Embed Size (px)
Citation preview

XANDRA APOLLO BAY ARARAT BACCHUS MARSH BAIRNSDALE BALLARAT BEAUFORT BEECHWORTH BENALDIGO BOORT BOX HILL BROADMEADOWS BUNDOORA BURWOOD EAST CANTERBURY CARLTON CASTERTOEMAINE CAUFIELD CHELTENHAM CLAYTON COBRAM COHUNA COLAC COLERAINE CORRYONG DANDENON
AYLESFORD EAST BENTLEIGH EAST MELBOURNE EAST RINGWOOD ECHUCA EDENHOPE EPPING FITZROY OOTSCRAY FOSTER FRANKSTON GEELONG HAMILTON HAMPTON HEALESVILLE HEATHCOTE HEIDELBERG OOD HORSHAM INGLEWOOD KERANG KEW KILMORE KOOWEERUP KYABRAM KYNETON LEONGATHA LORON MANANGATANG MANSFIELD MARYBOROUGH MILDURA MT ELIZA MYRTLEFORD NATHALIA NHILL NOBL
K NUMURKAH OMEO ORBOST OUYEN PARKVILLE PORT FAIRY PORTLAND PRAHAN ROBINVALE ROCHESTEBUD RUPANYUP SALE SANDRINGHAM SEYMOUR SHEPPARTON ST ALBANS ST ARNAUD STAWELL SWAN HINGATTA TERANG TIMBOON TRARALGON UPPER FERNTREE GULLY WANGARATTA WARRACKNABEAL WARRAGRNAMBOOL WERRIBEE WILLIAMSTOWN WINCHELSEA WODONGA WONTHAGGI YARRAM YARRAWONGA YEAANDRA APOLLO BAY ARARAT BACCHUS MARSH BAIRNSDALE BALLARAT BEAUFORT BEECHWORTH BENALLDIGO BOORT BOX HILL BROADMEADOWS BUNDOORA BURWOOD EAST CANTERBURY CARLTON CASTERTOEMAINE CAUFIELD CHELTENHAM CLAYTON COBRAM COHUNA COLAC COLERAINE CORRYONG DANDENON
AYLESFORD EAST BENTLEIGH EAST MELBOURNE EAST RINGWOOD ECHUCA EDENHOPE EPPING FITZROY OOTSCRAY FOSTER FRANKSTON GEELONG HAMILTON HAMPTON HEALESVILLE HEATHCOTE HEIDELBERG OOD HORSHAM INGLEWOOD KERANG KEW KILMORE KOOWEERUP KYABRAM KYNETON LEONGATHA LORON MANANGATANG MANSFIELD MARYBOROUGH MILDURA MT ELIZA MYRTLEFORD NATHALIA NHILL NOBL
K NUMURKAH OMEO ORBOST OUYEN PARKVILLE PORT FAIRY PORTLAND PRAHAN ROBINVALE ROCHESTEBUD RUPANYUP SALE SANDRINGHAM SEYMOUR SHEPPARTON ST ALBANS ST ARNAUD STAWELL SWAN HINGATTA TERANG TIMBOON TRARALGON UPPER FERNTREE GULLY WANGARATTA WARRACKNABEAL WARRAGRNAMBOOL WERRIBEE WILLIAMSTOWN WINCHELSEA WODONGA WONTHAGGI YARRAM YARRAWONGA YEAANDRA APOLLO BAY ARARAT BACCHUS MARSH BAIRNSDALE BALLARAT BEAUFORT BEECHWORTH BENALLDIGO BOORT BOX HILL BROADMEADOWS BUNDOORA BURWOOD EAST CANTERBURY CARLTON CASTERTOEMAINE CAUFIELD CHELTENHAM CLAYTON COBRAM COHUNA COLAC COLERAINE CORRYONG DANDENON
AYLESFORD EAST BENTLEIGH EAST MELBOURNE EAST RINGWOOD ECHUCA EDENHOPE EPPING FITZROY OOTSCRAY FOSTER FRANKSTON GEELONG HAMILTON HAMPTON HEALESVILLE HEATHCOTE HEIDELBERG OOD HORSHAM INGLEWOOD KERANG KEW KILMORE KOOWEERUP KYABRAM KYNETON LEONGATHA LORON MANANGATANG MANSFIELD MARYBOROUGH MILDURA MT ELIZA MYRTLEFORD NATHALIA NHILL NOBL
K NUMURKAH OMEO ORBOST OUYEN PARKVILLE PORT FAIRY PORTLAND PRAHAN ROBINVALE ROCHESTEBUD RUPANYUP SALE SANDRINGHAM SEYMOUR SHEPPARTON ST ALBANS ST ARNAUD STAWELL SWAN HINGATTA TERANG TIMBOON TRARALGON UPPER FERNTREE GULLY WANGARATTA WARRACKNABEAL WARRAG
A Safety and Quality Improvement Frameworkfor Victorian Health ServicesA Safety and Quality Improvement Frameworkfor Victorian Health Services
Better Quality,Better Health CareBetter Quality,Better Quality,Better Health CareBetter Health Care

Published by the Metropolitan Health and Aged Care Services Division Victorian Government Department of Human ServicesMelbourne VictoriaJuly 2005Also published on www.health.vic.gov.au/qualitycouncil
© Copyright State of Victoria, Department of Human Services, 2003
This publication is copyright. No part may be reproduced by any process except in accordance with the provisions of the Copyright Act 1968.
Design by Watts Design.
Victorian Quality Council SecretariatPhone 1300 135 427Email [email protected] www.health.vic.gov.au/qualitycouncil

A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
Con
tent
s 1. EXECUTIVE SUMMARY 2
2. FRAMEWORK OVERVIEW 6Framework Principles
Framework Dimensions
Key Organisational Elements
Dimensions of Quality
Roles and Responsibilities
3. AN ORGANISATION-WIDE APPROACH 13Governance, Leadership and Culture
Consumer Involvement
Competence and Education
Information Management and Reporting
4. EXAMPLE OF AN ORGANISATIONAL APPROACH 23
5. CONCLUSION 25
APPENDIX A THE SAFETY AND QUALITY MATRIX 26Safety
Effectiveness
Appropriateness
Acceptability
Access
Efficiency
APPENDIX B CLINICAL GOVERNANCE ROLES 42AT SIX HEALTH SYSTEM LEVELS
APPENDIX C FRAMEWORK CHECKLIST 49
APPENDIX D ACKNOWLEDGEMENTS 55

A safety and quality improvement framework for Victorian health servicesis an initiative of the Victorian Quality Council (VQC). It was developed asone component of a strategic approach to improving the safety andquality of patient care in Victoria across five areas: Establish a Safety andQuality Framework, Provide Improved Access to Better Data, InvolveConsumers in Improving Safety and Quality, Educate on Safety andQuality and Respond to Known Problems and Risks.
Exe
cutiv
e S
umm
ary
01
Executive Summary
02
The VQC Safety and Quality Framework is a strategicoverview of the key principles and practices necessaryfor the effective monitoring, management andimprovement of health services. Whilst the frameworkis applicable to health services of all sizes and types,its usefulness depends on the extent to whichorganisational and clinical leaders adapt it to localstructures, environments and needs. The framework isbuilt on a foundation of clinical governance, whichclearly delineates the board responsibility for ensuringthat service and care quality is addressed with thesame rigor as financial governance, and ensures thatcorresponding accountabilities are delegatedthroughout the organisation.
The intent of this framework is that it is applied to bestbenefit each individual organisation in improving thesafety and quality of care and services. Depending onthe quality maturity and program progress of anindividual health service, it may be applied as a model,a reference, a plan, a source of ideas or a benchmarkto review progress and identify quality improvement(QI) program gaps. Where specific examples ofactivities, structures and processes are given, theseshould be considered in terms of their relevance toyour organisation. The key to the usefulness of theframework is that it is applied to add value to healthservice safety and quality programs.

Governance& Leadership
1. Safety
ConsumerInvolvement
Competence & Education
Information Management
Govt Board CEO & Organisational Leaders
Clinicians& Teams
Consumers & Community
2. Effectiveness
3. Appropriateness
4. Acceptibility
5. Access
6. Efficiency
Governance& Leadership
Quality Committee
CLINICAL GOVERNANCE ROLES THROUGHOUT THE HEALTH SYSTEM
KEY ORGANISATIONAL ELEMENTS
DIM
EN
SIO
NS
OF
QU
ALI
TY
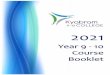
Applying organisational processes and roles to improve each dimension of quality
figure 1.0
The framework describes the intersection betweenfour critical organisational processes essential forquality improvement and each of the six dimensionsof quality, as well as exploring related roles andresponsibilities throughout the health system as seenabove in figure 1.0.
Access and efficiency have traditionally attracted themajority of the health care quality focus. Whilst theseare important quality components, this frameworkemphasises the other four equally significantdimensions and offers examples of how these mightbe measured and improved, and how the clinicalgovernance component of the board corporategovernance role can best be fulfilled.
The relevant literature clearly demonstrates that astrong and unwavering commitment to safety andquality results in demonstrable benefits, not only forpatients, but for the organisation, including lesscomplications and deaths, lower costs, greaterefficiency and improved clinical outcomes. A qualityprogram is only as successful as the culture withinwhich it is implemented, however. It is theresponsibility of the board and senior management topromulgate a culture wherein openness, mutualrespect and teamwork are encouraged and rewarded.This should provide the foundation for a plannedapproach to quality and safety that encompasses staffand patients’ values, identifies clear priorities,
allocates resources, provides education, addressesrisk, illustrates the QI methodology in use and outlinesthe supporting committee and reporting structures.
Developing a comprehensive approach to safety andquality improvement takes time and can be achievedvia a staged approach. Quality programs are iterativeand require constant development by the organisationto meet changing internal and external contexts,expectations and stakeholder needs. Health servicequality approaches also comprise many externalcomponents such as: accreditation standards andreviews, funding and policy imperatives and tools fromthe Department of Human Services (DHS), nationalinitiatives from bodies such as the Australian Councilon Safety and Quality in Healthcare and ideas fromprograms in other countries. This framework isconsistent with external requirements for safety andquality improvement programs and has also drawn onquality and safety research to integrate best practice insafety and quality program development andimplementation.
03
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES

Whatever approach is taken, however, a clinicalgovernance based model of safety and qualityimprovement will demonstrate some standard featuresacross all organisations. As a minimum requirement,boards should ensure that safety and qualitymanagement receives the same emphasis as financialmanagement, and is linked to strategic and businessplanning processes. An effective quality programrequires a planned approach, which enables boardsto provide evidence that:
there are appropriate organisational structures,processes and resources in place to monitor,manage and improve the safety of care andservices and the service delivery environment
the objectives of the quality program are clear and staff at all levels understand their related roles and responsibilities
staff have access to appropriate safety and qualitytechnical support and information to enable theireffective participation in improving care and services
consumers and carers are involved in safety andquality improvement in a variety of ways includingthrough feedback, complaints and improvementactivities
key areas of risk are identified, prioritised,managed and regularly reported
there is a strategy for managing thoseinternationally recognised problem areas in patientsafety and quality such as health service acquiredinfection, medication errors, pressure ulcers, falls, use of blood and blood products and painmanagement, including regular reporting, actionand follow up (a more comprehensive list ofsuggested data collection and reporting is foundin the “Information management and reporting”section of each dimension of quality in Appendix A)
there is a clear and transparent process for thereview of deaths and reporting and responding tosentinel and adverse events
patient care is based on best available evidenceand delivered by properly credentialed and trained staff
external reviews, such as accreditation, are usedas positive opportunities to review compliancewith standards
the health services benchmark with other likeorganisations on key areas of care and safety tofacilitate learning and improvement
there is ongoing development of an organisationalculture wherein participation and leadership insafety and quality improvement are resourced,supported, recognised and rewarded.
04

