Embed Size (px)
Citation preview

BACK HOME INDEX FORWARD
BETTER PRACTICE PROJECT
Aged & Community Services SA & NTCo-ordinator’s Handbook
INDEX FORWARD
BACK HOME INDEX FORWARD
1
C O N T E N T S
Foreword 3HACC Service Principles 4 About Appreciative Inquiry 5About the Handbook 6
DISCOVER1. Being prepared 82. Building rapport 103. Getting to know the person initially 134. Behaving appropriately 175. Finding strengths 206. Understanding needs 247. Identifying networks 298. Clarifying purpose 339. Understanding culture 36
DREAM10. Planning a response 4011. Creative options 4512. Consider the person’s roles 4913. Support relationships 5214. Encourage active participation in the response 5615. Health and well-being 58
DESIGN16. Agreeing goals 6317. The right response 6618. Resources, referrals and co-ordination 6919. Support community participation and informal networks 7120. Advocacy and safeguarding 74
DELIVER21. Check in 7722. Respond fl exibly 7923. Endings: Graduation, celebration and letting go 81
REFERENCES 85

BACK HOME INDEX FORWARD
2
CONTACT DETAILS Joyleen Thomas Manager, Better Practice Project
Aged & Community Services SA & NT246 Glen Osmond Road, Fullarton SA 5063
P: 08 8338 7111 F: 08 8338 7077 W: www.agedcommunity.asn.au E: [email protected]
Handbook compiled by Ronda Held www.rondaheld.com.au Editorial Assistance from Courtney Hall
Graphic Design by Douglas Molino www.douglasmolino.squarespace.com Stories used with permission.
Citation:Better Practice Project (2011). Imagining a Better Life for Older People:
Co-ordinator’s Handbook. Aged and Community Services SA/NT. Adelaide.
© Better Practice Project

BACK HOME INDEX FORWARD
3
This Handbook is a gift for Co-ordinators of home care services who are responsible for supporting people to remain living at home. We hope that it will be a helpful tool to open up the world of possibilities for creatively meeting people’s needs, and helping them to continue a meaningful lifestyle in the community.
The Co-ordinators of home care services set out each day to do their best for those they assist. However, they have many things to take into consideration along the way. Sometimes perceived obstacles and the demands of the paperwork can temporarily take our focus off what the person really wants and what will be benefi cial for them. We hope that the resources in this handbook will contribute to ensuring our practice moves further towards our visions and aspirations, not only for older people receiving services today, but for the support we want ourselves in the future. There is no doubt that expectations are already changing, and will continue to change into the future. Trends such as Consumer Directed Care help us to think about what it really means for older people to be in control of the services they receive. What are the strategies and techniques we need to make consumer direction a reality?
While the Handbook has a series of modules that may at fi rst appear to be sequential steps in planning home supports for people, they are actually more a number of considerations that need to be covered, not necessarily in the order presented. The handbook provides a range of thought starters, prompts, and important issues to consider in the process of assisting people, not necessarily all the answers. Pointers are given to other references that may be of assistance.
The Handbook is based on an Appreciative Inquiry (AI) approach (see below for more information on AI). This asks: “what do we do well now and how can we do it better?” Or in the case of older people “what are people’s strengths and capabilities, and how can we enhance them?” AI uses the four “D” cycle of: Discover, Dream, Design & Deliver. (1)
This handbook follows the stages of Appreciative Inquiry, rather than the traditional case management steps of assessment, planning, implementation and review. In some ways these categories are very similar, but by changing the language and approach, we are hopeful
that this may give people new ways to look at their role as a Co-ordinator.
The HACC Service Principles provide the foundation for the material in this Handbook.(2) The handbook has also referenced the Australian Standards for Case Management Services (3) to ensure that our approach also meets professional standards for good practice in Co-ordination and Case Management. To order a full copy of the Standards, go to www.cmsa.org.au/publications.htm.
This handbook also builds on the content of the Better Practice Project Handbook (2006) (4) which explored the key principles that underpin a person-centred approach to working with older people. This was aimed at a broader audience, but it provides a backdrop for this latest Handbook that is a more detailed practice guide tailored to the needs of Home Care Co-ordinators.
We hope that the Handbook will support you in your work and help you to:
• Focus on good questions that get to the heart of the issues and people’s real needs
• Help you to think “outside the square” in tricky situations
• Raise the bar about what is possible for people
• Keep a focus on the people you assist
• Develop the right relationship with the people you serve
• Help older people to remain “in the driver’s seat”
• Tackle the hard issues that some of us do not like to think about, such as “what is best for our health & well-being?”
• Work at setting goals with people and celebrating their achievement
• Think about what it might take for services to no longer be needed.
Thank you to all of the practitioners who provided comments on the drafts and contributed their real life stories to illustrate key points.
Joyleen Thomas Manager, Better Practice Project
FOREWORD
F o r e w o r d – A b o u t t h e c o - o r d i n a t o r s h a n d b o o k
BACK HOME INDEX FORWARD
4
SERV
ICE
(HAC
C) P
RINC
IPLE
S
S o u t h A u s t r a l i a n H o m e a n d C o m m u n i t y C a r e ( H A C C )S e r v i c e P r i n c i p l e s (2)
SERV
ICE
(HAC
C) P
RINC
IPLE
SSE
RVIC
E(H
ACC)
PRIN
CIPL
ES
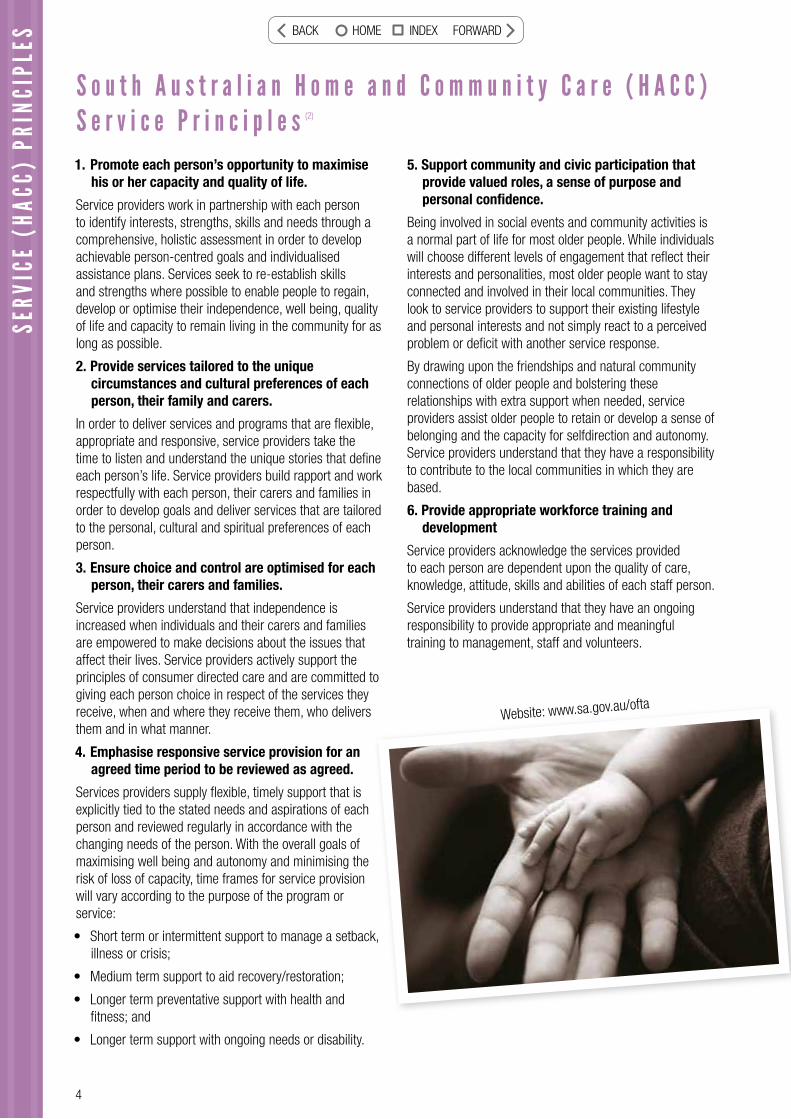
1. Promote each person’s opportunity to maximise his or her capacity and quality of life.
Service providers work in partnership with each person to identify interests, strengths, skills and needs through a comprehensive, holistic assessment in order to develop achievable person-centred goals and individualised assistance plans. Services seek to re-establish skills and strengths where possible to enable people to regain, develop or optimise their independence, well being, quality of life and capacity to remain living in the community for as long as possible.
2. Provide services tailored to the unique circumstances and cultural preferences of each person, their family and carers.
In order to deliver services and programs that are fl exible, appropriate and responsive, service providers take the time to listen and understand the unique stories that defi ne each person’s life. Service providers build rapport and work respectfully with each person, their carers and families in order to develop goals and deliver services that are tailored to the personal, cultural and spiritual preferences of each person.
3. Ensure choice and control are optimised for each person, their carers and families.
Service providers understand that independence is increased when individuals and their carers and families are empowered to make decisions about the issues that affect their lives. Service providers actively support the principles of consumer directed care and are committed to giving each person choice in respect of the services they receive, when and where they receive them, who delivers them and in what manner.
4. Emphasise responsive service provision for an agreed time period to be reviewed as agreed.
Services providers supply fl exible, timely support that is explicitly tied to the stated needs and aspirations of each person and reviewed regularly in accordance with the changing needs of the person. With the overall goals of maximising well being and autonomy and minimising the risk of loss of capacity, time frames for service provision will vary according to the purpose of the program or service:
• Short term or intermittent support to manage a setback, illness or crisis;
• Medium term support to aid recovery/restoration;
• Longer term preventative support with health and fi tness; and
• Longer term support with ongoing needs or disability.
5. Support community and civic participation that provide valued roles, a sense of purpose and personal confi dence.
Being involved in social events and community activities is a normal part of life for most older people. While individuals will choose different levels of engagement that refl ect their interests and personalities, most older people want to stay connected and involved in their local communities. They look to service providers to support their existing lifestyle and personal interests and not simply react to a perceived problem or defi cit with another service response.
By drawing upon the friendships and natural community connections of older people and bolstering these relationships with extra support when needed, service providers assist older people to retain or develop a sense of belonging and the capacity for selfdirection and autonomy. Service providers understand that they have a responsibility to contribute to the local communities in which they are based.
6. Provide appropriate workforce training and development
Service providers acknowledge the services provided to each person are dependent upon the quality of care, knowledge, attitude, skills and abilities of each staff person.
Service providers understand that they have an ongoing responsibility to provide appropriate and meaningful training to management, staff and volunteers.
k,
Website: www.sa.gov.au/ofta
BACK HOME INDEX FORWARD
5
“Appreciative Inquiry (AI) is the cooperative co-evolutionary search for the best in people, their organizations, and the world around them. It involves the discovery of what gives
“life” to a living system when it is most effective, alive, and constructively capable in economic, ecological and human terms. AI involves the art and practice of asking questions that strengthens the system’s capacity to apprehend, anticipate, and heighten positive potential.
All interventions focus on the speed of imagination and innovation instead of the negative, critical and spiraling diagnoses commonly used in organizations. The discovery, dream, design and deliver model links the energy of the
positive core to changes never thought possible.” (5)
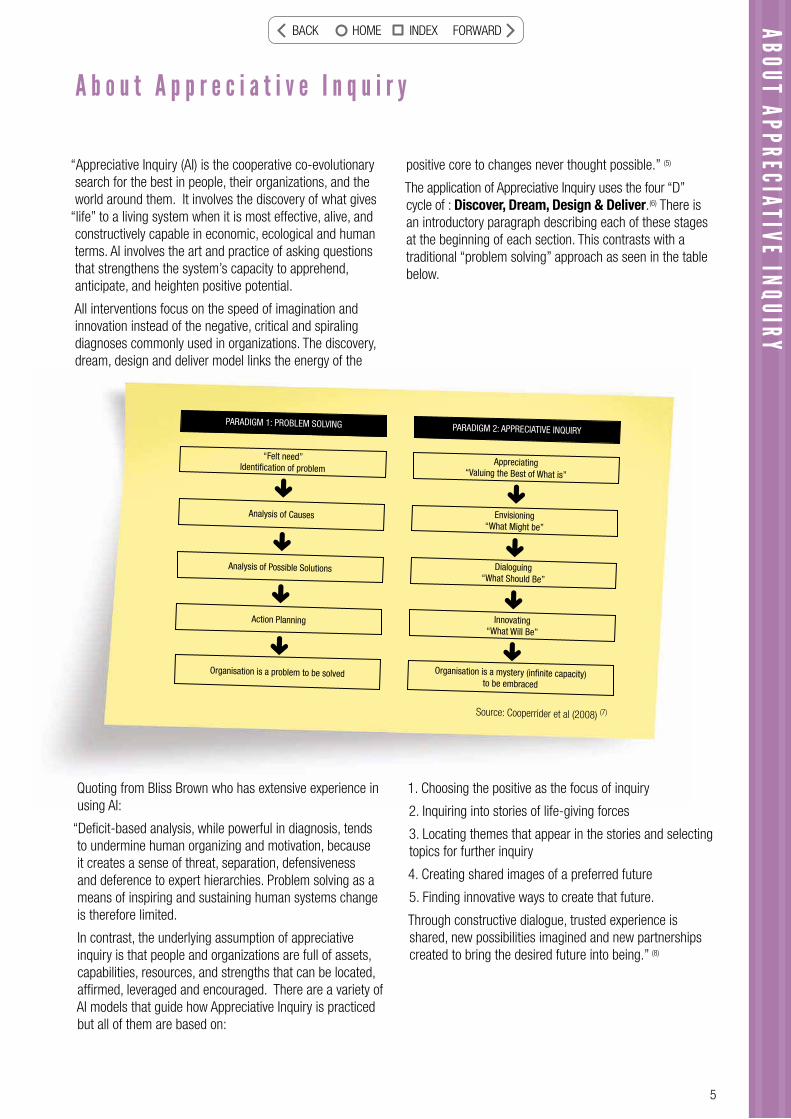
The application of Appreciative Inquiry uses the four “D” cycle of : Discover, Dream, Design & Deliver.(6) There is an introductory paragraph describing each of these stages at the beginning of each section. This contrasts with a traditional “problem solving” approach as seen in the table below.
ABOUT APPRECIATIVE INQUIRY
A b o u t A p p r e c i a t i v e I n q u i r y
Quoting from Bliss Brown who has extensive experience in using AI:
“Defi cit-based analysis, while powerful in diagnosis, tends to undermine human organizing and motivation, because it creates a sense of threat, separation, defensiveness and deference to expert hierarchies. Problem solving as a means of inspiring and sustaining human systems change is therefore limited.
In contrast, the underlying assumption of appreciative inquiry is that people and organizations are full of assets, capabilities, resources, and strengths that can be located, affi rmed, leveraged and encouraged. There are a variety of AI models that guide how Appreciative Inquiry is practiced but all of them are based on:
1. Choosing the positive as the focus of inquiry
2. Inquiring into stories of life-giving forces
3. Locating themes that appear in the stories and selecting topics for further inquiry
4. Creating shared images of a preferred future
5. Finding innovative ways to create that future.
Through constructive dialogue, trusted experience is shared, new possibilities imagined and new partnerships created to bring the desired future into being.” (8)
ABOUTAPPRECIATIVE
INQUIRYQ
Source: Cooperrider et al (2008) (7)
“Felt need”Identifi cation of problem
Appreciating“Valuing the Best of What is”
Analysis of Causes Envisioning“What Might be”
Analysis of Possible Solutions Dialoguing“What Should Be”
Action Planning Innovating“What Will Be”
Organisation is a problem to be solved Organisation is a mystery (infi nite capacity) to be embraced
PARADIGM 1: PROBLEM SOLVING PARADIGM 2: APPRECIATIVE INQUIRY
BACK HOME INDEX FORWARD

