Embed Size (px)
Citation preview

Acta Biomaterialia 8 (2012) 449–456
Contents lists available at SciVerse ScienceDirect
Acta Biomaterialia
journal homepage: www.elsevier .com/locate /actabiomat
Biocompatible polymer coating of titania nanotube arrays for improved drugelution and osteoblast adhesion
Karan Gulati a, Saminathan Ramakrishnan a, Moom Sinn Aw a, Gerald J. Atkins b, David M. Findlay b,Dusan Losic a,⇑a Ian Wark Research Institute, University of South Australia, Mawson Lakes Boulevard, Adelaide, SA 5095, Australiab University of Adelaide, Discipline of Orthopaedics and Trauma, Adelaide, SA 5000, Australia
a r t i c l e i n f o
Article history:Received 7 July 2011Received in revised form 28 August 2011Accepted 1 September 2011Available online 7 September 2011
Keywords:Titanium implantsDrug deliveryTitania nanotubesChitosanPLGA
1742-7061/$ - see front matter Crown Copyright � 2doi:10.1016/j.actbio.2011.09.004
⇑ Corresponding author. Tel.: +61 8 8302 6862; faxE-mail address: [email protected] (D. Losic
a b s t r a c t
Bacterial infection, extensive inflammation and poor osseointegration have been identified as the majorreasons for [early] orthopaedic implant failures based on titanium. Creating implants with drug-elutingproperties to locally deliver drugs is an appealing way to address some of these problems. To improveproperties of titanium for orthopaedic applications, this study explored the modification of titanium sur-faces with titaniananotube (TNT) arrays, and approach that combines drug delivery into bone and poten-tially improved bone integration. A titania layer with an array of nanotube structures (�120 nm indiameter and 50 lm in length) was synthesized on titanium surfaces by electrochemical anodizationand loaded with the water-insoluble anti-inflammatory drug indomethacin. A simple dip-coating processof polymer modification formed thin biocompatible polymer films over the drug-loaded TNTs to createTNTs with predictable drug release characteristics. Two biodegradable and antibacterial polymers, chito-san and poly(lactic-co-glycolic acid), were tested for their ability to extend the drug release time of TNTsand produce favourable bone cell adhesion properties. Dependent on polymer thickness, a significantimprovement in the drug release characteristics was demonstrated, with reduced burst release (from77% to >20%) and extended overall release from 4 days to more than 30 days. Excellent osteoblast adhe-sion and cell proliferation on polymer-coated TNTs compared with uncoated TNTs were also observed.These results suggest that polymer-modified implants with a TNT layer are capable of delivering a drugto a bone site over an extended period and with predictable kinetics. In addition, favourable bone celladhesion suggests that such an implant would have good biocompatibility. The described approach isbroadly applicable to a wide range of drugs and implants currently used in orthopaedic practice.Crown Copyright � 2011 Published by Elsevier Ltd. on behalf of Acta Materialia Inc. All rights reserved.
1. Introduction
Titanium (Ti) and titanium alloys are commonly used as ortho-paedic implants because of the desirable mechanical strength, lowdensity, excellent resistance to corrosion, and capacity to bondwith bones and other tissue without any cytotoxic effects [1]. Anon-reactive and biocompatible oxide layer that spontaneouslyforms on titanium surfaces in the body is responsible for theirbio-inertness and degradation resistance [1]. A number of ortho-paedic procedures, in which Ti-based implants are commonly used,have complications, or fail, for reasons that include bacterial infec-tion (osteomyelitis), local inflammation, bone destruction and im-paired bone healing [2,3]. Treatment of these complicationssystemically can be difficult. For example, treatment of infectioncurrently involves prolonged courses of high-dose intravenousand oral antibiotics [ ] to clear the infection [4]. However, systemic
011 Published by Elsevier Ltd. on b
: +61 8 8302 3683.).
drug administration for any condition, whether intravenous, intra-muscular or topically applied, has limitations, such as low drug sol-ubility, poor biodistribution, lack of selectivity, uncontrolledpharmacokinetics and serious side effects in non-target tissues[5]. Again taking the example of infection in bone, failure to elim-inate bacteria at the site of infection can lead to persistent infectionin the form of quiescent bacterial biofilms adherent to orthopaedicimplants. To address this, local drug delivery of antibiotics at theimplantation site is currently used, often as antibiotic-loaded bonecement, in order to prevent implant-associated infections byreducing the concentration of bacteria and/or impeding bacterialadherence to the implant surface [6]. However, the limitation ofthis method is that release of antibiotic from the cement occursin an unpredictable way.
