Embed Size (px)
Citation preview

Best Practices and Promising Agents in Pancreatic Cancer
This program is supported by educational grants from Celgene Corporation and Incyte.

About These Slides
� Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
� These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.

Core Faculty
Tanios S. Bekaii-Saab, MDCo-Leader, GI Cancer Program
Mayo Clinic Cancer CenterProfessor of MedicineDivision of Hematology and OncologyMayo Clinic
Phoenix, Arizona
Andrew H. Ko, MDProfessor
Division of Hematology/OncologyDepartment of MedicineUniversity of California, San FranciscoSan Francisco, California

Agenda
� Diagnosis and Staging Considerations
� Current Therapeutic Options for Metastatic Pancreatic Cancer
� Second-line Agents for Pancreatic Cancer
� Emerging Agents for Pancreatic Cancer
� Other Signaling Pathway Targets in Pancreatic Cancer
Diagnosis and Staging Considerations

Pancreatic Cancer: Scope of the Problem
� Projected 53,070 new cases of pancreatic cancer in US pts with 41,780 deaths in 2016
� Stage for stage, pancreatic cancer is associated with the lowest survival rates of any major cancer type
� Within the decade, pancreatic cancer is expected to rise to the second leading cause of cancer-related mortality in the United States (behind lung cancer)
� The vast majority of pts (80% to 85%) are inoperable at time of diagnosis
Slide credit: clinicaloptions.comSiegel RS, et al. Cancer facts & figures 2016.

Stage Classification* % at Diagnosis
5-Yr Survival, %
Localized/resectable
9 26
Localized/unresectable
28 10
Metastatic 53 2
Siegel R, et al. CA Cancer J Clin. 2015;65:5-29.
Pancreatic Cancer by Stage (SEER Database)
*Unknown: 10%; 5-yr survival 4.4%
Slide credit: clinicaloptions.com

Screening for Pancreatic Cancer: Screening for Pancreatic Cancer: Identifying HighIdentifying High --Risk IndividualsRisk Individuals
Demographic Factors Advancing Age, Male, Black, Ashkenazi Jewish Ancest ry
Known genetic syndromes � Lynch syndrome (HNPCC)� Familial breast cancer (BRCA2)
� Peutz-Jeghers� Ataxia-telangiectasia
� Familial atypical multiple mole-melanoma� Hereditary pancreatitis
Family history As number of first-degree relatives increases (1 → 2 → 3+), risk increases by 4.6→ 6.4→ 32.0 fold
Host/environmental factors � Diabetes mellitus (T2DM)• Meta-analysis: odds ratio = 1.82
• Need to distinguish T2DM as early symptom of pancreatic cancer vs an independent risk factor
� Chronic pancreatitis� Tobacco use
� Obesity
Slide credit: clinicaloptions.com
American Cancer Society. www.cancer.org. 2016.Adapted with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Pancreatic Adenocarcinoma. V.1.2016. © 2016 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of the NCCN. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc.

Current TherapeuticOptions for Metastatic
Pancreatic Cancer

Guidelines for Chemotherapy for Pts With Metastatic Pancreatic Adenocarcinoma
First-line Treatment
Category 1 NCCN Regimens
Other NCCN Regimens
Good performance
status
� FOLFIRINOX (preferred)� Gem + nab-paclitaxel
(preferred)� Gem + erlotinib
Category 2A�Gem + cape�Gem + cisplatin
Category 2B�GTX�FP + Ox
Poor performance status
� Gem monotherapyCategory 2B
�FDR gem�Cape or continuous infusion 5-FU
Adapted with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Pancreatic Adenocarcinoma. V.1.2016. © 2016 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of the NCCN. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc.
Clinical trial is the recommended first option for all pts.
Slide credit: clinicaloptions.com

Phase III Study: FOLFIRINOX vs Gemcitabine in Met Pancreatic Cancer
Pts with untreated metastatic pancreatic
cancer; ECOG PS 0/1; adequate BM, platelet count, liver and renal
function(N = 342)
Gemcitabine 1000 mg/m 2
weekly x 7 of 8, then weekly x 3 of 4
(n = 171)
FOLFIRINOXOxaliplatin 85 mg/m 2 +
LV 400 mg/m 2 +Irinotecan 180 mg/m 2 +
5-FU bolus 400 mg/m 2, then 2400 mg/m 2 IV over 46 hrs
(n = 171)
Stratified by ECOG PS (0 vs 1), center,tumor location (head vs other)
Conroy T, et al. N Engl J Med. 2011;364:1817-1825. Slide credit: clinicaloptions.com

FOLFIRINOX vs Gemcitabine: Baseline Characteristics (ITT)
Characteristic FOLFIRINOX (n = 171) Gemcitabine (n = 171)
Median age, yrs (range) 61 (25-76) 61 (34-75)
Male, n (%) 106 (62.0) 105 (61.4)
ECOG PS, n (%)
� 0 64 (37.4) 66 (38.6)
� 1 106 (61.9) 105 (61.4)
Pancreatic tumor location, n (%)
� Head 67 (39.2) 63 (36.8)
� Body 53 (31.0) 58 (33.9)
� Tail 45 (26.3) 45 (26.3)
Biliary stent, n (%)
� No 144 (84.2) 149 (87.1)
Conroy T, et al. N Engl J Med. 2011;364:1817-1825. Slide credit: clinicaloptions.com

