Embed Size (px)
Citation preview

Beyond the Red Leg: Cellulitis and Its Mimickers
Daniela Kroshinsky, M.D. M.P.H.
Associate Professor of Dermatology
Director of Inpatient Dermatology
Director of Pediatric Dermatology

Disclosures
Neither I nor my spouse/partner has a relevant financial relationship with a commercial interest
to disclose

Overview
• Cellulitis & Pseudocellulitis: Background
• Diagnosis: Typical vs. Variant vs. Pseudocellulitis
• Pseudocellulitis

Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul 19;316(3):325-37.

Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul 19;316(3):325-37.

Cellulitis
• Deep skin and subcutaneous fat infection
• Poorly-demarcated erythema, warmth, tenderness,
edema
• Rubor, calor, dolor, tumor: inflammation
• 2.2% of all general practitioner office visits
• US Outpatient + ED 2006: 14.5 million cases, $3.7 billion
• 4.6 million cases in 1997
The DRG Handbook: Comparative Clinical and Financial Benchmarks. Evanston, IL: Solucient; 2006.Cox NH, Colver GB, Paterson WD. Management and morbidity of cellulitis of the leg. J R Soc Med. 1998;91(12):634-637.Arakaki RY, Strazzula L, Woo E, Kroshinsky D. The impact of dermatology consultation on diagnostic accuracy and antibiotic use among patients with suspected cellulitis seen at outpatient internal medicine offices: A randomized clinical trial. JAMA Dermatol. 2014. David CV, Chira S, Eells SJ, et al. Diagnostic accuracy in patients admitted to hospitals with cellulitis. Dermatol Online J. 2011;17(3).

Cellulitis
Healthcare Cost and Utilization Project (HCUP). Nationwide Inpatient Sample (NIS) Most Frequent Conditions in U.S. Hospitals, 2011.
Christensen KLY, et al. Infectious disease hospitalizations in the United States. Clin Infect Dis Off Publ Infect Dis Soc Am. 2009;49(7):1025-1035.
Hersh AL, Chambers HF, Maselli JH, Gonzales R. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch Intern Med. 2008;168(14):1585-1591.
Goettsch WG, Bouwes Bavinck JN, Herings RMC. Burden of illness of bacterial cellulitis and erysipelas of the leg in the Netherlands. J Eur Acad Dermatol Venereol JEADV. 2006;20(7):834-839.
McNamara DR, Tleyjeh IM, Berbari EF, et al. Incidence of lower-extremity cellulitis: a population-based study in Olmsted county, Minnesota. Mayo Clin Proc. 2007;82(7):817-821.
• 10% of infectious disease-related US hospitalizations ‘98-’06
• Average length of stay 7-10 days, 15 days if recurrent
cellulitis
• 400,000 days/ year in the English National Health Service
• 73% increased rate of hospitalization in US from 1997-2011
– Five-fold increased hospitalization from 54yo to >=85yo
– Over 650,000 admissions

Chart1
Page 1
HMG FY11 Readmissions
0
5
10
15
20
25
30
35
40
45
Cellulitis &
Ras
h
Pulm
onar
y Oth
er
Eso
phag
itis
GI O
ther
Car
diac
Oth
er
Mus
culosk
elet
al
Vas
cula
r/Blo
od UTI
CHF
Oth
er
Pne
umon
ia
Neu
roPai
n
End
ocrin
e
Ren
al ID IBS
Pan
crea
s
Psy
cho-
social
Live
rAM
I
Diagnosis Group
# R
ea
dm
iss
ion
s
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
% T
ota
l R
ead
mis
sio
ns
FY11 Qty
Cum %
Table courtesy of D. Mari
Cellulitis at MGH: #15 Admission, #1 Readmission

Pseudocellulitis: The Problems
• Preliminary data: 7% of 500 inpatient consults over nine months for unresponsive cellulitis
– 85% = pseudocellulitis
• Very little agreement on the ‘gold standard’
– No laboratory criteria exist to confirm dx
• Dermatologist expertise facilitates the identification and proper treatment of actual mimicking diagnoses, reduced antibiotic use
Arakaki RY, Strazzula L, Woo E, Kroshinsky D. The impact of dermatology consultation on diagnostic accuracy and antibiotic use among patients with suspected cellulitis seen at outpatient internal medicine offices: A randomized clinical trial. JAMA Dermatol. 2014. David CV, Chira S, Eells SJ, et al. Diagnostic accuracy in patients admitted to hospitals with cellulitis. Dermatol Online J. 2011;17(3).

