Embed Size (px)
Citation preview
Beyond the BundleImproving Ventilator Related Outcomes through Multidisciplinary Collaboration
Definitions
VAE—Ventilator associated event—global term for NHSN reporting criteria
VAC: Ventilator Associated Condition: Patient has baseline period of stability or improvement on the vent, defined by >2 calendar days of stable or decreasing daily minimum Fi02 or PEEP values, then has:
Increase in daily minimum Fi02 of > 20% or Increased in daily minimum PEEP of > 3 cm H20
IVAC: Infection-related Ventilator Associated Complication: on or after calendar day 3 of mechanical ventilation, and within 2 days of worsening oxygenation, patient meets two criteria:
Temp > 38° C or < 36° C OR WBC > 12,000 or < 4,000 cells/mm3 AND Administration of a NEW antimicrobial agent(s)
PVAP: Possible Ventilator Associated Pneumonia: one of three criterion are met in positive organism growth/histology

Ventilator Associated Events
Magill, CDC, 2015
Case Study
76 year old male admitted for respiratory failure, new spontaneous subdural hematoma (non-surgical), probable aspiration during event. History of COPD, aspiration pneumonia. Unable to protect airway, so intubated. Initial vent settings, Fi02 100%, PEEP 5, PRVC w TV 450. Agitated at times, sedation started.
Day 2: Pressors weaned off and able to wean Fi02 to 40%. More responsive, but RASS -3 with no sedation. Tolerated spontaneous breathing trial (SBT) for 2 hours before 02 sat dropped to mid 80’s, brief increase in Fi02 then able to wean back to 40%.
Day 3 and 4: Stable, but remained obtunded with no sedation, SBT tolerated for 45 minutes. Supportive Care/Palliative Care consult. Family wanting everything done.
Day 5: Did not tolerate SBT, with elevated respiratory rate, heart rate, low sats; Fi02 increased to 60%, PEEP of 8cm to keep sats 90-91. Unable to wean Fi02 or PEEP through that calendar day. CTA negative for PE, increased consolidation right base. WBC elevated from 12 to 18. BC, sputum culture done, new antibiotic initiated. (meets for IVAC)
Day 6: Fi02 65-70% with PEEP, continues to be poorly responsive. Family debating about trache and PEG versus Comfort Cares
Day 8: Now unresponsive. Family elects to compassionately extubate. Patient expires within 2 hours. No new growth on cultures.
Cost of Ventilator complications
• At least 800,000 patients receive mechanical ventilation in the U.S. each year, with 10-20% of these developing a VAP, a complication with an associated 35% mortality (CUSP 4-MVP)
• The average ICU cost for the ventilated patient is $2300 per day. After the 4th day, this cost rises to over $3900 per day.
• A 20% reduction in ventilator days alone could save $2 million per year. (CUSP 4-MVP)
• The cost of one VAP is estimated to be $14,000 -$29,000, with an estimated total cost in the United States from $0.8 to $1.5 billion annually (Magill, et al, 2014).
• The Hospital Engagement Network set a goal of reduction of all-cause harm by 40%, including VAE’s.
VAE/VAP at CHI Health St. Francis
Process improvements initiated in 2012-2013 had virtually eliminated VAP’s at CHI Health St. Francis.
With the Centers for Disease Control’s (CDC) early 2015 VAP definition clarification and the resultant reductions in VAP rates nationwide, the focus has shifted to VAE’s, a precursor event (CDC, 2016, CUSP 4-MVP).
The shift in focus on VAE’s has presented a challenge, especially with complex neuro and end of life patients.
St. Francis saw a sharp increase in VAE’s after this redefinition, prompting the need for further process improvement

CUSP 4 MVP Participation
• National collaborative quality improvement project funded through the Agency for Healthcare Research and Quality (AHRQ). Sponsored by Armstrong Institute
• The purpose of CUSP 4 MVP-VAP is to improve care for mechanically ventilated patients and reduce the rate of patient harm associated with mechanical ventilation. Goals include:
Reduce ICU inpatient mortality
Prevent short-term complications, such as ventilator-associated pneumonia and sepsis
Reduce long-term physical, cognitive and psychological harm to ICU survivors
Decrease the number of mechanical ventilation days and overall length of stay
Enhance teamwork and communication
• CUSP = Comprehensive Unit-based Strategy Program
• MVP=Mechanically ventilated patient
Critical to Success
• Successful multi-disciplinary collaboration, including consistent daily rounds
• Active Supportive/Palliative Care team to assist in Goal setting/End of Life discussions
• Effective collaboration with Infection Prevention
• Physician engagement, including the Critical Care Committee
• Consistent use and revisions to evidence based guidelines:
• RT Driven Ventilator Management protocol
• Ventilator Sedation, Sedation Vacation protocol
Daily Care MeasuresCUSP 4 MVP
Phase I Process Improvement
• Participation in the CUSP 4-MVP Project was approved by Critical Care Committee on 7/15/15, with the decision to focus on daily care measures as the best opportunity for positive outcomes.• elevate HOB to > 30 degrees,
• minimize sedation level,
• use spontaneous awakening trial (SAT) with validated sedation scale daily,
• assess readiness to wean daily with spontaneous breathing trial (SBT),
• assess and address delirium,
• intentional use of subglottic suctioning.
