Embed Size (px)
Citation preview

Medical Dosimetry
Medical Dosimetry 39 (2014) 18–22
0958-39http://d
RepMemoriTel.: þ1
E-m
journal homepage: www.meddos.org
Bilateral implant reconstruction does not affect the quality of postmastectomyradiation therapy
Alice Y. Ho, M.D.,* Nisha Patel, M.D.,† Nisha Ohri, M.D.,‡ Monica Morrow, M.D.,§ Babak J. Mehrara, M.D.,‖
Joseph J. Disa, M.D.,‖ Peter G. Cordeiro, M.D.,‖ Weiji Shi, B.S.,¶ Zhigang Zhang, Ph.D.,¶ Daphna Gelblum, M.D.,*Claire T. Nerbun, M.S.,# Katherine M. Woch, M.S.,# Ase Ballangrud, Ph.D.,# Beryl McCormick, M.D.,* andSimon N. Powell, M.D., Ph.D.**Department of Radiation Oncology, Memorial Sloan-Kettering Cancer Center, New York, NY; †Drexel University College of Medicine, Philadelphia, PA; ‡Department of RadiationOncology, Mount Sinai School of Medicine, New York, NY; §Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, New York; ‖Department of Plastic Surgery,Memorial Sloan-Kettering Cancer Center, New York, NY; ¶Department of Biostatistics and Epidemiology, Memorial Sloan-Kettering Cancer Center, New York, NY; and #Department ofMedical Physics, Memorial Sloan-Kettering Cancer Center, New York, NY
A R T I C L E I N F O
Article history:Received 8 January 2013Accepted 14 August 2013
Keywords:Breast cancerImmediate reconstructionImplantPostmastectomy radiation
47/$– see front matter Copyright � 2014 Amx.doi.org/10.1016/j.meddos.2013.08.008
rint requests to: Alice Y. Ho, M.D., Departmal Sloan-Kettering Cancer Center, 1275 York A212 639 6773; fax: þ1 212 639 2417.ail: [email protected]
A B S T R A C T
To determine if the presence of bilateral implants, in addition to other anatomic and treatment-relatedvariables, affects coverage of the target volume and dose to the heart and lung in patients receivingpostmastectomy radiation therapy (PMRT). A total of 197 consecutive women with breast cancerunderwent mastectomy and immediate tissue expander (TE) placement, with or without exchange fora permanent implant (PI) before radiation therapy at our center. PMRT was delivered with 2 tangentialbeams þ supraclavicular lymph node field (50 Gy). Patients were grouped by implant number: 51%unilateral (100) and 49% bilateral (97). The planning target volume (PTV) (defined as implant þ chestwall þ nodes), heart, and ipsilateral lung were contoured and the following parameters were abstractedfrom dose-volume histogram (DVH) data: PTV D95% 4 98%, Lung V20Gy 4 30%, and Heart V25Gy 4 5%.Univariate (UVA) and multivariate analyses (MVA) were performed to determine the association ofvariables with these parameters. The 2 groups were well balanced for implant type and volume, internalmammary node (IMN) treatment, and laterality. In the entire cohort, 90% had PTV D95% 4 98%, indicatingexcellent coverage of the chest wall. Of the patients, 27% had high lung doses (V20Gy 4 30%) and 16% hadhigh heart doses (V25Gy 4 5%). No significant factors were associated with suboptimal PTV coverage.On MVA, IMN treatment was found to be highly associated with high lung and heart doses (bothp o 0.0001), but implant number was not (p ¼ 0.54). In patients with bilateral implants, IMN treatmentwas the only predictor of dose to the contralateral implant (p ¼ 0.001). In conclusion, bilateral implantsdo not compromise coverage of the target volume or increase lung and heart dose in patients receivingPMRT. The most important predictor of high lung and heart doses in patients with implant-basedreconstruction, whether unilateral or bilateral, is treatment of the IMNs. Refinement of radiationtechniques in reconstructed patients who require comprehensive nodal irradiation is warranted.