With the advent of nanotechnology, there has been an interestin using this emerging science for various orthopaedic applications[5]. Considerable research has been devoted to modification of Tisurfaces by coating, chemical modification and nanostructuringto improve bone integration of Ti implants [7–10]. The synthesis
ehalf of Acta Materialia Inc. All rights reserved.

450 K. Gulati et al. / Acta Biomaterialia 8 (2012) 449–456
of vertically aligned titania nanotube (TNT) arrays on Ti surfaceshas been recognized as a promising strategy in developing newimplantable drug delivery systems [11–16]. TNTs with excellentbiocompatibility, controllable dimensions, surface chemistry andhigh surface-to-volume ratio of their nanotube structures weredemonstrated to be superior platforms for local drug deliveryapplications [17–21]. Moreover, TNT films have been extensivelyexplored as adhesion and growth support substrates for boneand stem cells, for the prevention of bacterial adhesion, for drugdelivery and to enhance blood clotting for the control of haemor-rhage [21,22]. In addition, favourable bone cell growth, cell differ-entiation and apatite-forming abilities were demonstrated on TNTsurfaces, which make them attractive substrates for biomedicalapplications [23,24].
The aim of our study was to employ these proven advantages ofTNTs to improve properties of Ti for orthopaedic applications, com-bining optimized drug delivery with improved bone integration.The concept proposes to generate TNT arrays on a variety of tita-nium implants (plates, screws, wires, prostheses) in order to pro-vide drug delivery in a range of orthopaedic settings (fracture,joint replacement and osteomyelitis). The aim was to enable theapplication of a wide range of therapeutic agents from implants lo-cally in bone, and to do so with prolonged and predictable releasekinetics.
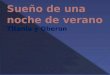
To enable controlled drug release kinetics from nanotube struc-tures, a simple method was employed for surface modification ofthe TNTs with polymers. A schematic of our polymer modificationstrategy is shown in Fig. 1. Previously, we have used plasma poly-merization as a means of controlling drug release from nanoporeand nanotube structures [20,25,26]. Here, we describe the signifi-cantly simpler method of solution casting (dip coating) for polymerdeposition. The process is based on the deposition of a thin poly-mer layer to cover the pore openings of the TNT structures, wherethe film thickness, chemical properties and degradability areexploited to control drug release from nanotubes. Two biocompat-ible and biodegradable polymers, poly(lactic-co-glycolic acid)(PLGA) and chitosan, were selected as they are the most exploredpolymers, widely used for drug delivery applications. These partic-ular polymers carry the additional benefit of having antibacterialand osseointegration properties [10,27–29]. The TNT/Ti implantswere loaded with indomethacin as a model of a water-insolubledrug to prove the drug delivery concept, although there are no lim-itations in terms of drugs that could be delivered by this approach[30]. Here we describe the drug release characteristics of polymer-
Fig. 1. Scheme of titania nanotube (TNT/Ti) implants modified with polymer film. (a) Badrug inside TNT structures; (c) chitosan or PLGA polymer film coated on TNT by dip coaproperties and bone integration. The scheme shows diffusion of drug molecules through
coated TNTs, and the adhesion to and proliferation of osteoblasticcells on these structures, to demonstrate the multifunctional capa-bility of TNT-modified implants.
2. Materials and methods
2.1. Materials
Ti foil (99.6% of Ti) with a thickness of 0.25 mm, supplied by Sig-ma–Aldrich (Australia), was used as model of Ti implant. Ethyleneglycol, ammonium fluoride (NH4F), chitosan (low molecularweight), PLGA and lactide:glycolide (50:50, mol. Wt. 40,000–75,000) were also obtained from Sigma–Aldrich (Australia). High-purity Milli-Q water, ultrapure grade (18.2 MX) sieved through a0.22 lm filter, was used.