6
A b o u t t h e H a n d b o o k
ABOU
T TH
E HA
NDBO
OK
This handbook is designed to give you a number of different approaches to each topic – some are thought starters, others will give you a deeper appreciation of an issue, some tools to assist you, or illustrate the topic with a story. Every person has a different learning style and will relate better to different parts to the material. The elements are included where they help enlighten the topic, so each element is not necessarily included in each topic.
You are encouraged to read the Handbook as you would a magazine, and use it in staff meetings, as orientation for new staff or to follow up the references provided to further your own development.
The elements include:
The appreciative question – begins our consideration of the topic in a positive mode by asking you to think of a situation in which you had a positive experience, and what you might learn from this in your work with older people.
The provocative proposition - bridges the best of what is and what might be, and captures the essence of this element of the Co-ordinator’s work.
Rationale – outlines why this particular process or step is important.
Word defi nition – to spark your thinking about what the words we use every day really mean.
Step-by-step guide – provides a “checklist” of things to consider in relation to this topic.
Tools – some techniques you may fi nd useful to delve more deeply into a particular topic.
Story – illustrating one or more of the principles and approaches unfolded in the Handbook.
Evidence base – resources, frameworks and research facts.
Roles – some tips to provide role clarity for Co-ordinators in relation to this topic.
Case Management Standards – a reference is provided to the National Standards for Case Management where these are particularly relevant to the topic.
Quotes – to provide some inspiration from the great thinkers over time!
Discussion question – thought starters for team meetings or discussions tackling some of the trickier issues relating to that topic.
BACK HOME INDEX FORWARD
7
Identify what gives lifeAppreciate the best of what is
These two phrases are somewhat in contrast to what we would initially have in mind when going out to do an “assessment”. We usually think about identifying problems, needs and what is wrong with a person. This is also part of the discovery process, but fi rst we focus on getting to know the person, their strengths and resources, and what is life-giving for them.
BACK HOME INDEX FORWARD
8
1 Being prepared
Rationale
People should not have to repeat information already provided to the service or referring agency. Workers need to give some thought to the issues that need to be covered in the fi rst visit. Preparation is required for issues such as whether an interpreter is needed, or whether a family member/advocate should be present.
Non judgemental - avoiding judgments based on one’s personal and especially moral standards (9)
The provocative proposition
Workers will gather all relevant information before arranging the fi rst visit but will be careful not to pre-judge the situation.
The appreciative question
Think about a time when you had prepared carefully before meeting someone for the fi rst time. How did it help?
“By failing to prepare, you are preparing to fail.” Benjamin Franklin
BACK HOME INDEX FORWARD
9
FIRST DATE:In many ways preparing for your fi rst contact with a person is like preparing
for a fi rst date!
◊ You want to make a good impression
◊ There is careful thinking and planning about how you will approach it
You put some effort into personal preparation, ie your appearance,
equipment (cleaning your car?) purse, diary, pen.
◊ You choose a suitable meeting place
◊ Remember they may have already had a fi rst date which may not have
been a good experience, or may have been great. You need to be prepared
for either!
Step-by-step guide
Gather any relevant background information from referral source and screening process:
• Note demographic information and other details to ensure people do not have to provide the information again • Note the reason for referral• Any considerations to ensure a successful fi rst meeting: For example, communication (language, cognitive
capacity, hearing); support needed (an advocate or interpreter); cultural factors• Respect confi dentiality.
Where appropriate telephone the person to establish:
• Who you are, where you are from and why you are phoning• The person’s preferred method of contact (day, time, place)• Preference to have a family member, friend or advocate present and ask who will arrange this• Identify if there is a need for an interpreter to be present• If visiting home then clarify staff risks (dogs etc) and access.
Case Management Standards
1A Case Identifi cation and Assessment
1B Gather information about Clients while respecting their confi dentiality and privacy with the aim of not duplicating assessments. (3)
Roles
Remember that relationship building and empowering the person begins from the very fi rst point of contact, including the initial phone call.
1 BEING PREPARED
Discussion question
How do you deal with a person who is reluctant to receive support? What do you do if on initial contact they refuse to see you?
BACK HOME INDEX FORWARD
10
2 Building Rapport
Rationale
When people are requesting personal assistance they may be asked to share very personal information. It is important to fi rst build trust so that an honest and open conversation can take place. The person needs to be able to be infl uential in defi ning their own needs and what support they require.
“Right relationship” is an ethical condition that exists between services and those they serve when the people served are seen and treated with appropriate respect, integrity and value and where they are enabled to be decisively infl uential in how they are to be assisted.(10) Step-by-step guide
Some ways to help build a positive relationship:• Arrive on time or let the person know if you are unavoidably late• Ensure the initial greeting is warm and welcoming• Introduce your self and provide identifi cation if necessary before entering the person’s home• Switch off your mobile phone and avoid other interruptions• Begin talking about something other than the assessment• Listen in a sensitive and non-intrusive manner• Speak in a conversational tone, avoid using jargon• Suspend your judgments and do not let assumptions get in the way• Let the person know you enjoy talking with them, it will help them relax• Involve family members or advocates in the conversations where appropriate• Provide relevant information about your service and those available from other agencies• Provide information in a way that enables them to make informed choices and decisions• Ensure that if you are to continue contact, you have gained clear consent from the person or their representative
to be involved with your program• Ensure the person understands their rights and responsibilities.
The appreciative question
Think about a time when you met someone for the fi rst time and you established a positive relationship quickly. What helped in that situation?
The provocative proposition
A positive relationship is the foundation stone for providing relevant support through understanding the person’s strengths and real needs. It is worth spending time building that relationship as an investment in the future.
BACK HOME INDEX FORWARD
11
2 BUILDING RAPPORT
Tools
QUESTIONINGTry to ask more open questions than closed questions.
An open question is one which cannot be answered with yes or no and which encourages a more detailed answer, for example:
• “What are your feelings about this?” • “What are the advantages of doing things the way
you have suggested?” • “What are the disadvantages?”
Avoid closed questions such as:
• “Are you feeling depressed?” • “Are you looking forward to Christmas?”
Another disadvantage of closed questioning is that the desired answer might be implied within the question and you might inadvertently steer the person to give an answer that they wouldn’t otherwise have given. An example of this would be:
“Do you want us to organise home care? The implied expected answer here is quite clearly “yes”. An open question would be “what has prompted you to contact our service?”
Try to frame questions in the positive.
“Tell me what a good day looks like for you”
“What is your favourite activity of the week?”
AVOIDING BIASIt is easy to make assumptions based on our experience in supporting older people. But remember everyone is a unique individual, with their own preferences and needs. A bias is any infl uence that changes an answer or an opinion from what it might have been without that infl uence. Ways you can avoid bias:
Be aware of your own opinions and perspectives and how these may be infl uencing your discussion.
Do not express your own opinions about how the person should respond (eg I think everyone should have physio).
Do not suggest answers even if the person wants your help. Help the person to think through the issue and use probing questions if necessary to encourage further conversation.
Be patient – allow the person time to think and don’t jump in. Acknowledge that these are diffi cult issues.
SIX TIPS FOR BUILDING AND MAINTAINING RAPPORTRapport building is the art of helping another person minimize their perceived difference between themself and yourself. This can be achieved by tactfully allowing the other party to see the common ground in your personality or point of view. Rapport happens at the subconscious level but here are a few ways that you can consciously
help the process along.
1. Rapport Starts at the Beginning. The best time to start building rapport is when you interact with a person for the fi rst time. Then each subsequent time that you meet ensure that you start by re-establishing rapport.
2. Give Appreciation and Importance to Others Accept that the most important person in the world in the eyes of most people is themself.
When interacting with someone else allow them to feel important. The easiest way to do this is to learn their name and use it often during your conversations.
If you are involved in some task with others, you can help them feel important by trusting them with appropriate responsibility and showing appreciation for their contribution. In fact, why not make a habit of showing genuine appreciation for things well done in all interactions with others.
3. The Skill of Asking Questions Remember that the person asking the questions is leading the direction of the conversation. Ask interesting questions that allow the other person to talk about themself or their interests and then listen attentively to what they are saying.
4. Active Listening
Listening is a skill and it’s easiest learned if you develop the habit of being genuinely interested in other people.
Allow the other person to do most of the talking unless they are specifi cally asking for your contribution or opinion.
Give them positive feedback followed by non-threatening questions that allow them to expand on what they are saying.
5. Keep Your Ego Under Control
Ego has been responsible for breaking rapport on more occasions that any other behaviour. Ego is a sign of low self worth. If you develop a strong feeling of self worth then you will not have the need to allow your ego to get in your way.
Be willing to admit you are wrong when you are. Do so quickly and happily and gratefully acknowledge the other person’s role in helping you see your error.
Be willing to allow others to take credit for your good ideas if it helps you achieve your desired end goal.
Rather than argue for your point of view every time you are challenged, encourage the other person to express their point of view. If you do have to state an opposing
BACK HOME INDEX FORWARD
12
Tools - continued
Case Management Standards
1. Case Identifi cation and Assessment
1A Ensure that Clients understand their rights and responsibilities, supported by evidence of Clients consenting to be involved in the program providing case management (3)
Roles
Being friendly does not necessarily mean being friends. While friendliness is important to rapport building, the worker also needs to be clear that they come in a professional role. Being a friend implies an ongoing commitment which a worker cannot promise.
In this early stage it is OK for a Co-ordinator to admit that you do not have all the answers. It is better to spend time getting to know the person and what they need, and offering to go away and research the possibilities. Rushing into solutions may mean that you miss important cues.
Assumptions are the termites of relationships. Henry Winkler (1945 - )
From consumers:
“Our Co-ordinator is knowledgeable to the extent that she is consistently proactive in anticipating areas of need and the measures that need to be taken or considered – especially valuable in the piecemeal operation of aged care funding. She is generous, thoughtful, calm, non-judgemental and practical.”
Commenting on support for their neighbour “We have observed the Co-ordinator’s skill in patiently winning her trust and fi nally achieving her acceptance of support which is enabling her to continue to live safely in her home. We consider her patience and skills to have been outstanding and worthy of recognition.”
Discussion Question
What do you do in a situation where you do not seem to be able to establish a positive relationship with a person, eg they do not seem to trust you, you may disagree with their values and priorities, or you seem to have a personality clash?
point of view, acknowledge the value of their point of view fi rst and then tactfully promote the additional benefi ts of your ideas. Gently lead them to your desired outcome by concentrating on the ways in which they would receive benefi ts, that they really want, from adopting the point of view that you are promoting.
6. Friendliness Nothing breeds friendliness like friendliness. Source: Delrojo (2010) (11)
BACK HOME INDEX FORWARD
13
3 Getting to know the person initially
3 GETTING TO KNOW THE PERSON INITIALLY
Rationale
In supporting people in the community we need to focus on the whole person, not just their defi cits or needs. If we understand what is important to the person we will ensure that if services are needed, those services support their lifestyle rather than the person fi tting their life around the service. We also need to consider that the best support may not necessarily come from a service but from informal networks or community resources instead.
Identity – the distinct personality of an individual, or individual characteristics.(12)
Step-by-step guide
Aspects such as the person’s history, work roles, family, interests and hobbies will all impact on how they might wish to be supported in the community. Explore these using open questions, such as “tell me about your family”.
Tools
What Matters to me
The following questions may provide thought starters in helping you to get to know a person:
• If you were asked by a child to tell them about the most important thing you have learned in your life, what would you say?
• What was the best period of your life? Why?
• What was the hardest period of your life? Why? Did you know it at the time? What did you learn?• What do you think was the best thing you ever did for someone else?• If you could have anything in the world, what would it be?
The appreciative question
Think about a time when you felt someone really understood you? What contributed to that understanding?
The provocative proposition
The Co-ordinator will understand enough about the person to be able to sensitively frame the assessment questions and gain a better understanding of their strengths and support needs. Where little information is known, the Co-ordinator will look for visual cues in the home to gain an insight into the person and conversation starters.
BACK HOME INDEX FORWARD
14
Tools - continued
• If you could give anything in the world to someone else, what would you give? To whom?• What projects have given you the most pleasure?• What have you worked hardest at (work, social causes, friendships, marriage, parenting)?• What role does spirituality have in your life?• What makes you feel most alive?• What common threads do you fi nd in the above – this may summarise what is most important to you.
There will be situations in which the person you are supporting cannot easily respond to your questions, for example if they have dementia. You will then need to fi nd out from those around them what is important to them. Source: Skeie et al (2007) (13)
Helen Sanderson uses a process called “Appreciations” to identify what is important to people.
Ask others signifi cant to the person:
What is important to ………….?
What do you like and admire about ………….?
How do we best support ………………..?
Verns gifts
• He teaches his grandchildren how to fi sh • He makes people laugh • He is creative with his hands • He is good in the garden and grows tasty
tomatoes
What we like and admire about Vern
• His positive outlook on life• His stories and his jokes • His cheeky nature • His excitement at dinner time
VERN
Source: Sanderson & Associates (2007) (14)
BACK HOME INDEX FORWARD
15
3 GETTING TO KNOW THE PERSON INITALLY
GOING SWIMMINGLY!
Donald is a 74 year old man who has led a very active life, his so
cial life
included weekly golf (winner of numerous trophies), swimming with four life long
mates
and he also travelled overseas ever
y two years on fi shing trips.
As a father he was actively involved with his children’s sporting and danci
ng interests.
Donald was, and is, a fi t and active man. He worked for over 50
years on the rail way in
varying capacities. Upon retirement Donald contin
ued his busy life with golf, swimming and
fi shing.
Two years ago Donald’s life changed with the onset of d
ementia. Donald was unable to do
and be all that he was. He was very frustrated with the knowledge that he cou
ld no
longer drive or participate in his pa
ssions of life. Donald was aware of the impact the
dementia was having on his wife, as her time was spent ensuring
Donald’s wellbeing and
safety. Donald, seeing what his life was, surrounded by
his memorabilia and memories
became frustrated and agitated expressin
g this verbally.
Donald wanted to be able to do something physical and maintain his health
as best he could.
It was at this point that he was introduced to t
he community liaison worker. Donald, his
wife and the worker discussed Donald’s need to be
physically active, whilst being aware of
the challenges and possible dangers
Donald faced. Donald said that he r
eally missed swim-
ming. His wife said that two of his old swimming mates were no longer alive, and that con-
tact with another was seldom, and the fourth friend had moved interstate.
Donald and the worker decided to
go to the swimming pool where Donald had swum for
many years. Although Donald’s memory wasn’t serving him very well he was able to swim
lap upon lap and enjoyed it greatly. Donald and the
worker joined in with the senior
swimming group, Donald was able to have so
cial contact with people of his own generation.
The acceptance and support of many of the group ena
bled Donald to attend swimming on
a weekly basis. As Donald began to engage with fellow swimmers the worker was able to
facilitate a network of support for Donald including
transport and supervision in a sensit
ive
and appropriate manner. Even thoug
h Donald quickly forgot who he was speaking with, he
had a sense of belonging by participating in w
hat had been a life activity.
GLY!i i l life
BACK HOME INDEX FORWARD

16
Resources
Roles
The extent to which you explore a person’s history and interests will depend on the scope of your service and the type of support you are requesting. The more you are likely to be involved with the person over a longer term, the more important it is to understand the person.
Discussion question
Sometimes it is important to try out the questions that we are asking other people on ourselves. Do you think it is important to understand what is important to you and what your goals and aspirations are, before asking other people the same questions?
“[The] sense of identity provides the ability to experience one’s self as something that has continuity and sameness, and to act accordingly.” ~ Erik H. Erikson
Helen Sanderson & Associates, (2007) Person Centred Thinking with Older People: Practicalities and Possibilities. (14)
Erik H. Erikson
BACK HOME INDEX FORWARD
17
4 Behaving appropriately
4 BEHAVING APPROPRIATELY
Rationale
This is important because older people are at risk of ageism and discrimination. People who work in aged care generally do so because of a genuine respect for and affi nity with older people. However sometimes we can unconsciously take on the prejudices of the wider community refl ected in the way we speak about older people or behave towards them, for example, speaking over people to their relatives, or using jargon that may demean people.
The provocative proposition
Services that support older people will make an extra effort to behave in a way that is positive and respectful of older people. This will enhance their sense of self worth and value in the eyes of others and the community generally.
Respect – esteem for or a sense of the worth or excellence of a person, a personal quality or ability, or something considered as a manifestation of a personal quality or ability (15)
Step-by-step guide
You can show respect by:
• Asking a person what they wish to be called (eg by their fi rst name, nickname or Mr. or Mrs. …)• Speak in a normal voice – don’t yell or use a sing-song voice• Avoid using jargon – explain things in a way that is easy to understand• Don’t equate the person with their disability • Speak directly to the person, even if they are unable to communicate, not to their relative, carer or interpeter• Be aware of your body language – keep an open posture, use eye contact appropriately (this may depend on the
person’s cultural background), sit or stand at the person’s level• Treat others as you would expect to be treated yourself.
The appreciative question
What does it feel like to be treated with dignity and respect? What are the particular behaviours that make youfeel this way?
BACK HOME INDEX FORWARD
18
ELDERSPEAK - From the New York Times
“Professionals call it elderspeak, the sweetly belittling form of address that has
always rankled older people: the doctor who talks to their child rather than to
them about their health, the store clerk who assumes that an older person does
not know how to work a computer, or needs to be addressed slowly or in a loud
voice. Then there are those who address any elderly person as “dear”.
“People think they’re being nice,” said Elvira Nagle, 83, of Dublin, Calif., “but when
I hear it, it raises my hackles”.
Now studies are fi nding that the insults can have health consequences, especially
if people mutely accept the attitudes behind them, said Beccy Levy, an associate
professor of epidemiology and psychology at Yale University, who studies the
health effects of such messages on elderly people.
“Those little insults can lead to more negative images of aging,” Dr. levy said.
“And those who have more negative images of aging have worse functional health
over time, including lower rates of survival.”
In a long-term study of 660 people over age 50 in a small Ohio town, published
in 2002, Dr. Levy and her fellow researchers found that those who had positive
perceptions of aging lived an average of 7.5 years longer, a bigger increase than
that associated with exercise or not smoking. The fi ndings held up even when the
researcher’s controlled for differences in the participants’ health conditions.
In her forthcoming study, Dr. Levy found that older people exposed to negative
images of ageing, including words like “forgetful”, “feeble” and “shaky”, per-
formed signifi cantly worse on memory and balance tests; in previous experiments,
they also showed higher levels of stress.
Despite such research, the worst offenders are often health care workers, said
Kristine Williams, a nurse gerontologist and associate professor at the University
of Kansas School of Nursing.
The researchers …. concluded that elderspeak sent a message that the patient
was incompetent and begins a negative downward spiral for older persons, who
react with decreased self-esteem, depression, withdrawal and the assumption of
dependent behaviors.
Dr. Williams said health care workers often thought that using words like “dear”
or “sweetie” conveyed that they cared and made them easier to understand.
“But they don’t realize the implications,” she said, “that it’s also giving a message
to older adults that they’re incompetent.” Source: New York Times (7.10.2008) (16)
18
BACK HOME INDEX FORWARD
19
4 BEHAVING APPROPRIATELY
Respect
Several years ago a group in Wisconsin comprising consumers, providers and case managers came together to defi ne what they considered to be quality in a person-centred system.(18) They came up with the acronym
“RESPECT” which stood for:
Relationships
Empowerment
Services Individualised
Physical and Mental health
Enhancement of Image
Community
Tools
Roles
Working in partnership implies a relationship between individuals or groups that is characterized by mutual cooperation and responsibility, developed for the purpose of achieving a specifi ed goal.
The level of maturity and skills of the person and/or their carer needs to be taken into account. Some people are very capable and aware of the system, while others may require a lot more guidance and explanation. Keep this in mind in the way you communicate with people.
Case Management Standards
Ethical Principles
The Case Manager:
• Will respect people’s rights to be an individual and refrain from value judgments.
• Will consider the best interests of the Client as paramount at all times. (3)
Only those who respect the personality of others can be of real use to them. Albert Schweitzer
Discussion question
What do you consider to be inappropriate behaviours when visiting the home of an older person? How would you deal with a situation where you observed a colleague, support worker or family member behaving in this way?
BACK HOME INDEX FORWARD
20
5 Finding strengths
The appreciative question
Think about a situation where someone has acknowledged your strengths and capabilities. How does that make you feel?
Rationale
Strengths-based practice assesses the inherent strengths of a person and their support network, and then builds on them. It utilizes these strengths to address the particular issues they may be facing at the time. It is about reframing perceptions to fi nd the good in even the worst situation.
Why is this helpful?• It is an empowering alternative to traditional approaches that focus only on defi cits and problems• It avoids stigmatizing language which people may begin to identify with, accept and feel helpless to change• It fosters hope by focusing on what has historically been helpful for the person, therefore using real successes to
set the groundwork for realistic expectations• It provides an inventory of the positive building blocks that already exist to provide the foundation for growth and
recovery• It reduces the power imbalance with the Co-ordinator by promoting the person as the expert in their
own lives in relation to what will and won’t work in their situation• It places the Co-ordinator in the role of partner or guide• It involves the person’s networks and helps them to feel like an integral part of the process• It works! (18)
See Topic 10 on planning for how you can build on this approach.
The provocative proposition
Co-ordinators will understand and build on a person’s strengths when arranging the supports they need to remain at home. This will support recovery and empowerment, helping the person to feel more in control of their situation.
BACK HOME INDEX FORWARD
21
Strength – an asset of special worth or utility Recovery - restoration or return to health from sickness; restoration or return to any former and better state or condition. (19)
5 FINDING STRENGTHS
Tools
Asset Based Community Development –Personal Assets Map
We can think about people’s gifts in three areas:
Gifts of the head – things I know something about and would enjoy talking about with others (eg history, art, music, birds)
Gifts of the hands – things or skills I know how to do and would like to share with other (eg carpentry, sports, gardening, cooking)
Gifts of the heart – things I care deeply about (eg protection of the environment, civic life, children). (20)
COSY CLUB
Barb is a neighbourhood support worker who is employed by Uniting Care
Wesley in Adelaide. A few years ago, Barb was asked to visit Colleanne, a
woman in her early 80s who was experiencing considerable depression after
the death of her husband. In her working life, Colleanne had worked with
socially isolated people, but now she was the one who was lonely and felt
useless. Colleanne made it clear to Barb that she believed that she had nothing
much to look forward to, and frankly, didn’t know what life about at this
stage. Now Barb is not really interested in offering services. Instead, Barb
believes strongly that “everyone has a great story to tell and gifts to share.
We just have to take the time to listen.”
Barb noticed that Colleanne had half a dozen extremely fi ne knitted tea
Resources
St. Luke’s Innovative Resources produce a set of “Strengths Cards” that could be of assistance in helping people to identify their strengths. You could show these cards to a person and ask them to pick the ones that best describe them. You could also use them in a family group or Circles meetings and ask everyone to pick cards that describe themselves and the person in focus. There is also a set of cards called “Age of Adventure” which explores the ways in which older people are still engaged in their communities.
You can order these cards from St. Luke’s Innovative Resources www.innovativeresources.org (22)
Helen Kivnick and Eric Erikson have identifi ed eight psycho-social themes that are a useful way of thinking about people’s strengths.
Strengths1 Hope and Faith2 Willfulness, Independence and Control3 Purposefulness, Pleasure and Imagination4 Competence and Hard Work5 Values and Sense of Self6 Love and Friendship7 Care and Productivity8 Wisdom and Perspective (21)
21
BACK HOME INDEX FORWARD

22
cosies on her sideboard. Not just ordinary tea cosies, but ones with knitted butterfl ies, bees, and gardens on them. About that time, the trendy T Bar had opened in Adelaide. Barb asked Colleanne if she could borrow a tea cosy to show to the T Bar, as she thought they might be interested in selling such wonderful tea cosies. Colleanne agreed, and the T Bar were delighted. They bought some and they sold really quickly. Barb went back to Colleanne, saying that she had found a market for the tea cosies.“Well and good” said Colleanne, “but I don’t really need the money—is there some group in UnitingCare Wesley Adelaide which could do with the donation of the money?”
Barb knew of another worker in the organisation, who was doing a fabulous project with women with an acquired brain injury.These women were getting together to create a quilt, with each panel made by an individual woman. The panels were well under way but the next step was a bit unclear. The worker was most appreciative of the prospect of the donation. Colleanne went to meet the women, and felt really inspired by what they were doing, and in great admiration of their courage in dealing with their disability.
The tea cosies kept selling and Colleanne could not keep up. So Barb put the word out among some other older women who were experiencing social isolation. They became the Cosy Club. They got together once a month to swap patterns. Later they all occasionally joined in with the women with acquired brain injury.
The Cosy Club has become a very active and committed group, supporting various projects and forming lasting friendships. Colleanne and Barb were later asked to present to a National Conference in Sydney to tell the story of the Cosy Club. Colleanne said that she had gone from having nothing to do, from feeling useless, to not having enough hours in the day. Source: UnitingCare Australia & Inspiring Communities (2009) (23)
Roles
An important role for Co-ordinators is that of “reframing”. In this way issues or challenges can be re-interpreted as strengths.
Another meaning or another sense is assigned by reframing a situation or context, thus sees a situation in another frame. A frame can refer to a belief, what limits our view of the world. If we let this limiting belief go, new conceptions and interpretation possibilities can develop. (24)
For example, a person may say: “I’m a terrible procrastinator – I just can’t make a decision”. You can re-frame that by saying: “You are obviously a very careful person and like to weigh up the pro’s and con’s before making a decision. Can I help to provide you with more information to help make your decision?”
You can also elicit the person’s story by asking questions to gain more detail or depth, and check the meaning of what they are saying.
BACK HOME INDEX FORWARD