FOLFIRINOX vs Gemcitabine: OS and PFS
100
75
50
00 3 6 9 12 15 1821 24 27 42
Mos
OS
(%
)
25
39363330
Median OS: 11.1 vs 6.8 mosHR: 0.57 (95% CI: 0.45-0.73; P < .001)
100
75
50
00 3 6 9 12 15 18 21 36
MosP
FS
(%
)
25
33302724
Median PFS: 6.4 vs 3.3 mos HR: 0.47 (95% CI: 0.37-0.59; P < .001)
Conroy T, et al. N Engl J Med. 2011;364:1817-1825.
GemcitabineFOLFIRINOX
GemcitabineFOLFIRINOX
OS PFS
Slide credit: clinicaloptions.com
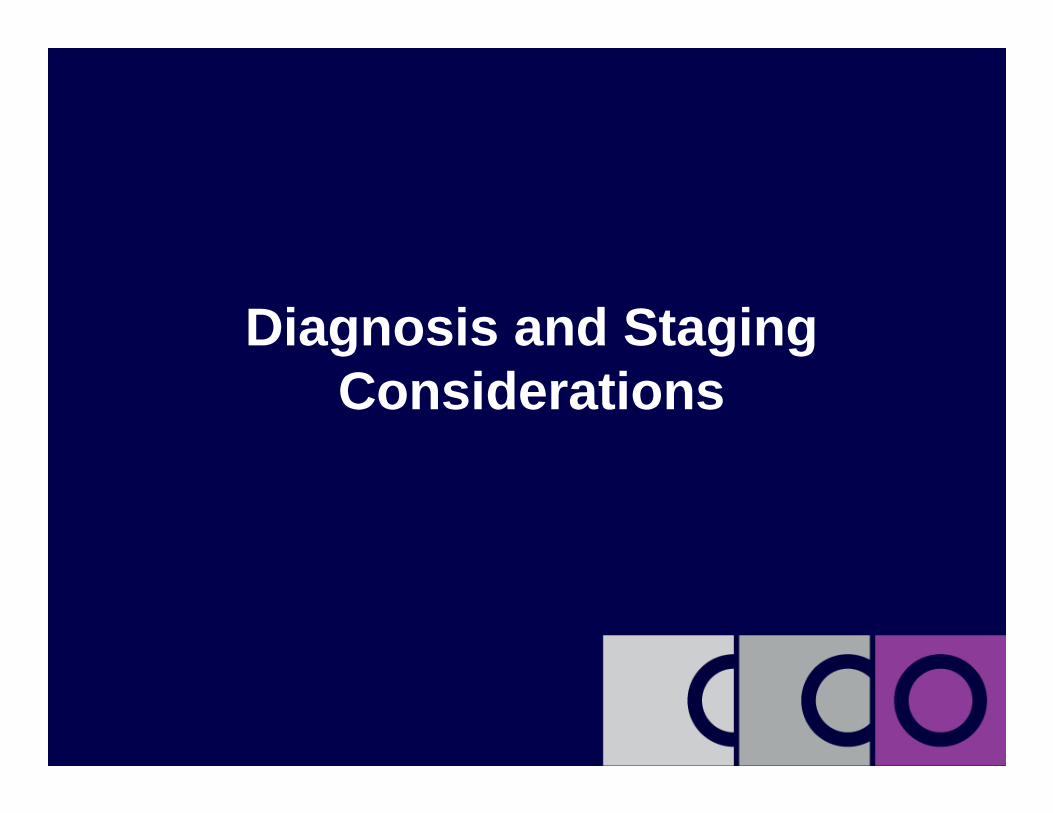
FOLFIRINOX vs Gemcitabine: Efficacy
Outcome FOLFIRINOX (n = 171)
Gemcitabine (n = 171)
HR(95% CI)
ORR,* % 31.6 9.4
Median PFS, mos 6.4 3.3 0.47 (0.37-0.59)P < .001
Median OS, mos 11.1 6.8 0.57 (0.45-0.73)P < .001
1-yr survival, % 48.4 20.6
Conroy T, et al. N Engl J Med. 2011;364:1817-1825. Slide credit: clinicaloptions.com
*RR, FOLFIRINOX vs gemcitabine: CR, 0.6% vs 0%, PR, 31.0% vs 9.4%.

FOLFIRINOX vs Gemcitabine: AEs
Grade 3/4 AE, % FOLFIRINOX (n = 171)
Gemcitabine (n = 171)
P Value
Hematologic
� Neutropenia 45.7 21.0 < .001
� Febrile neutropenia 5.4 1.2 .03
� Thrombocytopenia 9.1 3.6 .04
Nonhematologic
� Fatigue 23.6 17.8 NS
� Vomiting 14.5 8.3 NS
� Diarrhea 12.7 1.8 < .001
� Sensory neuropathy 9.0 0.0 < .001
� Elevated ALT 7.3 20.8 < .001
Conroy T, et al. N Engl J Med. 2011;364:1817-1825. Slide credit: clinicaloptions.com

Management of AEs: Irinotecan
� Diarrhea: early diarrhea usually transient, treat with atropine;late diarrhea (≥ 24 hrs after injection) may be life threatening, treat promptly with loperamide, fluids, and electrolytes
– Delay chemotherapy until pretreatment bowel ≥ 24 hrs without need for antidiarrhea medication; if grades 2-4 late diarrhea occurs, treat and decrease subsequent doses in current cycle
� Neutropenia: manage complications promptly with antibiotics
– Omit irinotecan during a cycle if neutropenic fever occurs or if ANC < 1500/mm3; after pt recovers to ANC ≥ 1500/mm3, subsequent doses should be reduced depending on the level of neutropenia observed
– Growth factor prophylaxis should be used with FOLFIRINOX
Irinotecan [package insert]. 2014. Slide credit: clinicaloptions.com

Management of AEs: Oxaliplatin
� Peripheral neuropathy: reduce dose if persistent grade 2 neurosensory events do not resolve; consider discontinuing oxaliplatin if persistent grade 3 neurosensory events
� GI AEs: delay treatment and reduce dose after recovery from grade 3/4 GI toxicities
� Neutropenia: delay until neutrophils ≥ 1.5 × 109/L after grade 4 neutropenia or febrile neutropenia and reduce next dose
� Growth factor prophylaxis should be used with FOLFIRINOX
� Thrombocytopenia: delay until platelets ≥ 75 × 109/L after grade 3/4 thrombocytopenia and reduce next dose
Oxaliplatin [package insert]. 2015. Slide credit: clinicaloptions.com

FOLFIRINOX vs Gemcitabine: Quality of Life
� Time until definitive deterioration > 20 points, EORTC-C30 global health status/QoL questionnaire
� Prolongation of QoL in pts treated with FOLFIRINOX compared with gemcitabine, despite greater toxicity
� Specifically, longer time to deterioration in:
– Global health status
– Physical, cognitive, and social functioning
– Symptoms such as fatigue, N/V, pain, and anorexia
Gourgou-Bourgade S, et al. J Clin Oncol. 2013;31:23-29 Slide credit: clinicaloptions.com
1.0
0.8
0.6
0.4
0.2
00 3 6 9 12
GemcitabineFOLFIRINOX
P < .001
Mos
Det
erio
ratio
n (P
roba
bilit
y)

