Embed Size (px)
Citation preview
Biliary Atresia - Advances in Etiology
and Early Diagnosis
Ronald J. Sokol, MD, FAASLD
Pediatric GI, Hepatology, Nutrition
Digestive Health Institute
Children’s Hospital Colorado
University of Colorado School of Medicine

Disclosure
• Consultant for Retrophin, Shire, Alexion and Albireo
• Grant support from NCATS and NIDDK of NIH, Alpha
One Foundation, Cystic Fibrosis Foundation

Objectives
• Biliary atresia – epidemiology and
endotypes
• Etiology & Pathogenesis
• Early Diagnosis and Screening

Biliary Atresia
• Most frequent and important liver disease causing obstructive
jaundice in 1st 3 mo.
• 1:8,000 (Asia) to 1:18,000 live births (Europe)
– U.S. ~ 1:13,000 rural = urban
– 300-400 new cases per year in U.S., 8-12 in Israel
• More common in girls, Asians, African-Americans, preterm
infants
• >40% of all liver transplants in children
• ~ 200 per year in U.S.

Illustration courtesy of
Robert E. Kramer, MD
BILIARY ATRESIA
Inflammatory
Fibrosing
Obstruction
Extrahepatic BD
First 3 months
Intrahepatic BDs

Phenotypes of Biliary Atresia
1. BASM
Polysplenia or Asplenia -
laterality defects
(situs, malrotation, midline
liver, interrupted IVC)
• Frequency: 8-12%, 3-4% in
Asia
• Association: IDM in UK
• Morphogenesis defect
2. BA with Multiple
Malformations
• At least one other major
congenital malformation,
not BASM
• Frequency: 10%
• Morphogenesis defect
Schwarz et al. Hepatology 2013

Phenotypes of Biliary Atresia
3. Isolated BA
• No other congenital anomalies
• Frequency: 75-80%
• BD formed but then was damaged by insult pre- or
postnatal
• ? Viral, toxin, immune/autoimmune, vascular etiology
or genetic
• Outcome better than BASM

Phenotypes of Biliary Atresia
4. Cystic BA
• Choledochal cyst (usually
hilar) + BA
• Frequency: 5-10%
• Prenatal identification
• Outcome: ? Improved
• CDC may lead to delayed
IOC and HPE
5. CMV-associated BA
CMV + IgM Ab
• Frequency: ~10%
• At presentation: older, higher
bilirubin, AST and APRI and
↑inflammation and fibrosis
on liver bx
• Poorer outcome (normal bili
post HPE in 15% vs. 52%)
J Pediatr Surg 50 (2015) 1739–1745

CMV-associated BA
• CMV not detected in
liver
• Brindley et al. did
show specific T-cell
reactivity to CMV in
50% BA patients
Hepatology 2012;55:1130–8
• ? Any role for
ganciclovir treatment

Candidate Etiologies of Biliary Atresia
• Defective morphogenesis (embryonic)
• Laterality sequence genes, others
• PKD1L1 Gene Variants in BASM
• Infectious
• Immune or autoimmune
• Toxin - ? Biliatresone-like substance
• Vascular

New Paradigm for BA Pathogenesis
Bezerra et al., NIH Workshop 2017, Hepatology 2018
Jaundice
Acholic Stools

New Paradigm for BA Pathogenesis
Bezerra et al., NIH Workshop 2017, Hepatology 2018

New Paradigm for BA Pathogenesis
Bezerra et al., NIH Workshop 2017, Hepatology 2018

New Paradigm for BA Pathogenesis
Bezerra et al., NIH Workshop 2017, Hepatology 2018

Genes: PKD1L1 and Biliary Atresia
• WES on 58 BASM trios (pt, MOC, FOC) –
from NIDDK-supported ChiLDReN
• 2,017 genes - ciliary structure or function
and putative BA susceptibility loci
• 5 subjects – rare, potentially deleterious homozygous, compound
heterozygous, or heterozygous missense variants in PKD1L1
• PKD1L1 interacts with PKD2 - involved in left-right embryonic
patterning, is present and functions in cholangiocyte cilium
• PKD1L1 – candidate gene causing BASM
Berauer J-P et al. Hepatology 2019

PKD1L1 IHC Expression in Bile Ducts
A. BA with
PKD1L1
variants D. ALGS
BD Paucity
C. Control
Livers
E-G. Normal
Infant Liver
H and E,
CK7,
PKD1L1