23
5 FINDING STRENGTHS
Discussion question
How do you handle a situation where a person cannot identify their own strengths? Perhaps they are depressed or grieving, or only want to see the world as “gloom and doom”.
Anthony Robbins points out that:“If we perceive something as a liability, that’s the message we deliver to our brain. Then the brain produces states that make it a reality. If we change our frame of reference by looking at the same situation from a different point of view, we can change the way we respond in life. We can change our representation or perception about anything and in a moment change our states and behaviors. This is what reframing is all about. “ (25)
BACK HOME INDEX FORWARD
24
The appreciative question
Think about a time when you were lacking something important in your life. How did you identify that need? What did others do that was helpful to you?
Rationale
It is important for the Co-ordinator to identify with the service user their most fundamental and urgent needs. The services or supports provided should address these most fundamental and urgent needs in order to be relevant to the person. The service should be in the amount needed, not too much or too little, and delivered in a timely manner.
It is also important to be aware of needs that are universal to all people and those specifi c to a person’s life experiences, frailty or impairment. Particular experiences of discrimination and loss may have an impact that creates a particular need. For example, a person who has moved around frequently may have a greater need for security and stability.
It is also important to recognise that experiences of loss or ageism may impact on a person’s self-confi dence and self-esteem, and their ability or willingness to express their needs. Some people may also have limited experiences of potential alternatives, and as a result, a person may express a need for what they know is available. Therefore, needs do not always equate with a person’s request, and Co-ordinators require the skill of helping a person to discern their real and fundamental needs.
No service can or should address all the needs of a person. Services should be clear about their scope and concentrate on competently addressing needs within that area. (see defi nition of “purview” in Topic 8). However, they should be aware of the other needs of the person and make referrals and/or advocate for these to be addressed by others.
The provocative proposition
While Co-ordinators will take a strengths-based approach to assessment, they will also identify the important needs of the person, both urgent and fundamental. Through conversation with the person and their network, the Co-ordinator will identify what the person wants assistance with, but also what may be needed to ensure their ongoing health and well-being.
6 Understanding needs
BACK HOME INDEX FORWARD
25
6 UNDERSTANDING NEEDS
Vulnerability - capable of or susceptible to being wounded or hurtNeed - a lack of something wanted or deemed necessary (26)
Step-by-step guide
To help discern people’s needs:
• Initially encourage the person to state their beliefs about what they need, trying to frame in the positive (eg “what would be helpful to your situation at present?” rather than “what is wrong with you?”)
• Check the accuracy of your understanding• Explore the needs as seen by others, eg “what does
your doctor think?”, or by asking others who are present
• Check with the person as to whether they agree with the views expressed by others
• You may wish to make suggestions based on your observations or knowledge of the situation. These suggestions may get to needs that are harder for the person to identify or discuss (eg “do you get a bit lonely being on your own here?”, or “how do you manage with your garden?”)
The exploration of specifi c needs around particular conditions may require further discussion at a later visit, or the involvement of a person with specialist skills (eg issues of dementia, mental health or chronic illness).
Tools
Important TO and important FOR
Helen Sanderson draws the important distinction between what’s important TO a person (what makes them happy, content and fulfi lled) from what’s important FOR a person (for their health and safety, their perception of being valued). It is important when discerning needs to fi nd a good balance between the two perspectives. (27)
Health and well-being
Co-ordinators may fi nd themselves needing to raise issues that are “important for” people, but which they may not initiate discussion about. The following checklist will help you think about areas that may need to be discussed to ensure a person can be healthy and safe at home.
Health issues checklist
While taking a wellness focus, Co-ordinators should also consider the possibility of the following issues that may impact on a person’s health and well-being and help to plan ways of addressing these issues.
• Home safety• Nutrition and hydration• Dental health• Medications• Exercise and mobility• Depression and anxiety• Dementia• Falls prevention (see Topic 15)• Emotional and spiritual needs• Isolation and loneliness• Family stress• Chronic disease
Distinguishing between a need and a response to a need
We often confuse a need with what might be a common response to that need. For example, a person does not need a wheelchair, but may need some assistance to move around. If a person has some ability to walk, then this need may be met in various ways, including assistance to walk, physical therapy to strengthen mobility, a wheelchair or a scooter.
Five Whys
One way to identify needs is to use the “Five Whys” exercise. Keep asking the questions “why?” until you get down to the real needs. For example, if a person is identifi ed as needing a “day program”, ask “why” fi ve times
1. Why? Because she has become isolated
2. Why? Because she cannot drive a car
3. Why? Because her husband recently died and he used to drive her everywhere
4. Why can she not go to the places she used to go with her husband? Because she cannot get there and does not feel comfortable going alone
5. Why does she not feel comfortable?
You can see that we have now identifi ed a number of needs that have little to do with going to a day program. A need for autonomy through access to transport, a need for belonging and acceptance, and perhaps a spiritual need relating to her feelings of grief for her husband. A day program may be able to meet some of these needs, but there may also be a range of other possible responses that are more relevant, such as taxi vouchers or a volunteer driver to take her to visit old friends, a regular lunch with some friends who have also been widowed etc.
BACK HOME INDEX FORWARD
26
GETTING TO THE REAL NEEDSKeith is an 86 year old man who lived alone in his own home for 10 years following his wife’s death from cancer. He had a stroke some 5 years ago that meant he needed to walk with a stick
and struggled with verbal communication. Despite this he continued to live at home and tend his beautiful garden that he had built up over the entire period of married life. He has a close relationship with his two daughters and his three grandchildren and 7 great grand children. Highlights of his year include taking part in the ANZAC Day parade and having a family Christ-
mas picnic each Christmas day in the parklands. He has a great love of the outdoors and in the
past taught several pet budgies to talk and sing songs. He was an accomplished tenor, played the mouth organ and before his retirement when he turned 65 years had been a manager in a bottle washing business. He is a member of the RSL and served with the army in the Second World War along with 2 of his 4 brothers all now deceased. He has one surviving sister aged 83 years whom he sees regularly.Keith had a fall in the garden injuring his hip, struggled to get inside his house but before he could call for assistance fell again and could not get up. His daughter found him on the fl oor on driving to the house when he did not answer his telephone. He had broken his hip badly and required hospitalisation. Despite hip surgery he was unable to weight bear. An Aged Care Assessment Team classifi ed him as high care and hospital staff advised that he would need nursing home care. He became very depressed and refused to have physiotherapy treatment and saw himself at the end of his life.His younger daughter was inspirational challenging her father and the service system to see a better life than a nursing home placement which he clearly did not want. She recognised his need to spend time in the outdoors and for companionship at the same time as appre-ciating the reality that he would not be able to continue to live in his own home without a carer. She understood his real needs as well as being able to recognise the needs arising from his disabilities caused by the stroke and fractured hip. She and her partner took him to live with them in their home
Continued on page 27
BACK HOME INDEX FORWARD

27
in the Adelaide Hills and organised the necessary equipment and home modifi cations so that
he did not need to stay longer in respite care while they waited for in home care support
from the community service agency. With his daughter’s persuasion he accepted a visiting
physiotherapy service and with assistance over several months was able to transfer to and
from his wheelchair. He now spends much time in the garden, visits family and old friends
with his daughter in a big old Mercedes and took part in the Anzac Day parade with his
daughter’s partner’s assistance. His other daughter also stays with him to give his carer
daughter and her partner a chance to take a break with trips away for short holidays
or to visit their own daughter in Melbourne. He has a modifi ed but enjoyable life style
with many of the things important to him still part of his life even though he was not
able to return to his own home and garden.
Frameworks to think about needs
Bradshaw (28) identifi es four main categories of need:
Normative need is need which is identifi ed according to a norm (or set standard); such norms are generally set by experts. Benefi t levels, for example, or building standards, have to be determined according to some criterion.
Comparative need concerns problems which emerge by comparison with others who are not in need. One of the most common uses of this approach has been the comparison of social problems in different areas in order to determine which areas are most deprived.
Felt need is need which people feel - that is, need from the perspective of the people who have it.
Expressed need is the need which they say they have. People can feel need which they do not express and they can express needs they do not feel.
Universal Human Needs
Wolfensberger has identifi ed ten areas of human need that are common for everyone. (29)
1. Bodily well-being2. Sense of personal security and safety3. Belonging to and with others4. Valued acceptance, esteem, respect and love by others5. Sexual relations, intimacy and giving and receiving affection6. Mental integrity and stability7. Autonomy, independence and control8. Aesthetic and higher cognitive needs9. Spiritual needs10. Happiness, contentment, felicity
6 UNDERSTANDING NEEDSBACK HOME INDEX FORWARD
28
Roles
The Co-ordinator’s role in understanding people’s real needs goes beyond just asking what the person wants, for the many reasons outlined in this Topic. The Co-ordinator’s skill in understanding the ageing process, as well as their ability to observe and sensitively uncover deeper needs, will ensure that the supports provided are the most relevant to the person’s situation and most likely to help them remain at home and as independent as possible.
“Everybody needs beauty as well as bread, places to play in and pray in where nature may heal and cheer and give strength to the body and soul.”
John Muir
Discussion Questions
How do you raise those tricky areas that people may not have described as a need, for example continence issues, memory loss, mental health issues? What about observations you have made about what might be “important for” the person, such as home safety issues, or personal habits that are damaging to their health?
BACK HOME INDEX FORWARD

29
7 Identifying networks
7 IDENTIFYING NETWORKS
Rationale
Relationships have an enormous infl uence on all people’s happiness, health and well-being. The ageing process can provide both opportunities and challenges in maintaining important relationships.
A co-ordinator should be aware of both the importance of assisting a person to preserve important relationships, and ensuring that the process of service delivery does not damage or displace people who are important to the person being supported.
A Relationship can be a connection, association or involvement; a connection between persons by blood or marriage; or an emotional or other connection between people. (30)
Step-by-step guide
There are two important reasons for understanding the signifi cant relationships in the lives of the people you are supporting:
1. To ensure that they are involved appropriately in the support plan for the person, and that the service does not take over roles that family or friends may be happy to fulfi ll.
2. To ensure that the service can support the maintenance of relationships that are important to the person, given the positive health benefi ts of doing so. This may range from supporting a spouse who is the main live-in carer for a person, maintaining contact with a close friend, or continuing relationships with grand-children.
When working with couples it is also important to consider their interdependence, and the importance of balancing the needs and wishes of both parties.
The appreciative question
Think about the people who are important to you. If you had a crisis or health issue – who would you turn to? Why?
The provocative proposition
Services will engage with relevant members of the person’s network (with their consent) and support the person to maintain important relationships.
BACK HOME INDEX FORWARD
30
Tools
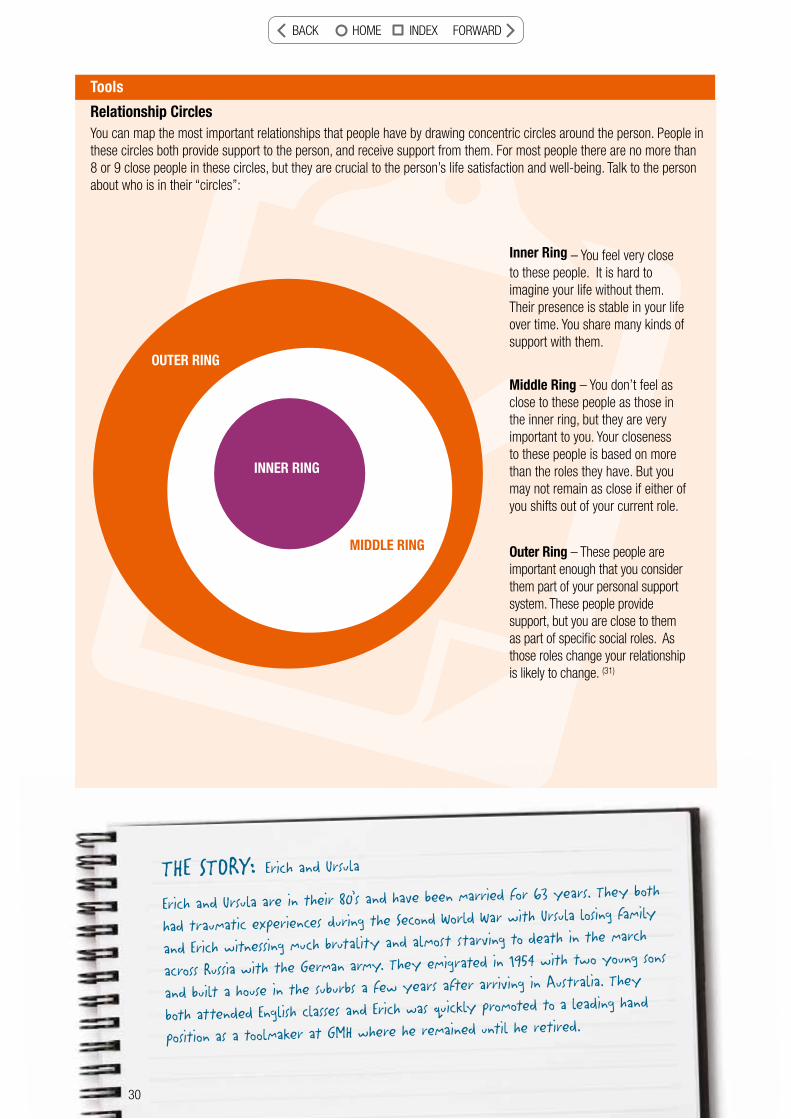
Relationship CirclesYou can map the most important relationships that people have by drawing concentric circles around the person. People in these circles both provide support to the person, and receive support from them. For most people there are no more than 8 or 9 close people in these circles, but they are crucial to the person’s life satisfaction and well-being. Talk to the person about who is in their “circles”:
Inner Ring – You feel very close to these people. It is hard to imagine your life without them. Their presence is stable in your life over time. You share many kinds of support with them.
Middle Ring – You don’t feel as close to these people as those in the inner ring, but they are very important to you. Your closeness to these people is based on more than the roles they have. But you may not remain as close if either of you shifts out of your current role.
Outer Ring – These people are important enough that you consider them part of your personal support system. These people provide support, but you are close to them as part of specifi c social roles. As those roles change your relationship is likely to change. (31)
THE STORY: Erich and Ursula
Erich and Ursula are in their 80’s and have been married for 63 years. They both
had traumatic experiences during the Second World War with Ursula losing family
and Erich witnessing much brutality and almost starving to death in the march
across Russia with the German army. They emigrated in 1954 with two young sons
and built a house in the suburbs a few years after arriving in Australia. They
both attended English classes and Erich was quickly promoted to a leading hand
position as a toolmaker at GMH where he remained until he retired.
INNER RING
MIDDLE RING
OUTER RING
30
BACK HOME INDEX FORWARD
31
7 IDENTIFYING NETWORKS
When their daughter went to high school Ursula started working as a carer of
young people with intellectual disability where she stayed until she retired.
They made life-long friends among the German community. However, only a few
are still alive and even these are not in recent contact due to the effects of
distance, health issues and limited mobility. Erich has been an active member of
the German Association for many years and regularly drinks at the bar with his
friends and associates. Ursula was less interested in the club and spent her leisure
time in art classes and china painting until her eyesight failed. Although she had
eye surgery and her sight was restored she never resumed her china painting.
During this period she suffered pain in her spine, became depressed and depen-
dent on drugs for pain management.
After moving into their current home Ursula became physically frail and struggled
to manage her depression. She now suffers memory loss and lacks the confi dence
to leave her home and is reluctant to visit family for social events and celebra-
tions. When home alone she becomes very agitated and forgets where Erich has
gone even though she is encouraged to write down where he is and when he will
return. Ursula receives home care support and respite.
Erich’s sight deteriorated and by the age of 80 he had only peripheral vision
and was not able to drive. He bought a gopher which he still uses for local shop-
ping, and he is able to take the bus to shopping centres and the city. He enjoyed
reading in his leisure time but can no longer read print even with a magnifying
device. He can see his large screen TV and manages electronic devices mainly
by memorizing the numbers and position of the buttons. Erich still goes to the
German Club to drink with his mates and watch the races on Saturdays when
his daughter, Anna is available to spend the afternoon with Ursula. Anna was
recently overseas and Erich became quite frustrated with not being able to get
out on Saturdays He suggested that Ursula could no longer manage and that they
should be looking at nursing home care for her. Anna had arranged for a respite
carer to be available on Saturdays but Erich refused the service saying that he
didn’t like carers in the house on the weekends. His son Hans visited from Sydney
one weekend and took Erich to the German Club. It emerged from the conversa-
tion that the real reason for not accepting the service was that he was not com-
fortable with the idea that a paid service was put in place so that he could go
out drinking. When Anna returned from overseas she again discussed possibilities for
support with the aged care coordinator and they worked out a new proposition.
A carer would come on Saturdays to take Ursula on a social outing or for a walk
to improve her fi tness and mobility. When the goal of the service was framed in
these terms this was seen by Erich as acceptable and he was able to resume his
trips to the German Club.
31
BACK HOME INDEX FORWARD
32
Roles
Co-ordinators cannot be family therapists, but can respect the importance of relationships in co-ordinating the support for a person. If the family relationships are complex or confl icting, you may want to consider a referral to a service that specializes in family counseling or mediation. Co-ordinators can also be alert to people who seem lonely or isolated, and consider how they can help to build a person’s networks when planning their support (see Topics 14 & 19).
Discussion question
Do you sometimes fi nd people in the network of the person you are supporting that you do not consider helpful to the person? It may be an interfering neighbour or a relative who seems abusive or aggressive. How do you handle these situations? Are relationships ever all good or all bad? Should such relationships be preserved?
“…good relationships do more than make us happy; they make us healthy. Scientists have demonstrated that being in close, positive relationships can improve physical health by countering stress and producing feelings of calm. These relationships can even prevent chronic health conditions in later life.” Source: Skeie et al (32)
A Maori Proverb - WHAKATAUKI (33)
“Let us be grateful to people who make us happy; they are the charming gardeners who make our souls blossom.” Marcel Proust.
Hutia te rito o te harakeke
Kei hea te komako e ko? Ki mai ki ahau
He aha te mea nui o tenei ao?
Maku e ki atu He Tangata! He Tangata! He Tangata!
If the centre of the fl ax is pulled out (and the fl ax dies) Where will the Bellbird sing? If you were to ask me What is the most important thing in the world? I would reply It is People! It is People! It is People!
BACK HOME INDEX FORWARD

33
8 Clarifying purpose
8 CLARIFYING PURPOSE
The appreciative question
Think about a time when you were grateful that someone was very honest with you about what they could and could not do to assist you? How did this help you at the time?
Rationale
It is important that the service does not create unrealistic expectations, but also that people are aware of the support available. The service should also be clear about the period of time for which the service might be available, and under what circumstances the service could cease.
Co-ordinators should encourage the person to take an active role in arranging their supports, and utilize a restorative approach to maximize their health and well-being.
The provocative proposition
Services will be clear about their role and what they can and cannot do for and with the person. Co-ordinators will also be clear about the approach that they are planning to take, such as encouraging independence, self direction and restoration of health where possible. The Co-ordinator’s role will be purposeful and goal-directed.
Purview - The “purview” of a service is the scope or limit of infl uence, authority, competence, responsibility or concern in the lives of service recipients that would generally be perceived as the appropriate and/or properly delegated one for a particular service. (34)
Restorative - Tending to impart new life and vigor to; invigorating - imparting strength and vitality; promoting recuperation; healthful - conducive to good health of body or mind (35)
Step-by-step guide
Being clear about the limits of the serviceIn order to avoid confusion and possible disappointment, the Co-ordinator should be very clear up front about what the service can and cannot do with the person. This should not pre-empt the discovery and dreaming stages, nor limit possible creativity, but rather create the boundaries within which you can work together. Factors that may need explanation are:
• What your role is and the limits of your authority
BACK HOME INDEX FORWARD
34
Step-by-step guide - continued
• Who is funding the services and the eligibility criteria• How family and friends can be involved• Any time limits for the service• The criteria for discontinuing the service• Roles and responsibilities of the person receiving services• Complaints mechanisms• The availability of independent advocates• The range of services available from your organization and other services in the community.
Duty of Care
The law imposes a duty of care on everyone (carers, the general public etc.). This is a duty to take reasonable care and avoid injury to other people or damage to property as a result of our action or inaction. There is a duty not to be careless, by taking reasonable steps to avoid harm, while supporting sensible risk-taking relevant for each individual.
In cases of professional negligence involving someone with special skill, that person is expected to show the skill of an average member of that profession. In working with people there is a need, through planning, to minimize possible harm. It is not possible to eliminate risk, only to formulate strategies to minimise it. Allowing someone to undertake or engage in a risky activity does not make you negligent. Failing to take any steps to minimise foreseeable harm could be. This is called the “dignity of risk”. (36)
Roles
In general terms, the more vulnerable a person and the less informal supports they have, the greater the role a service is likely to play in their lives (or the wider the “purview”).
Tools
Resolving ethical dilemmasSome questions to help you resolve ethical dilemmas that may have a duty of care component:
• What are the foreseeable risks in this situation? • What are the spiritual and cultural values of the
participant?• Do I understand and respect the views of both the
participant and their signifi cant others?• What impact does this issue have on the participant,
who has rights, dignity, and a hope for a better life?• What are my values?• Are my values in confl ict with those of the
participant?• Am I imposing my own values on the participant?• What circumstances affect the participant and/or
the participant’s family?• What is the social and health status of the
participant, and what other related factors may infl uence the situation?
• Do any of the stakeholders involved in the particular situation have a particular investment in the outcome because they have a special need, or because we have particular obligations to them?
• What are the professional values and standards applying to my role?
• What are the values and code of conduct of my organisation that are relevant to this situation?
• Which laws, if any, are relevant to this issue?• What is my legal duty of care?
The Optimal Solution
In navigating any ethical dilemma, the Co-ordinator should seek to combine all of the above considerations in order to help them determine the optimal solution for that particular situation. This optimal solution is arrived at by simply selecting the option with the highest overall ethics quotient and that produces the best possible outcome for those involved. (37)
BACK HOME INDEX FORWARD

