Embed Size (px)
Citation preview

Biochemical investigation ofAbnormal Growth
Tina YenMelbourne Pathology/ Royal Children’s Hospital
CPC Adelaide [email protected]

GH
1. Growth hormone (GH) is synthesized bysomatotrope cells in ant pituitary. GH =somatotropin.
2. GH release:
i. Triggered by GHRH (GH releasinghormone; somatocrinin)
ii. Triggered by GHS (or GHsecretagogue or ghrelin; not shown).
iii. Inhibited by somatostatin.
iv. Octreotide (Sandostatin), anoctapeptide that mimics naturalsomatostatin pharmacologically.
Physiology of Growth Hormone

As somatostatin increased,the circulating of GHdecreases.
1. somatostatin receptor ligands (SRLs)Octreotide (Sandostatin) andLanreotide, both as long-actinginjection. Mimic the action ofsomatostatin.
3. If GH and prolactin elevatedpatient is given dopamine agonists(cabergoline and bromocriptine).
2. GH receptorantagonistpegvisomant.

1. GH binds to growth hormone bindingprotein (GHBP).
2. GH stimulates insulin-like growthfactor-1 (IGF-1) secretion by the liver.
3. IGF-1 (= somatomedin-C) mediatespart of the action of GH.
3. IGF-1 binds to IGFBP (IGF-bindingproteins), the most common is IGFBP3.
Physiology of IGF-1

GH and IGF-1Growth
hormoneIGF-1
Official name Somatotropin Somatomedin-C
Site of production Ant pituitary Liver
Binding proteins GHBP IGFBP3
Binding to BP loosely tightly
Target tissues Liver Bone, other tissues
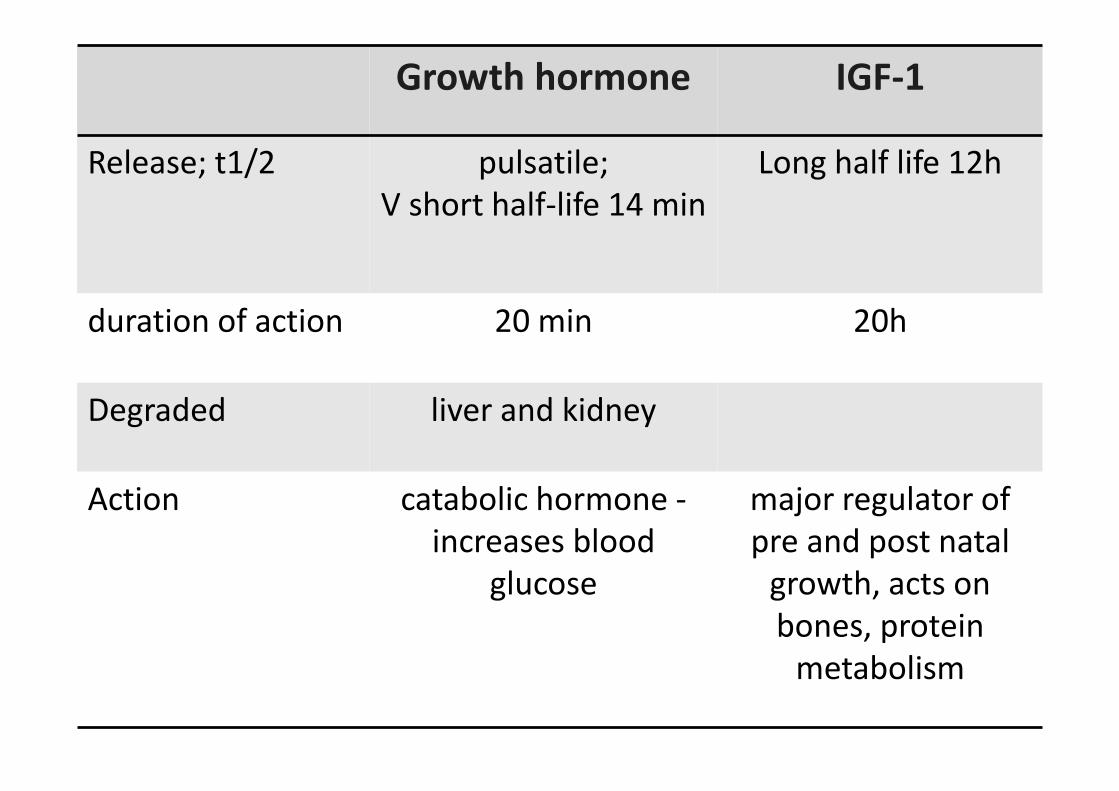
Growth hormone IGF-1
Release; t1/2 pulsatile;V short half-life 14 min
Long half life 12h
duration of action 20 min 20h
Degraded liver and kidney
Action catabolic hormone -increases blood
glucose
major regulator ofpre and post natal
growth, acts onbones, protein
metabolism
Characteristics of IGF1• IGF1 executes some of the actions of GH• 75% of circulating IGF1 is hepatocyte origin. Remainder is
autocrine or paracrine

Physiological regulators of GHSecretion
Stimuated by1. Hypoglycemia2. Fasting3. Starvation4. Exercise5. Stress and trauma6. Sepsis7. Initial stages of sleep
Inhibited by1. Hyperglycemia2. Increase in free fatty
acids in blood3. Later stages of sleep.
Insulin stimulates GH Glucose suppresses GH

Growth action of GH and IGF-1
• Epiphyseal plates of longbones ie. longitudinalbone growth
• After the epiphysealfusion bone grows inthickness throughoutthe life
• jaw and the skull bonesbecome thicker underthe influence of GH

GH metabolic role• include protein synthesis, lipolysis and lipid
oxidation, water-, phosphate- and sodium retentionand acts as an insulin antagonist.

