Embed Size (px)
Citation preview

Best Treatment for Best Treatment for Barrett’s is Barrett’s is
Surgery Surgery Bill Richards, MD Bill Richards, MD
FACSFACS
Professor and Chair Professor and Chair SurgerySurgery
University of South University of South AlabamaAlabama
College of MedicineCollege of Medicine

Barrett’s = Intestinal Barrett’s = Intestinal MetaplasiaMetaplasia
Metaplasia = change Metaplasia = change in cell-typein cell-type
Squamous to Squamous to specialized intestinal specialized intestinal cellscells
First described by First described by Norman Barrett in Norman Barrett in 19501950
Adaptive mechanismAdaptive mechanismto injuryto injury

Risk of Risk of Adenocarcinoma in Adenocarcinoma in
Barrett’s EsophagusBarrett’s Esophagus0.4-0.5% per year0.4-0.5% per year
5-10% lifetime5-10% lifetime

Current Current ManagementManagement of Barrett’s Patients* of Barrett’s Patients*Intestinal Metaplasia Surveillance (2-3 yrs)
Low grade dysplasia Surveillance (6-12 mo)
High grade dysplasia Surveillance (3 mo) vs. Esophagectomy
Adenocarcinoma Esophagectomy vs. Palliative Care
* May Differ per Institution

Esophageal Adenocarcinoma
Baseline Barrett’s
Esophagus
One Outcome of One Outcome of SurveillanceSurveillance

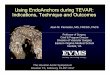
Mixed Reflux of Gastric and Duodenal Mixed Reflux of Gastric and Duodenal Juices is more Harmful to the Esophagus Juices is more Harmful to the Esophagus
than Gastric Juice Alone than Gastric Juice Alone Kauer WK et al Ann Surg 222: 525-533Kauer WK et al Ann Surg 222: 525-533
0
20
40
60
80
Normals No injury Esophagitis Barrett's
NormalsNo injuryEsophagitisBarrett's
Prevalence of esophageal bilirubinPrevalence of esophageal bilirubin exposureexposure

Bile Reflux Induces Bile Reflux Induces Adenocarcinoma of the Adenocarcinoma of the
EsophagusEsophagus
Ireland et al Ann Surg. 1996 September; 224(3): 358–371.

Antireflux SurgeryAntireflux Surgery 1976 Donahue and 1976 Donahue and
Bombeck defined a Bombeck defined a technique of "floppy" technique of "floppy" Nissen fundoplication Nissen fundoplication (FNF) that prevented (FNF) that prevented experimental experimental pathologic reflux pathologic reflux without preventing without preventing gaseous eructations gaseous eructations or vomiting (normal or vomiting (normal reflux) when reflux) when appropriate appropriate

LES Pressure Returns to LES Pressure Returns to Normal After Normal After
Laparoscopic FundoplicationLaparoscopic Fundoplication
0
2
4
6
8
10
12
14
16
Pressure (mm Hg)
NORMAL PRE-OP POST-OP
N=26
Peters JH et al. Ann Surg 1998;228:40-50.

24 Hour pH Studies after 24 Hour pH Studies after Laparoscopic Laparoscopic
FundoplicationFundoplication
AuthorAuthor # patients # patients
pH NegativepH NegativeFollow-up Follow-up
(months)(months)
HinderHinder (87%)(87%) 3-123-12
HunterHunter (91%)(91%) 1212
WatsonWatson (87%)(87%) 33
PetersPeters (93%)(93%) 2121

Does Nissen reduce NonAcid Does Nissen reduce NonAcid Reflux?Reflux?
Does Nissen reduce NonAcid Does Nissen reduce NonAcid Reflux?Reflux?
8 patients with Barrett’s 8 patients with Barrett’s
24 hour pH and nonacid relfux24 hour pH and nonacid relfux
- before (on omeprazole 20 mg BID)- before (on omeprazole 20 mg BID)
- after laparoscopic Nissen - after laparoscopic Nissen fundoplicationfundoplication

PPI Nissen
0
10
20
30
40
50
60ac
id e
pis
od
es (
n)
Data are shown as median (horizontal line), interquartile range (box), and 5th to 95th percentile (vertical line)
Acid Episodes
Acid Episodes

