Embed Size (px)
Citation preview

Benefits of Surgical Repair of Coarctation of theAorta in Patients Older Than 50 YearsMatthias Bauer, MD, Vladimir V. Alexi-Meskishvili, MD, PhD, Ulrike Bauer, MD,Diab Alfaouri, MD, Peter E. Lange, MD, PhD, and Roland Hetzer, MD, PhDDepartments of Cardiothoracic and Vascular Surgery, and Congenital Heart Diseases, Deutsches Herzzentrum Berlin, Berlin,Germany
Background. Most patients with unrepaired coarctationof the aorta die before the age of 50 years. In patients whopresent at an older age, the indications for surgicaltreatment are controversial because the benefits of oper-ating are unclear.
Methods. At follow-up investigation from 0.5 to 11.5years (mean, 4 years) after primary surgical correction ofcoarctation in 15 patients aged 50 to 63 years (mean, 54years), we analyzed the preoperative and postoperativecomplications, symptoms, need for antihypertensivedrugs, and blood pressure at rest and during exercise.
Results. Preoperatively no patient had normal bloodpressure at rest despite combined antihypertensive med-
ication. There was no significant mortality or morbidityafter repair. At follow-up examination only 3 patientshad at rest mild hypertension, the other 12 patients werenormotensive. Of the 11 tested patients, 8 displayedsystolic arterial hypertension during exercise.
Conclusions. Surgical correction of coarctation can beperformed after the age of 50 years with low surgical risk.Operation reduces systolic hypertension at rest and per-mits more effective medical treatment. Despite persis-tence of the hypertension during exercise, symptomaticimprovement occurs in most patients.
(Ann Thorac Surg 2001;72:2060–4)© 2001 by The Society of Thoracic Surgeons
Coarctation of the aorta has specific diagnostic andsurgical problems that are typical for the infant,
child, and adult. Because of the development of hyper-tensive heart and vascular disease, with severe localchanges, produced by the coarctation, most older pa-tients with uncorrected coarctation of the aorta die beforethe age of 50 years from complications such as congestiveheart failure, myocardial infarction, aortic rupture,stroke, or infective endocarditis. They also have a highersurgical risk than younger patients without such compli-cations [1, 2].
Although operation for coarctation of the aorta hasbeen successfully performed for 55 years [3], many ques-tions with regard to long-term survival, fate of arterialhypertension, and relief of symptoms remain unan-swered, especially in older patients. There are only a fewreports that deal with patients who were operated on atmore than 50 years of age [4–6].
In this report we analyzed the long-term results ofsurgical repair of coarctation of the aorta in 15 patientsolder than 50 years of age.
Patients and Methods
From April 1988 to August 2000, 15 patients aged 50 to 63years (mean, 54 years), underwent primary surgical re-pair of coarctation of the aorta in our institution. Diag-
nosis of the coarctation was established before 10 years ofage in 5 patients, between 11 and 30 years in 5 patients,between 31 and 50 years in 2 patients, and after 50 yearsof age in 3. Nine patients (60%) had associated cardiacdiseases. The clinical data of the patients are presented inTable 1. Before the operation coronary angiography wasperformed in all patients to confirm the diagnosis ofaortic coarctation.
The operation was delayed in 12 patients: 7 patientsinitially had refused the operation, and in 5 patientsconservative treatment only was recommended in otherfacilities. Surgical repair of the coarctation in 13 patientswas performed by the use of a 16-mm to 22-mm pros-thetic graft bypass from the left subclavian artery to thedescending aorta without aortic cross-clamping. In 2patients, because of the relatively small size of the leftsubclavian artery (� 60% of the diameter of the descend-ing aorta at the diaphragm), patch isthmoplasty wasperformed (aortic cross-clamp time was 10 and 12 min-utes). Neither cardiopulmonary bypass nor intraaorticshunts were used.
