Embed Size (px)
Citation preview
Beware: Ptosis with Exophthalmos
A rearview perspective Wade Reardon, MD Resident Physician, MUSC Storm Eye Institute Dr. Pamela Chavis, MD, project advisor
Analysis of Ocular Myasthenia Gravis and Thyroid Eye Disease
Financial Disclosures O None
Purpose O To examine:
O The co-existence of Thyroid eye disease with Ocular myasthenia
O Time to co-diagnosis O Potentially life threatening
complications
Background
1. Skuta G, et al. Basic and Clinical Science Course: Orbit, Eyelids and Lacrimal System, 2012. 2. Skuta, G, et al. Basic and Clinical Science Course: Update on General Medicine, 2012.
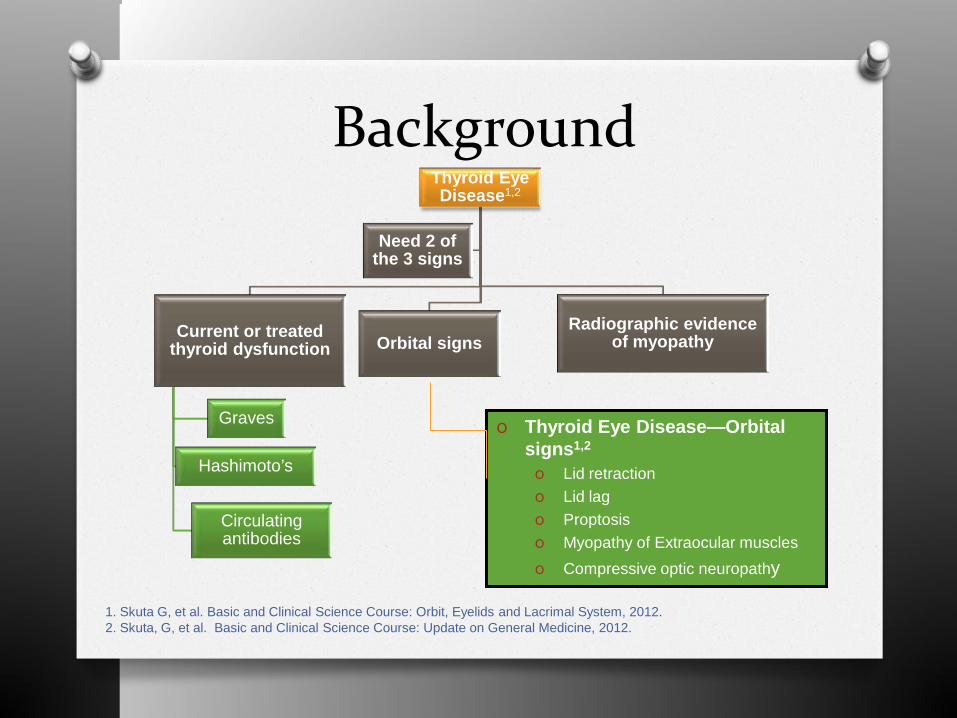
Thyroid Eye Disease1,2
Current or treated thyroid dysfunction
Graves
Hashimoto’s
Circulating antibodies
Orbital signs Radiographic evidence
of myopathy
Need 2 of the 3 signs
O Thyroid Eye Disease—Orbital signs1,2
O Lid retraction O Lid lag O Proptosis O Myopathy of Extraocular muscles O Compressive optic neuropathy
Background O Myasthenia Gravis– fluctuation and
fatiguability (ocular)3 O Ptosis (fatiguing) O Cogan’s Lid twitch O Enhancement of ptosis O Diplopia (variable degrees on serial
