Embed Size (px)
Citation preview

Evolving Indications forDOACs and Reversal Agents
ANIL K. BHANDARI, M.D.Director EPS, Good Samaritan/Harbor UCLA
Clinical Associate Professor of MedicineKeck School of Medicine, USC, Los Angeles

Lecture Outline
1 minute
3 minutes
2 minutes
16 minutes
Time
• What are DOACs?
• Established Indications for DOACs
• Reversal Agents
• Evolving Indications

Classification of Oral Anticoagulants (OACs)
Direct Indirect
ThrombinInhibitor
Factor XaInhibitor
Depletes synthesis of Vit K dependent clotting factors
Dabigatran(Pradaxa®)
Rivaroxaban (Xarelto®)Apixaban (Eliquis®)Edoxaban (Savaysa®)
WARFARIN
OAC

Variable DOACs Warfarin
Mechanism of action Factor X or Thrombin antagonist Depletes Factor V, VII, IXand X
Onset of actionPeak effectDuration of effect
15-30 minutes1-2 hours12-24 hours
>2-3 days4-7 days>3-5 days
Pharmacokinetics Predictable Highly variable
Need to monitor PT/PTT No Yes
Gender, race and age impact None / ± Significant
Dietary interactions None - Significant
Drug dose Fixed, renal adjustment + Highly variable No renal adjustment
Cost $300-400/mo $30-50 + Pro time
Antidotes Direct immediate reversal Indirect (Vit K, FFP)3-6 hours
How Are DOACsDifferent From Warfarin?
DOACs: Drug of Choice

Efficacy vs. Safety of NOACs vs Warfarin –Meta Analysis of 4 Trials
Ruff C, et al., Lancet. 2014;383:955-962

NOACs Treatment Trials
a. Schulman S, et al., Circulation. 2014;129:764-772[3]; b. Prins MH, et al., Thromb J. 2013;11:21[8]; c. Agnelli G, et al., N Engl J Med. 2013a;369:799-808[5]; d. Hokusai-VTE Investigators. N Engl J Med. 2013;369:1406-1415[4];
Recurrent VTE or VTE-related Death

NOACs Treatment Trials
a. Schulman S, et al., Circulation. 2014;129:764-772[3]; b. Prins MH, et al., Thromb J. 2013;11:21[8]; c. Agnelli G, et al., N Engl J Med. 2013a;369:799-808[5]; d. Hokusai-VTE Investigators. N Engl J Med. 2013;369:1406-1415[4];
Major Bleeding

Indication Dabigatran(Pradaxa®)
Rivaroxaban(Xarelto®)
Apixaban(Eliquis®)
Edoxaban(Savaysa®)
Non-valvularAFib
150 mg bid75 mg bid*
20 mg qd15 mg qd**
5 mg bid2.5 mg bid***
60 mg qd30 mg qd**
Acute Rx of DVT/PE
Parenteral 1 wk150mg bid
15 mg bid x 3 wks20 mg qd
10 mg bid x 1 wk5 mg bid
Parenteral x 1 wk60 mg qd
Extended prophylaxis after DVT/PE
NA 10 mg qd 2.5 mg bid NA
DVT prophylaxis after Hip/Kneereplacement
NA 10 mg qd 2.5 mg bid NA
FDA and Guidelines Endorsed Indications for DOACs
***
***
Creatinine clearance 15-30 ml/minCreatinine clearance 15-50 ml/minAge ≥80 yrs, body weight <60 kg, creatinine >1.5 mg/dl

Evolution in Baseline Treatment for Patients Enrolled in
Sequential Cohorts of GARFIELD-AF
Cohorts 1-5, N = 51,270Kakkar AJ, ESC, 2006. FP 412

Patients Who Should NOT Be Treated with a NOAC
• Mechanical heart valve
• Moderate or severe mitral stenosis
• ESRD on hemodialysis* (not guidelines endorsed) or hepatic impairment
• Extremes of weight (> 150kg or < 50kg)
• Pregnant or lactating women
• Children
• Poor adherence
[a,b]
[a,b]
Only apixaban /rivaroxaban may be used in stable patients on hemodialysis; avoid all other NOACs if CrCl < 15 mL/min
a. Heidbuchel H, et al., Europace. 2015;17:1467-1507; b. January CT, et al., J Am Coll Cardiol. 2014;64:e1-e76; c. Streiff MB, et al., J ThrombThrombolysis. 2016;41:32-67.