All 15 patients underwent follow-up examination inour institution 0.5 to 11.5 years (mean, 4 years) afteroperation. The recent follow-up data, which includedclinical examination, interview about symptoms, and theneed for antihypertensive medication, as well as bloodpressure measurement at rest and during bicycle exer-cise testing, were analyzed. The oldest patient at fol-low-up examination was 71 years old.
Systemic hypertension was defined when the right armblood pressure exceeded 140/90 mm Hg. A residualgradient was defined as a systolic blood pressure gradi-
Accepted for publication July 16, 2001.
Address reprint requests to Dr Matthias Bauer, Deutsches HerzzentrumBerlin, Augustenburger Platz 1, 13353 Berlin, Germany; e-mail: [email protected].
© 2001 by The Society of Thoracic Surgeons 0003-4975/01/$20.00Published by Elsevier Science Inc PII S0003-4975(01)03094-6
ent between the right arm and either leg of more than20 mm Hg at rest.
Results
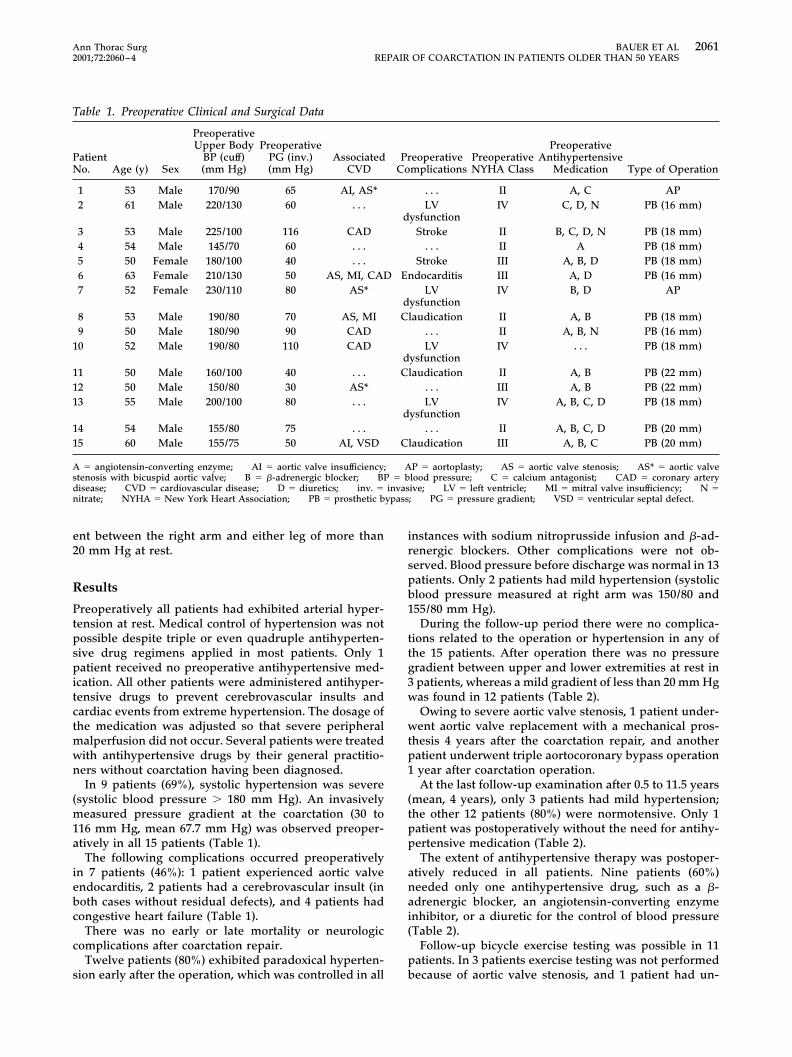
Preoperatively all patients had exhibited arterial hyper-tension at rest. Medical control of hypertension was notpossible despite triple or even quadruple antihyperten-sive drug regimens applied in most patients. Only 1patient received no preoperative antihypertensive med-ication. All other patients were administered antihyper-tensive drugs to prevent cerebrovascular insults andcardiac events from extreme hypertension. The dosage ofthe medication was adjusted so that severe peripheralmalperfusion did not occur. Several patients were treatedwith antihypertensive drugs by their general practitio-ners without coarctation having been diagnosed.