MPACT: Phase III Gemcitabine ± Nab -Paclitaxel in Metastatic Pancreatic Cancer
� Primary endpoint: OS
� Secondary endpoints: PFS, ORR, safety
Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703.
Pts with metastatic pancreatic cancer, no previous treatment for
metastatic disease, KPS ≥ 70, bilirubin
≤ ULN(N = 861)
Gemcitabine 1000 mg/m 2/wk IV +Nab-Paclitaxel 125 mg/m 2/wk IV
for 7 wks, and then on Days 1, 8, 15 Q4W(n = 431)
Gemcitabine 1000 mg/m 2/wk IV for 7 wks, and then on Days 1, 8, 15 Q4W
(n = 430)
Treat until PD
Stratified by KPS, region, liver metastasis
Slide credit: clinicaloptions.com

MPACT: Gemcitabine ± Nab -Paclitaxel in Metastatic Pancreatic Cancer—OS
Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703.
Gem + Nab-P
(n = 431)
Gem (n = 430)
HR (95% CI)
Median OS, mos
8.5 6.7 0.72 (0.62-0.83)P < .001
Slide credit: clinicaloptions.com
100
80
60
40
20
00 393 6 9 12 15 18 21 24 27 30 33 36
Gemcitabine + nab-paclitaxelGemcitabine
Mos
OS
(%
)

MPACT: Gemcitabine ± Nab -Paclitaxel in Metastatic Pancreatic Cancer—PFS*
Gem + Nab-P
(n = 431)
Gem (n = 430)
HR (95% CI)
Median PFS, Mos
5.5 3.7 0.69 (0.58-0.82)P < .001
Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703.
Mos
PF
S (
%)
Gemcitabine + nab-paclitaxelGemcitabine
1.0
0.8
0.6
0.4
0.2
00 3 6 9 12 15 18 21 24
*Based on independent review.
Slide credit: clinicaloptions.com

MPACT: Gemcitabine ± Nab -Paclitaxel in Metastatic Pancreatic Cancer: Efficacy
Outcome Gem + Nab-P(n = 431)
Gemcitabine (n = 430)
HR(95% CI)
ORR, % 23 7 P < .001
Median PFS, mos 5.5 3.7 0.69 (0.58-0.82)P < .001
Median OS, mos 8.5 6.7 0.72 (0.62-0.83)P < .001
1-yr survival, % 35 22
Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703. Slide credit: clinicaloptions.com
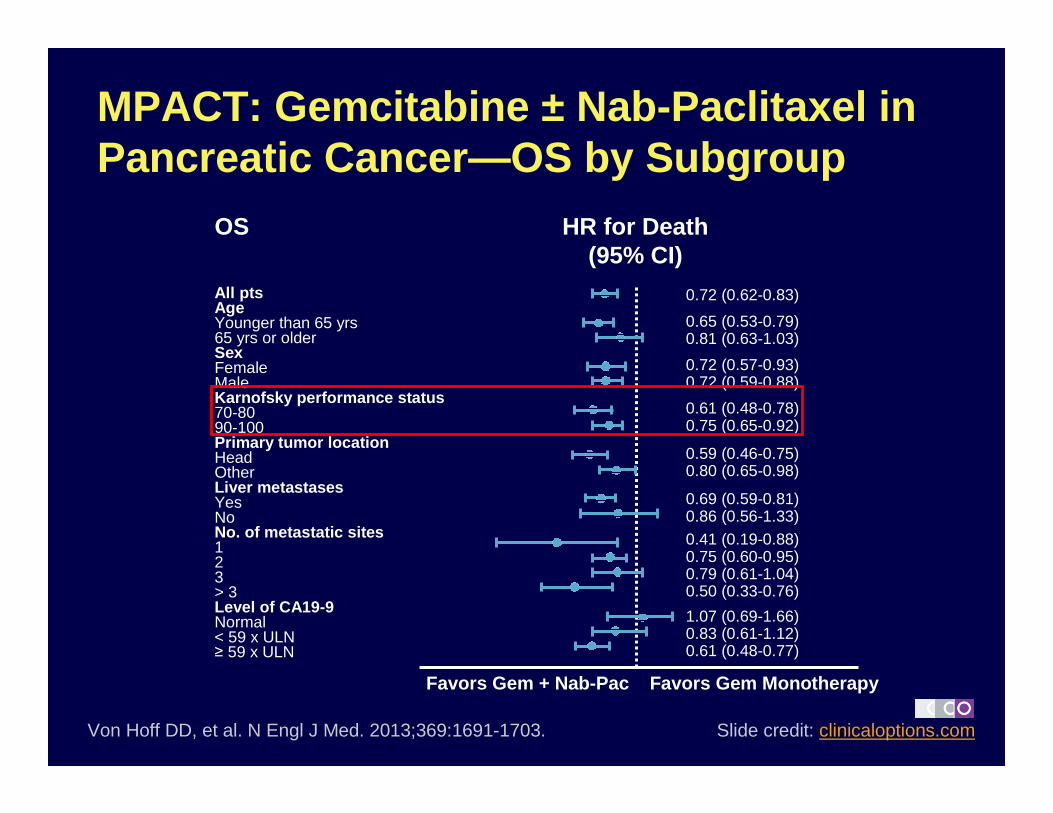
MPACT: Gemcitabine ± Nab -Paclitaxel in Pancreatic Cancer—OS by Subgroup
Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703.
Favors Gem + Nab-Pac Favors Gem Monotherapy
Slide credit: clinicaloptions.com
OS HR for Death (95% CI)
0.72 (0.62-0.83)
0.65 (0.53-0.79)0.81 (0.63-1.03)
0.72 (0.57-0.93)0.72 (0.59-0.88)
0.61 (0.48-0.78)0.75 (0.65-0.92)
0.59 (0.46-0.75)0.80 (0.65-0.98)
0.69 (0.59-0.81)0.86 (0.56-1.33)0.41 (0.19-0.88)0.75 (0.60-0.95)0.79 (0.61-1.04)0.50 (0.33-0.76)
1.07 (0.69-1.66)0.83 (0.61-1.12)0.61 (0.48-0.77)
All ptsAgeYounger than 65 yrs65 yrs or olderSexFemaleMaleKarnofsky performance status70-8090-100Primary tumor locationHeadOtherLiver metastasesYesNoNo. of metastatic sites123> 3Level of CA19-9Normal< 59 x ULN≥ 59 x ULN

