing has been realised during a event in the French Community. About 200pills have been tested by Test Marquis and 50 in laboratory.
• Needle exchange programme:In one festival, activities include syringe exchange programme for IVDUs attending theevent. About 1000 syringes exchanged.
• Examples of specific projects (heroin/other opiates, stimulants)Harm reduction brochures targeting young drug users have been developed in partnershipwith several organisations in the French Community. In 2001, were available brochureson amphetamines, hallucinogens, cannabis, XTC, cocaine and heroine. The first threebrochures have had an evaluation both quantitative and qualitative.
• “Bad trips” managementTargeting drug users experimenting bad trip, a team with psychologists and psychiatrician,nurses was present in one music festival. The objective is to avoid “over-medicalisation”and/or hospitalisation of theses cases through on-site assistance.
A detailed list is available in standard tables 21.
10.1.b Prevention of infectious diseases (delivery of services, at city level/in urbanenvironment)
French CommunityThe Plate-form for AIDS prevention has been set-up by a consortium of NGOs to developgeneral population projects. Modus Vivendi is responsible for the aids prevention activitiesspecifically targeting drug users. Different services are offered:

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200280
• Development and diffusion of Information material about aids, hepatitis B and C andother similar risks:
- Time table flyer with the addresses of the different needles exchangeprogrammes;- Brochure “Shooter propre”, targets intravenous drug users and provideinformation on how to inject safely;- Brochure “hepatitis B and C”: information brochures for drug users onhepatitis prevention.
• Needles exchange programmes:Different types of needles exchange programmes are available in the country except in theGerman Community: stationary, street programme and programmes in pharmacists.
• Injection kits: StérifixStérifix is a kit containing 2 syringes/needles, water for injection, disinfectant swabs, andinformation on the risk of transmission by syringe sharing and HIV screening centres. Thepackage is distributed by pharmacies.
• Prevention of sexual transmission: all harm reduction projects have a component onsafe sex and provide condoms (lubricants).
• Hepatitis B immunisation is poorly available, as intravenous drugs users are notidentified as a priority group in the Belgian Ministry of Health Hepatitis B immunisationpolicy. Therefore, the high costs of the vaccines make it access low.
• The ‘Operation BOULE DE NEIGE’, HIV, hepatitis and other risks related to drug usepeer prevention project aiming to reach, through a snowball methodology, target groupsnot easily reachable. (Ex)-drug users in short-term contracts ('jobist'), training them onHIV, hepatitis or overdoses prevention. After training, the “jobists” go back to the “ drugscene ” to contact drug users, diffuse their prevention messages and material and recruitnew candidates jobists.. The jobists are assisted in their work by a questionnaire that issecondary used to collect data on patterns of use, use and attitudes. Evaluation of eachintervention is made with the “jobists” and is both collective and individual. About 1500drug users, mainly IVDUs are reached every year in the French Community.Euro Boule-de-neige: with the support of EC-DGV, the project is currently transferred inFinland, Greece, Italy, Portugal, Spain, and Slovenia.In 2001, an operation “Boule de Neige” in prison was innovated (prison in Namur).
Flemish Community• Needle exchange programmes:Different types of needle exchange programmes are available in the country except in theGerman Community: stationary, street programme and programmes in pharmacists.
• Prevention of sexual transmission: all harm reduction projects have a component onsafe sex and provide condoms (lubricants).
• Hepatitis B immunisation is poorly available, as intravenous drugs users are notidentified as a priority group in the Belgian Ministry of Health Hepatitis B immunisationpolicy. Therefore, the high costs of the vaccines make it access low.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 81
• EXTRA : Peer Support networking in collaboration with outreach workers and needleexchange personnel. Training and support of (ex-)drug users for training their peers insafer use, communicable diseases, overdoseprevention, etc.
10.1.c Prevention of drug related overdoses
• Examples of ‘policies’ in overdose-prevention
Overdoses prevention: credit card size small 4 folders small brochure on overdosesprevention and guideline. (French Community)
In the Flemish Community, a local training in OD-prevention for drug workers and drugusers through the provincial co-ordinators of the needle exchange programmes is set up.Recruitment of drug users is done through advertising and personal contacts in lowthreshold drug services. In Antwerp it is worked out in close collaboration with the localdrug user union (the only one in the Flemish region of Belgium). An information brochureon OD-prevention is also available and distributed trough drug services, street cornerworkers and needle exchange programmes.
• Projects in high-risk settings (e.g. release from prison)No information available.
• Documentation, evaluation results, researchNo Information available.
10.1.d Users Rooms/Safe Injection Rooms (definitions and delivery of services)
Safe injections rooms do not exist in Belgium.
10.2. STANDARDS AND EVALUATIONS
10.2.a Existence of professional standards
In the French Community, there is a Euro Boule de Neige “Methodological snowballhandbook”. This handbook has been translated in English, Greek and Spanish.
In the Flemish Community, a handbook for syringe exchange programmes was developedand distributed amongst all participants. Its topics are e.g.: the legal framework, goodpractice, infectious diseases, health problems related to injecting, alternative ways ofusing, ….
PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200282
10.2.b Evaluation studies
All projects funded by the French Community have an evaluation component in theirmissions.
Flemish Community
There is a yearly evaluation of the needle exchange programmes in the Flemish region.This evaluation is done by a structured questionnaire that is filled in by drug usersfrequenting the exchange programmes. The questionnaire focuses on risk behaviour,health problems, quality of all aspects of the syringe exchange and demographic data.
10.2.c Training of staff
French CommunityTwo kinds of training (Modus Vivendi):• Professionals:Modules packages:
- Medical information- Prevention/ repression/ harm reduction: What for?- XTC, pills and other- Prevention by peers- Needle exchange- Or according to demand
• “Jobistes22” (peers):Modules packages:
- Diffusion of brochures: Harm reduction information in recreational settings- Boule de Neige (hepatitis, aids, …): see 10.1.b- Stérifix (promotion/evaluation): see 10.1.b- Festival: Harm reduction interventions in recreational settings
Handbook for jobsites.
Flemish CommunitySee 10b.
22 “a jobiste”: a french work used by the French-speaking Belgians to mean drug users or former drugs users
recruited to field work and make contacts with other drug users to find out what their drug habits andpractices are and inform them about risk prevention.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 83
10.2.d Major research projects
• Research action about the pertinence of a harm reduction intervention in recreationalsettings in Brussels (Modus Vivendi).
• Research action about problematic use of synthetic drugs (first exploration ofdemands and supply of treatment facilities (Modus Vivendi).
• A handbook, giving strategic ideas on the problem of ‘drug related harm’, was finalisedin 2001.

CHAPTER 11. Treatments
In the treatment of addiction, more attention is given to specific populations such aschildren of alcoholics, migrant populations, addicted mothers/parents with children, …More attention is also given to the combination of psychiatric disorders and addictionsproblems. A number of units for dual diagnosis are created, yet this is not the only answer.Also in the outpatient centres there has to be a specific offer for the dual diagnosispopulation.
11.1. “DRUG-FREE” TREATMENT AND HEALTH CARE AT NATIONAL LEVEL
11.1.a Objectives, definitions and criteria of admission
People who have problems with alcohol, medication or other drugs, can be helped indifferent settings for cure and/or care except for the German Community where there arenot specific treatment centers. There is a diversity of settings on different levels oftreatment and care. We distinguish inpatient treatment centres and outpatient treatmentcentres.The main providers of specialised inpatient treatment centres are crisis centres,therapeutic communities and drug units in psychiatric hospitals. Most of these settingsrequire a drug-free condition at the start and during the period of treatment. Some of thesecentres have a specialised detox-program. The objectives of treatment can be describedglobally as a drugfree reintegration in society . In recent years there is a larger number ofminor problematic drug abusers, for whom specific therapeutical settings for only minorsare set up. Their number may increase in the future.The main specialised outpatient centres are specialised centres for mental health, daycentres and Medical Social Care Centres (MSOCs). In these settings, the objectives oftreatment programmes may vary. Some aim at abstention, others aim at controlleddrinking or stabilised or controlled drug use.
In addition to the specialised drug treatment centers, many drug addicts seek help andassistance in general welfare centers, in general health services (general practitioners)and in the specialised self help groups which reach a vast proportion of the targetpopulation.
Most of the inpatient settings require a drug-free condition starting and during the periodof treatment. The objective of treatment in cure-programmes is staying clean.For those rehabilitations centres that have signed an INAMI convention, whether they beinpatient or outpatient, the final objective is the total eradication of addiction. However,there are other intermediate aims that are used as a means to attain the final objectiveand the psycho-social aspect of addiction is a fundamental part of treatment.Outpatient settings with therapeutical objectives (cure) have less control on using drugsduring the treatment period. Indeed, treatment can also focus on the well-being of patientsin their ordinary surroundings, which does not necessarily mean that they will stop usingdrugs.Some of the outpatient settings can work with the clients to controlled drinking or druguse.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 85
There are no uniform criteria of admission. They depend on the setting itself andeventually agreements with other centres forming part of a network. The therapeuticcommunities are therefore hard to get into as far as accessibility and requirements areconcerned: the admission procedure is long and tedious, physical addiction must endbefore the patient is accepted, the patient must be highly-motivated, group living is amajor part of the programme. On the other end of the spectrum, we find outpatient centresthat take in drug addicts quickly and easily. There are no prerequisites like an end tophysical addiction or strong motivation. In such centres, one-on-one treatment is the key.
11.1.b Availability, financing and organisation
On a regional level, there is a tendency that different settings co-operate in a network.However, there is still a long way to go. Structural and financial obstacles are preventingagencies from working together, taking the client’s needs as the starting point. Withinthese networks, the continuity of care is the central idea. An innovative project about casemanagement (low-threshold, intensive, personalised assistance) is up to guide a druguser through this treatment networks. One of the aims of this case management is to linkdifferent treatment episodes and the interventions of drug care professionals.
Several levels of power provide funding for drug rehabilitation departments. To give anoverview, mental health care centres are funded by the Walloon Region (COCOF for theBrussels Region). Hospitals and drug rehabilitation centres are funded by the FederalGovernment, the latter centres by way of INAMI conventions. There is also a third sourceof funding from the Ministry of the Interior for assistance and treatment structures (bothoutpatient and inpatient) that provide assistance to drug users. This funding takes theform of security and societal
In 2001 the day care hospital in Eupen as branch of St. Vith psychiatric hospital took upwork. So there are two day-hospitals (St. Vith and Eupen ) in the German speaking areawhich deal among other things with co-morbid drug-patients. But there is no aimedtherapeutic treatment only for addiction-patients.Both institutions have at their disposal around thirty places and the patients stay forbetween three and twelve month. They will be cared of a multidisciplinary team.
11.1.c Evaluation results, statistics, research and training
- Drug rehabilitation from 1980 to 1999", INAMI, Dept. of Health Care., June 2001.Up until the month of October 2000 included, individual requests to have insurance coverthe cost of the drug rehabilitation had to be filed with the Chief Medical Board for all drugaddicts undergoing rehabilitation in INAMI drug rehabilitation centres. INAMI gatheredstatistical data on certain aspects of individual requests during the period 1980-1999.Specific trainingFor the last 8 years, SSMG-Alto has provided training to general practitioners as well as toother social workers in the field.
The NADJA centre also offers training and supervision for institutions and social workersin the field. By working with centres in the field and using them to reach out to drugaddicts and potential consumers, the NADJA centre (Liege) seeks to make the most of the

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200286
existing network by creating links between the various disciplines through the use of thesame language. In 2000, basic training (module “Communication and addiction” ) andadvanced training (module “Aid Relations”) were offered.
There are specific training and education programs for these explicit subjects organisedby the VAD.
11.2. SUBSTITUTION AND MAINTENANCE PROGRAMMES
In Belgium, Methadone programmes are still waiting for a legal basis to broader operate.A new law will be prepared. Nevertheless, scientific conclusions are presented asrecommendations (Consensus Conference Methadone) issued by a panel of experts23.(See also chapter 10 Role of harm reduction within national drug policy)
11.2.a Objectives for substitution treatment
Substitution treatment is aimed to protect the health and quality of life of a patient with thefinal objective to achieve his ultimate withdrawal (Law Proposal 9/9/1999).
11.2.b Criteria of admission
Methadone treatment should be used in case of heroin or other opiates addiction. Thepatient should have at least 18 years old and be dependent for more than one year.
11.2.c Availability, financing, organisation and delivery of substitution treatmentservices
The MSc’s and a few day centres and low threshold programmes offer methadoneprograms. The number of general practitioners who prescribe methadone is unknown.Beside methadone, buprenorphine is also used to a lower extend as substitution forheroine.
11.2.d Substitution drugs and mode of application
It is recommended to start treatment with a Methadone dosage of about 30mg/day, tocheck the effect on the patient and not to prescribe take home dosages at least during thefirst 6 weeks. Generally speaking, substitution refers only to the use of Methadone orBurprenorphinee.
23For a full text see : http://www.health .fgov.be/CSH_HGR/