In 9 patients (69%), systolic hypertension was severe(systolic blood pressure � 180 mm Hg). An invasivelymeasured pressure gradient at the coarctation (30 to116 mm Hg, mean 67.7 mm Hg) was observed preoper-atively in all 15 patients (Table 1).
The following complications occurred preoperativelyin 7 patients (46%): 1 patient experienced aortic valveendocarditis, 2 patients had a cerebrovascular insult (inboth cases without residual defects), and 4 patients hadcongestive heart failure (Table 1).
There was no early or late mortality or neurologiccomplications after coarctation repair.
Twelve patients (80%) exhibited paradoxical hyperten-sion early after the operation, which was controlled in all
instances with sodium nitroprusside infusion and �-ad-renergic blockers. Other complications were not ob-served. Blood pressure before discharge was normal in 13patients. Only 2 patients had mild hypertension (systolicblood pressure measured at right arm was 150/80 and155/80 mm Hg).
During the follow-up period there were no complica-tions related to the operation or hypertension in any ofthe 15 patients. After operation there was no pressuregradient between upper and lower extremities at rest in3 patients, whereas a mild gradient of less than 20 mm Hgwas found in 12 patients (Table 2).
Owing to severe aortic valve stenosis, 1 patient under-went aortic valve replacement with a mechanical pros-thesis 4 years after the coarctation repair, and anotherpatient underwent triple aortocoronary bypass operation1 year after coarctation operation.
At the last follow-up examination after 0.5 to 11.5 years(mean, 4 years), only 3 patients had mild hypertension;the other 12 patients (80%) were normotensive. Only 1patient was postoperatively without the need for antihy-pertensive medication (Table 2).
The extent of antihypertensive therapy was postoper-atively reduced in all patients. Nine patients (60%)needed only one antihypertensive drug, such as a �-adrenergic blocker, an angiotensin-converting enzymeinhibitor, or a diuretic for the control of blood pressure(Table 2).
Follow-up bicycle exercise testing was possible in 11patients. In 3 patients exercise testing was not performedbecause of aortic valve stenosis, and 1 patient had un-
Table 1. Preoperative Clinical and Surgical Data
PatientNo. Age (y) Sex
PreoperativeUpper Body
BP (cuff)(mm Hg)
PreoperativePG (inv.)(mm Hg)
AssociatedCVD
PreoperativeComplications
PreoperativeNYHA Class
PreoperativeAntihypertensive
Medication Type of Operation
1 53 Male 170/90 65 AI, AS* . . . II A, C AP2 61 Male 220/130 60 . . . LV
dysfunctionIV C, D, N PB (16 mm)
3 53 Male 225/100 116 CAD Stroke II B, C, D, N PB (18 mm)4 54 Male 145/70 60 . . . . . . II A PB (18 mm)5 50 Female 180/100 40 . . . Stroke III A, B, D PB (18 mm)6 63 Female 210/130 50 AS, MI, CAD Endocarditis III A, D PB (16 mm)7 52 Female 230/110 80 AS* LV
dysfunctionIV B, D AP
8 53 Male 190/80 70 AS, MI Claudication II A, B PB (18 mm)9 50 Male 180/90 90 CAD . . . II A, B, N PB (16 mm)
10 52 Male 190/80 110 CAD LVdysfunction
IV . . . PB (18 mm)
11 50 Male 160/100 40 . . . Claudication II A, B PB (22 mm)12 50 Male 150/80 30 AS* . . . III A, B PB (22 mm)13 55 Male 200/100 80 . . . LV
dysfunctionIV A, B, C, D PB (18 mm)
14 54 Male 155/80 75 . . . . . . II A, B, C, D PB (20 mm)15 60 Male 155/75 50 AI, VSD Claudication III A, B, C PB (20 mm)
A � angiotensin-converting enzyme; AI � aortic valve insufficiency; AP � aortoplasty; AS � aortic valve stenosis; AS* � aortic valvestenosis with bicuspid aortic valve; B � �-adrenergic blocker; BP � blood pressure; C � calcium antagonist; CAD � coronary arterydisease; CVD � cardiovascular disease; D � diuretics; inv. � invasive; LV � left ventricle; MI � mitral valve insufficiency; N �nitrate; NYHA � New York Heart Association; PB � prosthetic bypass; PG � pressure gradient; VSD � ventricular septal defect.