Reversal Agents for DOACs
Background:
• 2.5 million patients in U.S. use DOACs
• Major bleeds in 1-3%
- ~ 117,000 patients hospitalized/yr
• In hospital mortality of 8%
- 25% for intracranial hemorrhages
• Most bleeding events effectively managed with supportive care
Temporary discontinuation may be all that is required.

Candidates for Reversal Agents
• Patients presenting with major bleed- Life threatening (e.g., intracranial)- Critical organ or closed-space (pericardial/retro peritoneal)- Ongoing bleeding despite measures to control
• Patients at high risk of bleeding
- Requiring emergent/urgent procedure- Expected long delay in hemostasis restoration (renal failure,
over-anticoagulation)
Prior to reversal: Type of DOACDose and time of last ingestionRenal function

Idarucizumab (Praxbind®) Andexanet alfa (Andexxa®)
Target Dabigatran Factor Xa inhibitors
Structure Humanized Fab fragment Recombinant Factor Xa variant (decoy)
Mechanism Binds Dabigatran with highaffinity
Competes with Factor Xa for inhibitor binding
FDA approved Oct 16, 2015 May 4, 2018
Administration Bolus Bolus + infusion
Onset of action Immediate Immediate
Dose 5 gm bolus 400 mg/800 mg bolus2-4 hour infusion
Cost for reversal $4,200 $34,000-68,000
Reversal Agents for DOACs

Patient Subset Target Benefit
Mechanical prosthetic valves Thrombus deposition on valve
Acute Coronary Syndrome MI, UA, stroke, death
Stable CAD/PAD MI, UA, stroke, acute limb ischemic events
Heart failure HF re-hospitalization, MI, stroke and death
DVT prophylaxis in medically ill patients DVT, pulmonary embolism, death
Afib in the setting of PCI Major bleeds
Potential Indications for DOACs

Dabigatran vs. Warfarin in Patients with Mechanical Heart Valves
RE-ALIGN
Premature termination in November 2012XEikelboom et al., N Engl J Med 2013;369:1206-1214

Thrombus Development After Plaque Disruption
White, H., Clin and Applied Thromb/Hemostasis 2014;20:516-523
Atherothrombosis

Primary and Secondary HemostaticResponses to Vascular Injury
White, H., Clin and Applied Thromb/Hemostasis 2014;20:516-523

Combined Anticoagulant and AntiplateletTherapy in
Vascular Disease
• Hemostatic mechanisms following plaque rupture involve both platelets and thrombin
• Thrombin activates coagulation factors (XI, XIII, thrombomodulin) and converts fibrinogen to fibrin
• Thrombin potent platelet activator
• Clinical outcomes likely to be improved by modulating both platelet-and thrombin-driven pathways
Rationale:

Unmet Need in Acute Coronary Syndrome Management
• Dual antiplatelet (DAP) agents represent cornerstone of therapy to prevent recurrent ischemic events
• Risk of residual ischemic events ~ 10% at 1 year despite significant benefits of DAP
• Persistent elevation of coagulation mechanisms for up to 6 months after ACS (Merlini et al., Circulation 1994;90:61-68
• Warfarin addition to mono- or dual APT, MI and stroke by ~ 20% but 8-fold major bleeds (Anand et al., JAMA 1999;282:2058)
Role of DOACs in ACS?

NOACs in ACS
ATLAS ACS2 – TIMI 51[a]
• Reduced doses of rivaroxaban (2.5 mg/5 mg twice daily) + DAPT
• Mortality benefit for lower-dose rivaroxaban
APPRAISE[b]
• Full-dose apixaban used
• Trial stopped due to excess bleeding and no efficacy signal
a. Mega JL, et al., N Engl J Med. 2012;366:9-19; b. Alexander JH, et al., N Engl J Med. 2011;365:699-708

Rivaroxaban in Acute Coronary Syndrome
• 15526 ACS patients randomized to Rivaroxaban 2.5 mg bid or 5 mg bid in addition to single or dual APT
• Compared to standard therapy, Rivaroxaban 2.5 mg bid reduced the risk of death from CV cause, MI or stroke by 16% (p<0.05) Stent thrombosis also by 35% (p=0.02)
• risk of major bleed and intracranial hemorrhage, especially with higher dose of Rivaroxaban
2.5 mg dose Rivaroxaban approved in Europe but not by FDA
ATLAS ACS2-TIMI51