On an operational level, it is up to the CEO and seniormanagers to make it easier for staff at all levels of theorganisation to do the right thing in the provision andimprovement of quality care and services than not.Research has shown that there are three keypredictors of staff involvement in safety and qualityactivities: the extent of support from their direct linemanager; a belief that the organisation will experienceoutcomes of value from the activities; and training inthe tools of change and improvement. Thus,embedding the improvement program in an organisationwill require engaging and building leaders andinnovators at all levels, from “board to bedside”.Information flow should ensure that the board,managers and committees receive regular reports onrelevant issues, that these are considered and actedupon and that feedback flows to those affected by andproviding the information.
Evidence of improvements should be widely circulatedand celebrated and staff should have access totraining that equips them to participate in qualityimprovement activities. This framework discusseseach of these key requirements in detail, boththeoretically, in the body of the document, andpractically, by offering ideas for implementation anddata reporting in Appendix A. An example of how theframework might be applied to the management of asentinel event is described in Section 4, and achecklist for organisational self-assessment againstthe framework elements is found in Appendix C.
If “improvement of health care performance hinges on changing the day-to-day decisions of doctors,nurses and other staff”7, then it is important that each individual’s role in achieving this is clearlydelineated. To this end, the framework identifiesgeneric clinical governance roles at six levels of thehealth system that can be adapted to individualorganisations (see Appendix B).
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
05

The Victorian Safety and Quality Improvement Framework builds on the salient NSW Health (1999) document “A Framework for Managing the Quality of Health Services in NSW”1 and also sources material fromthe safety and quality literature, the Victorian Department of HumanServices (DHS), and other relevant material such as hospital reviewreports and discussion papers.
Fram
ewor
k O
verv
iew
02Overview of the Victorian Safety and QualityImprovement Framework
The Framework is a generic strategic and principles-based document, which should be applicable tohealth services of any size. Whilst it is primarilyhospital-focused, the principles and frameworkelements, particularly those concerning clinicalgovernance and leadership, are applicable morebroadly across all aspects of service provision andcare. Organisational safety and quality improvement isillustrated using a matrix approach. Each of sixdimensions of quality is explored within health serviceroles and organisational environment.
Section 1, the Executive Summary and Section 2, the Overview, summarise the framework. The Executive Summary reads as a stand-alonedocument and can be used as a condensedreference to the framework. Section 3 explores theorganisational elements and their application to safety
and quality in more detail. Section 4 gives an example of how the framework might be applied to asentinel event. Appendix A shows the dimensions ofquality/organisational elements matrix in table formand gives examples and ideas of how they might beapplied, and suggests areas for data collection andreporting. Appendix B lists clinical governance rolesand responsibilities at a number of different levels in the health system. A checklist to assist withorganisational self-assessment and review is found in Appendix C.
06

The Framework for Managing the Safety and Qualityof Health Services in Victoria:
focuses on the safety and quality of clinical care
promotes leadership and accountability for thesafety and quality of health care with a systemicorientation
focuses on the principles for managing the safetyand quality of health services
provides an organisational focus for qualityactivities and reporting, recognising the essentialrole played by leaders, consumers and all healthservice staff in quality improvement
recognises the essential cultural requirements ofquality and safety improvement.
For the purposes of this framework, quality care isdefined as “the extent to which a health care serviceor product produces a desired outcome”.2
Quality improvement is defined as “the continuousimprovement of all processes and the products and services that are the outcomes of thoseprocesses”.13
Clinical Governance is defined using the AustralianCouncil on Healthcare Standards (ACHS) definition:“the system by which the governing body, managersand clinicians share responsibility and are heldaccountable for patient care, minimising risks toconsumers, and for continuously monitoring andimproving the quality of clinical care.”14
Safety is defined as “a state in which risk (measuredin terms of consequences and likelihood) has beenreduced to an acceptable level”.2
This framework is consistent with, and should beconsidered in conjunction with, relevant DHS policies,statutory and insurance processes and reportingrequirements, and relevant professional, industry and accreditation standards and protocols.
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
07

The principles that underpin the delivery of safe and high quality health care have beendeveloped from a variety of sources, including published literature and relevant reportsfrom Australia and other countries.
A quality oriented health service will reflect thefollowing characteristics1,4,5:
the health consumer as the primary focus of anymodel of health care quality management
the board, CEO and executive taking responsibilityfor creating and maintaining a structure, cultureand policies for managing the safety and quality ofhealth care
the health service board creating an open andhonest culture wherein responsibility for the qualityof the health care provided to consumers is clearlyarticulated and enacted at all levels
a systematic and system-wide approach tocontinuous improvement of the quality of caredelivered
an emphasis on preventing adverse outcomesthrough simplifying and improving the processesof care
those practising within the system takingappropriate responsibility for the standard of theirown practice and sharing responsibility forcreating and maintaining a system which providessafe, high quality health care
consumers being enabled and encouraged toparticipate effectively in both their own care andtreatment and the planning, delivery andevaluation of health services
consumers having ready access to effectivesystems of complaint and compliment
an emphasis on the development of partnershipsof care with consumers, staff within theorganisation and health workers in the community
a robust advisory and reporting structuredesigned to promote the improvement of healthservices and to provide regular information to thehealth service board on the quality and safety ofservices provided
health treatment and care based on the bestavailable evidence
the quality of health care measured systematicallywith a focus on the minimisation of inappropriatevariation in practice
all health care providers having access toinformation about the outcomes of the care theyprovide and the systems within which they work
a system driven by performance in the six primarydimensions of quality of health care
quality and safety information used in planningand resource allocation decisions within healthservices
the quality framework supported by high qualityorganisational structures and processes that havebeen evaluated by a recognised externalaccrediting body.
2A The Principles Underpinning theFramework
08

The framework describes the dimensions of quality and the cross dimensionalorganisational elements that underpin effective safety and quality improvement.
2B Framework Dimensions
09
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
A planned approach to safety and quality by key organisational elements:
a) Governance, Leadership and Culture
b) Consumer and Community Involvement
c) Competence and Education
d) Information Management and Reporting
At each level of the organisation: Government
Board
Quality Committee structure
CEO and Senior Clinicians and Managers
Clinicians and Teams
Consumer and Community
To monitor, manage and improve each dimension of quality:
1. Safety
2. Effectiveness
3. Appropriateness
4. Acceptability
5. Access
6. Efficiency

This framework distils and discusses four key organisational elements necessary for theeffective improvement of the quality of health care: Governance, Leadership andCulture; Community and Consumer Involvement; Competence and Education;Information Management and Reporting.
Governance, Leadership and Culture
Corporate governance describes the structures andprocesses put in place by boards to fulfil theirstrategic, statutory and financial obligations. Clinicalgovernance is a critical element of the corporategovernance of health services.
Clinical governance refers to boards’ accountabilityfor ensuring that a framework and rigorous systemsare established so health care safety and quality ismonitored and supported, evaluated and continuouslyimproved.4
Consumer and Community Involvement
Consumer involvement in health care is critical toeffective service planning and evaluation and to theachievement of optimum care outcomes. There aremany differing definitions of ‘consumers’ inhealthcare. For the purposes of this document, theterm consumer refers to people who either directly orindirectly make use of health services. This includesindividuals receiving, or who have received, healthcare services, whether individuals or in groupsaccording to similar backgrounds or health states. It also includes family and carers of those receivinghealth care. Community is described in thisframework as the population served by the healthservice, including future users and the widercommunity that benefits from health care services.8
Competence of, and Education to Support, HealthCare Providers
Competence is an overarching issue and a majorpriority for review and action in health services. This includes the competence of the organisation, the competence of multi-disciplinary care teams andthe competence of the individuals who deliver careand services.
Information Management and Reporting
Information management refers to the collection ofdata, the technology required to do so, including thesoftware and hardware, the reliability and validity ofthe data and how data are reported and convertedinto information to be used in practice. To supportthese processes, data and information should beavailable, accurate, timely and relevant. Ensuring thisincludes review of coding accuracy, robust datadefinitions and collection systems, and transparentanalysis and reporting processes.
2C Organisational Elements
10

Dimensions of quality in health care are variously described in the literature with anumber of different dimensions and definitions available.
2D Dimensions of Quality
For the purposes of this framework, the dimensions of quality are described as follows1:
Safety of health care: A major objective of any healthcare system should be the safe progress of consumersthrough all parts of the system. Harm arising from care,by omission or commission, as well as from theenvironment in which it is carried out, must be avoidedand risk minimised in care delivery processes.
Effectiveness of health care: Consumers of healthservices should be able to expect that the treatmentthey receive will produce measurable benefit. The effectiveness of health care relates to the extentto which a treatment, intervention or service achievesthe desired outcome.
Appropriateness of care: It is essential that theinterventions that are performed for the treatment of a particular condition are selected based on thelikelihood that the intervention will produce thedesired outcome for each patient. This means thatthe expected health benefit exceeds the expectednegative consequences by a sufficiently wide marginthat the procedure is worth doing. Essentially, theappropriateness of health care is about usingevidence to do the right thing to the right patient, atthe right time, avoiding over and under utilisation.
Acceptability of care: Opportunities must be providedfor health consumers to participate collaboratively withhealth organisations and service providers in healthservice planning, delivery, monitoring and evaluation atall levels in a dynamic and responsive way. Consumerand community participation should enhance the levelof acceptability of services, which is the degree to
which a service meets or exceeds the expectations ofinformed consumers.
Access to services: Health Services should offerequitable access to health services for the populationthey serve on the basis of need, irrespective ofgeography, socio-economic group, ethnicity, age or sex.This includes availability of services, such as waitingtimes for services and processes involved in accessingservices, physical and information access. The Victorianpublic health system, like others in Australia andinternationally, is experiencing unprecedented andsustained increases in demand. The issue of access toall health services is a critical one.
Efficiency of service provision: Health services mustensure that resources are utilised to achieve value formoney. This can be achieved by focussing onminimising the cost combination of resource inputs inthe production of a particular service as well as theallocation of resources to those services to provide thegreatest benefit to consumers. Allocative efficiencyinforms decisions on what services or treatments todeliver, whereas technical efficiency is concerned withreducing costs and minimisation of waste.
This classification system for quality recognises thateach dimension is not a completely separate entity.Each should be considered when developing andimplementing a system to improve the quality of careand services. There is significant overlap andinterdependence between them, however. 11
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES