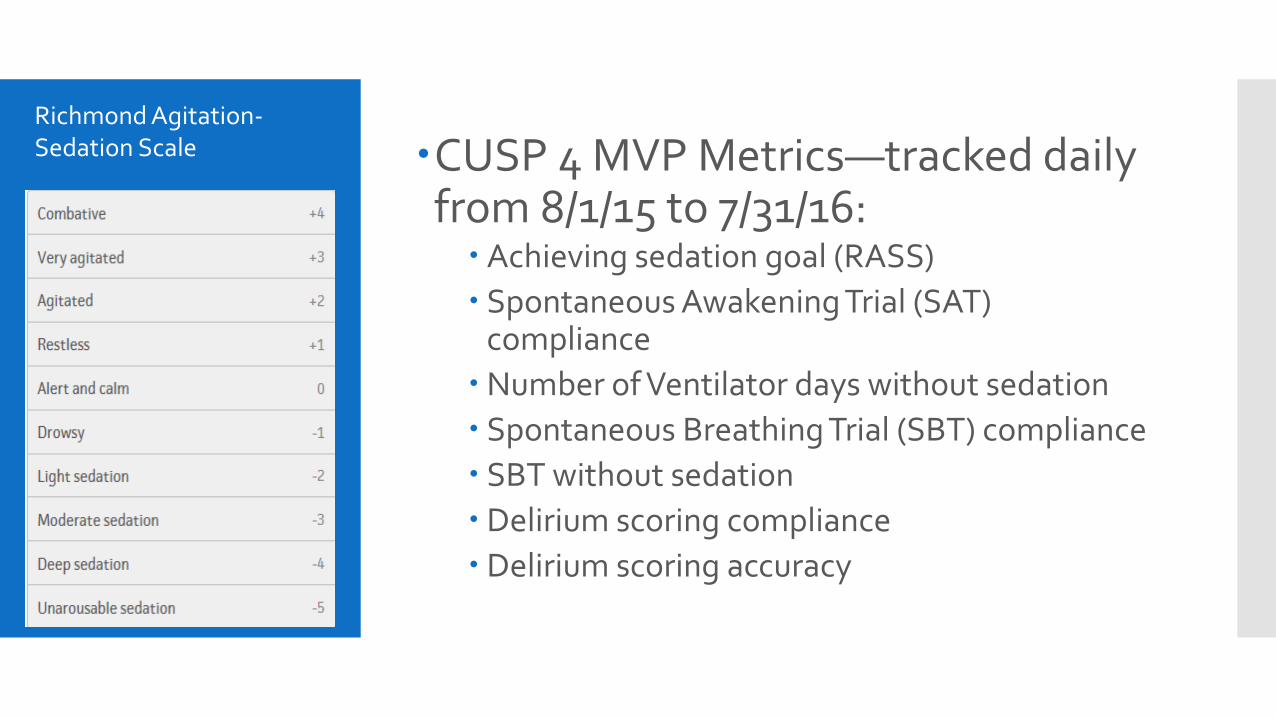
CUSP 4 MVP Metrics—tracked daily from 8/1/15 to 7/31/16:
Achieving sedation goal (RASS)
Spontaneous Awakening Trial (SAT) compliance
Number of Ventilator days without sedation
Spontaneous Breathing Trial (SBT) compliance
SBT without sedation
Delirium scoring compliance
Delirium scoring accuracy
Richmond Agitation-Sedation Scale
Delirium scoring using CAM-ICU
Use of Delirium Scoring and Order set initiated early in 2015, but not utilized effectively
Confusion Assessment Method (CAM-ICU) Assessment for Delirium, using RASS score:
If RASS is -4 or -5, then Stop and Reassess patient at later time. If RASS is above - 4 (-3 through +4) then Proceed to Next step
Does patient had acute change or fluctuating course of metal status?
Test for inattention by having the squeeze hand when nurse states “A” within a list of letters
What is current RASS—is there an altered level of consciousness
Is there disorganized thinking? Questions such as—can a stone float?
