Embed Size (px)
Citation preview

Benha University
Faculty of nursing
Fourth year final exam- first semester
Course title: psychiatric and mental health nursing
Date: 10/1/2013
Time allowed: 3 hours
Parts Questions Marks
Part( 1) Multiple-choice questions 7.5
Part(2) True and false 7.5
Part(3) Matching 10
Part(4) Short answer 10
Part(5) Fill in the blanks 20
Part(6) Essay 25
total 80
1
Part (1): Multiple-choice the following circle the best
answer:
1-Criteria for hypomanic episode includes all except….
A. Inflated self esteem or grandiosity
B. Decreased need for sleep
C. More talkative than usual or pressure to keep talking
D. Cause functional impairment, necessitate hospitalization,
or there are psychotic features
2-As per DSM-IV-TR classification, disorders with odd and eccentric
behaviours are classified under
A. Cluster A
B. Cluster B
C. Cluster C
D. Cluster D
3-When coping with a patient's inappropriate expression of anger, the
first step is to recognize:
A. Appropriate limit-setting techniques
B. Defense mechanisms that the patient is using
C. One's own response to anger in others
D. Systems theory approaches for effective change
4-The severe feeling of restlessness produced by some psychotropic
medications, which is often misinterpreted by patients as anxiety or a
recurrence of psychiatric symptoms, is known as:
A. akathisia
B. akinesia
C. bradykinesia
D. dystonia

2
5- Psychopathological consequence of crisis:
A. Anxiety disorder only.
B. Substance- Related disorders only.
C. Anxiety and substance related disorders.
D. None of the above.
6- Therapeutic community is promoted by:
A. Basic physiological needs are fulfilled.
B. The physical facilities are conductive to achievement of the
goals of therapy.
C. Community and family are included in the program of therapy
in an effort to facilitate discharge from the hospital.
D. All of the above.
7- A female client is admitted for surgery. Although not physically
distressed, the client appears apprehensive and alienated. A nursing
action that may help the client to feel more at ease includes:
A. Telling her that everything is all right
B. Giving her a copy of hospital regulations
C. Orienting her to the environment and unit personnel
D. Reassuring her that staff will be available if she becomes upset
8-The nurse is discussing the orientation phase. The student nurse
asks what the primary goal between the nurse and the client is
during this phase. The nurse should respond that primary goal is to:
A. Explain unit rules
B. Establish a relationship
C. Establish trust and support
D. Formulate a mutual plan of action
3
9-Therapeutic treatment of a client with ritualistic behavior should
be directed toward helping her to:
A. Redirect her energy into activities to help others
B. Learn that her behavior is not serving a realistic purpose
C. Forget her fears by administering anti anxiety medications
D. Understand her behavior is caused by unconscious impulses that
the fears
10-The following are clinical features of mania, except
A. Elation of mood
B. Disorientation
C. Pressure of speech
D. Grandiose delusions
11-The history of a patient reveals gradually occurring global
impairments of cognitive functioning, memory, and personality.
Which disorder would the nurse most likely suspect as the patient's
problem.
A. Depression.
B. Alzheimer's-type of dementia.
C. Vascular dementia.
D. Tardive dyskinesia.
12-Phenytoin may have adverse effects on the hematopoietic system.
All of the following have been reported EXCEPT:
A. macrocytic anemia.
B. hepatosplenomegaly.
C. folic acid deficiency
D. leukemia

4
13-In occupational therapy, the things you do each day are referred
to as:
A. Daily Routine.
B. Daily living Tasks.
C. Occupational activities.
D. Activities of Daily Living.
14-Combining MAOIs with SSRIs may cause:
A. Serotonin syndrome.
B. Extrapyramidal symptoms (EPS).
C. Neroleptic Malignant Syndrome (NMS).
D. Agranulocytosis
15-situation: F. age 18; returns home from school to discover that her
mother has been in a serious automobile accident. F. initially
responds to the news by yelling, "No I don't believe it. It can't be
true." F. is using which defense mechanism?
A. Introjections.
B. Suppression.
C. Denial.
D. Repression

5
Part (2): True and false
II -Read each statement carefully and circle (T) if the statement is true and
(F) if statement false
Items T F
1-In therapeutic environment restrictions and punishment are to be
encouraged.
T F
2-The crisis state is necessarily due to mental illness. T F
3- Waxy flexibility is typical of catatonic Schizophrenia. T F
4-Purging refers to a number of methods that a person may use to
remove food from his/her body in unhealthy ways.
T F
5- The highest priority post E.C.T is monitoring the respiratory status. T F
6- The nurse interprets a patient's fear of being in situations or places that
may be difficult or embarrassing to leave as evidence of social phobia.
T F
7-Agranulocytosis manifested by increase white blood cells. T F
8-Selecting topics of interest to the patient may block communication. T F
9-Sitting silence or quietly with depressed patient saying nothing convey
acceptance to him.