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 87
11.2.e Psycho social counselling
It is stated that psychosocial counselling and assistance to patients are factors improvingthe results of methadone treatment.
11.2.f Diversion of substitution drugs
No data available.
11.2.g Evaluation results, statistics, research and training
- Assessment of the medical-social assistance centres for drug users. ( Pelc, I. et al.2001) Evaluation des maisons d’accueil socio-sanitaire pour usagers de drogues,Rapport de synthèse global. SSTC).The research proposal covers assessment of the results of the (MASS/MSOC) activities24:Optimisation of their operation as a part of the regional assistance network,Optimisation of the function of the MASS/MSOC within the framework of a general policystrategy of assisting drug users.
- Evalumet, Alto-SSMG, Jan 2001 (Denis B., Van Woensel G., Lejeune D., Lafontaine EJB.):A transversal study was carried out from January to December 1999 covering 50 generalpractitioners from the ALTO Network, which includes 517 members. 42 doctorsparticipated in the study, which included at total of 559 drug rehab patients undergoingtreatment at the time of the study.The purpose of this study was to determine the efficacy of substitution treatmentsprescribed by general practitioners in order to assess the public health impact of thesepractices.The result of the study shows that treatments give generally positive results. However, itwas noticed that the first dosis of prescribed methadone are too high. In addition, the noncontrolled delivery of methadone in pharmacy sometimes happens too early in theprocess of the treatment. Training and intervision should be more promoted.
- Co-ordination and continuity of care in substance abuse treatment.Evaluation study in Belgium.Vanderplasschen W., De Bourdeaudhuij I., Van Oost P.(2002). European AddictionResearch, Karger, n° 8, p 10-21.The aims of the study was to evaluate two core aspects of quality of substance abusetreatment (co-ordination and continuity of care) in the province of East Flanders.It appears that relatively little information is registered concerning the course of thetreatment process and that only 10% of all client files contain a treatment plan. Followingthe introduction of a formalised plan that was regarded as a precondition for systematizingand otimizing communication between services, key informants considered theimplementation of a model of case management as an appropriate way of improving co-ordination and continuity of care in this region.
24 See http://www.belspo.be
PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200288
11.3. AFTER-CARE AND RE-INTEGRATION
11.3.a Links with national strategy and legislation (new developments)
Many inpatient treatment centres have their own after-care program. Therapeuticcommunities have their halfway houses. The drug centres in psychiatric hospitals offerday treatment and specific after-care programs for ex-patient and sometimes the partner.For people who have been hospitalised for a long period of time, aftercare is organised in‘protected housing’ projects.Re-integration contains different activities and the treatment focuses on varied levels as:housing, working, social network, social skills and administration. Some centres have theirown employment rehabilitation programs. The mission is to help the client to find a job bytraining, helping with the administration, drawing up a CV, preparing for job interview, etc.There is a need for drug specific centres to cooperate more with centres that arespecialised in job training such as VDAB and OCMW.
11.3.b Objectives, definitions and concepts of reintegration
Education and trainingAmong the specific training programmes, we find for example the SIAJeF programme(Liege), which makes use of professional instructors (construction, secretarial services,catering industry), the Essor programme, an on-the-job training company in Thuin orl’Espérance (Thuin), specific programme for alcoholic persons.EmploymentSome departments have the specific mission to reintegrate people by finding stable jobsfor them. In order to reach this aim, patients receive several types of aid: straightening outof the administrative situation, search for housing or training, specific job search (joboffers available at the centre, help drafting a CV, etc.)
HousingMany departments provide assistance in finding accommodation. Specific initiatives thatprovide accommodation exclusively to drug users are rare. There is one initiative,however, called "appartements encadrés" (Supervised apartments).
11.3.c Accessibility for different target groups (after treatment, after prison, forlong-term substitution clients)
After treatment: Re-integration occurs with the help of social workers who handle theadministrative tasks relating to the search for jobs and accommodation. They also provideassistance with straightening out the patient's administrative situation. This is offered as acomplement to the rehabilitation treatment given by the various outpatient centres.
After prison: Among these outpatient centres, a number of people prepare ex-convicts fortheir release from prison and help them carry out the necessary administrative tasks.
Other specific public: for people who have been institutionalised for a long period of time,after-care is offered through Habitations Protégées (protected housing): This departmentprovides aid and psychiatric care within society. This type of after-care is provided by

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 89
SIAJeF (Liege). Other institutions (Odyssée or the CHU, in Liege) also provide assistancewith social reintegration, namely through protected housing.
11.3.d Organisation, financing, managing, availability and delivery of services
OrganisationAfter-care and/or social and professional re-integration take place in various outpatient orinpatient structures. After-care may consist in individual follow-up treatment at anoutpatient centre or may come in the form of group support and mutual assistance withina department that is either actively involved in drug rehab or part of a residentialprogramme.
Reintegration is one of the specific missions of departments that are actively involved indrug rehab. Reintegration is also a key element in drug rehabilitation centres.
Specific departments include Habitations Protégées (protected housing).
11.3.e Statistics, research and evaluation results
No information available.
11.3.f Training
No information available.

CHAPTER 12. Interventions in the criminal justice system
The authorities are aware that drug use and drug trafficking exist in the prisons. Themagnitude of drugs in the detention centres has an important consequence to the prisonerand his environment. Detention centres cooperate with external specialised drugtreatment. VAD did a research into the support of drug specific centres to drug users inprisons in September 2001. This research gives an overview of the activities of the drugspecific settings in prisons. They organise different activities. Some centres organiseinformation and education sessions for the prisoners, some therapeutic settings arrangepsychosocial treatment or help for prisoners. The treatment or help varies from individualtreatment to treatment in group. Some organise introduction sessions in which prisonerslearn to know better the treatment possibilities after their detention. In the Flemishcommunity, a structural cooperation (“structuurplan”) between the prisons and the wholeof services offered by the Flemish government (culture, education, psychosocialtreatment, job training, job assistance) has been initiated in a pilot region.The drug specific centers also offer treatment (medical and social psychotherapeutic) to(ex) – prisoners who are in suspended release, probation, and free under conditions.There is a good co-operation between the detention centers and the drug specific centers.In 2002 two drug coordinators were appointed for coordination and development of adrug policy in prisons. In the Flemish prisons, there is an ongoing pilot project (“CentraalAanmeldingspunt”) that aims to improve the through care for prisoners. In this project,prison staff and specialised drug workers cooperate to liaison prisoners with treatmentupon release.
12.1. ASSISTANCE TO DRUG USERS IN PRISONS
Assistance to drug users is provided by the health services. In addition, there is a numberof external therapeutic services of external therapeutic services who can assist drug userswhen in prison. Finally, detained persons can also ask to see their own M.D., in this case,they must pay themselves the costs of care.
12.1.a Abstinence oriented treatments
• DRUG FREE DEPARTMENTSThere are some pilot projects of drug free departments in Flemish prisons. A trainingprogram for guards and prison personnel and for prisoners is realised. It focuses on druguse and HIV, Hepatitis, etc. A drug free, TC-like program exists in the prison of Ruiseledesince 1995.
• TREATMENT IN PRISONS-In co-operation with the prison authorities of St-Gilles in Brussels a specialisedprevention team has set up, during the past year, a prison section 'section primaire'. Theaims of this treatment programme were to prevent relapse offence behaviour amongprimary prisoners, drug addict or not, in fact people who are for the first time in prison for aperiod longer than six months. This programme works to promote a better rehabilitation inco-operation with outside specialised workers and the prison' personnel. Psycho-socialcounselling is provided by a specialised social worker.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 91
-TIMC (Toxicomanies et Interventions en Milieu Carcéral, 1997) is an EC collaborativenetwork involving participants from Belgium, France, Luxemburg and The Netherlands.It's aim is to create exchanges about drug use in prison and particularly focusing on therole of penitentiary workers and other workers outside of the prisons. Training ofpenitentiary workers is one main operational achievement. A drug use surveillancesystem started in 1997 in participating prisons. Data are monthly transmitted by fax to aco-ordination centre (Verviers/Nancy). Since then, this project is mainly financed by thejustice department.
12.1.b Substitution treatment
Substitution treatments are available in prisons but limited as described in the circularletter of the Ministry of Justice regarding the organisation of drug services in prison.
The main policy in terms of treatment to drug users is detoxification, possibly with theassistance of medications. Continuation of maintenance treatment is recommended in thecases of pregnant women, short-term detention (less than one year) and persons positivefor HIV or hepatitis. When a person is transferred to another prison for a short time,maintenance treatment must continued. Usually, no substitution treatments are initiated inprison. (More information in standard table 20).
12.1.c Harm Reduction measures
• Education, information material developed for outside prison can be distributed inprisons. In most prison, when entering, the detainees receive a package including severalinformation materials on HIV, hepatitis, tuberculosis and harm reduction linked to druguse. However, there is no strategy on informing prisoners of STDs and drugconsumption. Activities of this type may exist in certain institutions under the supervisionof an external NGO. The availability of information material depends on each individualprison and its medical service and/or on the possible presence of an NGO specialised inAIDS prevention.• Specific information material on AIDS and hepatitis prevention for drug users in prisonhas been developed by NGOs in co-ordination with health services of the penitentiaryadministration of Ministry of Justice and has been widely distributed in prisons25. Asecond edition has been developed, in 2000 including a specific chapter for women. Thisversion has been translated in dutch.• Condoms are available in all prison canteens. In practice, the canteens do not havetheir own stocks but have to procure them on demand at the local pharmacy. Thisexpensive and hardly discreet mode of distribution actually limits accessibility. A specificpackaging has been developed. Each packaging is composed of one condom and oneattached lubricant. Different ways of distributing have been studied according to eachprison. These are available in medical services, in social services and in rooms forconjugal visits.• Bleach is available in some prisons only for cleaning the cells. In 2002, all medicalservices were advised to make disinfectants available whenever prisoners ask for it.
25 “Vogue la Galère” Modus Vivendi Question santé 1998.« Wat als je binnen zit ? » Free Clinic 2000.

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 200292
• There is no needle exchange programme in prison.• There is a project to provide vaccination against hepatitis B to IV drug users. TheMinistry of Health – Institut supérieur d’hygiène, is developing a protocol for vaccinationand for treatment of hepatitis C. Currently some detainees have already been vaccinated.• Prison nurses have been trained on HIV, and hepatitis prevention.• In few prisons, there are also specific in-service training sessions organised for guardson harm reduction. However these activities are quite limited.
In 2001, an operation “Boule de Neige” in prison was innovated (prison in Namur). Itinclude prevention action on hepatitis, aids and harm reduction. Drug users or formerdrug users prisoners are recruited, formed and paid for transmitting information andsensibilisize others prisoners to harm reduction. In comparison with the methodology ofthe Snowball actions, these are adapted to the reality of penitentiary life. Withoutneglecting the problematic drug use, this operation is focused on more general topics ofHIV, and Hepatitis prevention, like harm reduction related to tattoo and piercing…
12.1.d Community Links
Some external therapeutic settings arrange treatment help in prison for prisoners. Theyalso organize introduction sessions to know better the treatment possibilities. Aftercare isoffered too by some of them when it concerns psychotherapeutic help. Social help isprovided by workers of the centers for juridical welfare.
“A qui s’adresser? (Capiti): handbook for detainees containing address and explicationabout specialised NGO in drug use.
12.2. ALTERNATIVES TO PRISON FOR DRUG DEPENDENT OFFENDERS
The federal drug policy paper takes health as its main focus and considers repression as‘the ultimum remedium’. As a result, a number of alternative judicial measurements(GAM) are put into practice which result in a closer cooperation between treatmentcenters and the judicial system.Another consequence of this starting point is that drug users in detention should get thechance to find a suitable form of treatment.For young drug users (not necessarily drug dependent offenders) who are arrested forpossession of drugs, police services can offer ‘therapeutical advise’. It is a method of earlydetection that gives the (younger) offender the opportunity to present themselves in aCenter for Mental Health Care for one or more exploring talks. In this way problems withdrug use or other problematic life fields can be detected in an early stage and can befollowed up by psychotherapeutic sessions. The drug user is stimulated to reflect on hisdrug use, and he has made acquaintance with care services so that he knows the way forasking help if it should be needed in the future.
1. Measures on the level of the public prosecutorThe public prosecutor can decide not to prosecute the case if the perpetrator agrees tocertain conditions. Several mechanisms are possible (p.e. pretorian probation, sentencemediation). These measures are most often used with first offenders. Although it is truethat these measures were installed to avoid imprisonment of a large category of offenders,

PART 3 Demand Reduction Interventions
Belgian National Report on drugs 2002 93
they also entail a risk of net widening. Conditions can include assessment (“therapeuticadvise”), drug education, treatment.2. Measures at the level of custodySince 1990, conditional release from custody is possible. Conditions can includeassessment, drug education or treatment.
3. Measures at the level of sentencingProbation is possible since 1964. In the case of probation with suspension, there istechnically no conviction: it is suspended for a maximum of five years. In the case orprobation with reprieve, there is a conviction, but no sentencing if the convicted personagrees to certain conditions for a maximum period of five years.
Conditional release (the law has been revised in 1998) is possible after one third of thesentence, with a minimum of three months. A specific measure (Minister of Justice circularletter n° 1710, February 2000) makes it possible for drug users who are convicted for asentence of maximum three years to leave even earlier if they enter treatment.
Different alternative ways to do prison time are available:- “half freedom”: the convicted person can leave the prison during day time for work or
treatment- electronic surveillance: the prisoner has to stay at home or be at the job or in therapy
during certain hours. This is controlled electronically. This possibility has recentlybeen made available to a larger group of drug users.
Weekend arrest and limited detention: these measures are not often used.
12.3. EVALUATION AND TRAINING
No evaluations of treatment for drug users in prison have been published, except for drugfree units. In one prison (St Gilles) a specific section has been established for detaineesentering the prison for the first time, the “section primaire”. This section has recently beenevaluated, through a questionnaire filled in by the inmates in this section. This evaluationshowed that persons admitted in this section are most interested in having access totraining activities and the lowest interest for access to “therapeutic” activities or services.The participation rate in this survey was 50% only.
In the Flemish Community training sessions in prisons are held, both for staff personneland detainees, on issues concerning HIV, hepatitis B &C. Training sessions on stickaccidents is organised for drug users, drug workers and city personnel. Finally there is thepossibility of risk behaviour-, safer use- and safer sex -training for staff personnel in drugservices and drug users.

CHAPTER 13. Quality Assurance
13.1. DESCRIPTION OF NEW TRENDS AND DEVELOPMENTS
No new information.
13.2. FORMAL REQUIREMENTS FOR QUALITY ASSURANCE
No new information.
13.3. CRITERIA AND INSTRUMENTS APPLIED IN QUALITY ASSURANCE
No new information.
13.4. APPLICATION OF QUALITY ASSURANCE PROCEDURES AND RESULTS
No new information.


PART IV. Key Issues
Chapter 14 : HARIGA Fabienne, TECCO Juan
Chapter 15 : HARIGA Fabienne, LAUDENS Fred, PECSTEEN Delphine,SLEIMAN Sandrine
Chapter 16 : LAUDENS Fred, PECSTEEN Delphine, SLEIMAN Sandrine


Belgian National Report on drugs 2002
CHAPTER 14. Demand reduction expenditures!on drugs in 1999
As mentioned in chapter 1, we do not have in Belgium a global overview of demandreduction expenditures on drugs. Thus, are presented in this chapter, two studies.
14.1. ECONOMIC BURDEN RELATED TO ADDICTION IN BELGIUM
In their article, Tecco and Hariga (2001) mentioned the great diversity of financing sourcesin Belgium. This diversity does not favour transparency. Consequent to the fact that manyfinancial sources have to be re-evaluated annually, long term vision is absent and joboffers are unattractive.A summary of their research is presented below. This summary is rudimentary andincomplete, as some of its figures are uncertain. Most budgets are inclusive (i.e. generaland psychiatric hospitals, general practitioners and for prevention: teachers, welfareworkers, ...) This makes it difficult to precisely describe the budget. This uncertainty ofinformation is worrying, considering the amounts allocated every year to health care.
The present inventory of the costs of drug addiction care deals only with a part of thecosts of treatment and prevention programs listed in the State budget specifically for thedrug users and the cost of hospitalisations and substitution treatments targeting peoplehaving a drug abuse as main diagnosis.
Drug addiction is sometimes not precisely defined. The initiatives of care concernespecially the heroin abuse but many centres broaden their therapeutic frame to otheraddictions, including sometimes alcohol.
Besides, the given costs are based on the budgets allocated by the variousadministrations, but non-profit-making organisations hire regularly staff on the basis ofprecarious contracts in order to fulfil their team work. For some organisations the cost ofthis staff does not take place in the financial reports that these organisations transmit tothe administrations subsidising them. It is interesting to underline that for instance in theWalloon Region in 1995, for 156 full-time contracts, there were 35.5 full-time precariouscontracts (A.L.E. (local agencies for employment) subsidised contracts, voluntary helpers,self-employed workers, etc.). As the budgets do not take the precarious contracts intoaccount, the costs are automatically underestimated for the Walloon Region.
We have been relying on the information available for the public and on those that thecare providers and the administrations agreed to transmit. In general, these various actorshave given data without almost any hesitation. All figures come from two sources: aninventory published in 2000 (1) and the web site of the Belgian Federal Ministry of SocialAffairs, Public Health and the Environment.