Cellulitis vs Pseudocellulitis
• Up to 33% represent ‘pseudocellulitis’, or other mimicking inflammatory skin conditions
• Diagnostic criteria are unclearly defined, variably applied
• Poorly-demarcated erythema, warmth, tenderness, edema
• Rubor, calor, dolor, tumor: inflammation (Celsus, 1st century AD)
• Per year, cellulitis misdiagnosis, hospitalization, and antibiosis leads to an estimated:
• 50,000 unnecessary hospitalizations
• $195 million in avoidable health care spending
• 9,000 nosocomial infections, 1,000 C. difficile infections
• Dermatology or Infectious Diseases consultation proposed as clinical gold standard
David CV et al. Diagnostic accuracy in patients admitted to hospitals with cellulitis. Dermatol Online J. 2011 Mar 15;17(3):1.Weng QY, Raff AB, Cohen JM, Gunasekera N, Okhovat JP, Vedak P, Joyce C, Kroshinsky D, Mostaghimi A. Costs and Consequences Associated With
Misdiagnosed Lower Extremity Cellulitis. JAMA Dermatol. 2016 Nov 2.

0
10
20
30
40
50
60
70
80
1+ kn
own
risk f
acto
r
H/O
skin
dise
ase
Active
canc
er
Diabe
tes
High-
Dose Im
mun
osup
p.
H/O
Tra
nsplan
t
Tinea
ped
is
ESRD
Known tra
uma
Chr
onic
Lym
phed
ema
Neu
trope
nia
AIDS
Ony
chom
ycos
is
Low-d
ose
Imm
unos
upp.
Risk Factors
% A
ffecte
d P
ati
en
ts
Cellulitis
Pseudocellulitis
Associated Risk Factors
P>.05
Strazzula L et al. Inpatient dermatology consultation aids diagnosis of cellulitis among hospitalized patients: A multi-institutional analysis. J AmAcadDermatol. 2015 Jul;73(1):70-5

Local Risk Factors Are More Significant in the Development of Leg Cellulitis Than Systemic Risk Factors
• A systematic review and meta-analysis over 70y
• Local significant risk factors: prior cellulitis, prior leg surgery, a ‘site of bacterial entry’ from wound, ulceration, excoriating skin disease or toe-web disease, chronic leg edema
• Obesity was the only potentially significant global health factor
• Evaluation and management of predisposing factors via regular follow-up visits may minimize risk
Quirke M et al. Risk factors for nonpurulent leg cellulitis: a systematic review and meta-analysis. Bjd. Literature review 19;45-7/15.

Multidisciplinary Approach to Cellulitis at MGH
• Dermatology consultation for patients presenting for presumed
cellulitis within 24 hours of IV antibiotic initiation
• 31% misdiagnosis rate
• Decrease in IV antibiotic use (<4 days: 86.3 versus 72.5; p=0.04)
as well as total duration of antibiotic use
• Decrease in hospital stay (<4 days: 76.1% versus 64.4%; p=0.14)
• Improvement at 2 week assessment (89.3% versus 68.3%
p<0.01) with no complications or increased risk of readmission
Ko LN, Garza-Mayers AC, St John J, Strazzula L, Vedak P, Shah R, Dobry AS, Rao SR, Milne LW, Parry BA, Kroshinsky D. Effect of
Demratology Consultation on Outcomes for Patients with Presumed Cellulitis. JAMA Dermatol. 2018 Feb 16.