T F
10-Gingival hyperplasia is a common side effect of phenytoin T F
11-Sublimation is the defense by which the stress appears in a more
acceptable manner.
T F
12-Therapeutic communication is a major tool in psychiatric nursing in a
therapeutic nurse-client relationship
T F
13-According to Dan Siegel after puberty it becomes impossible to learn
new skills.
T F
14-Biploar disorder and depression are the same thing. T F
15- Parkinsoian like tremors happen a result of intake of large dose of
major tranquilizer.
T F
6
Part (3): Matching
In the space provided in front of each statement in column (A) place the
corresponding number from column (B).
B A
A-Focuses on specific problems, such as poor self
concept, depression, extreme dependency and poor
medication
1- Conversion
E
B-The continuous repetition of the same word or
theme in response to different questions
2- Derealization
C
C-Feeling that one's environment is strange unreal
or unfamiliar
3- Echolalia
B
D-This drugs may cause tardive dyskineaia if taken
chronically
4- Insight
H
E-Is a mechanism by which emotional conflicts are
channeled into physical symptom or physical
illness
5- Individual psychotherapy
A
F-Absence of both emotional experience and
expression, the patient shows an emotional tone
associated with indifference
6- Neuroleptics
D
G-Signal anxiety as a result of conflict between id,
ego, and super ego
7- Primary prevention
J
H-Patient's awareness of his condition and the need
of treatment
8- Apathy
F
I-Exaggerated and invariably pathological fear of
some specific type of stimulus or situation
9- Phobia
I
J-Attempting to discover and eliminate the causes
of mental illness
10- Sigmund Freud
G

7
Part (4): Short answer
1- Explain cognitive disorder and mention types
Definitions:
Cognition:
Is the brains ability to process, retain and use information.
Cognitive abilities including reasoning, judgment, perception, attention,
comprehension, and memory. These cognitive abilities are essential for
many important tasks including making decision, solving problems,
interpreting the environment, and learning new information.
Cognitive disorders:
Is a disruption or impairment in these higher-level functions of the brain.
Or:
Refer to temporary or permanent neuron damage that result in
psychological or behavior dysfunction.
Cognitive disorder includes:
1- Delirium
2- Dementia
Delirium (acute confessional state)
Definition of delirium:
Is a disturbance in consciousness and change in cognition that develops
over short time? It is usually reversible if the underlying cause is
identified and treated quickly, however, if left untreated, delirium may
progress to dementia or to irreversible coma and death.
Definition:
Is a mental disorder marked by progressive deterioration in intellectual
functioning, memory and ability to solve problems and learn new skills
without impairment in consciousness.
2- Communication and its elements
1. Definition of communication :-
Is a continuous circular process by which information, such as ideas
and feelings is transmitted between people and their environment, it
involves symbols such as written words and spoken language,
Communication is an essential tool of psychiatric nursing, the
ultimate goal of communication is to understand and be understood
Elements of communication:-

8
1- The sender: (encoder) is the person who initiates that transmission
of message is both verbal and non verbal.
2-The receiver: (decoder) is the person who receives the message.
3-The message: Is the information that is transmitted and received it
is the verbal and non verbal expression of a rides, feelings and
experiences.
4-Feed back: It gives information to the sender about how they are
being perceived by others.
3-Explain defense mechanism and give one example
These are sometimes termed "Mental Mechanisms"
Adjustment Mechanisms" or "Ego Defense".
These are automatic and usually unconscious processes or act by the
individuals to: • Reduce or cope anxiety or fear
• Resolve emotional or mental conflict
• Protect one's self-esteem
• Protect one's sense of security
• Becomes pathologic when overused
In fact, due to the occurrence of stress, in trying to avoid painful
experience of anxiety, defenses arise and become characteristics of one's
own personality.
When rationally used, these defenses help to reduce tension and alleviate
anxiety. But when they fail to do so, they may turn pathological.
It s believed that by the tenth year of life, mental mechanisms are well
established. They may be used consciously or unconsciously and usually
used in combination with one another.
COMPENSATION
An attempt to overcome a real or imagined short coming, inferiority,
inabilities and weaknesses.
E.g. A blind woman becomes proficient in playing piano.
CONVERSION

9
Emotional problems are converted to physical symptoms.
E.g. A student unprepared for a report suffered headache the day she is
supposed to deliver her report.
DENIAL
Failure to acknowledge an intolerable thought, feeling, experience or
reality
E.g. A middle-aged man after being admitted to the CCU because of an
AMI, insists that he is in the
Hospital for just a diagnostic work-up.
DISPLACEMENT
To transfer an impulse or idea from a threatening object to a less
threatening object
E.g. An adolescent boy, after an argument with his father, goes to the
room and kicked his room’s door.