PART 4 Key Issues
Belgian National Report on drugs 2002 99
BUDGETS AND FUNDING ARRANGEMENTS
1. Federal Ministry of Health and Social Affairs
A. Treatment of drug addictsWe found that the treatment of drug addicts represents a budget of 100 million Euro peryear. (2)
* Psychiatric departments of general hospitalsBudget: 16 504 898 Euro* Medicine and surgery departmentsBudget: 5 221 847.38 Euro(In 1993, 26 587 hospitalisations occurred in medico-surgical wards for problems relatedto abuses and dependencies to substances, as main diagnosis. In 1996, the median costfor a day in those departments was 196.4 Euro).* Psychiatric hospitalsBudget: 46 262 528 Euro* Houses of psychiatric careBudget: 30 301 411 16 Euro* Protected housingBudget: 1 998 344.07 Euro
B. Functional rehabilitation centres for drug addicts (INAMI 1999 figures)(multidisciplinary care: medical, psychological and social)Budget: 22 530 859 Euro (2)* 16 342 383 Euro for residential programs (8 crisis intervention centres and 14therapeutic communities)* 6 188 475 Euro for ambulatory centres (6 day centres and 8 socio-health open housesfor marginalized drug users
1134 patients were treated in residential centres, 3248 in ambulatory centres (2672 insocio-health open houses) and 447 both residential and ambulatory centres.
C. The ambulatory consultations with methadone prescription.Budget: 8.92 millions Euro per year (1)In Belgium, the substitution without methadone is so marginal that it cannot be taken intoaccount in terms of expenditure. The global volume of prescribed methadone reached 104Kg. in 1996. Considering that the average prescribed dose is 50 mg per day, we canevaluate that the number of methadone doses reached 694 101 87 Euro in 1996. As aprescription of 50 mg of methadone costs 3 59 Euro, the total is evaluated to 7 476 468 71Euro. If we suppose that a drug user under substitution consults his physician every twoweeks for prescriptions, we evaluate a total of 148 165 consultations per year. As the costof a consultation in general medicine amounts to 9.77 Euro, we can calculate an overallcost of 1 447 698 18 Euro. This very basic calculation is of course poorly satisfactory andneeds to be sharpened. In Flanders, methadone is mostly distributed in daycentres andMASS and less by physicians.

PART 4 Key Issues
Belgian National Report on drugs 2002100
2. Federal Ministry of Internal Affairs
D. Ministry of the Internal Affairs (The global plan. Criminality prevention and of thereception of addicts)Budget: 7 800 450 67 Euro (2)* 1 673 281 29 Euro Prevention contracts (16 in Flanders, 12 in the Walloon region and 1in Brussels)* 6 127 169 38 Euro Security and society contracts (11 in Flanders, 5 in the Walloonregion and 6 in Brussels)
E. SPP (Secretariat for prevention policies) (1999)Budget: Unknown2 597 924 14 Euro (2) is the global SSP budget; the specific amount allocated to drugs isunknown.
3. Communities and Regions
F. The Flemish speaking community (2000)Budget: 2 816 070 44 Euro (2) (1 948 443 10 VAD + 371 840 29 provincial co-ordination).In addition to this budget, the prevention structure (through centres of mental health) isinclusive within the budget of the mental health centres.It finances prevention activities, the creation of data banks, to activities of co-ordination,dialogue, collaboration, accompaniments, training and educational events + provincial co-ordination.
G. The French-speaking Community. (2000)Budget: 1 239 467 Euro (2)Has competence over the framework of the fight against addiction, essentially over theprimary prevention).
H. The Walloon region (2000)Budget: 1 239 467 Euro (2)Supports projects coming within the scope of care in a broad sense.
I. Mixed Community Commission of the Region of Brussels-Capital (2000)Budget: 160 511 06 Euro (2)It finances mainly data collection and analyses, co-ordination activities, local annualreports and participation in Belgian and international networks.
J. French-speaking Community Commission of the Region of Brussels-CapitalBudget: 2 615 276 69 Euro in 2000 (2)Prevention, accompaniment, liaison, care and training.
K. Flemish-speaking Community Commission of the Region of Brussels-CapitalBudget: 116 509 96 Euro in 1997 (2)Co-ordination, prevention and other actions.
L. The German speaking community (2000)Budget: 252 851 40 Euro(2)Prevention of substance dependencies and also to dependencies in a broader sense notlinked to the substances.

PART 4 Key Issues
Belgian National Report on drugs 2002 101
M. REITOX
Cost of activities withinEMCCDA
Budget from EMCDDA
Focal Point 267 279 10 Euro 52567 09 EuroVAD 89 947 Euro 12 803 97 EuroEUROTOX 86 762 73 Euro 13 164 78 EuroCTB/ODB 75 499 99 Euro 9 758 52 Euro
ASL 5379 29 Euro 3774 52 EuroBIRN 7938 54 Euro 7938 54 Euro
CONCLUSIONNot forgetting the limited scope of the cost concerning more specifically the care marketfor the drug users and without confining the public policy to its budgetary dimension, it isinteresting to try to outline the financial aspects. The results have to be considered as sizeorders depending on calculation hypotheses that we wanted to detail as clearly aspossible. It may constitute a basis for discussions notably as regards the allocation ofresources between the care, the prevention and the substitution.
14.2. BELGIAN DRUG POLICY IN NUMBERS
More detailed information on expenditures will be available thanks to the research “TheBelgian Drug Policy in numbers26” (Promotors: Prof. dr. CASSELMAN J., Prof. dr. DERUYVER B., Prof. PELC I.). It will be ended in 2003.
1. Research aims
To date, Belgium has lacked any significant, concrete data on the drugs policy it ispursuing. No comprehensive overview exists of all the actors directly and indirectlyinvolved, nor of differences between funding sources. Nevertheless, this is a vitalcomponent in terms of the assessment of the policy being pursued.
As far back as 1997, the parliamentary working group concluded that a regulatedassessment of the measures being implemented was necessary if the intention were toadapt drug policies to developments within society (3).
The new federal drugs note also highlights the fact that the significant diversity in terms offunding sources has done nothing to promote policy transparency. An attempt to developan insight into who funds what and a compilation of a list of consultative structures arenecessary projects (4).
The European Union action plan to combat drugs 2000-2004 states that assessmentshould be one component in the European approach to fighting drugs. However, itappears that the required instruments, of which cost-effectiveness is one, are not yetadequate for drug policies to be assessed and therefore have to be developed further (5).
26 www.belspo.be/belspo/ostc/act_scien/fedra

PART 4 Key Issues
Belgian National Report on drugs 2002102
Outside Belgium, research has already been conducted within this context. However, thefocus abroad is still confined to partial aspects of the overall research question (forexample, assessment of treatment programmes for ‘problematic’ drug users (iv) ) or goesno further than estimating the cost of one aspect of drugs policy (for example, assistanceor prevention (6)).
For that reason, ‘drug policy in figures’ is intended to make a significant contribution byidentifying all agencies involved in drugs policy and also estimating the cost price of thevarious aspects of the policy being pursued. By simultaneously investigating whichsections of the drug-user population are being reached by the various actors involved, it ispossible to assess the benefits of the policy in respect of illegal drugs (and their users).
2. Research description
The investigation covers three phases:
PHASE A: Identification of the actors involved during drug policy implementation
Various actors play an active part in the policy on illegal drugs (and their users): agenciesfrom the health and welfare sector, police and judicial agencies, and policy actors. Anattempt will also be made to identify and list all existing consultative and coordinatingstructures. The relevant policy bodies at Federal, regional, provincial and local level will belocated.
The first research task therefore involves the identification of these actors. This will bedone using a classification in the fields of epidemiology-research, prevention-treatment,security and policy. This classification structure will be used throughout the variousresearch phases.
PHASE B: Cost price of the various components of the policy being pursued
Secondly, the project will examine what the cost price is for the various actors in relationto the pursued policy. ‘Cost price’ is understood to refer to funds made available to theactors.In the process, attention will be paid to the importance of ‘controlling supply’ versus‘limiting demand’ The cost price of controlling supply includes aspects like estimation ofthe cost of the criminal system, including police and customs, the public prosecutor’soffice, investigating magistrates, law courts and prisons, as well as alternative methodssuch as mediation in criminal cases and probation. The cost price of limiting demandcovers aspects that include the cost price of available low threshold care and treatmentfacilities, medical treatment for the effects of excessive and/or long-term drug use,treatment of drug-related diseases, as well as substitution and treatment programmes.
PHASE C: Population reached among drug users
Thirdly, the project will investigate how many and what types of drug users are beingreached by the services identified. This will provide us with an overall insight into thebenefits of the efforts made by these services.

PART 4 Key Issues
Belgian National Report on drugs 2002 103
14.3. REFERENCES
1)The cost of addiction care in Belgium. J.M. Tecco, O. Le Bon, P. Kopp, L. Joris, P.Verbanck, I. Pelc. Acta Psychiatrica Belgica 100 (3) mai/june 2000 pp 105 – 117
2) http://www.minsoc.fgov.be/cabinet/2001_01_19_note_politique_federale_drogues.htm#ah
3) Report on behalf of the working group appointed to study the issue of drugs, Gedr. St.,Kamer 1996-97, 1062/1, Conclusies en aanbevelingen, p. 5.
4) Policy note of the federal government on the drug issue, Brussels, 19 januari 2001, p.15-16 (http://www.minsoc.fgov.be/cabinet/2001_01_19_federale -beleidsnota_drugs.htm#federalenota).
5) European Union action plan to combat drugs 2000-2004, p. 7, 14.
6) X, 'Evaluating the Treatment of Drug Abuse in the European Union', EMCDDA,Luxembourg, 1999, 135 p.
7) For example: AD. ANDERSON, B. BOWLAND, W. CARTWRIGHT and B. BASSIN,Service-Level Costing of Drug Abuse Treatment, Journal of Substance Abuse Treatment,1998, Vol.15, n°3, p. 201-211; M. FRENCH and R. MARTIN, The Cost of Drug AbuseConsequences: A Summary of Research Findings, Journal of Substance AbuseTreatment, 1996, Vol. 13, n°6, p. 453-466; D. RICE, S. KELMAN, L. MILLER and S.DUNMEYER, The Economic Costs of Alcohol and Mental Illness, 1985, U.S. Departmentof Health and Human Agencies. DHHS, N°(ADM)90-1694, 1990.

Belgian National Report on drugs 2002
CHAPTER 15. Drug and alcohol use among young people aged 12-18
15.1. PREVALENCE, TRENDS AND PATTERNS OF USE
15.1.a General population survey and special survey on people 12-18
For these matters, refer to chapter 2.
Some additional elements are provided by the snowball operation (presented in 2.3.c andchapter 16), carried out in 2001-2002, in the French Community. Among the 1903persons contacted, 4.8% were young people, less than 19 years old (0-18 years). 21.1%of them are homeless, 90% are unemployed and 78.6% are without social welfareinsurance. 87.9% of them use illegal drugs.
Table 30 : Last month prevalence (%) of drug use,French Community, 2001-2002
Drugs Youngsters :less than 19 yearsN= 91
AdultsN=1812
Amphetamines 26.4 25.3Barbiturates 8.8 16.7Benzodiazepines 28.6 47.1Cannabis 79 80.6Codeine 8.8 16.8Cocaine 40.7 62.4Heroin 46.2 72.6LSD 27.5 23.8Methadone 17.6 27.4Morphine 15.4 16.2XTC 36.3 29.3UDI 23.1 47.4
The last month prevalences of cannabis and amphetamines uses seem to be quite similarin both age categories. Last month prevalences of cocaine, heroine andbenzodiazepines, barbiturates are higher in the adult category. In the contrary, last monthprevalence of XTC use is higher in the youngster’s category.
15.1.b Qualitative research on patterns of use
An exploratory survey about issues of new synthetic drugs has been conducted in 2000.In two festivals, 279 new synthetic drugs consumers have participated to the survey. Themajority of the respondents were from the Walloon region. 34% (95 persons) were in thecategory of 15-19 years old.
Main aim of this survey is to investigate the emergence of a problematic consumption ofnew synthetic drugs. This survey constitutes only a first approach to this problematic inmutation (Monheim et al. 2001).
PART 4 Key Issues
Belgian National Report on drugs 2002 105
Results show about 24% of the drug users (15-19 years old) stating they had adepression after a massive consumption of new synthetic drugs. However, it should betaken with caution, the meaning of “depression” for drug users may vary, moreover therelationship between the depressive state and the consumption has to be taken intoaccount.In addition, 32% of the youngsters, younger than 25 years old, report they lost contactwith their environment due to their nightlife. 32% only stated to be frequent drug users. Itis supposed that youngsters consume without knowing the product, their effects and theircapacity to support it. Their experiences are more extreme. The frequency of “problems”linked to the consumption of new synthetic drugs is close to the reported one by the olderdrug users.Generally speaking, the results show that many users encounter problems in relation withtheir consumption but only a small group consider their consumption as problematic. Amore smaller group external help.
These results are quite similar to these reported in a research about new synthetic drugsin the French Community, focusing on the category of 14-36 years old (Hacourt 2002).
15.1.c Perceptions about risks, benefits and image of specific drugs
The study conducted in the Brussels Capital Region shows results that generally confirmthese findings (Lambrecht 2002). The study carried out by the VUB in Flemish Brabantshows that the main motives not to use illegal drugs are indeed because they don’t needthose substances and because they are afraid of the consequences (afraid to becomeaddicted).
A school survey conducted in Charleroi shows some interesting perceptions towardssome specific drugs (Depaepe 2000). 62.2% of the respondents think that alcohol couldcause dependence, while only 49.4% thinks so for tobacco (and 42.0% for cannabis).Heroin causes addiction according to 67.9% of the respondents. Also, of alcohol,cannabis, ecstasy, heroin and tobacco, the drug most associated with violence is alcohol(56.0%). Furthermore, 60.1% thinks alcohol would evoke a health problem, as 67.7%thinks so for tobacco (as opposed to 37.4% for cannabis, 43.2% for ecstasy and 50.4% forheroin). Another remarkable observation is that 53.6% of the respondents associatetobacco with “un phénomène de mode”. Overall, the drugs are less associated with“pleasant” effects or consequences than with “negative” consequences.
15.1.d Trends in recent years
See chapter 6 for trends.
15.1.e New alternative information sources
StudentStart enquete : www.studentstart.be/drugsenqueteXTC enquete, prospective jeunesse : http://www.prospective-jeunesse.be