& 2014 American Association of Medical Dosimetrists.
Introduction
Maximizing survival and quality of life are complementarygoals in the treatment of breast cancer. Postmastectomy radiationtherapy (PMRT) and breast reconstruction are 2 modalities used to
erican Association of Medical Dos
ent of Radiation Oncology,venue, New York, NY 10065.
achieve these goals. By providing local control, PMRT improvesdisease-free survival in node-positive breast cancer.1 Breast recon-struction enhances cosmesis and contributes significantly topatients' quality of life.2 Opinions regarding the optimal integra-tion of these modalities vary. Some have suggested that immediatereconstruction hinders radiation treatment planning, whereasothers disagree.3–5 Despite the ongoing controversy, immediatereconstruction with a 2-stage tissue expander (TE)/permanentimplant (PI) continues to be a popular option chosen by manypatients.
imetrists

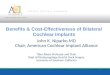
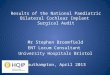
Fig. 1. Tangential beams in example patients with (A) unilateral and (B) bilateral implants. (Color version of figure is available online.)
A.Y. Ho et al. / Medical Dosimetry 39 (2014) 18–22 19
Over recent years, our department has treated a high volume ofpatients with bilateral implant reconstructions. Subsequently, thequestion of whether the presence of bilateral implants hindersradiation treatment planning in these patients has been raised.Precise geometric placement of the tangent beams is particularlycritical to minimize dose to normal organs and the contralateralside without compromising the ipsilateral target volume coverage(Fig. 1).
Our objectives were to quantify the effect of implant number(unilateral vs bilateral) and other implant and treatment factors ontarget volume coverage, and heart and lung dose in patients withbreast cancer who underwent immediate reconstruction andPMRT. In addition, the dose delivered to the contralateral implantwas quantified in patients with bilateral implants.
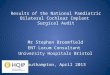
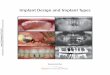
Fig. 2. Contoured structures and their respective dosimetric end points. (Colorversion of figure is available online.)
Methods and Materials
The study design was approved by the institutional review board at MemorialSloan-Kettering (MSKCC).
Patients
From 2004 to 2009, 974 patients with Stage II–III breast cancer underwentmastectomy and immediate TE placement at our institution. Of these, 307 receivedPMRT in our department. After excluding patients with a history of chest wallirradiation (5), receipt of nonstandard PMRT techniques (30), removal of theimplant before PMRT (15), and inaccessible treatment plans (60), 197 patientsconstituted the study cohort.
One hundred patients had unilateral and 97 bilateral breast prostheses (TEs orPIs). Of the 197 patients, 159 (80.7%) underwent exchange of the TE for PI(s) beforePMRT according to an institutional algorithm6; whereas 38 (19.3%) patientsunderwent irradiation of the TE and had the exchange for a PI performed afterPMRT. Of the 38 patients, 12 had unilateral TEs and 26 had bilateral TEs. All TEswere filled to the maximum planned volume before radiation therapy. Among the159 patients who received PMRT to the PI, 80 had unilateral and 79 had bilateralimplants.
Target delineation
Delineation of the target structures are shown in Fig. 2. The ipsilateral lung wasdefined using the automated tracking gradient contour function for lung paren-chyma in the MSKCC Top Module Treatment Planning System. The heart wasdefined as the cardiac silhouette starting inferior to the aortic arch and extendingdown to the inferior left ventricle. The contralateral implant was defined as thecontralateral prosthesis and overlying skin.
The planning target volume (PTVCW) consisted of the chest wall, implant,overlying skin, level I–II axillary lymph nodes, and internal mammary nodes(IMNs) when applicable. The supraclavicular lymph nodes and level III nodeswere not included in the PTV, as they were encompassed by a separate anterioroblique beam and would be unaffected by implant number. A uniform 3-mmmargin to account for respiratory motion and setup error was included withinthe PTV. The chest wall and axillary lymph nodes were contoured usingconsensus guidelines.7 IMNs were treated as per individual physician's discre-tion. When targeted, the IMNs were contoured within the first 4 intercostalspaces. In these cases, the chest wall and nodal target was termed PTVCW þ IMN.The dosimetric effects of supraclavicular fields were included in the dose-volumehistograms (DVH).
