-
REVIEW CURRENTOPINION Emotion regulation and mental health:
recentfindings, current challenges, and future
directionswww.co-psychiatry.coma b,cMatthias Berking and Peggilee
WuppermanPurpose of reviewIn recent years, deficits in emotion
regulation have been studied as a putative maintaining factor
andpromising treatment target in a broad range of mental disorders.
This article aims to provide an integrativereview of the latest
theoretical and empirical developments in this rapidly growing
field of research.
Recent findingsDeficits in emotion regulation appear to be
relevant to the development, maintenance, and treatment ofvarious
forms of psychopathology. Increasing evidence demonstrates that
deficits in the ability to adaptivelycope with challenging emotions
are related to depression, borderline personality disorder,
substance-usedisorders, eating disorders, somatoform disorders, and
a variety of other psychopathological symptoms.Unfortunately,
studies differ with regard to the conceptualization and assessment
of emotion regulation,thus limiting the ability to compare findings
across studies. Future research should systematically work touse
comparable methods in order to clarify the following: which
individuals have; what kinds of emotionregulation difficulties
with; which types of emotions; and what interventions are most
effective in alleviatingthese difficulties.
SummaryDespite some yet to be resolved challenges, the concept
of emotion regulation has a broad and significantheuristic value
for research in mental health.
Keywordsemotion regulation, mental disorders, psychopathology,
review, skillsaDepartment of Clinical Psychology and Psychotherapy,
Philipps-Univer-sity, Marburg, Germany, bJohn Jay College, City
University of New York,New York and cYale School of Medicine, New
Haven, Connecticut, USA
Correspondence to Matthias Berking, Department of Clinical
Psychologyand Psychotherapy, Philipps-University, Gutenbergstrasse
18, D-35032Marburg, Germany. Tel: +49 6421 282 4050; fax: +49 6421
282 4065;e-mail: [email protected]
Curr Opin Psychiatry 2012, 25:128134
DOI:10.1097/YCO.0b013e3283503669INTRODUCTION
Emotion regulation refers to extrinsic and intrinsicprocesses
responsible for monitoring, evaluating,and modifying emotional
reactions, especially theirintensive and temporal features, to
accomplishones goals [1]. After years as a major research topicin
developmental psychology and borderlinepersonality disorder (BPD),
the concept of emotionregulation has recently become popular in
generalmental-health and psychotherapy research. At thispoint, not
a month passes without at least one peer-reviewed publication on
emotion regulation in thecontext of depression, anxiety,
substance-relateddisorders, eating disorders, and so on.
However,despite its popularity, the concept struggles to
attainviability as a scientific construct due to variousunmet
challenges involving definition, assessment,and clinical
implications. Such problems have beendiscussed (although not
solved) in the context ofdevelopmental psychology [1,2], but not
yet inrelation to the specific needs of research with aclinical
focus. Therefore, the aim of this article isto, briefly, first,
review relevant findings regardingemotion regulation and
psychopathology and,second, address the above challenges as they
pertainto research focused on clinical psychology, psychia-try, and
psychotherapy.BRIEF OVERVIEW OF RELEVANT FINDINGS
A significant focus on emotion regulation can beobserved in the
following areas of clinical research.Volume 25 Number 2 March
2012
mailto:[email protected]
-
KEY POINTS
Deficits in emotion regulation are relevant in the contextof
various mental-health problems.
An overly broad conceptualization of emotionregulation threatens
its value as a heuristic paradigm.
Validity of assessment of emotion regulation needs tobe
improved.
A stronger clinical focus is needed in research onemotion
regulation.
Research needs to identify mechanisms by whichemotion regulation
skills affect psychopathology.
Emotion regulation and mental health Berking and
WuppermanClinical child and adolescent psychology
Evidence suggests that emotion regulation ininfants is initiated
largely by caregivers and gradu-ally becomes more self-initiated
over time [2]. Strat-egies evolve under the influence of
variousinteracting factors, including the quality of care-givers
support as the child learns to cope withdistressing situations [3].