PART 4 Key Issues
Belgian National Report on drugs 2002106
15.2. HEALTH AND SOCIAL CONSEQUENCES
15.2.a Deaths and overdoses
Youth deaths due to drug use seem to be rare in Belgium. In the period from 1991 until1996, 17 cases could be found when analysing the data from the National Institute ofStatistics. Since the number of cases per year is very low and therefore is verysusceptible to change, it is hardly possible to describe evolutions. It should be noticed too,that these numbers could underestimate the prevalence of drug-related deaths, becauseof possible other causes of death reported by the physicians who fill out the deathcertificates. Nevertheless, an overview of the cases is given in table 32 below. Pleasenote that alcohol is not included in the list of drugs; the same code system according tothe EMCDDA guidelines has been used as for mortality in part 2.
Table 31 : Number of drug-related deaths in 12-17 year-olds in Belgium according tosubstance, 1991-1996
Age Opiates Barbiturates Benzodiazepines Other/unknown*
Total
1991 15-17 0 0 0 1 11992 15-17 1 2 0 3 61993 15-17 1 0 1 1 31994 12-14
15-1702
10
00
00
3
1995 15-17 1 0 0 1 21996 15-17 2 0 0 0 2
Total 7 3 1 6 17*
Other unspecified substance or unknown substance
Opiates are involved in the largest part of drug-related deaths where the substance isknown. Also noticeable is the fact that there is only one case of drug-related death in the12-14 year-old category. However, as mentioned above, not much can be said aboutthese data since the number of cases is very limited.
15.2.b Hospital emergencies
No data available.
15.2.c Driving accidents
New specific statistics on drugs accidents related to drugs consumption were notpublished in 2001. See section 3.4.c for previous studies.
15.2.d Demand for treatment
Additional results related to the snowball operation already mentioned (15.1.a) shows that:- 23.1% of youngsters inject one drug compared to 47.4% in the adult category.

PART 4 Key Issues
Belgian National Report on drugs 2002 107
- 76.4% (><36.7% adults) have not yet undergone a substitution treatment prescribedby a doctor.
- 33% of these (>< 74% adults) are under methadone treatment.- 32% of the youngsters declare having multiple partners (29% in adults category) and
26% run sexual risks (19% for the older category).- Less than one third (29%) of young IDU reported to have been tested for HIV
compared to 74% of older IDU.- In the contrary, only 28% of young users and 69% adults have not been tested for
hepatitis.
15.3. DEMAND AND HARM REDUCTION RESPONSES
15.3.a Prevention programs and campaigns
All prevention activities are listed in standard tables 19 and 21, see also chapter 9 dealingwith prevention.
15.3.b Specific harm reduction interventions in parties,...including pill testing
These interventions are presented in chapter 10.
15.4. METHODOLOGICAL INFORMATION
15.4.a Limits in data available
Comparison of data from school surveys with different methodological approaches is animportant difficulty. Limits discussed in chapter 7 are also available for this key issue.
15.4.b Bibliographical references
- Monheim, M., Van Vreckem, S., Werbrouck, D., Végairginsky, C., Vandendorpe, F., VanHuyck, C., Leclercq, D., Hariga, F. (2001).Recherche exploiratoire : Usages problématiques de drogues de synthèse. Premièreexploration des demandes et offres de prise en charge.
- Hacourt, G. (2002).Usages et usagers de nouvelles drogues de synthèse, Ecstasy, pillules sans ordonances.L’Harmattan, Bruxelles.

Belgian National Report on drugs 2002
CHAPTER 16. Social Exclusion and reintegration
16.1. DEFINITIONS AND CONCEPTS
16.1.a Social exclusion
At the European Councils of Lisbon (March 2000), Nice (December 2000) and Stockholm(June 2001), Member States made a commitment to promote sustainable economicgrowth and quality employment in order to reduce the risk of poverty and social exclusionand to strengthen social cohesion in the Union between 2001-2010. To underpin thiscommitment, the Council developed common objectives in the fight against poverty andsocial exclusion. It also agreed that these objectives should be taken forward by MemberStates from 2001 onwards in the context of two-year National Action Plans againstpoverty and social exclusion (NAPsincl) (Council of the European Union 2001).Within these NAPs/incl, “drug abuse” and “alcoholism” have been identified as risk factors(among others) increasing social exclusion.
Further to the Member States commitment, a Belgian inter-governmental conference(CIG) has been set up. Constituted by 6 working groups, the CIG gathers the federal andfederate governments of the country . The fight against social exclusion is a responsibilityof both Communities Governments, Regions and Federal Government, each one of thosehaving with their own specific responsibilities.
One of these groups, « Commission of Social Affairs27 », is responsible for the BelgianNAPincl.
According to the Belgian NAPincl (2001), « social exclusion » is “linked to a process ofsocial rupture that appears in several aspects of life, the standard of living usuallyaccepted is not anymore reached. The poverty resulting from this process couldsubsequently be considered as a network of social exclusions, which strengthen eachother. Moreover, destitute persons are often unable to improve the situation bythemselves.”Then several indicators are useful to analyse the multidimensional character of povertyand social exclusion. These are related to: salary, employment, housing, health care,education, social integration and participation.
16.1.b Issues discussed regarding social exclusion/drugs
In the PANincl, it is mentioned that the socio-economic situation has an impact on theaccess to healthcare but it also influences the life expectancy. The target group of thisplan is the socially excluded population as a whole, including drug users, although theseare not distinguished from the rest of this population.
The Federal Drug Policy Note (2001) recognizes that the problematic use of legal andillegal drugs cannot be avoided in our society. As a consequence, this policy is based onthree key points :
27 For more information see http://www.begroting.be/f/h7/h7a/h7a4/h7a4c.htm#presse

PART 4 Key Issues
Belgian National Report on drugs 2002 109
- prevention for non users and non problematic users,- assistance harm reduction , reintegration for problematic users,- and repression.
The Federal Drug Policy Note also introduces the concept of “problematic drug use”defined as an uncontrollable drug use.
The prevention policy will consist of two components: at one hand structural prevention(struggle against poverty, urbanisation) and at the other hand intervention among people(health promotion, sanitary education). Youngsters in marginalized neighbourhoods,Horeca and penitentiary environment are vulnerable groups towards whom secondaryprevention should be aimed.
In addition, the Federal Drug Policy Note emphasizes the availability of a large range offacilities for people with problematic drug use. These facilities have to be harmonisedand coordinated through consultative structures. A multidisciplinary approach andspecialised help directed towards these people has to be integrated into the network ofexisting social and medical services (see also chapter 1).
For the federate entities (Communities and Regions), education and prevention are atglance and focuses on (Cellule Pauvreté 2001) :
- Improving prevention in poorest neighbourhoods,- Improving prevention and detection of « social disabilities »,- Improvement of professional integration,- Development of possibilities to practise sports and holidays accessibility as a tool
for health promotion.
16.2. DRUG USE PATTERNS AND CONSEQUENCES OBSERVED AMONGSOCIALLY EXCLUDED POPULATION.
16.2.a Prevalence of drug use and problematic drug use amongst specific sociallyexcluded populations
Epidemiological studies in specific socially excluded populations are rather infrequent.Qualitative, ethnographic and punctual are more usual.However, some studies were conducted till now among prisoners where illegal drugs areeasily available. Cannabis, heroin and benzodiazepines are the most common productsused. It is generally accepted that 50% of prisoners consume drugs and more precisely,one third are intravenous drug users (Birn 2001).
16.2.b Patterns of use
Sharing needles and equipments are reported as a common practice for injectors in prison(Birn 2001).

PART 4 Key Issues
Belgian National Report on drugs 2002110
16.3. RELATIONSHIP BETWEEN SOCIAL EXCLUSION AND DRUG USE
16.3.a Indicators of social exclusion among drug users
Some socio-economic data are usually available in the treatment demand indicator.
Due to the Snowball survey (mentioned in 2.3.c), some socio-economical indicators areavailable on a group of drugs users (Hariga F., personal Communication, 2002). In 2001(and beginning 2002), among the 1812 interviewed adults, older than 18 years, 22%report being homeless and 66% are unemployed. About 83% are covered by the socialsecurity system and 63% has already been under substitution treatment. At the momentof the snowball survey, 74.3% were under substitution treatment.
Contrary to the usually accepted idea, the consumption of “new synthetic drugs” is notlimited to recreational settings. There is an extension of this consumption to other settings,including among socially excluded persons. It is also in this group that the frequency ofrisk behaviours and “accidents” linked to this consumption is higher (Hacourt 2002).
Different working groups of social workers are involved in addressing documents, reportsto political authorities. In the Brussels area, for example, the CTB/ODB working group“Street 1st line28” has reported the following facts to the local authorities.
- There is an increasing trend of youngsters facing with social problems includingdrugs addiction. Even if they don’t seek or use regularly the available help fromsocial services, they are quite well informed about it.
- Alcoholism becomes commonplace with a less extended network of help.- Collaboration difficulties between social services and psychiatric hospital units
occurred. Moreover these units are not always adapted to the “decrochagesocial”.
- Orientation of drugs users is a difficult choice: how to choose between aspecialised service or a general one ?
- Clear agreements have to be found to organise work and collaboration betweendifferent services (having different objectives, aims, philosophy,)
- Necessity to improve the “administrative access” to the help network; and finally,- Progresses have to be done in the organisation of supervised apartments for
socially excluded persons.
16.3.b Data from research on social exclusion and drug use
Drug use is deeply linked with medical, social, economical, cultural, individual, and penaldimensions. It is also related to social representations and particularities of our modernsocieties.Some youngsters having some psychological, social and family problems join in the samegroup. They become involved in the unofficial economy of the illicit drug market.. Theirfeeling of professional exclusion starts at the adolescence. They develop identityreferences and social insertion on other things than those of the professional integration.However, to earn money is a transition ritual to become adult recognized by the society.Drug would be perceived as a factor of integration (Jamoulle 2001a).
28 CTB/ODB working group “Street and 1st line”, note 04/02/2002.

PART 4 Key Issues
Belgian National Report on drugs 2002 111
It appears that “…physical lack, the cost of products, mixtures and the decline of theirsocio-economic resources create the conditions of an emergency which invades theirdaily life. Many were precipitated into activities at high risks (prostitution, crime,..) andconfined in secret socialization”. Confronted in a spiral of uncertainty, some drug usersstarted behaviour of consumption to risks exponential (Jamoulle 2001b).
A qualitative research conducted in Liège, aimed to understand the relationships betweenthe consumption of drugs and the fact of being in the meantime a victim of a criminal act(Hodiaumont 2000). Indeed, the illegal nature of drugs market often conducts to violence,denouncement, offences, etc. Moreover, the need for money may lead to illegal activitiessuch as street prostitution. A drug user could also be considered as a victim of thesubstance he uses, when for example, he does criminal acts (non desired criminalbehaviour) under the influence of psychoactive substances. Generally it is noticed thatdrug users are not likely to consider themselves as victims. This may be explained by thefact that they couldn’t be perceived as a “weak person”.
According to the results of the research project « EUROEXCLUDES 29» (2001), more thanhalf of the 199 interviewed persons in Brussels were single and only 20.6% of them hadregular salary from work. About one third were put in prison, among them 18.8% injecteddrugs when imprisoned.
The way to conduct alcohol and drug prevention programs was investigated in youthorganisations for socially disadvantaged youth (De Donder et al., 2001).Even if the target population is not marked by an extensive drug use, drugs are a vast partof their lives. All of them know drug users in their surrounding. The youth organisationshave an important preventive role, in general as well as drug specific. The positiveinteractions within these settings improve the self-image and the strong cohesion betweenyoungsters and youth workers leads to a care-taking relationships.Most of the youth organisations have an elementary drug policy, mostly based on houseregulations. Regulations have to be understandable and recognisable for the youngsters.The first premise demands an open communication, the second a participation of theyoung in the creation of the rules. The subject of drug use should be ‘debatable’ at alltimes. If group activities on the subject take place, it should certainly reflect the socialworld of the target group.
16.4. POLITICAL ISSUES AND REINTEGRATION PROGRAMMES
16.4.a Policies around social exclusion issues and implications for responses tosocial exclusion
The Federal Drug Policy Note cites that :”It is necessary to always take account of the factthat the consumption of drugs goes together with individual and social problems: to tacklea drug-dependence cannot be efficient if the underlying problems are not highlighted. Inthat sense, the multidisciplinary aspect is very important”. With this aim, “…the facilitieswill be harmonized and will be coordinated thanks to the platforms of dialogue, to a wellorganised system of registration and to a formal control of the authorities. In the context of
29 Euroexcludes is a study (coordinated by the School of Public Health of Granada) which was carried in 6
European cities including Brussels. A summary is available at : http://www.easp.es