Radiation treatment
All patients received ipsilateral PMRT to a total dose of 50 to 50.4 Gy deliveredin 25 to 28 fractions. A 0.5- or 1.0-cm bolus over the chest wall was used on a dailybasis. No patients received a chest wall boost.
Radiation treatment was delivered using 2 tangential photon beams coveringthe chest wall, the implant and lower axillary nodes were matched to an anterioroblique field encompassing the supraclavicular fossa. The tangential fields wereeither planned with wedges (6%) or simplified intensity-modulated radiationtherapy (94%) technique.8 Treatment planning was performed using the MSKCCtreatment planning system,9–13 which has been previously described. Tissueinhomogeneity corrections were applied to all dose calculations. 6 or 15-MVphotons were utilized, depending on the medial-lateral separation of the patient.Patients with TEs received 15-MV photons to minimize attenuation from themetal port.14 When the IMNs were targeted, either wide tangential photons oranterior oblique electron fields matched to shallow tangents were used. Treat-ment plans were selected by the treating physician based on the optimalcombination of coverage and avoidance of excessive dose to normal tissue asseen on planning CT scans or DVHs or both. There were no formal dosimetricguidelines.
Dosimetric data
DVH data were generated for each patient. The volume of ipsilateral lungreceiving r 20 Gy (Lung V20) and the percentage of the prescription dose deliveredto Z 95% of the PTV (PTVCWD95 or PTVCW þ IMND95) was analyzed in all patients. Inbilateral implant patients, the Dmax and its location within the contralateral implantvolume was identified on the treatment plan.
Statistical analysis
Differences in clinical, anatomic, and dosimetric characteristics between groupswere assessed using the Pearson χ2 test, Fisher exact test, or t-test. Univariateanalysis (UVA) was performed to test the association of variables on each of thedosimetric end points. Multivariate analysis (MVA) was performed on the mainvariable of interest, implant number (unilateral vs bilateral), in addition to anyother variables that were significant (p o 0.05) on UVA.

Table 1Clinical and treatment characteristics by implant number
Total(n ¼ 197)
Unilateral(n ¼ 100)
Bilateral(n ¼ 97)
p Value
n % n % n %
Age at diagnosiso 50 y of age 129 65.5 53 53.0 76 78.4 0.0002Z 50 y of age 68 34.5 47 47.0 21 21.6
LateralityRight 89 45.2 46 46.0 43 44.3 0.81Left 108 54.8 54 54.0 54 55.7
Chemotherapy sequenceAdjuvant 171 86.8 86 86.0 85 87.6 0.87Neoadjuvant 25 12.7 13 13.0 12 12.4
Irradiated implant typePermanent implant 159 80.7 88 88.0 71 73.2 0.009Tissue expander 38 19.3 12 12.0 26 26.8
Radiation techniqueSimplified IMRT 185 93.9 95 95.0 90 92.8 0.523DCRT 12 6.1 5 5.0 7 7.2
Radiation planning field typeStandard tangents 173 87.8 88 88.0 85 87.6 1.00Wide tangents 16 8.1 8 8.0 8 8.2Electron strip þ tangents 8 4.1 4 4.0 4 4.1
Treatment of IMNsNo 174 88.3 89 89.0 85 87.6 0.83Yes 23 11.7 11 11.0 12 12.4
3DCRT ¼ 3-dimensional conformal radiation therapy; IMN ¼ internal mammarylymph nodes; IMRT ¼ intensity-modulated radiation therapy.