MPACT: Gemcitabine ± Nab -Paclitaxel in Pancreatic Cancer—AEs
Event, % Gem + Nab-P(n = 421)
Gem Only(n = 402)
AE leading to death 4 4
Hematolgic AEs grade ≥ 3
� Neutropenia 38 27
� Leukopenia 31 16
� Thrombocytopenia 13 9
� Anemia 13 12
Receipt of growth factors 26 15
Febrile neutropenia 3 1
Nonhematologic AEs grade ≥ 3*
� Fatigue 17 7
� Peripheral neuropathy 17 1
� Diarrhea 6 1
*≥ 5% of pts.Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703. Slide credit: clinicaloptions.com

Frontline Regimens for Pts With Metastatic Pancreatic Cancer
FOLFIRINOX vs Gem(N = 342)[1]
Nab-Pac + Gem vs Gem(N = 861)[2]
Median age, yrs (range) 61 (25-76) 62 (27-86)
Male, % 62 57
Region (NA/WE/EE/A), % 0/100 (France)/0/0 62/9/15/14
ECOG PS/KPS(0/100, 1/80-90, 2/60-70), %
37/62/1 16/76/8
Pan tumor location (H/B/T), % 39/31/26 43/31/25
Median involved metastatic sites, n 2 2.5
ORR, % 32 vs 9 23 vs 7
Disease control rate, % 70 vs 51 48 vs 33
Median PFS, mos 6.4 vs 3.3 5.5 vs 3.7
Median OS, mos 11.1 vs 6.8 8.5 vs 6.7
1. Conroy T, et al. N Engl J Med. 2011;364:1817-1825.2. Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703. Slide credit: clinicaloptions.com

First-line FOLFIRINOX vs Gemcitabine -Based Tx: OS (Retrospective Analysis)
� EMR data from US Oncology Network June 2010 to November 2013
� Dosing based on standard doses in US Oncology system
First-line Treatment N Median OS, Mos
FOLFIRINOX 666 11
Gem only or gem + other chemotherapy*
1567 7
Gem + nab-paclitaxel 189 10
Cartwright T, et al. ASCO 2014. Abstract 4132.
OS
(%
) *Gem only, n = 1141.
Slide credit: clinicaloptions.com
1.0
0.8
0.6
0.4
0.2
00 10 20 30 40 50
Mos
P < .0001
FOLFIRINOXGem-based therapyGem + nab-paclitaxel
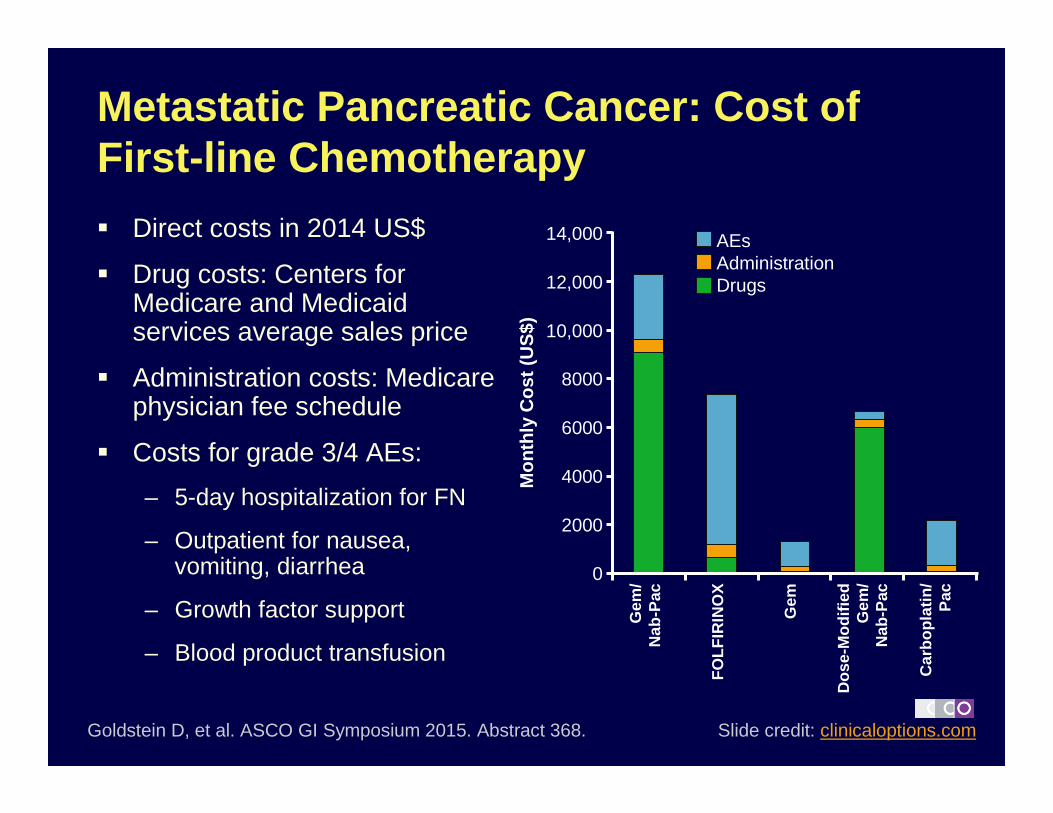
Metastatic Pancreatic Cancer: Cost of First-line Chemotherapy
� Direct costs in 2014 US$
� Drug costs: Centers for Medicare and Medicaid services average sales price
� Administration costs: Medicare physician fee schedule
� Costs for grade 3/4 AEs:
– 5-day hospitalization for FN
– Outpatient for nausea, vomiting, diarrhea
– Growth factor support
– Blood product transfusion
Goldstein D, et al. ASCO GI Symposium 2015. Abstract 368.
14,000
12,000
10,000
8000
6000
4000
2000
0
Mon
thly
Cos
t (U
S$)
Gem
/N
ab-P
ac
FO
LFIR
INO
X
Gem
Dos
e-M
odifi
edG
em/
Nab
-Pac
Car
bopl
atin
/P
ac
AEs AdministrationDrugs
Slide credit: clinicaloptions.com