(These are explored in more detail in Appendix B.)
1. Government (Department of Human Services) Role
DHS lays the foundation for clinical governance inlegislative, policy and funding frameworks.
2. The Board Role
The board has ultimate responsibility for the clinicalgovernance of a health service, and attention to thismust be as rigorous as that given to other corporateboard responsibilities.
3. The Quality Committee Role
The Quality Committee is the peak patient safety andquality committee in the organisation, however named,and takes an active safety and quality planning,monitoring and evaluation role on behalf of the board.
4. CEO and Senior Clinician and Management Role
The CEO and managers are central to operationalisingclinical governance.
5. Clinician and Team Roles
Whilst the board, CEO and managers provide theprinciples, systems and resources for good clinicalgovernance, it is the staff delivering services whoimplement and monitor these systems day to day.
6. Consumer/Community Role
Consumers want assurance that their care is safe,effective and appropriate. The wider community isbecoming increasingly knowledgeable about healthcare delivery and want to be active participants in thisprocess. The challenge is to involve these groups in ameaningful and positive way for both the consumersand health services.
12
2E Roles and Responsibilities

13
In this section, the principles of the organisational elements of theframework and their application are discussed in more detail: A. Governance, Leadership and CultureB. Consumer InvolvementC. Competence and EducationD. Information Management and Reporting
An example of an organisational approach to an element of safety and quality is given at the end of thissection. Examples of activities that relate to each element for each dimension of quality are found in thematrix in Appendix A.
An
Org
anis
atio
n-w
ide
App
roac
h
03An Organisation-wideApproach to Safety andQuality Improvement

Clinical governance emphasises the importance of boards governing clinical safety andquality with the same rigour as applies to corporate governance. Boards and executivestaff should regularly audit their knowledge and performance to identify gaps anddevelop appropriate orientation and education process to enable the governance role tobe effectively undertaken. Strong support should be given to the organisation pursuingvalid external assessment via an accreditation or certification program.5
A (i) GOVERNANCE
A. Governance, Leadership and Culture
As a minimum, boards should work with the CEO,clinicians and management to develop a quality planthat ensures key areas of risk are prioritised,monitored and regularly reported and that there is aclear and transparent process for responding tosentinel and major adverse events. Staff should beequipped and supported to engage in improving thesafety and quality of patient care. Boards should beconfident that there is a process in place to monitorthe safety of the environment, ensuring that patientcare is carried out by properly credentialed andtrained staff, that external reviews, such asaccreditation, are used as opportunities to reviewcompliance with standards and that consumers areinvolved in safety and quality improvement.
The four principles of effective
clinical governance arising from the
literature are:
build a culture of trust and honesty
through open disclosure in
partnership with consumers and
community
foster organisational commitment
to continuous improvement
establish rigorous monitoring,
reporting and response systems
evaluate and respond to key
aspects of organisational
performance.4
14

15
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
Building the right culture involves, among otherthings, creating a non-punitive environment whereblame is the exception rather than the rule, where theprinciples of open disclosure are embedded ineveryday practice, and where staff willingly report andlearn from problems and adverse events.
Fostering organisational commitment tocontinuous improvement includes assigning clearresponsibility to the CEO for leading a plannedapproach to safety and quality and monitoring keyaspects of organisational safety and qualityperformance. The CEO, in turn, builds anorganisational environment wherein safety and qualityare reviewed and improved through sound planning,committee, leadership, reporting and evaluationstructures at every level.5
Monitoring, reporting and response systemsmust be planned, robust and the focus of health careorganisations should go beyond meeting minimumstandards. The measures reviewed by the board andsubsequent improvements should be based onknowledge of key health care quality and risk issuesand sound safety principles. The focus should be onsystems improvement, while supporting andencouraging the application of evidence-basedpractice by individual clinicians. Boards andexecutives should have in place a process forresponding to adverse events and clinical governanceissues that is clear, transparent and consistent.
Evaluation and response to key aspects oforganisational performance should be approachedwith a strong focus on systems issues and systemsimprovements, as well as supporting andencouraging the application of evidence-basedpractice. Other related considerations include:
ensuring a range of qualitative and quantitativemethods is used to monitor performance
defining and streamlining the reporting processand structure to prevent information overload andensure appropriate feedback
ensuring the health care service responds in aplanned way to important safety and quality matters;
approving policies and changes enabling theorganisation to manage and reduce risks
delegating safety and quality improvement andreporting accountabilities throughout theorganisation
benchmarking and comparing organisationalperformance
sharing lessons learned on safety and qualityacross the health care industry
evaluating the board’s clinical governanceperformance regularly.

16
Lead a Culture of Improvement
Boards and senior managers must lead a culture of improvement. This includes supporting andimplementing relevant policies such as opendisclosure, consumer and community involvementand identifying, analysing and learning from errors andproblems. Improvements and change efforts mustinvolve individuals and teams and encourage inter-departmental and inter-disciplinary communication.Developing a culture of improvement will require thatboards, CEOs and managers at all levels are seen tobe involved in developing, supporting and rewardingstaff involvement. It may also involve identifying,encouraging and resourcing opinion leaders at alllevels to involve staff in various ways.
Empower and Resource Managers at all Levels
Boards and senior managers should empower andresource managers at all levels (both clinical andnon-clinical) to be involved in improving safety andquality. This includes tangible assistance such asfunding administration time, backfilling staff, increasingincentives and removing perverse incentives. It alsorequires the CEO and senior managers to clearlydelineate all managers’ responsibilities for improvingsafety and quality as part of position descriptions andperformance reviews, and for managers to make areciprocal commitment to fulfil those responsibilities.
Managers will be most open to full participation in theQI program when they feel supported by seniormanagers, are clear about the QI goals and their roleand responsibilities for achieving them, trained in theskills they need to fulfil their role and trusted to fulfilthose responsibilities. Another important role forsenior managers in assisting this process is thecreation of organisational slack, or space, formanagers and staff to use the quality program toplan, implement and evaluate innovative approachesto improvement.
Develop an Organisational Quality Improvement Plan
One of the most critical contributions a CEO canmake to an organisational safety and quality programis to lead the development of the organisationalquality improvement plan, which should map outthe why, what, who and how of safety and qualitymonitoring and improvement in the organisation.
Developing the Plan
This plan should be developed in conjunction withother senior and middle managers, clinicians andconsumers, and importantly, incorporateorganisational, consumer and staff professionalvalues. This places the safety and quality program inthe broader context of contributing to the strategicdirection, assists in setting priorities, and helpsengage staff by recognising and incorporating thevalues of those who will implement the program. A key element of this is the translation of the strategicvision for the organisation into operational prioritiesand implications for safety and quality.
Strong leadership is the foundation of an effective safety and quality improvementprogram. A review of both the generic leadership literature and specific safety andquality literature demonstrates four themes for effective leadership of safety and quality6:
A (ii) LEADERSHIP
A. Governance, Leadership and Culture

A quality improvement plan can be structured in manydifferent ways, for example, safety and qualityimprovement activities may be planned on the basisof the dimensions of quality, health service strategicpriorities, safety and quality priorities, organisationalstructures, accreditation frameworks or a combinationof these. Each organisation should develop anapproach that best fits their structure and culture formaximum QI program effectiveness.
The quality improvement plan will facilitate reportingand analysing errors and problems without blame ornegative consequence and outline the process forinvestigating, managing and reducing their occurrence.It will demonstrate that areas of risk are prioritised,monitored and minimised, professional, statutory andexternal standards are met and key areas of care andservice delivery are routinely monitored and improved.Responsibility and accountability of all levels of theorganisation should be clearly delineated at individual,team and committee levels. The policy on issues suchas qualified privilege and associated use of identifieddata should be explained. The board shouldunderstand and endorse the QI plan and be able tosupply documentary evidence of its implementationand outcomes to external evaluators.
Quality Improvement Methodology
The quality and safety process, whether embedded instrategic and operational plans, or a separate, butlinked process, should be built on a simpleimprovement methodology that is relevant to theorganisational context. The key to continuousimprovement is the feedback loop, where data andinformation collected are analysed, acted upon, theresults of action reviewed for effectiveness and allparties concerned kept informed of progress.Common improvement methodologies include: Plan, Do, Study, Act; Monitoring, Assessment, Action,Evaluation; Breakthrough Collaborative; Assess,Diagnose, Review, Implement and Six-Sigma.Whatever methodology is chosen, effective planning,change management approaches, information sharingand leadership are fundamental to success.
Any methodology will encompass a number ofcommon improvement tools and techniques including:
diagnostic, monitoring and priority-setting activitiessuch as identifying and managing risk via clinicalrisk management systems; clinical andperformance indicators; peer review; audit;morbidity and mortality review; improvement teams;practice review against evidence and standards(internal and external) and benchmarking
quantitative and qualitative data collection,analysis and presentation tools such aschecksheets; pareto charts; cause and effectdiagrams; brainstorming; process mapping;interviews and questionnaires
skills for enhancing the effectiveness ofcommunication, discussion and decision-makingsuch as team dynamics; communication andnegotiation skills; meeting processes; presentationskills and problem-solving techniques.
Improvements can be made, evaluated andembedded in an organisation’s process and outcomesin many ways, including:
developing and implementing new standards,policies and procedures
changing processes and practices
systems redesign
education and training
physical and equipment changes
strategic and operational plan review.
All changes should involve those impacted: staff,consumers and the community and otherstakeholders. An effective change managementmethodology that considers both the people andbusiness sides of change is critical to quality programsuccess and should be built into the quality plan.
Whatever method is used, it is critical that the QIprocess doesn’t overwhelm the quality programobjectives: “cynicism comes when the pursuit of theprogram is more important than the pursuit of quality”.11
17
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES

Encourage and Facilitate Staff Participation at all Levels
Quality improvement is often perceived by staff as“the top telling the middle what to do at thebottom”.12 Encouraging and facilitating theorganisation-wide participation of staff in the safetyand quality program is critical to its effectiveness andrelies on a number of leaders, both clinical and non-clinical, working together throughout the organisation.This requires an organisational culture thatencourages effective vertical and horizontalcommunication across professional boundaries and within hierarchies.
Studies of staff involvement in QI in the literature indicatesome key predictors of middle management and staffinvolvement in improvement activities, including:
the extent of support from their direct seniormanager
a belief that the organisation will experienceoutcomes of value from the activities
training in the tools of change and improvement.13
Responsibility for staff participation cannot, therefore, lie with the quality manager and other associatedpersonnel. The quality manager can and should assistwith encouraging staff involvement as a technical expert,for example, ensuring staff are trained and equipped toparticipate, setting up appropriate monitoring andreporting systems and providing guidance with planning,executing and evaluating activities. But the responsibilityfor staff participation in ensuring safe and high qualitycare requires the commitment and development offormal and informal leaders throughout the organisation.
Leadership development in safety and qualitycomprises a number of elements6:
a) A clear understanding of what leadership in safetyand quality means within a particular organisation,for example:
setting the safety and quality agenda
determining priorities
acting as champions
initiating activities.
b) Provision of incentives to take on a safety andquality leadership role such as time, resources,education, data, influence, research andpublication opportunities and supportiveorganisational structures and processes.
c) Specific training to equip leaders including:
managing change
leadership in health care
team building and motivation
safety and quality tools and techniques
meeting skills
negotiation and conflict management
communication and delegation
project planning and management
principles of adult learning.
Training and education should be implementedusing a variety of media:
short courses
mentorship
case studies and discussion
information presented by respected peers
literature, from peer-reviewed journals
action learning.
d) Changes to governance structures and roles toembed safety and quality leadership.
18