exams) O Obicularis oculi weakness
O Incidence roughly 1:10,000 to 1:50,000
3. Skuta, G, et al. Basic and Clinical Science Course: Neuro-Ophthalmology, 2012 4. Sathasivam, S. Current and emerging Treatments for the management of myasthenia gravis. Therapeutics and Clinical Risk management. 2011:7, 313-323 5. Mappouras, D. et al. Antibodies to acetylcholinesterase cross-reacting with thyroglobulin in myasthenia gravis and Graves disease. Clinical Exp Immunology 1995; 100: 336-343
Background O Myasthenia Gravis3,4,5:Important to
recognize O 85% of pts with ocular MGsystemic
disease in 2 years O 20% will need intubation and/or ventilator
support due to myasthenic crises in <1 year O Autoimmune related, Ab’s:
O Acetylcholine receptor (modulating, binding, blocking)
O Muscle Specific Kinase
3. Skuta, G, et al. Basic and Clinical Science Course: Neuro-Ophthalmology, 2012 4. Sathasivam, S. Current and emerging Treatments for the management of myasthenia gravis. Therapeutics and Clinical Risk management. 2011:7, 313-323 5. Mappouras, D. et al. Antibodies to acetylcholinesterase cross-reacting with thyroglobulin in myasthenia gravis and Graves disease. Clinical Exp Immunology 1995; 100: 336-343