Second -line Agents for Pancreatic Cancer

Novel Formulation: Nanoliposomal Irinotecan (MM -398)
� Nanoliposomal irinotecan
– Irinotecan: topoisomerase I inhibitor
– Liposomal formulation associated with preferentially increased tumor exposure to irinotecan
– Longer half-life, increased AUC, slower clearance, reduced volume of distribution vs free drug
– FDA approved October 2015 in combination with 5-FU and leucovorin for the treatment of pts with metastatic adenocarcinoma of the pancreas whose disease has progressed following gemcitabine-based therapy
Roy AC, et al. Ann Oncol. 2013;24:1567-1573.Drummond DC, et al. Cancer Res. 2006;66:3271-3277. Slide credit: clinicaloptions.com

NAPOLI-1: Nanoliposomal Irinotecan ±5-FU/LV vs 5 -FU/LV
� Phase III trial
Wang-Gillam A, et al. Lancet. 2016;387:545-557.
Nal-IRI 120 mg/m 2 Q3W(n = 151)
5-FU/LV2000/200 mg/m 2/wk x 4 Q6W
(n = 119)
*Combination arm added after safety data were available. Pts in 5-FU/LV arm used as controls for combination arm.
Nal-IRI 80 mg/m 2 + 5-FU/LV* 2400/400 mg/m 2 Q2W
(n = 117)
Pts with metastatic pancreatic cancer who
progressed on gemcitabine-
based therapy, KPS ≥ 70(N = 417)
Slide credit: clinicaloptions.com

NAPOLI-1: Nanoliposomal Irinotecan ±5-FU/LV vs 5 -FU/LV—Results
Tumor Response and Control
Nal-IRI + 5-FU/LV (n = 117)
5-FU/LV (n = 119)
Median PFS, mos(95% CI)
3.1(2.7-4.2)
1.5(1.4-1.8)
P = .0001
ORR, %(95% CI)
16(9.6-22.9)
1(0-2.5)
P < .001
CA19-9 reduction, % 36 12
P = .0009
Wang-Gillam A, et al. Lancet. 2016;387:545-557. Slide credit: clinicaloptions.com
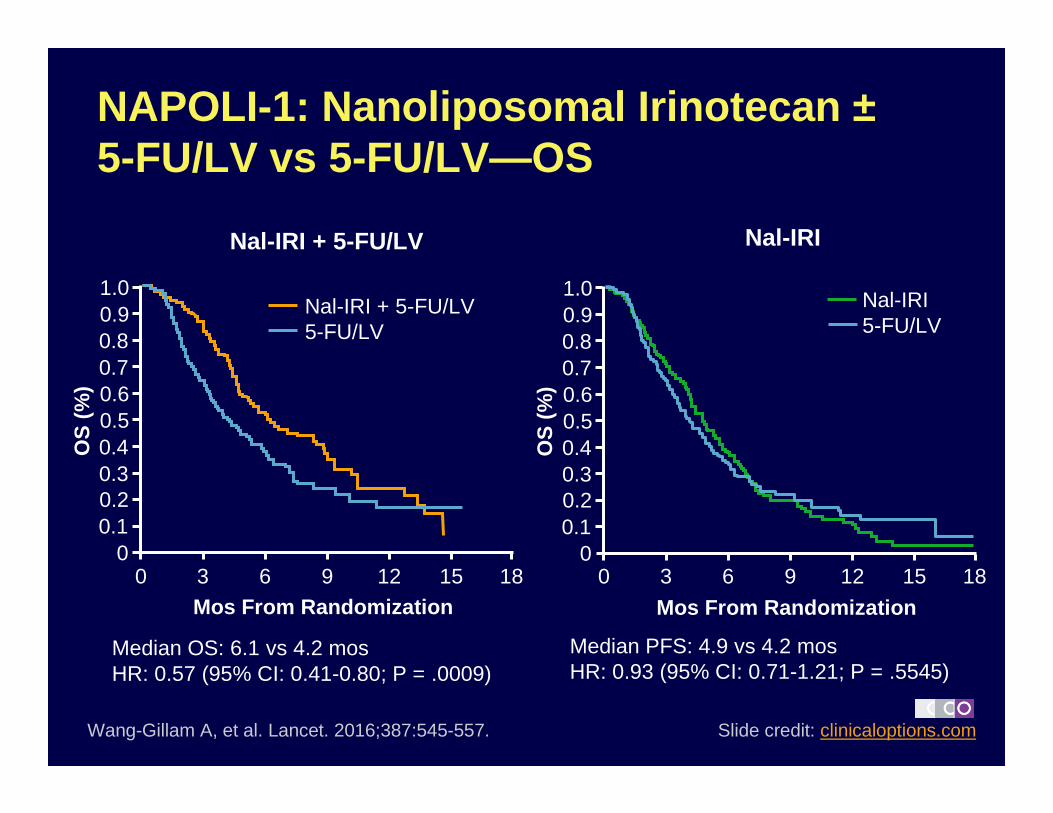
NAPOLI-1: Nanoliposomal Irinotecan ±5-FU/LV vs 5 -FU/LV—OS
1.00.90.80.70.60.50.40.30.20.1
0
OS
(%
)
0 3 6 9 12 15 18Mos From Randomization
Nal-IRI + 5-FU/LV5-FU/LV
1.00.90.80.70.60.50.40.30.20.1
0O
S (
%)
0 3 6 9 12 15 18
Mos From Randomization
Nal-IRI5-FU/LV
Nal-IRI + 5-FU/LV Nal-IRI
Wang-Gillam A, et al. Lancet. 2016;387:545-557.
Median OS: 6.1 vs 4.2 mos HR: 0.57 (95% CI: 0.41-0.80; P = .0009)
Median PFS: 4.9 vs 4.2 mos HR: 0.93 (95% CI: 0.71-1.21; P = .5545)
Slide credit: clinicaloptions.com
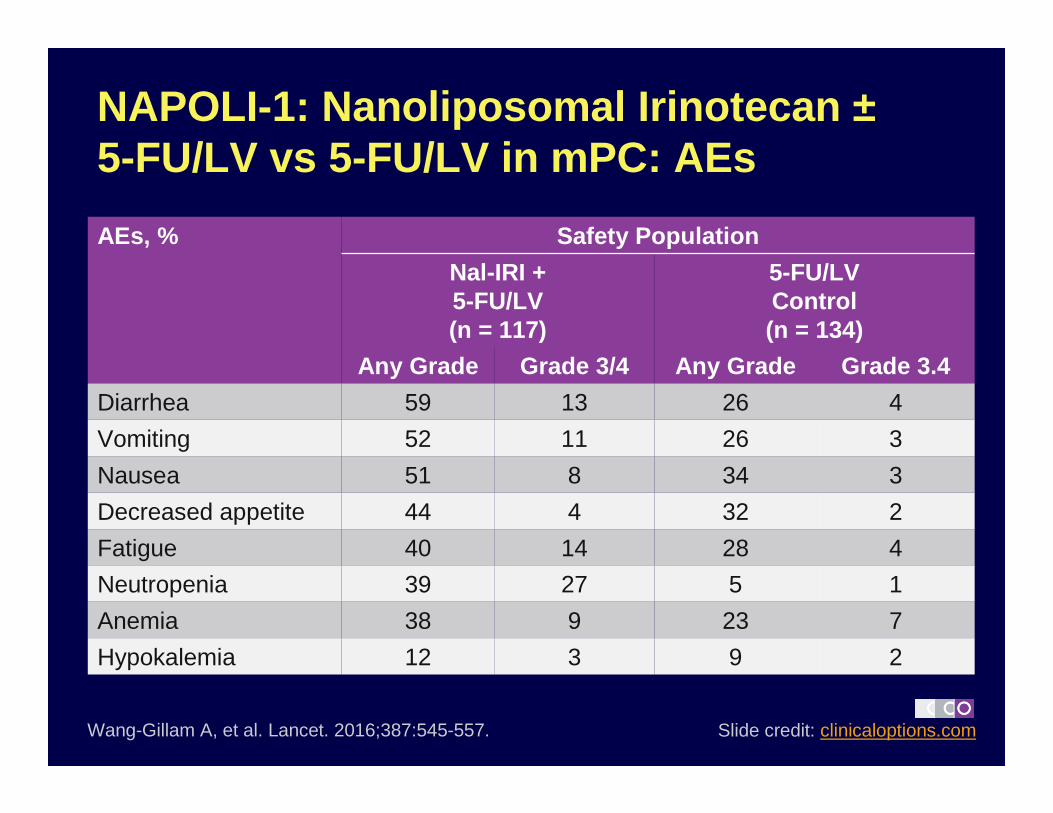
Wang-Gillam A, et al. Lancet. 2016;387:545-557.
AEs, % Safety Population
Nal-IRI + 5-FU/LV(n = 117)
5-FU/LVControl(n = 134)
Any Grade Grade 3/4 Any Grade Grade 3.4
Diarrhea 59 13 26 4
Vomiting 52 11 26 3
Nausea 51 8 34 3
Decreased appetite 44 4 32 2
Fatigue 40 14 28 4
Neutropenia 39 27 5 1
Anemia 38 9 23 7
Hypokalemia 12 3 9 2
NAPOLI-1: Nanoliposomal Irinotecan ±5-FU/LV vs 5 -FU/LV in mPC: AEs
Slide credit: clinicaloptions.com