2061Ann Thorac Surg BAUER ET AL2001;72:2060–4 REPAIR OF COARCTATION IN PATIENTS OLDER THAN 50 YEARS
dergone a leg amputation after an accident. Eight of the11 patients (72.7%) showed a pathologic blood pressureincrease at low exercise levels (50 W) or developed severearterial hypertension at higher exercise levels (systolicblood pressure � 195 mm Hg), which led to cessation ofthe exercise testing. In the other 2 patients the exercisetesting was stopped because of dyspnea (patient 10) andmuscle weakness (patient 11).
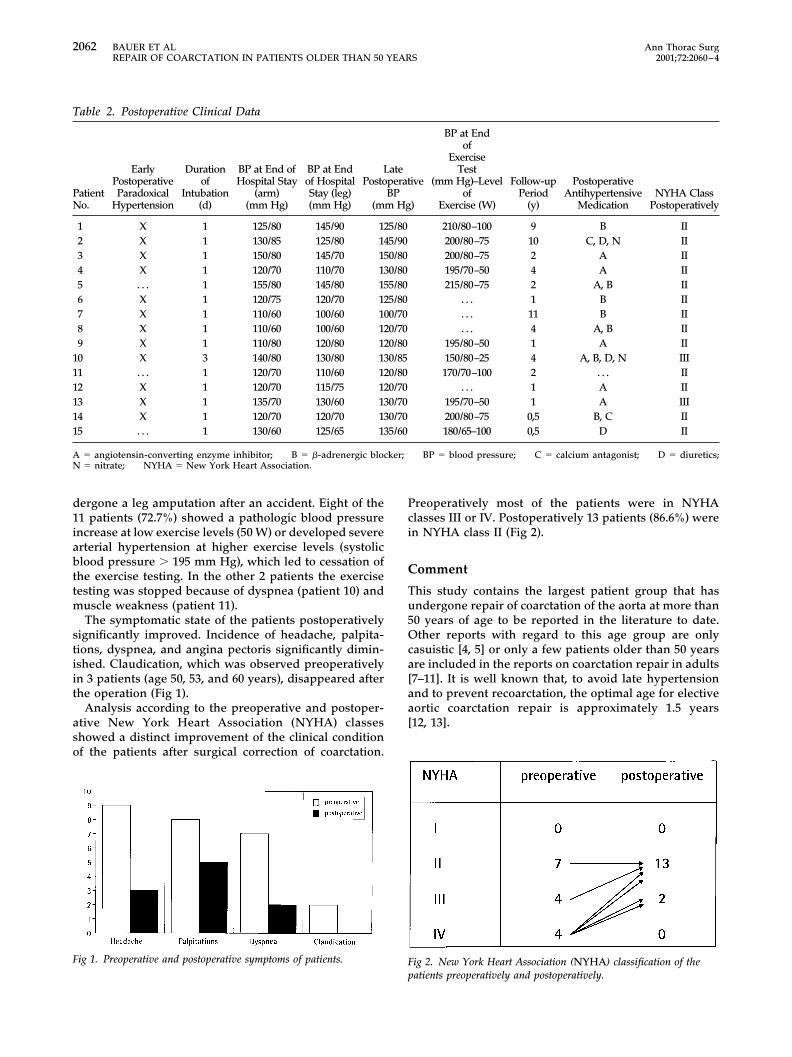
The symptomatic state of the patients postoperativelysignificantly improved. Incidence of headache, palpita-tions, dyspnea, and angina pectoris significantly dimin-ished. Claudication, which was observed preoperativelyin 3 patients (age 50, 53, and 60 years), disappeared afterthe operation (Fig 1).
