Embed Size (px)
Citation preview

CHAPTER 20
BENIGN BONE TUMORS OF THE FOOT AND ANKLE,
Robert R. Miller, D.P.M.
Stephen V. Corey, D.P.M.
Benign bone tumors of the foot and ankle typicallypresent both a diagnostic and therapeutic challengeto podiatric surgeons. These lesions have arelatively low incidence of occuffence in the footand ankle when compared to other regions of thebody, and the behavior of these lesions may mimicmalignant tumors. Not only is it impofiant torecognize a specific lesion to insure proper treat-ment, but the ability to differentiate a benign frommalignant process is of utmost importance.
It is difficult to determine the true incidence ofbenign bone tumors of the foot and ankle. Mostlarge studies do not distinguish individual tarsalbones, nor is there a distinction made befweenproximal and distal aspects of the tibia and fibula.Dahlin's Bone Tumors has reported findings of theMayo Clinic up until 7993.' Of a total of 2334benign bone tumors affecting the whole body,3.3o/o involved the foot and 19 .3o/o involved the tibiaand fibula. Of a total of 5642 malignant bonetumors affecting the entire body, 7.30/o involved thefoot and 12.40/o involved the tibia and fibula.
Table 1 displays the percentage of each lesionfound in the leg and foot. The lesions represent apercentage of local lesions compared to the totalnumber of lesions reported for the studies. It doesseem apparent that the overall incidence of footand ankle involvement is relatively low, but sometumors do occur with a somewhat frequent rate.Primarily, enchondroma, osteochondroma, osteoidosteoma, simple (unicameral) bone cysts, andaneurysmal bone cysts are somewhat common inthe foot and ankle.
RADIOGRAPHIC CHARACTERISTICS OFBENIGN BONE TUMORS
Several radiographic parameters have beendescribed to differentiate between benign andmalignant bone tumors. Although there areexceptions to each of these parame't-ers, most lesionscan be differentiated by following these guidelines.None of these guidelines alone can make thediagnosis of a benign or malignant bone tumor.
Table 1
Dahlin & Unni(1)EnchondromaOsteoid osteomaOsteochondroma
Resnick & Niwayama(2)EnchondromaOsteoid osteomaOsteochondromaSimple Bone CystAneurysmal Bone Cyst
SKELETAL LOCALIZAIION OF BENIGN BONE TUMORS
Tibia2o/o
79o/o
70%
3o/o
240/o
79o/o
6o/o
75o/o
Fibula!o/o
1o/ct
4o/o
2o/o
4o/o
4o/o
5o/o
7o/o
Foot2o/o
5o/o
7o/o
7o/o
l7o/o
60/o
7o/o
Bo/o
Total Lesions
748332/44
7028661
760488440)
CHAPTER 20 121
Cortical destruction is usually associated withmalignant lesions. Most benign lesions will have a
well-defined, intact overlying cortex within thebone of origin. Exceptions include benignprocesses such as giant cell tlrmors, aneurysmalbone cysts, eosinophilic granulomas, and infection,all of which can be associated with a variabledegree of cortical thinning and/or destruction.3
Periosteal reactions are non-specific findingswhich can occur in response to any process whichirritates the periosteum. Trauma, fracture healing,infection, as well as benign and malignant tumors,can cause periostitis. Most benign periostealreactions ate charucterized by a thick, densepattern where the affected bone has the abiliry torespond to the underlying pathology. This cangenerally occur because most benign processes areslow growing and allow adequate response time ofthe bone. On the other hand, a malignant oraggressive periosteal reaction is characterized by a
non-uniform region of bone production. Exampleswould include sunburst or lamellated periostealreactions where bone production is rapid and non-uniform. Most benign processes are characteizedby benign periosteal reactions, although anaggressive reaction can be seen in benign tumorssuch as aneurysmal bone cysts, aggressive giantcell tumors, eosinophilic granulomas, and osteoidosteomas.3 In general, malignant lesions will notcause benign periostitis.
The zone of transition is the border or marginwhich surrounds a lesion within the bone of origin.Helms states this is one of the most reliableindicators of a benign versus malignant lesion.3 A"narfow" or well-defined zone of transition is
characterizedby a margin that can be readily tracedwith a pencil or ball point pen. In contrast, a
"wide" zone of transition or ill-defined bordercannot readily be outlined or traced. Resnickdescribes three patterns of bone destruction:geographic, moth-eaten, and permeative.a Mostbenign bone tumors are characterized by a
"narrow'" (geographic) zone of transition, whereasmalignant or aggressive benign tumors ateassociated with a "wide" (moth-eaten or perme-ative) zone of transition.
Finally, the orientation of a lesion with respectto the long axis of a long bone can help todetermine a benign from malignant process. Mostbenign tumors of long bones will have a long axis
that is parallel to the long axis of the bone that isaffected. This is probably the least reliable featureas there are numerous exceptions, and probablyhas little to no value when evaluating tumors of thetarsal bones.