Emotion regulation skillsin children and adolescents have been
demon-strated to (negatively) predict (subsequent) external-izing
and internalizing problems in numerousstudies [4,5
&
].Borderline personality disorder
Substantial evidence supports emotion dysregula-tion as a core
construct underlying BPD. BPD isassociated with less emotional
awareness and clarity[6,7], less ability to tolerate distress when
pursuinggoals [8], the reported tendency to use harmfulemotion
regulation strategies (e.g., self-injury) inresponse to distressing
situations [9], and deficitsin the ability to use cognitive
reappraisal to regulateemotions [10
&
]. Persons with BPD tend to displaylower parasympathetic
activity in response toemotional stressors than do controls [11];
andemotion dysregulation predicts subsequent BPD fea-tures, even
when controlling for impulsivity [12].Finally, individuals with BPD
endorse deficits in allfacets of emotion regulation self-report
measures[13]; also, self-reported emotion regulation deficitsare
associated with amygdala activation [14
&
].Depression
Depression is widely conceptualized as a con-sequence of
dysfunctional emotion regulation[1517]. Consistently, depressed
individuals reportdifficulties, first, identifying emotions
[18,19];0951-7367 2012 Wolters Kluwer Health | Lippincott Williams
& Wilksecond, supporting themselves when experiencingnegative
emotions [20
&&
,21]; third, accepting andtolerating negative emotions [2226];
and, fourth,adaptively modifying emotions [2729]. Longitudi-nal
research shows that positive expectations aboutthe ability to
modify negative affect predictreductions in depression [29], and
dysfunctionalemotion-regulation strategies predict depressionlevels
2 years after initial assessment [30]. Further-more, experimental
studies show that depressedindividuals display difficulties
utilizing adaptiveemotion regulation strategies (e.g., accepting
nega-tive emotions [31]) and respond to negative moodinduction with
less effective emotion regulationstrategies (e.g., suppression)
than do nondepressedindividuals [32
&
].Anxiety disorders
Emotion regulation deficits are involved in a varietyof anxiety
disorders [33
&
]. Such deficits can result inineffective coping with
conditioned fear responses,leading the fear reaction to seem (even
more) aver-sive and uncontrollable thus reconditioning thereaction
and increasing the likelihood of avoidancebehaviors that may become
chronic. Consistently,when compared with nonanxious controls,
individ-uals with generalized anxiety disorder report
poorerunderstanding of emotions, greater negative reac-tivity to
emotions, and less ability to self-sootheafter experiencing
negative emotions [34,35] (seereference [36] for conflicting
findings on the abilityto identify and describe emotions). In
individualswith posttraumatic stress disorder (PTSD),
symptomseverity and impairment are both associated withlack of
emotional clarity, lack of emotional accept-ance, difficulty
engaging in goal-directed behaviorwhen upset, and an overall
limited ability to engagein emotion regulation strategies [37,38].
Emotionregulation difficulties also mediate the associationbetween
PTSD symptom severity and substance ab-use in patients with
histories of chronic abuse [39],and enhancement of emotion
regulation skills inthe first phase of PTSD treatment increases
theeffectiveness of the second (exposure-based)
phase[40].Substance-related disorder
One of the most prominent clinical factors in alco-hol and drug
use is difficulty coping with negativeaffect [41], to the extent
that substance misuse iswidely conceptualized as an effort to
regulate oravoid negative emotions [20
&&
,41,42,43&
]. Forexample, epidemiological and treatmentoutcomestudies show
that negative affect predictsins www.co-psychiatry.com 129
-
Behavioural medicinesubsequent desire to drink and drinking
levelin individuals treated for alcohol dependence[4448]; the
induction of negative affect predictsincreased urges to drink
[4951]; interventionsaimed at alleviating depressed mood or
anxietysymptoms have been shown to decrease relapseand severity of
use [52,53]; and deficits in emotionregulation skills predict
relapse during and aftercognitivebehavioral therapy for
dependence[20
&&
]. Additionally, cocaine-dependent individualsreport more
emotion regulation difficulties than docontrols, particularly
during early abstinence [54].Eating disorders
Increasing evidence suggests that eating disordersymptoms
(binging, purging, and/or restricting)serve as dysfunctional
attempts to regulate or sup-press negative emotions [5558]. For
example, nega-tive mood predicts binging and purging in
bulimianervosa [57,59,60], as well as binge episodes inbinge eating
disorder (BED) [6163]. Compared withcontrols, women with bulimia
nervosa, BED, andanorexia nervosa report greater difficulties
withemotional awareness [64,65,66
&
], greater tendencyto avoid emotions, and less ability to accept
andmanage emotions [67]. In a sample of adolescentgirls, low
awareness of emotions and dysfunctionalstyles of coping with
emotions partially mediated therelationship between body
dissatisfaction and buli-mia nervosa symptoms [68]. In college
students withBED, the frequency of binge episodes was predictedby
total score of the Difficulties in Emotion Regula-tion Scale (DERS)
[69], as well as every one of thesubscales [70]. Finally, women
with anorexia nervosareport significantly more difficulties in all
subscalesof the DERS than do nonpsychiatric controls
[71].Somatoform disorders
Emotion regulation has long been thought to play acentral role
in the development of somatoformsymptoms. In the 1970s, Nemiah and
Sifneos [72]introduced the concept of alexithymia
(difficultyidentifying and describing emotions): individualsunable
to detect, name, and express emotions wouldlikely have difficulties
using cognitive resources toregulate emotions and, thus, have an
increasedlikelihood of misrepresenting bodily
sensationsaccompanying emotions [73]. In the ensuing deca-des,
numerous empirical studies have provided sub-stantial evidence that
somatoform disorders areassociated with deficits in the abilities
to con-sciously experience and tolerate emotions, correctlyidentify
emotions, and accurately link emotions tobody sensations
[74,75,76
&
,7780].130 www.co-psychiatry.comRELEVANT CHALLENGESIn order to
enhance the viability of emotion regu-lation as a scientific
construct, the following chal-lenges must be addressed in
clinically focusedresearch.Definition-related challenges
Perhaps the primary concern regarding emotionregulation as a
scientific construct is that everythingseems to be emotion
regulation these days. Whetherit is worry, catastrophizing,
rumination, suppres-sion of emotional expression, and so on
variousconcepts formerly investigated as relevant phenom-ena on
their own are currently being subsumedunder the concept of emotion
regulation[81
&
,82,83]. However, such a loosely defined con-ceptualization runs
the risk of losing meaning and,thus, heuristic value. Therefore, a
critical assessmentis needed to specify what actually
constitutesemotion regulation. Of note is that emotion regu-lation
is traditionally defined in terms of function,not content. Every
process can be described asemotion regulation if driven by
(explicit or implicit)intentions, goals, and/or efforts to redirect
andmodify the flow of emotions [84]. In contrast, con-cepts such as
worry, catastrophizing, and rumina-tion are largely components of
affective states suchas anxiety and dysphoric mood [2]. Their
function isnot to regulate these states, but instead to assess
theseriousness of perceived threat or find a way out ofaversive and
uncontrollable situations. Therefore,these processes are often more
consistent witha self-regulation perspective, as opposed to
anemotion regulation perspective.