Table 2Patient characteristics by implant number
Total(n ¼ 197)
Unilateral(n ¼ 100)
Bilateral(n ¼ 97)
p Value
Implant and anatomic characteristics (median values)Implant height (cm) 12.3 12.3 12.3 0.37Implant width (cm) 12.4 12.9 12.0 o 0.0001Implant projection (cm) 5.2 5.3 5.1 0.74Implant volume (cm3) 486.9 510.7 469.2 0.12Tangent posterior separation(cm)
20.2 21.2 19.5 0.007
Lung volume (cm3) 1215.8 1202.3 1288.7 0.58Heart volume (cm3) 535.7 528.9 540.2 0.13
Dosimetric characteristicsPTVCWD95
o 98% 19 (9.6) 9 10 0.76Z 98% 178 (90.4) 91 87
PTVCWþIMND95 (n ¼ 23)o 98% 4 (17.4) 0 4 0.09Z 98% 19 (82.6) 11 8
Ipsilateral lung V20
o 30 144 (73.1) 75 69 0.54Z 30 53 (26.9) 25 28
Heart V25
o 5 166 (84.3) 82 84 0.38Z 5 31 (15.7) 18 13
A.Y. Ho et al. / Medical Dosimetry 39 (2014) 18–2220
Results
Baseline characteristics of patient groups
Treatment and relevant clinical characteristics of the unilateraland bilateral groups are compared in Table 1. Compared withpatients with unilateral implants, bilateral implant patients wereyounger (p ¼ 0.0002) and more than twice as likely to undergoirradiation of TEs (26.8% vs 12.0%, p ¼ 0.009). All patients receivedchemotherapy; most of it (87%) was adjuvant and 13% was neo-adjuvant using anthracycline and taxane-based or cyclophospha-mide, methotrexate, and 5-fluorouracil regimens. Only 23 patients(11.7%) received treatment of the IMNs (11 unilateral vs 12bilateral, p ¼ 0.83). Fifteen of these patients received treatmentwith wide tangential photons and 8 with an anterior obliqueelectron field matched to shallow tangents.
Median values for implant dimensions and anatomic character-istics between the 2 groups are included in Table 2. Implant height,projection, and volume were similar, as were median lung andheart volumes (all p 4 0.05). Median implant widths weresignificantly less in patients with bilateral implants (12.0 vs12.9 cm, p o 0.0001), reflecting the tendency for smaller implantwidths in patients who require juxtaposition of 2 implants on thechest wall. The median posterior separation of the tangent beamswas greater in patients with unilateral reconstructions (21.2 vs19.5 cm, p ¼ 0.007).
Frequency and distribution of dosimetric end points
Table 2 also demonstrates the categorical distribution of thedosimetric end points by groups. Most patients in the cohort hadexcellent coverage of the chest wall, as reflected by 90.4% ofpatients (178/197) with PTVCWD95 Z 98%. Nine patients withunilateral and 10 with bilateral breast prosthesis had PTVCW o 98%(p ¼ 0.76). Subset analysis of the 23 patients (11 unilateral and 12bilateral) in whom IMNs were included in the target volumes(PTVCW þ IMN) showed that 82.6% (19/23) of them achieved D95Z 98%.
All 11 patients with unilateral implants achieved D95 Z 98%, whereas4 of the 12 patients with bilateral reconstructions did not. Owing tothe small number of patients in this subgroup, this difference did notreach statistical significance (p ¼ 0.09).
Of the cohort, 73.1% (144/197) had ipsilateral lung V20 o 30%,with similar proportions of unilateral and bilateral patients withinboth dose categories (p ¼ 0.54). Most patients (84.3%) in the cohorthad low heart doses (V25 o 5%), again with no difference indistribution between the 2 groups (p ¼ 0.38).