Phase III Experience: Second -line Chemotherapy With Oxaliplatin
CONKO-003 [1] PANCREOX[2]
Pts (N = 268) PD on gem tx (n = 160) Previous gem tx (n = 108)
Treatment OFF 5-FU/LV mFOLFOX6 5-FU/LV
(n = 76) (n = 84) (n = 54) (n = 54)
OS, median 5.9 mos 3.3 mos 6.1 mos 9.9 mos
HR: 0.66 (95% CI: 0.48-0.91)P = .01
HR: 1.78 (95% CI: 1.08-2.93) P = .02
PFS, median 2.9 mos 2.0 mos 3.1 mos 2.9 mos
HR: 0.68 (95% CI: 0.50-0.94)P = .02
HR: 1.00 (95% CI: 0.66-1.53) P = .99
ORR, median NR 13.2% 8.5%
P = .36
1. Oettle H, et al. J Clin Oncol. 2014;32:2423-2429. 2. Gill S, et al. ASCO 2014. Abstract 4022. Slide credit: clinicaloptions.com

Current Treatment Sequencing for Metastatic Pancreatic Cancer
Slide credit: clinicaloptions.com
NCCN Category 1 recommended therapies in bold.
NCCN. Pancreatic adenocarcinoma. v1.2016.
FOLFIRINOX; fluoropyrimidine-based therapy
+ oxaliplatin
(PS 0/1): Gemcitabine-based (eg, gem/nab-paclitaxel,
gemcitabine)(PS 2 or less): Gemcitabine
monotherapy or BSC
??
Gemcitabine based (eg, gem/nab-paclitaxel,
gem/erlotinib )(Poor PS) Gemcitabine
(PS 0/1): Nanoliposomal irinotecan + 5-FU ;
fluoropyrimidine-based therapy(PS 2) Fluoropyrimidine alone
or BSC
(PS 0/1): Platinum-(??) based regimen if no prior exposure or
BSC
Firs
t Li
neS
econ
d Li
neT
hird
line

Emerging Agents for Pancreatic Cancer

Investigational Agents for Advanced Pancreatic Cancer
Class Examples
Novel cytotoxics� TH-302 (evofosfamide, hypoxia-activated
mustard) did not improve OS in pancreatic trial (2015)—Negative
Stromal-depleting agents� PEGPH20 (recombinant hyaluronidase)
� Vitamin D analogues� Necuparanib
Signal transduction inhibitors
� JAK inhibitors (ruxolitinib) —Negative� MM-141 (bispecific anti-IGFR/HER3 antibody)
� BTK inhibitors (ibrutinib)� Notch inhibitors (eg, demcizumab, tarextumab)—
Negative� PARP inhibitors (eg, olaparib)
Slide credit: clinicaloptions.comClinicalTrials.gov.