Culture is often referred to as ‘the way we do things around here’. Health care is said tohave a distinctive culture, departments and professions within health care have discretecultures and each health care organisation has its own unique culture. This is one of the reasons that quality improvement programs will be most effective if QI frameworks,principles and practices are applied in a way that is acceptable and appropriate to each organisation.
Culture is created from the top of the organisationand maintained at all levels. The culture of health careorganisations is particularly complex due to the natureof health care itself, the organisations in which it takesplace and the broad range of professions involved.Organisational culture may be a primary source ofresistance or a force for major improvement,depending on the initiative.
A health service culture wherein safety and quality arekey to core business requires clear and consistentleadership from boards, CEOs and senior managers.This can only be achieved if addressed in a variety ofways, including being embedded in organisationalstructures and governance, part of theaccountabilities of staff at all levels; activelyencouraged and rewarded; and the consumer voicestrengthened.4,5
Not everyone will embrace a move towards a culture based on clinical governance. Start with those who want to be involved (the innovators andopinion leaders) and demonstrate improvements toencourage others to follow. The cultural changerequired in the move towards clinical governanceshould be values-based, with the organisational and professional values of those involved used as the cultural foundation. In health care, a widely heldvalue is “the desire to help people by offering a highstandard of service in a timely and courteousmanner”.7 QI programs are more likely to fosterinvolvement if both formal and informal opinionleaders are seen to practically support this goal.
It is the responsibility of the board and CEO to createand lead a culture, within which it is easier for staff todo the right thing than not, at an individual, team andorganisational level. This requires a culture whereinsafety and quality improvement are encouraged andrewarded, and supported by structures andprocesses to facilitate involvement.
A (iii) CULTURE
19
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
A. Governance, Leadership and Culture

Consumer and Community Involvement is essential to effective safety and quality improvement.
B. Consumer and Community Involvement
Consumer involvement in quality and safetyimprovement can enhance and guide theorganisational QI program by:
providing a basis for dialogue between healthservices and consumers about improving services
improving the safety, effectiveness,appropriateness and acceptability of individualcare episodes
providing information to health services abouttheir impact on consumers
identifying priorities, expectations and needs
providing information about short and long termoutcomes of health care treatment
developing a culture of consumer and healthservice partnership
improving information quality and availability andconsent processes
engendering consumer and community supportfor health services
developing an understanding of the social view ofhealth and health of communities.1
To achieve this, consumer participation should befacilitated at all levels of the organisation, includingindividual care episodes, information development,strategic and service planning, staff and consumereducation and quality review and improvement. Such participation will necessitate the development of structures, polices and protocols that embedconsumer involvement at all levels of the organisation.
There is a range of material available on strategies forcommunity and consumer participation that will not berepeated here, except to stress that effectivecommunity and consumer involvement will requireeducation and training for both health services staff andthe consumer and community members involved. Thiscan help alleviate some of the difficulties that can befound in this collaboration and may include meetingprocedures, orientation to hospital structures and healthservice decision-making processes for the consumers;and communication, consultation and participativedecision-making skills for health services staff.
Boards, senior managers and committees with aconsumer focus such as Community AdvisoryCommittees, or other consumer oriented groups inthe health service, can monitor the extent ofconsumer participation by receiving information onareas such as: demonstrated evidence of consumerinvolvement in assessment of feedback about servicedelivery; changes as a result of complaints andfeedback; numbers of consumers involved in strategicand service planning and consumer response to newor updated treatment or service information.
20

C. Competence of, and Education to Support, Health Care Providers
Credentialing should be considered by theorganisation on the basis of:
eligibility for professional registration held andcurrent entitlement to practice
qualifications and training includingundergraduate, postgraduate and special trainingwith respect to privileges requested
clinical experience, competence and integrity in thefield of expertise in which privileges are sought
whether the candidates have involved themselves,and will continue to participate in, and subject theresults of clinical work to, quality reviewmechanisms including clinical audit, peer reviewand risk management processes
commitment to past and continuing professionaleducation
satisfactory professional referee reports includingpeer comments
acceptable and safe practice as evidenced bypersonal history of patient complaints, professionalbody investigations, indemnity and legal records
communication skills as demonstrated withpatients/families/communities/health care team
collaboration skills as demonstrated by effectiveinterdisciplinary team activities
management skills as demonstrated by costeffective and efficient resource utilisation
advocacy skills
academic and/or research skills includingcontinuing education aimed at the attainment ofbest practice models and practices.10
Targeted continuing education is a fundamentalcomponent of competence and professionaldevelopment. Education and training is consistentlyidentified in the literature as a key element ofsuccessful quality improvement, whether it be for anorganisation wide program or a specific practiceimprovement activity. This includes technical educationand training to update and improve patient care as wellas training in improvement tools and techniques.Education and training can take many forms, and acombination approach has been shown to be the mosteffective method for encouraging uptake including6:
mentorship
short courses/workshops
case studies
experiential learning opportunities
didactic information presented by respected peers
literature from peer reviewed journals
supervision of junior staff.
Key areas of knowledge for improving quality,specifically, include9:
quality improvement tools and techniques
professional/technical knowledge of best practice
understanding of the profile and needs of consumers
leading and making change in health care
collaboration in single and multi-disciplinary teams
health care processes and systems
human factors
social context and accountability.
Assessing, achieving and maintaining a high level of staff competence at all levels toensure the safe and effective delivery of health care is both a corporate and personalresponsibility. Achieving this requires close attention to recruitment, credentialing, peerreview, skills assessment, clinical supervision, recertification and continuing education.5,10
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
21

D. Information Management and Reporting
Information management should assist inmonitoring and evaluation of areas of risk for the board and senior managers, supporteffective clinical decision making for health care practitioners, inform the planning, delivery and improvement of effective andappropriate services and inform and involveconsumers and the community. The issue ofpublic reporting of safety and quality informationis topical, and Victorian health services arecurrently being encouraged to report publicly via Quality of Care reports.
Data collected for safety and quality should contributeto improvements in the care delivered to patients andto the outcomes of that care. If the results of datacollection and analysis are not fed back to thoseproviding and receiving services and to those whocollected it, meaningful change and improvement are unlikely to occur. Involving clinicians in decisionsabout data collection purpose, method andpresentation may improve reliability, validity and use of the information.1
Medical record documentation is critical to safety and quality, both to assist in care delivery and toinform reviews of the quality of the care provided.Clear, accurate and timely documentation should beencouraged and rewarded.
Boards and senior managers will need to allocateresources to the collection and analysis of timely, valid and reliable data. Data needs will be linked tothe strategic priorities of the safety and qualityprogram, part of which will encompass a reportingschedule of key data for boards, senior managers andkey committees, in much the same way, from a boardperspective particularly, that financial information isreported, discussed and acted upon.
Information management also includes benchmarkingand sourcing and implementing standards andevidence-based practice; in short, anything thatinvolves the collection and application of informationto inform and improve safety and quality.
The suggestions for data collection listed in the matrixin Appendix A should be read in conjunction withother internal and external reporting requirementssuch as those for DHS, funding and accreditation.
22

23
Org
anis
atio
nal
App
roac
h
04Example of an OrganisationalApproach to Safety andQuality Improvement

24
Organisational Elements and Roles:A. Governance, Leadership and CultureA transparent process for identifying, reporting andresponding to sentinel events has been developed byrelevant staff working in high-risk areas in conjunctionwith the relevant patient safety-related committee andsenior management, approved by the board via theQuality Committee, or equivalent committee thatoversees and reports quality and safety issues to theboard, and is documented in the organisational safetyand quality plan. It is clear, when a sentinel event occurs,how it will be managed at the local and organisationallevels, to whom it will be reported and how.
The board, managers and staff are clear about theirroles and responsibilities in reporting and managingthe event, and organisational and local leaders aretrained and equipped to lead the local managementof the event and its consequences. The board andsenior management provide positive feedback andsupport to those involved.
The organisation has implemented an open disclosurepolicy and procedure. Staff have received training in thisand are clear about their obligations in relation todealing with the patient and carers involved in the event.
B. Consumer and Community InvolvementThe organisation’s open disclosure policy clearlydescribes staff and patient rights and responsibilitiesin relation to an adverse event occurring. Patientshave been made aware of this in hospital and wardorientation, but once an event has occurred, this isreiterated to the patient and carers by the relevantsenior clinician with appropriate high-level support asplanned. All steps in the event management processare explained to the patient and carers as per thepolicy and they are kept informed of progress as itoccurs, including the period after discharge.
C. Competency and EducationThe extent to which the sentinel event in questioninvolves issues of competence and/or necessitatesfollow-up education will depend on the event itself.Most sentinel events will occur as a result of systemsbreakdown, where the competency of an individual orteam will not be an issue. The clinical risk manager, inconjunction with the staff and committees involved,may decide that education and training is a necessarypart of the response to the event.
Education and training may be used to assist staff torespond appropriately to the current event (or moreappropriately to the next one) or to equip staff to manageand investigate the event via root cause analysis, systemsreview, and team and communication skills.
If competency or skill is found to be a contributing factorto the event, however, the quality plan should describethe process for the individual or team to be supportedthrough an appropriate education and training process.Other staff involved in the area or clinical care in whichthe event occurred may also receive the training. If theevent is related to a wider concern about an individual orteam competence, this then becomes a professionalissue, to be managed as per the organisational policy,and is removed from the quality process.
D. Information Reporting and ManagementThis is a critical aspect of sentinel event management.The process for event identification reporting andreview should be clearly described in the quality (orrelated clinical risk management) plan. Staff at alllevels should be aware of their roles andresponsibilities in reporting the event. The informationshould be reported in a timely and appropriate fashionto the patient and carers, relevant local and seniormanagers, experts and committees (for example, an infection control event would be reported to theinfection control consultant and the infection controlcommittee) and the peak quality-related committeeand board. The feedback loop should facilitate timelyfeedback to those involved, incorporating support forthe patient and staff involved and clear expectationsof follow up and management.
Responsibility for reporting to external organisationsas appropriate such as the Department of HumanServices, the GP, the Coroner, Consultative Councilsand the insurers should be clearly delegated.
Information gathered in the management of thesentinel event should be fed into the broader safetyand quality information management system where itcan be used at local departmental or committee levelto inform ongoing diagnosis and improvement ofsystems problems.
Example: Sentinel event managementQuality Dimension: Safety

Con
clus
ion
05Conclusion
This framework describes a high quality health care system that has theconsumer as the primary focus and facilitates the health care teamproviding services that are safe, effective, timely and appropriate. In thissystem, clinicians collaborate to produce the best results and are clearabout and committed to their roles and responsibilities for safety andquality. Health care facilities are governed and managed by those with astrong commitment to and responsibility for the quality and safety of thecare and services provided and support this commitment throughpractical strategies. Such a system rejects a punitive approach thatblames individuals for poor quality and works continuously to developstaff and improve the systems of care to identify better ways of working,and to facilitate organisational learning for the purpose of betteraddressing the needs of the population it serves.
25