Laboratory Tests
• Growth hormone tests for excess– Random GH, IGF-1– OGTT with GH
• Growth hormone tests for deficiency– IGF-1 and IGFBP-3– GH Provocation tests

ACROMEGALY



Clinical presentation• acral and facial
changes• hyperhidrosis
(perspiration)• headaches• paresthesia• sexual dysfunction• HT• goiter• visual field defects
“.. RPA Where Are They Now ..”Season 1; Episode 8


Famous acromegalics• Richard Kiel; 1939 – 2014. • Rondo Hatton 1894 –1946

Pituitary gigantism
“ growth hormone excess is the single condition whichaccounts for nearly all cases of pathologic extreme height…”

Acromegaly - causes
• Pituitary adenoma 99%
• Excess secretion of GHRH byhypothalamic tumour
• Ectopic secretion of GH or GHRH by nonendocrine tumours
1%

Prevalence of acromegaly• annual incidence ~ 5 cases per 1 million pop per
year.• In Australia ~ 40 – 60 people are affected per million
(so ~ 1000 patients total)• Tumours slow growing; patients usually > 50 years at
presentation.• Long standing GH hypersecretion (usually been
present for ~ 10 years)• Macroadenoma 70%, microadenoma 30%• 60% secrete GH only; 25% secrete GH- and prolactin

Lab testing for acromegaly
• Diagnosis of acromegaly requires clinical andbiochemical evidence
• Elevated serum IGF-I– serum IGF-I levels are highly correlated to clinical
features of acromegaly and with 24-h mean GH.• Acromegaly in the absence of high IGF-I levels
is extremely rare (very few false negatives).• GTT with GH – confirmatory testing
A random serum IGF-I used to screen for GH excess

2014
Free from Endocrine Society US websiteFree on JCEM website

Melmed S (2006). Acromegaly. NEJM 355; 2558-73.
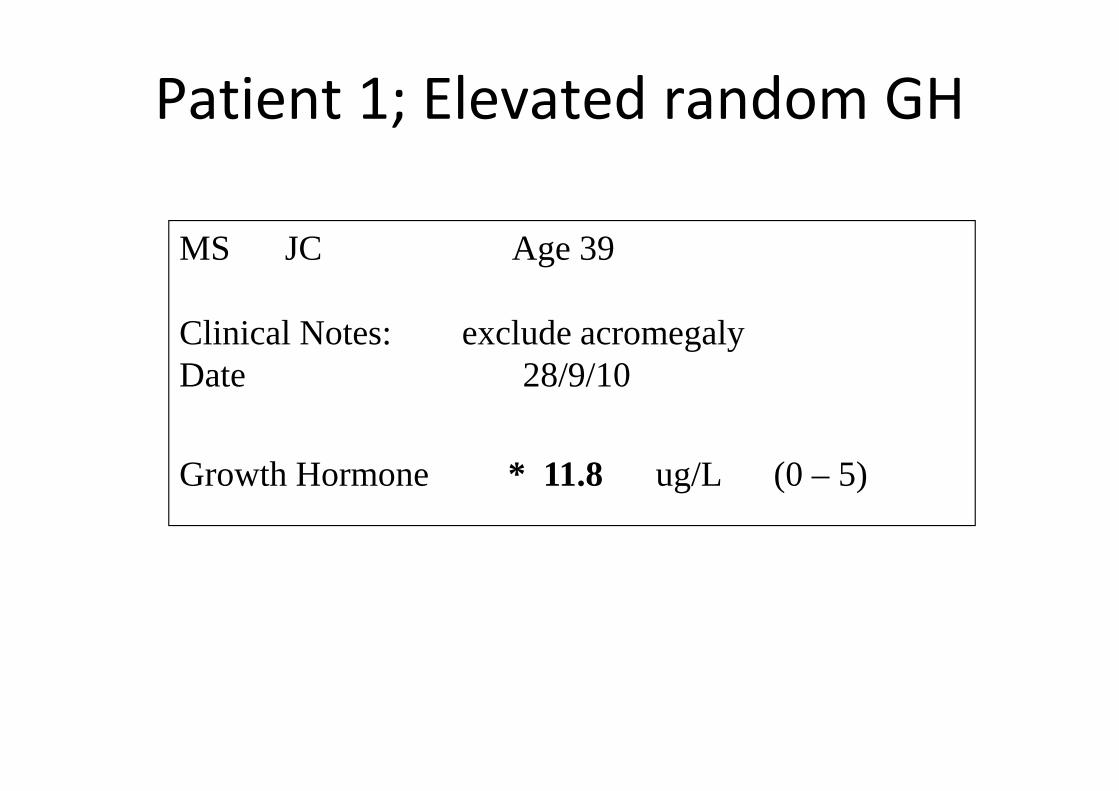
Patient 1; Elevated random GH
MS JC Age 39
Clinical Notes: exclude acromegalyDate 28/9/10
Growth Hormone * 11.8 ug/L (0 – 5)

Limitations of random GH• pulsatile release of GH by the pituitary• highest levels during sleep coordinated with sleep
stages.• Normal subjects - very low levels of GH during the
day.– 70-80% of normal GH results are < 1 ug/L.– GH pulse peaks can reach 20-40 ug/L.
• In acromegaly, there is increased pulse frequencyand more frequent high levels of GH. However theGH range is still 1 ug/L - >100 ug/L.

Disadvantages of random GH• Half life short 14 minutes (compared to IGF-1, 12h)• Random levels show great variability.• Normal GH difficult to define due to pulses.• False positive (elevated GH).
– A high GH value may occur in normal subject if samplecoincides with a GH pulse.
– GH increased in renal disease, cirrhosis, and malnutrition,and during physical or emotional stress.
• False negative (low GH)– Some patients with clinical acromegaly and low GH
• Diagnostic utility– overlap in GH values (healthy and acromegalic patients)
High GH in non-acro
Low GH in Acromegaly

MS JC Age 39
Clinical Notes: exclude acromegalyDate 28/9/10
IGF-1 26 nmol/L (16 - 64)
IGF-1 normal. Therefore not acromegaly.