Levell et al. Severe lower limb cellulitis is best diagnosed by dermatologists
and managed with shared care between primary and secondary care.
Br J Dermatol. 2011 Jun;164(6):1326-8.
• 210/ 635 referrals for lower limb cellulitis (33%) had other diagnoses which did not require admission
• 96% true cellulitis pts managed entirely as outpatients, many at home
• 28% patients with cellulitis had an underlying skin disease identified and treated → reduced the risk of recurrent cellulitis, leg ulceration, and lymphedema
• 18 /635 patients referred with lower limb cellulitis required hospital admission for conventional treatment (3%)

Microbiology: Common Pathogens
• Adults:
- Streptococcus pyogenes, Staphylococcus aureus
- MSSA>>>MRSA, unless traumatic
• Children:
• Staphylococcus aureus
– Previously Haemophilus influenza

Microbiology: Immunosuppression
• Mild/Moderate: DM, ESRD, Cirrhosis, PDN<20mg
– Staphylococci, streptococci
– Gram Negative Rods (GNR)
• Severe: neutropenic, PDN >20mg, other
immunosuppressives, AIDS
– Staphylococci, streptococci, GNR
– Atypical mycobacteria, deep fungal, nosocomials
Adapted from Bolognia Dermatology Fig 73.7

Multidisciplinary Approach to Cellulitis at MGH: Antibiotic Stewardship
• Mean number of antibiotics used: 2.8 (SD 1.3)
• 57.7% of all patients given longer than IDSA recommended
maximum antibiotic courses
• 68% of control patients given >=10days of antibiotics vs.
49% of intervention patients (p<0.01)
– Specialist recommendations often ignored; antibiotics
‘just in case’
• 20% of patients at MGH are on vancomycin
18Ko LN, Garza-Mayers AC, St John J, Strazzula L, Vedak P, Shah R, Dobry AS, Rao SR, Milne LW, Parry BA, Kroshinsky D. Effect of
Demratology Consultation on Outcomes for Patients with Presumed Cellulitis. JAMA Dermatol. 2018 Feb 16.

Vancomycin in the Emergency Department
19
J Emerg Med. 2015 Jul; 49(1): 50–57.

Antibiotic Stewardship: Treatment Algorithm for Nonpurulent Cellulitis
Adapted from: Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul 19;316(3):325-37.
(Add clindamycin if concern for necrotizing fasciitis)
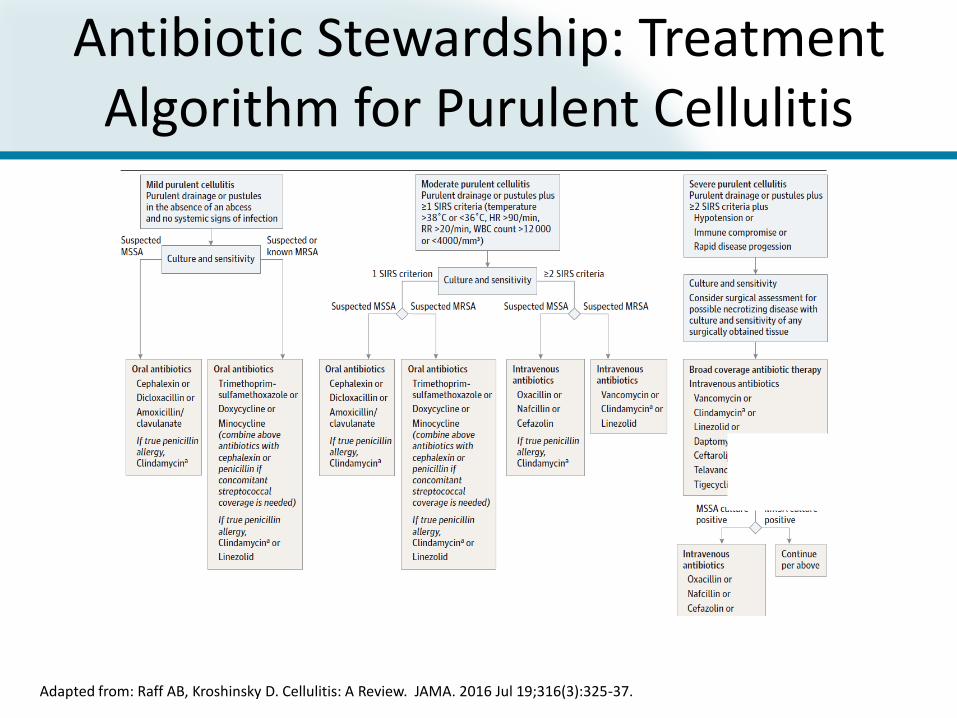
Antibiotic Stewardship: Treatment Algorithm for Purulent Cellulitis
Adapted from: Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul 19;316(3):325-37.