Analysis according to the preoperative and postoper-ative New York Heart Association (NYHA) classesshowed a distinct improvement of the clinical conditionof the patients after surgical correction of coarctation.
Preoperatively most of the patients were in NYHAclasses III or IV. Postoperatively 13 patients (86.6%) werein NYHA class II (Fig 2).
Comment
This study contains the largest patient group that hasundergone repair of coarctation of the aorta at more than50 years of age to be reported in the literature to date.Other reports with regard to this age group are onlycasuistic [4, 5] or only a few patients older than 50 yearsare included in the reports on coarctation repair in adults[7–11]. It is well known that, to avoid late hypertensionand to prevent recoarctation, the optimal age for electiveaortic coarctation repair is approximately 1.5 years[12, 13].
Fig 1. Preoperative and postoperative symptoms of patients. Fig 2. New York Heart Association (NYHA) classification of thepatients preoperatively and postoperatively.
Table 2. Postoperative Clinical Data
PatientNo.
EarlyPostoperativeParadoxical
Hypertension
Durationof
Intubation(d)
BP at End ofHospital Stay
(arm)(mm Hg)
BP at Endof HospitalStay (leg)(mm Hg)
LatePostoperative
BP(mm Hg)
BP at Endof
ExerciseTest
(mm Hg)–Levelof
Exercise (W)
Follow-upPeriod
(y)
PostoperativeAntihypertensive
MedicationNYHA Class
Postoperatively
1 X 1 125/80 145/90 125/80 210/80–100 9 B II2 X 1 130/85 125/80 145/90 200/80–75 10 C, D, N II3 X 1 150/80 145/70 150/80 200/80–75 2 A II4 X 1 120/70 110/70 130/80 195/70–50 4 A II5 . . . 1 155/80 145/80 155/80 215/80–75 2 A, B II6 X 1 120/75 120/70 125/80 . . . 1 B II7 X 1 110/60 100/60 100/70 . . . 11 B II8 X 1 110/60 100/60 120/70 . . . 4 A, B II9 X 1 110/80 120/80 120/80 195/80–50 1 A II
10 X 3 140/80 130/80 130/85 150/80–25 4 A, B, D, N III11 . . . 1 120/70 110/60 120/80 170/70–100 2 . . . II12 X 1 120/70 115/75 120/70 . . . 1 A II13 X 1 135/70 130/60 130/70 195/70–50 1 A III14 X 1 120/70 120/70 130/70 200/80–75 0,5 B, C II15 . . . 1 130/60 125/65 135/60 180/65–100 0,5 D II
A � angiotensin-converting enzyme inhibitor; B � �-adrenergic blocker; BP � blood pressure; C � calcium antagonist; D � diuretics;N � nitrate; NYHA � New York Heart Association.
2062 BAUER ET AL Ann Thorac SurgREPAIR OF COARCTATION IN PATIENTS OLDER THAN 50 YEARS 2001;72:2060–4
In our patients the preoperative pressure gradientsvaried from 25 to 118 mm Hg, but the pressure gradientwas not decisive as an indication for operation. The goalof operation in this group of patients was to decrease theleft ventricular afterload and to increase the possibility ofmore effective medical treatment of hypertension afterrelief of coarctation. The surgical approach by means ofextraanatomic bypass techniques was first described byBlalock and Park in 1944 [14]. They performed an end-to-side anastomosis of the left subclavian artery with theaorta distal to the stenosis.