REACH International Registry
Alberts et al., Eur Heart J 2009;30:2318-2326

Vascular Events in REACH Registry
Alberts et al., Eur Heart J 2009;30:2318-2326

Rivaroxaban With or Without Aspirin in Stable CAD and/or PAD
• 27395 patients with stable CAD/PAD, enrolled from 2013-16 randomized to 3 arms:- Riva 2.5 mg bid + ASA 100mg- Riva 5 mg bid- ASA 100mg
COMPASS Trial
• Primary Outcome- Efficacy: Composite of MI, stroke or CV death- Safety: Major bleeding (modified ISTH criteria)
• Trial stopped earlier on Feb 6, 2017 due to superior efficacy of Riva over ASA
Eikelboom et al., NEJM 2017;377:1319-30

Patient CharacteristicsCOMPASS Trial
Eikelboom et al., NEJM 2019
Variable Riv 2.5 mg bid+ ASA RIV 5 mg bid ASA alone
No. of patientsAge, years
9152 68 ± 8
911768 ± 8
912668 ± 8
Vascular diseaseCADPAD
91%27%
90%27%
90%27%
HypertensionDiabetesPrevious strokePrevious MIHeart failure
75%38%3.8%62%21%
75%38%3.8%62%21%
75%38%3.7%63%22%
StatinsACE/ARB
90%71%
90%72%
89%71%

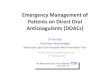
Primary Outcome in COMPASS
Eikelboom et al., NEJM 2017;377:1319-30

COMPASS: Efficacy Outcomes
* HR and P value vs. aspirin alone.
Eikelboom, JW, et al., N Engl J Med 2017;377:1319-1330.

P-Value
Outcome RIV + ASA RIV alone ASA
RIV + ASAvs.
ASA
RIVvs.
ASA
Major bleeding 3.1% 2.8% 1.9% <0.001 <0.001
Fatal bleeds 0.2% 0.4% 0.2% 0.32 0.41
Site of bleedsGICNSSkinURI
1.5%0.3%0.3%0.1%
1.0%0.5%0.3%0.3%
0.7%0.5%0.1%0.3%
<0.0010.600.010.16
0.040.020.010.20
Net Clinical Benefit Outcome* 4.7% 5.5% 5.9% 0.001 0.36
Bleeding Events and Net Clinical Benefit in COMPASS Trial
* Net composite of reduction in CV death, stroke, MI and adverse increase in fatal/critical organ bleed
Eikelboom et al., NEJM 2017;377:1319-30
0.3%

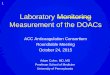
Primary Outcome in COMPASS:CAD vs PAD
Anand et al., JACC 2018;71:2306-2315
Primary Outcome
Group Riv+ ASA ASA alone Hazard Ratio p value
CAD 4% 6% 0.74 <0.0001
PAD 5% 7% 0.72 <0.005
Significantly fewer amputations 19/2139 in Riv + ASA vs 36/2123 in ASA (p<0.02)

COMPASS: Prognosis After MALE by Treatment Group
* HR determined by time-dependent Cox model.
Anand SS, et al., J Am Coll Cardiol 2018;71:2306-2315

Rivaroxaban for Stable CAD/PAD
• Approved on Oct 11, 2018
• Indication:- To reduce the risk of major CV events: stroke, MI or death
• Dose:
- 2.5 mg bid in combination with ASA (75 mg to 100 mg) daily
- No dose adjustment for CrCl

COMMANDER HF: Design
* Standard of care for HF and CAD as prescribed by the patient’s managing physician.
ClinicalTrials.gov. NCT01877915; Zannad F, et al., Eur J Heart Fail. 2015;17:735-742

Outcome in COMMANDER
HF Trial
Primary Outcome: Death, MI or stroke
Zannad et al., NEJM 2018;379:1332-42

DVT Prophylaxis in Patients with Medical Illness
• 36 million annual hospitalizations and half due to medical illness
• About 20% of medically ill patients at risk of VTE
• LMWH in hospital prophylaxis: enoxaparin 40 mg/d standard of care
• Once discharged but not prophylaxed, these patients are at high risk for VTE (DVT + PE): 1-2% risk at 1 month
• Unmet need for extended duration and prophylaxis