DISSOCIATION
The unconscious separation of painful feelings and emotions from an
unacceptable idea, situation, or object.
A pretty nurse tells how important to review months before the board
exam .But failed to remember her past board failures. E.g. Rape, trauma
FANTASY
Conscious distortion of unconscious feelings or wishes
A boy who is being bullied by his friends wished he had the power of
Wolverine.
IDENTIFICATION
A conscious or unconscious attempt to model oneself after a respected
person.
“I want to be just like you… a very good reviewer …… nurse
INTROJECTION

10
Unconsciously incorporating wishes, values, attitudes of others as if they
were your own.
While her mother is gone, a young girl disciplines her brother just like
her mother would.
If a nurse fails to get sufficient satisfaction in her job, instead of blaming
her supervisors she may feel is inadequate
PROJECTION
Blaming someone else for one’s difficulties or placing one’s unethical
desires on someone else.
E.g. A student who failed a subject blames his failure on poor teaching.
REACTION FORMATION
A conscious behavior that is the exact opposite of an unconscious feeling.
E.g. an older brother who dislikes his younger brother sends him gifts for
every holiday.
RATIONALIZATION
An individual finds a justifiable cause and acceptable reasons just to be
saved from an embarrassing and anxiety producing thoughts or
situations.
E.g. A basketball player claims that he missed the shot and lost the game
because of the distractions made by the audience.
REGRESSION
Return to earlier and more comfortable developmental level.
E.g. an examinee went directly to her room and sleeps in fetal position
and thumb sucks after knowing she failed the board exam.
REPRESSION
Unconscious and involuntary forgetting of painful ideas, events and
conflicts.
E.g. A nursing student who failed the recent board exam, can’t remember
any of the questions asked
11
SUPPRESSION
Voluntary exclusion from awareness, anxiety-producing feelings, ideas
and situations.
E.g. A nursing student states, “I cannot talk about my recent board,
please change the topic.”
SUBSTITUTION
Replacing the desired unattainable goal with one that is attainable.
E.g. A woman who failed the nursing board exam 3 times, worked as a
nursing aide just to be in the hospital.
SUBLIMATION
Channeling instinctual drives into acceptable activities.
A former hit man, talks about the importance of life, democracy, justice,
and following laws of the land.”
SYMBOLIZATION
Less threatening object is used to represent another.
E.g. A woman, missing her husband finds comfort in hugging her son who
looks like his father.
UNDOING
An attempt to erase an act, thought, feeling, guilt or desire
E.g. A man gives her wife a bunch of roses after their argument last night
4-Bipolar disorder and types
Definition: Bipolar disorder, also known as manic-depressive illness, is a brain
disorder of mood regulation that causes unusual shifts in mood,
energy, activity levels, and the ability to carry out day-to-day
tasks………………………………………………………………………………
Types":
12
According to the DSM, there are four basic types of bipolar disorder:
o Bipolar I Disorder
o Bipolar II Disorder
o Cyclothymia
o Bipolar Disorder Not Otherwise Specified (N.O.S).
1-Bipolar I Disorder is mainly defined by manic or mixed episodes that last at least seven
days, or by manic symptoms that are so severe that the person needs
immediate hospital care. Usually, the person also has depressive
episodes, typically lasting at least two weeks. The symptoms of mania or
depression must be a major change from the person’s normal behavior.
2-Bipolar II Disorder The diagnosis of this bipolar disorder requires:
-Presence or history of one or more major depressive episode.
-Presence or history of at least one hypomanic episode.
-There has never been a manic episode or a mixed episode
3-Bipolar Disorder Not Otherwise Specified (BP-NOS)
It is diagnosed when a person has symptoms of the illness that do not
meet diagnostic criteria for either bipolar I or II. The symptoms may not
last long enough, or the person may have too few symptoms, to be
diagnosed with bipolar I or II. However, the symptoms are clearly out of
the person’s normal range of behavior.
4-Cyclothymic Disorder, or Cyclothymia •Is a mild form of bipolar disorder.
•Diagnosis requires a 2 year history of numerous of hypomanic and mild
depressive symptoms that do not meet criteria for a major depressive
episode and the patient has not been without symptoms for more than 2
months.
•No major depressive disorder, manic or mixed episode has been present
during the first 2 years of the disturbance.

13
Some people may be diagnosed with rapid-cycling bipolar disorder.
This is when a person has four or more episodes of major depression,
mania, hypomania, or mixed symptoms within a year. Some people
experience more than one episode in a week, or even within one day.
Rapid cycling seems to be more common in people who have severe
bipolar disorder and may be more common in people who have their first
episode at a younger age.
Part (5): Fill the blanks
1-Positive concepts of mental health include
1-Positive attitude toward self (high self esteem): The person has a
realistic awareness of his /her abilities and limitation and also has
objective view of self.