MS JC Age 39
Clinical Notes: exclude acromegalyDate 28/9/10
IGF-1 26 nmol/L (16 - 64)
… 1.1 We recommend measurement of IGF-1 levels in patients with typicalclinical manifestations of acromegaly, especially those with acral and facialfeatures… 1.4 We recommend against relying on the use of random (serum) GH levelsto diagnose acromegaly…
Endocrine Society 2014
GH during OGTT
• Give 75 g of oral glucose; samples at 0, 30, 60,90, and 120 min for glucose and GH levels.
• An inability to suppress GH secretion to < 1μg/L during 2 hours after an oral glucose loadis diagnostic of acromegaly.
… 1.5 In patients with elevated or equivocal serum IGF-1 levels we recommendconfirmation of the diagnosis by finding lack of suppression of GH to 1ug/Lfollowing documented hyperglycemia during an oral glucose load.
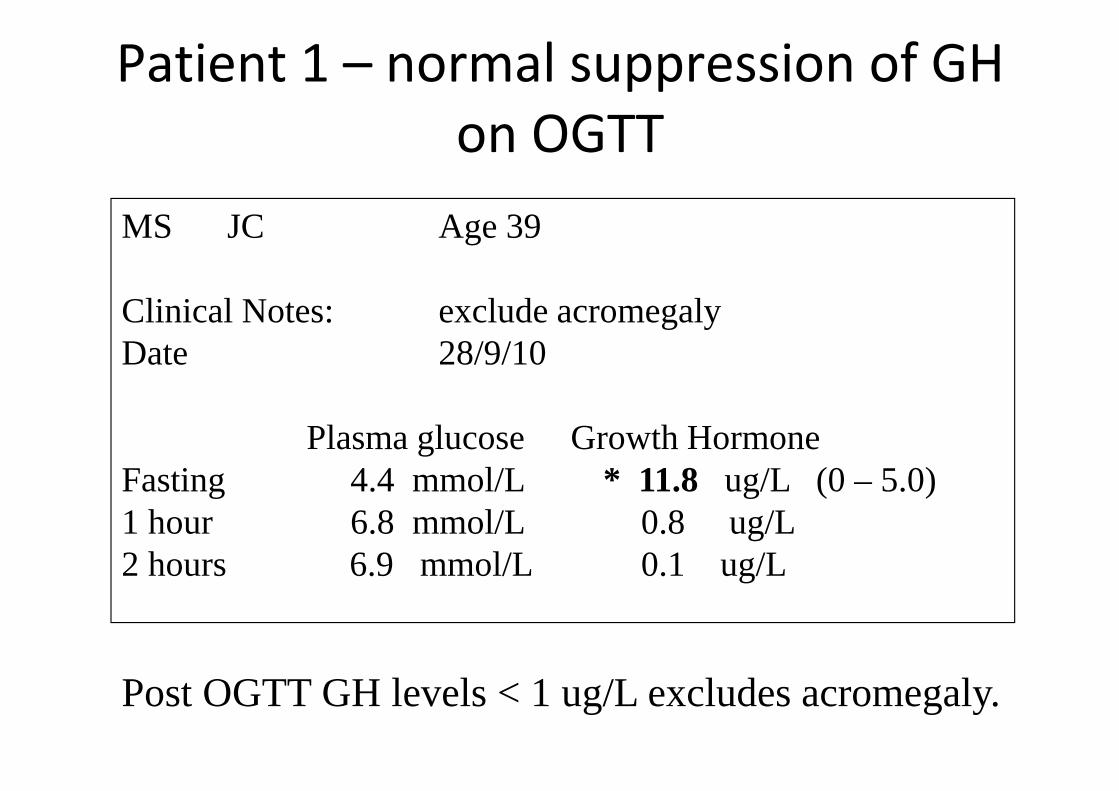
Patient 1 – normal suppression of GHon OGTT
MS JC Age 39
Clinical Notes: exclude acromegalyDate 28/9/10
Plasma glucose Growth HormoneFasting 4.4 mmol/L * 11.8 ug/L (0 – 5.0)1 hour 6.8 mmol/L 0.8 ug/L2 hours 6.9 mmol/L 0.1 ug/L
Post OGTT GH levels < 1 ug/L excludes acromegaly.

Patient 2 – failure to suppress duringOGTT
MS HM Age 45
Clinical Notes: ? acromegalyDate 9/8/10
Plasma glucose Growth HormoneFasting 4.8 mmol/L * 10.3 ug/L (0 – 5.0)1 hour 6.0 mmol/L 6.4 ug/L2 hours 6.8 mmol/L 7.1 ug/L
Failure of GH to be suppressed – consistent withacromegaly

MS HM Age 39
Clinical Notes: exclude acromegalyDate 31/8/10
IGF-1 * 84 nmol/L (12 - 47)
IGF-1 elevated

Post OGTT GH• Achieving a nadir serum GH < 1 ug/L in 2h 75 g OGTT
excludes the diagnosis. Must include glucose levelsto verify that hyperglycemia has been achieved.
• Possible reasons for patients with “suppressed postglucose load GH” and “high random GH”?
• “Mild GH hypersecretion” – patient who additionallyhas random GH still < 1 ug/L and mild increasedserum IGF-1, and surgically confirmed GH-producingpit tumor.
• Older patients, female, obesity and elevated BMImay show abnormal post-glucose GH suppression (?need normal ranges for these variables).

Nadir GH – appropriate cut off?
• A nadir serum GH < 0.4 ug/L after an oralglucose load has been considered forestablishing the diagnosis (rather than 1 ug/L).
• However not in guidelines at present, due to– assay precision at low end– GH immunoassays not uniformly standardised– poor reproducibility between laboratories

GH IMMUNOASSAYS

An optimal GH assay should have:• 1. Calibration to the new 2nd international standard
98/574 for somatotropin.• rec DNA–derived hGH (IS) 98/574) used by
manufacturers to standardise the GH assay.• Information by manufacturer on the antibody
specificity to GH isoforms (mainly monomeric 22 kDaisoform).
• When the calibrators were standardized to 98/574(which contains 96% 22-kDa GH) there was a shift tolower GH values, due to preferential detection of 22 k-Da isoform.

• 2. Sensitivity of 0.05 g/L at inter-assay CV of 20%.• Reproducibility near the lower ref limit is critical
because baseline (non pulse GH is very low) andglucose suppressed GH used for Dx and monitoringof acromegaly.

• 3. There is no reference measurement procedure forGH so EQA demonstration of equivalent resultsamong a group of routine methods for a panel ofpatient samples will be necessary.
• Ideally large pools of longitudinally available QC serawith documented commutability, that coverconcentrations relevant to clinically cutoff points,need to be available and distributed acrosslaboratories for comparative studies.

