Embed Size (px)
Citation preview

Downloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.org
Beyond Hydronephrosis: Ultrasound of the Kidneys with CT and MR correlation
Brian C. Allen, MDMelanie P. Caserta, MD
Downloaded from sar2013.conferencespot.org

LEARNING OBJECTIVES
Indications for US InfectionRenal MassesEchogenic structuresVascular
Downloaded from sar2013.conferencespot.org

INDICATIONS FOR RENAL ULTRASOUND
Renal Failure – evaluate for hydronephrosis (rare cause), medical renal disease Hematuria – stones, mass Complications of Infection Congenital vs acquired anomalies Characterize lesions seen by CT – is it a cyst or solid
mass? Renal Vascular Evaluation Renal vein thrombosis Renal artery stenosis (MRA or CTA study of
choice) AVF, pseudoaneurysm etc…
Downloaded from sar2013.conferencespot.org

RENAL INFECTION: IMAGING APPROACH
Uncomplicated pyelonephritis No imaging needed Often normal imaging appearance
Complicated pyelonephritis US – primary role to look for complications Evaluate for pyonephrosis, large renal/perirenal
abscesses, obstruction, stones as possible nidus for infection
CT Small abscesses, gas forming infection
Downloaded from sar2013.conferencespot.org

PYELONEPHRITIS
Focal pyelonephritis may appear echogenic due to hemorrhage
Look For:Renal enlargementHypo or hyper echogenicityPatchy echogenicityThickened urotheliumLoss of CM differentiationAbscess
Downloaded from sar2013.conferencespot.org

COMPLICATIONS OF PYELONEPHRITIS: ABSCESS
Look for: Poorly marginated, thick
walled hypoechoic mass Internal debris Acoustic enhancement May appear solid
Should not have internal flow
Stones or gas Perinephric extension
Standard treatment Percutaneous drainage +
antibiotics If small, can be treated
effectively with antibioticsDownloaded from sar2013.conferencespot.org

COMPLICATIONS OF RENAL INFECTION: PYONEPHROSIS
Look for: Presence of mobile debris and
layering material in a hydronephrotic kidney This is an accurate (96%) sign to
differentiate pyonephrosis from hydronephrosis in patients with clinical evidence of renal infection1
Thickening of urothelial lining Treatment = percutaneous
nephrostomy Can cause rapid and permanent
decrease in renal function Can progress to sepsis if not
treated quickly
1 AJR 1983;140: 991-993.Downloaded from sar2013.conferencespot.org

COMPLICATIONS OF RENAL INFECTION: EMPHYSEMATOUS PYELONEPHRITIS
Almost exclusively in diabetics Also seen in immunocompromised Obstruction is also a risk factor
Aggressive variant of acute pyelonephritis Can be fatal
Two types Type I = True emphysematous pyelonephritis Surgical emergency – Tx is nephrectomy + Abx
Type II = Renal or perirenal fluid and gas containing abscess +/- gas in renal pelvis
If suspected on US Get a CT to determine location and extent of gas
Downloaded from sar2013.conferencespot.org

COMPLICATIONS OF RENAL INFECTION: EMPHYSEMATOUS PYELONEPHRITIS
Highly echogenic areas within renal parenchyma with shadowing Ring down artifacts from air bubbles Gas in perinephric space may obscure kidney
COURTESY OF HISHAM TCHELEPI, MDDownloaded from sar2013.conferencespot.org

RENAL INFECTION: LESS COMMON ENTITIES
Tuberculosis Infection = reactivation of hematogenous spread Most common clinical manifestation of extrapulmonary TB1
General Imaging Features in Urinary Tract Calcification Cavities Strictures +/- Abdominal LAD
Xanthogranulomatous pyelonephritis (XGP)2
Chronic inflammatory process associated with longstanding obstruction Pathologic response to infection is the formation of inflammatory masses by lipid
laden macrophages Organisms: P. mirabilis, E. coli
Opportunistic Infection (Immunocompromised patients) Transplant patients at risk Fungal Infection
HIV nephropathy1 RadioGraphics 2007; 27:1255-1273 2 RadioGraphics 2008; 28: 255-276 Downloaded from sar2013.conferencespot.org

