Embed Size (px)
Citation preview
8/3/2019 Belgium Phase 1 Requirements
http://slidepdf.com/reader/full/belgium-phase-1-requirements 1/6
88 ICT l www.samedanltd.com
ICT Regulatory & Business Practice
RegulatoryRequirements
Walter Janssens, Kristof Bonnarens and Greet Musch at the Federal Agency for Medicinal
and Health Products, Belgium, discuss regulatory requirements in early-phase development
Questions have often been asked about the possibility of
conducting exploratory clinical trials and microdose studies to
obtain data in humans, in order to decide on the feasibility of
starting full development. These trials would be conducted
with limited human exposure and therefore are also supported
by limited, but essential, preclinical data. At this stage, the
availability of the investigational medicinal product is limited.
To allow these kinds of trials, and in order to provide clear
instructions, a guidance document was developed in
consultation with the stakeholders. Since June 2007,
exploratory clinical trial applications (eCTA), also termed
Phase 0 studies, have been evaluated in Belgium according to
this guidance document. The number of eCTA, which are
mostly, but not exclusively, first-in-human studies, suggests
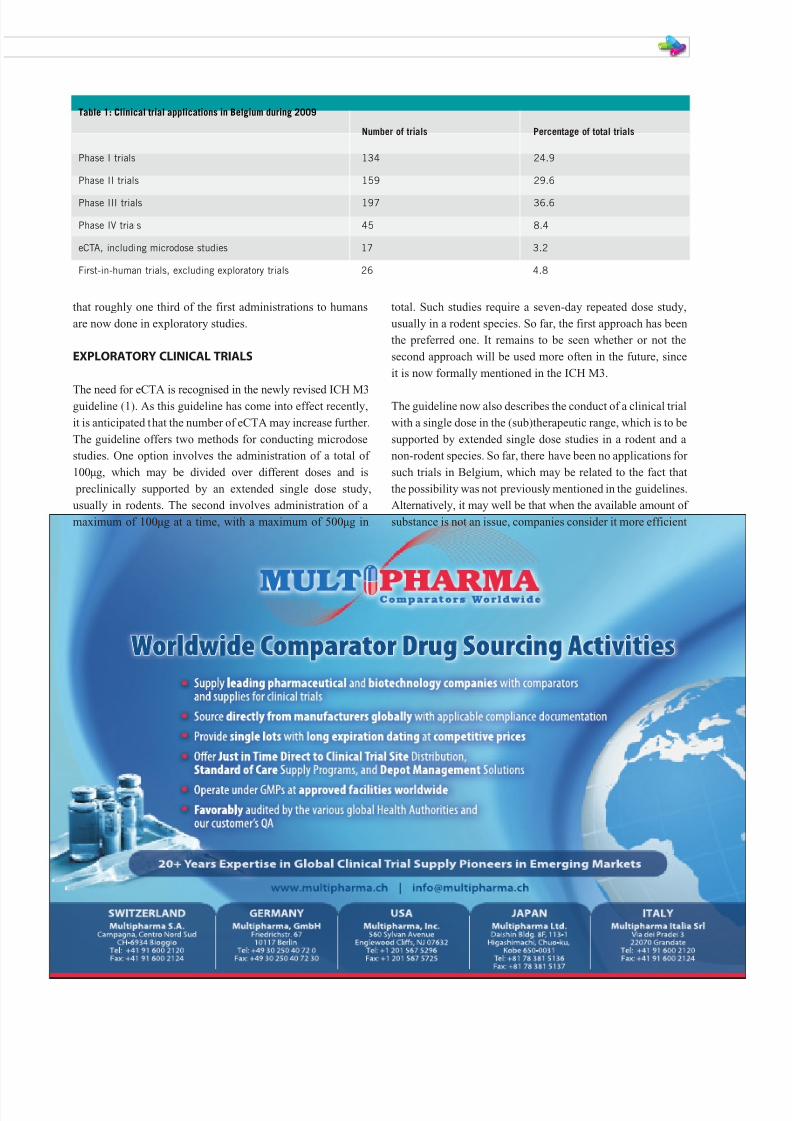
The number of clinical trials in early-phase development that are submitted to
the Belgian Federal Agency for Medicines and Health Products (FAMHP) is
relatively high. This is exemplified by the number of Phase I and Phase II
studies in Table 1. Although these numbers also include clinical trials that are
conducted with products that are already in further stages of development,
they reflect, to a large extent, first trials in humans, and other Phase I or IIa
clinical trials with the aim of establishing the doses to be used in Phase IIb
and Phase III studies. The number of first-in-human trials is given separately
and sometimes includes Phase II trials. This number further illustrates the
relative importance of early-phase clinical trials in the clinical trial activities
that were submitted to the FAMHP.