With regard to the suppression of the emotionalexpression, it is
of note that at least in clinicalpopulations such attempts are
usually driven bythe intention to avoid negative evaluation by
others(and/or by oneself for feeling out of control
and/ordisplaying emotions in front of others). Given thatemotions
can exist without being expressed andthat one does not necessarily
strive to regulateemotional experience when suppressing
emotionalexpression, we propose that this process should notbe
considered an emotion regulation strategy per se.Future research
should work to distinguish moreclearly between the suppression of
emotion (poten-tially an emotion regulation strategy) and the
sup-pression of the expression of emotion (unlikely anemotion
regulation strategy).Assessment-related challenges
One of the most relevant challenges remains thedevelopment of
instruments and procedures thatvalidly and reliably assess emotion
regulation.Volume 25 Number 2 March 2012
-
Emotion regulation and mental health Berking and WuppermanCommon
problems with current practices includesimply assessing intensity
of negative emotions(e.g., sadness in depression) and concluding
thatdeficits in emotion regulation must be present ifindividuals
are unable to reduce the intensity ofunwanted emotions. However,
depression is definedthrough the existence of such unwanted
emotions;thus, the heuristic value of such a conclusion isclearly
limited unless the emotion regulationdeficits are specified and
assessed separately.Additionally, it is of note that often emotions
areassessed with problematic instruments. Forexample, the trait
version of the widely usedState-Trait Anxiety Inventory by
Spielberger et al.[85] includes the item I feel like crying. As
crying iscommonly acknowledged as an indicator of sadness(not
anxiety), the face validity of this scale isseverely
compromised.
Another challenge is the use of self-reportmeasures, which have
been criticized on thegrounds that assessing emotional awareness
anddifferentiation with self-reports is paradoxical[86]. However,
as it is possible that at least on atrait level individuals may be
able to reportsuch skills with the help of social comparisonsand
feedback received from others, these instru-ments might be useful
in spite of this argument.Nevertheless, the validity of self-report
definitelyrequires further research. Another challenge is
thatnumerous emotion regulation measures inquireabout methods of
coping with emotions or feel-ings without specifying to what
emotion thequestion is referring. However, depressed personsare
likely to refer to feelings of sadness, despair, andhopelessness,
whereas anxious persons would bemore likely to refer to feelings of
fear and anxiety.If studies using these instruments find that
depres-sed persons are less able to engage in a certainemotion
regulation skill, such a finding might bedue to specific skills
deficits of depressed persons but it might also be due to specific
characteristics ofthe emotion to which the person refers
whenanswering the question. Thus, the validity of suchinstruments
should be investigated carefully, andemotion-specific self-reports
should be developed[87,88].
Experimental assessment of emotion regulationalso has problems
and limitations. With regard toecological validity, every aspect of
an experimentshould be examined carefully to determine
whetherparticipant performance is affected by the stimuliused to
elicit the emotion, the instructions on howto regulate the emotion,
and/or the surroundings inwhich the experiment occurs. Moreover, of
noteis that experimental paradigms only investigateshort-term
effects of emotion regulation strategies0951-7367 2012 Wolters
Kluwer Health | Lippincott Williams & Wilkin certain
situations. Thus, in order to provide themost valid assessment of
emotion regulation, itsantecedents, and its consequences, future
researchshould combine self-reports (questionnaire or,preferably,
ecological momentary assessment pro-cedures) with experimental
assessments and applymultitraitmultimethod procedures to
longitudinaldesigns.Challenges regarding valid and
clinicallyrelevant conclusions
The surge in popularity of emotion regulationresearch has
increased the risk of premature con-clusions regarding clinical
relevance. For example,the vast majority of studies on emotion
regulationand psychopathology employ cross-section designsand argue
that cross-sectional associations provideevidence that emotion
regulation deficits contrib-ute to the development and maintenance
of psy-chopathology. However, as deficits in emotionregulation may
also develop as a result of a mentaldisorder, additional
prospective research addressingboth putative causal pathways is
dearly needed [89].