2-Progress toward growth, development and self actualization: It is
ability of the individual to plan for the future, to use his capabilities,
outside interests and relationship.
3-Autonomus behavior: It refers to the individual’s ability to perform in
an independent self directed manner and to make his own decision
without external influence.
4-Tolerance of life’s uncertainties: Facing the challenges of day to day
living with hope and positive outlook
5-Mastery of the environment: The person can deal with and influence
the environment in capable, competent, and creative manner.
6-Perception of Reality: Distinguishing fact or real world from dream or
fantasy (positive indicator of mental health)
7-Stress Management: Experiencing congruent emotions in daily life.
Tolerating stress provoking situations in an adaptive, creative, and
flexible way
9-Resilience or integrative capacity: Is the ability to adjust (cope with) to
difficult and painful situations and events
14
2-Mention three approaches of crisis intervention
Three approaches of crisis intervention:
- Affective.
- Cognitive.
- Environmental modification
3-The aims of community mental heath services are
- The aims community mental health services are:
o Promotion of mental health
o Prevention of mental illness
o Care, treatment and rehabilitation of mentally ill patient.
4-Manifestations of stupor
1-paients doesn't respond to any stimuli. Neither external questions or painful
stimuli, nor internal 'hunger, thirst or distended bladder).
2- Dripping of saliva, retention of urine and feces
3-negativism, automatic obedience, catalepsy and waxy flexibility
4-mutism
5-patient is inactive or retention
6- Sleep disturbance as insomnia
7-visual hallucination
5-Nursing role in seclusion
1-secluding an individual is done quickly and efficiently with a concern for the
client's dignity and value as a person
2- The room is prepared in individual and the purpose of seclusion explained
3- Potentially dangerous clothing or possessions are removed\
4- The patient must be assessed at regular intervals usually every 15 mintes and
their behavior documented
5- Documentation to drink water and void or defecate
6- Medications is often administrated and the client in formed that it is help him
feel better
Part (6): Essay
Explain the etiology of child psychiatry (5 grades)
1. General causes:
15
a. Genetic factors: Disorder can be related to mental
impairment or mental retardation, as well as schizophrenia,
autism, bipolar disorder, obsessive-compulsive disorder.
b. Birth trauma: Decreased oxygen supply during birth affects
infant's central nervous system (CNS) and is related to
developmental deficits.
c. Maternal factors (including drug and alcohol abuse) are
related to developmental deficits (i.e., fetal alcohol
syndrome, cocaine- addicted neonates).
2. Family Systems theory: Severe emotional problems in
children and teens are thought to involve family system
elements.
a. Overanxious or rigid parenting.
b. Conflict relationship.
c. Double-bind or inconsistent combination patterns
d. Blurring of ego boundaries, poor differentiation of
individual identity.
3.Behavioral theory: Maladaptive behavior is learned from
reinforcement of maladaptive responses; appropriate behaviors are not
reinforced.
4.Socio-cultural theory: Environmental factors
adversely affect
Normal growth and development
a. Poverty associated with premature birth, with birth weights
from inadequate prenatal care and prenatal nutrition
b. Family violence and abuse
c. Inadequate guidelines for children, healthcare, and
parental supervision
d. Lack of school success (both academic and peer
related), which can negatively affect ego development