8/3/2019 Belgium Phase 1 Requirements
http://slidepdf.com/reader/full/belgium-phase-1-requirements 2/6
that roughly one third of the first administrations to humans
are now done in exploratory studies.
EXPLORATORY CLINICAL TRIALS
The need for eCTA is recognised in the newly revised ICH M3guideline (1). As this guideline has come into effect recently,
it is anticipated that the number of eCTA may increase further.
The guideline offers two methods for conducting microdose
studies. One option involves the administration of a total of
100µg, which may be divided over different doses and is
preclinically supported by an extended single dose study,
usually in rodents. The second involves administration of a
maximum of 100µg at a time, with a maximum of 500µg in
total. Such studies require a seven-day repeated dose study,
usually in a rodent species. So far, the first approach has been
the preferred one. It remains to be seen whether or not the
second approach will be used more often in the future, since
it is now formally mentioned in the ICH M3.
The guideline now also describes the conduct of a clinical trial
with a single dose in the (sub)therapeutic range, which is to be
supported by extended single dose studies in a rodent and a
non-rodent species. So far, there have been no applications for
such trials in Belgium, which may be related to the fact that
the possibility was not previously mentioned in the guidelines.
Alternatively, it may well be that when the available amount of
substance is not an issue, companies consider it more efficient
Number of trials Percentage of total trials
Phase I trials 134 24.9
Phase II trials 159 29.6
Phase III trials 197 36.6
Phase IV trials 45 8.4
eCTA, including microdose studies 17 3.2
First-in-human trials, excluding exploratory trials 26 4.8
Table 1: Clinical trial applications in Belgium during 2009

8/3/2019 Belgium Phase 1 Requirements
http://slidepdf.com/reader/full/belgium-phase-1-requirements 3/6
90 ICT l www.samedanltd.com
to conduct 14-day repeated dose studies from the beginning,
as opposed to conducting two extended single dose studies,
and may therefore prefer to use one of the approaches that
would also allow repeated administration to humans.
The guideline lists two possibilities to support the conduct of
exploratory clinical trials with a maximal duration of 14 days.
The first possibility is based on the conduct of a rodent and a
non-rodent study of 14 days. The other possibility involves a14-day toxicity study in a justified rodent species and a
confirmatory study in a non-rodent at a dose yielding an
exposure similar to the rodent no observable adverse effect
level (NOAEL), and with a duration of at least the clinical
exposure. In addition, safety pharmacology and genotoxicity
studies should be available. For further discussion of the other
preclinical requirements, the ICH M3 guideline should be
consulted. Whereas the ICH M3 guideline gives five
examples to conduct exploratory trials, it also states that other
scientifically justified possibilities may be considered. In
such cases, previous consultation with the competent
authority may be required. Therefore, the procedure for submission of eCTA in Belgium involves a presubmission and
a scientific advice procedure can also be started.
STARTING DOSE
The establishment of a safe starting dose is the first concern
that needs to be addressed. First of all, a pharmacodynamic
rationale should be provided indicating that there is scientific
support for potential therapeutic effects. This should be based
on knowledge of the disease process and on the package of in
vitro and animal in vivo data showing that the substances
concerned influence target organs, cells or mechanisms insuch a way that they can be assumed to modify the pathology.