35
8 CLARIFYING PURPOSE
Discussion question
What do you do when you are faced with a situation where the person you are working with has needs that are clearly beyond the scope of the program you are working in?
Case Management Standards
Guiding principles (p6)3. Case Management is Purposeful
The actions of Case Managers must address the specifi c needs of Clients as documented in the Client’s goals. The interventions used should be in line with the best evidence available that show they can meet the Client’s needs. Case management must balance Client needs with the available resources by assisting Clients in the selection of services and resources that are of the highest possible quality within the accessible range of services.
In order to link clients with the most appropriate services and resources, the Case Manager must be aware of their own limitations in terms of their
knowledge and experience. Case Managers will refer Clients to specialists who have skills and knowledge beyond those of the Case Manager.
4. Case Management promotes sustainable solutions
Case Managers endeavour to move through crises to develop sustainable solutions for Clients. Sustainability is achieved when the Case Manager works with the Client to implement a plan of care that:
• Fits within the available resources of Clients, families, programs and funding bodies;
• Addresses current needs and probable future needs; and
• Moves beyond crises to sustainable solutions. (3)
“Our duty is to encourage every one in his struggle to live up to their own highest idea, and strive at the same time to make the ideal as near as possible to the Truth.” Swami Vivekananda
hat do you do when you are faced with a situation where e person you are working with has needs that are clearly yond the scope of the program you are working in?
BACK HOME INDEX FORWARD
36
9 Understanding culture
The appreciative question
Think about the elements of your background and upbringing that make you unique? How do you remain connected to the traditions and beliefs that are important to you?
Rationale
Co-ordinators need to be aware of how their own cultural background infl uences their preferences and decision-making, and the importance of providing culturally sensitive services in order to effectively meet the needs of people from other cultures. Services must be provided without discrimination and with the appropriate supports, such as interpreters.
The provocative proposition
Co-ordinators will be sensitive to the cultural background of the person being supported, and how this impacts on their ability to communicate, their preferences for how they are supported, and the role of their family and informal support network. They will also consider the cultural impact on food choices, appropriate leisure activities and the role of spiritual support.
Culture - the totality of socially transmitted behavior patterns, arts, beliefs, institutions, and all other products of human work and thought.Discrimination - treatment or consideration of, or making a distinction in favor of or against, a person or thing based on the group, class, or category to which that person or thing belongs rather than on individual merit. (38)
BACK HOME INDEX FORWARD
9 UNDERSTANDING CULTURE
Step-by-step guide
The following is a list of considerations when providing culturally appropriate support:
Communication • Effective communication is crucial to the physical
and emotional well-being of the person being supported
• Provide information in the person’s language – written or verbal depending on their literacy.
Interpreting• Use professional interpreting and translating
services (do not rely on family and friends)• This is especially important for assessment and
care planning• It is crucial if informed consent is required
Use of bi-lingual staff• This is to be encouraged but always check the
person’s preferences (it may not always be appropriate in small communities)
• Explore the availability of bi-lingual volunteers to provide social support.
Health and personal care• Ensure all health and personal care plans and
reviews identify and support the cultural, linguistic and spiritual needs of care recipients
• Provide information about health and personal care services - including information on specifi c procedures that may be unfamiliar to care recipients - in the preferred language of care recipients and their families
• Consult care recipients and their families regarding the infl uence of culture and religion on health and personal care services
• Consult care recipients and their families regarding whether or not open discussion of diagnosis and prognosis is appreciated - and balance this with legal requirements around issues of informed consent
• Establish the cultural and religious impact on the acceptability of certain treatments and medications
• Ensure family members’ role in decision-making about care has been clearly established and documented
• Ensure an effective communication strategy is in place to address medical and other emergencies for care
recipients from culturally and linguistically diverse backgrounds
• Consider the cultural, linguistic and spiritual needs of care recipients when referrals are made to external health service providers, and ensure they use accredited interpreting services as required
• Provide care recipients with a choice of bilingual health practitioners and pharmacists where possible
• Support your care recipients’ right to access complimentary or traditional therapies, and assist them to make informed choices
• Ensure that the staff responsible for the provision of health and personal care have been trained in cultural awareness, appropriate communication and the correct use of telephone and on-site interpreting services.
Dementia• Ensure that people with dementia and their families
are aware of the dementia support services available through Alzheimer’s Australia.
Cultural awareness• Understand how a person’s culture may inform their
values, behaviors, beliefs and assumptions. • Utilize the resources available to understand more
about the particular culture of the person you are working with, for example. Source: Centre for Cultural Diversity (39)
Discrimination• Be aware of both the moral and the legal obligations
to avoid discrimination on the grounds of the culture or language of the person
• Although there may be culturally specifi c aged care services, everyone has the right to access
mainstream services.th of
s
mainstream services.
37
BACK HOME INDEX FORWARD

38
Tools
Thinking about Indigenous Elders
There are specifi c cultural factors to be considered when working with Indigenous elders and their communities:
• The person you are working with has a choice in deciding which personal information is provided. Respect that it is their life story that you are learning about.
• Don’t ask information that you don’t actually need to know.
• Don’t make assumptions.• The right environment is crucial. Take care that you
meld into the person’s choice of environment so that they can take the lead.
• Work with the person and their family to maintain as much independence as possible. Show respect for the person’s family.
• If possible, buddy up with a worker who has knowledge and experience of the person’s culture.
• Don’t tell the person what YOU think they need (ie don’t put words into their mouths).
• Use simple language – avoid jargon and acronyms.• Remember that you are having a conversation,
not conducting an interrogation!
Remember that many Indigenous older people have experienced signifi cant losses and traumas, and it is important that the service does not contribute to any further losses. (40)
Resources
Centre for Cultural Diversity in Ageing www.culturaldiversity.com.au
Case Management Standards
Ethical principles
The Case Manager must operate without discrimination or harassment to others. (3)
Discussion question
How do you approach a situation where you are confronted with cultural practices that you do not necessarily agree with?
“If we spent as much time trying to understand behaviour as we spend trying to manage or control it, we might discover that what lies behind it is a genuine attempt to communicate”. (41)
38
confrontenecessar
BACK HOME INDEX FORWARD
39 39
Identify what might beHave a vision for the future
Planning supports for people in the community should be based on what is important to them, both now and in the future. The services or informal supports can then be designed in the next stage to support that lifestyle. The Dream stage is about encouraging the person to think about the future, based on what they have enjoyed or accomplished in the past, rather than focussing on perhaps a recent event that has led them to need your support.
39
BACK HOME INDEX FORWARD
40
10The appreciative question
Think about a time when you were able to articulate to someone your dreams in life and what was important to you. What happened as a result of that?
Rationale
Now that you have come to know the person and built rapport, it is important to develop a support plan with the person that builds on this knowledge to identify their goals and preferences, and how your support can assist them to achieve these.
The provocative proposition
The person will be decidedly infl uential in planning the supports they require to be able to live a full and purposeful life in the community. They will be encouraged to talk about their aspirations.
Life purposeLiving a life of passion and signifi cance requires knowing what your defi nite purpose in life is. Defi ning and living your life purpose gives you an overwhelming sense of fulfi llment and meaning to your existence because it provides a way for you to use your values and passions and directs them towards a meaningful objective. Your life purpose is the essence of who you are as a person. Once you know what your purpose in life is, you will be able to wake up each morning knowing that every action that you take that day will move you one step closer towards your ultimate purpose in life.The Components of Life Purpose Often people confuse their life purpose with their profession or their various roles in life (i.e. mother, father, husband, wife, etc.). While your profession or role can serve as the vehicle through which you can reach your life purpose, your professional title or role is not in and of itself your purpose in life. Knowing what your purpose in life is motivates you towards ultimate achievement and enables you to live a passionate life. Life purpose is made up of two important components: Core values and associated passions. To fi nd your purpose, use the following formula:Core Values + Associated Passions = PurposeCore values. These are the fundamentally beliefs, morals, and standards that defi ne you as a person and which guide your behavior. While other aspects of your life change, your core set of values do not change. Core values are what you tell a person who asks you, “What do you stand for in your life?”Associated Passions. Associated passions are the vehicles by which you can fully express and share your core values. They are the things that you love to do in life. They can also be specifi c talents, skills and abilities that you possess which fully express the associated value. They can also include things that you have never tried before, but have a desire to experience someday. (42)
Being frail or having a disability does not mean that life no longer has purpose. However, we may need to assist people to see how they can live out their core values and pursue their passions within their physical or cognitive limitations.
Planning a response
BACK HOME INDEX FORWARD
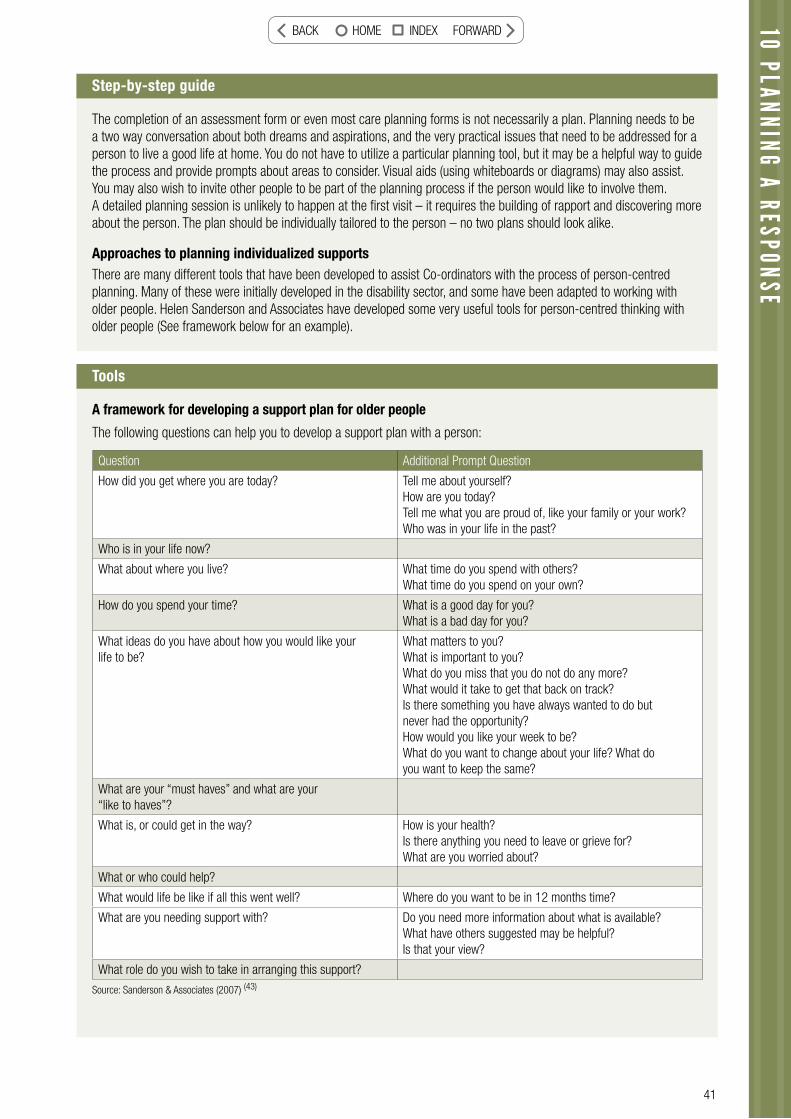
41
10 PLANNING A RESPONSE
Step-by-step guide
The completion of an assessment form or even most care planning forms is not necessarily a plan. Planning needs to be a two way conversation about both dreams and aspirations, and the very practical issues that need to be addressed for a person to live a good life at home. You do not have to utilize a particular planning tool, but it may be a helpful way to guide the process and provide prompts about areas to consider. Visual aids (using whiteboards or diagrams) may also assist. You may also wish to invite other people to be part of the planning process if the person would like to involve them. A detailed planning session is unlikely to happen at the fi rst visit – it requires the building of rapport and discovering more about the person. The plan should be individually tailored to the person – no two plans should look alike.
Approaches to planning individualized supportsThere are many different tools that have been developed to assist Co-ordinators with the process of person-centred planning. Many of these were initially developed in the disability sector, and some have been adapted to working with older people. Helen Sanderson and Associates have developed some very useful tools for person-centred thinking with older people (See framework below for an example).
Tools
A framework for developing a support plan for older people
The following questions can help you to develop a support plan with a person:
Question Additional Prompt Question
How did you get where you are today? Tell me about yourself?How are you today?Tell me what you are proud of, like your family or your work?Who was in your life in the past?
Who is in your life now?
What about where you live? What time do you spend with others?What time do you spend on your own?
How do you spend your time? What is a good day for you?What is a bad day for you?
What ideas do you have about how you would like your life to be?
What matters to you?What is important to you?What do you miss that you do not do any more? What would it take to get that back on track?Is there something you have always wanted to do but never had the opportunity?How would you like your week to be?What do you want to change about your life? What do you want to keep the same?
What are your “must haves” and what are your “like to haves”?
What is, or could get in the way? How is your health?Is there anything you need to leave or grieve for?What are you worried about?
What or who could help?
What would life be like if all this went well? Where do you want to be in 12 months time?
What are you needing support with? Do you need more information about what is available?What have others suggested may be helpful? Is that your view?
What role do you wish to take in arranging this support?
Source: Sanderson & Associates (2007) (43)
BACK HOME INDEX FORWARD

42
Tools - continued
Resources and strengthsDr. Helen Kivnick has developed an approach known as “Vital Involvement in Old Age” (44). This focuses on the strengths and resources that older people have that can be utilized to address the issues they may face in relation to frailty or ill health. Rather than focusing on problems, which may actually exacerbate ill health, this approach utilizes people’s strengths to enhance their quality of life. Vital involvement is a person’s meaningful engagement with the world, where people use their capacities and make contributions of value.
The fi gure below describes domains of life and health in terms of two axis. One is a continuum from negative to positive, that is from weakness, illness and problems in one direction to strengths, wellness and assets in the other direction. The second axis is the continuum from the individual to their environment.
So Quadrant 1 would include individual symptoms and conditions (such as disability, disease or injury). Quadrant 2 would include individual strengths and assets (such as reasonable stamina, optimism, lifelong engagement in physical exercise). Quadrant 3 includes environmental strengths and supports (such as social networks, available transport, accessible housing, community resources) and Quadrant 4 includes environmental obstacles and stressors (such as the ill health of a carer, extremes of weather, lack of needed equipment in the home).
In vital involvement practice, Co-ordinators seek not just to address people’s individual and environmental issues to move them to the mid-point of the axis so they can just “survive” day to day, but rather to a point where they can continue those activities that provide meaning to their lives. In addition, the strengths of the person and their environment are utilized to help address the issues that are preventing such engagement.
Roles
In the process of planning, the role of the Co-ordinator is one of facilitation, which literally means to “make things easier” for a person. You do this by asking the right questions and leading people through a process that enables them to discover what their goals and preferences are, and what sort of support will help them to live a full life. You may also provide information about what is possible, or encourage people to “think outside of the square”.
1 3
2 4
LIFE AND HEALTH DOMAINS
PROBLEMSRISKSBARRIERS
STRENGTHSASSETS
ABILITIESSUPPORT
PERSON
ENVIRONMENT
PERSONAL PROBLEMS:
RISKS
PERSONAL STRENGTHS:SUPPORTS
ENVIRONMENTAL PROBLEMS:
RISKS
ENVIRONMENTAL STRENGTHS:SUPPORTS
+-
Source: Kivnick & Stoffel (45)
BACK HOME INDEX FORWARD
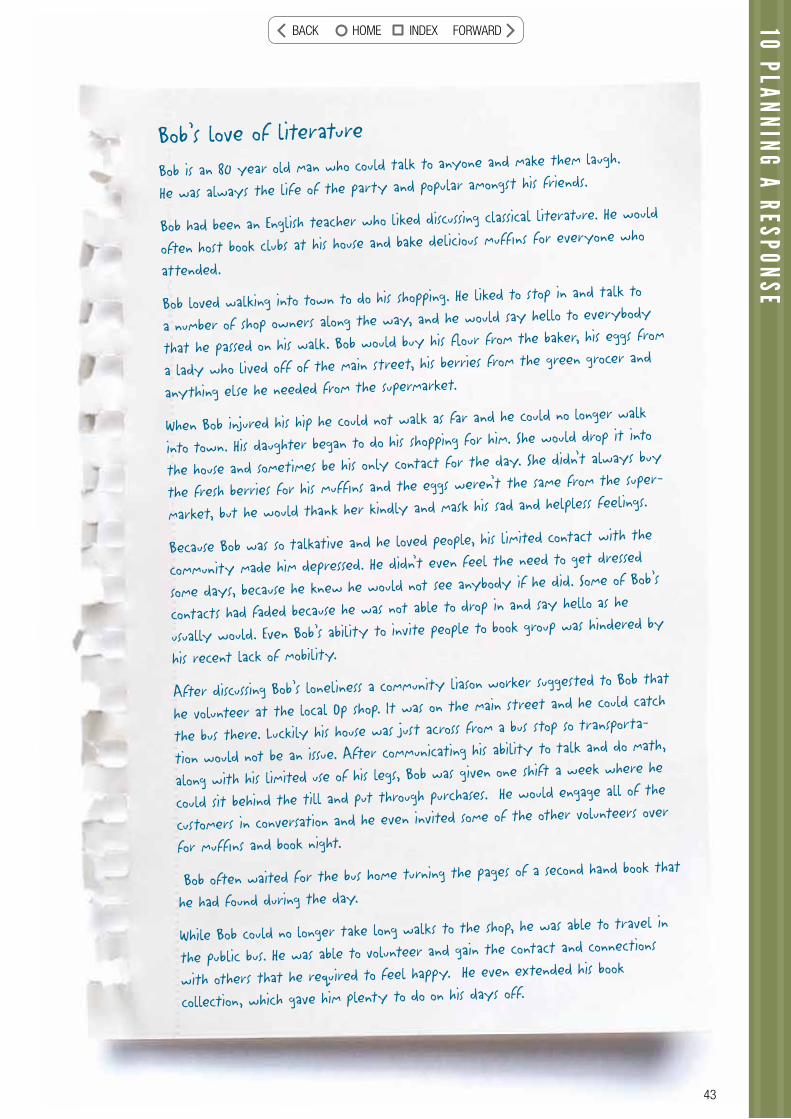
43
10 PLANNING A RESPONSE
Bob’s love of literature
Bob is an 80 year old man who could talk to anyone and make them laugh.
He was always the life of the party and popular amongst his friends.
Bob had been an English teacher who liked discussing classical literature. He would
often host book clubs at his house and bake delicious muffi ns for everyone who
attended.
Bob loved walking into town to do his shopping. He liked to stop in and talk to
a number of shop owners along the way, and he would say hello to everybody
that he passed on his walk. Bob would buy his fl our from the baker, his eggs from
a lady who lived off of the main street, his berries from the green grocer and
anything else he needed from the supermarket.
When Bob injured his hip he could not walk as far and he could no longer walk
into town. His daughter began to do his shopping for him. She would drop it into
the house and sometimes be his only contact for the day. She didn’t always buy
the fresh berries for his muffi ns and the eggs weren’t the same from the super-
market, but he would thank her kindly and mask his sad and helpless feelings.
Because Bob was so talkative and he loved people, his limited contact with the
community made him depressed. He didn’t even feel the need to get dressed
some days, because he knew he would not see anybody if he did. Some of Bob’s
contacts had faded because he was not able to drop in and say hello as he
usually would. Even Bob’s ability to invite people to book group was hindered by
his recent lack of mobility.
After discussing Bob’s loneliness a community liason worker suggested to Bob that
he volunteer at the local Op shop. It was on the main street and he could catch
the bus there. Luckily his house was just across from a bus stop so transporta-
tion would not be an issue. After communicating his ability to talk and do math,
along with his limited use of his legs, Bob was given one shift a week where he
could sit behind the till and put through purchases. He would engage all of the
customers in conversation and he even invited some of the other volunteers over
for muffi ns and book night.
Bob often waited for the bus home turning the pages of a second hand book that
he had found during the day.
While Bob could no longer take long walks to the shop, he was able to travel in
the public bus. He was able to volunteer and gain the contact and connections
with others that he required to feel happy. He even extended his book
collection, which gave him plenty to do on his days off.
43
BACK HOME INDEX FORWARD