16
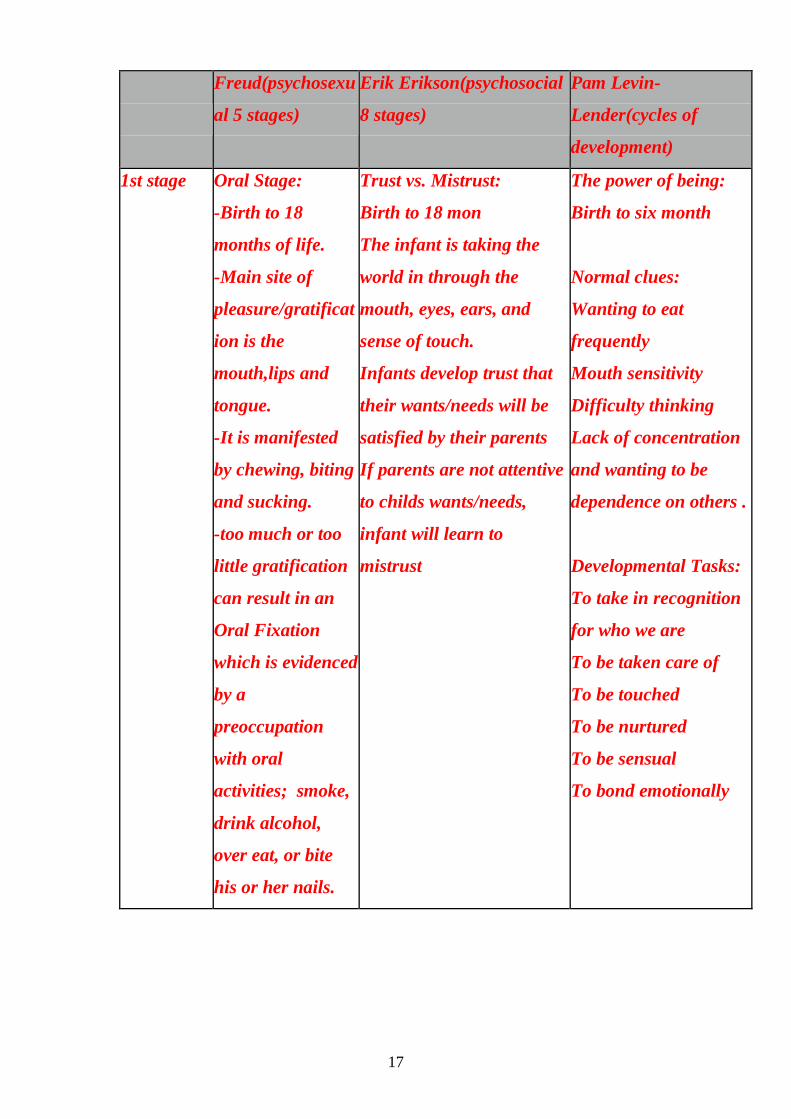
List common theories that explain personality development through
stages, and describe briefly one of them (10 grades)
common theories are:
-psychosexual theory ( Freud),
-the psychosocial stages (Erik Erikson) and
-the cycle of development (Pam Levin-Landher) :
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
Personality
developmen
t
-According to
Freud’ nearly all
children pass
through five
psychosexual
stages. -These
stages involve
seeking pleasure
from specific parts
of the body
Erikson states that each
person experiences eight
'psychosocial crises'
(internal conflicts linked to
life's key stages) which
help to define his or her
growth and personality.
Growth is a cycle of
development composed
of seven stages which
begin in childhood and
repeat throughout life
17
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
1st stage Oral Stage:
-Birth to 18
months of life.
-Main site of
pleasure/gratificat
ion is the
mouth,lips and
tongue.
-It is manifested
by chewing, biting
and sucking.
-too much or too
little gratification
can result in an
Oral Fixation
which is evidenced
by a
preoccupation
with oral
activities; smoke,
drink alcohol,
over eat, or bite
his or her nails.
Trust vs. Mistrust:
Birth to 18 mon
The infant is taking the
world in through the
mouth, eyes, ears, and
sense of touch.
Infants develop trust that
their wants/needs will be
satisfied by their parents
If parents are not attentive
to childs wants/needs,
infant will learn to
mistrust
The power of being:
Birth to six month
Normal clues:
Wanting to eat
frequently
Mouth sensitivity
Difficulty thinking
Lack of concentration
and wanting to be
dependence on others .
Developmental Tasks:
To take in recognition
for who we are
To be taken care of
To be touched
To be nurtured
To be sensual
To bond emotionally

18
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
2nd stage The Anal Stage
18mon – 3 years .
Main site of
pleasure/gratificat
ion is the anus .
-Child is
struggling to
control
bowel/bladder
function (toilet
training)
-If toilet training
is difficult, child
may become
anally fixated and
may not pass
beyond Anal Stage
In adults, this may
manifest itself as
Obsessive
Compulsive
Personality
Disorder
-Successful
resolution leads to
development of a
capacity for
independence and
personal initiative
Autonomy vs. Shame and
Doubt:
Age 18 Mon-3years.
Child no longer wants to
be told what to do by
parents, tries to assert
his/her autonomy
Child will learn to become
autonomous if parents
allow them a sense of
control over their life
If children are criticized,
overly controlled, or not
given the opportunity to
assert themselves, they
begin to feel inadequate in
their ability to survive, and
may then become overly
dependent upon others,
lack self- esteem, and feel
a sense of shame or doubt
in their own abilities.
The power of Doing:
6 to 18 months
Normal Clues:
Wanting a variety of
stimulation
Wanting to see, hear,
taste, touch, smell new
things and to expand
and explore the world
Developmental Tasks:
Wanting to explore the
environment without
having to think about it
and to develop a
sensory awareness by
doing.

19
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
3rd stage The Phallic Stage:
- 3- 6 year.
-Main site of
pleasure/gratificat
ion is the genitals
-This focusing
lays the
foundation of
gender identity.
-Freud described
the Oedipal and
Electra complex
during this stage.
-A fixation at this
stage could result
in sexual
deviancies (both
overindulging and
avoidance) and
weak or confused
sexual identity
according to
psychoanalysts.
Initiative vs. Guilt
Age 3-6
Child initiates motor and
intellectual activity.