https://medschool.vanderbilt.edu/trauma-and-scc/files/trauma-and-scc/public_files/Protocols/RASS%20and%20CAM-ICU.pdf
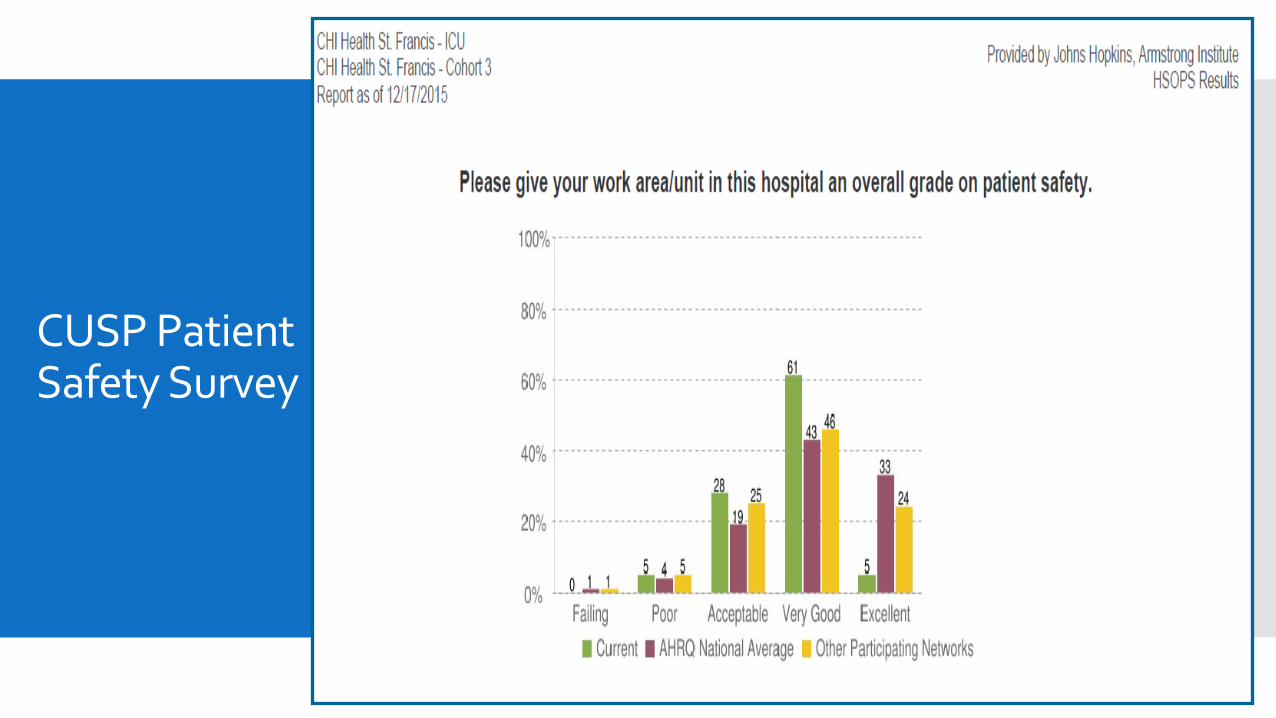
CUSP Patient Safety Survey
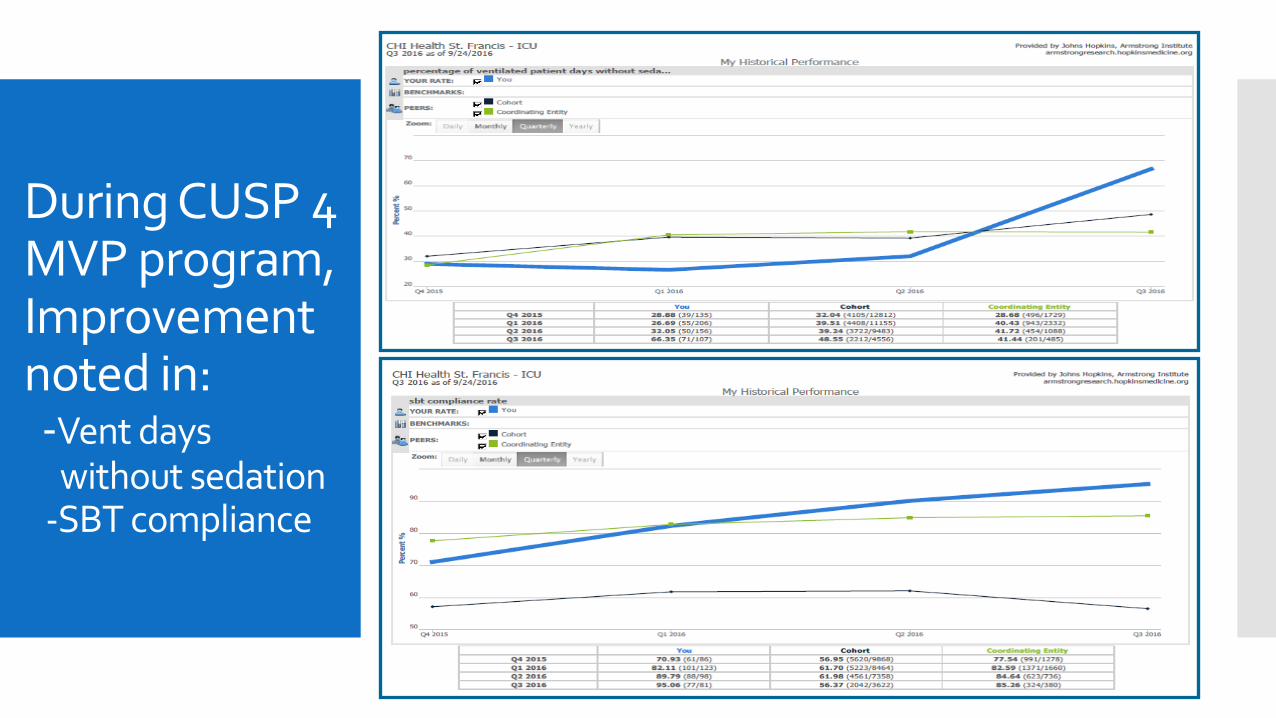
During CUSP 4 MVP program, Improvement noted in:-Vent days
without sedation-SBT compliance
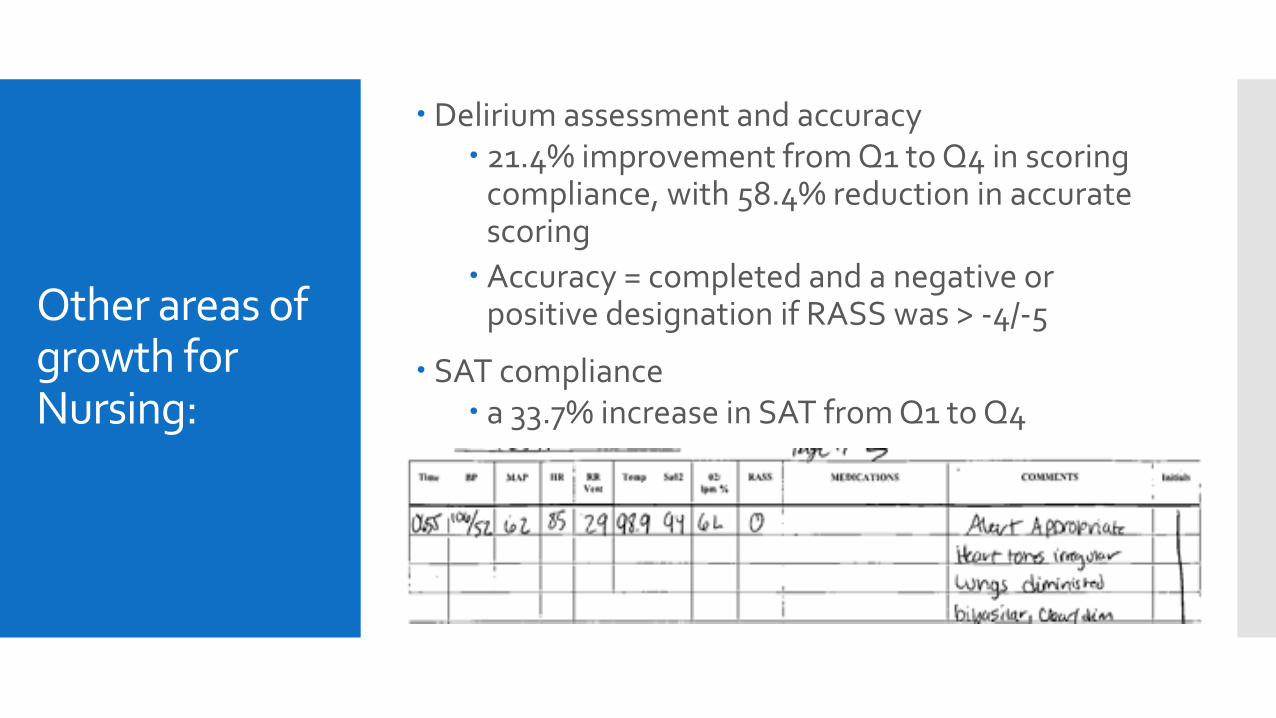
Other areas of growth for Nursing:
Delirium assessment and accuracy 21.4% improvement from Q1 to Q4 in scoring
compliance, with 58.4% reduction in accurate scoring
Accuracy = completed and a negative or positive designation if RASS was > -4/-5
SAT compliance a 33.7% increase in SAT from Q1 to Q4
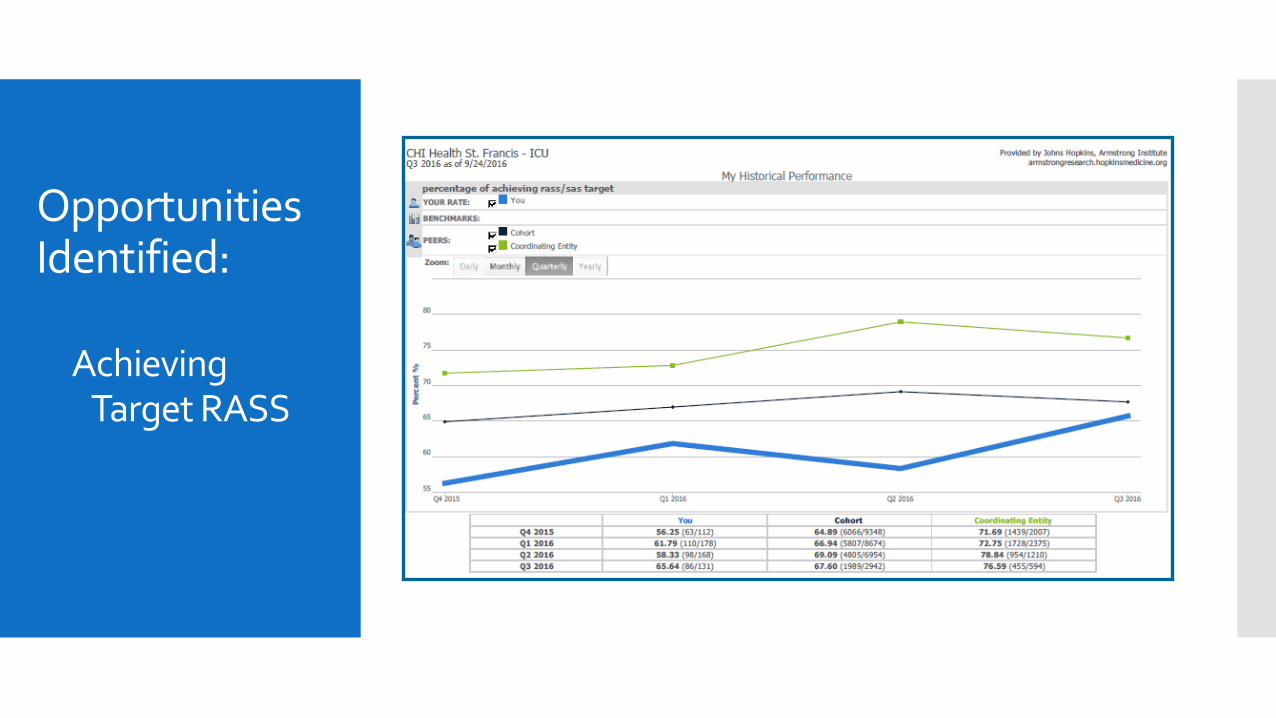
Opportunities Identified:
Achieving Target RASS
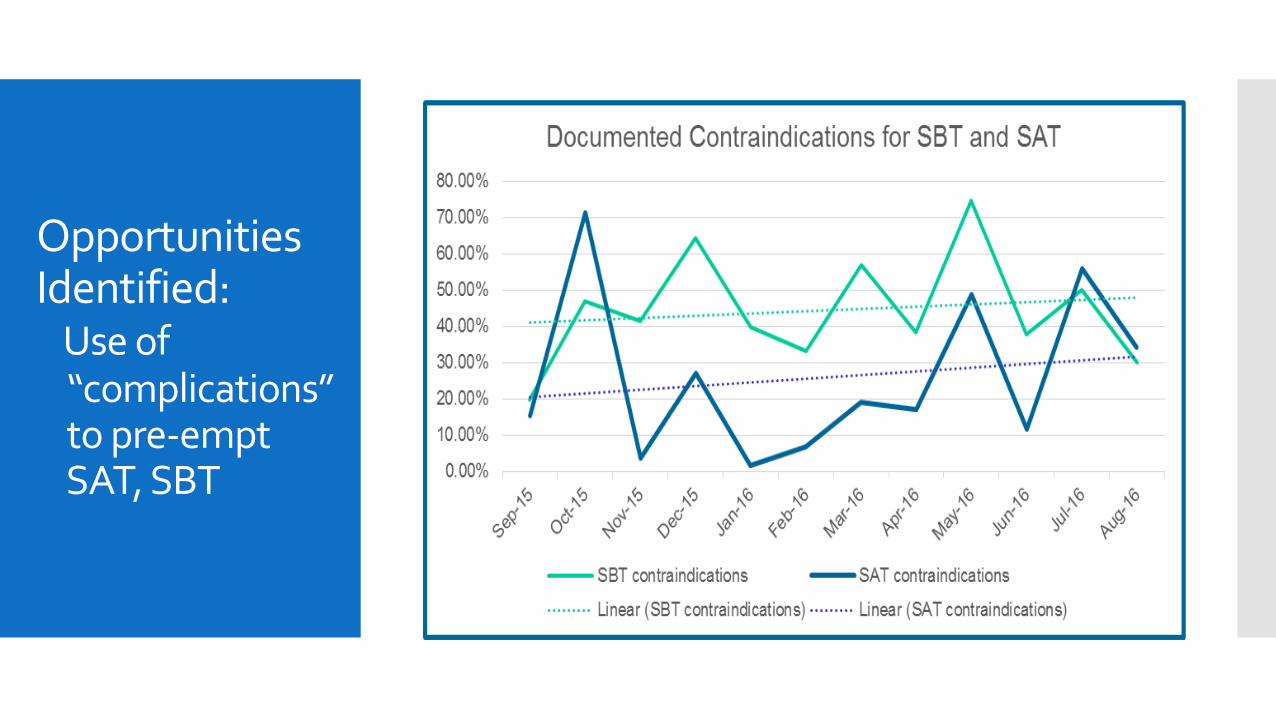
Opportunities Identified:
Use of “complications” to pre-empt SAT, SBT
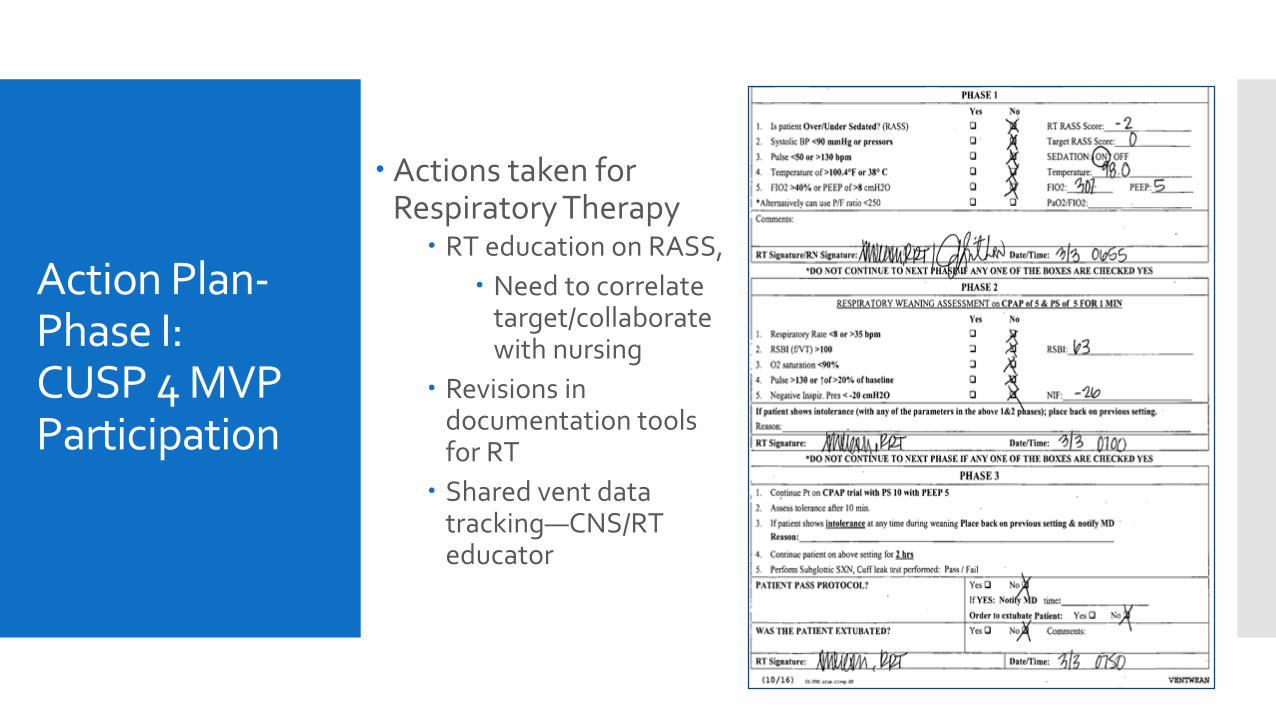
Action Plan-Phase I:CUSP 4 MVP Participation
Actions taken for Respiratory Therapy
RT education on RASS,