In experimental research, generalizability isoften an issue. For
example, findings that reapprais-ing the situation is a more
effective strategy thansuppressing the expression of emotions [83]
haveoften been used to argue that strategies with a focuson
antecedents of emotions (e.g., the situation cue-ing the emotion,
the perception of the situation, orthe appraisal of the situation)
are more effectivethan strategies with a focus on the
emotionalresponses themselves (e.g., the expression of theemotion).
However, for a valid test of this hypo-thesis, a representative
sample of each categorymust first be drawn and evaluated. This need
isparticularly relevant in that other response-focusedstrategies
such as expressing an emotion throughappropriate actions, utilizing
self-soothing strat-egies, and the dialectical behavior therapy
skill ofopposite action have been utilized successfully
intherapeutic treatments for several years.
Moreover, basic research on emotion regulationoften focuses on
stimuli, emotions, and emotionregulation strategies that, although
relevant to thegeneral population, might be of limited relevancefor
patients experiencing psychiatric disorders.Thus, more clinically
focused research is neededto address this gap. Additionally,
studies are neededto investigate the mechanisms by which
specificemotion regulation skills interact to affect
psycho-pathology in clinical populations [90
&
]. As such,future research should include mediation analysesin
prospective randomized controlled trials toidentify changes in
emotion regulation mostins www.co-psychiatry.com 131
-
Time
Sym
pto
m s
ever
ity
(a) Patient
Type of disorder
Severity of disorder
Chronicity of disorder
Level of comorbidity
Personality traits
Social support
Strengths/resources
etc.
(1) Riskfactor
(4) Treatmenttarget
(2) Maintaining factor
(b) ER skills deficits
Awareness/clarity
Understanding
Acceptance/toleranceSelf-compassion
Situation selection
Attention deployment
Situation improvement
Reappraisal
etc.
(c) Emotions(& other affective responses)
Stress
Anxiety
Anger
Sadness
etc.
Shame
Guilt
Fear
(3) Symptom/consequence
(d) Interventions
Focus on one/few vs.broad range of skills
Implicit vs. explicitskills training
Cognitive techniques
etc.
Focus on one/few vs.broad range of emotions
Experiential techniques
Mindfulness-basedtechniques
Behavioral techniques
(5) Mechanismof change
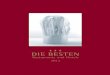
FIGURE 1. Areas for future research on emotion regulation in the
mental-health field. ER, emotion regulation.
Behavioural medicinestrongly associated with subsequent
treatment out-come. Then, implicit or explicit strategies topromote
these changes need to be developed andevaluated in randomized
clinical trials. If shown tobe effective, these strategies should
then be detailedto the extent that they could be used alone
orincorporated into existing evidence-based treat-ments [91].
Thereby, psychotherapy research wouldmove away from evaluating only
broad categories ofpsychotherapeutic interventions (which often
seemto overlap on specific levels [92]) and wouldinstead also
include a focus on specific interventionsfor specific
problems.CONCLUSION
Although emotion regulation has become a popularscientific
concept, the quest for conceptual clarity,valid assessment, and
accurate conclusions aboutimplications has only begun. Thus,
without claim-ing to offer solutions for all the challenges
associ-ated with this concept, we have provided a briefoverview of
relevant findings and offered a fewcaveats for consideration in
future research. At thispoint, available data indicate that emotion
regula-tion is associated with various forms of psycho-pathology
and might be considered a putativetransdiagnostic factor relevant
for the development,maintenance, and treatment of several mental
dis-orders. Future research should include more strin-gent methods
of investigating causal relationshipsand work to clarify the
following: which patients or132 www.co-psychiatry.comat-risk
individuals have; what types of difficulties inthe regulation of;
what emotions; and what inter-ventions are most effective in
alleviating these diffi-culties (Fig. 1).
In this context, future research should aim todistinguish
between deficits in emotion regulationskills as a risk factor;
maintaining factor; symptom/consequence of the disorder; treatment
target; and/or mechanism of change (Fig. 1). This task
willobviously be complex and require substantialresources. If
researchers could agree upon a commondefinition, methods to elicit
emotions and assessemotion regulation strategies, and means
throughwhich the causal effect of emotion regulationon
psychopathology could be investigated, thenavailable resources
could be pooled, findings fromvarious work groups could be
compared, and coor-dinated research activities could be initiated.
If theseactivities consider the specific characteristics ofemotion
regulation in a clinical context, and if thisresearch is conducted
with the necessary scientificvigor, the emotion regulation paradigm
will have aneven greater heuristic value for research on
mentalhealth, psychopathology, and psychotherapy.
Acknowledgements
The authors thank Elena Heber for assisting in theliterature
review on which this article is based. Pre-paration of this article
was supported by GrantsPA001-113040 and PZ00P1-121576/1 from the
SwissNational Science Foundation to M.B. and by GrantDF08-028 from
the Donaghue Foundation to P.W.Volume 25 Number 2 March 2012
-
Emotion regulation and mental health Berking and
WuppermanConflicts of interest
There are no conflicts of interest.REFERENCES AND
RECOMMENDEDREADINGPapers of particular interest, published within
the annual period of review, havebeen highlighted as:
& of special interest&& of outstanding interest
Additional references related to this topic can also be found in
the CurrentWorld Literature section in this issue (p. 162).