RENAL INFECTION: LESS COMMON ENTITIES
TB US insensitive for early disease but look for1: Irregular hypoechoic masses connecting to collecting system
without hydronephrosis Papillary destruction/necrosis Echogenic masses in pyramids Distorted renal contour Calcifications Urothelial mucosal thickening Small fibrotic thick walled bladder
XGP US appearance Staghorn stone in pelvis + dilated calyces Perinephric fluid Perinephric inflammatory tissue Anechoic or hypoechoic round masses replacing renal parenchyma
1 RadioGraphics 2007; 27:1255-1273Downloaded from sar2013.conferencespot.org
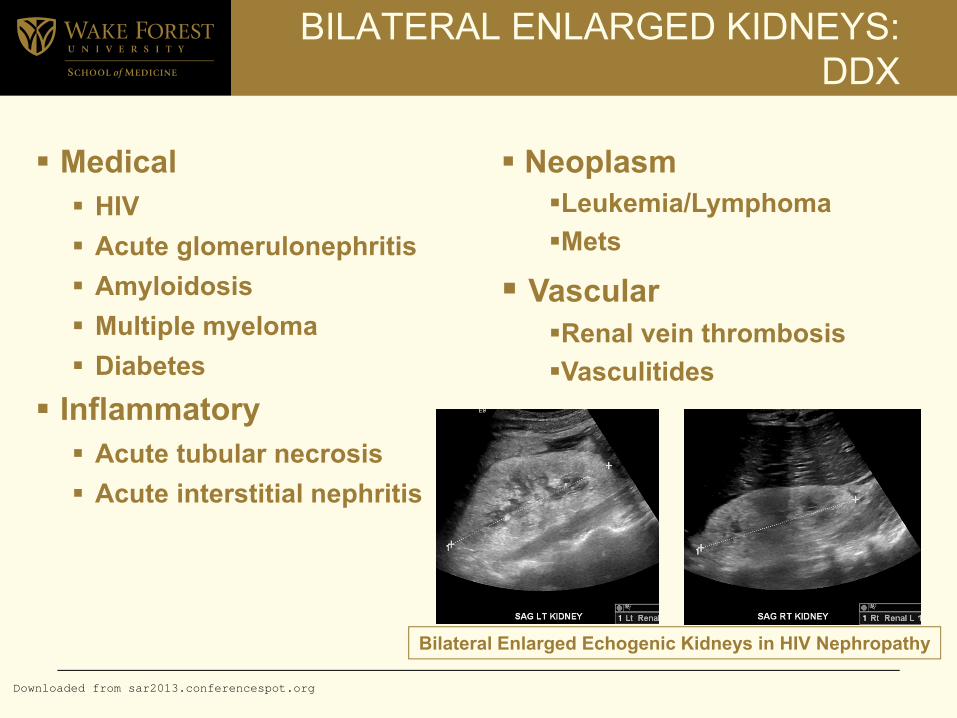
BILATERAL ENLARGED KIDNEYS: DDX
Medical HIV Acute glomerulonephritis Amyloidosis Multiple myeloma Diabetes
Inflammatory Acute tubular necrosis Acute interstitial nephritis
NeoplasmLeukemia/LymphomaMets
VascularRenal vein thrombosisVasculitides
Bilateral Enlarged Echogenic Kidneys in HIV Nephropathy
Downloaded from sar2013.conferencespot.org

RENAL MASS:IMAGING APPROACH
Cyst or solid? Internal architecture of a cystic lesion is often better seen on US
than on CT Expansile vs Infiltrative (Ball vs Bean)? Fat containing? Solitary or Multiple? Low threshold for recommending CT or MR if suspect a mass Watch out for mimics of mass – high frequency techniques may help
sort these out Dromedary hump Fetal Lobulation Focal parenchymal hypertrophy adjacent to scar
TCC Faceless kidney appearance Fungus ball and blood clot in ddx when see material in collecting
system
Downloaded from sar2013.conferencespot.org

CYST
US can show more complex internal architecture than CT Don’t apply the Bosniak Classification to cysts on US1
Simple Cyst Complex cyst Recommend CT/MRI for further
characterization if: Thickened wall Multiple or thick septations Extensive mural or septal calcification Mural or septal nodularity Thick or nodular calcifications
6 month follow up US if: Internal echoes Few thin septations
1 Radiology 2011; 262: 781-785Downloaded from sar2013.conferencespot.org

ANGIOMYOLIPOMA
Most common benign renal tumorMost are detected incidentally Tumor size >4cm = increased bleeding risk Lipid rich AML is characteristically echogenic
BUT need to confirm fat content!May have increased flow on color Doppler
which can make it difficult to differentiate from RCCApprox 1/3 of small (<3cm) hyperechoic
masses at US may represent RCC1
1 Radiology. 1993; 188:431-434.Downloaded from sar2013.conferencespot.org

ECHOGENIC RENAL FOCI
Nephrolithiasis Vascular calcificationsNephrocalcinosisGas forming infectionPapillary necrosisCystic disease
Downloaded from sar2013.conferencespot.org

NEPHROLITHIASIS
Gray-scale – sensitivity of 24-57% compared to CT1,2
Stones of sufficient size – echogenic and shadow Small stones (< 5 mm) – echogenic
Color Doppler – color comet-tail or “twinkle” artifact May increase sensitivity, but overestimates size Positive predictive value = 78-94%3,4
False negatives: Smooth surfaced stones (uric acid and calcium oxalate monohydrate stones) may not twinkle5
False positive – vascular calcification and refractive shadowing from renal sinus fat, non-calcified foci
1 Radiology 2002;222:109-13 2 J Clin Ultrasound 2007;235:256-613 Radiology 2011;259:911-6 4 J Ultrasound Med 2012;31:1619-1625 5 AJR 2003;180:215-22Downloaded from sar2013.conferencespot.org