Need to correlate target/collaborate with nursing
Revisions in documentation tools for RT
Shared vent data tracking—CNS/RT educator
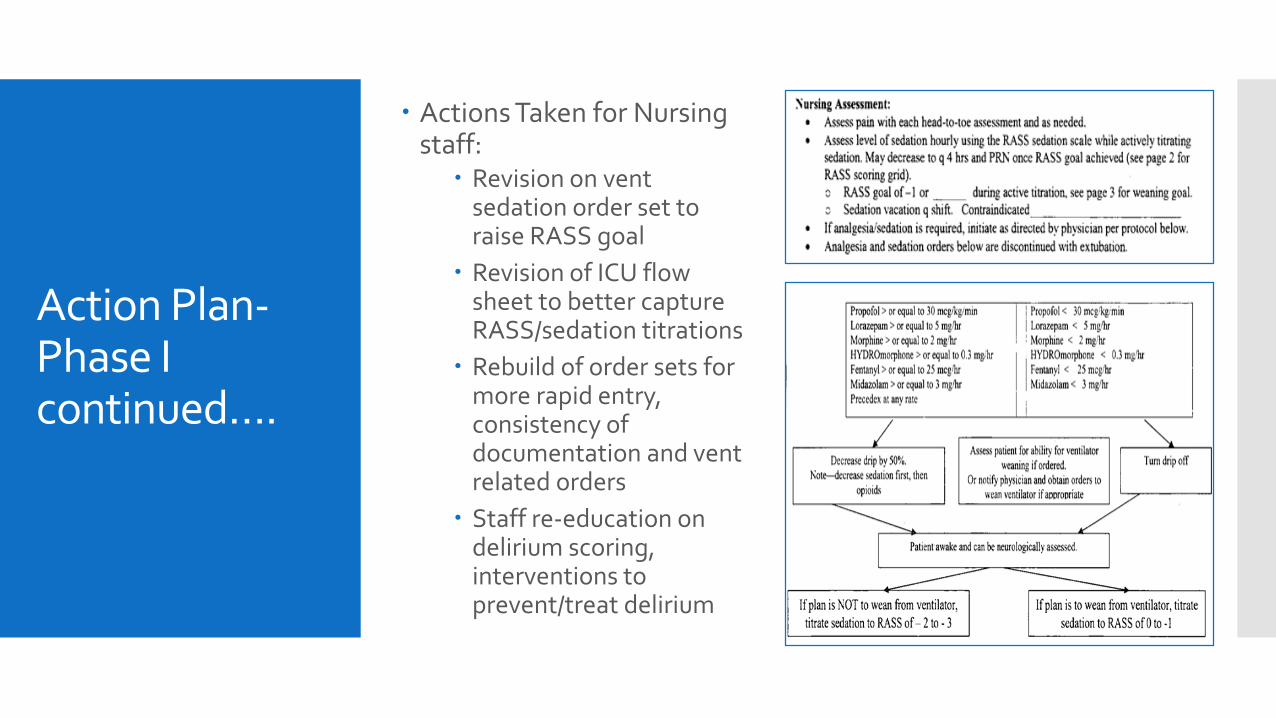
Action Plan-Phase I continued….
Actions Taken for Nursing staff:
Revision on vent sedation order set to raise RASS goal
Revision of ICU flow sheet to better capture RASS/sedation titrations
Rebuild of order sets for more rapid entry, consistency of documentation and vent related orders
Staff re-education on delirium scoring, interventions to prevent/treat delirium
Challenges
Mixed acuity unit
High census
Very complex patients with extended ventilator use
Locum pulmonologists
Staff turn over
Habits formed—need to refocus/reinforce Continued practice of using “complications” such as
pressors, temp, sedation to rule out weaning for entire calendar day, instead of forming a plan to address the complication and try later
Multiple competing process changes
Case Study