This package should also allow the concentrations or
exposures that can be presumed to cause such a therapeutic
effect to be determined. Importantly, the lowest exposure level
that would cause a biologically relevant effect should also be
estimated from these data. This is of particular importance if
the substance is a first-in-class product that addresses a new
target that has not yet been investigated in humans or where
relatively little knowledge has so far been accumulated. Such
knowledge would be needed to implement the EMA guideline
on the mitigation of risks in first-in-human clinical trials,
because the starting dose should then definitely take theminimal anticipated biological effect level into account (2). It
is obvious that in such cases the animal species that were used
should be justified, and the similarities and differences
between the animal target and the human target should
be described.
In cases where interference with the target can be predicted,
the pharmacodynamic action should still be taken into
account to choose the starting dose. Indeed, the anticipated
effect should remain within limits that are predicted to be
safely tolerated by the healthy volunteers or patients involved
in the trial; this will allow a decision to be made on whether
further development is warranted or not. The other important
determinant of the starting dose is the NOAEL in the most
sensitive species. When two rodent and non-rodent species are
used in the toxicology testing, the starting dose should not
exceed two per cent of the AUC at the highest dose in the
species with the lowest exposure if no toxicity was observed.
If toxicity is observed, or when toxicity relies on the
rodent species with confirmatory testing in non-rodents, the
NOAEL should be used to guide the selection of the starting
dose. The starting dose should lead to a maximal expected
exposure of two per cent of the AUC at NOAEL in the mostsensitive species. It should be noted that if the non-rodent
species is more sensitive to adverse effects than the non-
rodent in the last approach, further testing in the non-rodent
may be required.
DOSE ESCALATION
After the establishment of a safe starting dose, it is equally
important to consider the dose escalation procedure. It is
indeed possible that adverse effects to humans may not
manifest themselves at the first low dose, but they may
become more prominent when really active doses are reached during dose escalation. Fortunately dose escalation can be
guided by the observations at the lower doses in humans with
regard to pharmacokinetics, first indications of the magnitude
of the pharmacodynamic effect, measurement of biomarkers
related to potential adverse effects or the first signs of
evolving untoward effects in addition to the existing animal
data. Since exploratory clinical trials are not supposed to aim
to establish the maximal tolerated dose, the occurrence of
adverse effects may be a reason to halt dose escalation.
Anyway, clear stopping rules should be given in the protocol,
based on the preclinical findings. Effects, whether considered
pharmacodynamic or adverse, that occur during anexploratory trial should be monitorable and be neither severe
nor serious. If unexpected adverse effects occur during the
conduct of an exploratory clinical trial, this would certainly be
considered a clear sign that further dose escalation is not
possible or at least must be reconsidered.
MAXIMAL DOSES
The maximal dose that may be administered in an exploratory
clinical trial is determined in the first place by the limits given
in the guideline. The limit is obvious in the case of microdose
studies; otherwise the maximal dose is defined by the NOAELin animals. The exposure in humans should not surpass one
half of the AUC at NOAEL in rodents or the AUC at NOAEL
in non-rodents, whichever is lower. In those cases where no
toxicity is determined in animals, it is not possible to monitor
for potential prodromes of adverse effects, but on the other
hand the substance under investigation may have a large
safety margin. To remain on the safe side, the maximal
exposure in humans in this case should not exceed one tenth
of the lowest AUC at NOAEL in the most sensitive species. As
indicated above, the observed effects during the dose
escalation may also result in an upper boundary to the
allowable dose in humans. If the animal data predict that
adverse effects will be monitorable and limited in magnitude,
the observations in humans may allow escalation of the dose

8/3/2019 Belgium Phase 1 Requirements
http://slidepdf.com/reader/full/belgium-phase-1-requirements 4/6
www.samedanltd.com ICT l 91
beyond the limits that are proposed in the guideline. In
general, this would require an amendment to the protocol to
be submitted.