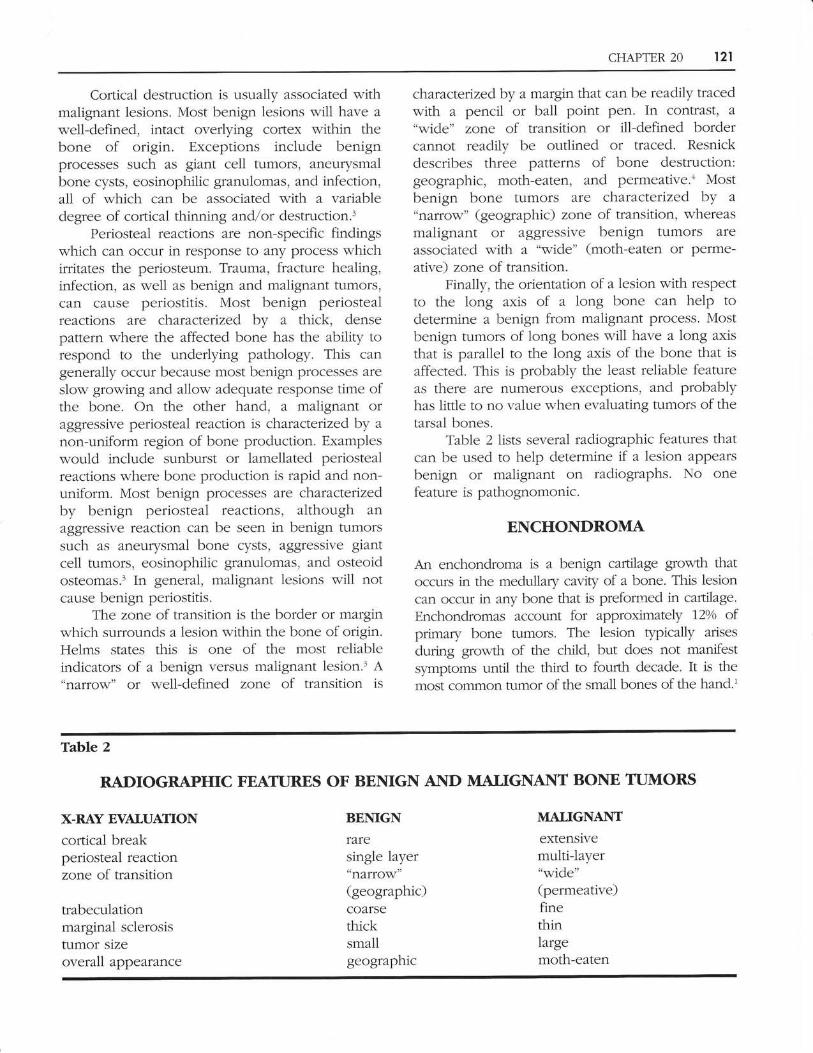
Table 2 lists several radiographic features thatcan be used to help determine if a lesion appearsbenign or malignant on radiographs. No onefeature is pathognomonic.
ENCHONDROMA
An enchondroma is a benign cartilage growth thatoccurs in the medullary cavity of a bone. This lesioncan occur in any bone that is preformed in cartilage.
Enchondromas account for approximately 72o/o ofprimary bone tumors. The lesion typically arises
during growth of the child, but does not manifestsymptoms until the third to fourth decade. It is the
most cofirmon tumor of the small bones of the hand.'
Table 2
X-RAY EVAIUAIIONcortical breakperiosteal reactionzone of transition
trabeculationmarginal sclerosistumor sizeoverall appearance
RADIOGRAPHIC FEAIIIRES OF BENIGN AND MATIGNAIIT BONE TUMORS
BENIGN
fzfesingle layer"nafrow"(geographic)COATSE
thicksmallgeographic
MALIGNANT
extensivemulti-layer"wide"(permeative)finethinlargemoth-eaten

122 CHAPTER 20
Enchondromas are thought to represent themost common tumor of the foot.1.56 Common sitesinclude the phalanges, metatarsals, and tarsalbones. The lesion is typically associared with pain-less swelling unless pathologic fracture occurs.Fractures through the lesion are common.
The radiographic features are by no meansunique. Typically, a radiolucency is encounteredwith a variable degree of thinning of the overlyingcortex. Often, pllnctate radio-densities can beappreciated which represent calcification of thematrk within the lesion. The presence of pinhead-to match head-sized radiopacities (reflecting calcifi-cation) in the regional area helps to clinch thediagnosis.T The tumor is most commonly located inthe central to distal aspect of the phalanges andmetatarsals.