PART 4 Key Issues
Belgian National Report on drugs 2002112
a multidisciplinary approach, the help specialized to the drug addicts must be integrated inthe network of the existing social and medical facilities”.
Low-threshold services like MASS/MSOC and other harm reduction interventions (formore details see Part 3) are more and more implemented. But as mentioned in theFederal Drug Policy Note, specific programmes for drug users in prison and professionalintegration programmes for stabilised users are still lacking.
16.4.b Elements of treatment focusing on reintegration within general drug services
One of the action points presented in the Federal Drug Policy Note, is to involve “casemanagers” in the system of assistance to drug users.Drug users having social reintegration problems will be helped individually by these casemanagers. Their mission will also be to improve the communication among differenttreatment centres.
16.4.c Results from outcome evaluation
No information gathered.
16.5. METHODOLOGICAL INFORMATION
16.5.a Limits in data available
First of all, comparison between “socially excluded drug users” and “non socially excludedusers” is quite difficult.An immeasurable part of the population is probably socially excluded and never appearsin the statistics by remaining hidden from the different help networks. Progress in thedefinition of indicators, for homeless people still has to be done.
In addition to ethnographic studies on drug users, main quantitative information availablein Belgium is issued from the treatment demand indicator. The socio-demographicinformation raised is related to gender, age, living status (with whom and where),nationality, labour status and the highest educational level completed. However, theseindicators are not enough accurate to study in depth the complex relation between socialexclusion and drug use.
16.5.b Main studies and research
Below are listed some current researches in this field.
- The Role of health promotion in tackling inequalities in health (2001).Two-year project coordinated by the Flemish Institute for Health Promotion (VIG) with theEuropean Network of Health Promotion Agencies (ENHPA). National and local strategies

PART 4 Key Issues
Belgian National Report on drugs 2002 113
and policies which have proved their effectiveness in using health promotion to improvethe health of deprived people were explored. Policy recommendations were addressed topolicy makers.
- New vulnerable groups in the Belgian health care system.It is a current project (2000-2003) coordinated by Prof. Dr. Louckx.30 (VUB).
- Snowball Heroin Study.This research is a current collaborative project between the Institute Public Health, FreeClinic and Modus Vivendi. The aim of this national study is to investigate somecharacteristics of a group of heroin users via standardized interviews.In more details, the objectives are :- to get information on the socio-demographic features of these drug users and investigatethe geographical variations of these characteristics,- to describe patterns of drug use and importance of polydrug use. The latency period (theperiod between first heroin use and first treatment demand) and the duration of the heroinuse will be inferred from these information.- evaluate some health consequences related to heroin use and sexual behaviour such asthe risk of infectious diseases particularly related to intra-venous drug use, and the risk ofoverdoses,- inquire about the use of health care in order to determine the probability of treatmentdemand for heroin consumption. It should therefore be possible to infer the prevalencerate of heroin use combining the estimate of the in-treatment rate with external informationon treatment demand collected by the monitoring systems existing in Belgium.
- Follow-up study after 5 years of cocaine and crack users in Antwerp.(Informal control mechanisms among cocaine and crack users in the metropolitan area ofAntwerp).Prof. Decorte (KUL).This study focused on drug users not in contact with institutions (hidden population).Current project from 1 January 2002 - 31 December 2003
- The influence of social networks on retention in and success after therapeutic communitytreatment.Veerle Soyez (UG).
16.5.c References
- Centre pour l’égalité des chances et la lutte contre racisme, Service de lutte contre lapauvreté, la précarité et l’exclusion sociale. En dialogue, six ans après le RapportGénéral sur la pauvreté. Juin 2001.Centrum voor gelijkheid van kansen en voor racismebestrijding, Steunpunt tot bestrijdingvan armoede, bestaeensonzekerheid en sociale uitsluiting. In dialoog, zes jaar na hetalgemeen verslag over amroede. Juni 2001.
- Commission du suivi des Affaires sociales (2001).Plan d’Action National d’Inclusion sociale. Bruxelles.
30 For a summary of the project http://www.sstc.fgov.be/belspo/ostc/act_scien/fedra/pres_uk.stm

PART 4 Key Issues
Belgian National Report on drugs 2002114
- De Donder, E., Rosiers, J., Vandenberghe, E (2001).Thuis in vrije tijd. Een verkennend onderzoek over preventie van alcohol- endrugproblemen in jeugdwerkingen met maatschappelijk achtergestelde jongeren. Brussel:VAD.
- Escuela Andaluza de Salud Pública (2001).Research project on risk behaviours, life styles and knowledge among socially excludedpeople, drug users at risk for HIV/AIDS in Europe (EURO-EXCLUDES).Final report.
- European Council (2001).Joint Report on Social Inclusion.Brussels.
- Flemish Institute for Health Promotion (VIG) in collaboration with the European Networkof Health Promotion Agencies (ENHPA), (2001).The Role of health promotion in tackling inequalities in health.Round table Conference report, 5 December 2001, Brussels.
- Hacourt, G. (2002).Usages et usagers de nouvelles drogues de synthèse, Ecstasy, pillules sans ordonances.L’Harmattan, Bruxelles.
- Hodiaumont, F.(2000).La victimisation criminelle des usagers de drogues, Etude réalisée auprès d’un échantillonde toxicomanes liégeois. Travail de fin d’études.Université de Liège.
- Jamoulle, P.(2001).Les conduites liées aux drogues dans les zones de précarité.Psychotropes, vol 7 n°3-4 p11.De Boeck et Larcier, Bruxelles.
- Jamoulle, P.(2001 a).Styles de vie lies aux drogues et trajectories de sortie de toxicomanie.Psychotropes, vol 7 n°3-4 p73.De Boeck et Larcier, Bruxelles.
- Jamoulle, P. (2001 b).Les conduites liées aux drogues dans les zones de précarité, Enquête de terrain auprèsdes professionnels.Revue Psychotropes, vol 7 n°3-4, Bruxelles.
- Ministère fédéral des affaires sociales de la santé publique et de l’environnement,Cellule Pauvreté (2001).Mise en oeuvre du rapport général sur la pauvreté. Rapport d’avancement.Bruxelles.

PART 4 Key Issues
Belgian National Report on drugs 2002 115
- Rea, A. et al.(2001).La problématique des personnes sans-abri en Région de Bruxelles-Capitale.Rapport pour la Commission Communautaire Commune, Bruxelles.
- Vercaigne, C., Walgrave, L., Mistiaen P., Kesteloot, C. (2001).Urbanisation, exclusion sociale des jeunes et criminalité de rue.SSTC, Bruxelles.
- Vranken J. (2001)Armoede en sociale uitsluiting : jaarboek 2001.Leuven Acco.
References

BIBLIOGRAPHY
ALTO SSMG (1995).Les fruits d’une experience : Accompagnement de toxicomanes par des médecinsgénéralistes.Bruxelles.
ALTO SSMG, Denis, B. , Van Woensel, G., Lejeune, D., Lafontaine, J-B (2001).Evalumet.Bruxelles.
Andries, C., Lambrecht, C. (2000).Procesevaluatie pilootproject “naar een gezondheidsbeleid in Brusselse scholen”Eindrapport.VUB-Brussels Gezondheidsoverleg Directie Welzijn en Gezondheid VlaamseGemeenschapscommissie.
Bechet, S. (1994).Etude d’un échantillon de patients toxicomanes admis au service des urgences de l’hôpitalSt-Pierre.Bruxelles.
BELGIAN ROAD SAFETY INSTITUTE (1998).Belgian Toxicology and Trauma Study, Belgian Society of emergency and disaster medicine,Toxicological Society of Belgium and Luxembourg.
Beutels, M., Van Damme, P., Aelvoet, W., Desmyter, J., Dondeyne, F., Goilav, C. et al.(1997).Prevalence of hepatitis A, B and C in the Flemish population.Eur. J. Epid., 13, 275-80.
Beyens, K., Snacken, S., Eliaerts, C. (1993).Barstende muren, Overbevolkte gevangenissen: omvang, oorzaken en mogelijkeoplossingen, p. 326. Kluwer-Gouda Quint, Antwerpen-Arnhem.
Bils, L., Gosset, C., Bertrand, J. (2000).Enquête de diagnostic social dans trois écoles secondaires de Verviers - 1999.CCAD,ULG.
BIRN (2000).Report on Treatment Demands in Belgium : data 1998.EMCDDA Field trial exercise 2000. Brussels.
BIRN (2001).Belgian National Report on Drugs 2001.Brussels.
Casselman, J., Meuwissen, K., (2001).Evaluatie van de medisch-sociale opvangcentra voor druggebruikers. Deelrapport Antwerpen-Genk/Limburg.DWTC, Brussel.
References
Belgian National Report on drugs 2002 119
CERES (Centre d'Enseignement et de Recherche en Education pour la Santé, ULG)(2000).Opération de prévention des toxicomanies dans certains établissements d'enseignementsecondaire de langue française. Rapport d'évaluation.Liège.
Circulaire Ministérielle du 12 septembre 1995 remplaçant la circulaire du 7 mars 1995 relativeau recrutement par les communes de personnel supplémentaire pour l’encadrement desmesures judiciaires alternatives au sein du Plan global pour l’emploi, la compétitivité et lasécurité.Moniteur belge / Belgisch Staatsblad, 09/11/1996.
Colla, M. (1998).Het drugbeleid in België, actuele ontwikkelingen.In Het drugbeleid in België : actuele ontwikkelingen, ed. B. De Ruyver, P. De Somere, G.Vermeulen, A. Noirfalise and Ch. Figiel, p. 35.Drugbeleid 2000 Maklu, Antwerpen,– Bruylant, Brussel.
Conseil Supérieur d’Hygiène , Sous-Section I.1.1 Assuétude, Ministère des Affaires Sociales,de la Santé Publique et de l’Environnement (2000).Suivi de la conférence de consensus méthadone de 1994 : évaluation des recommendationsformulées en 1994 et propositions complémentaires.Bruxelles.
Conseil Supérieur d’Hygiène , Sous-Section I.1.1 Assuétude, Ministère des Affaires Sociales,de la Santé Publique et de l’Environnement (2000).Rapport de suivi de la conference de consensus sur la méthadone.Bruxelles.
de Bruijn, L, Smits, D. (2002).Drugverslaafden met jonge kinderen. Draaiboek voor opvoedingsondersteuning bijdrugverslaafde ouders in een ambulante setting.VAD, Brussel.
De Clerck, S. (1996).Politique pénale. Exécution des peines. Note d’orientation, p.75.Ministère de la Justice, Bruxelles.
De Clerck, S. (1998).Het drugbeleid in België, actuele ontwikkelingen. In Het drugbeleid in België, actueleontwikkelingen, ed. B. De Ruyver, P. De Somere, G. Vermeulen, A. Noirfalise and Ch. Figiel,p. 43.Drugbeleid 2000, Maklu, Antwerpen,– Bruylant, Brussel.
Decorte, T. (1999).Informal control mechanisms among cocaine and crack users in the metropolitan area ofAntwerp (Belgium).Thesis Katholieke Universiteit Leuven. Leuven.
De Donder, E., Rosiers, J., Vandenberghe, E. (2001).Thuis in vrije tijd. Een verkennendonderzoek over preventie van alcohol- en drugproblemen in jeugdwerkingen metmaatschappelijk achtergestelde jongeren. Brussel. VAD.

References
Belgian National Report on drugs 2002120
Dehaes, W. (1987).Looking for effective drug education programmes : 15 years exploring the effects of differentdrug education programs.Health Education Research, Volume 2, n° 4, pp. 433-438.
Delwaide, J., Gérard, Ch., Sondag, D., Belaiche, J. (1997).Les modes de transmission du virus de l’hépatite C.Rev. Med. Liége, 52, pp. 388-391.
De Maere, W., Hariga, F., Bartholeyns, F., Vanderveken, M. (2000).Druggebruik in de gevangenisomgeving. Ontwikkeling van een epidemiologischonderzoeksinstrument. Onderzoek uitgevoerd in opdracht van DWTC/SSTC.
Denis, B., Hayani, A., Jamoulle, M. et al.(1993).Toxicomanie et virus de l'hépatite C, B et HIV.Bulletin de la Société Clinique de l'Hopital Civil de Charleroi, 44, pp. 209-213.
Denis, B., Dedobbeleer, M., Collet, T. et al. (2000).High prevalence of hepatitis C virus infection in Belgian intravenous drug users and potentialrole of the Cotton-filter in transmission.Acta Gastro-Enterologica Belgica, Vol LXIII.
Depaepe, P., De Clerck, B.(2000).Enquête réalisée au sein de la population scolarisée de Charleroi portant sur le phénomènedes drogues en 1999.Coordination Drogue, Ville de Charleroi.
Depaepe, P. (2002).Enquête-sentinelles, Analyse descriptive de l’évolution des données de 1995-2001.Coordination Drogue, Ville de Charleroi.
Derluyn, I., Vanderplasschen, W. & Broekaert, E. (2000).Drugverslaafden met jonge kinderen. Een exploratief onderzoek naar modellen enopvoedingsondersteunende methodieken bij de hulpverlening aan drugverslaafde ouders metjonge kinderen.VAD, Brussel
Derluyn, I., Calle, D. ,Vanderplasschen, W. & Broekaert, E. (2002).Drugverslaafden met jonge kinderen. Concept- en methodiekontwikkeling vooropvoedingsondersteuning in een residentiële setting.VAD, Brussel.
De Ruyver, B. (1996).Druggebruikers in de strafrechtsbedeling. In: Balthazar T, Bogaert M, De Ruyver B,Dewallens D, Maximus L; Juridische aspecten van druggebruik, p.21-23, 28-29 and 18.Mys & Breesch, Gent.
De Ruyver, B., VanImpe, K., Vander Beken, T. (2000a).Chapter 6, Belgium In Prosecution of drug users in Europe, Varying pathways to similarobjectives, A study of DrugScope, ed. N. Dorn, B. De Ruyver, C. Black, B. Lisgarten, K. VanImpe, T. Vander Beken, pp. 21-41.UK and Ghent University, Belgium.

References
Belgian National Report on drugs 2002 121
De Ruyver, B., Casselman, J., Meuwissen, K., Bullens, F., Van Impe, K. (2000b).Het Belgisch drugbeleid anno 2000: een stand van zaken drie jaar na de aanbevelingen vande parlementaire werkgroep drugs, p.63.Universiteit Gent, Onderzoeksgroep Drugbeleid, Strafrechtelijk beleid en Internationalecriminaliteit, Gent.
De Ruyver, B., Bosman, G., Bullens, F., Vander Laenen, F., (2001).Evaluatie van de medisch-sociale opvangcentra voor druggebruikers. Deelrapport Gent-Oostende.DWTC, Brussel.
De Sleutel (2000).Jaarverslag 1999.Merelbeke.
De Sleutel (2001).Jaarverslag 2000.Merelbeke.
D’Haeseleer, H. (1997).Project Ninove Rookvrije Stad. Gezondheidsenquête Ninoofse scholieren.Ninove, Dienst Sociale Zaken.Driesen, G., De Maere, W., Kinable,H., Todts, S. (1997).Risicogedrag bij injecterende druggebruikers in Vlaanderen. Rapport van het GIG-project.Antwerpen.
Dubois, P. (1995).Illegal drug among military conscripts.Ann. Med. Milit. Belg. 9(2) pp.89-96.
European Commission (1999).Communication to the Council and the European Parliament on a European Union ActionPlan to Combat Drugs (2000-2004).COM (1999) 239, Brussels.
European Centre for the Epidemiological Monitoring of AIDS (2000).HIV/AIDS surveillance in Europe. End-year report 1999, n° 62.European Monitoring Centre for Drugs and Drug Addiction (2000).Annual report on the state of the drugs problem in the European Union 2000.Lisboa.
European network for AIDS prevention in Prison (1998).2nd report.
FARES (2001).Rapport épidémiologique de la tuberculose en Belgique - 2000..Bruxelles.
FARES/VRGT (2002).Rapport épidemiologique 2001.In press.