ESTIMATING HUMAN DOSES
One of the ways to transform animal doses into human doses
remains the classic scaling method that takes body surface
into account, and can always be used to check human doses
calculated in other ways (3,4). If there is a large discrepancy between modelled human doses and scale doses, this should
be justified. Nowadays, companies often use models that
should predict human exposure at a certain dose, based upon
observations in animals. Measured exposures in animals at
NOAEL and at doses indicative for therapeutic efficacy can
further be used to predict human doses that will be
marginally active, will have pharmacodynamic effect or may
cause adverse effects. In vitro concentrations to induce
activity and plasma concentrations in animals at effective or
toxic doses may further be used to refine predictions of the
starting dose. Since these estimates will be subject to a
number of uncertainties, and humans may be more sensitivethan expected or may reach higher exposure, a safety factor
should be taken into account. Once the first data in humans
has been obtained, the predictions can be further refined. A
pause when nearing potentially critical exposures in humans
may be required.
MAGNITUDE OF PHARMACODYNAMIC EFFECTS
In exploratory clinical trials, a certain predefined
pharmacodynamic effect may be required. When the
substance under investigation targets a new mechanism that
has not yet been explored in humans, the maximal effect mayneed to be set at a lower level, or be approached in smaller
steps than with a known mechanism of action. The decision on
what effect is acceptable also depends on whether the effect
aimed at is, for instance, a receptor or enzyme occupation,
inhibition or activation of the target, which organs and organ
systems are likely to be affected, and how target occupation is
correlated to a physiological effect. In this context, it is also
important to consider whether healthy volunteers will be
involved in the trial, with the advantage of better control and
less variability, or whether stable, otherwise healthy patients
with moderate disease will be involved. The latter may allow
better prediction of target involvement and potential
therapeutic benefit, in addition they may tolerate a
pharmacodynamic effect better.
PRESUBMISSION PROCEDURE
In Belgium, a presubmission procedure has been agreed
between the agency and the different stakeholders. This
means that in the conduct of exploratory trials, the applicant
is supposed to provide an outline of the project, indicate
what preclinical data will be available and identify potential
issues that may be discussed before the submission of the
actual trial application. This will allow a face-to-face
meeting, teleconference or written discussion between theagency, applicant and ethics committee when needed, to
discuss diversions from the guideline and on safety issues
when a substance with a new mechanism of action is
involved. In a large majority of cases, such a formal meeting
was not deemed necessary after the presubmission
procedure was activated. On the other hand, it should be
noted that only in exceptional cases were major issues
raised by the agency during the evaluation, possibly because
any issues were cleared beforehand. In general, the
presubmission procedure does not seem to cause time
delays and the regular 15-day deadline foreseen by Belgian
Law for review of a Phase I CTA can also be maintained for eCTAs.
CLASSIC PHASE I TRIALS
The main difference between exploratory clinical trials and
Phase I trials is that the potential toxicity is better defined in
the animal experiments. Usually the safety pharmacology, and
in particular the cardiovascular safety pharmacology, will be
better addressed in a dedicated study, whereas for exploratory
trials this may be studied in the course of the toxicology
studies. The augmented degree of documentation of effects
allows the substance to be dosed higher, and dose escalationmay go up to the maximal tolerated dose in classic Phase I
studies. Obviously the severity and seriousness of expected
adverse effects at a given exposure should be taken into
account in order to determine the maximal dose that can be
administered. With regard to the starting dose and dose
escalation, the same rules as for exploratory clinical trials can
be applied and the same guidelines should be followed.
Whereas exploratory clinical trials mostly seem to be
performed when there is a choice to be made between different
substances and it allows projects to be terminated in a very
early phase when relatively little investment has already been
made, the classic Phase I study allows easier connection to
further development and, if there is no choice to be made, may
save some time. Whereas there is no presubmission procedure
In Belgium, a presubmission procedure has been agreed between the
agency and the different stakeholders. This means that in the conduct
of exploratory trials, the applicant is supposed to provide an outline
of the project, indicate what preclinical data will be available and
identify potential issues that may be discussed before the submission
of the actual trial application.