PKD1L1 IHC Expression in Bile Ducts
A. BA with
PKD1L1
variants D. ALGS
BD Paucity
C. Control
Livers
E-G. Normal
Infant Liver
H and E,
CK7,
PKD1L1

PKD1L1 IHC Expression in Bile Ducts
A. BA with
PKD1L1
variants D. ALGS
BD Paucity
C. Control
Livers
E-G. Normal
Infant Liver
H and E,
CK7,
PKD1L1

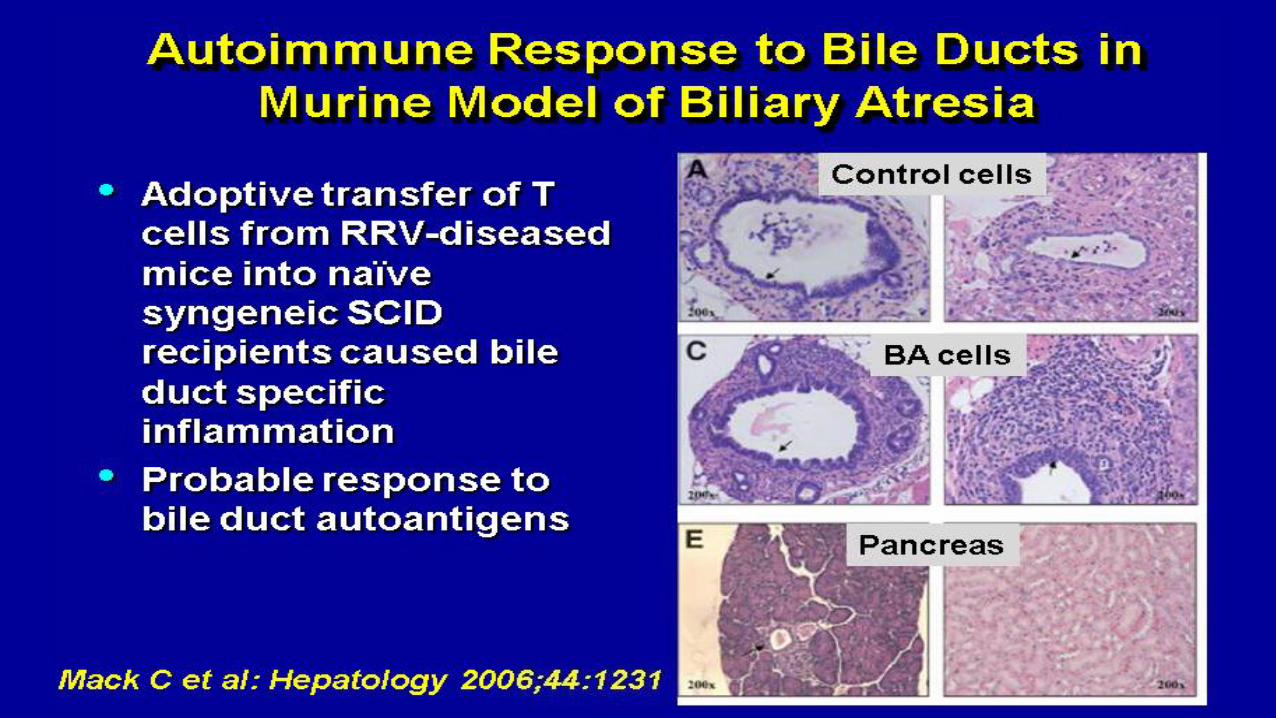
Infectious Etiology of Biliary Atresia
• Main candidate Viruses
– Rotavirus
– Reovirus
– Cytomegalovirus (CMV)
• Mouse models – perinatal infection causes bile
duct injury and obstruction
• Human data – association of evidence of
increased infection rates with BA vs. controls

Courtesy of Cara Mack



Asai, A. et al. Nat. Rev. Gastroenterol. Hepatol. 12, 342–352 (2015)
Viral-Induced Pathogenesis of Biliary Atresia
Innate and Adaptive
Immunity Pathways

Toxin: Biliatresone – Toxic Cholangitis & BA
• Outbreaks of BA in lambs during droughts in Australia
• R. Wells team harvested plants in New South Wales during
2007-2008 drought
• Dysphania – sequential fractionation of the plants, guided by
a zebrafish bioassay
• Isolated a previously unknown toxin that causes selective
extrahepatic biliary tree atresia in zebrafish
Lorent K et al., Science Transl Med 2015;7:286ra67