2.2. Fabrication of TNT arrays on Ti
The Ti foil was mechanically polished and cleaned by sonicationin acetone for 30 min prior to anodization. To prepare a TNT layeron Ti, two anodization steps were performed using a specially de-signed electrochemical cell and computer-controlled power supply(Agilent), using previously described procedures [20,31,32]. A spe-cially designed electrode holder permitted only a circular area of Timetal, of diameter 1 cm, to be available for anodization. The sameset-up can be used for synthesis of TNT arrays on orthopedic im-plants, including screws, plates and prostheses. In the first anod-ization step a constant voltage of 100 V was applied for 2 h inNH4F/ethyleneglycol electrolyte (3% water and 0.3% NH4F) at20 �C. The resultant TNT layer was removed (mechanically fol-lowed by sonication), leaving the nanotextured titanium surfacefor the second anodization. The second anodization step was per-formed using the same conditions (100 V) as the first anodizationwith an anodization time of 1 h to make an �50 lm thick TNTslayer on Ti with perfectly ordered nanotube structures, as pre-sented schematically in Fig. 1a. Unlike the first TNT layer, preparedby the first anodization, this final layer is rigid and stable enoughfor the proposed implant applications. The voltage–current, volt-age–time and current–time signals were adjusted and continu-ously recorded (Labview, National Instruments) during theanodization process to assure reproducibility of the fabricationprocess.
re TNT layer formed on Ti substrate by electrochemical anodization; (b) loading ofting (thin and thick) with the aim to control drug release and improve antibacterial
the polymer matrix.

K. Gulati et al. / Acta Biomaterialia 8 (2012) 449–456 451
2.3. Drug loading
A solution of indomethacin (1% (w/v)) was prepared in ethanol,for use as a model drug. Titania nanotube surfaces were cleanedusing deionized water and dried in nitrogen. Exactly 100 ll ofthe drug solution was pipetted onto the nanotube surface and al-lowed to dry in air. After drying, the surfaces were wiped using asoft tissue in order to remove excess drug accumulated on thesurface. The loading, drying and wiping steps were repeated 20times in order to load a substantial amount of drug into thenanotubes.
To determine the amount of loaded and released drug in theTNT samples, thermogravimetric analysis (TGA) was performed be-fore and after the polymer coating, and at the end of the releaseexperiment. In order to find the correct range of the drug decom-position, 20–25 mg of drug was loaded into the platinum pan ofthe thermogravimetric analyzer and heated from 20 to 800 �C,and its characteristic weight loss peak was obtained.
2.4. Polymer coating of drug-loaded TNT
Polymer solutions of chitosan (1% (w/v), chitosan + 0.8 vol.%acetic acid in deionized water) and PLGA (1% (w/v) in chloroform)were prepared. The dip-coating process was performed by dippingthe TNT/Ti implant into the polymer solution, followed by dryingin an oven at 70 �C for 10 min. The dip coating is a quick process,so we believe the amount of drug incorporated into the polymerlayer during this process is negligible and does not affect the drugrelease kinetics. To prevent this possibility, before each dip-coatingstep the surface of the TNT substrates was thoroughly cleanedusing a soft tissue followed by very brief rinsing with buffer tomake sure that the drug is removed from the top surface. Thethickness of the deposited polymer was controlled by the numberof dippings (between 1 and 5) and monitored by elipsometry, usinga silicon wafer as the substrate. For this study, drug release fromTNT prepared with thin (one dip coating) and thick (five dip coat-ings) coatings was explored.
2.5. Drug release characterization
Drug release from the drug-loaded and polymer-coated (PLGAand chitosan) TNT implants was investigated by immersion in5 ml of phosphate-buffered saline (PBS), the amount of drug re-leased being measured using ultraviolet–visible (UV–Vis) spectros-copy, as described previously [33]. Measurements were taken atshort intervals during the first 6 h to monitor the initial burst re-lease, followed by testing every 24 h to observe the delayed releaseuntil the entire drug amount was released into the surroundingPBS. Absorbance was measured at 320 nm and the correspondingdrug concentration was calculated based on the calibration curveobtained for the drug. Ultimately, the release profiles of eachexperimental set were expressed for burst and delayed release ina plot with release percentage vs. time. The drug release percent-age (wt.%) was calculated from the amount of drug released intothe buffer solution divided by the total amount of drug (weight) re-leased at the end of the release (determined by a UV–Vis spectro-photometer) multiplied by 100. This cumulative weight oramount of drug released determined by UV–Vis spectrometry atthe end was used as 100%. The agreement between this value ob-tained after polymer coating and the value of total drug loadeddetermined by TGA before coating was confirmed for each sample.TGA after drug release with polymer-coated TNT samples was alsoperformed to ensure that the drug was completely released fromthe sample.