1. Thompson RA. Emotion regulation: a theme in search of
definition. MonogrSoc Res Child Dev 1994; 59:2552.
2. Cole PM, Martin SE, Dennis TA. Emotion regulation as a
scientific construct:methodological directions for child
development research. Child Dev 2004;75:317333.
3. Morris AS, Silk JS, Steinberg L, et al. The role of the
family context in thedevelopment of emotion regulation. Soc Dev
2007; 16:361388.
4. Eisenberg N, Cumberland A, Spinrad TL, et al. The relations
of regulation andemotionality to childrens externalizing and
internalizing problem behavior.Child Dev 2001; 72:11121134.
5.&
Kim J, Cicchetti D. Longitudinal pathways linking child
maltreatment, emotionregulation, peer relations, and
psychopathology. J Child Psychol Psychiatry2010; 51:706716.
This article presents sorely needed prospective studies on the
associationbetween emotion regulation and psychopathology, while
also including a focuson the processes potentially responsible for
such association.6. Leible TL, Snell WE Jr. Borderline personality
disorder and multiple aspects of
emotional intelligence. Pers Indiv Differ 2004; 37:393404.7.
Wolff S, Stiglmayr C, Bretz HJ, et al. Emotion identification and
tension in
female patients with borderline personality disorder. Br J Clin
Psychol 2007;46:347360.
8. Gratz KL, Rosenthal MZ, Tull MT, et al. An experimental
investigation ofemotion dysregulation in borderline personality
disorder. J Abnorm Psychol2006; 115:850855.
9. Wupperman P, Neumann CS, Whitman JB, Axelrod SR. The role of
mind-fulness in borderline personality disorder features. J Nerv
Ment Dis 2009;197:766771.
10.&
Schulze L, Domes G, Kruger A, et al. Neuronal correlates of
cognitivereappraisal in borderline patients with affective
instability. Biol Psychiatry2011; 69:564573.
This article offers experimental and physiological findings as
evidence that in-dividuals with BPD display deficits in the emotion
regulation strategy of cognitivereappraisal.11. Kuo JR, Linehan MM.
Disentangling emotion processes in borderline person-
ality disorder: physiological and self-reported assessment of
biological vul-nerability, baseline intensity, and reactivity to
emotionally evocative stimuli. JAbnorm Psychol 2009;
118:531544.
12. Tragesser SL, Solhan M, Brown WC, et al. Longitudinal
associations inborderline personality disorder features: diagnostic
interview for border-lines-revised (DIB-R) scores over time. J
Personal Disord 2010; 24:377391.
13. Gratz KL, Gunderson JG. Preliminary data on an
acceptance-based emotionregulation group intervention for
deliberate self-harm among women withborderline personality
disorder. Behav Ther 2006; 37:2535.
14.&
Niedtfeld I, Schulze L, Kirsch P, et al. Affect regulation and
pain in borderlinepersonality disorder: a possible link to the
understanding of self-injury. BiolPsychiatry 2010; 68:383391.
This study demonstrates that self-report emotion regulation
measures displayexpected associations with physiological data in
individuals with BPD, while alsoproviding evidence that pain
reduces negative affect in BPD individuals thusprompting such
individuals to use self-injury as an emotion regulation
strategy.15. Gross JJ, Munoz RF. Emotion regulation and mental
health. Clin Psychol Sci
Pr 1995; 2:151164.16. Kring AM, Werner KH. Emotion regulation
and psychopathology. In: Philippot
P, Feldman RS, editors. The regulation of emotion. Mahwah, New
Jersey:Lawrence Erlbaum Associates Publishers; 2004. pp.
359385.
17. Hollon SD, Munoz RF, Barlow DH, et al. Psychosocial
intervention develop-ment for the prevention and treatment of
depression: promoting innovationand increasing access. Biol
Psychiatry 2002; 52:610630.
18. Honkalampi K, Saarinen P, Hintikka J, et al. Factors
associated with alex-ithymia in patients suffering from depression.
Psychother Psychosom 1999;68:270275.
19. Rude SS, McCarthy CT. Emotional functioning in depressed and
depression-vulnerable college students. Cogn Emotion 2003;
17:799806.
20.&&
Berking M, Margraf M, Ebert D, et al. Emotion regulation skills
as a predictor ofrelapse during and after treatment of alcohol
dependence. J Consult ClinPsych 2011; 79:307318.
This study is the first to investigate prospective effects of
emotion regulation onrelapse in alcohol-dependent patients both
during treatment and during follow-up.0951-7367 2012 Wolters Kluwer
Health | Lippincott Williams & Wilk21. Gilbert P, Baldwin MW,
Irons C, et al. Self-criticism and self-warmth: animagery study
exploring their relation to depression. J Cogn Psychother
2006;20:183200.
22. Brody CL, Haaga DAF, Kirk L, Solomon A. Experiences of anger
in people whohave recovered from depression and never-depressed
people. J Nerv MentDis 1999; 187:400405.