Patient admitted after found unresponsive on floor by family. History alcohol abuse. Extensive subdural hematoma. To ICU post-crani. Vent Fi02 100%, PEEP of 5. RT able to wean vent as indicated. On propofol for sedation. Left sided pneumonia
Day 2—Fi02 30%, PEEP of 5. Keppra added for seizures, agitated at times, does not follow commands,
Day 3—Fi02 30%, titrated briefly to 50%, PEEP 5, pulmonology coverage change
Day 4—Fi02 30%, change to Pressure control, PEEP increased to 8. Chest x-ray stable, WBC stable at 5.2
Day 5 (Saturday)—Fi02 30%, PEEP 8
Day 6 (Sunday)—Fi02 30%, PEEP down to 6 later in day
Day 7—Fi02 30%, PEEP 4-6 during day.
ICU notified of VAC status based on increase in PEEP over weekend
Day 8—stable vent settings
Day 9—extubated, patient survived to discharge
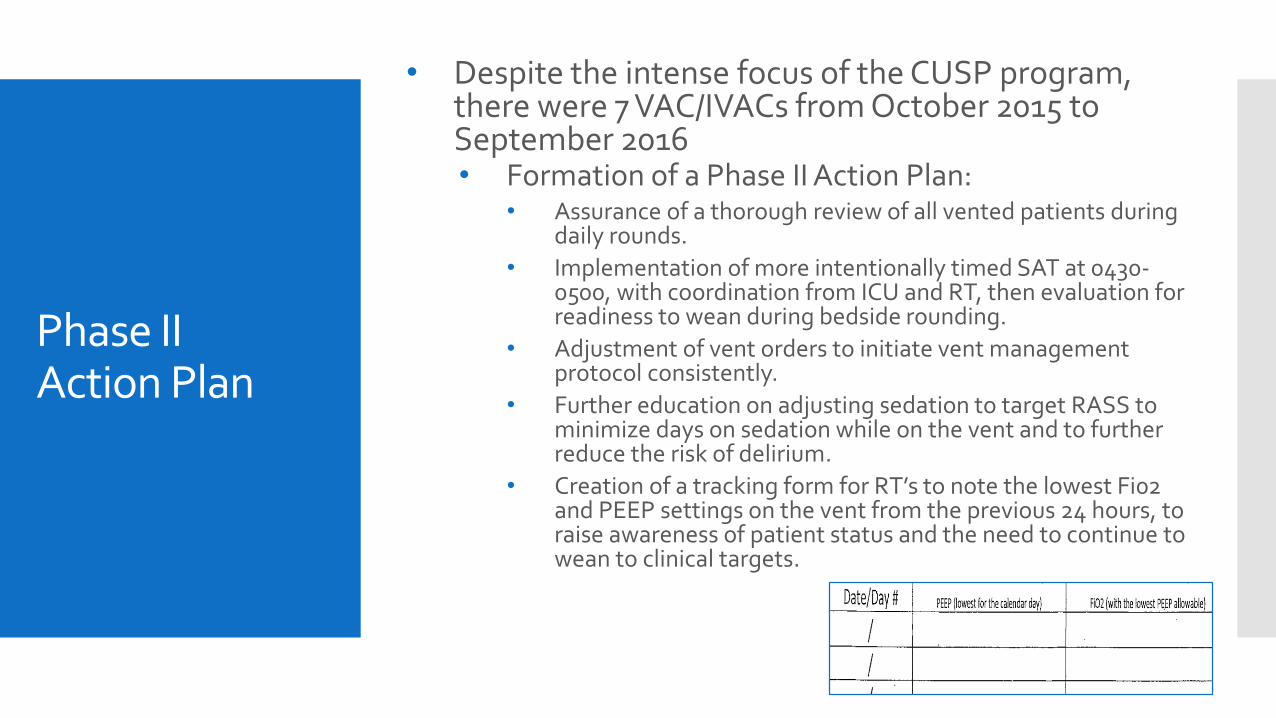
Phase II Action Plan
• Despite the intense focus of the CUSP program, there were 7 VAC/IVACs from October 2015 to September 2016• Formation of a Phase II Action Plan:
• Assurance of a thorough review of all vented patients during daily rounds.