Treatment should be aimed at the preventionof pathologic fracture, especially if the lesion isfound in the small bones of the hands and feet.Curettage with bone grafting is the most commonmethod of treatment. Curettage with cryotherapy isanother treatment modality. The recurrence rateafter resection of the lesion is low.
OSTEOID OSTEOMA
An osteoid osteoma is characterized by a centralnidus that is typically less than one centimeter insize. Another distinct feature is that the nidus isusually surrounded by a variable degree of reactivesclerosis.
Osteoid osteomas account for approximately770/o of all primary bone tumors. Most patients withthis lesion are between the ages of 10 and 25 yearsold. The lesion is characterized by nocturnalpain that is frequently rapidly relieved by theadministration of aspirin or nonsteroidal anti-inflammatories. There is evidence that the pain maybe mediated by prostaglandins.'
Osteoid osteomas probably represent thesecond most common tumor of the foot, with thetalr-rs being most commonly affected.6 A11 othertarsal and leg bones can be affected. The painassociated with the lesion is often worse withweight bearing and ambulation. Clinical signs caninclude pain with joint range of motion, an antalgicgait, and muscle atrophy which may mimic aneuromuscular disease or a systemic form ofarthdtis. Most commonly, the lesion will reveallocalized edema and tenderness on physicalexamination.
The radiographic features of the lesion can bedistinct when present. The lesion is characterizedby a central nidus (appears radiolucent) and avariable amount of reactive sclerosis. These find-ings are usually very obvious if the lesion is presentin long bones and has a cortical location. Lesionsoccurring in primary cancellous bone may notshow such distinct features. Three out of tenosteoid osteomas of the foot reported by Shereff etal. had normal routine radiographs, but weredetected with tomography.'\7hen lesions are notvisualized by plain radiographs, most can belocated with the use of a CT scan.
The mainstay of treatment seems to becomplete surgical resection of the nidus. Often,incomplete resection of the nidus may affordpartial to total relief of symptoms.lo In order toadequately resect the lesion, it must first be local-ized within the parent bone. Most often this isaccomplished by the use of a CT scan, but othermethods which have been described include theuse of radioactive isotopes (such as technetium),and tetracycline with UV light fluorescence.Surgical resection seems to be associated with anapproximately 2o/o recufrence rate. Spontaneousregression of untreated osteoid osteomas has beenrepofted, although no histologic confirmation wasobtained in many of the cases.'n
OSTEOCHONDROMA
An osteochondroma is a hyaline cartilage cappedprotrusion on the external surface of a bone.Osteochondromas are the most common primarybone tumors and account for approximately 50o/o ofall benign bone tumors. Almost any age group canbe affected, although most patients will presentwith this lesion in the second to third decade.Malignant transformation has been described inapproximately 1o/o of these lesions, and shouldalways be suspected if this lesion is painful.Complications that have been described with thislesion include fracture at the base of the lesion,infarction of the osseous stalk, impingement oflocal tendons and nelves, pseudoaneurysm ofadjacent blood vessels, and bursae formation overthe tip of the lesion.'u
\7hen present in the foot, the lesions seem tooccur most commonly in the metatarsals, tarsalbones, and phalanges. It can also be found nearthe metaphyseal region of the tibia and fibulaabout the ankle joint. Most frequently, the lesion

CFIAPTER 20 123
will present as a painless mass that can be aggra-vated by weight bearing and ambulation. Thelesion is often found incidentally when routineradiographs are obtained.
The radiographic features of this lesion areunique and distinct from any other bone tumor.The lesion is characterized by a "stalk" that usuallyemanates from the metaphyseal region of a longbone. The base and stalk of the lesion containcortical and medullary bone that are in directcontinuily with the bone of origin. The lesion alsofrequently points "away" from the joint near whichit arises.
One lesion that must be differentiated from anosteochondroma is a subungual exostosis. Majordifferences include the following:
A subungual exostosis does not exhibitcortical or medullary continuily with the boneof origin.
A subungual exostosis arises from the tip of aphalanx (which is not metaphyseal bone).
The cartilage cap of a subungual exostosisconsists of fibrocartilage, whereas the cap of anosteochondroma consists of hyaline caftilage.
A subungual exostosis displays histologicfeatures which consist of spindle cell pro-liferation.
The treatment of an osteochondroma typicaliyconsists of excision of the tumor flush with thebone of origin. Not all lesions need to be resected,but indications would include pain or disability, anabnormal increase in size or pain, or radiographicfeatures that suggest malignancy. Resection hasbeen associated with an approximately 20/o
fecurfence fate.
STMPLE (UlVrCeUERAr) BONE CYST
Simple bone cysts are fluid-filled solitary cysts thattypically arise in the metaphyseal region of longbones. These lesions are most frequently seenin the femur and humerus of children andadolescents. In adults the lesion is most commonlyfound in the calcaneus and ilium. The lesion israrely symptomatic unless pathologic fracture hasoccurred. Often the lesion will produce mild andvague symptoms, but attention is usually directedto the lesion as a result of minor or incidentaltrauma.