23. Campbell-Sills L, Barlow DH, Brown TA, Hofmann SG.
Acceptability andsuppression of negative emotion in anxiety and
mood disorders. Emotion2006; 6:587595.
24. Conway M, Csank PR, Holm SL, Blake CK. On individual
differences inrumination on sadness. J Pers Assess 2000;
75:404425.
25. Hayes SC, Strosahl K, Wilson KG, et al. Measuring
experiential avoidance:a preliminary test of a working model.
Psychol Rec 2004; 54:553578.
26. Leahy RL. A model of emotional schemas. Cogn Behav Pract
2002; 9:177191.
27. Catanzaro SJ, Wasch HH, Kirsch I, Mearns J. Coping related
expectanciesand dispositions as prospective predictors of coping
responses and symp-toms. J Pers 2000; 68:757788.
28. Ehring T, Fischer S, Schnuelle J, et al. Characteristics of
emotion regulation inrecovered depressed versus never depressed
individuals. Pers Indiv Differ2008; 44:15741584.
29. Kassel JD, Bornovalova M, Mehta N. Generalized expectancies
for negativemood regulation predict change in anxiety and
depression among collegestudents. Behav Res Ther 2007;
45:939950.
30. Kraaij V, Pruymboom E, Garnefski N. Cognitive coping and
depressivesymptoms in the elderly: a longitudinal study. Aging Ment
Health 2002;6:275281.
31. Liverant GI, Brown TA, Barlow DH, Roemer L. Emotion
regulation in unipolardepression: the effects of acceptance and
suppression of subjective emo-tional experience on the intensity
and duration of sadness and negative affect.Behav Res Ther 2008;
46:12011209.
32.&
Ehring T, Tuschen-Caffier B, Schnuelle J, et al. Emotion
regulation andvulnerability to depression: spontaneous versus
instructed use of emotionsuppression and reappraisal. Emotion 2010;
10:563572.
This article investigates, first, the spontaneous use of the
emotion regulationstrategies of reappraisal and (arguably)
suppression of emotional expression and,second, the effects of
instructed use of these strategies in recovereddepressedindividuals
vs. healthy controls.33.&
Cisler J, Olatunji B, Feldner M, Forsyth J. Emotion regulation
and the anxietydisorders: an integrative review. J Psychopathol
Behav 2010; 32:6882.
This article works to conceptualize and present a proper
definition of emotionregulation, while also integrating relevant
findings regarding emotion regulation,anxiety disorders, and
affective neuroscience.34. Tull MT, Stipelman BA, Salters-Pedneault
K, Gratz KL. An examination of
recent nonclinical panic attacks, panic disorder, anxiety
sensitivity, andemotion regulation difficulties in the prediction
of generalized anxiety disorderin an analogue sample. J Anxiety
Disord 2009; 23:275282.
35. Mennin DS, Heimberg RG, Turk CL, Fresco DM. Preliminary
evidence for anemotion regulation deficit model of generalized
anxiety disorder. Behav ResTher 2005; 43:12811310.
36. Novick-Kline P, Turk CL, Mennin DS, et al. Level of
emotional awareness as adifferentiating variable between
individuals with and without generalizedanxiety disorder. J Anxiety
Disord 2005; 19:557572.
37. Cloitre M, Miranda R, Stovall-McClough KC, Han H. Beyond
PTSD: emotionregulation and inter-personal problems as predictors
of functional impairmentin survivors of childhood abuse. Behav Ther
2005; 36:119124.
38. Tull MT, Barrett HM, McMillan ES, Roemer L. A preliminary
investigation of therelationship between emotion regulation
difficulties and posttraumatic stresssymptoms. Behav Ther 2007;
38:303313.
39. Staiger P, Melville F, Hides L, et al. Can emotion-focused
coping helpexplain the link between posttraumatic stress disorder
severity and triggersfor substance use in young adults? J Subst
Abuse Treat 2009; 36:220226.
40. Cloitre M, Koenen KC, Cohen LR, Han H. Skills training in
affective andinterpersonal regulation followed by exposure: a
phase-based treatment forPTSD related to childhood abuse. J Consult
Clin Psych 2002; 70:10671074.
41. Baker TB, Piper ME, McCarthy DE, et al. Addiction motivation
reformulated:an affective processing model of negative
reinforcement. Psychol Rev 2004;111:3351.
42. Cooper ML, Frone MR, Russell M, Mudar P. Drinking to
regulate positive andnegative emotions: a motivational model of
alcohol use. J Pers Soc Psychol1995; 69:9901005.
43.&
Wupperman P, Marlatt GA, Cunningham A, et al. Mindfulness
andmodification therapy for behavior dysregulation: results from a
pilot studytargeting alcohol use and aggression in women. J Clin
Psychol 2011; 67:117.
This article integrates previous findings to argue for the role
of specific emotionregulation deficits in harmful dysregulated
behaviors, while also providing evidencethat severe behavioral
dysregulation can be reduced by a therapy primarilytargeting
emotion regulation skills of tolerance and acceptance.44. Falk D,
Yi H, Hilton M. Age of onset and temporal sequencing of
lifetime
DSM-IV alcohol use disorders relative to comorbid mood and
anxiety dis-orders. Drug Alcohol Depend 2008; 94:234245.ins
www.co-psychiatry.com 133
-
Behavioural medicine45. Gamble SA, Conner KR, Talbot NL, et al.