8/3/2019 Belgium Phase 1 Requirements
http://slidepdf.com/reader/full/belgium-phase-1-requirements 5/6
92 ICT l www.samedanltd.com
for classic Phase I trials, the Belgian agency has a scientific
advise procedure in place when an applicant wants to address
issues that may arise beforehand.
BIOTECHNOLOGY-DERIVED PRODUCTS
For biotechnology products, the ICH S6 guideline provides
guidance to the preclinical requirements that addresses
issues like the species specificity of the interaction of the
product with its target, the need to conduct some studiessuch as genotoxicity studies, and particular aspects of
safety pharmacology testing (5). This guidance document is
currently in a revision process and the procedure for
scientific advice may be helpful to discuss unclear issues if
these may have major repercussions. Most studies with
biotechnology-derived products are conducted according to
a classic Phase I approach. This may be linked to the fact
that the ICH S6 guideline is the most important guidance
for such products and the amount of preclinical testing
needed may already be relatively limited, therefore the
exploratory approach does not always provide major
advantages. Furthermore, the fact that such products requirea complex production process and thus there is often no
choice to be made between different products may in part
explain that limited numbers of eCTAs were submitted in
the past with these products.
CANCER PATIENTS
The ICH S9 guideline gives indications about preclinical
requirements for the conduct of clinical trials in patients
with advanced cancers, and it is important to keep this
limitation in the scope of the guideline in mind (6). It has
implications for the early-phase studies in such patients. Ingeneral, it lessens the requirements in comparison to other
products. However, for such studies, a flexible dose-finding
design may be a major factor to consider. Whether seamless
flexible designs would be acceptable may depend on the
available preclinical data and stopping criteria and needed
monitoring that can be derived from it. The starting dose
should be estimated as one that will cause a pharmacologic
effect and is not likely to surpass the maximal tolerated
dose, it is clear that preclinical pharmacodynamic,
toxicological and pharmacokinetic data should be sufficient
to do so. Whereas the maximal dose will generally be
determined by the tolerability, it is obvious that preclinical
data may be helpful in predicting that dose, moreover it
could be argued that increasing the dose far above one that
is maximally active may not yield much additional
therapeutic effect. This may be addressed in the preclinical
setting to a certain extent. Thus, careful consideration of the
amount and type of preclinical data that will be available
About the authors
Walter Janssens is a Zoologist and has a
PhD from the University of Antwerp; he later
did research at the University of Leuven inthe Center for Thrombosis and Vascular
Research. He then became a research
scientist in the pharmaceutical industry
with an emphasis on cardiovascular and
gastrointestinal physiology and pharmacology and migraines.
From 2002 until May 2006 he worked on toxicological aspects
of the use of industrial chemicals in a regulatory context at the
Scientific Institute of Public Health in Brussels. In May 2006,
he became senior assessor of preclinical aspects in clinical
trial applications at the R&D department of the Federal
Agency for Medicinal and Health Products. He is also
coordinator for early-phase development at the Agency.
Email: [email protected]
Kristof Bonnarens graduated from the
University of Ghent in 2001, with a degree
in Industrial Pharmacy. After a short career
in the pharmaceutical industry, he joined
the R&D department within the Federal
Agency of Medicines and Health Products
in January 2005. He is the interim Head of
Division in R&D. He is a member of the EudraCT working
group, and is involved in several IT-projects concerning
clinical trials.
Greet Musch is an Industrial Pharmacist
and has a PhD in Pharmaceutical andBiomedical Sciences at the Free University
of Brussels. She worked in the
pharmaceutical industry for eight years,
where she was responsible for all chemical
and pharmaceutical analytical activities
related to the development of new innovative drugs. She then
moved to Federal Public Health services as a Senior Quality
Assessor where she assisted in several projects related to
CHMP, as well as to generics. Since August 2004 she has
been in charge of the R&D department within the Federal
Agency of Medicines and Health Products in Belgium, and has
been Director General of Pre-Authorisation at the Agency since
January 2009. She is a member of the EU Ad Hoc Group on
implementing guidelines for clinical trials as well as of the
Clinical Trial Facilitation Group.