• Implementation of more intentionally timed SAT at 0430-0500, with coordination from ICU and RT, then evaluation for readiness to wean during bedside rounding.
• Adjustment of vent orders to initiate vent management protocol consistently.
• Further education on adjusting sedation to target RASS to minimize days on sedation while on the vent and to further reduce the risk of delirium.
• Creation of a tracking form for RT’s to note the lowest Fi02 and PEEP settings on the vent from the previous 24 hours, to raise awareness of patient status and the need to continue to wean to clinical targets.
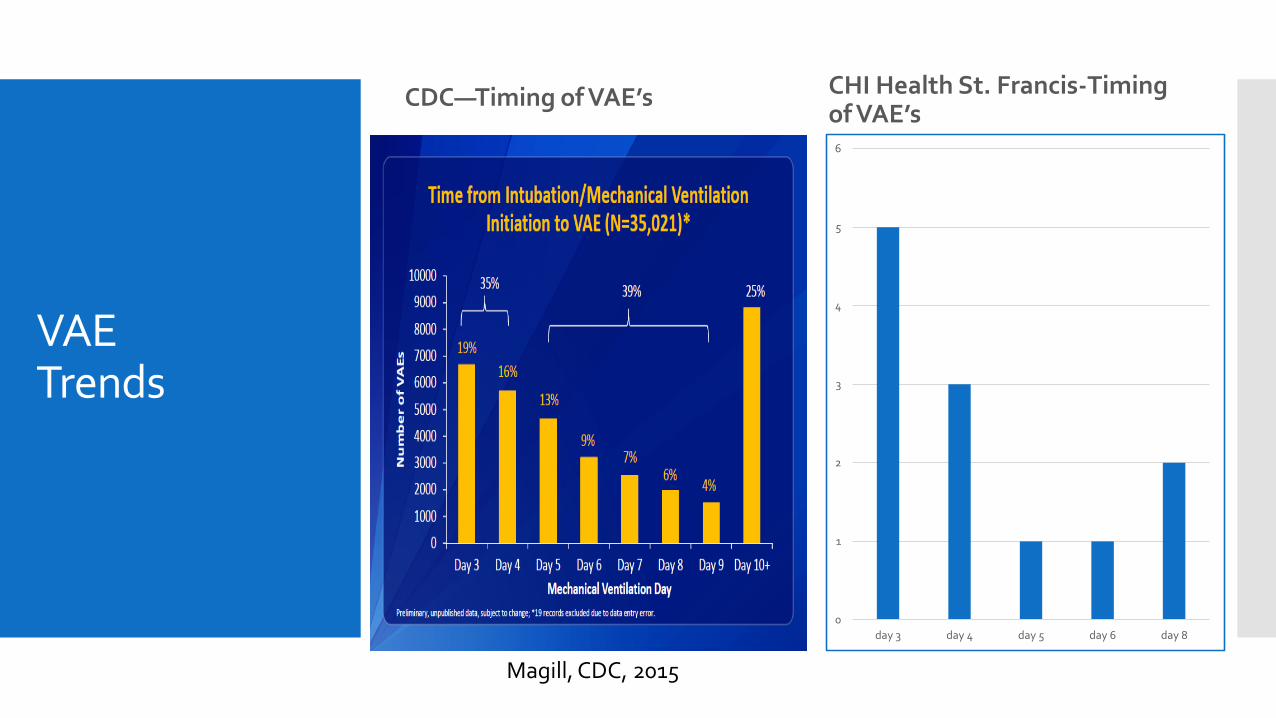
VAE Trends
CDC—Timing of VAE’s CHI Health St. Francis-Timing of VAE’s
Magill, CDC, 2015
0
1
2
3
4
5
6
day 3 day 4 day 5 day 6 day 8
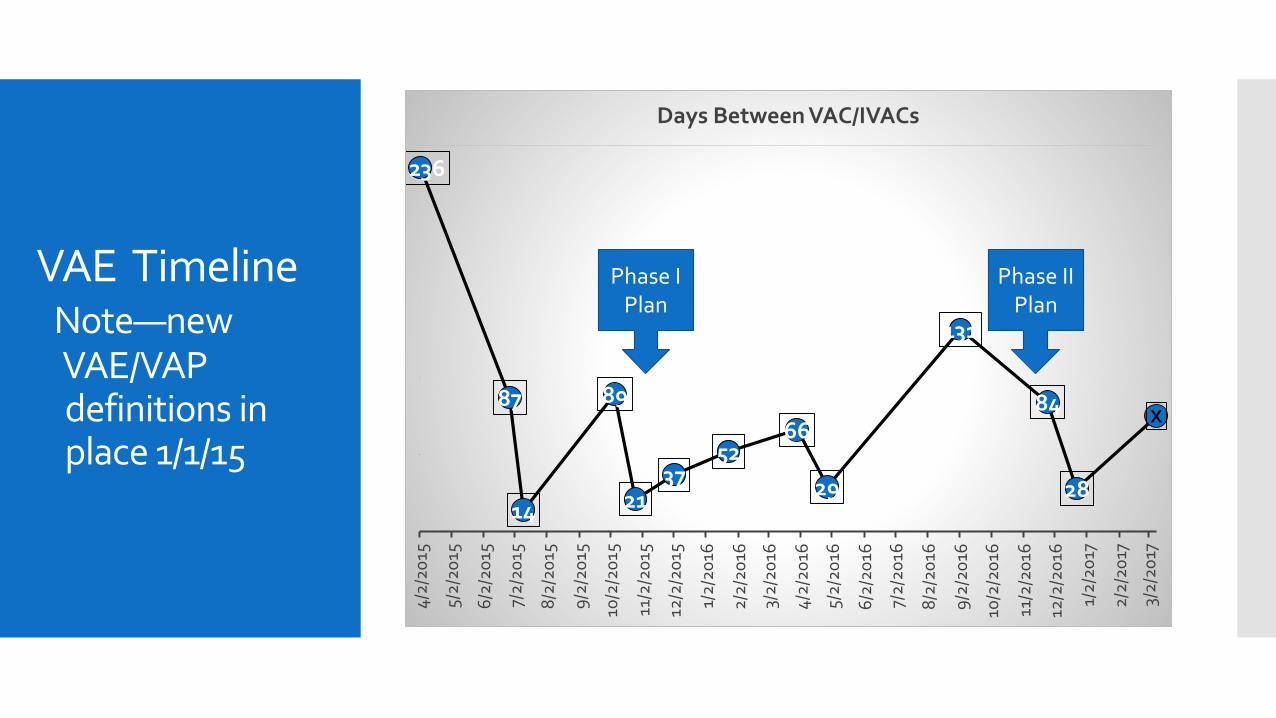
VAE TimelineNote—new VAE/VAP definitions in place 1/1/15
236
87
14
89
2137
5266
29
131
84
28
X4
/2/2
015
5/2
/20
15
6/2
/20
15
7/2
/20
15
8/2
/20
15
9/2
/20
15
10/2
/20
15
11/2
/20
15
12/2
/20
15
1/2
/20
16
2/2
/20
16
3/2
/20
16
4/2
/20
16
5/2
/20
16
6/2
/20
16
7/2
/20
16
8/2
/20
16
9/2
/20
16
10/2
/20
16
11/2
/20
16
12/2
/20
16
1/2
/20
17
2/2
/20
17
3/2
/20
17
Days Between VAC/IVACs
Phase II Plan
Phase I Plan
Plan-Study-Do-Act Phase IIPhase IIb
Examining processes during daily rounding and data trends, it was evident that some aspects were not occurring as designed:
Lack of RN signatures on RT weaning sheet to indicate daily plan collaboration
Lack of agreement from start of day RASS target and actual RASS score between RT and Nursing
Continued use of “complications” to pre-empt SBT and SAT