• 4. laboratory report of GH in mass units (i.e.,micrograms per liter).
• 5. other issues:– % assay cross-reactivity with 20-kDa GH,
placental GH, and therapeutic GH analogs– GHBP interference– Stability over time


AACB harmonisation GH – step 1• Diagnosis of GH deficiency and
acromegaly and funding for GHtreatment depend on GH levels andconsensus guidelines (ie definedclinical decision points).
• variation between GH assays withsame sample
• Despite recommendation to useug/L, 60% labs in Endo QAP stillreport in mU/L

Step 1 to GH harmonisation
Step 2 to GH harmonisation• Between method differences in hGH• agreement to using correction factors to harmonise
hGH (agreed “in principle”). Not ideal situation.However this is important if internationalharmonisation not imminent.
• Differences in reference intervals and decisionpoints
• If assays not harmonised – consider publishingplatform specific ref intervals/clinical decision points.
Currently your GH assay should be validated with a normal range forsuppressed GH levels after oral glucose load (OGTT)

IGF-1 IMMUNOASSAYS

IGF-1 is critical todiagnosis
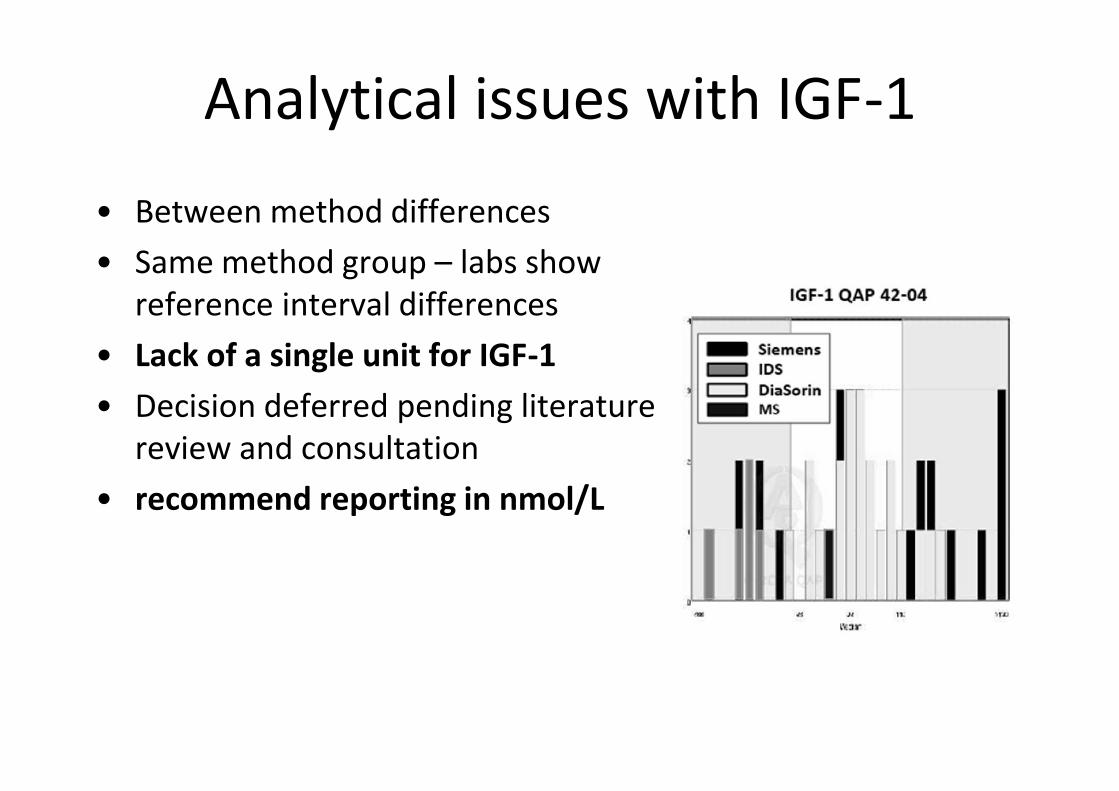
Analytical issues with IGF-1• Between method differences• Same method group – labs show
reference interval differences• Lack of a single unit for IGF-1• Decision deferred pending literature
review and consultation• recommend reporting in nmol/L


GROWTH FAILURE
“DWARFISM”

Disorders of growth in children
• growth assessment inpaediatric practice
• Diseases that specificallyaffect growth axis
• Disease states thatcauses weight loss, eg.malnutrition, cancer,immunosuppression.

GH deficiency (GHD)
• Newborn GHD• Infant/Congenital GHD• Childhood GHD• Delayed puberty• Transition (Adolescent - Adult)

GH deficiency in the newborn
• Severe congenital GH deficiency (newborn) is rare (1:50 000 newborns).
• Causes life-threatening hypoglycaemia in the firstweek of life.
• Diagnostic criteria DIFFER to that used for classicalchildhood onset GHD (ages 4 – 8y) where typicalpresentation is growth failure, reduced growthvelocity, delayed bone age, and low serum IGF1.

Newborn GH
• 1. birth weight, length, may be normal (growthparameters may not yet have been affected).
• 2. Baseline serum GH levels are higher in first weekof life compared to children (neonatal hyper-somatotrophism)
• 3. Dynamic function testing are not approved inneonates.
• 4. Rapid diagnosis required Rx with GHsupplementation.

Random GH – limited utility
• Random results not used for Dx• Undetectable GH strongly suggestive (but not
diagnostic).• Main use is in excluding GH deficiency as
cause of neonatal hypoglycaemia.
GH level > 20 mU/L during hypoglycaemia excludes GH deficiency.

GH @ Day 3
• Historically random GH >20 mU/L excludesneonatal GHD.
• 2010 – a cut-off of 7 ug/Lfor single GHmeasurement has 100%sensitivity and 98%specificity for GHD.
• RI 7.0 – 39.4 ug/L
J Clin Endocrinol Metab 95: 2219–2226, 2010

What happens after week 1?
• GH levels in healthy newborns decline fromweek to week.
• Neonatal multiple pituitary deficiency may bediagnosed after 4 weeks of age suggest useof newborn screening card for GH assessment.