Methods O Retrospective review of patient data,
spanning from 2005-2013 O 9 patients selected
O TED + Myasthenia Gravis
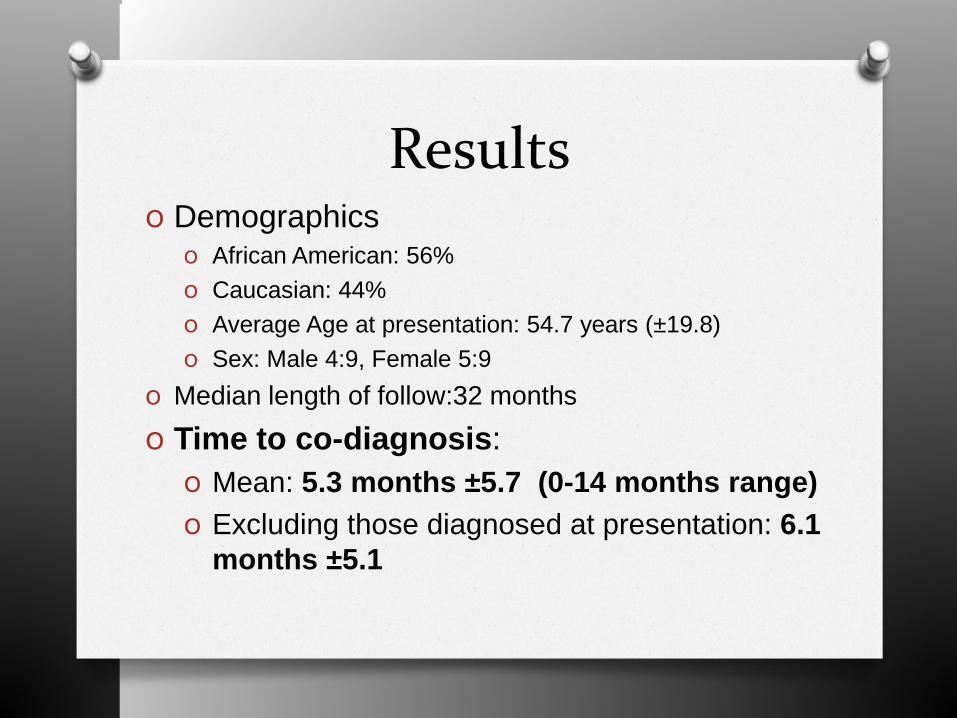
Results O Demographics
O African American: 56% O Caucasian: 44% O Average Age at presentation: 54.7 years (±19.8) O Sex: Male 4:9, Female 5:9
O Median length of follow:32 months
O Time to co-diagnosis: O Mean: 5.3 months ±5.7 (0-14 months range) O Excluding those diagnosed at presentation: 6.1
months ±5.1
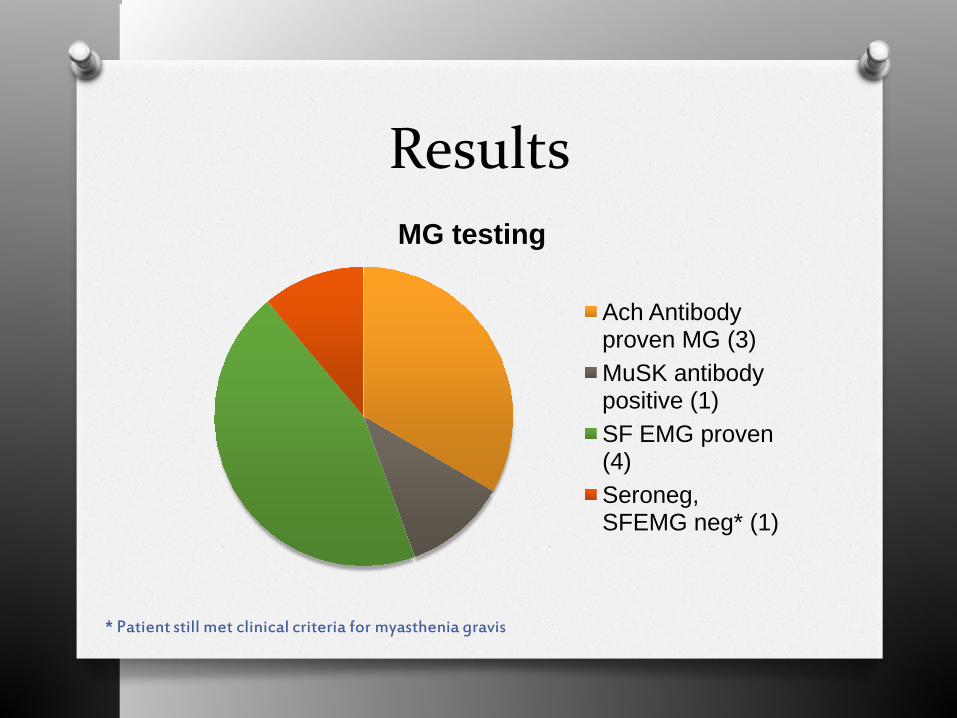
Results MG testing
Ach Antibody proven MG (3) MuSK antibody positive (1) SF EMG proven (4) Seroneg, SFEMG neg* (1)
* Patient still met clinical criteria for myasthenia gravis
Results O Complications:
O 2 patients were known to have severe respiratory issues O 1 of which had multiple hospitalizations for
respiratory crises O Same patient required ventilator assistance
prior to diagnosis of myasthenia
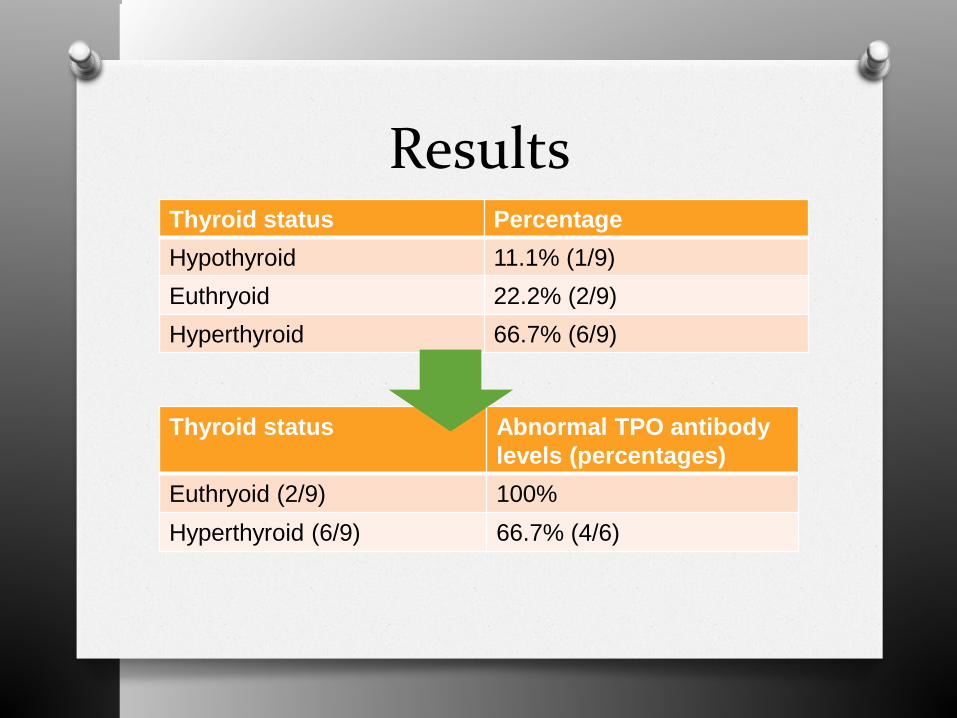
Results Thyroid status Percentage Hypothyroid 11.1% (1/9) Euthryoid 22.2% (2/9) Hyperthyroid 66.7% (6/9)