Investigational Immunotherapies for Advanced Pancreatic Cancer
Category Agent(s)
Vaccines � CRS-207 (mesothelin-expressing Listeria)—Negative in ECLIPSE trial combined with GVAX
� GVAX� Algenpantucel-L (‘Hyperacute’ vaccine)� Reolysin—Negative
Immune checkpoint inhibitors
� Anti–PD-1 and anti–PD-L1 antibodies (eg, PD-1 nivolumab, pembrolizumab; PD-L1, atezolizumab)� Anti–CTLA-4 antibodies (eg, tremelimumab)
� IDO inhibitors (eg, indoximod)
Anti-CD40 MAbs � Multiple agents
CCR2 inhibitors � PF-04136309
Slide credit: clinicaloptions.comClinicalTrials.gov.

Slide credit: clinicaloptions.com
Stromal-Depleting Therapies: Do They Impede Drug Delivery?
Courtesy of E. Collisson.
Stromal-Targeted Agents
� Hedgehog inhibitors[1]
� Recombinant human hyaluronidase: PEGylated-rHuPH20[2]
� Anti-CD40 monoclonal antibodies[3]
� Vitamin D analogues[4]
1. Olive KP, et al. Science. 2009;324:1457-1461.2. Provenzano PP, et al. Cancer Cell. 2012;21:418-429.3. Beatty GL, et al. Science. 2011;331:1612-1616.4. Sherman MH, et al. Cell. 2014;159:80-93. Slide credit: clinicaloptions.com

Phase II HALO -109-202: Addition of PEGPH20 to Gem/Nab -P in Metastatic PC
� Primary endpoint: PFS
� Secondary endpoints: ORR, OS, safety, PK
Pts with stage IV pancreatic cancer,
no prior tx for metastatic disease,
KPS ≥ 70%(planned N = 279)
Gemcitabine 1000 mg/m 2 +Nab-Paclitaxel 125 mg/m 2
1x/wk for 3/4 wks/cycle
PEGPH20 3 µg/kg IV 2x/wk in cycle 1 then weekly +Gemcitabine 1000 mg/m 2 +Nab-Paclitaxel 125 mg/m 2
1x/wk for 3/4 wks/cycle
Slide credit: clinicaloptions.comClinicalTrials.gov. NCT01839487.
Treat until progression, intolerable
toxicity, death, or choice to
discontinue

Phase II HALO -109-202: Results
Population, % (Responders/Total)
Gemcitabine +Nab-Paclitaxel +
PEGPH20
Gemcitabine + Nab-Paclitaxel
P Value
Total 41 (30/74) 34 (21/61) .48
HA-high 52 (12/23) 24 (5/21) .04
HA-low 37 (14/38) 38 (9/24) .96
Hingorani SR, et al. ASCO 2015. Abstract 4006.
Higher rate of thromboembolic events on PEGPH20-containing arm during first stage of enrollment (42 vs 25%); mitigated during second stage with addition of
prophylactic enoxaparin
Slide credit: clinicaloptions.com

How Immunogenic Is Pancreatic Cancer?
� Limited infiltrating effector T-cells seen in tumor specimens
� Modest mutational burden relative to more immunogenic tumors
� Minimal clinical activity observed in unselected pancreatic cancer pts with anti–CTLA-4 and anti–PD-1 monoclonal antibodies
� Can pancreatic cancers be “primed” to become more immunogenic?
Slide credit: clinicaloptions.com
von Bernstorff W, et al. Clin Cancer Res. 2001;7(3 suppl):925s-932s.Clark CE, et al. Cancer Lett. 2009;279:1-7. Royal RE, et al. J Immunother. 2010;33:828-833. Topalian S, et al. N Engl J Med. 2012;366:2443-2454. Alexandrov LB, et al. Nature. 2013;500:415-421.
Pilocytic astrocytomaALL
MedulloblastomaAML
Kidney chromophobe
ThyroidCLL
Neuroblastoma
Glioblastoma
PancreasBreast
Gliona low grade
Lymphoma B-cell
Myeloma
ProstateOvary
Kidney papillary
Kidney clear cellLiver
Uterus
Stomach
Head and neckCervix
Colorectum
Esophagus
Melanoma
Lung squamous
Lung adenocarcinoma
Bladder
1,000
100
10
1.0
0.001
0.01
0.1
Som
atic
Mut
atio
n P
reva
lenc
e (N
umbe
r M
utat
ions
per
Meg
abas
e)
Lung small cell

� Potent activation of innate and antigen-specific immune response
� Deletion of virulence genes (actA, inlB)
� Insertion of mesothelin expression cassette –validated immune target
Immunotherapy Platforms in Pancreatic Cancer
GVAX PancreasIrradiated, whole-cell tumor vaccine
CRS-207 Live-attenuated Listeria monocytogenes
GVAX
GM-CSF
Dendritic cell
Antigen uptake and activation
T-cell
Tumor antigens
Tumor celldestruction
Slide credit: clinicaloptions.comLe DT, et al. J Clin Oncol. 2015;33:1325-1333.Le DT, et al. ASCO GI 2014. Abstract 177.
∆actA ∆inlB

Phase II Study: GVAX/CRS -207 vs GVAX Alone in Metastatic Pancreatic Cancer
� Prior phase I trial of CRS-207 showed markedly improved survival (17 months) in 3 pancreatic cancer pts who had previously undergone “boost” with GVAX vaccine
� Primary objective: OS
Arm A (n = 60)
Arm B (n = 30)
20-wk treatment course*: 6 doses, Q3W
Le DT, et al. Clin Cancer Res. 2012;18:858-868. Le DT, et al. J Clin Oncol 2015;33:1325-1333. Slide credit: clinicaloptions.com
R
Pts with metastatic pancreatic cancer; failed or refused chemotherapy
24 mos of follow-up
24 mos of follow-up
*Additional courses if clinically stable
Randomized 2:1
CY/GVAX
CRS-207