If given this opportunity,
children develop a sense of
initiative, and feel secure
in their ability to lead
others and make decisions.
-Conversely, if criticized or
controlled, children
develop a sense of guilt
and will therefore remain
followers, lacking in self-
initiative.
The Power of
Thinking:
18 Months to 3 years
Normal clues:
Wanting to be different
from others.
Developing a separate
position
Rebelling, saying “No,
I won’t”
Developmental Tasks:
Testing reality.
Pushing against others
Establishing
independence
Expressing negativity
and learning to think.
20
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
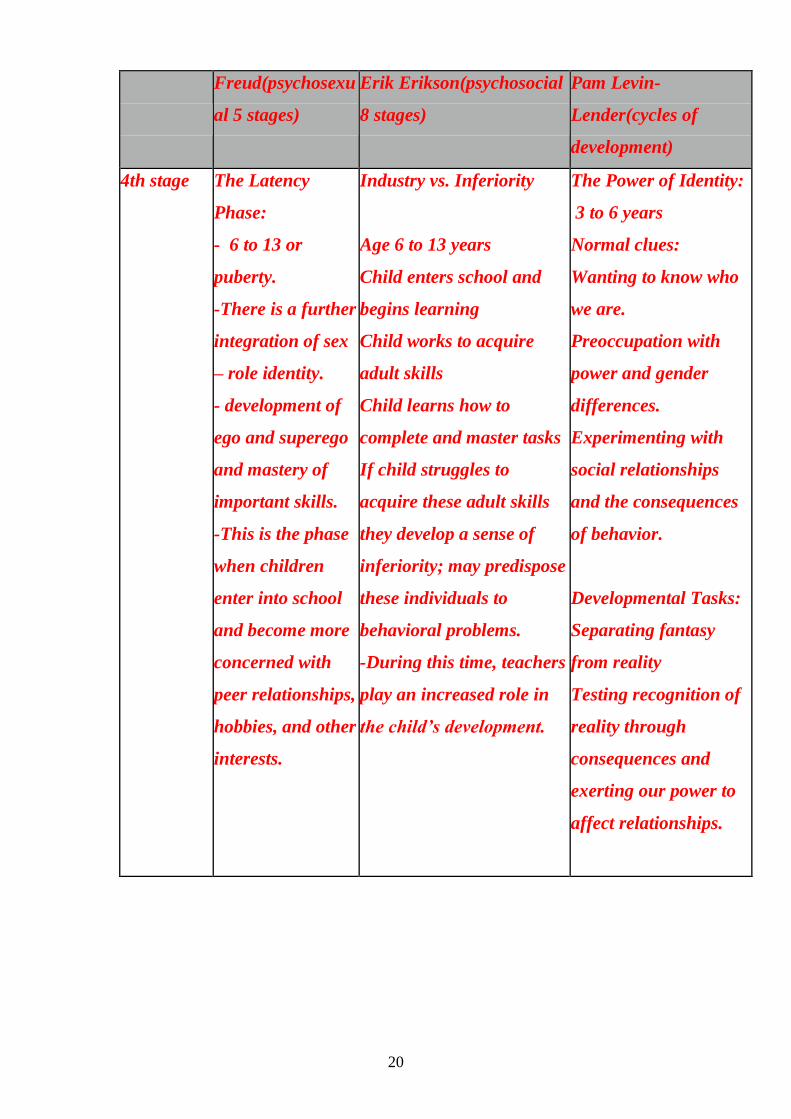
4th stage The Latency
Phase:
- 6 to 13 or
puberty.
-There is a further
integration of sex
– role identity.
- development of
ego and superego
and mastery of
important skills.
-This is the phase
when children
enter into school
and become more
concerned with
peer relationships,
hobbies, and other
interests.
Industry vs. Inferiority
Age 6 to 13 years
Child enters school and
begins learning
Child works to acquire
adult skills
Child learns how to
complete and master tasks
If child struggles to
acquire these adult skills
they develop a sense of
inferiority; may predispose
these individuals to
behavioral problems.
-During this time, teachers
play an increased role in
the child’s development.
The Power of Identity:
3 to 6 years
Normal clues:
Wanting to know who
we are.
Preoccupation with
power and gender
differences.
Experimenting with
social relationships
and the consequences
of behavior.
Developmental Tasks:
Separating fantasy
from reality
Testing recognition of
reality through
consequences and
exerting our power to
affect relationships.

21
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
5th stage The Genital
Stage:
-Age 13 to
adulthood
-Sexual urges are
once again
awakened.
-The primary
objective of this
phase is the
ultimate
separation from
dependence on
and attachment to
the parents and
the establishment
of adult, mature
relationships.
-The person
reaches a
satisfying capacity
for self realisation
and meaningful
participation in
the areas of work
and love; fulfilling
one’s adult roles
and duties.