22
TMP/SMX: 2 DS tabs BID for patients >100kg, immunosuppression, trauma-induced SSTI
Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul 19;316(3):325-37.
Outpatient Prescriptions
• Multicenter, double-blind, randomized superiority trial in 5 US EDs
• 500 cellulitis outpatients > 12 yo with no wound, purulent drainage, or abscess (confirmed by bedside ultrasound)
• Randomized to two treatment arms: – Cephalexin, 500 mg 4 times daily, plus SMX-TMP, 320 mg/1600 mg
twice daily, for 7 days or
– Cephalexin plus placebo for 7 days
• Clinical cure in 83.5% of cephalexin plus SMX-TMP group vs 85.5% in the cephalexin group (95% CI, −9.7% to 5.7%; P = 0.50)
Moran GJ, et al. Effect of Cephalexin Plus Trimethoprim-Sulfamethoxazole vs Cephalexin Alone on Clinical Cure of Uncomplicated Cellulitis: A Randomized Clinical Trial. JAMA 2017;317(20):2088-96.

Predisposing Factors to Cellulitis
• Trauma:
– Piercings
– IVDA/‘popping’
– Bites
– Self-induced
• Tinea pedis/ onychomycosis
• Uncontrolled edema
Bjornsdottir S et al. Risk factors for acute cellulitis of the lower limb; a prospective case-control study. Clin Infect Dis 2005; 41: 1416-1422.
Roujeau JC et al. Chronic dermatomycoses of the foot as risk factors for acute bacterial cellulitis of the leg: a case-control study. Dermatology
2004; 209; 301-307.





Chronic Ulcers & Infection
• Diabetic, stasis, decubitus
• Culture usually
– Polymicrobial
– Not involved in cellulitis
– Unnecessarily broad
coverage
-Lee PC, Turnidge J, McDonald PJ. Fine-needle aspiration biopsy in diagnosis of soft tissue infections. J Clin Microbiol. 1985;22(1):80-83.-Drinka P, Bonham P, Crnich CJ. Swab culture of purulent skin infection to detect infection or colonization with antibiotic-resistant bacteria. J Am Med Dir Assoc. 2012;13(1):75-79.

Chronic Ulcers & Infection
• Signs of infection:
– New onset pain
– Increased erythema
• Usually multiorganism
– Anaerobes, Gram-negative aerobes

Predisposing Factors for Recurrence
• Peripheral vascular disease
• LN dissection
• XRT
• Liposuction
• Leg vein harvesting for CABG
• IVDA, skin popping
• Tinea pedis, onychomycosis
• Underlying vascular and lymphatic disease due to prior episodes

Possible Complications of Typical Cellulitis
• Bacteremia
• Lymphadenitis
• Subacute bacterial endocarditis
• Glomerulonephritis
• Elephantiasis nostra verrucosa


34


Evaluation
• History
– Onset and duration: first or recurrent episode
– Local symptoms: pain/ pruritus/ burning/ dysesthesia
– Associated symptoms: SOB, arthritis, diarrhea, headache,
cough, chills, fever
– Course/ progression
• Past medical, family, social history
• Medications

Evaluation: Objective
• General appearance
• Vital Signs:
– Fever: infection or systemic inflammation
• Pattern of fever (ie diurnal- Still’s disease)
– Tachycardia, hypotension
• LAD: infectious, inflammatory, neoplastic

Atypical Features or Unresponsive to Treatment:
• Resistant pathogens
• Cellulitis variant (ie- necrotizing, fungal)
• Pseudocellulitis