References• Bidlingmaier and Freda (2010). Measurement of human
growth hormone by immunoassays: Current status, unsolvedproblems and clinical consequences. Growth Hormone & IGFResearch 20 (2010) 19–25.
• Arafat AM et al (2008). Growth Hormone response during oralglucose tolerance test. JCEM 93: 1254 – 1262.
• Freda P (2004). Acromegaly; diagnostic pitfalls. TheEndorcinologist 14: 277 – 287.
• Bidlingmaier M (2009). Pitfalls of Insulin-like Growth Factor 1.Horm Res; 71(suppl 1):30–33

Consensus Statement on the Standardization andEvaluation of Growth Hormone and Insulin-like
Growth Factor AssaysDavid R. Clemmons,1* on behalf of the conference participants
Growth hormone (GH) and insulin-like growth factorI (IGF-I) measurements are widely used in the diagno-sis of disorders of GH secretion, evaluation of childrenwith short stature from multiple causes, managementof disorders that lead to nutritional insufficiency orcatabolism, and monitoring both GH and IGF-I re-placement therapy. Therefore, there is an ongoing needfor accurate and precise measurements of these 2 pep-tide hormones. Representatives of the Growth Hor-mone Research Society, the IGF Society, and the IFCCconvened an international workshop to review assaystandardization, requirements for improving assaycomparability, variables that affect assay interpreta-tion, technical factors affecting assay performance, as-say validation criteria, and the development and use ofnormative data. Special attention was given to preana-lytical conditions, the use of international commutablereference standards, antibody specificity, matrix re-quirements, QC analysis, and interference by bindingproteins. Recommendations for each of these variableswere made for measurements of each peptide. Addi-tionally, specific criteria for IGF-I were recommendedfor age ranges of normative data, consideration of Tan-ner staging, and consideration of the effect of bodymass index. The consensus statement concludes thatmajor improvements are necessary in the areas of assayperformance and comparability. This group recom-mends that a commutable standard for each assay beimplemented for worldwide use and that its recom-mendations be applied to accomplish the task of pro-viding reliable and clinically useful results.© 2010 American Association for Clinical Chemistry
Measurement of circulating growth hormone (GH)2
and insulin-like growth factor I (IGF-I) concentrationsrepresents a cornerstone of the diagnosis and monitor-ing of pituitary and other medical disorders, which in-
clude such GH-related disorders as acromegaly andGH deficiency, as well as numerous metabolic disor-ders (1–5 ).
Considerable differences exist between the cur-rently available assays with respect to the results of GHand IGF-I measurements (6 –9 ). These differences arelargely due to heterogeneity in assay characteristics.Harmonization and comparability of GH and IGF-Iassays are required to provide transparent and usefulguidelines for the management of disorders of the GH–IGF-I axis (10 ). The Growth Hormone Research Soci-ety, in collaboration with the IFCC, the InternationalSociety for IGF Research, and the Pituitary Society, or-ganized an expert workshop to define criteria, strate-gies, and ways to implement harmonization of GH andIGF-I assays. This document reflects the recommenda-tions of that workshop.
Current Obstacles to GH and IGF-I AssayStandardization
To address the fundamental obstacles to assay stan-dardization requires an understanding of the proper-ties and limitations inherent in immunoassays. Thelack of GH and IGF-I assay standardization has led tomajor differences in the values of hormone concentra-tions obtained with different assays (6, 7 ). An impor-tant contributor is the use of different calibrator mate-rials (11 ). Currently, not all GH assays are calibrated toa common international reference preparation (7 ).Furthermore, the available standard for IGF-I assays,87/518 (available from the WHO), is recognized ashaving an incorrectly assigned concentration (12 ).Heterogeneous analytes pose an additional problem.Circulating GH, for example, consists of various forms,including monomers, dimers, and other posttransla-tionally modified products, the detection of which var-ies among assays (13 ). Therefore, an individual GH or
1 Department of Medicine, University of North Carolina School of Medicine,Chapel Hill, NC.
* Address correspondence to the author at: CB# 7170, 8025 Burnett Womack,Division of Endocrinology, University of North Carolina, Chapel Hill, NC 27599-7170. Fax 919-966-6025; e-mail [email protected].
Received May 17, 2010; accepted December 14, 2010.Previously published online at DOI: 10.1373/clinchem.2010.1506312 Nonstandard abbreviations: GH, growth hormone; IGF-I, insulin-like growth
factor I; GHBP, GH-binding protein; IGFBP, IGF-binding protein; IS, internationalstandard; NIBSC, National Institute of Biological Standards and Control.
Clinical Chemistry 57:4555–559 (2011) Special Reports
555

IGF-I sample measured by different assays can yieldvery different results, because assays differ with respectto the epitope specificity of the antibodies used andbecause the different types of antibodies vary in theirability to bind to the different molecular forms of GHand IGF-I. The reporting of assay results also varies(14 ). For example, GH assay results have been ex-pressed not only in mass units but also in internationalunits, which have been arbitrarily defined and do nothave a clear relationship to mass. GH measurementsare subject to interference by a number of factors, in-cluding GH-binding protein (GHBP), which corre-sponds to the circulating extracellular domain of theGH receptor (15 ). Similarly, IGF-binding proteins(IGFBPs) may interfere with IGF-I assays (6 ). As withany assay, matrix components can also variably inter-fere with both GH and IGF-I measurements. The ef-fects of these variables on assay results are not alwaysapparent to the assay user.
General Requirements for Improving AssayComparability
The foremost fundamental requirement for improvingthe comparability of GH and IGF-I assay methods is touse a single universally accepted standard for each hor-mone assay. Each GH or IGF-I assay should also specifythe analyte being measured, the specificities of the an-tibodies used, and the assay’s susceptibility to bindingprotein interference. The epitope of the antibodyshould be stated if it is known. Normative data areneeded for each GH and IGF-I assay. Assay compara-bility also requires standardization of preanalyticalconditions, an understanding of matrix properties, im-plementation of appropriate internal QC procedures,and participation in an external QC program.
GH Assay
PREANALYTICAL CONDITIONS
Although some analytes are susceptible to many phys-ical conditions, GH and IGF-I are relatively stable (16 ).Their stability in blood is such that separation of serumfrom blood cells is recommended within 2 h of collec-tion. GH and IGF-I are stable in serum for severalweeks at �20°C. The clinical conditions under whichGH should be sampled during a dynamic test for GHdeficiency or acromegaly will vary with the test and thepatient population being assessed. Performance ofthese dynamic tests should be guided by published pro-tocols (17–19 ).
STANDARDS AND ANTIBODY SPECIFICITY
Discrepancies between GH assays can be reduced if acommon pure standard preparation is used for calibra-
tion (11 ). A new preparation has recently becomeavailable, the Second International Standard for som-atropin (a recombinant DNA– derived human GH, in-ternational standard (IS) 98/574), and is being used bymanufacturers for standardization of GH assays. It isavailable from National Institute of Biological Stan-dards and Control (NIBSC). This material is of highpurity (�96% 22-kDa GH) with desirable characteris-tics (bioactivity, stability, availability, and so forth)(20 ), but a demonstration of its commutability has notyet been published (21 ). In view of the importance ofthe validation of commutability (22 ), publication of apeer-reviewed commutability study is strongly recom-mended. If it is commutable among the various assaymethods with patients’ clinical samples, we recom-mend that all manufacturers adopt this standard toprovide consistency in standardization. IS 98/574 hasbeen assigned a unitage of 1.95 mg per ampoule. Bydefinition, 1 mg equals 3 IU. We recommended thatGH concentrations be reported in mass units.
The ideal assay should use antibodies of high affin-ity and specificity. Assays should be specific for the 22-kDa form of human GH. Reproducibility may be themost critical near the lower limit of the analytical inter-val. Growth hormone is secreted in a pulsatile fashion,and some values can be very low. The ability of glucoseto suppress GH is used in the diagnosis and monitoringof acromegaly; therefore, it is important that assaymanufacturers are able to provide accurate measure-ments at the lower end of the GH assay interval. Pres-ently, we recommend that assays achieve a lower limitof quantification of 0.05 �g/L with a CV of �20%.
MATRIX REQUIREMENTS
The matrix used in calibrators should mimic the prop-erties of nonpathologic human serum as closely as pos-sible; however, that may still leave a residual matrix-related bias requiring compensation in the valueassigned to the calibrator used with a specific assay pro-cedure. Because no reference measurement procedureexists for GH (or IGF-I), the demonstration of equiva-lent results among a group of routine methods for apanel of patient samples will be necessary whenmethod-specific calibrators are used. If such a panel isunavailable, it may be necessary to use serum from an-other species that maintains optimal linearity and re-covery of known quantities of the hormone.
GHBP INTERFERENCE
Each assay should specify its degree of interference byGHBP within its physiological interval (23 ). To inves-tigate this interference requires that samples be spikedwith recombinant GHBP and incubated for at least 12hours to allow formation of the GH/GHBP complexbefore measurement (24 ).
Special Reports
556 Clinical Chemistry 57:4 (2011)