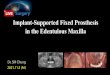
Lastly, dose to the contralateral breast implant was assessedin the 97 patients with bilateral implants. The median contrala-teral implant volume and distance between the 2 implants was447.2 cm3 and 5.4 cm, respectively. The tangent beams traversedthrough the contralateral implant in 14 patients, 5 of whom hadthe IMNs targeted. The Dmax ranged from 9% to 122% of theprescription dose (Fig. 3). The Dmax was located within themedial aspect of the flap overlying the contralateral implant inall 14 cases. There were no cases among unilateral implantpatients in which the radiation beams exited through thecontralateral breast tissue. The volumes of both expanders werecompared separately among the 26 patients with bilateral TEsand found to be within 3.4% to 5.0% variation of each other (datanot shown).
UVA and MVA
The results of the UVA and MVA of the variables performedon each of the dosimetric end points are presented in Table 3.On UVA, implant number was not significantly associated withhigh heart or lung doses and did not affect coverage of thetarget volume (all p 4 0.05). Given the lack of associationbetween the remainder of the variables and PTVCW � IMND95 o 98%,MVA was not performed. Among the variables examined, highposterior separation (4 24 cm) was significantly associated withheart V25 Z 5% on both UVA (p ¼ 0.031) and MVA (p ¼ 0.016).The effect of implant type (PI vs TE) on heart V25 Z 5% reachedborderline significance on UVA (p ¼ 0.051); thus MVA was notperformed. Treatment of the IMNs was the only inde-pendent predictor of radiation receipt to the contralateral implant(p ¼ 0.001).

Fig. 3. Receipt of radiation to contralateral breast among 14 patients, ordered from lowest to highest percentageDmax value. (Color version of figure is available online.)
A.Y. Ho et al. / Medical Dosimetry 39 (2014) 18–22 21
Discussion
The delivery of PMRT in the setting of bilateral implantreconstruction has become an increasingly common treatmentscenario over the past decade. Increasing nationwide rates ofcontralateral prophylactic mastectomy and the broader use ofPMRT for node-positive patients are contributing factors to thefrequency of this approach.15 Patients with breast cancer may alsofind bilateral implant reconstruction appealing because
Table 3Univariate and multivariate analyses
PTVCW � IMN
D95 o 98%Lung V20
Z 30%Heart V25
4 5%Receipt ofcontralateralradiotherapy
Univariate analysis (p value)Treatment ofIMNs
0.56 o 0.0001 0.046 0.001
Implantnumber
0.76 0.54 0.38 NP
Tangentposteriorseparation
0.99 0.4651 0.031 0.28
Irradiatedimplant type
0.16 0.47 0.051 0.15
Implant height 0.86 0.5987 0.24 0.74Implant width 0.29 0.7437 0.09 0.99Implantprojection
0.59 0.85 0.38 0.35
Ipsilateralimplant volume
0.95 0.69 0.84 0.53
Contralateralimplant volume
0.79 0.38 0.67 0.25
Distancebetween implants
0.24 0.94 0.76 0.08
Laterality 0.22 0.53 NP 0.21Multivariate analysis (p value)Treatment ofIMNs
NP o 0.0001 0.022 0.001
Implantnumber
NP NP NP NP
Tangentposteriorseparation
NP NP 0.016 NP
NP ¼ not performed.
simultaneous reconstruction of both breasts is convenient andenhances cosmesis by optimizing symmetry.16
Given the growing popularity of this approach, we questionedwhether the presence of a contralateral implant would hindertreatment planning in patients with breast cancer who requiredPMRT. The effect of bilateral reconstruction on PMRT was eval-uated by using dosimetric end points for chest wall coverage andheart and lung dose, which served as surrogates for the quality ofPMRT. The cohort was well balanced with respect to the number ofpatients with unilateral and bilateral reconstructions and treat-ment, and implant-specific variables, which facilitated comparisonbetween groups.
Relative to patients with unilateral implants, we found that thepresence of bilateral implants neither compromised target volumecoverage nor increased ipsilateral lung and heart doses. Despitethe small percentage of patients in whom the IMNs were targeted,treatment of the IMNs was the only independent predictor ofincreased dose to the ipsilateral lung, heart, and contralateralimplant. This result is consistent with prior reports of increasedcardiac and pulmonary dose in reconstructed patients receivingIMN irradiation.5,17 Until long-term data from randomized trialsproving the efficacy of IMN irradiation become available, thesefindings highlight the dilemma of balancing potential benefits vsthe toxicities of IMN irradiation in patients who undergo breastreconstruction.