Effects of pretreatment andposttreatment depressive symptoms on
alcohol consumption following treat-ment in project MATCH. J Stud
Alcohol Drugs 2010; 71:7177.
46. Hodgins DC, El-Guebaly N, Armstrong S. Prospective and
retrospectivereports of mood states before relapse to substance
use. J Consult ClinPsych 1995; 63:400407.
47. Swendsen JD, Tennen H, Carney MA, et al. Mood and alcohol
consumption:an experience sampling test of the self-medication
hypothesis. J AbnormPsychol 2000; 109:198204.
48. Willinger U, Lenzinger E, Hornik K, et al. Anxiety as a
predictor of relapsein detoxified alcohol-dependent clients.
Alcohol Alcohol 2002; 37:609612.
49. Cooney NL, Litt MD, Morse PA, et al. Alcohol cue reactivity,
negative-moodreactivity, and relapse in treated alcoholic men. J
Abnorm Psychol 1997;106:243250.
50. Birch CD, Stewart SH, Wall A, et al. Mood-induced increases
in alcoholexpectancy strength in internally motivated drinkers.
Psychol Addict Behav2004; 18:231238.
51. Sinha R, Fox HC, Hong KA, et al. Enhanced negative emotion
and alcoholcraving, and altered physiological responses following
stress and cue ex-posure in alcohol dependent individuals.
Neuropsychopharmacology 2009;34:11981208.
52. Brown RA, Evans DM, Miller IW, et al. Cognitive-behavioral
treatment fordepression in alcoholism. J Consult Clin Psych 1997;
65:715726.
53. Watt M, Stewart S, Birch C, Bernier D. Brief CBT for high
anxiety sensitivitydecreases drinking problems, relief alcohol
outcome expectancies, andconformity drinking motives: evidence from
a randomized controlled trial. JMent Health 2006; 15:683695.
54. Fox HC, Axelrod SR, Paliwal PP, et al. Difficulties in
emotion regulation andimpulse control during cocaine abstinence.
Drug Alcohol Depend 2007;89:298301.
55. Fairburn CG, Cooper Z, Shafran R. Cognitive behaviour
therapy for eatingdisorders: a transdiagnostic theory and
treatment. Behav Res Ther 2003;41:509528.
56. Penas-Lledo E, Vaz Leal FJ, Waller G. Excessive exercise in
anorexia nervosaand bulimia nervosa: relation to eating
characteristics and general psycho-pathology. Int J Eat Disorder
2002; 31:370375.
57. Smyth JM, Wonderlich SA, Heron KE, et al. Daily and
momentary mood andstress are associated with binge eating and
vomiting in bulimia nervosapatients in the natural environment. J
Consult Clin Psych 2007; 75:629638.
58. Wild B, Eichler M, Feiler S, et al. Dynamic analysis of
electronic diary data ofobese patients with and without binge
eating disorder. Psychother Psycho-som 2007; 76:250252.
59. Crosby RD, Wonderlich SA, Engel SG, et al. Daily mood
patterns andbulimic behaviors in the natural environment. Behav Res
Ther 2009;47:181188.
60. Smyth JM, Wonderlich SA, Sliwinski MJ, et al. Ecological
momentary assess-ment of affect, stress, and bingepurge behaviors:
day of week and time of dayeffects in the natural environment. Int
J Eat Disorder 2009; 42:429436.
61. Chua JL, Touyz S, Hill AJ. Negative mood-induced overeating
in obese bingeeaters: an experimental study. Int J Obes Relat Metab
Disord 2004; 28:606610.
62. Hilbert A, Tuschen-Caffier B. Maintenance of binge eating
through negativemood: a naturalistic comparison of binge eating
disorder and bulimia nervosa.Int J Eat Disorder 2007;
40:521530.
63. Stein RI, Kenardy J, Wiseman CV, et al. Whats driving the
binge in bingeeating disorder: a prospective examination of
precursors and consequences?Int J Eat Disorder 2007; 40:195203.
64. Bydlowski S, Corcos M, Jeammet P, et al. Emotion-processing
deficits ineating disorders. Int J Eat Disorder 2005;
37:321329.
65. Carano A, De Berardis D, Gambi F, et al. Alexithymia and
body image in adultoutpatients with binge eating disorder. Int J
Eat Disorder 2006; 39:332340.
66.&
Svaldi J, Caffier D, Tuschen-Caffier B. Emotion suppression but
not reapprai-sal increases desire to binge in women with binge
eating disorder. PsychotherPsychosom 2010; 79:188190.
This article uses an experimental design to clarify the causal
impact of putativeemotion regulation strategies on core symptoms of
BED.67. Corstorphine E, Mountford V, Tomlinson S, et al. Distress
tolerance in the
eating disorders. Eat Behav 2007; 8:9197.68. Sim L, Zeman J.