QUALITY CONTROL
Laboratories should use internal QC materials inde-pendent of those provided by the assay manufacturer.All laboratories measuring GH should participate in anaccredited proficiency testing/external quality assess-ment program that uses materials that have beenproved commutable at a national, and ultimately atan international, level. The availability of such a pro-gram at an international level would accelerateharmonization.
When commutable materials are available, we en-courage the IFCC, in collaboration with national col-leges of pathology (including the College of AmericanPathologists), to facilitate the worldwide exchange ofproficiency testing/external quality assessment infor-mation and reports for the sharing of best practices. Adesirable goal is to develop a centralized advisory groupthat will facilitate such sharing at an international level.Best practice for thresholds for variation betweenmethods needs to be established to ensure comparabil-ity of quality. The characterization of each assay mustinclude studies that define the reactivity of each of themajor forms of GH in that assay.
Large pools of longitudinally available QC serawith documented commutability and covering con-centrations relevant to clinically important cutoffpoints, such as those for the diagnosis of GH deficiency,need to be available and distributed across laboratoriesfor the purpose of comparative studies.
PRESENTATION OF ASSAY RESULTS
The laboratory report presented to the clinician shouldgive GH results in mass units (i.e., micrograms per li-ter). Because discrepancies can remain despite theadoption of a uniform standard, potentially because ofdifferences in reagents, some laboratories have consid-ered adopting conversion factors to compare the re-sults of different assays. Such conversion factors do notaccount for all assay differences, however, and their useis discouraged.
COOPERATIVE EFFORTS AND EDUCATION
Implementation of the use of IS 98/574 requires thebringing together of representatives of professional or-ganizations, manufacturers, proficiency-testing pro-viders, and key opinion leaders to endorse this effort.Use of the reference standard can also be encouragedby educational initiatives that will disseminate infor-mation on its use, as well as by the adoption of policiesby journals that require use of the internationally ad-opted standard in GH assays in studies they publish.
Information available in a manufacturer’s assayliterature should specify the following: the identity ofthe reference preparation; calibration information, in-cluding traceability to the international reference stan-
dard; assay cross-reactivity with 20-kDa GH, placentalGH, and therapeutic GH analogs; GHBP interference;limits of quantification; assay performance at the upperand lower limits of the normative reference intervals;and QC data. A manufacturer must communicate tothe laboratories major changes in assay components orperformance that could affect clinical diagnostic ortherapeutic decisions. Laboratories then must commu-nicate this information to clinicians in a timelymanner.
IGF-I Assay
CHARACTERISTICS OF THE IGF-I REFERENCE STANDARD
The IS 02/254 WHO reference standard has recentlybecome available. It is a �97%-pure recombinantstandard and has been well characterized by theNIBSC. IS 02/254 has been analyzed in �20 laborato-ries and has been shown to be bioactive and stable(12, 21, 25 ). If this standard is documented to be com-mutable with patients’ clinical samples among the var-ious assay methods, then journals, societies, and regu-latory authorities should advocate the use of the newstandard to minimize the interassay differences thatarise from the use of different standards. Although theuse of conversion factors is not encouraged, their usewill be necessary during the transition period. Conver-sion factors should be used only within the samereagent set, however, not for conversion of IGF-Iconcentrations between methods. If the standard iscommutable, assays should be recalibrated withthe new standard, and the normative intervalreestablished.
CHARACTERISTICS OF QC SAMPLES
As part of the validation procedure, we recommend theestablishment of a set of reference samples, to be dis-tributed internationally to monitor the concordancebetween assay methods. These reference samples willconsist of human serum pools that contain low, me-dium, and high concentrations of IGF-I and GH. Sam-ples from patients with a variety of conditions in whichIGFBPs can influence IGF-I assay results (e.g., type 1diabetes mellitus, chronic renal failure, cirrhosis, GHdisorders) should be used to directly compare the re-sults of IGF-I measurements obtained with differentassays (6 ). This information should be made availableto end users, as should information regarding assayperformance characteristics and interference byIGFBPs.
THE BIOLOGICAL VARIATION OF IGF-I
Given the 3%–36% within-individual biological im-precision of IGF-I assays (26 ), caution should be exer-cised in the interpretation of a single IGF-I value, par-
GH and IGF-I Assays Special Reports
Clinical Chemistry 57:4 (2011) 557