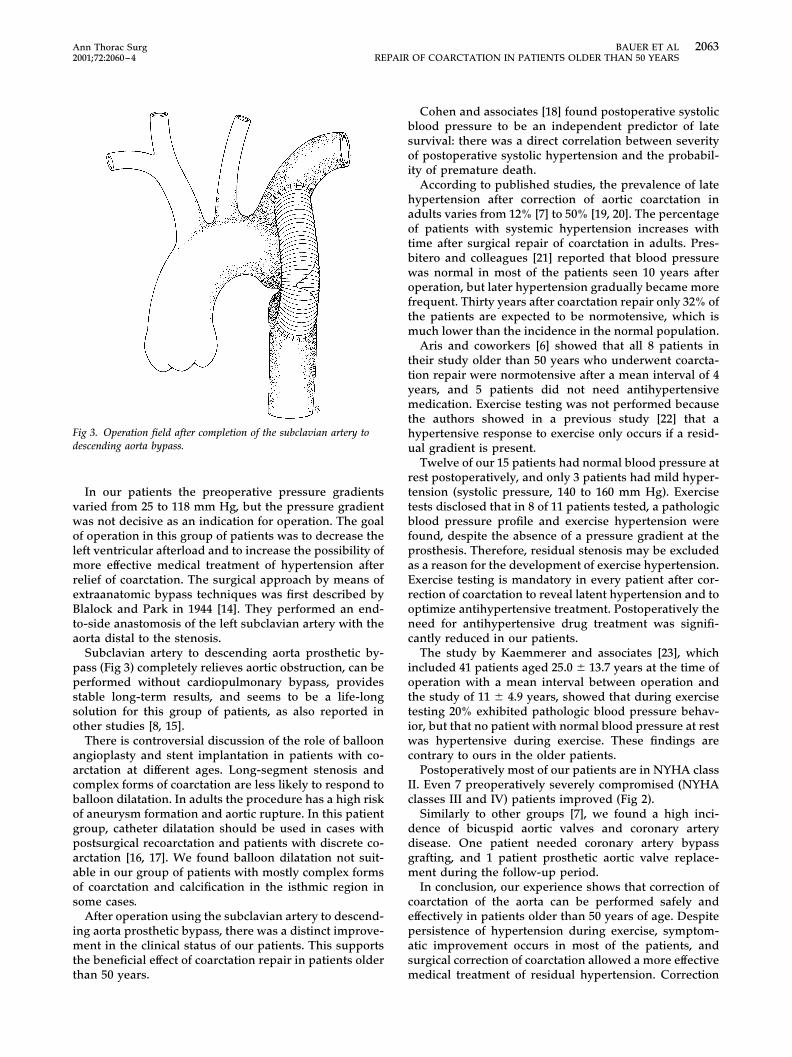
Subclavian artery to descending aorta prosthetic by-pass (Fig 3) completely relieves aortic obstruction, can beperformed without cardiopulmonary bypass, providesstable long-term results, and seems to be a life-longsolution for this group of patients, as also reported inother studies [8, 15].
There is controversial discussion of the role of balloonangioplasty and stent implantation in patients with co-arctation at different ages. Long-segment stenosis andcomplex forms of coarctation are less likely to respond toballoon dilatation. In adults the procedure has a high riskof aneurysm formation and aortic rupture. In this patientgroup, catheter dilatation should be used in cases withpostsurgical recoarctation and patients with discrete co-arctation [16, 17]. We found balloon dilatation not suit-able in our group of patients with mostly complex formsof coarctation and calcification in the isthmic region insome cases.
After operation using the subclavian artery to descend-ing aorta prosthetic bypass, there was a distinct improve-ment in the clinical status of our patients. This supportsthe beneficial effect of coarctation repair in patients olderthan 50 years.
Cohen and associates [18] found postoperative systolicblood pressure to be an independent predictor of latesurvival: there was a direct correlation between severityof postoperative systolic hypertension and the probabil-ity of premature death.