44
Case Management Standards
Standard two – PlanningGuidelines:
Case Managers are expected to:
2A Provide clients with appropriate information relating to their identifi ed needs, supporting the client’s ability to make informed decisions.
2B Develop Client’s decision-making abilities and independence skills to foster personal growth.
2C Evaluate any barriers that may restrict the Client’s ability to meet the expected goal and determine strategies to minimise the impact of barriers.
2D Develop and implement a plan that is within the fi nancial resources available to support the Client.
2E Document Client goals (including measurable criteria) to determine the effectiveness of the interventions provided.
2F Use collaboration to generate innovative responses to meet Client needs where immediate solutions are not available.
2G Refl ect and operate in an ethical manner as per the CMSA Ethical Principles. (3)
Discussion question
Have you ever had situations where it is diffi cult to engage a person or their networks in the planning process? How could you describe the benefi ts of planning to a person?
“The purpose of life is a life of purpose.” Robert Byrne
BACK HOME INDEX FORWARD
45
11 Creative options
The appreciative question
Think about a time when you felt “stuck” in dealing with an issue and someone was able to look at the situation in a totally different way. How did that help you to fi nd a constructive way out of your situation?
The provocative proposition
The Co-ordinator demonstrates the ability to make exceptions, minimise bureaucratic processes, and shows fl exibility and creativity in meeting individual needs. Service recipients are encouraged to question service practices when they are unnecessarily restrictive or rigid.
11 CREATIVE OPTIONS
Rationale
Services can have a tendency to propose standardised solutions to issues facing service users which can prevent individualised solutions being crafted. Factors not relating to the needs of the person (such as staff, funder or organisational needs) can gain priority over the service user’s needs. This area of quality requires services to be fl exible and creative in meeting the needs of service users and overcoming the barriers that may prevent this from occurring.
Creativity The ability to transcend traditional ideas, rules, patterns, relationships, or the like, and to create meaningful new ideas, forms, methods, interpretations, etc.; originality, progressiveness, or imagination.
Step-by-step guide
To encourage creative responses:
• The service enables creativity at an individual level in response to needs and does not have unnecessary restrictions that inhibit individuality
• Each set of circumstances will be given due regard at all times• The service encourages innovation and creativity with due attention to risks • Processes are in place to ensure service recipients feel free at all times to question service practices when they
perceive them to be unduly rigid or restrictive• Co-ordinators look for the possibilities rather than the barriers • Staff are able to challenge unnecessary restrictions within the service.
BACK HOME INDEX FORWARD
46
Tools
Tools
Creative Thinking CardsOne tool that can help your creativity is the Creative Whack Pack of cards. Each card gives you a different strategy to look at an issue or situation in a new way. Try it when you are stuck! (48)
There are many similar tools available free on the web. www.innovationtools.com (49)
The Six Thinking Hats (or modes) - De Bono (46)
It is a simple, technique that helps people become more effective. You can learn how to separate thinking into six distinct categories. Each category is identifi ed with its own colored metaphorical “thinking hat.” By mentally wearing and switching “hats,” you can easily focus or redirect your thoughts or your conversation. You will need all six hats in the process of working with a person, but in this section we want to highlight the need to sometimes put on the “green hat” and forget about the others (like the black hat telling you something is not possible or not allowed!) to help stimulate your creativity to tackle complex issues.
The White HatThe White Hat calls for information known or needed.
The Red HatThe Red Hat signifi es feelings, hunches, and intuition.
The Black HatThe Black hat is judgment—the devil’s advocate or why something may not work.
The Yellow HatThe Yellow hat symbolizes brightness and optimism.
The Green HatThe Green hat focuses on creativity: the possibilities, alternatives, and new ideas.
The Blue HatThe Blue Hat is used to manage the thinking process.
Within Edward de Bono’s Six Thinking Hats process, Green Hat Thinking focuses on creativity & innovation: possibilities, alternatives, solutions, new ideas. Green Hat Thinking pro-vides a specifi c time that is dedicated to creative thinking and innovation. Green Hat Thinking helps us fi nd new ways of doing things, and it also provides an opportunity to think about ways to overcome concerns identifi ed during Black Hat Thinking.
Green Hat Thinking may be used on its own or within a Six Thinking Hats sequence where the hats are used in a particular order to thoroughly explore a subject.
The Ten Minute MeetingThis is a technique to engage your colleagues in helping you with an issue without taking up a lot of their time. This kind of conversation may happen in your organization already over a cup of tea, but you can also utilize it to help generate creative responses. Ask a few colleagues if they can meet with you for 10 minutes. Spend a minute outlining the situation you are facing, and then ask each one in turn to make a suggestion or ask a question. The purpose is not to evaluate each suggestion, but to get a list of ideas to follow up (it may help to have a whiteboard). When you have your list, thank your colleagues and take the list away to think about.
Types of Creativity (47)
Fluency - The ability to generate a number of ideas so that there is an increase of possible solutions or related products.Flexibility - The ability to produce different categories or perceptions whereby there are a variety of different ideas about the same problem or thing.Elaboration - The ability to add to, embellish, or build off of an idea or product.Originality - The ability to create fresh, unique, unusual, totally new, or extremely different ideas or productsComplexity - The ability to conceptualize diffi cult, intricate, many layered or multifaceted ideas or products.Risk-taking - The willingness to be courageous, adven-turesome, daring -- trying new things or taking risks in order to stand apart.Imagination - The ability to dream up, invent, or to see, to think, to conceptualize new ideas or products - to be ingenious.Curiosity - The trait of exhibiting probing behaviors, asking and posing questions, searching, being able to look deeper into ideas, and the wanting to know more about something.
BACK HOME INDEX FORWARD

47
MORE THAN ONE WAY TO SKIN A CATI called on Mrs Gordon at home following her discharge from hospital and was greeted by her
grandson who shares the home with her. She was lying in bed with her quilt covered in a
confusion of papers; unpaid bills, mail and documents. It was obvious that Mrs Gordon was still in
a lot of pain and the medication had made her slow thinking and vague. She certainly struggled
to get a handle on why I was there and what I was able to do to support her.
In order not to add to her confusion I tried to explain as succinctly as possible that my
involvement in her life was to assist her to regain her health status and support her in her
rehabilitation after a longish stint in hospital. Together we were able to establish that her
most pressing needs were to have assistance with showering as she was struggling to walk, some
equipment to help her in her day to day home life, along with some help cleaning. She was most
adamant about the cleaning as she was feeling very out of control in her usually spotless house.
With all of the paperwork at hand, the house was in disarray; the cupboards were cluttered with
foodstuffs, the fl oors were unswept and the carpets were littered with lint and grime.
Her grandson Jake had done his best but to quote Mrs Gordon, ‘Men don’t seem to see a mess’.
Her grandson had looked after his own space and done the washing and that was about it. It was
obvious however in talking with Jake that he was very concerned about his grandmother with
whom he had lived since he was a baby. He had organised a bell system so that his grandmother
could ring for him if she needed anything.
So the home help services commenced and over time, with adjustments to her medication coupled
with Mrs Gordon’s determination, an attribute that I grew to see was part and parcel of this stoic
country lady, her health status improved.
Over time the home returned to its original state of tidiness and order, refl ecting the way
that Mrs Gordon operated. Very quickly I discovered that she had been an astute business
woman employing a wide range of people on her rural property. She told me that she had been
supportive of young employees who needed a bit more nurturing and tried to be fair and give
people a go.
It was for this reason that she was anxious about her grandson Jake who was on the cusp of leaving
his teen years behind, but who was to this date unemployed. Jake spent most of his days lounging
around at home with a steady stream of ‘mates’ joining him in idleness. He didn’t have his driver’s
licence and before her illness Mrs Gordon had been accompanying him on his endless drives to
strengthen his driving experience.
It was obvious that if Jake’s situation improved Mrs Gordon would also be at a better place
emotionally. The fi rst thing we discussed was the driving. To assist Mrs Gordon a volunteer was
organised who spent some time joining Jake on his drives and freed up some time for Mrs Gordon.
It took some time but with the volunteer and the services of a driving instructor Jake gained his
licence. This was a huge step and meant that he could now begin looking for a job.
11 CREATIVE OPTIONSBACK HOME INDEX FORWARD
48
Mrs Gordon’s upbringing and own work ethic meant she could not rest with her grandson only
getting occasional seasonal work and being fi nancially abused by unscrupulous employers. It
was determined that Jake needed gainful employment. I spoke to people I knew
in a range of
industries but to no avail – it seemed the timing and economic down turn meant jobs were not
easy to fi nd. However it was a casual conversation with a colleague about the problem of Jake
that changed the tide. She knew someone who was employing people for his business and
was
not having success with prospective candidates.
I visited Mrs Gordon and Jake and talked about the prospect of full t
ime employment. I
communicated that it was imperitive that Jake convey to the prospective employer that he was
keen and committed. The rest is history - Jake grabbed the opportunity at hand and has now
been employed for six months. His self worth and esteem have lifted as he has been given more
and more responsibility within the job. He had shown aptitude and initiative and his grandmother
has expressed the thrill of seeing him organise himself each night for the day ahead ie getting
tools ready and lunch packed, going to bed early as he needed to rise early, sharing driving with
other employees while still doing the washing for her much more frequently. Jake loves his job
and enthusiastically shares with his grandmother about his daily tasks and this connection has
made them closer than ever.
Mrs Gordon now goes out each week to a Club which she loves. She told me she looks forward to
meeting her friends at the Club and has been propagating pla
nts to give away there. Her health is
now an exciting mix of contentment and challenge. As the situation with Jake changed so has Mrs
Gordon. Life for her has never been better.
Roles
While a Co-ordinator has a duty of care to ensure a sensible response to a person’s needs, they also have a responsibility to think laterally to fi nd ways around issues. They may also need to advocate for the person when unnecessary bureaucratic restraints or rules are inhibiting the ability to meet the person’s needs.
Case Management Standards
2. Case Management advocates for client rightsCase Managers advocate (when needed) for the rights of Clients within the funding and legislative frameworks that affect the relationship between the Client, service providers and payers. This is achieved through an effective relationship with the Clients, where the Case Manager assesses and develops the ability of the Client to advocate for themselves.
Discussion question
How do you approach a situation where you and the person you are working with have come up with a creative solution to the situation you are facing, but this solution falls outside of your service’s guidelines?
CCCCCrrrrreeeeaaaatttttiiiiivvvviiiitttttyyyyyyy iiiiisssssss ttttttthhhhhhheeee aaaaabbbbbiiiiillllliiiiittttttyyyyyyy ttttttooooo mmmmmaaaakkkkkeeee ssssooommetthhiing original, to imagine things that ativity is the ability to look dddddddooooonnnnn’’ttttt eeeexxxxiiiissstttt, aandd to come up with new ideas. Creativity is the ability to look
ay items and events in new ways. Creativity can make common at everyday items and events in nthings special and special things more common! (50)
BACK HOME INDEX FORWARD
49
12 Consider the Person’s Roles
The appreciative question
Think about the most important roles you have in your life. What privileges do these roles bring? What responsibilities do they imply?
The provocative proposition
The Co-ordinator recognises the importance of valued roles and provides support for the people they are working with to defend, maintain and enhance existing values roles, and to fi nd new valued roles in the community that are consistent with their identity, age and gender.
Rationale
Roles provide a place for people in society and it is more likely that those with positive roles will be afforded other “good things” in life. Roles will infl uence many other aspects of a person’s life and without positive roles service recipients can easily fall into negative roles.
Research indicates that being productive and contributing are important for older people. (51)
Ikigai – Japanese term “that which most makes ones life seem worth living” (52)
Social RoleA social role may be viewed as a combination of behaviours, functions, relationships, privileges, duties and responsibilities that are socially defi ned, are widely understood and recognised within a society, and are characteristic and expected of a person who occupies a particular position within a social system.(53)
Step-by-step guide
Helping people to plan ways to support valued roles means:
• pursuing valued roles and friendships within the community as a priority, rather than just doing activities and fi lling time;
• pursuing the most valued roles that are realistically achievable based on each person’s interests;• setting standards high, stretching to accomplish more and not settling for what is easy or convenient;• challenging negative stereotypes and prejudices by proving them wrong through practical example;• pursuing social inclusion and individualized support rather than segregation and group activities;• helping people to have meaningful lives that enable them to pursue their interests and passions;• having high expectations of what is possible for people, despite frailty, disability or cognitive impairment;• helping people to make their own decisions, maximizing their independence and autonomy;• talking about the barriers and fi nding ways to overcome them;• being an empowered and valued part of the community, not just being physically present.
Source: Ramsay (2007) (54)
12 CONSIDER THE PERSONS ROLESBACK HOME INDEX FORWARD

50
Tools
Discussion question
How do you think about roles for people who are very limited in their physical and cognitive capacity?
“All the world is a stage, And all the men and women merely players. They have their exits and entrances; Each man in his time (sic) plays many parts.”William Shakespeare
Think about how you might support a person’s current roles, or fi nd new roles in the areas of:
a. relationships – parent, sibling, grandparent, friend, neighbourb. work or volunteering (see Bob’s Love of Literature, Topic 10)c. education – teacher, student or mentord. recreation and leisure, hobbies – bowler, patchworker, swimmer, art appreciatore. public life – citizen, voter, activist, council memberf. religious or belief systems – congregation member, organist, philosopher.
Remember valued roles are possible even when someone’s physical or cognitive abilities are quite restricted. There are “being” roles as well as “doing” roles. Some roles will have a greater infl uence on a person’s life than other roles.
We also need to be careful to avoid negative roles that are common for older people, such as child roles, sickness roles, the role of being a burden or incompetent.
Roles are conveyed through a number of means including the places where people are seen, the people and groups they mix with, the language used to talk about or with them, the activities they participate in and their personal appearance.
BACK HOME INDEX FORWARD
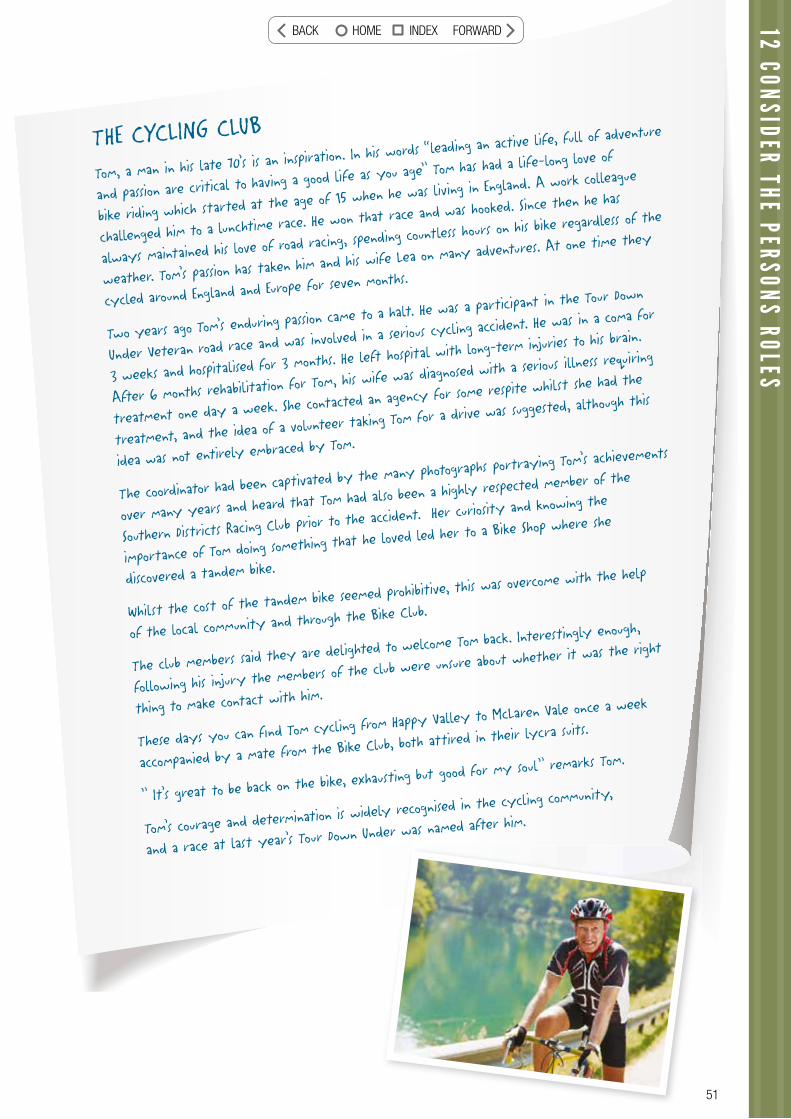
THE CYCLING CLUB
Tom, a man in his late 70’s is an inspiration. In his w
ords “leading an active life, full of adventu
re
and passion are critical to having a good life
as you age” Tom has had a life-long love of
bike riding which started at the age of 15 when he was living in England. A
work colleague
challenged him to a lunchtime race. He won that race and was hooked. Since then he has
always maintained his love of road racing, spending c
ountless hours on his bike regardless of the
weather. Tom’s passion has taken him and his wife Lea on many adventures. At one time they
cycled around England and Europe for seven m
onths.
Two years ago Tom’s enduring passion came to a halt. He was a participant in th
e Tour Down
Under Veteran road race and was involved in a seriou
s cycling accident. He was in a coma for
3 weeks and hospitalised for 3 months. He left hospital
with long-term injuries to his brain.
After 6 months rehabilitation for Tom, his wife was diagnosed with a serious illness re
quiring
treatment one day a week. She contacted an agency for some respite whilst she had the
treatment, and the idea of a volunteer taking To
m for a drive was suggested, although this
idea was not entirely embraced by Tom.
The coordinator had been captivated by the many photographs portray
ing Tom’s achievements
over many years and heard that Tom had also been a highl
y respected member of the
Southern Districts Racing Club prior to the a
ccident. Her curiosity and knowing the
importance of Tom doing something that he loved led her to a Bike Shop
where she
discovered a tandem bike.
Whilst the cost of the tandem bike seemed prohibitive, this w
as overcome with the help
of the local community and through the Bike Club.
The club members said they are delighted to welcome Tom back. Interestingly enough,
following his injury the members of the club were unsure about whether it was the right
thing to make contact with him.
These days you can fi nd Tom cycling from Happy Valley to McLaren Vale once a week
accompanied by a mate from the Bike Club, both attired in their lycra suits.
” It’s great to be back on the bike, exhausti
ng but good for my soul” remarks Tom.
Tom’s courage and determination is widely recognised in the cy
cling community,
and a race at last year’s Tour Down Under was named after him.
12 CONSIDER THE PERSONS ROLESBACK HOME INDEX FORWARD

52
13The appreciative question
Have you ever made a new year’s resolution to spend more time with your family or friends, or to make contact with people you have lost touch with? How did you go about doing that? What were the benefi ts?
The provocative proposition
In the planning process, Co-ordinators will look at the important relationships and networks that have been identifi ed in the discovery process. They will work with the person to identify how the relationship can be supported, valued and developed, and the relevant people involved.
If loneliness or isolation is identifi ed as an issue, the Co-ordinator will help the person to identify opportunities for social interaction based on the person’s interests. Where the person has a carer living with them or a person who is very involved in their care, there is also a need to plan how to support that person in their caring role.
Support relationships
Rationale
People’s networks may naturally decline as they age, when friends die or transport and mobility make it more diffi cult to keep in touch. This does not mean that relationships are any less important for older people. We know that
“…good relationships do more than make us happy; they make us healthy. Scientists have demonstrated that being in close, positive relationships can improve physical health by countering stress and producing feelings of calm. These relationships can even prevent chronic
health conditions in later life.” (55)
Carers are also crucial in helping many older people remain at home. They may be family members or friends living with the person, or coming in regularly to provide support or check on the person. It is important that the service does not take over what a carer may be happy to do, but also that they plan support that will help the carer to maintain their role.
BACK HOME INDEX FORWARD
53
13 SUPPORT RELATIONSHIPS
Belonging - acceptance as a natural member or part (56)
Step-by-step guide
Supporting carersCarer’s Australia (57) is the peak body for carers and this is their advice to help support carers:
Share the care with other family members or friendsCommunicate your needs to those around you. Suggest ways that others can help, and accept offers of support.
Take some time to care for yourselfRediscover your interests and hobbies – join a local club or group, or take up a new activity.
Stay in touchDon’t leave it too long to contact friends. Sometimes it just takes a phone call to help you feel connected again.
Have a health check - make this a priorityTalk to your GP about your concerns and how you’re feeling.
Get to know other carers and learn from themJoin a carer support group – receive support and learn some useful tips from others in similar situations.
Make sure you have all the information you need Contact your local carer service or advice line to see what is available in your community.
Tools
In topic 7 we used Relationship Circles to identify important relationships in the person’s life. When planning with the person you can use this information to identify who the person wants to maintain contact with, and how you can support this to happen. Where a person is very vulnerable, you may wish to more formally establish a “Circle of Support” to help safeguard the person’s health and well-being. With the persons’ agreement, this may involve convening a meeting of the people
who care about the person to be involved in the planning and dreaming about what may be possible. If a person is unable to consent (for example has advanced dementia), the circle may be formed to safeguard the person or support the family. The Circles approach has been used more to support people with disabilities, but could be equally relevant for older people. (58)
and well-being. With the persons’ agreement, this mayons’ aginvolve convening a meeting of the people of the
BACK HOME INDEX FORWARD
54
ANOTHER SONG TO SINGGrant was in dire straits. He was the carer for his wife Jean who had been
diagnosed with a terminal condition. He was struggling with the day to day care
needs that were part and parcel of Jean’s current situation. Grant wanted to be
free to invest as much time as possible being a loving husband to Jean while there
was life to be enjoyed together.
Grant and Jean had met years ago when they shared a love of dancing, fun and
music. The dancing days had gone but the sparkle that danced between them
when they were together was a testimony to a stunning relationship that had
lasted the test of time.
Music was still an integral part of their lives, in particular classical music that
wafted from their home as one drew near. It was clear that if we could orches-
trate a range of services including personal care, cleaning and some respite Grant
would have a song in his heart.
The services began and life took a harmonious turn where all needs seemed to
be getting met – well almost. Grant was a professional singer but had put this
area of his life on hold except for some solo engagements at his local church and
he was missing this involvement. I felt that this could be easily fi xed with some
respite occurring on Sundays on a fortnightly basis, however there was a hitch.
I discovered the local church wasn’t just around the corner but in fact was about
a half to three quarters of an hours drive away which meant respite would need
to be for about 2 and a half hrs and already the package was close to the maxi-
mum time allowance.
After much digging and delving we found a volunteer service that was willing to
come to the party on Sundays on a fortnightly basis. Grant could continue to
use his gifts and feel secure in knowing Jean was cared for while he was out of
the house. Jean and the volunteer became fi rm friends and played a variety of
board games and enjoyed each other’s company.
This arrangement continued until Jean’s condition deteriorated to the point where
she could no longer stay at home. We then assisted Jean and Grant to relocate
to the country where their daughter cared for Jean with the assistance of
another country organisation who we brokered until Jean eventually became
hospitalised.
The music has faded somewhat from Grant’s life now that he has returned to his
old unit alone. We have been able to support him as he faces life without Jean,
his car and to a certain extent his daughter.
I caught up with him the other day and I could hear ABC Classic FM resounding
from his sound system – it played ‘All my life’s a Circle’ – quite fi tting really
now Grant is singing solo again.
BACK HOME INDEX FORWARD
55
13 SUPPORT RELATIONSHIPS
Roles
In helping people to overcome isolation and connect with the community the role of the Co-ordinator is one of facilitator. You are not there to be the person’s friend (although you can be friendly) but to help them connect with old friends or make new ones. Some ideas to help this process:
• Be open to listening to, trusting and accepting others• Break the cycle of isolation by looking for ways to bring the person into everyday contact with others – at the
shops, local church, library or community centre• Search for strengths and capacities that might facilitate a meaningful connection• Ask people – don’t wait for someone to volunteer. Ordinary people may hold the key to hospitality and friendship• Trust the wisdom of the community – brainstorm with others to produce ideas you may not have on your own• Strengthen and re-kindle existing relationships – think about how you can nurture those relationships that
already exist• Use your imagination – believe in the vision that people can belong!• Find and work with bridge builders – these are people who have a wide range of connections in the community.
They can introduce the person to others • Consider the importance of rhythms and routines – it is often good to do things at the same time and same
place• Recognise the importance of the simple and the ordinary – celebrate with things that are quite signifi cant,
such as connecting with a neighbour. (59)
Discussion question
How to you deal with a situation where you are working with a person who is very isolated but resists your efforts to help them connect with other people, or has characteristics that may make it diffi cult for others to accept them (such as poor personal hygiene or a challenging personality)? Is belonging still important for these people?
A Place to Belong (59)
“Quality of life is having something to do, having someone to do it with, and having something to look forward to.” Neil Barringham. (59)
BACK HOME INDEX FORWARD
56
14 Encourage active participation in the response
The appreciative question
Think about a time when you approached a health care professional and felt empowered to be involved in making decisions about your treatment and future care. How did they approach it? How did it make you feel?
The provocative proposition
The planning approach taken with people will encourage their active participation in the process, and Co-ordinators will encourage people to “dream” about options that enable them to be as independent and autonomous as possible, rather than solutions that will lead to ongoing dependence on the service.
Rationale
Person-centred care aims to reorient service provision in two ways. One is to counter the emergence of organization or illness-centric systems that may be detrimental to holistic care of a person. (60) The second is to enable people to take a lead in planning all aspects of how the service they receive is delivered, that is to actively involve the person in the decision-making process wherever possible. (61)
Enable - To supply with the means, knowledge, or opportunity; To make feasible or possible. (62
Also recall the defi nition of “Right Relationship” in Topic 2.
Step-by-step guide
Active participation will be encouraged by:• Using language and patterns of communication that
encourage people and their families to participate in all care decisions, eg. asking rather than telling
• Describing the support process as a shared function to promote a sense of autonomy rather than exerting power or control over the person
• Asking people and their families how much they would like to be involved in the process, continuously soliciting their input
• After you have met with the person for the discovery or dreaming/planning process, asking for feedback about how it went and how they felt at the end; clarifying what each of you has agreed to do as a result
• Providing information about resources and contact details to make it easy for the person to follow up leads themselves
• Checking in from time to time to see if they are feeling overwhelmed with their role or happy with the balance; check in with families as well. (63)
BACK HOME INDEX FORWARD