ticularly if it is close to a reference limit. Assays forsamples that yield borderline results should be re-peated with a separate blood sample. The clinical con-text of the patient needs to be incorporated into theinterpretation of the result. Consideration should begiven to performing other tests, such as dynamic GHstimulation/suppression tests.
VARIABLES THAT AFFECT ASSAY INTERPRETATION
Multiple physiological variables and clinical conditionscan affect the concentrations of IGF-I. Age, pubertalstage, pregnancy, and extremes of body mass index areespecially important and need to be taken into consid-eration when interpreting results. In adults, sex andethnicity are minor contributors to variation in IGF-Iconcentrations. Circadian and meal-related changesdo not appear to affect IGF-I measurements (6 ). Assayvalidation should be undertaken for such conditions astype I diabetes mellitus and chronic renal failure. Spe-cific diseases, such as diabetes, hepatic and renal dis-ease, and nutritional compromise, can affect IGF-Iconcentrations; therefore, caution should be used ininterpreting results for patients with these conditions.Some medications, such as oral estrogen, can also affectIGF-I concentrations (27 ).
TECHNICAL FACTORS AFFECTING ASSAY PERFORMANCE
Protocols for sample collection and handling should beprovided for each assay method. The use of serum isrecommended. The use of anticoagulants in the collec-tion tube will require separate validation. Blood sam-ples should be processed within 2 h to avoid an artifac-tual increase in results.
A major factor affecting assay performance is thepresence of IGFBPs in the sample. An assay that recog-nizes IGF-I without any interference from binding pro-teins would be ideal. In general, IGFBPs interfere withIGF-I detection to produce falsely low values. In prac-tice, this problem is usually managed by the use of areagent that dissociates IGF-I from the IGFBPs, fol-lowed by preventing reassociation of the IGFBPs withIGF-I.
The method for preventing IGFBP interferenceshould be validated and stated for each assay. The cur-rent reference method for eliminating IGFBP interfer-ence is gel chromatography at low pH. All methodsmust demonstrate that IGFBP interference has beensubstantially removed (�95%), and the clinical condi-tions under which residual IGFBPs may still cause in-terference should be stated.
Physicians should be informed of the technicalspecifications of the assay with regard to specific clini-cal conditions. The clinician is also responsible for be-ing aware of any clinical conditions (6 ) that make the
interpretation of results for total serum IGF-Ichallenging.
VALIDATION OF ASSAY PERFORMANCE
The manufacturer should use nonpathologic sera, aswell as sera from patients with GH disorders, type 1diabetes mellitus, chronic renal failure, and cirrhosis,during assay validation, and they should report thisinformation. Assay results should be shown to beequivalent to those obtained after gel chromatographyperformed at low pH. Before processing (as recom-mended by the kit manufacturer), samples should bespiked with a range of IGFBP concentrations (IGFBP-2and IGFBP-3) up to twice the upper limit of the refer-ence interval to ensure the absence of interference.Properly designed studies should document the recov-ery of added highly purified IGF-I (6 ).
NORMATIVE DATA
Normative data should be based on a random selectionof individuals from the background population, andthis population sample should include representationfrom all age groups. Individuals with medical condi-tions (e.g., cirrhosis, poorly controlled diabetes, renalfailure) and taking medications (e.g., estrogen) thatmay affect the outcome are excluded. Normative datashould include the central 95% interval (2.5–97.5 per-centiles) and be reported in mass units and, after ap-propriate transformation for data nonnormality, as SDscores (equivalent to the z score, which represents thenumber of SDs a given result is above or below theage-adjusted mean).
The IGF-I concentration shows the greatestchange during childhood and puberty and thenchanges more slowly with advancing age. For the gen-eration of normative data, the stratification of agegroups should be based on properly designed studiesand statistical analysis of normative data (28 ). Specialconsiderations for children and adolescents should in-clude narrow age ranges (e.g., every 3 years) and Tan-ner stages. Studies must include adequate numbers ofreference individuals in the age intervals with rapidlychanging IGF-I concentrations to ensure reliable esti-mates of reference intervals at these ages (28 ).
Sex-specific IGF-I reference intervals are requiredfor ages between 6 and 18 years (6 ). There is littlechange in IGF-I across the interval of body mass indexvalues from approximately 22 to 37 kg/m2, but signifi-cantly lower IGF-I values have been observed aboveand below these values. This fact should be taken intoaccount when interpreting results (6 ).
GH stimulation and suppression tests are valuabletools in the diagnosis of GH deficiency and excess, re-spectively. As long as different assays give different re-sults for GH, however, it is mandatory to use appropri-
Special Reports
558 Clinical Chemistry 57:4 (2011)