Thyroid status Abnormal TPO antibody levels (percentages)
Euthryoid (2/9) 100% Hyperthyroid (6/9) 66.7% (4/6)
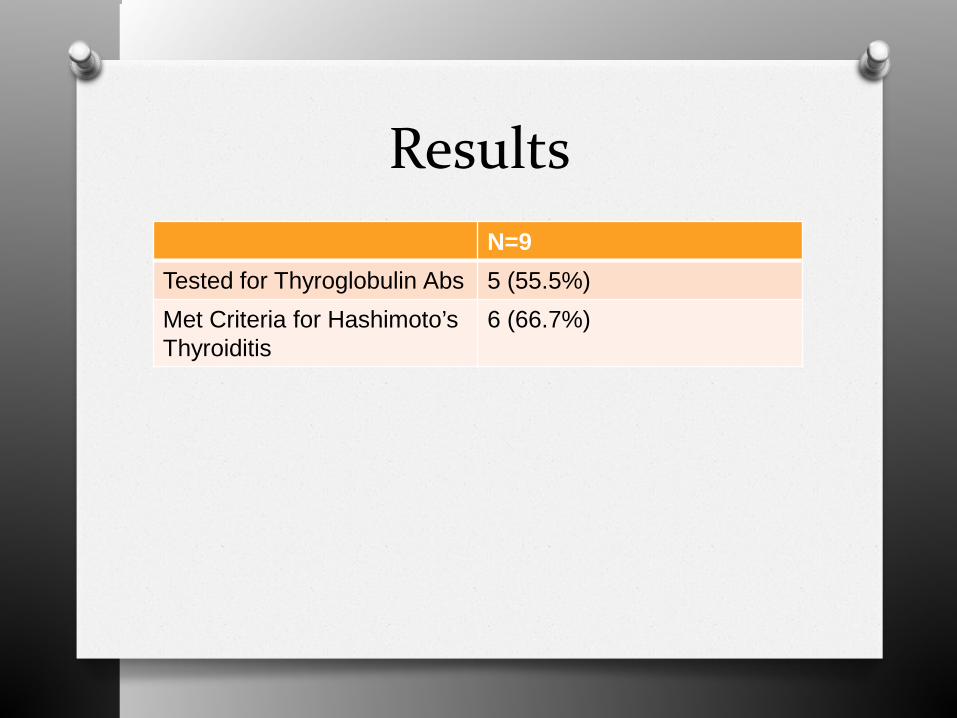
Results N=9
Tested for Thyroglobulin Abs 5 (55.5%) Met Criteria for Hashimoto’s Thyroiditis
6 (66.7%)
Conclusions/Pearls O MG and TED are not mutually exclusive,
but can exist simultaneously O Antibody testing alone is insufficient if
negative O Follow of up to 1 year may be needed to
make co-diagnosis O If MG is missed, could have dire
consequences O Hashimoto’s thyroiditis should be
considered in patients with apparent TED and MG
Thank you O Dr. Pamela Chavis O Dr. David Stickler O Ms. Brenda Thompson O Dr. Lucian Del Priore O Dr. Rupal Trivedi
Questions?
![Index [link.springer.com]978-0-387-92855-5/1.pdf · Bell’s palsy acquired myogenic ptosis, 95 congenital myogenic ptosis, 79 involutional ptosis, 74 patient selection, 156 prior](https://img.pdfslide.net/doc/110x75/5e0ec41cf5a39e518c0f1033/index-link-978-0-387-92855-51pdf-bellas-palsy-acquired-myogenic-ptosis.jpg)










![ptosis [emedicine]](https://img.pdfslide.net/doc/110x75/577cdd4a1a28ab9e78acb3ee/ptosis-emedicine.jpg)