57
14 ENCOURAGE ACTIVE PARTICIPATION IN THE RESPONSE
Tools
Levels of empowerment
Michael Kendrick (64) proposes a simple test to discern whether a person who is assisted by services is actually being enabled to make a signifi cant difference, through their own actions, on the character of the service they are receiving. More precisely, of the many important decisions taken that result in the actual design and operation of the services they ultimately receive, how many of these were made by the person, and how many were made by others, on behalf of the person.
Six levels are proposed:
Level One: This is a level where the person does not make any substantive decisions about their service.
Level Two: This is a level where the person does not make any substantive decisions about their service, but where the person is routinely informed about the decisions others will be making on their behalf.
Level Three: This is the level at which the person is routinely asked to give advice, (i.e. is consulted), by the
actual decision-makers, about his/her personal service decisions.
Level Four: This is the level at which the person begins to routinely personally make a signifi cant minority of the substantive decisions that constitute their personal service. A signifi cant minority, in statistical terms, might range from 25%-45% of key decisions.
Level Five: This is the level at which the person routinely begins to personally make a signifi cant majority of the substantive decisions that constitute their personal service. A signifi cant majority, in statistical terms, might range from 55%-90% of key decisions.
Level Six: This is the level at which the person is so routinely making the vast majority of key decisions that they simply do not any longer believe that they have a meaningful empowerment issue.
Roles
As an enabler, the role of a Co-ordinator is not to do everything for a person, but to help them to be as much in control as possible and as independent as possible. This can be done by providing information and choices, and continually checking in with the person whether they would like to follow up an action themselves or to have assistance with that.
Case Management Standards
2. PLANNING
2B Develop Client’s decision-making abilities and independence skills to foster personal growth. (3)
Discussion question
How do you involve a person in decision-making about their own support when they cannot communicate verbally or have a cognitive impairment such as Dementia?
5
n in decision-making about y cannot communicateimpairment
BACK HOME INDEX FORWARD
58
15 Health and well-being
The appreciative question
Think about a time when you were ill or you had injured yourself and required assistance to perform some tasks. Did you think that this would last forever or were you looking forward to the time when you could again do that task for yourself? What was most helpful to you in this situation?
The provocative proposition
The aim of all services is to promote healthy ageing, which is done through timely interventions that prioritise capacity building and restorative care that will maintain and promote people’s health, well-being and independence.
Rationale
If services are only considered to be in the business of maintenance and support for people, then we miss opportunities to enable people to be more independent, and possibly not be as reliant on services in the longer term. More active or restorative approaches to home care are gaining credence as a way of improving the lives of older people, and also reducing the ongoing demand on services.
Step-by-step guide
Ensuring the health and wellbeing of older people and promoting recovery and re-ablement requires consideration of:
• Assessment of health needs, involving other relevant professionals as required
• The prevention of disease
• Promoting activities known to promote good health (such as good nutrition and exercise) and reducing unhealthy habits
• Helping them to access treatment when required in a timely manner
• Promoting rehabilitation and recovery as soon as possibly after an event
• Encouraging re-ablement after an illness or incident, that is learning or re-learning the skills of daily living, or utilizing relevant equipment to compensate for the impairment
• Helping people to manage chronic disease to reduce the impact on their lives
• Collaborating with other health services to ensure clarity on common goals, and that all possibilities and constraints are considered
• Considering emotional and spiritual well-being as well as physical health.
There is also a need to balance people’s health needs and other parts of their life. While encouraging people to do things for themselves is positive, if it takes a long time or means that they are missing out on important activities or interactions, then it may be preferable for the person to have assistance.
BACK HOME INDEX FORWARD
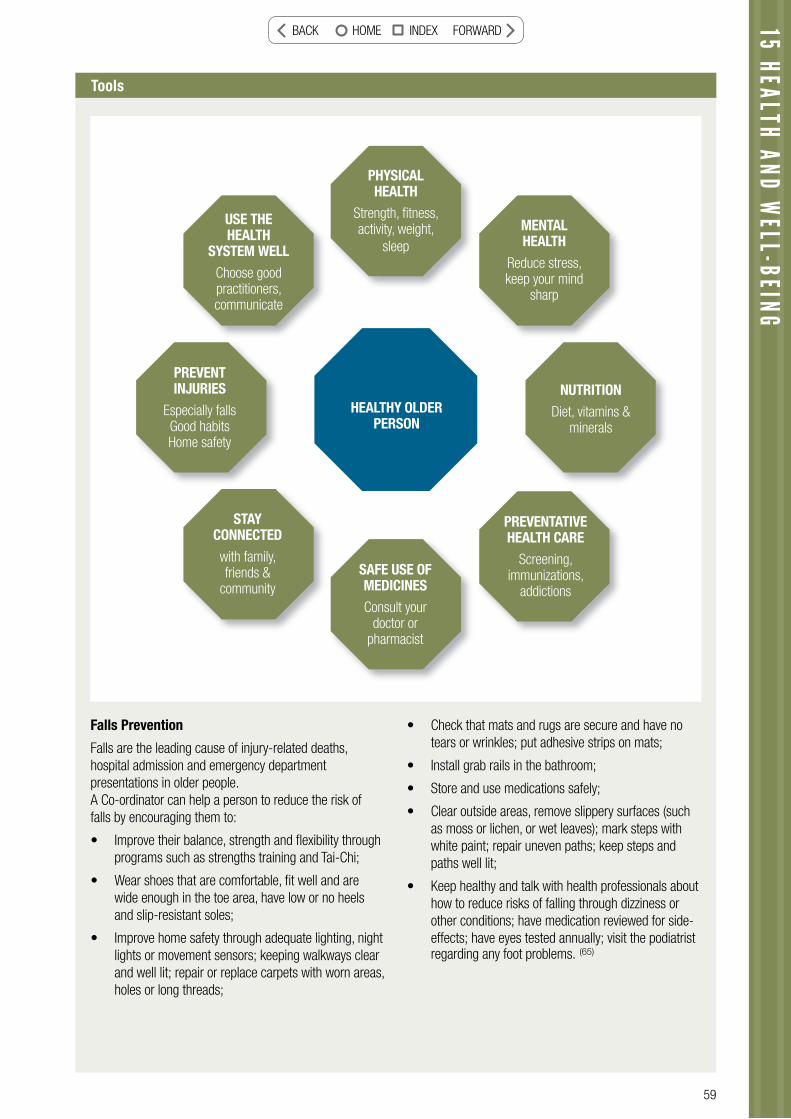
59
15 HEALTH AND WELL-BEING
Tools
Falls Prevention
Falls are the leading cause of injury-related deaths, hospital admission and emergency department presentations in older people. A Co-ordinator can help a person to reduce the risk of falls by encouraging them to:
• Improve their balance, strength and fl exibility through programs such as strengths training and Tai-Chi;
• Wear shoes that are comfortable, fi t well and are wide enough in the toe area, have low or no heels and slip-resistant soles;
• Improve home safety through adequate lighting, night lights or movement sensors; keeping walkways clear and well lit; repair or replace carpets with worn areas, holes or long threads;
• Check that mats and rugs are secure and have no tears or wrinkles; put adhesive strips on mats;
• Install grab rails in the bathroom;
• Store and use medications safely;
• Clear outside areas, remove slippery surfaces (such as moss or lichen, or wet leaves); mark steps with white paint; repair uneven paths; keep steps and paths well lit;
• Keep healthy and talk with health professionals about how to reduce risks of falling through dizziness or other conditions; have medication reviewed for side-effects; have eyes tested annually; visit the podiatrist regarding any foot problems. (65)
PHYSICAL HEALTH
Strength, fi tness, activity, weight,
sleep
MENTAL HEALTH
Reduce stress, keep your mind
sharp
USE THE HEALTH
SYSTEM WELLChoose good practitioners, communicate
NUTRITIONDiet, vitamins &
minerals
PREVENTATIVE HEALTH CARE
Screening, immunizations,
addictions
PREVENT INJURIES
Especially falls Good habits Home safety
STAY CONNECTEDwith family, friends &
communitySAFE USE OF MEDICINESConsult your
doctor or pharmacist
HEALTHY OLDER PERSON
BACK HOME INDEX FORWARD
60
COOKING HER WAY BACK TO HEALTH
Denise found herself losing motivation, just sitting and staring most of the day.
Some days she couldn’t even be bothered showering or dressing. She hadn’t done
any painting or creative writing for ages and couldn’t be bothered meeting with
her friends or listening to her music. She was also fi nding it diffi cult to manage
her mental health issue, and kept having ‘episodes’. When Denise went to the Doc-
tor he said she now has diabetes and advised her to change her eating habits.
Denise had always ‘lived on frozen meals’ and never bothered to learn to cook.
The Doctor told Denise she could get some help through a local agency and gave
her the number to call.
Denise phoned the agency and told them what the Doctor had said. Denise said
she wanted to learn about diabetes, what kind of food she needed to eat and
how to cook it. Denise said she didn’t want other people telling her what to do
and wanted to live her life her way.
The agency said that a worker, Jennifer, could spend some time with Denise each
week, for up to six months. It would be up to Denise to let Jennifer know what
help she wanted. When Denise said she didn’t have a lot of money left by the
time she had paid for her medicine, the agency said Denise would only have to
pay a small amount. Denise said she was keen to ‘pay her way’ and was confi dent
she would manage this. The agency said they would phone Denise before the end
of the six months to see how she was going and to see if she needed more help.
They also let Denise know she could call them at any time if she wasn’t happy
or needed any changes.
Roles
The Co-ordinator will not necessarily have expertise on all areas of health but needs to be open to working with a range of health professionals in order to support a healthy ageing approach. The skill of the Co-ordinator’s role is to encourage the discussions about health issues, provide information, and help the person to think about how they can improve their health and take preventative measures.
Discussion question
How do you approach a situation where it is clear to you that someone is engaging in behaviors that are harmful to their health, but do not want to discuss the issue or ignore your attempts to help them to change that behaviour (for example a problem with smoking, alcohol abuse, refusing to get medical treatment or leaving things around that may increase the risk of falls)?
BACK HOME INDEX FORWARD
61
15 HEALTH AND WELL-BEING
Jennifer visited Denise at home and said she had diabetes too. Jennifer said she didn’t know a lot about diabetes either and had been planning to go to some information meetings at the local Health Service. Denise said she would like to go too, so they arranged to meet there for six-weeks and learn together.Jennifer went with Denise to her local shopping centre so Denise could learn to identify what vegetables and fruit looked like and how to check freshness and the amounts needed. Denise told Jennifer what she liked to eat and they found easy to cook recipes in magazines and at the Health Service.Every week they would shop for the food, return to Denise’s home and prepare and cook the food. Jennifer only gave Denise help when she asked, or when she could see a ‘meal disaster’ about to happen. They had a lot of laughs and Denise found out she liked to cook and was inviting her friends over to try out her new skills.
Denise phoned the agency after fi ve months to say she didn’t need Jennifer’s help any more. Denise said she had learnt all she needed to know, that she knew how to shop, cook and was enjoying the food. Denise thanked the agency for the help and said she would phone again if she needed to. The Doctor was pleased with the changes that Denise had made.
World Health Organisation defi nition of Active Ageing: (66)
“Active ageing is the process of optimizing opportunities for health, participation and security in order to enhance quality of life as people age. It applies to both individuals and population groups. Active ageing allows people to realize their potential for physical, social, and mental well-being throughout the life course and to participate in society, while providing them with adequate protection, security and care when they need.The word “active” refers to continuing participation in social, economic, cultural, spiritual and civic affairs, not just the ability to be physically active or to participate in the labour force. Older people who retire from work, ill or live with disabilities can remain active contributors to their families, peers, communities and nations. Active ageing aims to extend healthy life expectancy and quality of life for all people as they age.“Health” refers to physical, mental and social well being as expressed in the WHO defi nition of health. Maintaining autonomy and independence for the older people is a key goal in the policy framework for active ageing. Ageing takes place within the context of friends, work associates, neighbours and family members. This is why interdependence as well as intergenerational solidarity are important tenets of active ageing.”
BACK HOME INDEX FORWARD
6262
Identify what should be the idealCo-construct the future design
The “provocative proposition” in each topic is a statement of possibilities that bridges what is ideal and what is possible. That is the task of this stage, often thought of as the “goal-setting” and “implementation” stages of case management. The information we have gained about people’s individual preferences and needs through a person-centred planning process, is then translated into agreed goals and activities. These activities will allow all parties (service user, informal networks and the Co-ordinator) to contribute towards the achievement of the set goals.
“impimpge,ge
f d wd w
pepeeedsdse
ess, sel
propr
dandndaof thisist
oal-s-oaages esg
The eThp
stagstaettingngti
of casafinformfoin
eopleleo
and ndmanamana
ation nioindivdin
s throrothds
agemeg mwe haw a
idual duaough ghu
s, is ttis
ossibio s biwhat is powhat is p
, often thf en t
opopof possibilitipo bi it
possposd whwwhthothoge, oge
“imple“imple
62
BACK HOME INDEX FORWARD
16 Agreeing goals
The appreciative question
Think about a time when you really set your heart on achieving something. Were you really clear about what you wanted? Did that help you to achieve it? Were other people involved in helping you to achieve your goal?
The provocative proposition
After getting to know a person and understanding their strengths and aspirations, Co-ordinators will agree to realistic goals with the person. These goals will defi ne what the partnership with the service will aim to achieve with the person, and how each of the parties will contribute.
Rationale
If services are only considered to be in the business of maintenance and support for people, then we miss opportunities The process of setting goals is integral to your work as a Co-ordinator. Goals are a way to gain agreement between you and the person being supported about your purpose for being there and how you can help them achieve their goals.
Step-by-step guide
• First you need the person to agree their overall aim of being supported by your service. This is an overall medium to long term outcome, perhaps relating to one of the life areas below (for example, I really want to remain at home; or I want to be independent of supports as soon as possible).
• It is then important to describe the current situation in relation to that aim. Write down a description and quantify if possible. This “baseline measurement” will help later to identify what has been achieved and to celebrate success.
• Then agree what the specifi c goals are over the following few months that will help to achieve the overall aim in the longer term. Goals should be SMART
● Specifi c ● Realistic ● Measurable ● Time specifi c ● Achievable
• The goals should also be expressed in the person’s words, not jargon.
• Then defi ne the actions that the Co-ordinator and the person or family agree to undertake in order to work towards this goal.
• All parties should agree and sign the goals document.
• In your reviews, come back to the goals and document progress.
16 AGREEING GOALS
Goal - the result or achievement toward which effort is directed (67)
ument progress.
63
BACK HOME INDEX FORWARD

64
Tools
Life areas
The following are possible life areas in which goals may be set. The process of goal setting is highly individualized, so not everyone will have goals in all of these areas, rather they are possible areas to consider.
1. Bodily integrity, health and well-being
2. Personal security and relationships, including support for carers
3. Supporting the continuation of roles or assisting to gain new roles in work, education, recreation, community life, family life
4. Supporting people to gain autonomy and control over their life, and enable choices
5. Enrichment of life experiences and community involvement
6. Maintaining, developing and enhancing skills and abilities
7. Economic security and independence
8. Discovery and expression of self and individual uniqueness and spirituality.
Source: Wolfensberger (68)
Roles
The person may expect that your role is just to arrange practical assistance, or to do everything for them. You need to be clear that goal-setting is a shared process which is focused on their needs and life goals. That may also mean broadening their horizons to think about their social and spiritual domains, for example, and not just physical issues. At this stage you should also be helping them to identify the roles that are important to them, and how you can support the maintenance of those roles. Cultural factors also need to be taken into account.
AIMCURRENT SITUATION
GOAL ACTIONS RESPONSIBILITY TIME FRAME
Life area Eg Bodily Integrity, Health and Well-being
Example:Improve Physical well-being
Cannot move around the house without physi-cal support from carers
To improve independence with mobility as evidenced by the ability to move around the home with a walking aid within 3 months
*Arrange Occu-pational Therapy Assessment* Select needed aids/equipment & apply for funding to purchase*Do a home safety audit
*Rectify any falls risks
Co-ordinator
Co-ordinator & older person
Home Owner(Co-ordinator provide checklist)
Home Owner/family
Within 2 weeks
Within 2 weeks of receiving assess-ment report
Within 3 weeks
Within 6 weeks
Life area Eg Enrichment of life experiences and community involvement
Example:Reconnect with old friends
Not going out due to lack of transport and embarrassment about impact of stroke on speech & mobility
To attend bowling club once a week for lunch with former bowling friends
*Arrange Trans-port* Find appropriate carer or compan-ion to get ready and accompany*Contact friends*Assess if communication assistance/aids needed
Co-ordinator
Co-ordinator & older person
Older person with assistance Referral to speech therapist
Within 3 weeksWithin 2 weeks
Within 3 weeksRefer within a week
BACK HOME INDEX FORWARD
65
Case Management Standards
2. PLANNING2E Document Client goals (including measurable criteria) to determine the effectiveness of the interventions provided. (3)
Discussion question
Have you ever been in a situation where you may see a long-term goal that is possible or you feel is desirable for a person, but you are unable to discuss that with the person? How could you approach that in a goal-setting session? Is it always necessary to agree on all goals up front?
You are never too old to set another goal or to dream a new dream. C S Lewis
Knowing your destination is half the journey. Anon
A goal without a plan is just a wish. Larry Elder
settgoa
Knojour
A goLarry E
16 AGREEING GOALSBACK HOME INDEX FORWARD
66
17The appreciative question
Think about a time when you received a very personalized service that made you feel special and unique, perhaps from a hotel or restaurant, or a health service. What did people do that made it special?
Rationale
Having agreed to take on certain tasks, it is important that the Co-ordinator fulfi lls these commitments. This will ensure that the service is seen as reliable and trustworthy. It is also true that the way in which services are delivered (ie the attitudes of staff or the degree to which they are culturally appropriate) will be just as important as the nature of the services themselves in being able to achieve the set goals.
Culturally Valued Analogue (69) -The concept of looking at how a similar need is met in the valued society, and using this as a model for service development.A Culturally Valued Analogue is something which is:• encountered with reasonable frequency in the valued sector of society• with which most sectors of society would be familiar• of which most members of society would hold positive expectations and images• which constitutes a valued parallel to a practice performed by or with devalued people.Human services usually address the same human needs that all people have including physical care, a place to live, opportunities for growth and development, health care, and education. However, the manner in which many services address these needs can alter. The result of this is that people who receive services can be seen as “different” which can reinforce stereotypes. The more those services match the valued equivalent, the more positive the image of the people who utilize that service will be. It is helpful to think about what “home life” or “community life” typically look like for people. What kinds of roles and relationship do most people have? (Note: The Appreciative Questions at the beginning of each topic in this handbook help you to think about the Culturally Valued Analogue of each process we are describing).
The Right Response
The provocative proposition
Having come to understand the person, their strengths and needs, and the goals that are important to them, the Co-ordinator will arrange the supports that they have agreed to in a timely and effi cient manner. These supports may include paid services as well as facilitating links to community resources and supporting informal networks. The supports will be provided in a way that is typical for any valued citizen in the community (see defi nition of Culturally Valued Analogue below).
BACK HOME INDEX FORWARD
67
Step-by-step guide
Factors to be considered when fi nding the right response for a person:
• Is the response the most typical way to meet this need?
• The agreed assistance should be documented in a care plan. This should describe not only what is to be done, but explain this in the context of the goals that have been set, and also include how the person would like the task to be completed
• Check that the timing of services meets the person’s lifestyle and needs (eg being assisted to shower and dress in time for important social activities)
• Where possible, ensure that the care worker selected is an appropriate match in terms of personality,
cultural background and other factors; enable the person to be involved in the choice of care worker
• Introduce the care worker to the person and explain their role
• Consider if the care worker requires training or credentialing for any of the tasks they are required to perform
• If involving volunteers, make sure they are clear about their role and what tasks are required of them and the expected behaviours
• Think about higher order needs, such as spiritual and emotional needs that go beyond the practical support requirements, and how you may assist in meeting these needs.
17 THE RIGHT RESPONSE
QUALITYIn talking with a man who had been a master chef for most of his life I was reminded once again
just how important is a quality product. He told me that he had a wonderful apprenticeship, four
years in all, on luxury ships. He felt he had
the best life possible, working in a job he love
d and
living in the marine environment. He loved the sea and he thoroughly enjoyed providing beautiful
meals for the passengers who also chose to spend
their holidays cruising around.
He told me that a quality product in the food industry depended on three i
ngredients:
• The meals must be visually appealing/appetizing
• The meals should be prepared using the very best ingredients
• The food should taste wonderful
He said the type of passenger that patronized a cruise sh
ip expected the very best of service
in all departments, especially the cuisine. The quality of food would actually determine to a
large part how people enjoyed the cruise.
He said he learnt very quickly that near enough is
not good enough. Whether he was
preparing breakfast or creating a gourmet’s delight for the C
aptain’s dinner, the same kind of
care and precision went into the preparation and presentation.
He said that the same standards have spilled over into his own life. When his wife was very
ill and her appetite very poor, he would create for her t
asty morsels that incorporated his
‘cruise ship standards’. His efforts were rewarded with the sight, smell and taste of the
food,
enticing her to nourish her frail body.
BACK HOME INDEX FORWARD