Identity vs. Role
Confusion:
Age 13-21
Group identity and
preoccupation with
appearances
People at this stage
develop their own morality
and ethics and deal with
social expectations for
behaviors
This is the stage at which
individuals struggle to
develop their identity
Children are becoming
more independent, and
begin to look at the future
in terms of career,
relationships, families,
housing, et
The Power of Being
skillfull:
6 to 12 years
Normal clues:
Arguing and hassling
with others’ morals,
values and methods.
Wanting to do things
our own way and
nobody else’ s.
Developmental Tasks:
Experimenting with
different ways of doing
things.
Making mistakes to
find out what works.
Arguing with others
about how they do
things
22
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
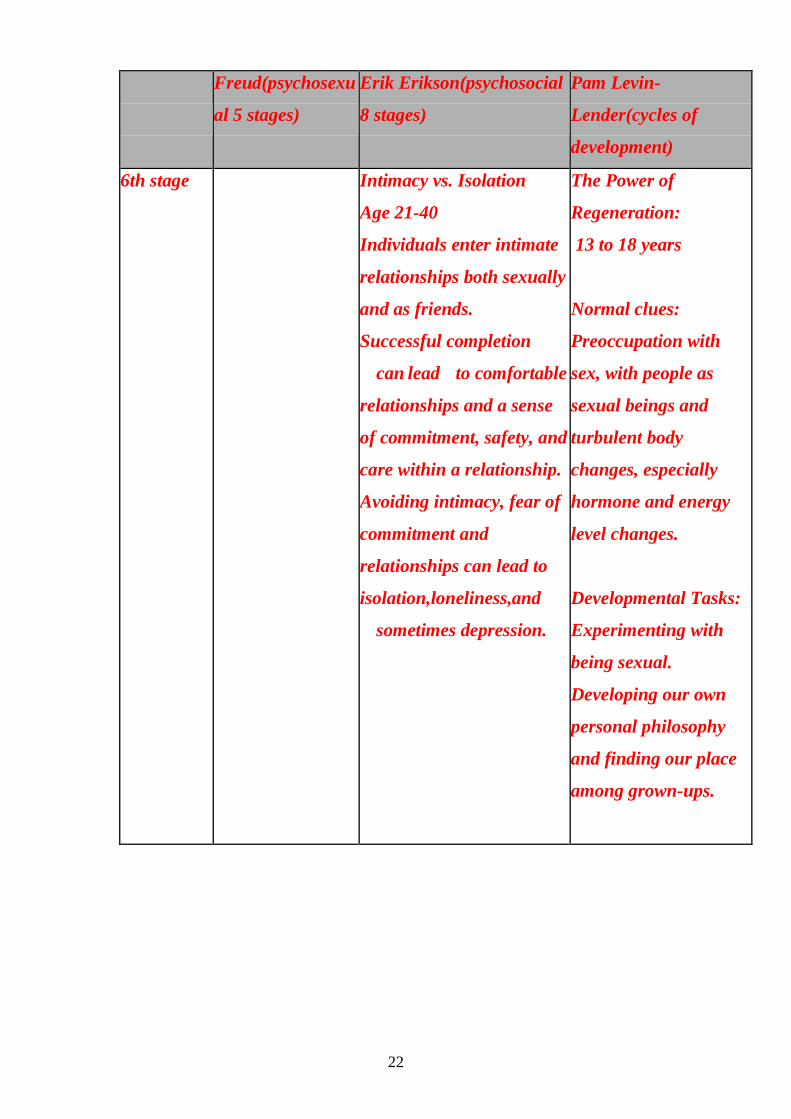
6th stage Intimacy vs. Isolation
Age 21-40
Individuals enter intimate
relationships both sexually
and as friends.
Successful completion
can lead to comfortable
relationships and a sense
of commitment, safety, and
care within a relationship.
Avoiding intimacy, fear of
commitment and
relationships can lead to
isolation,loneliness,and
sometimes depression.
The Power of
Regeneration:
13 to 18 years
Normal clues:
Preoccupation with
sex, with people as
sexual beings and
turbulent body
changes, especially
hormone and energy
level changes.
Developmental Tasks:
Experimenting with
being sexual.
Developing our own
personal philosophy
and finding our place
among grown-ups.