26
App
endi
x Appendix AThe Safety and Quality Matrix
A

THE SAFETY & QUALITY MATRIX
Safety
Boards accepts ultimate accountability and responsibility for the safety and qualityof services and care and ensure they are fully informed regarding performance inrelation to key areas of risk, patient feedback, service delivery, patient outcomesand staff competence.
Boards and executives delegate accountability for safety at all levels of theorganisation. This involves creating and supporting opportunities for safety andquality leadership development and participation at all levels of the organisation viaprovision of succession planning, education, resources, backfilling and incentivesystems.
Boards create a culture where open disclosure, reporting and learning from errorsand adverse events and clear accountability for and participation in safetyimprovement are embedded and rewarded.
Boards and executives support this culture by resourcing and encouraging rootcause analyses, systems review, implementation of best practice and appropriateeducation and training.
Boards and executives encourage care and service delivery that is patient-focused,and provide an environment where consumers and the community participateequally with health services in safety improvement.
Boards and executives ensure there is a committee, data collection and reportingstructure that facilitates discussion of, and a planned approach to, safety, includingresolution of safety and quality problems, and review and improvement ofperformance.
Executive and senior managers ensure that there is a mechanism in place wherestandards, policies and procedures for safety are regularly reviewed and updated.
Safety is reviewed with regard to the Department of Human Services Clinical RiskManagement Program requirements.
A. GOVERNANCE,LEADERSHIP AND CULTURE
Organisational Element Dimension of Quality: Safety
27
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES

Health care leaders create and support a culture wherein consumer input intoindividual care and overall safety improvement is expected, supported byorganisational policy and procedure, and respected.
Consumers avail themselves of opportunities to participate in the monitoring andimprovement of health care safety, both on an organisational and personal level.
Individual consumers inform themselves of the risks of their care and treatmentchoices by reviewing available information.
Consumers are informed of adverse events, errors and problems relating to theircare and participate in review and corrective action.
Consumers work with clinicians to improve safety by asking appropriate questionsabout, and participating in, the care and treatment they are receiving.
Consumers contribute to the development of consumer information about safetyissues such as risks and side effects.
Consumers take the opportunity to make complaints when dissatisfied, andprovide feedback about care, treatment and services.
Appropriate consent processes are in place to support informed consent.
Health care organisations regularly seek and review consumer complaints andfeedback to identify and address safety issues.
Credentialing is critical to delivery of safe care and services. Credentialingprocedures are designed to ensure that health professionals practice within thelimits of their competence and provide opportunity for regular review and approvalof the scope of an individual’s practice.
Board, executive and senior managers should be satisfied that robust credentialingpolicies and processes are in place for all current clinical staff and that these aresupported by appropriate committee and reporting structures.
Participation in activities that improve the safety of care and services should beconsidered as an element of the credentialing and privilege process. These willinclude specific improvement activities as well as daily contributions to patient carequality such as effective teamwork and communication.
B. CONSUMER AND COMMUNITYINVOLVEMENT
C. COMPETENCE AND EDUCATION
THE SAFETY & QUALITY MATRIX
Safety
Organisational Element Dimension of Quality: Safety
28

THE SAFETY & QUALITY MATRIX
Safety
Board and executive staff should provide sufficient resources to ensure rigoroussystems are in place to recruit and retain competent staff. This includes optimumand consistent processes for advertising, shortlisting, interviewing, selection,orientation, staff development and promotion, and performance review andcoaching. Education and incentives should be put in place to assist managers torecruit and maintain competent staff.
Supervision and mentoring should be provided for new and junior clinical staff.Mechanisms must be established for managers to select and provide appropriatestaff and supervision across each shift.
All clinicians and technical staff skills should be regularly assessed for safety by acompetent peer group to determine competence for performing a particular task orusing a new technology. Methods for early detection of problems with performanceshould be in place.
Where certification (both clinical and non-clinical) applies, mechanisms should be inplace to ensure these are reviewed and current. Provision should be made forpractitioners to update their skills and knowledge as appropriate, and practitionersshould commit to fulfilling this responsibility.
Monitoring of numbers of procedures performed by both individual clinicians, andthe organisation overall, should be undertaken to ensure that sufficient numbers arebeing done to maximise them being carried out in a safe and effective way.
Continuing education regarding safety issues is pivotal. Individual practitioners havea responsibility to undertake continuing education appropriate to their role andspeciality, and also in safety related monitoring, management and improvementtools and techniques. Such education may include:
the nature of error and its management
understanding the impact of culture on safety
effective communication, teamwork and conflict resolution
problem solving and decision making
change management
sharing mental models
human factors
tools and processes for monitoring, analysing and improving safety.
C. COMPETENCE AND EDUCATION(CONT’D)
Organisational Element Dimension of Quality: Safety
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
29

THE SAFETY & QUALITY MATRIX
Safety
Boards and executives are responsible for planning and resourcing an informationsystem on safety that: identifies risk areas, collects and analyses data and reports andfeeds back those data to inform the monitoring, management and improvement ofpatient safety.
Provision is made for clinicians to be involved in collection, analysis and discussion ofrisk-related information via administration time, staff backfilling, easy access to relevantreports and training in appropriate tools. Consumers are involved in discussion anddecision-making regarding improvements resulting from data reporting and analysis.
Safety-related professional, accreditation and industry standards should be widelyavailable and their implementation regularly reviewed against actual practice. Healthservices should fulfil clinical risk management and safety-related DHS reportingrequirements.
A minimum data set, relevant to the health service, should be developed for reportingto the board, peak quality-related committees, executive, managers and clinicianleaders. This should include key areas of risk such as adverse and sentinel events andnear-misses, including, but not restricted to:
a) Medication errors
b) Patient falls
c) Infection control
d) Blood and blood product use
e) Pressure ulcers
f) Pain management
g) Death rates
h) Cases reported to the coroner
i) Sentinel events as defined by the Department of Human Services.
Other areas for review may include:
unplanned return to operating room for certain procedures
unexpected admission to ICU
unexpected deaths and severe complications relating to specific proceduresrelevant to the health service
clinical indicators relating to safety.
D. INFORMATIONMANAGEMENT AND REPORTING
Organisational Element Dimension of Quality: Safety
30

THE SAFETY & QUALITY MATRIX
Effectiveness
Organisational Element Dimension of Quality: Effectiveness
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
31
Sustained improvement in the quality of health care requires a commitment tohealth care based on sound scientific principles and evidence, and the effectivedelivery and communication of that care.
Boards and executives will ensure processes are in place for drawing on theliterature and other sources of research and standards to develop guidelines,pathways, policies and protocols based on sound evidence.
Responsibility and accountability for identification, implementation, review,evaluation and communication of evidence-based care should include involvementof clinicians and opinion leaders to ensure effective local adaptation.
Boards create a culture of recognition and reward for effectiveness of care,treatment and communication, for individual and team-delivered care.
Boards and executives are responsible for creating a culture that respects andencourages patient participation in, and contribution to, the effectiveness of thecare and services provided, including provision of an environment where there areopportunities for patient input and feedback.
Consumers have a key role to play in the effectiveness of care and servicesprovided. This requires collaboration between consumers and clinicians on at leastthree levels: in direct care and associated communication; in patient informationdevelopment; and between the health service and the community in planning,developing and implementing service and care improvement.
Consumers should be involved in developing meaningful information on which tobase decisions about their health and to inform participation in their care.
Consumers and clinicians collaborating on individual care episodes should agreeon a course of treatment, with both parties fulfilling their obligations to ensure thegreatest chance of effectiveness.
Processes for complaints and feedback about care and service effectivenessshould be clear, user-friendly and accessible. Such feedback should be respondedto in a timely fashion and incorporated into service and case review.
A. GOVERNANCE,LEADERSHIP AND CULTURE
B. CONSUMER AND COMMUNITYINVOLVEMENT

THE SAFETY & QUALITY MATRIX
Effectiveness
Individual and team competence are critical to delivery of effective care andservices. Credentialing procedures are designed to ensure that health professionalspractice within the limits of their competence and provide opportunity for regularreview and approval of the scope of individual practice. board, executive and seniormanagers should ensure that robust credentialing policies and processes are inplace for all current clinical staff, backed up by appropriate committee andreporting structures.
All clinicians’ skills should be regularly assessed for effectiveness by a competentpeer group to determine competence for performing a particular task, using a new technology and communication with consumers, their carers and the healthcare team. Methods for early detection of problems with performance should be in place.
Supervision should be provided for new and junior clinical staff. Mechanisms mustbe established for managers to select appropriate staff and supervision acrosseach shift to ensure effective care delivery.
Monitoring of numbers of procedures performed by both individual clinicians, andthe organisation overall, should be undertaken to ensure that sufficient numbers arebeing done to maximise them being carried out in a safe and effective way.
Where certification (both clinical and non-clinical) applies, mechanisms should be inplace to ensure these are reviewed and current. Provision should be made forpractitioners to update their skills and knowledge as appropriate to maintain andimprove effectiveness.
Continuing education regarding effectiveness is pivotal. Individual practitioners have a responsibility to undertake continuing education appropriate to their roleand speciality.
Board and executive staff should provide sufficient resources to ensure rigoroussystems are in place to recruit and retain competent staff. This includes consistentand optimum processes for advertising, shortlisting, interviewing, selection,orientation, staff development and promotion and performance review andcoaching. Support, education and incentives should be put in place to assistmanagers to recruit and maintain effective staff.
C. COMPETENCE AND EDUCATION
Organisational Element Dimension of Quality: Effectiveness
32

THE SAFETY & QUALITY MATRIX
Effectiveness
A range of clinical indicators and audit tools is available for the collection ofprocess and outcome data on the effectiveness of care and services and theseshould be adopted as appropriate.
Processes should be put in place to identify ineffective care and service viamonitoring and review processes such as clinical audit, indicators, adverse eventsand pathway variance analysis.
Information about new technologies and treatments should be made widelyavailable to those involved in their implementation.
There should be a process whereby evidence-based information that has thepotential to improve service and care effectives is identified, locally evaluated andadapted if appropriate. Reviewing the percentage of eligible clinicians who areinvolved in development, application and review of guidelines and evidenceapplication, for example, may assist in informing and identifying clinical leaders andreinforcing the seriousness with which the organisation views these activities.
High risk, high volume and high cost areas should be regularly monitored foreffectiveness and reports sent to relevant clinician leaders in those areas, and tocommittees such as credentialing, new technology and innovation, clinical risk andclinical review for action.
These may include:
% of best practice guidelines in use
% of patients receiving appropriate treatment within the evidence-basedtimeline, eg. prophylactic antibiotics in surgery; stroke admissions having a CATscan with a certain time of arrival in the Emergency Department
Screening rates
Avoidable deaths.
Professional, accreditation and industry standards should be widely available andtheir implementation regularly compared against actual practice.
D. INFORMATIONMANAGEMENT AND REPORTING
Organisational Element Dimension of Quality: Effectiveness
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
33