2.6. Structural characterizations
Structural characterization of the prepared TNT/Ti implants be-fore and after drug loading and after polymer coating and drug re-lease were performed using a field emission scanning electronmicroscope (Philips XL 30). The samples were cut into small(approximately 10 mm � 10 mm) pieces, mounted on a holderwith double-sided conductive tape and coated with a layer of plat-inum 3–5 nm thick. Images with a range of scan sizes at normalincidence and at a 30� angle were acquired from the top and bot-tom surfaces and cross-sections. The pore diameters were directlymeasured from scanning electron microscopy (SEM) images withsoftware by drawing a line across the diameter of the pore. To ob-tain an average value, at least five pore diameters were determinedfrom a single SEM image (image size of 2 lm � 2 lm) acquiredfrom at least five different spots on the TNT sample.
2.7. Osteoblastic cell culture
As a model of human osteoblastic cell behaviour, the osteosar-coma cell line HOS (American Type Culture Collection, Rockville,MD, USA) was used. The cells were cultured in a-modified minimalessential medium (Gibco) supplemented with ascorbate 2-phos-phate (100 lM; Gibco), fetal calf serum (FCS, 5 vol.%; Sigma) and1% penicillin/gentamycin (Sigma) at 37 �C in 5% CO2. Ti metal, un-coated TNT/Ti and TNT/Ti coated with chitosan and PLGA weretested for cell adhesion studies. All substrates were gas sterilizedand then placed in 12-well cell culture plates (Nunc). Uncoated tis-sue culture plastic was used as a control substrate. HOS cells wereremoved from culture flasks by trypsinization and resuspended at1 � 106 cells ml�1. A 100 ll aliquot (1 � 105 cells) was added toeach well containing substrate and the plates incubated at 37 �C.Cell adhesion was determined after 1.5 and 7 h. For this, wells werecarefully flooded with 3 ml of culture medium. The medium wasthen removed and the substrates rinsed gently twice with PBS.All washes were pooled and the unattached cell number deter-mined by counting. Relative cell adhesion was assessed using thecrystal violet method, as described previously [34]. Attached cellswere fixed with 200 ll of 10% buffered formalin for 5–10 min, fol-lowed by washing again twice with PBS. The samples were stainedwith 2–3 drops of 1% (w/v) crystal violet for 20 min. After stainingand incubation, the excess stain was removed by washing in tapwater. The cell-associated stain was then extracted with acetic acid(10 vol.%, 200 ll well�1) for 20 min and the absorbance at 570 nmmeasured by spectrophotometry. One-way analysis of variance,followed by Tukey’s post hoc analysis, was used to examine differ-ences in cell adhesion. A value for p < 0.05 was consideredsignificant.
2.8. Osteoblast morphology
Cell morphology was assessed using phalloidin staining, as de-scribed previously [35]. Plastic (control), Ti metal, uncoated TNT/Ti,TNT/Ti coated with chitosan and PLGA samples were sterilized andseeded with HOS cells, as described above. After 7 h of incubation,the medium was removed and the cells washed twice with PBS.The cells were then fixed in 4% (w/v) paraformaldehyde/PBS for10 min and rinsed once in PBS, before being permeabilized in buf-fer containing 0.1% (w/v) saponin (Sigma, Australia) in HHF (Hanks’buffered salt solution + 5% FCS) for 10 min. Cells were washedtwice in PBS containing Tween-20 (0.1 vol.%) and blocked withHHF containing goat serum (5%), bovine serum albumin (1%) andsodium azide (0.1% w/v). After rinsing twice with HHF, phalloi-din-tetramethyl rhodamine isothiocyanate (5 lg ml�1 in PBS; Sig-ma) was added and the samples incubated for 30 min in the darkat room temperature and then washed twice with HHF. To

452 K. Gulati et al. / Acta Biomaterialia 8 (2012) 449–456
visualize nuclei, three drops of 40,6-diamidino-2-phenyindole(DAPI; Sigma) was added to each well and the samples incubatedfor 5 min at room temperature, rinsed twice in HHF and thenmounted in Prolong Gold™ anti-fade reagent (Invitrogen, Carlsbad,CA, USA). Cell morphology was then visualized using confocalmicroscopy (Nikon C1-Z Confocal Microscope), as described [36].