References
Belgian National Report on drugs 2002122
Goelens, I., De Clerck, B. (2000).Recueil de données épidémiologiques concernant les usagers de produits psychotropesillicites en contact avec des instances d'aide dans la région de Charleroi. Analyse descriptivede l’évolution des données de 1995 à 1999.Coordination Drogue, Ville de Charleroi.
Hanak C., Streel E., Tecco J., Gilson S., Lefere A., Fauconnier F., BrownO., Clément B., Bredas Ph., Massaut J., Pelc I., Verbanck P. (2000).Clinical evaluation of a new detoxification technique for opiate-dependent patients.Poster présenté au XXII nd C.I.N.P. Congress, Brussels, July 9-13, 2000Clinique d'Alcoologie et de Toxicomanies - C.H.U. Brugmann, Bruxelles.
Harding, TW. (1987).AIDS in Prison.The Lancet, November 28, 1987, p 1260-63.
Hariga, F., Goosdeel, A. (1997).Rapport Boule de Neige 96.Modus Vivendi, Bruxelles.
Hariga, F. (1998 a).Analyse des données Boule de Neige 1997.Modus Vivendi - Carnet du Risque N° 3. Bruxelles.
Hariga, F. (1998 b).Rapport comptoir d'échange CCLA (Citoyen comme les autres) 1997– 1998.Modus Vivendi, Bruxelles.
Hariga,F. (1998 c).VIH, Hépatites et comportements à risque dans les prisons européennes - rapport Belgique1997.Modus Vivendi - Carnet du risque N° 25. Bruxelles.
Hariga, F., Van Huyck, C., Lazarou, A. (1999).Rapport de recherche action Dour 1998.Modus Vivendi - Carnet du risque N°16. Bruxelles.
Hariga, F. (1999).Evaluation du programme Stérifix 1998.Modus Vivendi - carnets du risque. Bruxelles, 1999.
Hariga, F. (1999)Rapport Boule de Neige 98.Modus Vivendi, Bruxelles.
IDEWE (1994).De prevalencie van infecties in penitentiaire instellingen in Belgie, Onderzoek rapport.Leuven.
Jamoulle, P. (2000).Drogues de rue.Collection Oxalis, Editions De Boeck, Paris-Bruxelles.

References
Belgian National Report on drugs 2002 123
Kinable, H.(1999).Bevraging van Vlaamse leerlingen in het Kader van een drugbeleid op school.Syntheserapport januari-juni 1999.VAD.
Kohn, L., Piette, D. (1997).La consommation de cannabis chez les jeunes à Bruxelles.Les Cahiers de la Santé de la Commission Communautaire Française.ESP-PROMES, ULB, Bruxelles.
Kohn, L., Piette, D. (1998).La consommation de cannabis chez les jeunes : etude préliminaire.ULB-Promes, Bruxelles.
Korn, M., Chamberlant, B., Siegelbaum, F., Bollette, Ph. and Thys P.Rapport d’activité du centre de santé mentale du CLIPS, Liège.
Lambrecht, P., Andries, C., De Bock, M., Wydoodt, J-P. (1996).Middelengebruik in de hoofdstad. De hoofdstad van Middelengebruik.VUB, Brussel.
Lambrecht, P., Andries, C., Engels, T.(2002).Risicogedrag in de hoofdstad De hoofdstad van risicogedrag ?VUB, Brussel, p 248.
Lambrecht, P., Andries, C., Engels, T. (2002).Trends in het Genotmiddelengebruik bij adolescenten van Vlaams-Brabant.VUB, Brussel, p 202.
Ledoux, Y., Sand, F., Corten, Ph., Roussaux, JP. and Remy, C. (1992).Evaluation d’un traitement de la toxicomanie aux opiacés par un groupe de médecinsbruxellois (RAT) par la thérapie de substitution methadone.ULB, Institut de psychiatrie, Bruxelles.
Ledoux, Y., Pelc, I., Roussaux, J.P. (1993).Le devenir des toxicomanes et d'alcooliques après traitement : le rôle des rapports familiauxet interpersonnels.Nouvelles de la science et des technologies, vol. 11, n°4, pp. 71-80.
Ledoux, Y. and coll. ( 1996).La mortalité chez des patients pris en charge dans des centres conventionnés, INAMI; Soinsde santé, Comité d’assurance (rapport de 1993).ULB, Bruxelles.
Ledoux, Y., Preumont, C., Bils, L. (1999).Estimation du nombre d'usagers d'opiacés dans la Communauté française de Belgique.CCAD - Notes épidémiologiques n°1. Bruxelles.
Lequarré, F. (2000)Qualitative evaluation of the Liege model of methadone treatment.
References
Belgian National Report on drugs 2002124
Leus,E., Desmet, A., Walckiers, D. (2001).Development of the Early Warning System on New Synthetic Drugs at Public Health Level inBelgium. Progress Report.Scientific Institute of Public Health, Rapport D/2001/2505/11, Brussels.
Wet 16 maart 1999 tot wijziging van de wet betreffende de politie over het wegverkeer,gecoördineerd op 16 maart 1968, B.S. 30 maart 1999, 10157-10160.Loi 16 mars 1999modifiant la loi relative à la police de la circulation routière, coordonnée le 16 mars 1968, M.B.30 mars 1999, 10157-10160.
Lombaert, G., Raes, V.(2000).Middelengebruik in relatie tot de leefwereld van jongeren, Onderzoeksresultaten van eenindividuele bevraging bij 4588 leerlingen in Brugge.De Sleutel.
Maes, E. (2002).Studie van de evolutie van de gedetineerdenpopulatie volgens misdrijfcategorie (1980-1998).Panopticon, Tijdschrift voor strafrecht, criminologie en forensisch welzijnswerk, afl. 4, 340-350.
Maes, L., Vereecken, C. (1999).Database 'Jongeren en gezondheid 1998 (part of a WHO cross national study).University of Ghent, department of Public Health, Ghent.
Minne, M., Vandeurzen, J. (1997).Rapport fait au nom du groupe de travail chargé d’étudier la problématique de la drogue /Verslag namens de werkgroep belast met het bestuderen van de drugproblematiek; Chambredes Représentants de Belgique / Belgische Kamer van Volksvertegenwoordigers.Bruxelles / Brussel; juin 1997; 1062/3 – 96/97; p. 698
Ministerie van Justitie, Dienst Strafrechtelijk Beleid (1999).Evaluatie van de gemeenschappelijke richtlijn dd. 8 mei 1998 van de Minister van Justitie enhet College van Procureurs-generaal betreffende het vervolgingsbeleid inzake bezit endetailhandel van illegale verdovende middelen, p.23.Ministerie van Justitie, Dienst voor Strafrechtelijk Beleid, Brussel.
Ministère de la Justice, Point d’Appui statistique, Service de la politique criminelle (2001).Données statistiques en matière de condamnations, suspensions, internements, 1996.Bruxelles.
Ministry of Social Affairs (1998).RCM-RPM Flash /MKG-MPG flash.Brussels.
Parmentier, S., Peters, T. (May 1-3, 1998).Pre-adjudication dispositions in sentencing. Experiences with prosecutorial diversion inWestern Europe with a focus on Belgium and the Netherlands, International Conference onSentencing Policy in Comparative International Perspective: Recent Changes Within andAcross National Boundaries, p. 1.University of Minnesota Law School.
Patesson, R., Steinberg, P. (2000).Les Belges et la drogue, enquête réalisée par l’ULB à la demande de la Fondation Rodin, del’asbl Drogue 2000 et du journal Le Soir. Bruxelles.
References
Belgian National Report on drugs 2002 125
Pelc, I., From, L., Nicaise, P. (2001).Evaluation des maisons d'accueil socio-sanitaire pour usagers de drogues. Rapport desynthèse local, Mons Charleroi.SSTC, Bruxelles.
Pelc, I., De Ruyver, B., Noirfalise, A., Maquet, C. et al., (2001).Evaluatie van de medisch-sociale opvangcentra voor druggebruikers. Algemeen rapport.DWTC, Brussel.
Picard E. (1997).Proposal for taking into account the medical, psychological and social aspect of parenthoodamong drug-using female prisoners.Communication, Paris.
Piette, D., Prevost, M., Boutsen, M. et al. (1997).Vers la santé des jeunes en l’an 2000 : Une étude des comportements et modes de vie desadolescents de la Communauté française de Belgique de 1986 à 1994. Health Behaviour inSchool-aged Children. A World Health Organisation Cross-national Study, soutenu par laCommunauté française de Belgique.ULB-Promes, Bruxelles.
Piette, D., De Smet, P. (2000).Rapport Sanomètre : Comportement de santé des adultes en Communauté française.Promes-ULB, Bruxelles.
Pinto,E., Reggers, J., Delhez, M., Fuchs,M., Venneman,I., Lamy, M. and Ansseau, M. (2001).Le sevrage ultra-rapide des toxicomanes aux opiacés sous anesthesie générale : résultatspréliminaires du protocole liégeois.Revue Médicale de Liège, 56, pp. 572-576.
Preumont, C., Bils, L. (2000).Evolution des données relatives à l’indicateur ‘Demandes de traitement’ pour les usagers dedrogues illicites de 1993 à 1998 en Communauté française de Belgique.CCAD, Bruxelles.
Quataert, P., Van Oyen, H. (1995).Gegevensinzameling in verband met middelengebruik door middel van CATI.IHE/Episerie n°6, COOV, IHE, Brussel.
Raes, V. (1995).Het alcohol en druggebruik bij schoolgaande jongeren in Brugge, gegensverzamelingschooljaar 1993-1994.De Sleutel.
Renard, F., Tafforeau, J., Vanderveken, M., Stroobant, A. (1995).Monitoring de la Prévention du Sida en Communauté française de Belgique. Situation en1994.IHE, Bruxelles.
Réseau TIMC (1997).Rapport final 96-97.Praxis et Odyssée, Verviers-Nancy.

References
Belgian National Report on drugs 2002126
Roose, N., Verstuyf, G., Michiels, S. (1999).Voorlopig rapport bevraging samenwerking drughulpverlening - justitie.VAD, Brussel.
Sartor, F., Van Der Linden, H., Desmet, A., Walckiers, D., De Saint-Hubert, B., Leurquin, P.,Van Oyen, H.(2000).Transformation du Point Focal belge sur les drogues et les toxicomanies en un ObservatoireBelge des Drogues et des Toxicomanies. Etude de faisabilité. Service d’Epidémiologie,Bruxelles (Belgique). Institut Scientifique de la Santé Publique, IPH/EPI reports n°2000-020.N° D/2000/2505/43.Transformatie van het Belgisch Focal Point voor drugs en drugsverslaving in een BelgischWaarnemingscentrum voor drugs en drugsverslaving. Haalbaarheidstudie. AfdelingEpidemiologie, November 2000, Brussels (België). Wetenschappelijk Instituut Volksgezonheid,IPH/EPI Reports N°2000-020. N° D/2000/2505/45
Sartor, F., Walckiers, D. (2001).The prevalence of problematic drug use. Methodological aspects and feasibility in Belgium.Arch. Public Health, 59, pp.77-100.
Sartor, F., Walckiers, D., Sasse, A., Bils, L. (2001).Estimate of the prevalence of injecting drug use in Belgium.Arch. Public Health, 59, pp.63-75.
Sasse, A., Van Der Heyden, J., Stroobant, A. (1998).Evolution de l’infection VIH en Belgique 1984-1996.Arch Public Health, 56, pp.187-198.
Sasse, A., Van Kersschaever, G., Stroobant, A. (2001).Le SIDA en Belgique – Situation au 31 décembre 2000.Institut Scientifique de la Santé Publique, Rapport semestriel n°52, Bruxelles.
Sasse, A. (2002).Le SIDA en Belgique – Situation au 31 décembre 2001.Institut Scientifique de la Santé Publique, Rapport semestriel n°54, Bruxelles.
Schepers, A. (1997).Druggebruik en bemiddeling in strafzaken. In: De Ruyver, B., Hap, M., Marchandise, Th.,Schleiper, A., Vermeulen, G. (red.); Drugbeleid 2000.Maklu Uitgevers; Antwerpen/Apeldoorn; p379-380.
Secrétariat Permanent à la Politique de Prévention du Ministère de l'intérieur (2001).Drogues et usage de drogues.Bruxelles.
SGAP/APSD (1998).Aperçu de la criminalité 1997-1998, Statistiques criminelles interpolicières intégrées.
Smets, J. (1996).Jeugdbeschermingsrecht, p.821.Kluwer, België.

References
Belgian National Report on drugs 2002 127
Snacken, S. (1997).Surpopulation des prisons et sanctions alternatives. In Travail d’intérêt général et médiationpénale. Socialisation du pénal ou pénalisation du social?, ed. P. Mary, pp. 367-401.Bruylant, Brussel.
Tafforeau, J., Vanderveken, M., Renard, F.(1995).Evaluation de la prevention du SIDA parmi la population toxicomane : enquête auprès d’unréseau de médecins généralistes de ALTO-SSMG en Communauté française en 1994.IHE, Bruxelles.
Tecco, J., Hariga, F. (2001).The economic burden related to addiction in Belgium.Brussels.
Todts, S., Fonck, K., Colebunders, R., Vercauteren, G., Driesen, K., Uydebrouck, M. etal.(1997).Tuberculosis, HIV, hepatitis B and risk behaviour in a Belgian prison.Arch Public Health, 55, pp 87-98.
VAD (2002).Preventie van Alcohol en andere drugproblemen, Monitoring van activiteiten 2001.Brussel.
VAD (2002).Leerlingenbevraging, schooljaar 2000-2001.Brussel.
Van Baelen, L., Wydoodt, JP (1998).Vlaamse Registratie Middelengebruik (VRM), jaarrapport 1996.VAD.
Vandenbroucke, M., Joosen, B.La problématique des toxicomanes illégaux dans les prisons belges. Situation au 1 décembre1993. Information criminographique, Bruxelles.
Vandenbussche, E., Wydoodt, J.P. (2000).Vlaamse registratie Middelengebruik (VRM): Registratiegegevens 1998.VAD, Brussel.
Vandenbussche, E. (2001).Vlaamse registratie Middelengebruik (VRM): Registratiegegevens 1999.VAD, Brussel.
Vander Beken, T. (2000).In The role of the public prosecutor in the European criminal justice systems, ed. T. VanderBeken and M. Kilchling, pp. 29-37.Koninklijke Vlaamse Academie voor Wetenschappen en Kunsten, Brussels.
Vanderplasschen, W., De Donder, E., Lenoir S., Roets, G. (2001). De leerlingenbevragingover een drugbeleid op school: een bruikbaar instrument?. Brussel: VAD, gent: UniversiteitGent, vakgroep Orthopedagogiek.