BetrixabanClinical features
a. Chan NC, et al., Vasc Health Risk Manag. 2015;11:343-351; b. Cohen AT, et al., N Engl J Med. 2016;375:534-544; c. BEVYXXA™ PI 2017.
• FXa inhibitor[a]
• 19- to 25-h half-life[a]
• Low peak:trough ratio[a]
• 17% renal clearance[a]
• Antidote (Andexanet)[a]
• Lower thrombus burden due to better “clean-out” of veins with betrixban explains “legacy effect”[b]
Indication and usage[b]
• Indicated for VTE prophylaxis in adult patients hospitalized for an acute medical illness who are at risk for thromboembolic complications due to moderate or severe restricted mobility and other risk factors for VTE
• Safety and efficacy have not been established in patients with prosthetic heart valves

APEX Study Design
*Heart failure decompensation, respiratory failure, infection without septic shock, rheumatic disorders, ischemic stroke (with immobilization).Cohen AT, et al., N Engl J Med. 2016;375:534-544

APEX Primary Efficacy Endpoint
Cohen AT, et al., N Engl J Med. 2016;375:534-544
• Asymptomatic proximal DVT, symptomatic proximal/distal DVT, non-fatal PE, VTE-related death

MARINER Study Design• Phase 3 randomized trial evaluating the efficacy and safety of rivaroxaban vs
placebo on reducing post-discharge VTE in high-risk medically ill patients with 30-day follow-up
*Estimated enrollment submitted April 10, 2017. † Taken daily, with or without food. †† Day 1-45. ClinicalTrials.gov. NCT02111564.

AF Patients Undergoing PCIACC/AHA Guidelines - 2016
• Assess ischemic and bleeding risks
• Keep triple therapy as short as possible - dual therapy in select patients
• Clopidogrel is the preferred P2Y12 inhibitor
• Low dose ASA (<100 mg) preferred
• Consider INR target 2.0-2.5 for Warfarin
• Use PPIs in those with GI bleed Hx
Levine et al., JACC 2016;68:1082-1115

Triple vs. Dual Combination Therapy Post PCI: WOEST Trial
*Vitamin K antagonist indicated for patients with AF/flutter, mechanical heart valve, apical aneurysm, pulmonary embolus, peripheral artery disease, or ejection fraction < 30%.
Dewilde WJM, et al., Lancer 2013;381:1107-1115
• 573 patients receiving OAC* and undergoing PCI were assigned to clopidogrel alone (dual therapy) or clopidogrel + aspirin (triple therapy) for 1 year in open-label, multicenter, randomized trial
Results:
• Most bleeding episodes occurred within 180 days of PCI
• Rate of thrombotic and thromboembolicevents did not differ between treatment groups
• Study supported that OAC is as good as aspirin in preventing thrombotic events (e.g., stent thrombosis) but was not powered to detect difference
• Prompted need for change in clinical decisions

New Era with NOACs: PIONEER AF PCI Study Design
a. Gibson CM, et al., Am Heart J. 2015;169:472-478.e5; b. Gibson CM, et al., N Engl J Med. 2016;22;375:2423-24434

PIONEER AF-PCI:Clinically Significant Bleeding
Gibson CM, et al., N Engl J Med. 2016;22;375:2423-24434
• Both doses of rivaroxaban were lower than the dose traditionally used for stroke prevention and AF-Also reduced combined endpoint of re-hospitalizations and all-cause mortality-Are we confident these doses maintain protection against stroke and systemic
embolism?

PIONEER AF-PCI: MACE
Gibson CM, et al., N Engl J Med. 2016;22;375:2423-24434

Summary Statements for DOACs
• DOACs recommended over warfarin for nonvalvular AF (except moderate/severe MS and prosthetic mechanical valves (2019 ACC Guidelines for AF)
• DOACs preferred over War and LMWH for acute and extended RX of acute PE and DVT
• Rivaroxaban and ASA indicated for reducing major vascular events in stable CAD/PVD
• After coronary stenting in AF pts, double therapy with clop and Rivaroxaban/dabigatran reasonable over triple Rx