Inconsistent use of same RASS goal for physicians, nursing and RT
Phase II-b Action Plan: Case reviews with Nursing and RT when gaps noted
RT re-education: Reviewed RASS goals, documentation expectations with RT, role modeling of RT/nursing planning conversation
Nursing re-education: consistent use of order sets, need for target RASS, assure collaboration with RT
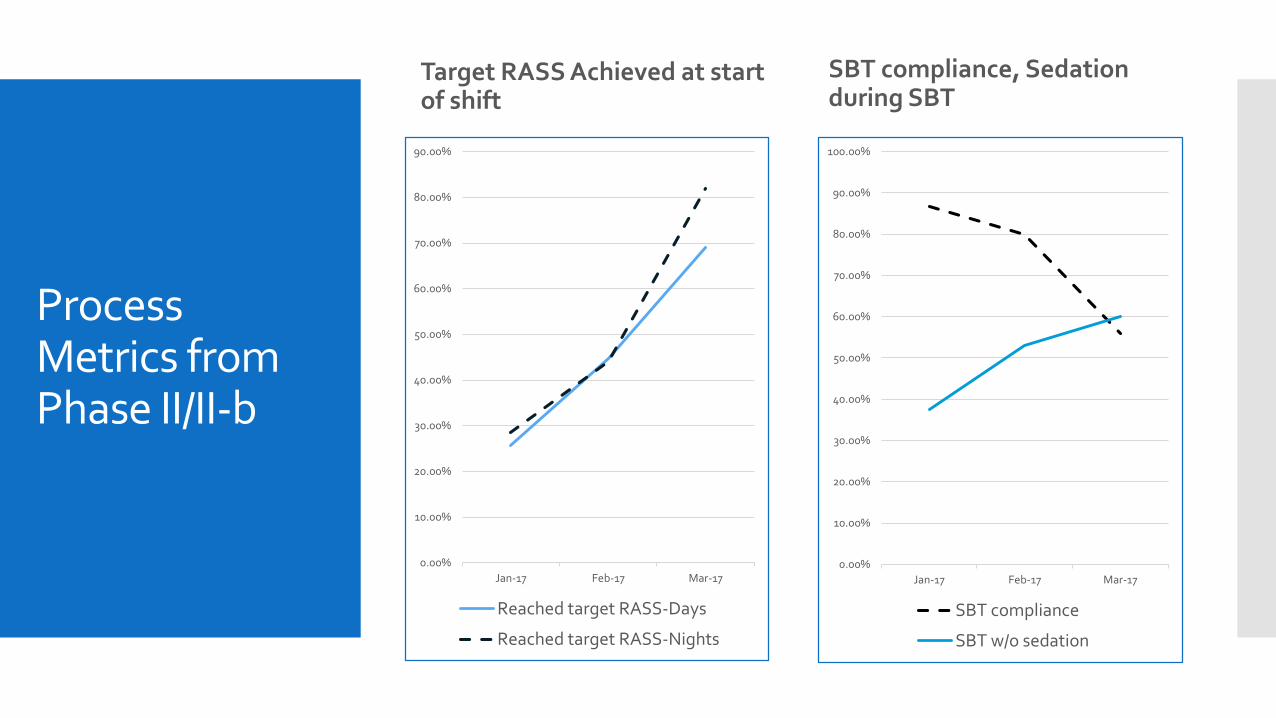
Process Metrics from Phase II/II-b
Target RASS Achieved at start of shift
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
Jan-17 Feb-17 Mar-17
Reached target RASS-Days
Reached target RASS-Nights
SBT compliance, Sedation during SBT
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Jan-17 Feb-17 Mar-17
SBT compliance
SBT w/o sedation
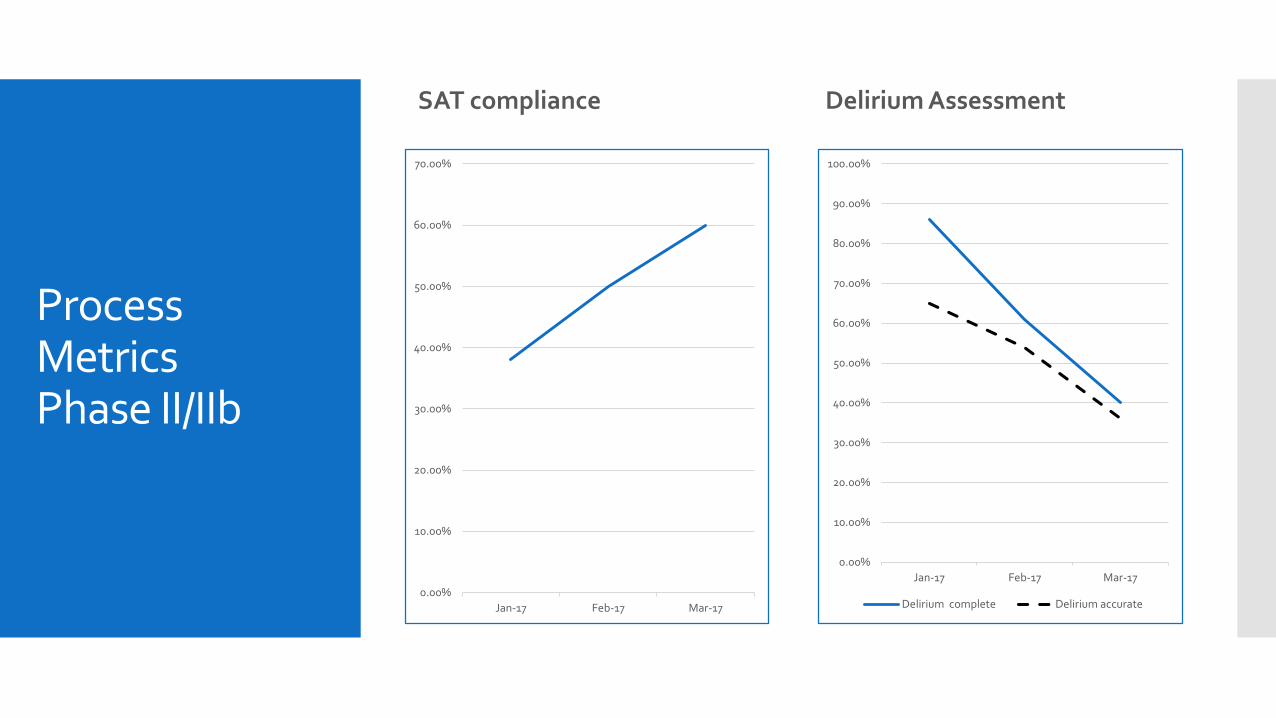
Process Metrics Phase II/IIb
SAT compliance
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Jan-17 Feb-17 Mar-17
Delirium Assessment
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Jan-17 Feb-17 Mar-17
Delirium complete Delirium accurate
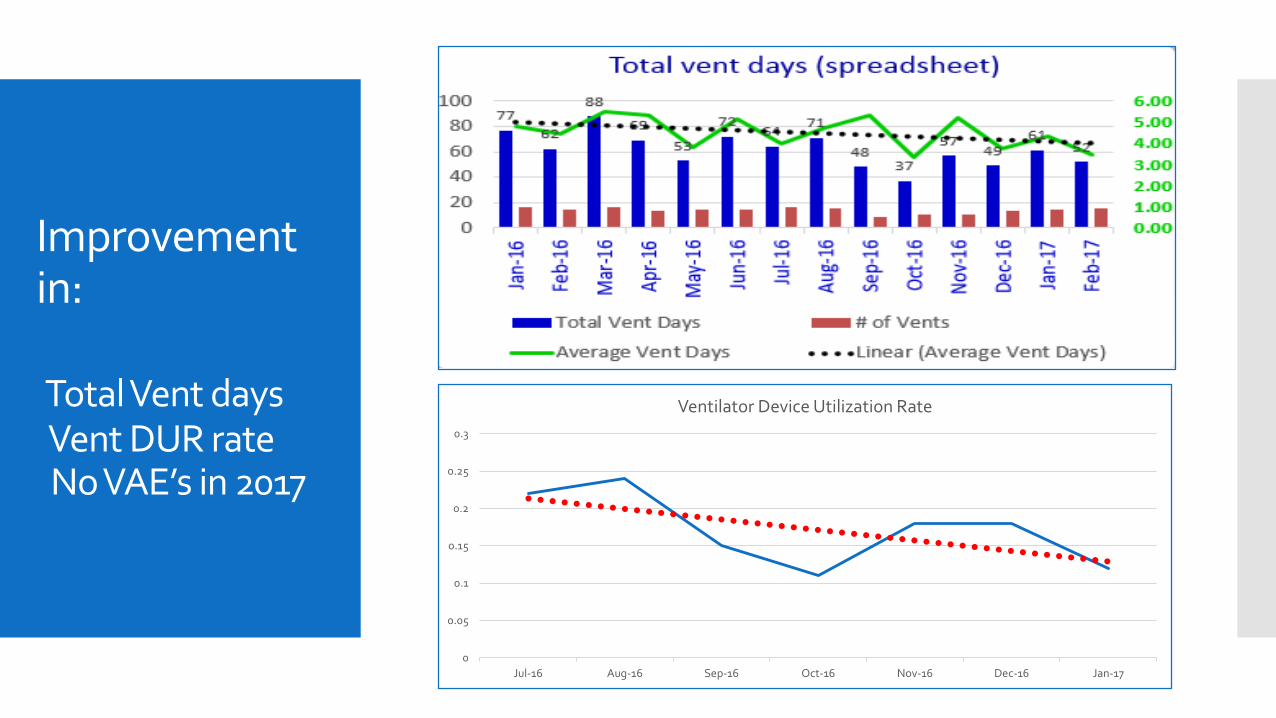
Improvement in:
Total Vent days Vent DUR rateNo VAE’s in 2017
0
0.05
0.1
0.15
0.2
0.25
0.3
Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
Ventilator Device Utilization Rate
Summary
Involvement in national collaborative CUSP 4 MVP instrumental in ongoing process improvements for CHI Health St. Francis
Process Improvement requires consistent multi-disciplinary collaboration
Daily clinical targets must be formed to dictate plan of care
Practice guided by evidence based practices/order sets