68
Are we always testing what we do against our value base? Do we present ourselves i
n a
way that is appealing; neat/tidy appearance, respecti
ng of people’s ideas and property.
Do we offer a quality service, always prepared to ‘bend over backwards’ to provide the
very best we can? Are we prepared to go ‘that extra mile’ for people by going out on a
limb for them so that they are listened to and valued?
Do people taste and see that what we provide is good? Is
the proof of the service pudding
in the eating/sampling? When we discover a fi ne restaurant with delicious food the
idea is
to patronize it on special occasions so that
the food always remains a treat. If, however,
we decided to eat there with frequent regularit
y the whole taste/enjoyment experience
would not be the same. The same with the service ‘restaurant’. The idea is to
be available
to assist and encourage natural networks so that we become a facilitator to fl av
ouring the
lives of people with the ‘normal ‘ community supports. When the clients are feasting on us
continually, devouring platefuls of ours and other ser
vices, in fact greedily wanting more,
they go from quality to quantity, from ‘TheManse’ to “Charlie’s Diner”. Our help becomes a
hindrance in living a normalized existence. They
go from satisfaction to indigestion as they
over eat on a diet that holds no substance
and no lasting social, physical or mental rewards.
We should be endeavouring to provide a cuisi
ne that that keeps people fi t and continua
lly
building on life strengths rather than a ser
vice diet that leads to gluttony and apathy.
Roles
Ensuring the right response is arranged does not necessarily mean doing everything for the person. The Co-ordinator should check which things the person may wish to arrange for themselves, or which they would prefer family members or friends to do. The role of the Co-ordinator in these situations may be to provide information or resources to assist others to arrange supports.
Discussion question
How do you deal with a situation where a person you are supporting does not seem to get along with any of the support workers you are providing to assist them?
BACK HOME INDEX FORWARD
69
18The provocative proposition
The Co-ordinator recognizes that they are a part of broader system of services and community resources that can assist the older person. They will utilize these resources to the benefi t of the older person, and recognize the limitations of their own expertise. When referrals are made, the Co-ordinator will ensure that the person or their representative is well informed about the referral, has given their consent, and that relevant information is forwarded to ensure the person does not have to repeat the information provided to the Co-ordinator.
Rationale
No one service can or should address all of the needs of a person. To be coherent, a service will be competent at addressing one particular area of need. However, to ensure other needs are met services must work together, with the person at the centre, to determine who can best meet the different needs of the person while sharing the common goals of the person/family. A Co-ordinator may need to consult another service that has special expertise in a particular area (eg working with people with Dementia).
Where the service recipient requires more than one service these should be provided in a continuous fashion, with good co-ordination. Relevant service workers need good relationships and communication between services.
18 RESOURCES, REFERRALS AND CO-ORDINATION
Resources, Referrals & Co-ordination
The appreciative question
Think about a time when you needed to arrange an event (perhaps a wedding or birthday party) and had many different things to consider (venue, menu, invitation lists, decorations etc.). How did you go about fi nding out about all the options? What helped you to co-ordinate all the elements to create the fi nal event? Were there any people who were particularly helpful in this process? Why?
BACK HOME INDEX FORWARD
70
Co-ordination – The harmonious adjustment or interaction of parts.Synergy - The interaction of two or more agents or forces so that their combined effect is greater than the sum of their individual effects. (70)
Step-by-step guide
Service Coordination principles
The following principles underpin good co-ordination between services:
• A central focus on consumers - Service delivery needs to be driven by the needs of consumers and the community rather than the needs of the system, or those who practice in it
• Partnerships and collaboration - Service providers work together and take responsibility for the interests of consumers, not only within their own service but across the service system as a whole, including General Practitioners and Allied Health professionals
• The social model of health - A distinct conceptual framework for thinking about health. This framework is concerned with addressing the social and environmental determinants of health and wellbeing, as well as biological and medical factors. This includes the spiritual and family connections that contribute to wellbeing
• Competent staff - The elements of Service Coordination must be undertaken by staff who are appropriately skilled, qualifi ed, experienced, supervised and supported
• A duty of care - A duty to take reasonable care of a person. The duty of care extends to Service Coordination, where staff have a duty of care to provide accurate and timely information, and assist consumers with referrals
• Protection of consumer information - improved information management practice is critical. Consumer Consent and information about Privacy requirements are designed to improve information fl ow, practice and consumer outcomes
• Engagement of other sectors - Service Coordination embraces the broadest range of partnerships across service provider types (small, large, non-government, government) and across disciplines, including general practice
• Consistency in practice standardsService Coordination enables services to remain independent of each other as entities but work in a cohesive and coordinated way to ensure that consumers experience a seamless and integrated service response.
Source: Dept . Human Services. Victoria (2009) (71)
Roles
The Co-ordinator’s responsibility does not end when they have sent a referral, but is also responsible for following up the outcome and suggesting alternatives if the referral is not accepted. The Co-ordinator needs to be the pivotal connector of all the different services, ensuring no duplication. Their role is also to follow through on any specifi c ways in which services should be provided in order to maintain independence.
Synergy — the bonus that is achieved when things work together harmoniously. Mark Twain
Discussion question
As a Co-ordinator who is working to use a strengths-based approach with people, how do you work well with other parts of the system that focus on defi cits and require people to be as frail as possible in order to qualify for additional supports?
BACK HOME INDEX FORWARD
71
1919 SUPPORT COM
MUNITY PARTICIPATION & INFORM
AL NETWORKS
Support Community Participation &Informal Networks
The provocative proposition
The Co-ordinator will recognise the potential value and effectiveness of both formal and informal supports. The service takes care to preserve and enhance informal supports from family, friends and generic community resources and will not replace these with formal supports.
The Co-ordinator recognises the value and importance of being pro-active in facilitating the successful use of relevant generic community resources by service recipients.
Rationale
In the Discovery phase the Co-ordinator has identifi ed the important networks and community links that the person wishes to maintain or develop. The challenge in the Design and Delivery phase is how to bring this about.
There can be many barriers to community participation, both in community attitudes and in practical areas such as transport and accessibility of community venues. Positive community participation helps to break down stereotypes and increase community understanding of older people. The continued segregation of any group of people who have become isolated will reduce their acceptance by the community.
We have already discussed how personal relationships are benefi cial for a person’s health. (Topic 13)
The appreciative question
Think about a time when you were warmly welcomed into a new group or returned to a group that you had not been part of for a while. What was special about the way that people behaved? How did it make you feel?
A Network is an association of individuals having a common interest, formed to provide mutual assistance, helpful information, or the like (72)
Social Capital is a sociological concept used to describe the connections within and between social networks with the aim of highlighting the value of such networks to individuals, the community and the economy. Putnam speaks of two main components of the concept: bonding social capital and bridging social capital. Bonding refers to the value assigned to social networks between homogeneous groups of people. Bridging refers to that of social networks between socially heterogeneous groups. Typical examples are that criminal gangs create bonding social capital, while choirs and bowling clubs create bridging social capital. Bridging social capital is argued to have a host of other benefi ts for societies, governments, individuals, and communities; Putnam likes to note that joining an organization cuts in half an individual’s chance of dying within the next year. Source: R. Putnam (2001) (73)
BACK HOME INDEX FORWARD
72
Step-by-step guide
In order to support the involvement of informal networks, Co-ordinators need to:
• demonstrate an awareness of the right response to each specifi c need (ie. a formal or informal response)
• honour and value the contribution of family, friends and informal networks
• fi nd ways to maintain and promote involvement by informal networks
• provide information about community activities and opportunities to experience different activities
• follow up on people’s interests, gifts, talents and aspirations
• consider reconnecting with past friends and associates identifi ed in the discovery phase
• arrange practical supports to facilitate participation,
such as transport and/or fi nancial assistance
• ensure service arrangements (such as the provision of personal care) are able to be provided in a timely manner to enable involvement in community activities
• provide the personal support and encouragement required to facilitate participation in ways that counteract negative community perceptions
• seek out companions to accompany people on activities
• work with community groups to encourage understanding and acceptance of people who are frail or have cognitive impairments
• choose care workers who can role model positive interactions in community activities
• create opportunities and facilitate connections, then step back and allow them to take their course. (59)
Discussion question
How do you support someone who seems to have few networks and contacts to develop new relationships?
What should young people do with their lives today? Many things, obviously. But the most daring thing is to create stable communities in which the terrible disease of loneliness can be cured. Kurt Vonnegut, Jr.
Research Fact
Participation, including participation in social activities, is central to older adult’s view of what constitutes successful ageing. (75)
Roles
A Co-ordinator can take on the role of community connector, or link the person with someone who is good at connecting. The Co-ordinator can identify opportunities and links that may increase opportunities to participate in the community and build relationships. Most importantly, the Co-ordinator and the services provided should not be a barrier to this occurring.
Tools
Community inclusion can be like an “iceberg”, where being in the community is only the tip of the iceberg. This is presence, where I see others and I am seen. Beyond that is participation – where I know others and I am known. At the deepest level is belonging – where I miss others and I am missed. (74)
To understand belonging we need to consider a number of aspects:
• Location – where are the places that a person relates to?
• Identity – what are the roles that are important to the person? (see Topic 12)
• Interests – what are their interests and passions?
• Personality – people like to belong in different ways. Some prefer a structured setting while others like to be informal.
While it is important for people to be able to go out into the community, for some people their restrictions may be such that we need to build a community around where they are. (59)
There can be no vulnerability without risk; there can be no community without vulnerability; there can be no peace, and ultimately no life, without community. M. Scott Peck
BACK HOME INDEX FORWARD
THE STRENGTH OF COMMUNITYA 90 year old lady, Mrs Smythe, lives alone and has a
diagnosis of dementia. She has been a widow for 10 yrs.
Her “younger “ brother who is 85 years old also lives alone
in a neighbouring suburb. Her brother is her main carer
and still drives. Together they do most things such as
shopping, attend church, paying bills. Mrs Smythe also
attends regular church activities including the weekly
drop-in group.
Mrs Smythe has been cautious of accepting “services” into her home. By using a gentle and sensitive
approach she and her brother have become comfortable with the regular contact and involvement
of their Co-ordinator. Up until now they have rejected the offer of other practical assistance. The
major concern is how she will manage if there are any problems with her brother’s health. The
program pays for fortnightly homecare, plus occasional extras e.g. an electrician to move power
points in the bedroom to an accessible height. This will reduce the risk of tripping over numerous
power leads.
During one visit Mrs. Smythe did express an interest in joining an exercise group. The Co-ordinator
researched groups that operated in her area. All of the options were discussed at a home visit. She
chose a local group at a neighbourhood house. Mrs Smythe did not own a pair of track suit pants so
she had to go out and purchase a pair. Her Co-ordinator reminded her to do this and her neighbour
took them up for her.
A care worker was arranged, carefully chosen for their knowledge and experience of working
with people with dementia. This worker was to transport and accompany Mrs. Smythe to her
Strength Training Group. It took three attempts to get her to the fi rst group. She kept forgetting,
had a doctor’s appointment, and then didn’t feel well enough to go. With the assistance of her
brother giving her a reminder call early on the day, the worker giving her a call an hour before
she arrived, and the cooperation of the G.P. signing the medical release she fi nally attended!
At her fi rst class the whole group gave her a round of applause when they learned of her age!
Mrs. Smythe is also building a trusting relationship with the worker, who will be able to assist in
other ways when or if the need arises.
Note: A few months down the track Mrs. Smythe fell at home but did not sustain any fractures.
We cannot be sure that this was due to the strength training, but it may well have helped! This
story shows how all of the resources of the community, the neighbourhood and her informal
supports assisted Mrs. Smythe to achieve a positive outcome.
19 SUPPORT COMM
UNITY PARTICIPATION & INFORMAL NETW
ORKS
73
BACK HOME INDEX FORWARD
74
20
The appreciative question
Think about a time when you felt unable to stand up for yourself, and were reliant on someone else to advocate for you, perhaps because you were unwell, or you did not understand the area (eg a complex legal process). What was helpful to you in that situation?
The provocative proposition
In implementing the agreed plan, a Co-ordinator may need to advocate on behalf of a person to gain access to the services or the supports that they need. Where possible, the person should be encouraged to advocate for themselves and to access external advocacy services or informal personal advocacy support. Where a person is very vulnerable or has a cognitive impairment, the Co-ordinator needs to put in place relevant safeguards to protect the person from harm and potential exploitation.
People will also be encouraged to express their views about the quality of the services they receive, and the Co-ordinator will act on this feedback.
Advocacy and Safeguarding
BACK HOME INDEX FORWARD
75
Rationale
People in receipt of services can be at risk of losing their autonomy and having their basic rights taken away. This is particularly the case where a person loses some of their cognitive abilities.
Many service users feel that they should be grateful for service provided and are afraid to complain for fear of losing help. Opportunities need to be provided for service users and their families to be involved in the evaluation of service to enable quality improvements that are most relevant to service users.
A powerful safeguard for any service recipient, especially when they are vulnerable, is the presence of at least one independent party (quite often in the form of a freely given relationship) that represents the interests of a service recipient as if those interests were their own.
Step-by-step guide
The respect for the autonomy and rights of service users will be demonstrated by:
• encouraging people to make their own choices and allowing the dignity of risk
• upholding the rights of service users to the extent that is culturally accepted
• assist and support service users in the responsible exercise of their rights, such as enabling access to advocacy services, having appropriate and effective internal complaints mechanisms
• Ensuring service recipients are informed about relevant advocacy bodies
• Being open to the involvement of such parties by a) reducing unnecessary blocks to advocates having information (and unhelpful confi dentiality procedures), b) ensuring information on important meetings is made available well in advance
• Listening to and acting upon reasonable requests and recommendations from advocates
• Seeking advice from statutory bodies in situations where competence of the service recipient to make critical life decisions is questioned
• Seeking opinions, comments and critique from external sources (academic sources, consultants, external evaluation teams).
20 ADVOCACY AND SAFEGUARDING
Advocacy - the act of pleading for, supporting, or recommending; active espousal.Safeguard - something that serves as a protection or defense or that ensures safety; a precautionary measure. (76)
Discussion question
How do you encourage a person to express an honest view about the services they are receiving, especially when they seem concerned about the possibility of losing the service?
“Education is a better safeguard of liberty than a standing army.” Edward Everett Hale (1822-1909)
Roles
Where you see a pattern in the unmet needs or issues experienced by the people you are supporting, you may have a role in advocating at a system level rather than an individual one. You should bring this to the attention of your manager with some suggestions about what you think could be done to help the situations.
Tools
Safeguards can be:
• Preventative – designed to prevent any harm coming to a person (eg careful planning that takes into account the risks or vulnerabilities of the person)
• Developmental - develop/ enhance people’s capacity to prevent harm (eg educating or informing a person about options)
• Corrective - actions and features designed to remediate and control occurrence of harmful effects (eg complaints or appeals mechanisms).
Source: Kendrick (2002) (77)
Case Management Standards
3. MONITORING
3E Support the Client’s self-advocacy skills wherever possible. (3)
BACK HOME INDEX FORWARD

7676
Identify how to empower, learn, and improviseSustain what gives life
The delivery stages (sometimes known as destiny) is the time of continuous learning, adjustment and improvisation in working towards the shared ideals. The process of learning about a person and planning supports is never one-off, as situations change, goals are achieved and new aspirations arise. Sometimes advocacy is needed with others who are part of the design, to ensure that they play their part.
d planningngnanpds situations nsiotsas
and new aspspawdanadvocacccvaddvoccvpart of ortpaplay theiethypl
spirationsatirp onsacy is needed wenes y c ded the design, to igesdhet n,r parttar
to part. rta
n, ,eir part. tar
dd toto
76
BACK HOME INDEX FORWARD
77
21 Check In
The appreciative question
Have you ever started in a new and unfamiliar job and had a supervisor who checked in regularly to see how you were getting on? Did you have a formal review at the end of your probationary period? What was particularly helpful in this process?
The provocative proposition
Co-ordinators will maintain regular contact to ensure that services are being provided as agreed and that the person is satisfi ed with the quality and reliability of services. Where issues arise, the Co-ordinator will follow up and resolve these promptly. Where goals relate to the support of informal networks or linking with community resources, the Co-ordinator will also monitor how these are going and work with the person to overcome any barriers that may arise.
Formal reviews will also be held on a regular basis where all arrangements can be reviewed in a face-to-face meeting, and progress in achieving goals can be documented.
Rationale
The process of supporting a person does not stop when goals are agreed or a care plan is written. Co-ordinators need to ensure that the plan is being carried out as agreed, and that what is provided is what is really needed to achieve the agreed goals. The process of getting to know a person is a continuous one, and over time different needs and goals may become evident. Both ongoing monitoring, and a formal review process are important in the delivery stage.
Step-by-step guide
In order to monitor and review the supports being arranged:
• Ask people how they are going and whether the support of your organization and others is making a difference.
• Check if there have been any negative impacts of receiving the support.
• Check if goals have been achieved and whether ongoing support is needed, or whether a new goal or different types of support are required.
• Remember to involve relevant family members or advocates in a formal review process.
• Check with family members about whether they are happy with the roles they have taken on, whether they are feeling under pressure or would like to re-negotiate their agreements.
• Provide information about any new resources that may be relevant for the person.
• Qualifi ed interpreters should be used for any reviews involving a person whose fi rst language is not English.
• Remember to check not only how your own service is going, but also whether other services you have arranged or referred the person to are still being provided in a satisfactory manner.
21 CHECK INBACK HOME INDEX FORWARD
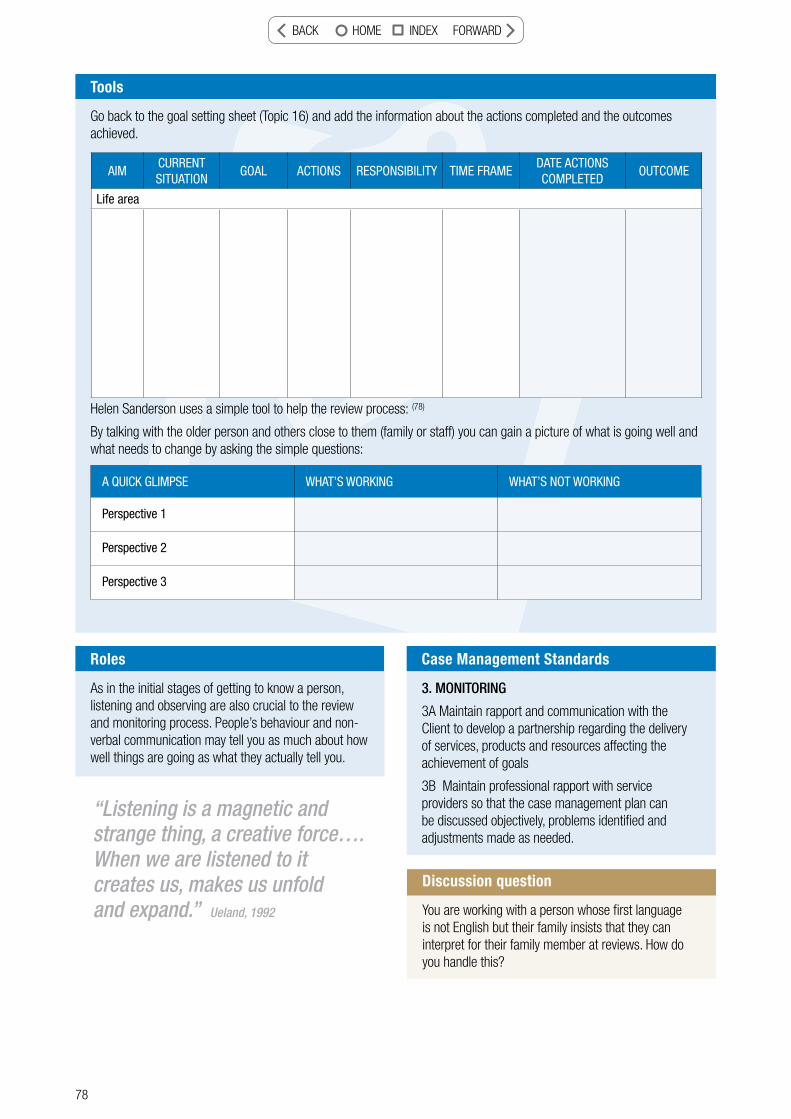
78
Roles
As in the initial stages of getting to know a person, listening and observing are also crucial to the review and monitoring process. People’s behaviour and non-verbal communication may tell you as much about how well things are going as what they actually tell you.
Tools
Go back to the goal setting sheet (Topic 16) and add the information about the actions completed and the outcomes achieved.
Helen Sanderson uses a simple tool to help the review process: (78)
By talking with the older person and others close to them (family or staff) you can gain a picture of what is going well and what needs to change by asking the simple questions:
A QUICK GLIMPSE WHAT’S WORKING WHAT’S NOT WORKING
Perspective 1
Perspective 2
Perspective 3
AIMCURRENT SITUATION
GOAL ACTIONS RESPONSIBILITY TIME FRAMEDATE ACTIONS COMPLETED
OUTCOME
Life area
Case Management Standards
3. MONITORING
3A Maintain rapport and communication with the Client to develop a partnership regarding the delivery of services, products and resources affecting the achievement of goals
3B Maintain professional rapport with service providers so that the case management plan can be discussed objectively, problems identifi ed and adjustments made as needed.
Discussion question
You are working with a person whose fi rst language is not English but their family insists that they can interpret for their family member at reviews. How do you handle this?
“Listening is a magnetic and strange thing, a creative force….When we are listened to it creates us, makes us unfold and expand.” Ueland, 1992
BACK HOME INDEX FORWARD
79
22Rationale
The monitoring and review process is designed to ensure that support is occurring as planned, but is more than likely to uncover some issues that need to be addressed. It would be very easy to provided excuses for any shortfalls (such as “that is the way it is done around here” or “the system does not allow us to do that”) rather than think about creative ways of ensuring the need can be met. Systems can be challenged, and creative thinking can help to fi nd ways around perceived barriers. (see Topic 11).
Step-by-step guide
In order to respond fl exibly to changing needs you may need to consider:
• If formal responses are not working, assess whether an informal response could be more appropriate
• Check if the reasons you have been given for something not being “allowed” are real, and if there is a mechanisms for challenging the decision
• Use creative thinking techniques (Topic 11) to help overcome issues and barriers
• Continue to ground your responses in the needs and aspirations of the person
• Involve the person and their networks in generating alternative ideas and advocating for fl exible responses
22 RESPOND FLEXIBLY
Flexible - Responsive to change; adaptable (79)
Respond Flexibly
The appreciative question
Have you ever had your heart set on something (such as going away on a holiday) and come across what seemed like an insurmountable barrier? (such as missing your plane or losing your luggage). Did you ever experience a person who helped you to negotiate the system to get you to where you wanted to be? What did they do? How did it make you feel?
The provocative proposition
Co-ordinators will be ready to adapt to a person’s changing circumstances and use creative means to overcome any issues relating to ongoing support, or barriers to achieving the agreed goals. Bureaucratic processes will be kept to a minimum and Co-ordinators may need to advocate for the person, or encourage self-advocacy to ensure that the support provided is meeting their needs and goals.
BACK HOME INDEX FORWARD