Diagnostic Testing for Cellulitis
• Labs
• Cultures
• Biopsy
• Imaging
• Special tests directed at pseudocellulitis
Diagnostic Testing for Cellulitis
• Labs: CBC w/ differential, CMP
• Cultures:
– Blood: 91% negative and usually not helpful• 19% S.pyogenes, 38% other β-hemolytic streptococci, 14% S.aureus,
28% Gram-negative
• ~50% of positive blood cultures represent contaminants
– Skin swabs, biopsy, aspiration usually low yield• Highly variable results
– Not recommended for uncomplicated/routine cellulitisLazzarini L, Conti E, Tositti G, Lalla F de. Erysipelas and cellulitis: clinical and microbiological spectrum in an Italian tertiary care hospital. J Infect. 2005;51(5):383-389. Hook EW 3rd, Hooton TM, Horton CA, Coyle MB, Ramsey PG, Turck M. Microbiologic evaluation of cutaneous cellulitis in adults. Arch Intern Med. 1986;146(2):295-297.Krasagakis K, Valachis A, Maniatakis P, Krüger-Krasagakis S, Samonis G, Tosca AD. Report: Analysis of epidemiology, clinical features and management of erysipelas. Int J Dermatol. 2010;49(9):1012-1017 Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of america. Clin Infect Dis Off PublInfect Dis Soc Am. 2014;59(2):e10-e52. Bates DW, Goldman L, Lee TH. Contaminant blood cultures and resource utilization. The true consequences of false-positive results. JAMA. 1991;265(3):365-369.Duvanel T, Auckenthaler R, Rohner P, Harms M, Saurat JH. Quantitative cultures of biopsy specimens from cutaneous cellulitis. Arch Intern Med. 1989;149(2):293-296Chira S, Miller LG. Staphylococcus aureus is the most common identified cause of cellulitis: a systematic review. Epidemiol Infect. 2010;138(3):313-317. Gunderson CG, Martinello RA. A systematic review of bacteremias in cellulitis and erysipelas. J Infect. 2012;64(2):148-155.

Inability of PCR, Pyrosequencing, and Culture to Identify the Cause of Cellulitis
• US ED evaluation of 49 subjects
– Samples taken from infected and unaffected skin
– No statistically significant differences between sides
– S. pyogenes > MSSA, no MRSA
• Conclusions: bacterial cause cannot be determined by comparison of prevalence and quantity of pathogens
Crisp JG et al. Inability of Polymerase Chain Reaction, Pyrosequencing, and Culture of Infected and Uninfected Site Skin Biopsy Specimens to Identify the Cause of Cellulitis. Clin Infect Dis. 2015 Aug 3.
Blood Cultures in Cellulitis
• 183 patients presenting to the MGH ED 10/2014 – 2/2016
with a presumed diagnosis of cellulitis
• 32.8 % (60) patients received blood cultures
– 90% (54/60) did not meet IDSA guidelines
– 96.7% (58/60) no growth (1 growth, 1 contaminant)
• Extrapolated annual national cost of diagnostic imaging and
blood cultures for presumed cellulitis: $226.9 million dollars
Ko L, Kroshinsky D. JAMA Internal Medicine.

When to Biopsy
• Atypical case in immunosuppressed patient
• Concern about non-bacterial etiology
– Special stains, cultures
• Concern for pseudocellulitis

Differential Diagnosis for Cellulitis
Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul 19;316(3):325-37.

Imaging: Only to Rule Out Other Conditions
• X-ray
– Osteomyelitis (chronic), foreign body
• Ultrasound
– Abscess, pyomyositis
• CT
– Osteomyelitis, pyomyositis*, necrotizing fasciitis*
• MRI
– Osteomyelitis*, pyomyositis, necrotizing fasciitis
Gold, RH, Hawkins, RA, Katz, RD. Bacterial osteomyelitis: Findings on plain radiography, CT, MR, and scintigraphy. AJR Am J Roentgenol1991; 157:365.

Imaging in Cellulitis
Test Total Tests
Obtained
Tests Changing
Diagnosis
Ultrasound - N(%) 85 (46.4) 1 (1.1)
Plain Radiograph - N(%) 53 (29.0) 1(1.9)
Computed Tomography - N(%) 29 (15.8) 2 (6.9)
Magnetic Resonance - N(%) 11 (6.0) 4(36.4)
• 183 patients presenting to the MGH ED 10/2014 – 2/2016 with a
presumed diagnosis of cellulitis
• 67.8% received imaging
• 22.3% received more than one test, up to four
Ko L, Kroshinsky D. JAMA Internal Medicine.
Conclusions
• Cellulitis is a common, costly, frequently overdiagnosed condition
• Consider alternate diagnoses in atypical cases or cases unresponsive to standard treatment
• Limit use of biopsies, imaging, ulcer and blood cultures
• Review antibiotic stewardship guidelines