Most studies with biotechnology-derived products are conducted
according to a classic Phase I approach.This may be linked to the fact
that the ICH S6 guideline is the most important guidance for such
products and the amount of preclinical testing needed may already
be relatively limited, therefore the exploratory approach does not
always provide major advantages.
8/3/2019 Belgium Phase 1 Requirements
http://slidepdf.com/reader/full/belgium-phase-1-requirements 6/6
should lead to the most eff icient and patient friendly way to
conduct the first clinical trials.
QUALITY AND GMP ASPECTS
The guideline CHMP/QWP/185401/2004 forms the basis
for evaluation of the quality of experimental medicines (7).
For biotechnology-derived products, the specif ic guidelines
depend on the nature of the product should be applied. Theactive substance used in exploratory trials may be
synthesised in a pilot lab, but it is imperative that an
adequate description of the product and the impurities that
it may contain should be provided. However, once the active
substance has been produced and characterised, there is no
reason why the GMP rules that are in effect for classic
Phase I studies should not be followed. This means that in
principle the Phase I unit should apply for an authorisation
for production of experimental medicinal products and that
an inspection should take place before this authorisation
can be granted. In Belgium, a hospital pharmacy is legally
allowed to perform reconstitution and packaging activitiesfor in hospital use. This means that if the Phase I unit where
early-phase clinical trials are performed is part of the
hospital, it can rely on its hospital pharmacy for such
activities – limited only for use in the same hospital. It
could be that limited and specif ic production activities may
be needed in a Phase I unit that, although located in a
hospital, are not a part of that hospital in legal terms.
Limited and explicitly defined production activities, only
for internal use, may be envisaged after inspection.
References
1. EMA/CPMP/ICH/286/95 Revision 2, Note for guidance
on non-clinical safety studies for the conduct of
human clinical trials and marketing authorization for
pharmaceuticals
2. EMA/CHMP/SWP/28367/07, Guideline on strategies toidentify and mitigate risks for first-in-human clinical
trials with investigational medicinal products
3. Freireich EJ, Gehan EA, Rall DP, Schmidt LH, and
Skipper HE, Quantitative Comparison of Toxicity of
Anticancer Agents in Mouse, Rat, Hamster, Dog,
Monkey, and Man, Cancer Chemotherapy Reports 50:
pp219-244, 1966
4. FDA Guidance for Industry. Estimating the Maximum
Safe Starting Dose in Initial Clinical Trials for
Therapeutics in Adult Healthy Volunteers
5. EMA/CHMP/ICH/302/95, Note for guidance on
preclinical safety evaluation of biotechnology-derivedpharmaceuticals
6. EMA/CHMP/ICH/646107/2008, Note for guidance on
nonclinical evaluation for anticancer pharmaceuticals
7. EMA/ CHMP/QWP/185401/2004, Guideline on the
requirements to the chemical and pharmaceutical
quality documentation concerning investigational
medicinal products in clinical trials
Managing Clinical Trials A unique, dedicated CRO/CMO
serving pharmaceutical, biotech
and medical device companies
G US
G
EUG Asia
G Pacific Rim
For details, visit our website at:
www.irclc.com
Mid Valley Professional Plaza
7651 S. 700 West, Suite 105Salt Lake City, UT 84047, US
Tel: +1 801 233 0075
Email: [email protected]





















![Phase 2 Requirements for Final Rule [Read-Only]](https://img.pdfslide.net/doc/110x75/61d277570213f44f880d50c2/phase-2-requirements-for-final-rule-read-only.jpg)