References
Belgian National Report on drugs 2002128
Vanderplasschen W., De Bourdeaudhuij I., Van Oost P.(2002).Co-ordination and continuity of care in substance abuse treatment.Evaluation study in Belgium.European Addiction Research, Karger, n° 8, p 10-21.
Vanderveken, M., Meremans, P. (2000).Rapport épidémiologique 1998. CTB-ODB, Bruxelles.
Van Mol, F., Lauwers, N. (1994).Drogues et Prisons. La réalité Pénitentiaire en Matière de Drogue. Actes de la journéed’étude du 22 avril 1994.Présence et Action culturelles, Panopticon, 7/8.
Van Mol, F. (1997).Questionnaire EU network for the prevention of hepatitis and HIV infection in Prisons.
Verhaegen, D., Raes, V., Van Der Kreeft, P., Maertens, G. (1998).Focus of drugs. Verwerking en bespreking van de resultaten van leerlingenbevraging van driescholen in Beveren in het schooljaar 1997-1998.Stad Beveren en De Sleutel.
Verhaegen, D., Raes, V. (1997).Middelengebruik in relatie tot de omgeving bij schoolgaande jongeren in Brugge: eenonderzoek tijdens het schooljaar 1996-1997.Brugge, De Sleutel - vzw Provincialaat der Broeders van Liefde en Stad Brugge.
Verhellen, E. (1996).Jeugdbeschermingsrecht, p.616.Mys & Breesch, Gent.
Verwilghen, M. (2000).Plan fédéral de sécurité et de politique pénitentiaire, p.276.Ministère de la Justice, Bruxelles.
Vranckx, A., De Clercq, M., Navarro, F., Piette, D. (1996).Study of the mental health of youth in secondary schools of Brussels-Capital.ULB-Promes, Brussels.
Walckiers, D., Sartor, F., Sasse, A., Bils, L. (1999).Country Report : Belgium. In : Study to Obtain Comparable National Estimates of ProblemDrug Use Prevalence for all EU Member States.European Monitoring Centre for Drugs and Drug Addiction (EMCDDA, Final Report of projectCT.97.EP.04); Lisbon.
Wanlin, M. (1998).Rapport épidémiologique de la tuberculose 1997 - Région wallonne - Région de Bruxelles-Capitale. FARES, Bruxelles.

References
Belgian National Report on drugs 2002 129
DATA BASES -WEBSITES
Data Bases
Belgian Senate
http://www.senat.be
Federal Service of Information of Council of Ministershttp://faits.fgov.be/cgi/sga_cnct/sfi?LANG=FR
Moniteur Belge, Belgisch Staatsblad.
http://194.7.188.126/justice/index_fr.htm
National Institute of statistics
http://www.statbel.fgov.be
FEDRA Federal Research Actionshttp://www.sstc.fgov.be/belspo/ostc/act_scien/fedra/pres_uk.stm
Web Sites
Arbeitsgemeinschaft für Suchtvorbeugung und Lebensbewältigung (ASL)http://www.asl-eupen.purespace.de/vorbeugungsmodell.htm
Belgian Governmenthttp://www.fgov.be
Centre d'Enseignement et de Recherche en Education pour la Santé
http://www.ste.fapse.ulg.ac.be/STE/Ceres/Pages/fceres.htm
De Sleutelhttp://www.desleutel.org
European Institutionshttp://www.europa.eu.int
Ghent University
http://www.rug.ac.be
Flemish Institute for Health Promotionhttp://www.vig.be
French Community-Health Department
http://www.cfwb.be/sante/index.html
Health Council
http://www.health.fgov.be/CSH_HGR/index.html
Infor Drogueshttp://www.infor-drogues.be
INAMI/RIZIV
http://www.inami.fgov.be
References
Belgian National Report on drugs 2002130
Ministry for Social Affairs, Health and Environment.http://www.minsoc.fgov.be
Ministry of Justicehttp://www.just.fgov.be
Prospective Jeunesse
http://www.prospective-jeunesse.be
Sesamehttp://www.sesame.be/
Université Libre de Bruxelles (ULB)
http://www.ulb.ac.be
ULB Unité de Promotion Education Santé
http://www.ulb.ac.be/esp/promes/sommaire.html
Université de Liègehttp://www.ulg.ac.be
University of Antwerpen
http://www.ufsia.ac.be/
University of Leuvenhttp://www.kuleuven.ac.be
Vereniging voor Alcohol- en andere Drugproblemenhttp://www.vad.be


Annexes


Annexes
Belgian National Report on drugs 2002134
ANNEX 1 : DRUG MONITORING SYTEM AND SOURCES OF INFORMATION
ÿ Description of the Belgian National Focal Point and partners
The Belgian Information Reitox Network (BIRN) was created in 1995 and links theNational Focal Point (FP) with the Sub-Focal, umbrella organisations for a region orcommunity specialised in drug matters. The Focal Point is the direct link between theEMCDDA and the BIRN.The Belgian Information REITOX Network (BIRN) BIRN members meet almost everymonth. Expert working groups (reference groups) on the key indicators, on demandreduction and on the Early Warning System meet regularly.A Steering Committee, meeting at least once a year, ensures the follow-up of theREITOX network activities. Representatives of the administrations and ministers fromdifferent governmental levels (federal, regional and community), as well as theBelgian representatives in the Management Board and Scientific Committee of theEMCDDA are members of this steering committee. Exchange of informationbetween Focal Point and member of the Management Board is regular, such as forinstance before and after EMCDDA meetings.A member of the BIRN participates in the meetings of the group Epidemiology of thePompidou Group.
EMCDDA
BELGIAN REPRESENTATIVES EMCDDA
STEERINGCOMMITTEE
ManagementBoard
ScientificCommittee
BIRN
IPH
Focal Point
ASL EUROTOX Sub-Focal Points ODB-CTB VAD
GermanSpeaking
Community
FrenchCommunity
Region ofBrussels
FlemishCommunity

Annexes
Belgian National Report on drugs 2002 135
THE FOCAL POINT : ORGANISATION, STRUCTURE AND BUDGET
The Focal Point is located at the Scientific Institute of Public Health (I.P.H.), formerlyInstitute of Hygiene and Epidemiology. It is the scientific research institute of theministry of Social Affairs, Public Health and the Environment. The Focal Point isfunded and managed in collaboration with the Communities and the federalministries.The Focal Point's mission is to respond to queries from EMCDDA, to collect andsynthesise epidemiological data on the drug problem, to participate in activities of theBIRN, and to ensure dissemination of information both between the Belgian partners,and between these partners and the EMCDDA.In 1999, the budget of the Focal Point is 5.6 million BEF (140,000 EURO). The wholeof this amount comes from the Flemish and French Communities. A financial supportis also available from EMCDDA (shared between the Focal Point and the Sub-FocalPoints for the completion of some core tasks). A feasibility on the transformation ofthe Belgian Focal Point in a Belgian Monitoring Centre is supported by the FederalMinistry of Public Health.
THE SUB-FOCAL POINTS
Vereniging voor Alcohol- en andere Drugproblemen - VAD
The VAD (Association for Alcohol and other Drug Problems) was established in 1982and is active in the Flemish Community (5.9 million inhabitants in Flanders andaround 0.2 million Flemish in Brussels).
ObjectivesThe goals of the VAD are- the study, the prevention and treatment of problems related to alcohol and otherdrug use through:- the organisation of training- the organisation of discussion platforms and networks- the co-ordination and support of existing and innovative initiatives in the field ofstudy, prevention and treatment- the organisation of a telephone help line- the collection of data.
Structure and organisationThe VAD is a non-profit organisation grouping 47 member organisations which havepreventive and curative goals. The members constitute the General Assembly whichdesignates a Committee of Directors. The members of this Committee of Directorsdesignate a Management Committee and allocate the responsibilities. The dailyoperations of the VAD are carried out by staff under the supervision of a director.
Financing and budgetThe VAD is an official institution within the Flemish Institute for the Promotion ofHealth. As such, for 1998, it received a fixed subsidy of 20 million BEF (500 000EURO). In addition to this basic subsidy, the VAD receives subsidies for thepreparation and implementation of specific projects, which are often short-term. ForEuropean projects, VAD receives funds from EMCDDA through the BIRN.
External relations and collaborations

Annexes
Belgian National Report on drugs 2002136
As the Flemish Sub-Focal Point, together with the Focal Point and the other Sub-Focal Points, it is part of the Belgian Information Reitox Network (BIRN), andensures that its engagements with the European Monitoring Centre for Drugs andDrug Addiction in Lisbon, are honoured. There is active participation with thePompidou Group, with the European Drug Prevention Week and with WHO.
EUROTOX - EUROTOX
EUROTOX was established in 1990 and regroups three organisations active indifferent fields linked to drug use:
- Infor-Drogues telephone help line, prevention, and outpatient treatment- Modus Vivendi : AIDS prevention, harm reduction, training, liaison and
research- Prospective Jeunesse : prevention, training and assistance.
ObjectivesThe specific objectives of Eurotox are :
- to carry out research projects in the field of drug use- to organise conferences, seminars- to observe drug use phenomenon in the French Community of Belgium.
Structure and OrganisationEurotox is a non profit organisation. Its General Assembly and Executive Board iscomposed of representatives of the three organisations, Infor-Drogues, ModusVvendi and Prospective Jeunesse.
Financing and budgetIn addition to the funds in each of the members association, current funding level ofEurotox is 5.5 million BEF (137 500 EURO) a year.
External relations and collaborationsSince September 2000, Eurotox is part of the BIRN, as Sub-Focal Point for theFrench Community of Belgium.
Concertation Toxicomanies Bruxelles - Overleg Druggebruik Brussel - CTB-ODB
The CTB-ODB (the Brussels Drug Addiction Programme) was set up by a ministerialDecree of 15 September 1994. The programme covers the Brussels-Capital Regionwhich is made up of 19 urban municipalities, representing a population of almost onemillion inhabitants.
ObjectivesThe Brussels Drug Programme, with an emphasis on reducing demand, bringstogether those involved in helping drug addicts in prison, treatment centres, crisiscentres and short stay centres, hospital centres, 24-hour hot-line services,prevention, mental health care centres, assistance, rehabilitation, day centres andambulatory care.
Annexes
Belgian National Report on drugs 2002 137
Two objectives of CTB/ODB deal with external collaborations (with the variousauthorities in Belgium and with international collaborators).
Structure and organisationA co-ordinator has been engaged by the association to implement the programme;he is assisted by a part-time secretary. The co-ordinator regularly reports to aSteering Committee made up of representatives of the associations, of thecompetent ministers, of the "Concertation and Co-ordination Committee” (see below)and of observers representing the Minister-President of the Region and the ministerscompetent for Assistance to persons. The Concertation and Co-ordinationCommittee is made up of experts from the field (social and medical), as well aslawyers, delegates from the Justice Department, from the Public Prosecutor's office,and the federal and local police forces.
Financing and budgetThe programme's budget is established annually. The amount for the first year was 5million BEF (125 000 EURO), and for the current year 6 million BEF (150 000EURO). A part of this amount helps to fulfil European obligations. Additional supportfrom EMCDDA through the BIRN is available for specific EMCDDA core-tasks.
Arbeitsgemeinschaft für Suchtvorbeugung und Lebensbewältigung - ASL
The ASL (Association for drug use prevention and for a better quality of life) is anautonomous NGO since 1997 (it was part of the Centre for Mental Health since1980), and officially recognised by the Government of the German-speakingCommunity. The care activity of the ASL extends to the 70,000 inhabitants of thenine municipalities of the German-speaking Community of Belgium.
ObjectivesThe ASL is responsible for drug use primary prevention in the German-speakingCommunity. It is also partially involved in secondary prevention. The goals of theASL are to make the entire population aware of the dangers of addiction of all kindsand to improve the quality of life. It encourages healthy activities for the well being ofthe population and co-ordinates current activities. With regard to its area ofresponsibility, the ASL makes efforts in order to establish a dynamic relationship withthe political decision makers in the German-speaking Community.The ASL, in its role as co-ordination institution within the German-speakingCommunity in Belgium, is responsible for co-ordinating the registration of statisticaldata, including the record of the first treatment demand.
Structure and OrganisationThe ASL is mainly made up of voluntary workers. At every level of society, there is ateam of workers developing and co-ordinating the prevention effort. All the teams areco-ordinated by a central co-ordination team. In recent years, the ASL hasconcentrated its activities at the level of the municipality. It aims to create a workinggroup in each municipality which will bring together, in the heart of the municipality,all those people who are interested in active prevention.The prevention model developed by ASL was evaluated by a group of experts(University of Fribourg, Switzerland) in 1997: it was certified effective and consistentthrough its global and community approach.Financing and budget

Annexes
Belgian National Report on drugs 2002138
The ASL is subsidised by the government of the German-speaking Community. Itreceives the amount of 4.7 million BEF (120 000 EURO) to cover staff and operatingcosts. The staff consist of a full-time co-ordinator, a therapist in drug addiction, andseveral secretaries (70 hours per week). Additional support from EMCDDA throughthe BIRN is available for specific EMCDDA core-tasks.
External relations and collaborationsIt is part of the Belgian Information REITOX Network.The ASL collaborates with partners in eleven West and East European countries.The objective is to adopt a long term, global community approach to preventiveactions in the municipalities of these countries. This project is supported by the EU.
ÿ Early Warning System on New Synthetic Drugs: Sources of information
The Early Warning system in Belgium does not focus on NSDs only. All drugs canbe subject to an Early Warning and thus information on other drugs is collectedthrough the same network that is used for the synthetic drugs.
There are several channels through which different kinds of information can becollected. These channels all have their plusses and shortcomings, but together theygive a quite good overview of the situation.
1) Scientific information on NSDs: This kind of information can be supplied by thelaboratory network that consists of both forensic and non-forensic toxicologicallaboratories. These laboratories perform analyses on samples of drugs and/orbiological samples such as blood, urine, … of drug users. Analyses on seized drugscan provide chemical information on NSDs and data on the appearance of drugs(e.g. weight, colour or monogram when it concerns a tablet). Biological samples(originating from emergency wards, drug treatment centres, autopsies…) provideinformation on the effects of drug use.
2) Social and cultural information on NSDs: The kind of information hereby meant,comes from the users and field workers, is not linked to specific cases and can becollected by the Focal Point and the Sub-Focal Points. Important sources are thePoison Control Centre and the "drug telephone helplines" (Druglijn and Infor-drogues) that collect information from the phone calls they receive from people indistress or asking for information. It is however not easy to detect new syntheticdrugs at users’ level in an early stage, because drug users can seldom provideinformation on the chemical composition of the drugs they use. NSDs are oftenpresented in the form of tablets bearing logos that provide no clue to the chemicalcontents. This obviously complicates the exchange of information on new syntheticdrugs. Therefore the laboratory network and the social-cultural network should becomplementary: chemical and clinical information can serve to identify NSDs moreefficiently at users’ level.3) Medical information and information on drug-related emergencies. This kind ofinformation can serve to assess health consequences of drug use and to monitordrug use trends. Sources for this kind of information are emergency departments andother hospital wards and to some extent, the Poison Control Centre and thetelephone helplines. One of the problems encountered in this field is the fact thatdetailed information on the substance involved in the intoxication is often missing.Information can also be found in the press. Although the press cannot be considered

Annexes
Belgian National Report on drugs 2002 139
as a reliable source, since articles in newspapers can be based on rumours and donot ensure coverage of all intoxications in a certain region, it can be a starting pointfor further research.