Development of effective decision making tools/documentation resources
Effective process improvement requires: Clear process and outcome metrics
Effective surveillance to determine needed course adjustments
A team dedicated to improve patient outcomes
Critical Care Committee as of 2015 at start of CUSP Cohort 3: Paula Ryan, RN and Carrie Morse, RT co-chairs
Dr. Hatoum, Pulmonology; Dr. Anderson, Neuro-surgery;Abby Gallagher, Pulmonology NP;
Barb Nickel APRN-CNS, Ashley Hermesch, Director Critical Care, ICU RN’s: Andrea Brouillette, James Disney, Katie Kingsley, Chris Goplin, RT, Scott Erikson, PT
References:
• Centers for Disease Control (CDC), January 2016, Pneumonia (Ventilator-associated [VAP] and non-ventilator-associated pneumonia [PNEU] event. Retrieved on 8/6/16 from: http://www.cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf
• Centers for Disease Control (CDC), (2017), Device Associated Module: VAE. Retrieved on 3/17/17 from: https://www.cdc.gov/nhsn/PDFs/pscManual/10-VAE-FINAL.pdf
• Johns Hopkins CUSP 4-MVP program: Improving Care for Mechanically Ventilated Patients. https://armstrongresearch.hopkinsmedicine.org/Default.aspx
• Magill SS, Edwards JR, Bamberg W, et al. (2014), Multistate Point-Prevalence Survey of Health Care–Associated Infections. N Engl J Med;370:1198-208.
• Ventilator-Associated Event Surveillance: CDC Updates, Shelley S. Magill, MD, PhD, July 16, 2015, Centers for Disease Control. Retrieved on 3/17/17 from: http://c.ymcdn.com/sites/www.cste.org/resource/dynamic/forums/20150727_150946_14454.pdf
• http://www.icudelirium.org/docs/WakeUpAndBreathe.pdf, Vanderbilt