Patient centred care is key to appropriate treatment. Appropriateness requiresadaptation to each individual patient. This requires patients to participate in theircare by providing all information relevant to treatment decisions. The patient mustbe provided with the means to do so, such as access to interpreters.
Patients should be given the opportunity to increase the appropriateness of theircare by participating in the planning and delivery of their care. This will requirepolicies and protocols to be implemented to embed this in the routine of wards,theatres and other departments.
Consumers and community may be involved in appropriateness by assisting ininformation development for review of disease-specific care and services.
B. CONSUMER AND COMMUNITYINVOLVEMENT
THE SAFETY & QUALITY MATRIX
Appropriateness
Boards and executives have a responsibility to ensure that their health servicesprovide appropriate care.
This requires mechanisms that promote and embed evidence-based practice thatinvolves, and is tailored to, individual patients and is delivered in a timely andcorrect manner.
Boards and executives should delegate accountability for ensuring appropriate careto senior clinicians within an appropriate committee structure.
Boards should receive regular reports on appropriateness issues such as overuse,underuse and misuse of care, including utilisation rates for high volume, high costand high complaint areas.
Overuse should be addressed to reduce undue risk related to interventions andassociated waste. Measures of underuse will require evidence to demonstratewhen a particular intervention should be used, and practice measured against thisto ensure all eligible patients are receiving the maximum health benefit.
A. GOVERNANCE,LEADERSHIP AND CULTURE
Organisational Element Dimension of Quality: Appropriateness
34

THE SAFETY & QUALITY MATRIX
Appropriateness
Appropriateness of care is a consideration for assessing clinician competence andcredentialing. Clinical reviews, adverse events and utilisation rates showingoveruse, underuse and misuse by unit and clinician will assist in the review ofongoing privileges and the need for education and training.
C. COMPETENCE AND EDUCATION
Organisational Element Dimension of Quality: Appropriateness
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
35
Utilisation rates are central to reviewing appropriateness of care. Relevantcomplaints, clinical audit, review of new technologies and procedures and qualityimprovement projects can also be sourced to build a picture of appropriatetreatment in particular disease categories.
High volume, high cost and high complaint areas as relevant to the individual healthservice should be regularly monitored for appropriateness, eg:
caesarean section
coronary angioplasty
cholecystectomy
hysterectomy
lens and cataract procedures
tonsillectomy
colonoscopy
transurethral prostatectomy.
Other measures could include:
numbers of tests ordered for specific conditions
percentage of patients for which a pain assessment is conducted
percentage of specific conditions for which best practice guidelines are applied.
Professional, accreditation and industry standards should be widely available andtheir implementation regularly compared against actual practice.
D. INFORMATIONMANAGEMENT AND REPORTING

The community in general and consumers in particular make a salient contributionto acceptability of care.
Community participation can provide assistance to boards, executives and staff inhealth service planning, delivery, monitoring and evaluation at all levels.
Individual consumers can provide real-time feedback about acceptability of careand services, and there will need to be a process in place whereby suchinformation is sought, noted and fed into a review mechanism.
Consumers should be aware of a clear, accessible complaints process that enablesthem to make a complaint at any time without fear, favour or prejudice. Complaintsshould be viewed as a valuable source of safety and quality information.
Complaints should be dealt with according to a planned process, developed inconjunction with consumers. This process should be made clear to thecomplainant, and include investigation, resolution and follow-up of the complaint incollaboration with the complainant as equal partners in the process.
THE SAFETY & QUALITY MATRIX
Acceptability
Acceptability is the degree to which a service meets or exceeds the expectationsof informed consumers.
Acceptability is key to patient centred care. Boards and executives should developa clear vision of what this means for the health service, in conjunction with clinicaland non-clinical staff, and consumers, and put in place structures and processesfor achieving this.
These may include seeking information from Community Advisory Committeesand/or other community and consumer groups regarding acceptability issues; forexample, reviewing complaints and satisfaction feedback to identify problems andworking with consumers to develop new processes for improving acceptability.
Mechanisms should also be put in place for the collection and application of real-time individual consumer feedback.
Boards and executives should regularly review and reward practitioners and teamsdemonstrating high levels of acceptability in their care, and provide education andsupport to assist all staff to address acceptability in their day-to-day activities.
Acceptability can form a key part of health service staff performance review andcan include feedback from patients and peers.
The Community Advisory Committee, or other consumer focused committee orgroup may be empowered to take the lead on acceptability of care with board andexecutive support.
A. GOVERNANCE,LEADERSHIP AND CULTURE
B. CONSUMER AND COMMUNITYINVOLVEMENT
Organisational Element Dimension of Quality: Acceptability
36

Complaints and other feedback should be actively sought as a valuable source ofacceptability information.
Patient satisfaction, one-to-one interviews and focus groups may be used to elicitinformation. This information should be channelled into a process that reviewssafety and quality data, to help paint a complete picture.
The information should be made available to the staff involved, boards, executivesand department heads for the purposes of review, analysis and action planning.
Boards and executives should ensure that identified problems are addressed to thesatisfaction of consumers and the community, and that consumers are involved inaction planning and follow-up.
Reporting on acceptability issues to consumers and the community should beincluded in the health service Quality of Care report.
Professional, accreditation and industry standards should be widely available andtheir implementation regularly compared against actual practice.
D. INFORMATIONMANAGEMENT AND REPORTING
THE SAFETY & QUALITY MATRIX
Acceptability
C. COMPETENCE AND EDUCATION
Organisational Element Dimension of Quality: Acceptability
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
37
Education and training for staff can be provided in areas such as:
patient rights and responsibilities
patient involvement in their care
communication and consultation
a multidisciplinary team approach to acceptability.
consumers themselves relating their experiences is a powerful educational tool.
Education of consumers to facilitate participation in their care and organisationalimprovement may include:
health service structures and organisation
disease-specific information
administrative processes such as admission and discharge procedures
safety and quality information.
Review of staff competence and performance should include acceptability issuessuch as complaints and feedback from patients and peers.

Access refers to the extent to which a population or individual can obtain healthservices. This may include when it is appropriate to seek health care and the abilityto geographically, physically and economically seek out appropriate care.
Boards have a responsibility to understand the population they serve and to makesound resource allocation decisions regarding how best to serve that population.
Boards should create and foster a culture where resources are utilised to providemaximum access to the community served.
This includes empowering executives and managers to put in place policies andprocedures that streamline admission and discharge procedures and associateddecision-making, address population, geographic and physical access, and reviewutilisation and throughput data.
Consumers on a personal level and the community on a population level can offervaluable input to issues of access.
Individual consumers can comment on their own experience of access to theservice whether it be financial, geographic, physical or processes-related such asadmissions, discharge and waiting time.
Consumers can help improve and streamline access by availing themselves ofrelevant information regarding these processes and following instructions for arrivaltimes, making appointments, booking interpreters and discharge procedures.
The community can participate in strategic decisions affecting access, such asresource allocation, reviews of physical access and service planning and processreview to streamline access.
Consumers and the community can also inform access to information including:public information about the safety and quality of health services; appropriate useof emergency services; clinical treatment choices and options; interpreter issues;risk areas and general information about health service processes to assistconsumers and staff to work together for efficient and effective care.
A. GOVERNANCE,LEADERSHIP AND CULTURE
B. CONSUMER AND COMMUNITYINVOLVEMENT
THE SAFETY & QUALITY MATRIX
Access
Organisational Element Dimension of Quality: Access
38

THE SAFETY & QUALITY MATRIX
Access
Maximising access within available resources requires a high level of expertise in allaccess-related areas: physical, population, processes, prioritisation and resourceallocation. Boards and executives should empower managers to recruit, train andretain personnel who can contribute effectively to this area.
Consumers participating in access-related decisions should be provided withappropriate training to make a considered contribution.
C. COMPETENCE AND EDUCATION
Organisational Element Dimension of Quality: Access
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
39
Valid and reliable information systems are critical to access-related planning anddecision-making. Those involved in access decision-making require robustinformation and training in interpreting and applying the information.
Regular information should inform the board, executive, clinical and non-clinicalmanagers and consumers and the community of the status of access to theirservices. This may include:
waiting list data by category
time to first appointment
waiting times for all services
triage times in Emergency
admission times to various areas of the health services
travel times to the health service
rural and remote patient access issues
access to interpreters
access blocks.
Detailed requirements for access reporting on issues such as hospital demandmanagement reporting are available from DHS.
Professional, accreditation and industry standards should be widely available andtheir implementation regularly compared against actual practice.
D. INFORMATIONMANAGEMENT AND REPORTING

Consumers and community members may participate in efficiency-relateddecisions regarding planning new services or reviewing existing services.
It is important that both communities and health services are well informed to makethese decisions and that discussions follow a clear and transparent process.
Effective decision-making in this complex area will depend on both the consumersand health service staff involved participating in an informed and collaborativemanner. Both parties should be experienced in consumer participation at this level.
B. CONSUMER AND COMMUNITYINVOLVEMENT
THE SAFETY & QUALITY MATRIX
Efficiency
Efficiency is an economic concept that implies that choices in health care deliveryand treatments should be made to derive the maximum total benefit from availableresources.
Setting resource allocation priorities based on economic efficiency requiresconsideration by boards, executives and Clinicians of the relative costs and benefits(or outcomes) of alternative health care interventions. The two relevant aspects ofeconomic efficiency to be considered are technical and allocative efficiency.
Technical efficiency is about providing the highest quality services for the lowestcost. This does not provide sufficient information to decide whether or not aparticular treatment or service should be undertaken in the first place, or whetherone type of treatment is preferable to another.
Allocative efficiency addresses how to achieve the optimal mix of health caretreatments and services to maximise total benefits (outcomes) from availableresources. Two aspects of allocative efficiency are relevant to boards, executivesand clinical leaders: first, choosing between disease states (eg. should morevascular or orthopaedic surgery be undertaken?) and choosing alternatives withindisease states (eg. between prevention initiatives and treatment of lung cancer).
Boards and executives should resource, train and empower clinician, general,finance and IT managers to effectively collaborate in efficiency-related datacollection and decisions.
There is a process in place for identifying and eliminating waste across theorganisation.
A. GOVERNANCE,LEADERSHIP AND CULTURE
Organisational Element Dimension of Quality: Efficiency
40

THE SAFETY & QUALITY MATRIX
Efficiency
Organisational Element Dimension of Quality: Efficiency
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
41
Both health service personnel and any consumers/community members involved inefficiency decisions should be appropriately educated and trained to do so.
Important skills to bring to such discussions include an understanding of resourceallocation and economic concepts as well as problem-solving and decision-makingskills. Those participating will also need to consider the broader funding andstrategic context.
As with all aspects of safety and quality, access to reliable and valid information iscritical to effective efficiency decision-making.
Efficiency requires that general, clinical, financial managers and IT work together topool relevant information.
Boards and executive staff should adequately resource the collection of efficiencyrelated data to ensure informed decisions are made. This may include:
average length of stay
cost per case mix-adjusted separation
cost per outpatient accession of service
eective patients admitted on day of surgery
elective patients cancellations
cost per treatment alternative.
Professional, accreditation and industry standards should be widely available andtheir implementation regularly compared against actual practice.
C. COMPETENCE AND EDUCATION
D. INFORMATIONMANAGEMENT AND REPORTING