According to published studies, the prevalence of latehypertension after correction of aortic coarctation inadults varies from 12% [7] to 50% [19, 20]. The percentageof patients with systemic hypertension increases withtime after surgical repair of coarctation in adults. Pres-bitero and colleagues [21] reported that blood pressurewas normal in most of the patients seen 10 years afteroperation, but later hypertension gradually became morefrequent. Thirty years after coarctation repair only 32% ofthe patients are expected to be normotensive, which ismuch lower than the incidence in the normal population.
Aris and coworkers [6] showed that all 8 patients intheir study older than 50 years who underwent coarcta-tion repair were normotensive after a mean interval of 4years, and 5 patients did not need antihypertensivemedication. Exercise testing was not performed becausethe authors showed in a previous study [22] that ahypertensive response to exercise only occurs if a resid-ual gradient is present.
Twelve of our 15 patients had normal blood pressure atrest postoperatively, and only 3 patients had mild hyper-tension (systolic pressure, 140 to 160 mm Hg). Exercisetests disclosed that in 8 of 11 patients tested, a pathologicblood pressure profile and exercise hypertension werefound, despite the absence of a pressure gradient at theprosthesis. Therefore, residual stenosis may be excludedas a reason for the development of exercise hypertension.Exercise testing is mandatory in every patient after cor-rection of coarctation to reveal latent hypertension and tooptimize antihypertensive treatment. Postoperatively theneed for antihypertensive drug treatment was signifi-cantly reduced in our patients.
The study by Kaemmerer and associates [23], whichincluded 41 patients aged 25.0 � 13.7 years at the time ofoperation with a mean interval between operation andthe study of 11 � 4.9 years, showed that during exercisetesting 20% exhibited pathologic blood pressure behav-ior, but that no patient with normal blood pressure at restwas hypertensive during exercise. These findings arecontrary to ours in the older patients.
Postoperatively most of our patients are in NYHA classII. Even 7 preoperatively severely compromised (NYHAclasses III and IV) patients improved (Fig 2).
Similarly to other groups [7], we found a high inci-dence of bicuspid aortic valves and coronary arterydisease. One patient needed coronary artery bypassgrafting, and 1 patient prosthetic aortic valve replace-ment during the follow-up period.
In conclusion, our experience shows that correction ofcoarctation of the aorta can be performed safely andeffectively in patients older than 50 years of age. Despitepersistence of hypertension during exercise, symptom-atic improvement occurs in most of the patients, andsurgical correction of coarctation allowed a more effectivemedical treatment of residual hypertension. Correction
Fig 3. Operation field after completion of the subclavian artery todescending aorta bypass.
2063Ann Thorac Surg BAUER ET AL2001;72:2060–4 REPAIR OF COARCTATION IN PATIENTS OLDER THAN 50 YEARS

of coarctation may therefore be performed in the olderpatient to prevent the complications of chronic arterialhypertension in the further course of the patient’s life.
The authors thank Anne M. Gale for editorial assistance, JuliaStein for statistical advice, and Reinhold Giering-Jaensch forproviding the illustration.
References
1. Ostermiller WE, Somerndike JM, Hunter J, et al. Coarctationof the aorta in adult patients. J Thorac Cardiocasv Surg1969;61:125–30.
2. Campbell M. Natural history of coarctation of the aorta. BrHeart J 1970;32:633–40.
3. Crafoord C, Nylin G. Congenital coarctation of the aorta andits surgical treatment. J Thorac Surg 1945;14:347–61.
4. Patel Y, Jilani MI, Cho K. Coarctation of the aorta presentingin a 79-year-old male. Thorac Cardiovasc Surg 1998;46:158–60.
5. Cayenne S, Sahgal P, Mistra VK, Conrad A, Jonas E. Asymp-tomatic patient with coarctation of the aorta presenting latein life: an unusual case and review. Cardiovasc Rev Rep1996;17:48–53.