MEDULLARY NEPHROCALCINOSIS
Calcification of the renal pyramids rather than the collecting systemDDx – medullary sponge kidney, renal
tubular acidosis and hyperparathyroidismGray-scale Early – echogenicity at tip or periphery of
medullary pyramids (Anderson-Carr kidney)Progresses to diffusely increased
echogenicity and shadowingSonographic findings (crystallization) predate
radiograph and CT findingsDownloaded from sar2013.conferencespot.org

CORTICAL NEPHROCALCINOSIS
Calcification of the renal cortexDDx – renal cortical necrosis, oxalosis,
Alport’s syndrome, transplant rejection, chronic glomerulonephritisGray-scaleEchogenic renal cortexLoss of corticomedullary differentiationPosterior acoustic shadowing
Downloaded from sar2013.conferencespot.org

PAPILLARY NECROSIS
Renal medulla and papillae are vulnerable to ischemic necrosis due to blood supply and hypertonic environment
Causes: Diabetes, analgesic abuse, sickle cell disease, obstructive uropathy, pyelonephritis, renal vein thrombosis, tuberculosis
Gray scale Hypoechoic papillae Cystic spaces in the medullary pyramids; may mimic
caliectasis Echogenic foci in the medullary pyramid represents
necrotic papillae Hydronephrosis is common
Color Doppler Sloughed papillae may cause a color comet-tail artifact May mimic renal calculi
Downloaded from sar2013.conferencespot.org

GAS
Emphysematous pyelonephritis – rare, life threatening necrotizing infectionEmphysematous pyelitis – gas within the
collecting system, more benign clinical courseGray-scaleEchogenic fociReverberation artifact (“dirty” shadowing)
in non-dependent positionRequires high index of suspicion
Downloaded from sar2013.conferencespot.org

LITHIUM TOXICITY
Chronic lithium use may lead to nephrogenic diabetes insipidus and chronic renal insufficiency Tubulointerstitial nephritis, with tubular microcysts
and interstitial fibrosis DDx includes polycystic renal disease and
glomerulocystic disease Ultrasound 1-2 mm microcysts may appear as echogenic foci
and may be misinterpreted as calcifications High frequency transducers, harmonic imaging,
cine clips allow identification of enhanced through transmission *
* J Ultrasound Med 2012; 31: 637-44Downloaded from sar2013.conferencespot.org

VASCULAR LESIONS
Arteriovenous fistulaPseudoaneursymNutcracker syndromeRenal arterial hypertensionRenal vein thrombosis
Downloaded from sar2013.conferencespot.org

PSEUDOANEURYSM
Etiology Penetrating trauma – stab and gunshot wounds Iatrogenic - percutaneous biopsy, nephrostomy
tube placement, surgery Tumors Vasculitis
Symptoms: Gross hematuria, flank pain, hypertension Treatment None – many heal spontaneously* Coil embolization
*Clin Nephrol 2002;58:398-404Downloaded from sar2013.conferencespot.org

PSEUDOANEURYSM
Gray scale – cystic spacesDuplex color DopplerSwirling pattern in the lumen (“yin-yang”) “to and fro” flow in the neck – flow in
during systole and out during diastolePseudoaneurysms are often associated with
arteriovenous fistulas *Low resistance high velocity pattern
* Ultrasound The Requisites, 2nd Ed, p.143Downloaded from sar2013.conferencespot.org

ARTERIOVENOUS FISTULA
Etiology Penetrating trauma – stab and gunshot wounds Iatrogenic Percutaneous biopsy Nephrostomy tube placement Surgery
May be asymptomatic, gross hematuria, urinary tract obstruction, renal insufficiency or hypertension Treatment None – 75% spontaneously close at 4 weeks* Coil embolization
*Clin Nephrol 2002;58:398-404Downloaded from sar2013.conferencespot.org

ARTERIOVENOUS FISTULA
Often no changes on gray scale unless accompanied by a pseudoaneurysmDuplex color Doppler Increased arterial peak systolic and
diastolic velocityDecreased resistanceArterialization of the draining veinSoft tissue vibration
Downloaded from sar2013.conferencespot.org

NUTCRACKER SYNDROME
Renal vein entrapment syndrome Compression of the left renal vein between the aorta
and SMA Elevated renal vein pressure Collateral vessels
Young, previously healthy patients Intermittent gross hematuria, +/- flank pain Ultrasound: Compression of the renal vein Elevated flow velocity using Duplex color Doppler *
3 mm Hg gradient at angiography is used to diagnose renal venous hypertension
• Radiology 1996; 198: 93-7• AJR 1999; 172: 39-43
Downloaded from sar2013.conferencespot.org





