There are as many roles in health care safety and quality improvement asthere are people involved. This section of the framework proposes sixkey levels at which responsibilities and accountabilities must be clear andfunctioning effectively to ensure safe and high quality care and services.
App
endi
xB
Appendix BClinical Governance Roles at Six Health System Levels
42

They do this by:
developing and supporting legislation andregulation which promote clinical governance as akey tenet of health service governance
allocating responsibility for clinical governance tohealth service boards and clearly communicatingthe responsibilities and expectations involved
implementing accountability and reportingmechanisms to ensure clinical governanceresponsibilities are met
funding demonstration projects, integratingfindings into policy and facilitating the spread offindings across the health system
supporting health services in managing andreporting quality and safety issues
coordinating state-wide data collection of keyindicator data and providing health services withcomparative performance data
encouraging quality systems development anddata collection through funding incentives.
DHS lays the foundation for clinicalgovernance in legislative, fundingand policy frameworks.
1. Government (Department of Human Services) Role
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
43

The board provides leadership in this area by:
sending a strong message through theorganisation and to the community via words anddeeds that safety and quality are priority issues forthe health service
ensuring the CEO, senior managers and seniorclinicians clearly understand and enact theirresponsibilities and enable clinical governanceprinciples and processes to be applied throughoutthe health service via appropriate structures,policies, processes and resources
monitoring the overall state of safety and quality inthe health service by seeking, analysing anddiscussing relevant information, and responding toissues as appropriate
demonstrating to external and internal reviewbodies that the board understands and carries outits clinical governance role
ensuring a culture and practice of partnership withconsumers and the community in reporting,discussing and addressing adverse events andsafety and quality issues
ensuring the health service acts in accordancewith relevant legislation, regulation and otherrelevant standards and initiatives, and supportingpolicies which improve safety and quality
implementing the four key principles of clinicalgovernance:
build a culture of trust and honesty throughopen disclosure in partnership withconsumers and community
foster organisational commitment tocontinuous improvement
establish rigorous monitoring, reporting andresponse systems
evaluate and respond to key aspects oforganisational performance.4
undertaking regular self assessment as a basis formembers’ clinical governance skills andinformation development.
2. The Board Role
44
The board has ultimate responsibility for patientcare safety and quality and attention to this must be as rigorous as that given to all otherboard corporate responsibilities.

A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
3. The Quality Committee Role
45
It does this by:
working with the CEO and senior managers todetermine the best approach to planning,implementing, evaluating and improving safetyand quality in the organisation, and monitoring theprogress of the approach taken
translating the strategic direction of the healthservice into implications for safety and quality
ensuring the quality plan is related to strategicand business plans, that the CEO is adequatelyresourcing the plan’s implementation and that animprovement methodology appropriate to theorganisation is adopted
analysis and discussion of safety and qualityinformation and taking action, or delegating actionto the CEO, in response to this information
ensuring quality technical support, education,information and opportunity are provided to assiststaff, consumer and community input intoplanning and improving safety and qualitysystems
prioritising and focussing on the key safety andquality issues for the organisation
reporting data and quality plan progress to theboard
evaluating and recommending the implementationof appropriate data collection, education,communication and information tools to facilitateconsumer and staff involvement
developing information and communicationprocesses for public reporting of safety andquality information
responding to DHS and other organisations’safety and quality initiatives and requests.
The Quality Committee, howevernamed, is the peak bodyresponsible for overseeing the quality program in anorganisation. Depending on theorganisation, this may comprise a suite of committees that addressvarious components of quality, a stand-alone committee, or aregular agenda item on anotherbroader committee. Whatever thestructure, the Quality Committeetakes an active safety and qualityplanning, monitoring and evaluationrole on behalf of the board.

They do this by:
espousing and enacting commitment to clinicalgovernance by their attitude to, and involvementin, safety and quality issues
seeking education and information to equipthemselves to lead the safety and quality program
enabling the development and evaluation of asafety and quality plan and structure whichinvolves consumers and clinical and opinionleaders, to monitor, improve and respond to thesafety and quality of care and services
empowering and holding accountable staff at alllevels to be appropriately involved in monitoringand improving care and services
providing planning, infrastructure and resourcesthat enables the collection, reporting andbenchmarking of valid, reliable and relevant safetyand quality data
ensuring systems are in place to facilitate safe,quality care, including the application of bestavailable evidence, learning from problemsexperienced within the organisation and in otherhealth services and systems
ensuring all staff are clear about the principles andpractices of safety and quality by providinginformation, education and technical support, andholding senior staff accountable for modellingdesired behaviour and practices
fostering a culture which does not blame, butrather seeks to solve problems and learn fromthem and supporting staff in this process
establishing open information exchange withconsumers and the wider community, in relation toissues of clinical error, and problems andachievements in service delivery
acting on recommendations where problems withquality are apparent via events or data monitoring
ensuring staff are trained and empowered torespond appropriately to adverse events
providing data and information to the peak qualitycommittee and board relevant to their role, and toDHS and other relevant organisations asappropriate.
4. CEO and Senior Clinician and Management Role
The CEO and managers at all levels are central to operationalising clinical governance.These roles may vary depending on seniority and delegation, but essentially allmanagers play a critical safety and quality leadership role.
46

5. Clinician and Team Role
47
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
They do this by:
providing safety and quality leadership atprofessional and team level
translating high-level quality strategies intooperational improvement activities
participating in the development, implementationand evaluation of quality and safety plans,systems and activities
openly communicating and reporting safety andquality problems and adverse events, andparticipating in developing solutions
adhering to policies and procedures forpreventing, reporting and disclosing adverseevents
delivering care and services according to healthservice protocols and policies
developing a partnership approach with patientsand their carers in individual episodes of care aswell as the prevention, treatment and discussionof adverse events
participating in activities that identify and addressareas for improvement from the patient and staffperspective
participating in a team approach to patient care,quality improvement and problem-solving.
Whilst the board, CEO andmanagers provide the principles,systems and resources for goodclinical governance, it is the staffdelivering services who implementand monitor these systems day to day.

Consumers and the community have a salient role toplay by:
receiving, analysing and responding to informationfrom health services on safety and quality issuesin the spirit in which it is offered, that is, as asystems learning and improvement mechanism
offering constructive feedback, both formal andinformal, regarding the safety and quality of healthservices, both as individual consumers and as acommunity of stakeholders
working with health services to improve services,both in response to an individual adverse eventand at a systems review level
feedback to the health service regardingexperiences of the care provided
developing disease-specific and generalinformation to assist other consumers to betternavigate care and services
contributing to safety and quality improvement viainvolvement in individual episodes of care,information development, education and systemsreview
taking responsibility for health service safety byseeking relevant information and asking pertinentquestions of both individual health practitioners asconsumers and of the organisation as a whole.
6. Consumer/Community Role
Consumers want assurance that their care issafe, effective and appropriate. The widercommunity is becoming increasinglyknowledgeable about health care delivery andwant to be active participants in this process.The challenge is to involve these groups in ameaningful and positive way.
48

App
endi
x
CAppendix CChecklist for Reviewing your Safety and QualityProgram Against the Framework Elements
49

50
This checklist is a tool to assist health services review their safety and quality programagainst the framework elements. It is not intended as a review of the effectiveness of aquality program, but as a guide to the generic structural and process elements essentialto achieving effectiveness.It may be undertaken as a self-assessment at all levels of the organisation, or as a focus for discussion about the quality program.
Where an element is checked as “process established and working effectively”, the next question to be answered is “how do we know?”
The board:
a. governs clinical safety and quality with the samerigour as applied to corporate governance andreviews this via regular self-assessment
b. discusses and responds to priority safety andquality matters at every board meeting
c. regularly reinforces and demonstratescommitment to safety and quality to allstakeholders
d. empowers and supports the CEO to take steps toassure and improve safety and quality
e. ensures consumers are informed of, and activelyinvolved in, key improvement initiatives
f. ensures safety and quality initiatives areconsistent with government and quality councilpriorities and external requirements
g. commits a defined percentage of the annualbudget to achieving defined safety and qualitygoals and monitors expenditure and associatedoutcomes
h. clarifies the direction and priorities for safety andquality in the strategic plan
i. establishes measurable performance goals andtargets
j. establishes clinical safety and quality as coreorganisational values
k. ensures the organisation benchmarks andcompares performance in safety and quality
Processesestablished
and workingeffectively
Processes inplace but need
enhancement
Processesunder
development
No processesin place for
this element
1. GOVERNANCE, LEADERSHIP AND CULTURE

51
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
The CEO and leaders throughout the organisation:
l. actively support and assist the board in theclinical governance role
m. ensures clinician and staff buy-in to help developand implement safety and quality initiatives
n. focus strongly on reducing preventable errors byimproving systems
o. ensure safety and quality risks are proactivelyidentified and managed through effective systems,delegation of accountabilities and properly trainedand credentialed staff
p. ensure changes and improvements are sustainedbeyond the short-term
q. assign sufficient personnel and resources tosupport the organisation’s safety and qualityinitiatives
r. establish a non-punitive environment,apportioning blame only in exceptional andappropriate circumstances
s. ensure staff, consumers and other stakeholdersare informed about (and actively involved in) theorganisation’s safety and quality issues andinitiatives
t. encourage and reward safety and qualityimprovements
u. ensure the organisational values and structuressupport staff to openly disclose errors
v. support the implementation of an improvementplan and methodology relevant to theorganisational structure and culture, based onbest available evidence, innovation and systemsimprovement
w. openly, willingly and regularly report relevantsafety and quality issues and improvements tostakeholders, including action taken to addressproblems
x. respond to and share lessons learned with thewider health care community
Processesestablished
and workingeffectively
Processes inplace but need
enhancement
Processesunder
development
No processesin place for
this element
1. GOVERNANCE, LEADERSHIP AND CULTURE

a. consumer and community participation inimproving safety and quality is an accepted partof the organisation’s functioning
b. consumer and community feedback is regularlysought and is integrated into improvementactivities
c. complaints are managed respectfully andeffectively and the information fed into systemsimprovements
d. protocols are in place to enable consumers toparticipate in their care
e. consumers are made aware of the process forparticipating in their care
f. sufficient information and opportunity are providedfor consumers to participate meaningfully in theircare
g. health service staff are aware of, and trained in,protocols and procedures for enabling consumerparticipation in their care, including effectivecommunication
h. consumers and community members are involvedin consumer information development
i. consumers are invited to relate their health serviceexperiences as part of the safety and qualityimprovement program
j. consumers and community members are invitedto review and improve current services and assistin planning new ones
Processesestablished
and workingeffectively
Processes inplace but need
enhancement
Processesunder
development
No processesin place for
this element
2. CONSUMER AND COMMUNITY INVOLVEMENT
52