Minimizing irradiation of the contralateral breast is an impor-tant goal when treating patients with bilateral breast reconstruc-tions. Among 97 patients with bilateral implants, 14 (14.4%)received dose to the contralateral implant. Examination of thetreatment plans of these patients revealed that these Dmax pointswere located within the medial aspect of the flap overlying thecontralateral implant. The magnitude of dose varied widely andwas attributable to incidental scatter dose or high separation fromthe beams entering through the medial aspect of the contralateralimplant. However, the following caveats must be taken intoconsideration when interpreting the Dmax values: (1) Dmax repre-sents the maximum dose to a small point, rather than a definedvolume and (2) at the time of treatment, efforts were made to tapethe contralateral implant away from the treatment field. Therefore,the reported Dmax may be an overestimate of the true maximumdose delivered to the contralateral reconstructed breast. Interest-ingly, the distance between implants was not found to affect

A.Y. Ho et al. / Medical Dosimetry 39 (2014) 18–2222
contralateral breast dose, as most patients in the bilateral cohorthad at least a 3-cm gap between implants.
TEs often contain 25% to 30% more saline than a PI, the purposeof which is to create an ample pocket within the chest wallmusculature in anticipation of subsequent exchange with a PI.Given their larger size, the feasibility of irradiating TEs has beenquestioned by clinicians, but never rigorously reported. In ourstudy, TEs were irradiated in 38 patients who received neoadju-vant chemotherapy, owing to clinical concerns of delaying radia-tion therapy in this population of patients who tend to presentwith advanced-stage disease. Irradiation of TEs was not found tosignificantly affect any of the measured dosimetric end points(Table 3), thus dispelling concerns that the overinflated shape ofTEs can compromise PMRT delivery.
A significant limitation of the study that warrants mention wasthe inability to capture the effect of individual anatomy on thedosimetric end points. Curvature and depth of the chest wall aswell as distance between the heart and chest wall can varysignificantly between patients. Given the absence of a reliablemetric to measure these anatomic characteristics, we could notfactor them into the analysis. Secondly, in patients with bilateralTEs, it is common for clinicians to remove saline from thecontralateral TE when arrangement of the tangent beams appearssuboptimal at the time of simulation. In anticipation of criticismthat such a practice could bias the results of the study, theindividual TE volumes of the 26 patients with bilateral TEs werecontoured and found to be within 5% of each other. This con-cordance between TE volumes confirms our belief that fluid wasnot withdrawn from one of the TEs to facilitate treatment plan-ning. Lastly, it is possible that the significant number of inacces-sible treatments plans that were excluded could have biased ourresults.
In summary, compared with patients with unilateral implants,the presence of bilateral implants did not affect target coverage orheart and lung dose in patients receiving PMRT. Among all theimplant and treatment variables analyzed, treatment of the IMNswas the only predictive factor for increased dose to the heart, lung,and contralateral implant. This effect was seen independent ofimplant number. Although we demonstrated that most patients inthe cohort, including women with bilateral implants, had accept-able treatment plans, these data nevertheless underscore thepotential to further improve radiation techniques in women withimplant reconstruction who receive comprehensive nodal irradi-ation. Multibeam intensity-modulated radiation therapy photonplans or proton therapy may serve as an alternative to conven-tional techniques and represent future topics for research in thisgrowing population of patients with breast cancer.
Conflict of Interest
Dr. Cordeiro received a grant from Allergan, which providesfinancial and material support for participation in a multicenterclinical research study. The other authors have no conflicts ofinterest.
References
1. Clarke, M.; Collins, R.; Darby, S.; et al. Effects of radiotherapy and of differencesin the extent of surgery for early breast cancer on local recurrence and 15-yearsurvival: an overview of the randomised trials. Lancet 366:2087–106; 2005.