The cyst is usually found in the central aspectof long bones. In the calcaneus, the lesion can befound inferior to the posterior facet. The cortex ofthe parent bone is always intact, unless fracture hasoccurred. A characteristic feature is the fallenfragment sign. This represents a free fragment ofcortical bone which by gravity falls to the lowestportion of the cyst. The fragment can fall freelyas the result of the cyst being fluid filled andunilocular.
Curettage and bone grafting of the lesion is
the conventional method of treatment. Scaglietta etal. showed favorable results in 90o/o of patientstreated by intralesional injection of methylpred-nisolone acetate.l The cyst is obserued foropacification over the next 3 to 6 month period toevaluate for healing. Regardless of the method oftreatment, recurrence rates have been reported as
high as 200.0 to 5000.
ANEURYSMAL BONE CYST
This lesion accounts for approximately 5o/o ofprimary bone tumors. Nearly B0% of these lesionsoccur in patients less than 20 years of age. Of 257
cases of benign bone tumors of the foot treated atthe Bone Tumor Center of the Ptizzoli Institute,approximately 700/o of the tumors were aneurysmalbone cysts.l'
There is some confusion in the literature as towhether this is a primary or secondary lesion. Someauthors believe that the tumor is a primary lesionthat arises as ^n independent entity, whereasothers believe the lesion arises from anotherpre-existing lesion. Two lesions which seem tocommonly give rise to an aneurysmal bone cystinclude giant cell tumors and chondroblastomas.
Pain and swelling of varying duration are themost common presenting symptoms. Lesionswhich are in close proximity to joints may causepain with joint motion or even an apparenlsynovitis. Pathologic fracture is common.Aneurysmal bone cysts often show rapid enlarge-ment during pregnancy.
Plain radiographs often reveal a metaphyseallesion located in an eccentric position. Corticalthinning and osseous expansion are frequentlynoted features. Fluid-fluid levels are characteristicand seen on both CT scans and MRI. The fluid-fluidlevels represent loculated areas within the cyst thatcontain degraded blood products, serum, andtumor fluid.

124 CI]APTER 20
The most successful treatment reported byDahlin has been surgical removal of the entirelesion, or as much of it as possible.' Bone graftingof the resultant defect may be required. Curettagewith cryotherapy and en bloc resection have alsobeen described. Excision of the lesion is associatedwith a 70o/o to 30o/o recurrence rate.
SUMMARY
Recognition of benign bone tumors of the lowerextremity is afi important skill for podiatricsurgeons. Not only is it important to be able torecognize individual benign bone tumors, but it isalso very important to be able to distinguish benignfrom malignant lesions. Treatment and appropriatereferral of bone tumors is based on the ability torecognize the lesion, an understanding of currenttreatment methods, and the skills of the surgeon.
REFERENCES
Dahlin D, Unni KK: Bone Tumors, General A$)ects and Data on1.1,087 Cases,5rh ed, Philadelphia, PA: Lippincott-Raven; L996.Resnick D, Niwayama G:Diagnosis of Bone and Joint Disorders,Vol. 6, Philadelphia, PA: W.B. Saunders; 1988.Helms CA:Malignant Bone and Soft Tissue Tumors. InFurulamentals of Diagnostic RadiologtBaltimore, MD: \7i11iams &\(zilkins: 1994.Resnick D:Tumors and Tumor-1ike Lesions of Bone: RadiographicPrinciples. In Bone c1n(l Joint Imaging, Philadelphia, PA: W.B.Saunders; 1!89.Shajowicz F: Tumors and TumorJike Lesions of Bone andJointsNew York, NY:Springer-Verlag; 1981.
Steiner GC: Neoplasms of tbe Fctot and Leg, Baltimore, MD:'Williams & Y/ilkins; 1990.
Jaffe HL: Atlas of Bone Patholog,t With Clinical and RacliograpbicCorelations, Philadelphia, PA: J.B. Lippincott; 1992.
Gitelis S, Wilkins R, Conrad EU:Benign bone tufi1ors. J BoneJointSurg 77 A:77 56-17 82, 1995.Shereff MJ, Cullivan W'T, Johnson KA:Osteoid Osteoma of thefoot, J Bone Joint Surg 65$38-641, 1983.Huvos AG :Bone Tumors: Diagnosis, Treatment, and Prognosis,Philadelphia, PA: W.B. Saunders; 1991.Casadei R, et al.:Aneurysmal bone cyst and giant ce1l tumor of thetoot, Foot Ankle 77487-495, 1995.
1.
2.
3.
5.
6.
7.
8.
o
10.
11.