23
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
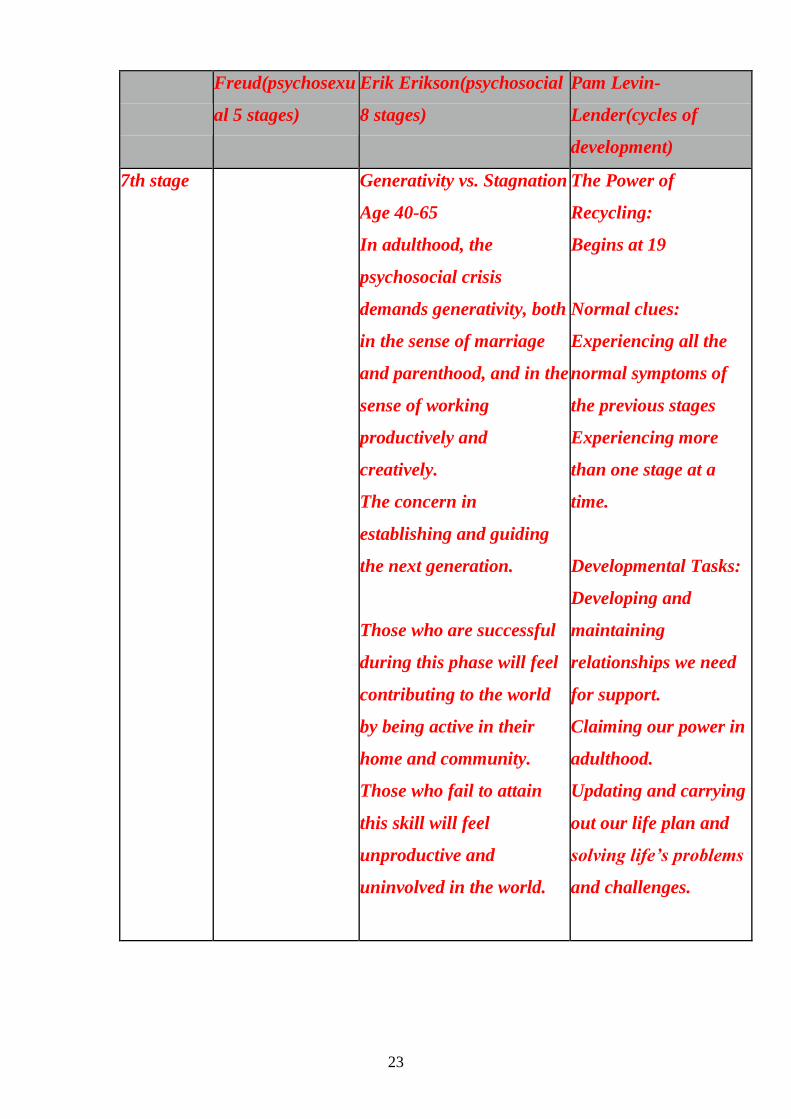
7th stage Generativity vs. Stagnation
Age 40-65
In adulthood, the
psychosocial crisis
demands generativity, both
in the sense of marriage
and parenthood, and in the
sense of working
productively and
creatively.
The concern in
establishing and guiding
the next generation.
Those who are successful
during this phase will feel
contributing to the world
by being active in their
home and community.
Those who fail to attain
this skill will feel
unproductive and
uninvolved in the world.
The Power of
Recycling:
Begins at 19
Normal clues:
Experiencing all the
normal symptoms of
the previous stages
Experiencing more
than one stage at a
time.
Developmental Tasks:
Developing and
maintaining
relationships we need
for support.
Claiming our power in
adulthood.
Updating and carrying
out our life plan and
solving life’s problems
and challenges.

24
Freud(psychosexu
al 5 stages)
Erik Erikson(psychosocial
8 stages)
Pam Levin-
Lender(cycles of
development)
8th stage Integrity vs. Despair
Over age 65.
is focused on reflecting
back on life
Sense of satisfaction with
one’s life vs. despair over
an inability to acheive your
goals.
If we see our lives as
unproductive, feel guilt
about our pasts, or feel
that we did not accomplish
our life goals, we become
dissatisfied with life and
develop despair, often
leading to depression
and hopelessness.
Discuss the nurse's role and function in the therapeutic milieu(10
grades)
To manage & coordinate from a holistic view rather than a
fragmented perspective of other MH team members this allows
nursing to ensure continuity of care. Nurse’s also assess
physiological & psychological status continually, influence of the
milieu therapy, provide physical & safety care, medication
25
administration & education, psychosocial care, mental health &
health education.
Further explanation of the above terms:
Physical & safety care – assess the patient’s ability to perform
ADLs, signs of physical illness or adverse reactions to
psychotropic drugs or reactions to withdrawal/detoxification when
indicated. Assess self-destructive or other-destructive behaviors.
Perform periodic safety checks (be sure to do it in a way as to not
violate patient rights).
Frequently patients with destructive tendencies are treated in
Partial Programs, here safety contracts are used (a type of
behavior approach). Contracts can be formed between patients and
peers as well.
Adequate staffing is very important, usually there is one per five
patients, at least one activity therapist available 12hrs/day & two
other paraprofessionals or MH workers.
In Partial Programs a ratio of one to ten patients is considered
safe, with again one activity therapist & two other professionals.