Emotion regulation factors as mediators between body
dissatisfaction and bulimic symptoms in early adolescent girls.
J Early Adolesc2005; 25:478496.134 www.co-psychiatry.com69. Gratz
K, Roemer L. Multidimensional assessment of emotion regulation
anddysregulation: development, factor structure, and initial
validation of thedifficulties in emotion regulation scale. J
Psychopathol Behav 2004;26:4154.
70. Whiteside U, Chen E, Neighbors C, et al. Difficulties
regulating emotions: dobinge eaters have fewer strategies to
modulate and tolerate negative affect?Eat Behav 2007; 8:162169.
71. Harrison A, Sullivan S, Tchanturia K, Treasure J. Emotion
recognition andregulation in anorexia nervosa. Clin Psychol Psychot
2009; 16:348356.
72. Nemiah JC, Sifneos PE. Psychosomatic illness: a problem in
communication.Psychother Psychosom 1970; 18:154160.
73. Taylor GJ, Bagby RM, Parker JDA. Disorders of affect
regulation: alexithymia inmedical and psychiatric illness. New
York, New York: Cambridge UniversityPress; 1997.
74. De Gucht V, Heiser W. Alexithymia and somatisation: a
quantitative review ofthe literature. J Psychosom Res J 2003;
54:425434.
75. Lumley MA, Stettner L, Wehmer F. How are alexithymia and
physical illnesslinked? A review and critique of pathways. J
Psychosom Res 1996; 41:505518.
76.&
Subic-Wrana C, Beutel ME, Knebel A, Lane RD. Theory of mind and
emotionalawareness deficits in patients with somatoform disorders.
Psychosom Med2010; 72:404411.
This article includes one of the rare exceptions of studies
using measures otherthan self-reports when assessing emotional
awareness in somatoform disorders.Moreover, it addresses
alexithymia in the context of deficits in theory of mind
insomatoform symptoms.77. Subic-Wrana C, Bruder S, Thomas W, et al.
Distribution of alexithymia as a
personality-trait in psychosomatically ill in-patients: measured
with TAS-20and LEAS. Psychother Psychosom Med Psychol 2002;
52:454460.
78. Subic-Wrana C, Bruder S, Thomas W, et al. Emotional
awareness deficits ininpatients of a psychosomatic ward: a
comparison of two different measuresof alexithymia. Psychosom Med
2005; 67:483489.
79. Waller E, Scheidt CE. Somatoform disorders as disorders of
affect regulation:a study comparing the TAS-20 with nonself-report
measures of alexithymia.J Psychosom Res 2004; 57:239247.
80. Waller E, Scheidt CE. Somatoform disorders as disorders of
affect regulation:a development perspective. Int Rev Psychiatr
2006; 18:1324.
81.&
Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation
strategiesacross psychopathology: a meta-analytic review. Clin
Psychol Rev 2010;30:217237.
This article provides an informative meta-analytic review of
emotion regulation as atransdiagnostic construct. It also serves as
an example of the all-too-commonpractice of subsuming various
mental processes formerly investigated asscientific constructs in
their own right under the concept of emotion regulation.82. Aldao
A, Nolen-Hoeksema S. When are adaptive strategies most predictive
of
psychopathology? J Abnorm Psychol 2011. [Epub ahead of print]83.
Gross JJ, John OP. Individual differences in two emotion regulation
pro-
cesses: implications for affect, relationships, and well being.
J Pers SocPsychol 2003; 85:348362.
84. Koole S. The psychology of emotion regulation: an
integrative review. CognEmotion 2009; 23:441.
85. Spielberger CD, Gorsuch RL, Lushene RE. Manual for the
State-Trait AnxietyInventory. Palo Alto, California: Consulting
Psychologists Press; 1970.
86. Lane RD, Sechrest L, Riedel R. Sociodemographic correlates
of alexithymia.Compr Psychiatry 1998; 39:377385.
87. Ebert D, Christ O, Berking M. Development and validation of
a self-reportinstrument for the assessment of emotion-specific
regulation skills. Diagnos-tica (in press).
88. Solbakken O, Hansen R, Havik OE, Monsen JT. Assessment of
affectintegration: validation of the affect consciousness
construct. J Pers Assess2011; 93:257265.
89. Berking M, Orth U, Wupperman P, et al. Prospective effects
of emotionregulation on emotional adjustment. J Couns Psychol 2008;
55:485494.
90.&
Berking M, Poppe C, Luhmann M, et al. Emotion-regulation skills
andpsychopathology: is the ability to modify emotions the pathway
by whichall other skills affect mental health? J Behav Ther Exp Psy
(in press).
This study represents a first step toward investigating the
methods by whichdifferent emotion regulation processes interact
when affecting mental health.91. Berking M, Wupperman P, Reichardt
A, et al. Emotion-regulation skills as a
treatment target in psychotherapy. Behav Res Ther 2008;
46:12301237.92. Ablon JS, Jones EE. Validity of controlled clinical
trials of psychotherapy:
findings from the NIMH Treatment of Depression Collaborative
ResearchProgram. Am J Psychiatry 2002; 159:775783.Volume 25 Number
2 March 2012