Lorent K et al., Science Transl Med 2015;7:286ra67
Zebrafish Assay

Inflammatory vs. Fibrotic Endotypes
• Gene expression profiling of liver done on BA infants
• Identified two transcriptional profiles (endotypes)
correlating with liver biopsy findings: inflammatory vs.
fibrotic
• Different outcomes (SNL) for the two endotypes
• Could this guide treatment after Kasai HPE?
• For example, are there subtypes that might respond to anti-
inflammatory treatments (precision Rx)?
Moyer K, et al. Genome Medicine 2010; 2: 33

Transcriptional Endotypes of BA
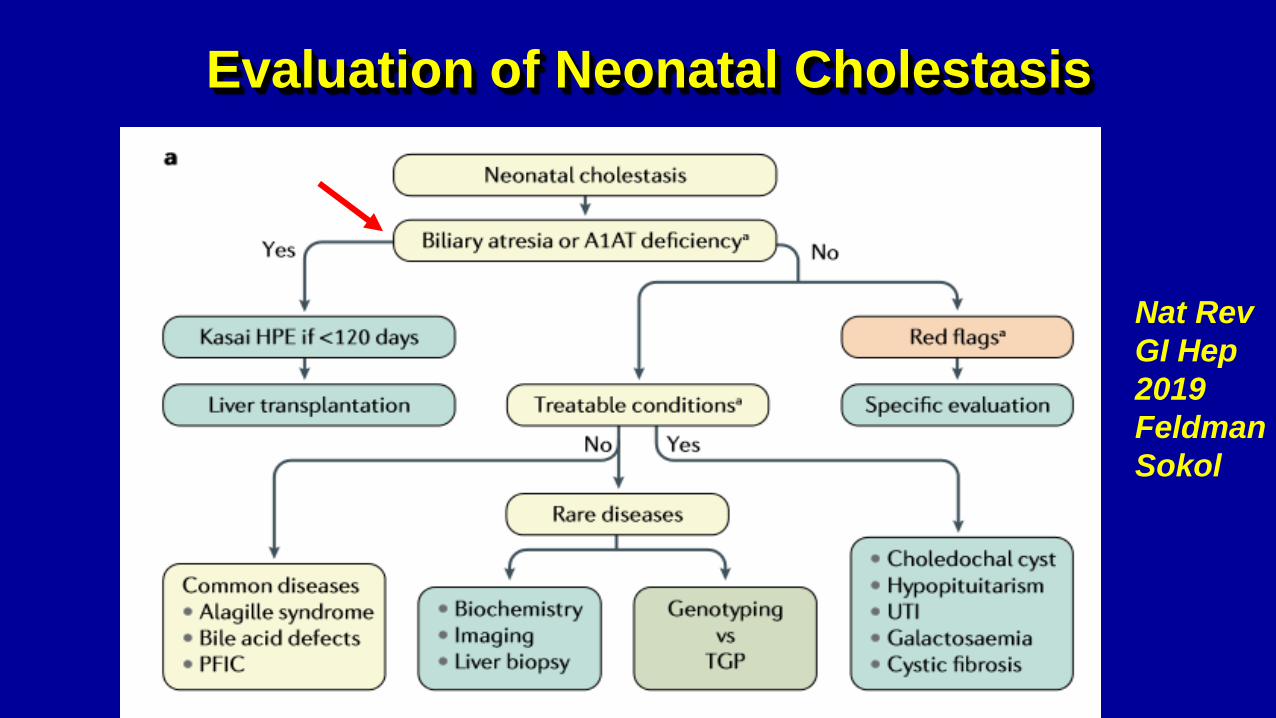
Evaluation of Neonatal Cholestasis
Nat Rev
GI Hep
2019
Feldman
Sokol

Diagnostic Tests for Biliary Atresia
• Liver Blood tests
• Exclude other diseases
• Ultrasonography
• Scintigraphy
• Duodenal bile collection
• Liver biopsy
• Cholangiography
intraoperative, ERCP, transhepatic
cholecystography, MRCP

Diagnostic Tests for Biliary Atresia
• Liver Blood tests
• Exclude other diseases
• Ultrasonography
• Scintigraphy
• Duodenal bile collection
• Liver biopsy
• Cholangiography
intraoperative, ERCP, transhepatic
cholecystography, MRCP
A1AT
ALGS
CF

RRV
Mouse
ModelLiver - BA
patients
Liver Expression of MMP7 in BA
J Surg Res. 2010 April ; 159(2):
611–617
Modern Pathology (2005) 18,
941–950