2. Elder, E.E.; Brandberg, Y.; Bjorklund, T.; et al. Quality of life and patientsatisfaction in breast cancer patients after immediate breast reconstruction: aprospective study. Breast 14:201–8; 2005.
3. Motwani, S.B.; Strom, E.A.; Schechter, N.R.; et al. The impact of immediatebreast reconstruction on the technical delivery of postmastectomy radiother-apy. Int. J. Radiat. Oncol. Biol. Phys. 66:76–82; 2006.
4. Koutcher, L.; Ballangrud, A.; Cordeiro, P.G.; et al. Postmastectomy intensitymodulated radiation therapy following immediate expander-implant recon-struction. Radiother. Oncol. 94:319–23; 2010.
5. Ohri, N.; Cordeiro, P.G.; Keam, J., et al. Quantifying the impact of immediatereconstruction in postmastectomy radiation: a large, dose-volume histogram-based analysis. Int. J. Radiat. Oncol. Biol. Phys. 2012 84:e153-e159.
6. Wright, J.L.; Cordeiro, P.G.; Ben-Porat, L.; et al. Mastectomy with immediateexpander-implant reconstruction, adjuvant chemotherapy, and radiation forstage II-III breast cancer: treatment intervals and clinical outcomes. Int. J.Radiat. Oncol. Biol. Phys. 70:43–50; 2008.
7. Radiation Therapy Oncology Group. RTOG Breast Cancer Contouring Atlas.Available at: http://www.rtog.org/CoreLab/ContouringAtlases.aspx.
8. Chui, C.S.; Hong, L.; McCormick, B. Intensity-modulated radiotherapy techniquefor three-field breast treatment. Int. J. Radiat. Oncol. Biol. Phys. 62:1217–23; 2005.
9. Burman, C.; Chui, C.S.; Kutcher, G.; et al. Planning, delivery, and qualityassurance of intensity-modulated radiotherapy using dynamic multileaf colli-mator: a strategy for large-scale implementation for the treatment of carci-noma of the prostate. Int. J. Radiat. Oncol. Biol. Phys. 39:863–73; 1997.
10. Chui, C.S.; LoSasso, T.; Spirou, S. Dose calculation for photon beams withintensity modulation generated by dynamic jaw or multileaf collimations. Med.Phys. 21:1237–44; 1994.
11. Mohan, R.; Barest, G.; Brewster, L.J.; et al. A comprehensive three-dimensionalradiation treatment planning system. Int. J. Radiat. Oncol. Biol. Phys. 15:481–95;1988.
12. Spirou, S.V.; Chui, C.S. Generation of arbitrary intensity profiles by dynamicjaws or multileaf collimators. Med. Phys. 21:1031–41; 1994.
13. Spirou, S.V.; Chui, C.S. A gradient inverse planning algorithmwith dose-volumeconstraints. Med. Phys. 25:321–33; 1998.
14. Damast, S.; Beal, K.; Ballangrud, A.; et al. Do metallic ports in tissue expandersaffect postmastectomy radiation delivery? Int. J. Radiat. Oncol. Biol. Phys.66:305–10; 2006.
15. Tuttle, T.M.; Habermann, E.B.; Grund, E.H.; et al. Increasing use of contralateralprophylactic mastectomy for breast cancer patients: a trend toward moreaggressive surgical treatment. J. Clin. Oncol. 25:5203–9; 2007.
16. Cordeiro, P.G.; McCarthy, C.M. A single surgeon's 12-year experience with tissueexpander/implant breast reconstruction: part II. An analysis of long-termcomplications, aesthetic outcomes, and patient satisfaction. Plast. Reconstr.Surg. 118:832–9; 2006.
17. Chen, R.C.; Lin, N.U.; Golshan, M.; et al. Internal mammary nodes in breastcancer: diagnosis and implications for patient management—a systematicreview. J. Clin. Oncol. 26:4981–9; 2008.