80
Roles
The Co-ordinator’s role is to continue to stand by the person and fi nd fl exible ways to support a good life in the community and meet their most important needs. However, resources are not infi nite so you there is a need to be creative about different ways to respond, and to focus on the needs that are the most important to address.
Case Management Standards
3. MONITORING
3C Adjust services, supports and resources to best meet the needs of the Client in line with identifi ed goals. (3)
Discussion question
What are some ways to overcome service constraints due to the limits of available fi nancial resources? How should a Co-ordinator respond if there is no more money available for a person’s support?
Be clear about your goal but be fl exible about the process of achieving it. Brian Tracy
Be infi nitely fl exible and constantly amazed. Jason Kravitz
Tools
The Doughnut
You and your colleagues may have different ideas about what your core responsibilities are and where you can use creativity and judgement. In some situations this will not be problematic, however, if the differences are substantial, you may fi nd it useful to carry out the doughnut exercise as a team of professionals to ensure the best use of available resources.”
There are often not suffi cient resources to provide everything that a person may need, so being clear about the core responsibilities helps to focus attention on priorities. Outside of that, there may need to be more creativity in thinking about ways to respond to needs. This clarity also helps people to be accountable. Where an issue is not the responsibility of your service, you may need to make a referral to another service or community resource. (80)
OUR RESPONSIBILITY
USE JUDGEMENT AND CREATIVITY
NOT OUR RESPONSIBILITY
BACK HOME INDEX FORWARD
81
23 Endings - Graduation, Celebration and Letting Go
The appreciative question
Think about a time when you had a “good ending” – perhaps leaving a job or graduating from a course. While endings often lead us to feel sad, what made this situation a positive one for you?
The provocative proposition
Co-ordinators will be clear from the fi rst interaction with a person about the scope of the service and the criteria for the service eventually ending. When a review indicates that the service is no longer needed, the person is no longer eligible, or the person is seen to need a higher level of support, this will be discussed as soon as possible with the person and their family. They should be informed of other available resources and supports, and the process for accessing these. Of course there may be many other reasons why a service ends, such as if the person dies suddenly or is admitted to hospital. It is still important in these situations for a Co-ordinator to talk with the person or their family and be clear about the ongoing role of the service, and refer them to other relevant supports if required.
Rationale
Most support programs have a specifi c purpose. People cannot necessarily be guaranteed of ongoing support if their needs and circumstances change. Co-ordinators should also be aiming to increase a person’s independence through utilizing a restorative approach and therefore be aiming to reduce the reliance on ongoing supports. As Co-ordinators you will build a positive rapport with people over time, it may sometimes be diffi cult to discuss the need to end the service. The more that these situations are discussed up front, the more realistic expectations may be about the ongoing role of the service.
Step-by-step guide
In order to bring the relationship between your service and the service recipient to a satisfactory ending you will need to consider:
• Ensuring that you have been clear about service expectations up front
• Explained clearly why the service is ending and what alternative supports are realistically available for the person
• Make relevant referrals, provide all the necessary information and follow these through
• Celebrate achievements if the person has achieved their goals and no longer requires support
• Provide feedback to the person about what you see as their strengths and achievements during the time you have known them
• Acknowledge potential feelings of grief and loss if the service is ending due to a bereavement or crisis. Ensure that the service user has relevant supports to help them through this time.
23 ENDINGS - GRADUATION, CELEBRATION AND LETTING GOBACK HOME INDEX FORWARD
82
Tools
Grief and Loss (from Living as an Older Person) (81)
It is important for Co-ordinators to understand the emotions associated with grief and loss, whether it is with families, older people grieving a spouse or the need to leave their home, or their own feelings when ending a support relationship. Stages of grief have been identifi ed, but current thinking indicates that these can be fl uid rather than sequential, and people may move in an out of these emotions. These emotions can be considerable, but are a normal part of the grieving process.
Stages of Grief:
1. Shock
2. Emotional release
3. Isolation and depression
4. Physical symptoms of distress
5. Inability to cope with life
6. Sense of guilt
7. Anger and resentment
8. Inability to return to normal activities
9. Gradual awareness of reality and return of hope
10. Adjustment to reality.
Some of the most important needs of grieving people include:
• To feel SUPPORT. We need to recognise that loss raises all sorts of feelings and that to cope people need the care, love, support and understanding of others
• To face REALITY. The process of recovery is linked to acceptance of the loss. Acceptance will not come until reality is faced
• To express FEELINGS (emotional release). It seems important that people experiencing grief and loss should be helped, encouraged and allowed to express their feelings. This may be through tears and talking. Too often “would be helpers” supress rather than encourage and facilitate emotional release
• We need to recognise that being upset is healthy and helpful rather than harmful
• To move towards the re-establishment of ongoing living. For many this is diffi cult, and for a period of time (often many months) painful and unthinkable.
The extent of someone’s grief will be infl uenced by the situation and nature of the relationship as well as many other factors. There is no magic time period by which someone’s grief should be resolved, but if you are concerned that a person is experiencing an abnormal grief reaction you should involve a counsellor with expertise in this area.
BACK HOME INDEX FORWARD
83
GRADUATION DAYMusic pervaded the air as I moved into the auditorium.
The gentle, earthy sounds of pan- pipes seemed to
seep into my mind and soothe my body as I sunk into
a surprisingly comfortable chair. Huge arrangements of
orchids caught my eye and I knew Jim would approve of
this touch for his special day.
He had a fetish for orchids, they were housed in his
hot house at the back of his house and lovingly attended by him with just the
right amount of fertilizer and water. It was right that the people in the know make this day
as special as possible for Jim. Jim had the habit of making things right for others. The kids across
the way who enjoyed endless treats, the neighbours who knew Jim would lend a bed for the
overfl ow at their house for those special occasions when extra family needed shelter and his
grandchildren who knew the generosity of his monetary handouts.
The chairs around me were fi lling up. Some people I knew; his son and daughter-in-law, his
grandchildren (whose photos I’d seen on the fi replace) and his cleaner and her husband. Others I’d
only heard about, so I played a people jigsaw in my mind, trying to fi t particular people with the
roles I thought they may have played in Jim’s life.
My mind was brought back to the present with the fading out of the music and the moving
to the front of the people involved with the graduation ceremony. We were welcomed with
warmth and then told about Jim, his life and achievements. Many of the anecdotes I had heard
before but some were new and I got a difference sense of Jim and what made him tick. Even his
grand-daughter came forward and contributed to the ceremony, her words a special gift to her
grandfather.
As graduation ceremonies go this was both touching and seeming right. Death, in the Christian
sense is the graduation from one life to another. Jim in his 92nd year had graduated well. Until
his untimely death, he had remained in his own home. He had renovated his kitchen area so that it
was new and functional. His garden was his pride and joy. Even with his knee replacements and
walking frame he managed to potter, prune and take pride in its neat and tidy appearance. Home
cleaning and shopping from Community Options, weekly meals from Meals on Wheels and transport
from Veterans Affairs enabled Jim to live life to his satisfaction.
As long as Jim could watch his beloved sport, especially football and cricket in the comfort of his
suede designer recliner, with a few sweet treats for good measure, he was content. Jim’s life had
undergone many changes; from married to widower, from able bodied to tottery. However, in all
the changes he had choices, his choices and that made the difference.
From life to life; Jim graduated with honors.
23 ENDINGS - GRADUATION, CELEBRATION AND LETTING GOBACK HOME INDEX FORWARD

84
Roles
The Co-ordinator needs to acknowledge that although they are in a professional relationship, they may have come to know a person very well through supporting them over a period of time. As with all relationships it is important to have good closure. If the person is moving on from the program, take the time to say goodbye and make sure all loose ends are tied up. If a person has had to move suddenly (eg to hospital), try to take the time to visit and say goodbye. However, as it is a professional relationship, make sure you do not make promises you cannot keep, such as promising to keep in touch. Remember that you have now completed the role you were asked to take on, and have carried it out to the best of your ability!
Discussion question
How do you overcome the sense of insecurity that a service recipient may feel if the service is no longer able to be provided? How can you assist a successful transition to the next stage of support or independent living?
BACK HOME INDEX FORWARD
85
REFERENCES
ReferencesFOREWORD
1. Sue Hammond & Jo Hall (2001) What is Appreciative Inquiry? www.thinbook.com/docs/doc-whatisai.pdf (accessed 9.06.10)
2. South Australian Home and Community Care (HACC) Service Principles (2010). Government of South Australia Adelaide
3. Kerrie Maher & Brad Cooper eds. (2008) National Standards of Practice for Case Management. Case Management Society of Australia. Melbourne.
4. Aged & Community Services SA&NT (2006) Better Practice Project Handbook. Adelaide.
ABOUT APPRECIATIVE INQUIRY
5. David L. Cooperrider, Diana Whitney, and Jacqueline M. Stavros (2008) The Appreciative Inquiry Handbook: For Leaders of Change, 2nd Edition. Berrett-Koehler Publishers, Inc. and Crown Custom Publishing, Inc. USA.
6. Sue Hammond & Jo Hall (2001) What is Appreciative Inquiry? (see 1)
7. The Appreciative Inquiry Handbook (see 1.) p 16
8. Bliss Browne, Imagine Chicago (undated). What is Appreciative Inquiry? Her work can be found at www.imaginechicago.org
TOPIC 1
9. www.merriam-webster.com (accessed 29.09.11)
TOPIC 2
10 . Dr. Michael Kendrick. Workshop Materials on Right Relationship (unpublished). Related work can be found at www.kendrickconsulting.org.au
11. James Delrojo (2010) Six Tips for Building and Maintaining Rapportwww.enhancedhealing.com/articles/view.php?article=862 (accessed 25.02.10)
TOPIC 3
12. www.thefreedictionary.com (accessed 7.06.10)
13. Mark Skeie, Janet Skeie & Julie Roles (2007) Mapping Your Retirement: A Personal Guide to Maintaining Your Health, Managing Your Money and Living Well. MYR Publications, USA, pp 19-21.
14. Helen Sanderson & Associates (2007) Person Centred Thinking with Older People: Practicalities and Possibilities. www.helensandersonassociates.co.uk (“Appreciations” at pp 21-26).
TOPIC 4
15. www.dictionary.com (accessed 29.09.11)
16. New York Times (7.10.2008) Elderspeak
17. Donna McDowell (1995) The Challenge of Meeting Individual Needs. Paper for the Aged Care Australia Conference, 9 November 1995, Canberra, p 220.
TOPIC 5
18. Todd R. Lyons (2010) Strengths Based Social Work Practice. http://en.wikibooks.org/wiki/Strengths-Based_Social_Work_Practice (accessed 29.09.11)
19. www.dictionary.com accessed (8.4.10)
20. UnitingCare Australia & Inspiring Communities (2009) Building Belonging: Celebrating Inclusive Communities. Asset Based Community Development Workshop Handbook, p 26.
21. E. H. Erikson et al (1986) Vital Involvement in Old Age
22. St. Luke’s Innovative Resources, Bendigo. www.innovativeresources.org (accessed 25.09.11)
23. UnitingCare Australia & Inspiring Communities (2009) (see 20). Cosy Club story p 15.
24. www.wikipedia.org (accessed 25.02.10)
25. Anthony Robbins (1997) Unlimited Power: The New Science of Personal Achievement. Simon & Schuster. NY
TOPIC 6
26. www.dictionary.reference.com (accessed 29.09.11)
27. Sanderson et al. (2007) – see 14
28. J.R. Bradshaw (1972) The Taxonomy of Social Need in McLachlan, G. (ed), Problems and Progress in Medical Care, Oxford University Press: Oxford
29. Dr. Wolf Wolfensberger Universal Human Needs (workshop materials)
TOPIC 7
30. http://dictionary.com (accessed 29.09.11)
31. J.R. Bradshaw in An Introduction to Social Policywww.2.rgu-ac.uk/publicpolicy/introduction/contents.htm (accessed 29.09.11)
32. Adapted from Antonucci & Akiyama, 1987 and Kahn & Antonucci, 1980 in Mark Skeie, Janet Skeie & Julie Roles (2007) (see 13), p34
33. Carmichael, 2006; Taylor et al 2000 in Mark Skeie, Janet Skeie & Julie Roles (2007) (see 13), p32.
34. Maori Proverb (WHAKATAUKI), FTM Aotearoa. http://ftmaotearoa.tripod.com (accessed 8.4.10)
TOPIC 8
34. Dr. Wolf Wolfensberger et al (3rd Rev. Ed. - 2007) PASSING Manual: A Tool for Analyzing Service Quality According to Social Role Valorization Criteria. Training Institute for Human Service Planning, Leadership and
BACK HOME INDEX FORWARD

86
Change Agentry, Syracuse University. USA. Defi nitions, p 30
35. www.thefreedictionary.com (accessed 25.02.10)
36. Ellison (2007) Duty of Care, Critical Thinking, and Ethicswww.restlessdance.org/resources/Resources%20word/Duty%20of%20Care.doc (accessed Dec 2009)
37. Adapted from UnitingCare Community Options (2008) Framework for Ethical Decision making. www.ucco.org.au/Files/FrameworkforEthicalDecision-Making.pdf (accessed 25.02.10)
TOPIC 9
38. www.dictionary.com (accessed 25.02.10)
39. Centre for Cultural Diversity in Ageing www.culturaldiversity.com.au/NationalResources (accessed 25.02.10)
40. Aged & Community Services SA&NT. Better Practice Program (April 2009) Aboriginal & Torres Strait Islander Home & Community Care Workers Forum. Unpublished Proceedings. South Australia.
41. Centre for Cultural Diversity in Ageing (See 40)
TOPIC 10
42. Tristan Loo (2006) How to Defi ne Your Life Purpose http://ezinearticles.com/?How-to-Defi ne-Your-Life-Purpose&id=331527
43. Adapted from Helen Sanderson & Associates (2007) (see 14) , p 89,90
44. Dr. Helen Kivnick. Workshop Materials.
45. Dr. Helen Kivnick & S.A. Stoffel (2005) Vital Involvement Practice: strengths as more than tools for solving problems. J Gerontol Soc Work. 2005;46(2):85-116.
TOPIC 11
46. Dr. Edward DeBono (1985). Six Thinking Hats: An Essential Approach to Business Management. Little, Brown, & Company. Also at www.debonoconsulting.com/Six_Thinking_Hats.asp (accessed 25.02.10)
47. Squidoo (2008) Types of Creativity www.squidoo.com/fosteringcreativity (accessed 10.06.10)
48. Roger von Oech (2009) Creative Whack Pack www.creativethink.com/products.html (accessed 25.02.10)
49. Innovation Tools www.innovationtools.com (accessed 25.02.10)
50. The defi nition of creative is …relative www.squidoo.com/fosteringcreativity (accessed 10.06.10)
TOPIC 12
51. Civic Ventures, 2007, cited in Mark Skeie, Janet Skeie & Julie Roles (2007) (see 13), p 51
52. Matthews, 1996, cited in Mark Skeie, Janet Skeie & Julie Roles (2007) (see 13), p 51
53. Susan Thomas & Dr. Wolf Wolfensberger (1999) An Overview of Social Role Valorization in R.J.Flynn & R.A. Lemay (eds) in A Quarter-Century of Normalization and Social Role Valorization: Evolution and Impact, University of Ottawa Press, p 126.
54. Summarised from Scott Ramsay (2007) Roles Based Planning: A Thoughtful Approach to Social Inclusion AND Empowerment, 2nd ed. Anti-Marginalization Task Force, Calgary, AB. pp32,33
TOPIC 13
55. Carmichael, 2006; Taylor et al. 2000, cited in Mark Skeie, Janet Skeie & Julie Roles (2007) (see 13), p 32
56. www.dictionary.com (accessed 25.02.10)
57. Carers Australia www.carersaustralia.com.au (accessed 10.06.10)
58. Circles Network: Building Inclusive Communities (2009) www.circlesnetwork.org.uk (accessed 10.06.10)
59. Neil Barringham (2009) A Place to Belong. Workshop materials www.aplacetobelong.org.au
TOPIC 14
60. Mansell & Beadle-Brown, 2004 cited in Bridget Ryburn et al (2008) The Active Service Model: A conceptual and empirical review of recent Australian and International literature (1996-2007). Australian Institute for Primary Care, La Trobe University, Melbourne, p 29. www.latrobe.edu.au/aipc
61. Mead & Bower, 2000, cited in Bridget Ryburn et al (2008) (see 60), p29.
62. www.dictionary.com (accessed 25.02.10)
63. Adapted from Raiff et al. (1993) Advanced Case Management: New Strategies for the Nineties. Sage Publications, USA. P 83
64. Dr. Michael Kendrick (March 2004) Discerning Actual levels Of Substantive Empowerment Planet Advocacy, Issue Number 7, pp 6-7. www.kendrickconsulting.org/docs/Empowerment%20Levels.doc
TOPIC 15
65. Dept. Health, Western Australia (2008) Your Home Safety Checklist. Stay on Your Feet WA. http://www.health.wa.gov.au/docreg/Education/Prevention/Injury_Prevention/HP79 26_SOYF_home_safety_checklist.pdf
66. World Health Organization (2010) What is active ageing? www.who.int/ageing/active_ageing (accessed 10.06.10)
BACK HOME INDEX FORWARD

CONTACT DETAILS
Joyleen Thomas, Manager Better Practice Project Aged & Community Services SA & NT246 Glen Osmond Road, Fullarton SA 5063P: 08 8338 7111 F: 08 8338 7077 W: www.agedcommunity.asn.au E: [email protected]
BACK HOME INDEX





