Serum MMP7 Elevated in BA
AUC ROC = 0.96
J Pediatr 2019; 208: 30-37

MMP7 Clinical Test Available

Treatment & Outcomes of Biliary
Atresia
• Progressive liver injury with cirrhosis in 95% of adult biliary
atresia patients with native liver
Lykavieris et al., Hepatology, Vol 41, 2005
• Kasai portoenterostomy: removal of occluded
extrahepatic bile duct and Roux-en-Y jejunum
to porta hepatis
• Succesful bile drainage in 30-70% cases
• 70-80% of children with biliary atresia will
require liver transplant in childhood

< 31 days : 99 patients
31 to 60 days : 435 patients
61 to 90 days: 361 patients
> 90 days : 132 patients
1027 patients 1986-2009
P<0.0001
Age (years)
Age at Kasai operation:
0
,2
,4
,6
,8
1
0 5 10 15 20 25
J Hepatol 2013; 58(6):1209-17
Survival with Native Liver & Age at Kasai
Operation - France

Goal for Timing of BA Diagnosis
• Goal:
– Establish diagnosis of BA before 30-45 days of life
– Portoenterostomy prior to 30-45 days of life
• Education efforts over past 30 years have failed to
change average age at Dx
– 65-70 days in ChiLDReN research network (15 sites)
Wang KS, et al. Newborn Screening for Biliary Atresia. Pediatrics 2015:136:e1663

No Change in Average Age at Kasai France 743 BA patients – 1986-2002
Serdinet et al, Pediatrics 2009;123:1280
We need to move the needle!!!!
HOW?
Stool Color Card
Neonatal Conjugated Bilirubin Level

Acholic Stools


Age at HPE (Kasai)
74% have Kasai surgery before 60 days of age
Better Survival with Native Liver
Less need for Liver transplantation
Would Stool Color Card Screening Work
in Israel?
• BA is 3x more prevalent in Taiwan – knowledge greater
• A 1-month WCC visit (for the HBV vaccine) is required in
Taiwan, not in U.S.
• What would be adherence?
• Would it be cost-effective? YES
• Needs to be piloted
• PoopMD App may help standardize “acholic” Mogul DB, PLoS One.
2015 Jul 29;10(7):e0132270

How about using Serum
Conjugated Bilirubin as a
Newborn Screen?

Newborn Conjugated Bilirubin
as Screen for BA
• Texas Children’s Hospital 2007-2010
• Serum bili (total & direct/conjug) measured on every newborn in some
hospitals in Houston, TX
• 73 BA pts. & 75 normal newborn controls (300 values)
• Look back at serum bilirubin levels and % conjugated or direct
in 1st 96 hours
• 34 of 73 BA patients had bilirubin levels available (27 direct and
7 conjugated)
Harpavat S et al. Pediatrics 2011; e1428

Total and Direct Bilirubin Levels in 1st 48
hours of Life
J Pediatr 2011

Direct Bilirubin 1st 96 hours in BA
J Pediatr 2011
20%
BA Patients

DB/TB Ratio at 24-48 hrs.
J Pediatr 2011
20%
79% BA
< 20%
BA Patients

DB/TB Ratio at 24-48 hrs.
J Pediatr 2011
20%
> 99% Controls
< 10% DB/TB
10%
BA Patients

Questions Raised
• Why were so many BA infants with elevated Direct Bilirubin
as newborn not f/u’d?
– perhaps the DB:TB felt to be normal
• Are we using the wrong cholestasis cut-off for DB/TB ratio in
first 4 days of life?
– Should it be Direct > 10% of Total Bilirubin (not 20%)
• Should all infants get direct as well as total bilirubin?
– “Newborn” screening for cholestasis

?

Take Home Points
• Etiology of Biliary Atresia still not clear, however
genomics technology will lead to discovery of new
genetic causes for some cases
• Etiology of bulk of BA cases (isolated) still not clear
• Diagnosis needs to be made before 30-45 days for best
outcomes from Kasai HPE
• Screening will be only effective way to earlier diagnosis

Thank You









![Ultrasonographic findings of type IIIa biliary atresiabiliary atresia. Further, there have been only a few reports on the US findings of biliary atresia based on its types [33,34]](https://img.pdfslide.net/doc/110x75/60a90a6926e7a533947d7637/ultrasonographic-findings-of-type-iiia-biliary-atresia-biliary-atresia-further.jpg)



