6. Aris A, Subirana T, Ferries P, Torner-Sole M. Repair of aorticcoarctation in patients more than 50 years of age. AnnThorac Surg 1999;67:1376–9.
7. Fraser RS, Stobey J, Rossall RE, Dvorkin J, Taylor RF.Coarctation of the aorta in adults. Can Med Assoc J 1976;115:415–7.
8. Wells WJ, Prendergast TW, Berdjis F, et al. Repair of coarc-tation of the aorta in adults: the fate of systolic hypertension.Ann Thorac Surg 1996;61:1168–71.
9. Lawrie GM, DeBakey ME, Morris GC, Crawford ES, WagnerWF, Glaeser DH. Late repair of coarctation of the descendingthoracic aorta in 190 patients. Arch Surg 1981;116:1557–60.
10. Clarkson PM, Nicholson MR, Barratt-Boyes BG, Neutze JM,Whitlock RM. Results after repair of coarctation f the aortabeyond infancy: a 10 to 28 year follow-up with particularreference to late systemic hypertension. Am J Cardiol 1983;51:1481–8.
11. Vigano M, Ressia L, Gaeta R. Long-term follow-up afterrepair of coarctation of the aorta in adults. Ann Thorac Surg1997;63:1827–8.
12. Brouwer RM, Erasmus ME, Ebels T, Eijgelaar A. Influence ofage on survival, late hypertension, and recoarctation inelective aortic coarctation repair. Including long-term resultsafter elective aortic coarctation repair with a follow-up from25 to 44 years. J Thorac Cardiovasc Surg 1994;108:525–31.
13. Seirafi PA, Warner KG, Geggel RL, Payne DD, Cleveland RJ.Repair of coarctation of the aorta during infancy minimizesthe risk of late hypertension. Ann Thorac Surg 1998;66:1378–82.
14. Blalock A, Park EA. Surgical treatment of experimentalcoarctation (atresia) of the aorta. Ann Surg 1944;119:445–56.
15. Grinda JM, Mace L, Dervanian P, Folliquet TA, Neveux JY.Bypass graft for complex forms of isthmic aortic coarctationin adults. Ann Thorac Surg 1995;60:1299–302.
16. Gibbs JL. Treatment options for coarctation of the aorta.Heart 2000;84:11–3.
17. Fawzy ME, Sivanandam V, Galal O, et al. One- to ten-yearfollow-up results of balloon angioplasty of native coarctationof the aorta in adolescents, and adults. J Am Coll Cardiol1997;30:1542–6.
18. Cohen M, Fuster V, Steele PM, Driscoll D, McGoon DC.Coarctation of the aorta. Long-term follow-up and predic-tion of outcome after surgical correction. Circulation 1989;80:840–5.
19. Westaby S, Parnell B, Pridie RB. Coarctation of the aorta inadults. Cinical presentation and results of surgery. J Cardio-vasc Surg 1987;28:124–7.
20. Maron BJ, O’Neal-Humphries J, Rowe RD, Melerts ED.Prognosis of surgically corrected coarctation of the aorta: a20-year postoperative appraisal. Circulation 1973;47:119–26.
21. Presbitero P, Demarie D, Villani M, et al. Long term results(15–30 years) of surgical repair of aortic coarctation. BrHeart J 1987;57:462–7.
22. Subirana MT, Borras X, Roca J, Serra JR, Torner-Soler M.Evolution de la hipertension arterial en pacientes operadosde coarctation de aorta en edad adulta. Rev Esp Cardiol1987;40(Suppl 1):9.
23. Kaemmerer H, Oelert F, Bahlmann J, Blucher S, Meyer GP,Mugge A. Arterial hypertension in adults after surgicaltreatment of aortic coarctation. Thorac Cardiovasc Surg1998;46:121–5.
2064 BAUER ET AL Ann Thorac SurgREPAIR OF COARCTATION IN PATIENTS OLDER THAN 50 YEARS 2001;72:2060–4