Toxicities related to CRS-207: transient fevers, rigors, lymphopenia
GVAX/CRS-207 vs GVAX Alone in Metastatic Pancreatic Cancer: Results
� 2 randomized trials are evaluating GVAX/CRS-207 vs SOC chemotherapy
– ECLIPSE (NCT02004262)
– STELLAR: second- or third-line treatment ± nivolumab (NCT02243371)
Le DT, et al. J Clin Oncol 2015;33:1325-1333 Slide credit: clinicaloptions.com
1.0
0.8
0.6
0.4
0.2
00 3 6 9 12 15 18 21
Mos
OS
(P
roba
bilit
y)
Cy/GVAX + CRS-207Cy/GVAX
34/45 (75.6)17/21 (81.0)
9.7 (6.1-10.5)4.6 (3.8-8.5)
P = .017 (1 sided)P = .033 (2 sided)
HR: 0.53
Events, n/N (%)
Median, Mos (95% CI)

Phase IIb ECLIPSE: GVAX/CRS -207 vs CRS-207 or Chemo Alone in mPC
� Primary endpoint: OS
� Secondary endpoints: safety, response
Pts 18 yrs of age or older
with previously treated metastatic pancreatic cancer,
ECOG PS 0/1(N = 301)
Cyclophosphamide 200 mg/m 2
Day 0 of Wks 1, 4 +GVAX Pancreas Vaccine (5 × 10e8 cells)
Day 1 of Wks 1, 4 +CRS-207 (1 × 10e9 CFU)
Wks 7, 10, 13, 16
CRS-207Wks 1, 4, 7, 10, 13, 16
Slide credit: clinicaloptions.comClinicalTrials.gov. NCT02004262.
Chemotherapy(various)

Other Signaling Pathway Targets in Pancreatic Cancer

Molecular Subtypes of Pancreatic Cancer
� Genomic analyses of 456 pancreatic ductal adenocarcinomas identified molecular subtypes of pancreatic cancer
� 32 recurrently mutated genes
– KRAS, TP53, SMAD4, CDKN2A
– 10 pathways
– KRAS, TGF-b, WNT, NOTCH, ROBO/SLIT signaling, G1/S transition, SWI-SNF, chromatin modification, DNA repair and RNA processing
� Expression analyses defined subtypes that correlate with histology:
– Squamous
– Pancreatic progenitor
– Immunogenic
– Aberrantly differentiated endocrine/exocrine (ADEX)
Bailey P, et al. Nature. 2016;531:47-52. Slide credit: clinicaloptions.com

Core Signaling Pathways Are Altered in Most Pancreatic Cancers
Regulatory Pathway or Process Genetic Alteration of ≥ 1 Gene, %
Apoptosis 100
Hedgehog signaling 100
KRAS signaling 100
Regulation of G1/S phase transition 100
TGF-b 100
Wnt/Notch 100
JNK signaling 96
Regulation of invasion 92
DNA damage control 83
Homophilic cell adhesion 79
Small GTPase-DEP signaling 79
Integrin signaling 67
Jones S, et al. Science. 2008;321:1801-1806. Slide credit: clinicaloptions.com

Agent* MOA Phase PlannedN
Comments
Ibrutinib[1]
(RESOLVE)BTK inhibitor II/III 326 Stage IV, KPS ≥ 70
Necuparanib[2] Heparin sulfate mimetic
I/II (randomized) 180 Drug engineered to reduce anticoagulant
activity
MM-141[3] Bispecific mAb: IGF-IR and
ERBB3
II (randomized) 260 Pts selected for high free serum IGF-1
Indoximod[4] IDO (indoleamine
2,3-dioxygenase)
inhibitor
Ib/II (nonrandomized)
98 IDO = enzyme that catalyzes degradation
of L-tryptophan �suppresses T cell
function (= immune checkpoint inhibitor)
Other Novel Signaling Pathway Inhibitors Under Investigation in Metastatic PDAC
*All being studied in combination with gemcitabine/nab-paclitaxel.
1. ClinicalTrials.gov. NCT02436668. 2. ClinicalTrials.gov. NCT01621243. 3. ClinicalTrials.gov. NCT02399137. 4. ClinicalTrials.gov. NCT02077881. Slide credit: clinicaloptions.com

Which Subsets of Pts Might Benefit From Specific Therapies?
� BRCA- or PALB2- mutation carriers
– Olaparib: 5/23 pts (22%) with objective response, 8/23 (35%) with stable disease > 8 wks[1]
– Veliparib: 0/16 pts with objective response, 5/16 (31%) with stable disease > 8 wks[2]
� MSI-high/mismatch repair-deficient (dMMR)
– 2 of 4 pts with dMMR pancreatic cancers showed objective response by RECIST to pembrolizumab[3]
1. Kaufman, et al. J Clin Oncol. 2015;33:244-250. 2. Lowery, et al. ASCO 2015. Abstract 358. 3. Le D, et al. ASCO 2015. Abstract 195. Slide credit: clinicaloptions.com

Conclusion
� Improving frontline and second-line treatment options
– 2 frontline regimens, FOLFIRINOX and gemcitabine/nab-paclitaxel, have demonstrated survival benefit (vs gemcitabine alone) in phase III studies
– Evidence for second-line/salvage treatment in this disease with nanoliposomal irinotecan and 5-FU after gemcitabine-based therapy
– Fluoropyrimidine-based and gemcitabine-based regimens are additional options for second-line/salvage therapy
� Novel therapeutics
– Active area of research
– Multiple ongoing randomized phase II/III trials
– Biomarker evaluation underway Slide credit: clinicaloptions.com

Go Online for More CCO Coverage of Pancreatic Cancer!
Slides of key data from this and other programs on pancreatic cancer
CME-certified video module on pancreatic cancer with expert faculty commentary on key studies
clinicaloptions.com/oncology