53
A SAFETY AND QUALITY IMPROVEMENT FRAMEWORK FOR VICTORIA’S HEALTH SERVICES
a. robust certification and credentialing policies andprocedures are in place for all current clinical staff
b. credentialing responsibilities are clearly delineatedto organisational leaders and committees
c. participation in activities that improve the safetyand quality of the care delivered is considered asa key element of credentialing
d. there is a policy and procedure in place forsupervision and mentoring of new and junior staff,both clinical and non-clinical
e. appropriately trained and qualified staff arerostered across each shift
f. support, education and resources are allocated toassist managers with successful recruitment andretention of staff
g. clinician and technical staff skills are regularlyassessed for safety by a competent peer group
h. regular checks are performed to ascertain thatclinicians are performing sufficient numbers ofprocedures to maximise the chances of thembeing performed safely
i. continuing clinical education is encouraged andsupported and clinician responsibility to keepabreast of current knowledge and evidence-basedpractice is fulfilled
j. all staff are trained and equipped to participateeffectively in safety and quality improvementactivities
k. clinical staff understand safety improvementtechniques such as error prevention andmanagement, effective teamwork andcommunication, and human factor analysis
Processesestablished
and workingeffectively
Processes inplace but need
enhancement
Processesunder
development
No processesin place for
this element
3. COMPETENCE AND EDUCATION

a. sufficiently rigorous information systems are inplace to identify, monitor and respond to risks andimportant aspects of care
b. there is an effective information flow for safety andquality matters to and from the board
c. the organisation meets external stakeholderreporting requirements including: DHS,accreditation, insurance and coroner requirements
d. a minimum data set, relevant to the safety andquality priorities of the organisation, is regularlyreported to the board, CEO and organisationalleaders and committees
e. data reported are discussed, responded toappropriately, including a feedback loop to thosewho initiated the data collection
f. safety and quality-related professional,accreditation and industry standards are widelyavailable and their implementation regularlyreviewed
g. the board, CEO and senior clinicians andmanagers encourage and reward reporting andlearning from errors and adverse events
h. results of improvement activities are widelycirculated
i. consumers have access to, and contribute to,reliable information about their care and relatedhealth care services
j. all patients sustaining an adverse event areinformed of the event and proposed follow-up in atimely and appropriate manner
k. staff willingness to report adverse events isreviewed and responded to
Processesestablished
and workingeffectively
Processes inplace but need
enhancement
Processesunder
development
No processesin place for
this element
4. INFORMATION MANAGEMENT AND REPORTING
54

App
endi
x
DAppendix DAcknowledgements
55

56
References
1. NSW Health, 1999, A Framework for Managingthe Quality of Health Services in NSW, NSWHealth Department, Sydney.
2. Australian Council for Safety and Quality in HealthCare, 2001, 1st National Report on Patient Safety,Canberra.
3. Victorian Department of Human Services, 2003Hospital Admission Risk Program, Melbourne.
4. McLean, J 2002, The Board’s Clinical GovernanceRole, Discussion Paper, Bayside Health, Melbourne.
5. Douglas, N, Ross, H, Davies, J, 2003,Investigations, Inquiries and Royal Commissions:Do They Effect Change? papers presented inPlenary Session 5, The Australian Conference onSafety and Quality in Health Care, Perth.
6. Victorian Quality Council, 2003, Discussion paperson Safety and Quality Education and ClinicalLeadership, Melbourne.
7. Ham, C, 2003, Improving the performance ofhealth services: the role of clinical leadership, The Lancet, published online March 25.
8. Consumer Focus Collaboration, 2000, Improvinghealth services through consumer participation – a resource guide for organisations, CommonwealthDepartment of Health and Aged Care, Canberra.
9. Batalden, PB, Berwick, D, Bisongano, G 1998,Knowledge domains for health care studentsseeking competency in the continual improvementand innovation of health care, Institute for HealthCare Improvement, Boston.
10. ACSQHC 2002, National Guidelines for Credentialsand Clinical Privileges, Australian Council for Safetyand Quality in Health Care, Canberra.
11. Yandrick, RM 1994, ‘Corrosive effects of failed TQ efforts’, Quality, vol. 33, no. 3, pp. 26-28.
12. Davies, H & Fisher, R 2001 ‘Engaging middlemanagers in TQM’, Paper presented at the ThirdInternational Conference on Quality, Innovationand Knowledge Management, Malaysia.
13. Australian Council on Healthcare Standards,2002, The EQuIP Guide, 3rd ed., ACHS, Sydney.
14. ACHS, 2003 ACHS News, Issue 12, ACHS, Sydney.
VQC Clinical Governance Working Group
Dr Michael Walsh (Chair)
Professor Peter Choong
Dr David Hillis
Dr Jane Hendtlass
Dr Peter Greenberg
Dr Christine Walker
Associate Professor Christine Kilpatrick
Mrs Kerry Bradley
Ms Stella Axarlis (up to 16 June 2003)
Dr Cathy Balding (VQC Manager)
Health services that provided feedback
Austin Health
Barwon Health
Bayside Health
Echuca Regional Health
Goulburn Valley Health
Mercy Hospital for Women
Moyne Health Service
Peter Mac
Royal Victorian Eye & Ear Hospital
St Vincent’s Health
West Wimmera Health Service
Department of Human Services
Dr Jenny Bartlett (Chief Clinical Advisor)
Ms Sue Brennan (Manager, Residential ServicesUnit, Aged Care)
The Victorian Quality Council gratefully acknowledges funding from the Victorian Department of Human Services.
Written by Cathy Balding on behalf of the VQCClinical Governance Working Group.
The Victorian Quality Council thanks all those who contributed to this framework.

“Different sections of the framework will be usefulfor different parts of the organisation.”(Metropolitan health service quality manager)
“One of the difficulties that CEOs face is
establishing a connected organisational
structure and a safety and quality structure,
and this framework allows for a
re-assessment of existing structures.”
“The clear message is that there must be
total commitment from the top and that
means that the Board needs to be educated
in their role and makes it clear to the CEO
what is expected.” (Metropolitan health service CEO)
“This document will set the structure,
identify the parameters and gain more
recognition for clinical governance.”(Rural hospital DON)
“It makes sense for our organisation
and the framework is easy to
understand.”(Metro health service DON)“The framework is practical and clear.”
(Specialist health service quality manager)
“I particularly liked the proposed minimum
data set.”(Regional health service CEO)
“It is an easy to read, common sense
approach to the implementation of a safety
and quality [framework] within health
services.”(Rural health service quality manager)
“The information on roles and responsibilitieswill be integrated into our staff developmentprogram.”(Metropolitan health service CEO)
“We will incorporate the practical
examples into our quality plan.”(Regional health service clinical risk manager)
“We will use this as a benchmark to
review our existing quality program
and plan for the future.”(Regional health service medical director)
3233

XANDRA APOLLO BAY ARARAT BACCHUS MARSH BAIRNSDALE BALLARAT BEAUFORT BEECHWORTH BENALDIGO BOORT BOX HILL BROADMEADOWS BUNDOORA BURWOOD EAST CANTERBURY CARLTON CASTERTOEMAINE CAUFIELD CHELTENHAM CLAYTON COBRAM COHUNA COLAC COLERAINE CORRYONG DANDENON
AYLESFORD EAST BENTLEIGH EAST MELBOURNE EAST RINGWOOD ECHUCA EDENHOPE EPPING FITZROY OOTSCRAY FOSTER FRANKSTON GEELONG HAMILTON HAMPTON HEALESVILLE HEATHCOTE HEIDELBERG OOD HORSHAM INGLEWOOD KERANG KEW KILMORE KOOWEERUP KYABRAM KYNETON LEONGATHA LORON MANANGATANG MANSFIELD MARYBOROUGH MILDURA MT ELIZA MYRTLEFORD NATHALIA NHILL NOBL
K NUMURKAH OMEO ORBOST OUYEN PARKVILLE PORT FAIRY PORTLAND PRAHAN ROBINVALE ROCHESTEBUD RUPANYUP SALE SANDRINGHAM SEYMOUR SHEPPARTON ST ALBANS ST ARNAUD STAWELL SWAN HINGATTA TERANG TIMBOON TRARALGON UPPER FERNTREE GULLY WANGARATTA WARRACKNABEAL WARRAGRNAMBOOL WERRIBEE WILLIAMSTOWN WINCHELSEA WODONGA WONTHAGGI YARRAM YARRAWONGA YEAANDRA APOLLO BAY ARARAT BACCHUS MARSH BAIRNSDALE BALLARAT BEAUFORT BEECHWORTH BENALLDIGO BOORT BOX HILL BROADMEADOWS BUNDOORA BURWOOD EAST CANTERBURY CARLTON CASTERTOEMAINE CAUFIELD CHELTENHAM CLAYTON COBRAM COHUNA COLAC COLERAINE CORRYONG DANDENON
AYLESFORD EAST BENTLEIGH EAST MELBOURNE EAST RINGWOOD ECHUCA EDENHOPE EPPING FITZROY OOTSCRAY FOSTER FRANKSTON GEELONG HAMILTON HAMPTON HEALESVILLE HEATHCOTE HEIDELBERG OOD HORSHAM INGLEWOOD KERANG KEW KILMORE KOOWEERUP KYABRAM KYNETON LEONGATHA LORON MANANGATANG MANSFIELD MARYBOROUGH MILDURA MT ELIZA MYRTLEFORD NATHALIA NHILL NOBL
K NUMURKAH OMEO ORBOST OUYEN PARKVILLE PORT FAIRY PORTLAND PRAHAN ROBINVALE ROCHESTEBUD RUPANYUP SALE SANDRINGHAM SEYMOUR SHEPPARTON ST ALBANS ST ARNAUD STAWELL SWAN HINGATTA TERANG TIMBOON TRARALGON UPPER FERNTREE GULLY WANGARATTA WARRACKNABEAL WARRAGRNAMBOOL WERRIBEE WILLIAMSTOWN WINCHELSEA WODONGA WONTHAGGI YARRAM YARRAWONGA YEAANDRA APOLLO BAY ARARAT BACCHUS MARSH BAIRNSDALE BALLARAT BEAUFORT BEECHWORTH BENALLDIGO BOORT BOX HILL BROADMEADOWS BUNDOORA BURWOOD EAST CANTERBURY CARLTON CASTERTOEMAINE CAUFIELD CHELTENHAM CLAYTON COBRAM COHUNA COLAC COLERAINE CORRYONG DANDENON
AYLESFORD EAST BENTLEIGH EAST MELBOURNE EAST RINGWOOD ECHUCA EDENHOPE EPPING FITZROY OOTSCRAY FOSTER FRANKSTON GEELONG HAMILTON HAMPTON HEALESVILLE HEATHCOTE HEIDELBERG OOD HORSHAM INGLEWOOD KERANG KEW KILMORE KOOWEERUP KYABRAM KYNETON LEONGATHA LORON MANANGATANG MANSFIELD MARYBOROUGH MILDURA MT ELIZA MYRTLEFORD NATHALIA NHILL NOBL
K NUMURKAH OMEO ORBOST OUYEN PARKVILLE PORT FAIRY PORTLAND PRAHAN ROBINVALE ROCHESTEBUD RUPANYUP SALE SANDRINGHAM SEYMOUR SHEPPARTON ST ALBANS ST ARNAUD STAWELL SWAN HINGATTA TERANG TIMBOON TRARALGON UPPER FERNTREE GULLY WANGARATTA WARRACKNABEAL WARRAG
Better Quality,Better Health Care