PPI Nissen
0
10
20
30
40
50
60
70
80
90
no
n-a
cid
ep
iso
des
(n
)
9
Data are shown as median (horizontal line), interquartile range (box), and 5th to 95th percentile (vertical line)
Non-Acid EpisodesNon-Acid Episodes
P=0.001

Conclusions: PConclusions: Patients with atients with Barrett’s esophagusBarrett’s esophagus
Conclusions: PConclusions: Patients with atients with Barrett’s esophagusBarrett’s esophagus
Nissen eliminates acid and non-acid Nissen eliminates acid and non-acid refluxreflux
PPI’s fail to eliminate acid reflux in PPI’s fail to eliminate acid reflux in 33-50% 33-50%
PPI’s do not reduce non-acid refluxPPI’s do not reduce non-acid reflux

Conservative treatment versus Conservative treatment versus antireflux surgery in Barrett's antireflux surgery in Barrett's
oesophagus: long-term results of a oesophagus: long-term results of a prospective study.prospective study.
Barrett’s Esophagus
27 medical Treatment 32 Fundoplication
22% Dysplasia 2.3% Dysplasia
Ortiz et al Br J Surg. 1996 Feb;83(2):274-8

Regression of Barrett’s Regression of Barrett’s after Fundoplicationafter Fundoplication
STUDYSTUDY # PATIENTS # PATIENTS short short segmentsegment
% % REGRESSIOREGRESSIONN
U WASHINGTONU WASHINGTONAnn Surg. 2003 October; 238(4): 458–Ann Surg. 2003 October; 238(4): 458–
466466
6161 56%56%
USCUSCAnn Surg. 2001 October; 234(4): Ann Surg. 2001 October; 234(4):
532–539532–539
2626 14%14%

Standard of care = Standard of care = removalremoval of pre- of pre-
cancerous lesionscancerous lesions colon polyps (7 M annual U.S. colon polyps (7 M annual U.S.
colonoscopies)colonoscopies) cervical dysplasiacervical dysplasia breast massesbreast masses dermatologic lesions (moles, actinic dermatologic lesions (moles, actinic
keratoses)keratoses)
Should We Treat Barrett’s?Should We Treat Barrett’s?

Techniques for Mucosal Techniques for Mucosal AblationAblation
MechanicalMechanical Endoscopic mucosal resection (EMR)Endoscopic mucosal resection (EMR)
PhotochemicalPhotochemical Photodynamic TherapyPhotodynamic Therapy
ThermalThermal Argon plasma coagulationArgon plasma coagulation Multi-polar coagulationMulti-polar coagulation Bipolar energyBipolar energy Lasers: Argon, Nd: YAG, KTP-YAGLasers: Argon, Nd: YAG, KTP-YAG Low-flow cryoablationLow-flow cryoablation

Overall ConclusionsOverall Conclusions
Balloon-based ablation can eliminate Balloon-based ablation can eliminate all histological evidence of IM after all histological evidence of IM after 1-2 treatments1-2 treatments
No safety issuesNo safety issues LGD and HGD trials underwayLGD and HGD trials underway
Promising early resultsPromising early results Early data shows complete elimination Early data shows complete elimination
of dysplasia after one treatment as of dysplasia after one treatment as possiblepossible

ConclusionConclusion
This is an exciting, rapidly growing This is an exciting, rapidly growing field.field.
Currently, there is no ideal ablative Currently, there is no ideal ablative modality. modality.
Patients should be treated with very Patients should be treated with very close followup.close followup.
Multimodal ablative therapy may Multimodal ablative therapy may have significant role.have significant role.

SummarySummary
Barrett’s associated with Non Acid Barrett’s associated with Non Acid and Acid Reflux and Acid Reflux
Non acid and acid reflux can cause Non acid and acid reflux can cause esophageal cancer in experimental esophageal cancer in experimental animalsanimals

SummarySummary
Nissen significantly reduces acid and Nissen significantly reduces acid and non acid refluxnon acid reflux
PPI’s reduce acid reflux only and PPI’s reduce acid reflux only and normalize 50-80% of patientsnormalize 50-80% of patients

SummarySummary
There is no proof that Nissen There is no proof that Nissen fundoplication can prevent fundoplication can prevent progression to cancer.progression to cancer.
But Nissen fundoplication is the only But Nissen fundoplication is the only modality that can reduce both acid modality that can reduce both acid and non acid reflux and has been and non acid reflux and has been shown to reverse Short Segment shown to reverse Short Segment Barrett’sBarrett’s