ately validated, assay-specific reference data for thesestudies. These considerations should also include theeffect of body mass index and age. The development ofnormative data for children is recognized to be chal-lenging, for a variety of reasons, and is limited by theability to recruit healthy children into such studies.
Author Contributions: All authors confirmed they have contributed tothe intellectual content of this paper and have met the following 3 re-quirements: (a) significant contributions to the conception and design,acquisition of data, or analysis and interpretation of data; (b) draftingor revising the article for intellectual content; and (c) final approval ofthe published article.
Authors’ Disclosures or Potential Conflicts of Interest: No authorsdeclared any potential conflicts of interest.
Role of Sponsor: The funding organizations played no role in thedesign of study, choice of enrolled patients, review and interpretationof data, or preparation or approval of manuscript.
Acknowledgments: The participants thank Jane Fruchtnicht for herhelp in organizing the conference and Laura Lindsey for her help inpreparing the manuscript. Contributors to the Consensus Statement:Alecia Algeciras-Schimnich, Margherita Banci, Gerhard Baumann,Robert Baxter, Martin Bidlingmaier, Beverly Biller, David E. Bruns, Fe-lipe Casanueva, Phillippe Chanson, Jens Christiansen, Peter Clayton,David Clemmons, Pinchas Cohen, Cheri Deal, Andy Ellis, Robin A.Felder, Pamela Freda, Jan Frystyk, Richard Fulanetto, H. Mario Geysen,Shelia Hanna, Philip Harris, Ken K.Y. Ho, Andrew Hoffman, Jeff Holly,Reiko Horikawa, Gudmundur Johnannsson, Anna-Marie Kappelgaard,Susan Kirshner, David Kleinberg, John Kopchick, Derek LeRoith, SaulMalozowski, Kathy Maugh, A. Wayne Meikle, Shlomo Melmed, PharisMohideen, Clement Olivier, Bernhard Saller, Rudolf Schemer, AkiraShimatsu, Christian Strasburger, Catharine M. Sturgeon, Mario Thevis,Michael Thorner, Peter Trainer, Yi Tsong, Mary Lee Vance, GwenWark, and Ingrid Zegers. We thank James C. Boyd for discussions re-garding the determination of reference intervals and z scores.
References
1. LeRoith D, Yakar S. Mechanisms of disease. Met-abolic effects of growth hormone and insulin-likegrowth factor 1. Nat Clin Pract Endocrinol Metab2007;3:302–10.
2. Clemmons DR. Modifying IGF1 activity: an ap-proach to treat endocrine disorders, atheroscle-rosis and cancer. Nat Rev Drug Discov 2007;6:821–33.
3. Ho KKY, on behalf of the 2007 GH DeficiencyConsensus Workshop participants. Consensusguidelines for the diagnosis and treatment ofadults with GH deficiency II: a statement of theGH Research Society in association with the Eu-ropean Society for Pediatric Endocrinology, Law-son Wilkins Society, European Society of Endocri-nology, Japan Endocrine Society, and EndocrineSociety of Australia. Eur J Endocrinol 2007;157:695–700.
4. Melmed S, Casanueva F, Cavagnini F, Chanson P,Frohman L, Grossman A, et al. Guidelines foracromegaly management. J Clin EndocrinolMetab 2002;87:4054–8.
5. Giustina A, Barkan A, Channson P, Grossman A,Hoffman A, Ghigo E, et al. Guidelines for thetreatment of growth hormone excess and growthhormone deficiency in adults. J Endocrinol Invest2008;31:820–38.
6. Frystyk J, Freda P, Clemmons DR. The currentstatus of IGF-I assays—a 2009 update. GrowthHorm IGF Res 2009;20:8–18.
7. Bidlingmaier M, Freda PU. Measurement of hu-man growth hormone by immunoassays: currentstatus, unsolved problems and clinical conse-quences. Growth Horm IGF Res 2009;20:19–25.
8. Seth J, Ellis A, Al-Sadie R. Serum growth hormonemeasurements in clinical practice: an audit ofperformance from the UK National External Qual-ity Assessment scheme. Horm Res 1999;51:13–9.
9. Morsky P, Tiikkainen U, Ruokonen A, MarkkanenH. Problematic determination of serum growthhormone: experience from external quality assur-ance surveys 1998-2003. Scand J Clin Lab Invest
2005;65:377–86.10. Trainer PJ, Barth J, Sturgeon C, Wieringaon G.
Consensus statement on the standardisation ofGH assays. Eur J Endocrinol 2006;155:1–2.
11. Tanaka T, Tachibana K, Shimatsu A, KatsumataN, Tsushima T, Hizuka N, et al. A nationwideattempt to standardize growth hormone assays.Horm Res 2005;64(Suppl 2):6–11.
12. Quarmby V, Quan C. How much insulin-likegrowth factor (IGF-I) circulates?: impact of stan-dardization on IGF-I assay accuracy. Dev BiolStand 1999;97:111–8.
13. Baumann G. Growth hormone heterogeneity:genes, isohormones, variants, and binding pro-teins. Endocr Rev 1991;12:424–49.
14. Pokrajac A, Wark G, Ellis AR, Wear J, Wieringa JE,Trainer PJ. Variation in GH and IGF-I assays limitsthe applicability of international consensus crite-ria to local practice. Clin Endocrinol (Oxf) 2007;67:65–70.
15. Ebdrup L, Fisker S, Sorensen HH, Ranke MB,Ørskov H. Variety in growth hormone determina-tions due to use of different immunoassays andto the interference of growth hormone-bindingprotein. Horm Res 1999;51:20–6.
16. Derr RL, Cameron SJ, Golden SH. Pre-analyticconsiderations for the proper assessment of hor-mones of the hypothalamic-pituitary axis in epi-demiological research. Eur J Epidemiol 2006;21:217–26.
17. Molitch ME, Clemmons DR, Malozowski S, Mer-riam GR, Shalet SM, Vance ML, Stephens PA.Evaluation and treatment of adult growth hor-mone deficiency: an Endocrine Society ClinicalPractice Guideline. J Clin Endocrinol Metab 2006;91:1621–34.
18. Growth Hormone Research Society. Consensusguidelines for the diagnosis and treatment ofgrowth hormone (GH) deficiency in childhoodand adolescence: summary statement of the GHResearch Society. J Clin Endocrinol Metab 2000;85:3990–3.
19. Giustina A, Barkan A, Casanueva FF, Cavagnini F,Frohman L, Ho K, et al. Criteria for cure ofacromegaly: a consensus statement. J Clin Endo-crinol Metab 2000;85:526–9.
20. Bristow AF, Jespersen AM. The Second Interna-tional Standard for somatropin (recombinantDNA-derived human growth hormone): prepara-tion and calibration in an international collabor-ative study. Biologicals 2001;29:97–106.
21. Sturgeon C, Ellis AR, Al-Sadie R. UK NEQAS forpeptide hormones: annual review for 2009. Edin-burgh (UK): National External Quality AssessmentService; 2010. p 22–6.
22. Miller WG, Myers GL, Rej R. Why commutabilitymatters. Clin Chem 2006;52:553–4.
23. Jan T, Shaw MA, Baumann G. Effects of growthhormone-binding proteins on serum growth hor-mone measurements. J Clin Endocrinol Metab1991;72:387–91.
24. Popii V, Baumann G. Laboratory measurementsof growth hormone. Clin Chim Acta 2004;350:1–16.
25. Burns C, Rigsby P, Moore M, Rafferty B. The FirstInternational Standard for Insulin-like GrowthFactor-I (IGF-I) for immunoassay: preparation andcalibration in an international collaborative study.Growth Horm IGF Res 2009;19:457–62.
26. Milani D, Carmichael JD, Welkowitz J, Ferris S,Reitz RE, Danoff A, et al. Variability and reliabilityof single serum IGF-I measurements: impact ondetermining predictability of risk ratios in diseasedevelopment. J Clin Endocrinol Metab 2004;89:2271–4.
27. Clemmons DR. IGF-I assays: current assay meth-odologies and their limitations. Pituitary 2007;10:121–8.
28. CLSI (formerly NCCLS). Defining, establishing andverifying reference intervals in the clinicallaboratory: approved guidelines – third edition.CLSI document C28A3E. Wayne (PA): CLSI; 2008.
GH and IGF-I Assays Special Reports
Clinical Chemistry 57:4 (2011) 559