Annexes
Belgian National Report on drugs 2002140
Belgian Information REITOX Network : Structure
FOCAL POINT
IPH - ISP – WIVScientific Institute of Public HealthInstitut Scientifique de la Santé PubliqueWetenschappelijk Instituut VolkgezondheidRue J. Wytsmanstraat, 14B - 1050 BRUSSELS
Responsible : Denise WALCKIERS
Scientific collaborators : Kathy Colpaert, Guido Jossels, Edith Leus, JuanPablo Protto, Francis Sartor, Sandrine SleimanAdministrative collaborator : Dominique Haezebrouck
Tel : 32-2/642.57 12; Fax : 32-2/642.54.10
Belgium
e-mail : [email protected] Web site : http://www.iph.fgov.be/reitox
SUB-FOCAL POINTS
ASL :Arbeitsgemeinschaft für Suchtvorbeugungund LebensbewältigungKlosterstrasse, 3B - 4700 EUPEN
Responsible : Norbert GENSTERBLUMTel. : 32-87/74.36.77; Fax : 32-87/74.04.72e-mail : [email protected]
The German speaking Community
CTB / ODB :Concertation Toxicomanies BruxellesOverleg Druggebruik BrusselQuai du commerce/ handelskaai ,7B - 1000 BRUXELLES–BRUSSEL
Responsible : Mark VANDERVEKENTel : 32-2/289.09.60; Fax : 32-2/512.38.18.
e-mail : [email protected]
The Region of Brussels-Capital
EUROTOX :(Com.française)
Rue de Haerne, 51B - 1040 BRUXELLES
Responsible : Fabienne HARIGATel. : 32-2/644.22.00Fax : 32-2/644.21.81
e-mail : [email protected]
The French Community
VAD :Vereniging voor Alcohol- en andere
DrugproblemenTollenaerestraat, 15
B - 1020 BRUSSEL
Responsible : Ilse De MAESENEIRETel : 32-2/423.03.46; Fax : 32-2/423.03.34
e-mail : [email protected]
The Flemish Community

Annexes
Belgian National Report on drugs 2002 141
ANNEX 2 LIST OF TABLES
Table 1 : Lifetime prevalence rate (%) of cannabis use among the adult population, FrenchCommunity, 96-2000 29
Table 2 : Lifetime prevalence (%) of drug use among the school population aged 15-18 yearsfor Flemish and French Communities, 94-2000 31
Table 3 : Last month prevalence (%) of drug consumption among students, FlemishCommunity schools, 2000 32
Table 4 : Frequency (%) of cannabis use during the last month; Flemish Community schools,94-2000 32
Table 5 : Lifetime prevalence of injecting drug use in the population aged 15-64 years, in 95and 1997 34
Table 6 : Number and prevalence of opiate users in the French Community, 93-1994 35Table 7 : Percentage of injecting users in Charleroi, 95-2001 35Table 8 : Percentage of lifetime and current IDUs and sharing syringes among current IDUs,
French Community, 93-2001 36Table 9 : Percentage of current IDUs according to drug used, French Community, 99-2001 36Table 10 : Percentage of IDUs, Rock festival, French Community, 96-2001 37Table 11 : Proportion of poly-drug use, Rock festival, French Community, 96-2001 37Table 12 : Proportion of drug-related deaths with certificates mentioning involvement of
psychoactive substances (%), Belgium, 91-1996 39Table 13 : Percentage of self-reported HIV-seropositivity among IDUs asking for treatment in
centres of the French and Flemish Communities, 93-2000 42Table 14 : Sero-prevalence of HIV in an outpatient clinic, Antwerp, 2001 43Table 15 : Percentage of hepatitis B infected among IDUs asking for treatment, in centres of
the French and Flemish Communities, 97-2000 44Table 16 : Percentage of hepatitis C infected among IDU asking for treatment, in centres of
the French and Flemish Communities, 97-2000 45Table 17 : Sero-prevalence (%) of HBV and HCV in an outpatient clinic, Antwerp, 2001 45Table 18 : Number of drivers and number of substances for which they were tested positive in
the Rosita-study, 99-2000 46Table 19 : Frequency of occurrence of the substances controlled by the law of 16/03/99 in the
samples tested positive during the Rosita-study 47Table 20 : Number and proportion (%) of infringements related to narcotics according to the
type of infringement, Belgium, 96-2000 49Table 21 : Evolution of conviction and dismissal 96-2000 51Table 22 : Number of detainees for drug-related offences, Belgium, 90-1998 51Table 23 : End of year population (%) for drug-related offences per legal status,
Belgium,1998 52Table 24 : Mean price at street level of some illegal substances, Belgium, 96-2001 55Table 25 : Mean purity at street level of some illegal substances, Belgium, 2000-2001 55Table 26 : Distribution of substances in samples of drugs seized in 2000 and 2001 56Table 27 : Distribution of synthetic drugs in samples of drugs seized in 2000 and 2001 57Table 28 : Telephone help-lines 2000-2001 73Table 29 : Percentage by age of callers, 2001 74Table 30 : Last month prevalence (%) of drug use, French Community, 2001-2002 104Table 31 : Number of drug-related deaths in 12-17 year-olds in Belgium according to
substance, 91-1996 106

Annexes
Belgian National Report on drugs 2002142
ANNEX 3 LIST OF FIGURES
Figure 1 : Proportion of young people aged 13-17 years having used a drug at leastonce and during the last month, French Community secondary schools 1988-1998 33
Figure 2 : Number of drug-related deaths according to the EMCDDA selections A, Band C, Belgium, 1991-1996 39
Figure 3 : Percentage of IDUs among new HIV-cases from 1986 to 2001 in Belgium 41Figure 4 : Percentage of IDUs among new HIV-cases from 1986 to 2000 in Belgium,
according to sex 41Figure 5 : Number of people taken in for questioning, Belgium, 1997-2000 50Figure 6 : Quantities of products seized 1985-2000, Belgium, 54

Annexes
Belgian National Report on drugs 2002 143
ANNEX 4 LIST OF ABBREVIATIONS
APSD/SGAP Algemene Politiesteundienst / Service Général d’Appui Policier
ALTO Alternatives aux Toxicomanies
ASBL Association Sans But Lucratif (non-profit organisation)
ASL Arbeitsgemeinschaft für Suchtvorbeugung und Lebensbewältigung
AVAT Aide Vervietoise aux Alcooliques et Toxicomanes
BCR/CBO Bureau Central de Recherche - Programme Drogue / Centraal Bureau voor Opsporing– Programma Drugs / Central investigation office – Drug programme
CAD Centrum voor Alcohol- en andere Drugproblemen (Hasselt)
CAPA Centre d’Actions de Prévention des Assuétudes
CAT Centrum voor studie, behandeling en preventie van Alcoholisme en andereToxicomanieën (Ghent)
CBO/ BCR Centraal Bureau voor Opsporing – Programma Drugs / Bureau Central de Recherche -Programme Drogue / Central investigation office – Drug programme
CCAD Comité de Concertation sur l’Alcool et les autres Drogues
CCLA Citoyen Comme Les Autres
CGG Centrum voor Geestelijke Gezondheidszorg
CIC CrisisInterventieCentrum
COCOF Commission Communautaire Française (Communauté française à Bruxelles)
CPAS/OCMW Centre Public d’Aide Sociale / Openbaar Centrum voor Maatschappelijk Welzijn
CTB/ODB Concertation Toxicomanies Bruxelles / Overleg Druggebruik Brussel
CFWB Communauté française Wallonie Bruxelles
DWTC/SSTC Federal Diensten voor Wetenschappelijke, Technische en Culturele aangelegenheden/ Services fédéraux des affaires Scientifiques, Techniques et Culturelles
EDDRA Exchange On Drug Demand Reduction Action
EMCDDA European Monitoring Centre for Drugs and Drug Addiction
FNRS Fonds National de Recherche Scientifique
GEMT Groupe d’Etude des Maladies liées à la Toxicomanie
GERRMM Groupe d'Etude pour une Réforme de la Médecine Rhin-Meuse
HBSC Health Behaviour in School-aged Children
INAMI/RIZIV Institut National d’Assurance Maladie-Invalidité/RijksInstituut voor Ziekte- enInvaliditeitsverzekering
IPH/ISP/WIV Scientific Institute of Public Health/ Institut Scientifique de la Santé Publique/Wetenshappelijk Institut Volksgezondheid
ISP/WIV/IPH Institut Scientifique de la Santé Publique/Wetenshappelijk Institut Volksgezondheid/Scientific Institute of Public Health
IVDU Intra-Venous Drug Use
IVDUs Intra-Venous Drug Users
KUL Katholieke Universiteit Leuven
LOGO Loco-regionaal-Gezondheidsoverlegen Organisatie (Flemish Community)
MASS/MSOC Maison d’Accueil Socio-Sanitaire / Medisch-Sociale Opvang Centra
MKG/RCM Minimale Klinish Gegevens / Résumé Clinique Minimal
MPG/RPM Minimale Psychiatrische Gegevens / Résumé psychiatrique Minimal
MSOC/MASS Medisch-Sociale Opvang Centra / Maisons d’Accueil Socio-Sanitaire
OCMW/CPAS Openbaar Centrum voor Maatschappelijk Welzijn / Centre Public d’Aide Sociale
OCRTIS Central Office for the Repression of Illicit Narcotics Trafficking
PZ Psychiatrisch Ziekenhuis
Annexes
Belgian National Report on drugs 2002144
PPP Provinciale Preventieplatforms (Flemish Community)
PAAZ Psychiatrische Afdeling van een Algemeen Ziekenhuis
RCM/MKG Résumé Clinique Minimum / Minimale Klinish Gegevens
REITOX Réseau Européen d'Information sur les drogues et Toxicomanies / Europeaninformation network on drugs and drug addictions
RIZIV/INAMI RijksInstituut voor Ziekte- en Invaliditeitsverzekering/Institut National d’AssuranceMaladie-Invalidité
RPM/MPG Résumé Psychiatrique Minimum / Minimale Psychiatrische Gegevens
SGAP/APSD Service Général d’Appui Policier / Algemene Politiesteundienst
SODA Stedelijk Overleg Drugs – Antwerpen
SPZ Sozial Psychologisches Zentrum
SSTC/DWTC Services fédéraux des affaires scientifiques, techniques et culturelles / Federaldiensten voor wetenschappelijke, technische en culturele aangelegenheden
TG Therapeutische Gemeenschap
TIMC Toxicomanies et Interventions en Milieu Carcéral
ULB Université Libre de Bruxelles
UNDCP United Nations International Drug Control Programme
UG Universiteit Gent
ULG Université de Liège
VAD Vereniging voor Alcohol- en andere Drugproblemen
VIG Vlaamse Instituut voor Gezondheidspromotie
VLOR Vlaamse Onderwijs Raad (Flemish Community)
VRM Vlaamse Registratie Middelengebruik
VSPP Vast Secretariaat voor het Preventiebeleid / Secrétariat Permanent à la Politique dePrévention
VAD Vereniging voor Alcohol en andere Drug problemen
VVBV Vlaamse Vereniging voor Behandelingscentra in de Verslaafdenzorg
VZW Vereniging Zonder Winstoogmerk (non-profit organisation)
WIV/ISP/IPH Wetenshappelijk Institut Volksgezondheid/ Institut Scientifique de la Santé Publique//Scientific Institute of Public Health

Annexes
Belgian National Report on drugs 2002 145
ANNEX 5 INDEX
A
arrests 7, 48
B
budget 21, 22, 97, 98, 99, 133, 134, 135, 136
D
doping 17, 23Drug Cell 4, 5, 12, 16, 21
E
EWS 54, 77
F
Federal Drug Policy Note 11, 16, 17, 19, 20, 107, 108, 110, 111
H
HBSC 5, 29, 30, 58, 59helplines 72, 136hepatitis 6, 7, 27, 41, 60, 64, 76, 79, 81, 90, 91, 92, 106, 117, 119HIV 6, 7, 15, 17, 27, 33, 39, 60, 64, 79, 89, 90, 91, 92, 106, 113, 119
I
IDU 7, 33, 35, 39, 42, 106
L
local communities 73
M
media 19, 20, 74mental health care 12, 13, 23, 27, 84, 135Methadone 35, 72, 76, 85, 103
N
needle exchange 14, 76, 77, 78, 79, 80, 81, 90
O
overdoses 6, 38, 60, 79, 80, 105, 112
P
prison 13, 42, 44, 51, 76, 77, 79, 80, 87, 89, 108, 110, 111, 134public opinion 19, 64
R
Rosita-study 45
S
Security and Society Contracts 14, 22

Annexes
Belgian National Report on drugs 2002146
Snowball surveys 34substitution treatments 12, 13, 17, 86, 90, 97syringes 35, 78, 79
T
TDI 5, 6, 37, 47, 59, 60