3. Results and discussion
The morphology of the prepared TNT/Ti substrates was charac-terized by SEM and is summarized in Fig. 2. A typical cross-sec-tional image of free-standing TNT structures, removed from theTi substrate for imaging purposes, is presented in Fig. 2a. The thick-ness of the TNT layer was about 50 lm, which was controlled byselecting the appropriate voltage (100 V) and anodization time(1 h). A whole TNT layer with a diameter of 1 cm, formed on a Tifoil substrate, is shown in Fig. 2a (inset). A high-resolution imageof the cross-sectional SEM image of the TNT layer shows a verti-cally aligned and densely packed array of TiO2 nanotubes acrossthe entire structure (Fig. 2b). SEM images of the top nanotube sur-face (Fig. 2c) show pores with diameters of 120 ± 20 nm. The porediameters can be controlled by varying the anodization potential(60–120 V). Thus, for this study, titania nanotubes with pore diam-eters of �120 nm and a length of 50 lm were prepared, in order tomaximize their drug-loading capacity. Although Ti foil was used asa model substrate in this work, the formation of TNTs on medical Tior Ti alloy implants can be similarly accomplished.
The anti-inflammatory, water-insoluble drug indomethacin waschosen as a test drug to be loaded inside the nanotubes. In practice,any drug can be loaded into this system, including those with cur-rent or potential use in bone therapy (antibacterial drugs, bonemorphogenetic proteins (BMPs), anti-resorptive agents, anabolicagents or anti-cancer drugs) [4,5]. The amount of loaded indometh-acin in TNTs was determined from TGA graphs to be 1.54 mg cm�2,
Fig. 2. Series of SEM images of TNTs fabricated by electrochemical anodization of Ti in NTNT layer and the entire structure on the Ti substrate (inset); (b, c) the top surface, showiof the barrier layer. The TNT layer was removed from the underlying Ti for imaging pur
which is adequate to provide a continuous supply of drug into thebone microenvironment with optimal therapeutic concentration tosuppress (in this case) inflammation. It is important to state thatthe drug-loading capacity of TNTs can be tuned by the dimensionsof the nanotube structures (pore diameter, pore length) and thesize of the Ti implants to meet specific therapeutic requirements,depending on the drug, implant, bone and specific condition tobe targeted.
The deposition of PLGA and chitosan polymers onto drug-loaded TNT/Ti by a dip-coating process was evaluated by SEMcharacterization. Typical images of a prepared polymer layer arepresented in Fig. 3, showing an ultrathin and a thick layer coveringthe TNT surface. In the case of the thin polymer film, prepared by asingle deposition step, a high-resolution image (Fig. 3a, inset)shows depressions in the film, which correspond to pore structuresand indicate the formation of a very thin layer on the surface. SEMimages of the top surface of the thick-coated films, prepared by thefive-dip coating procedure, showed a featureless surface of TNT forboth polymers (data not shown). Corresponding cross-sectionalSEM images for both thin and thick films on TNTs are presentedin Fig. 3b and c (chitosan) and d–f (PLGA).
The thickness of the thin polymer layer was difficult to estimateby SEM. Elipsometry was used to determine the thickness of thepolymers, and values of 200–300 nm for chitosan and 300–400 nm for PLGA were obtained for the thin layers. The thicknessof the thick polymer layers, prepared by five dip-coating steps,was determined by SEM to be between 2 and 2.5 lm for both poly-mers. In both cases, pores were covered with polymer layer but atdifferent thicknesses, and we predicted that drug release charac-teristics would be governed by the thickness of the polymer layer,its degradation rate and its chemical composition.
In our previous studies, we showed that the surface modifica-tion of TNTs via plasma polymerization allows control over porediameter, and tailoring of new functionalities has the potential to
H4F/ethyleneglycol electrolyte. (a) Typical cross-sectional image of self-supportingng the nanopores and nanotube structures; (d) the bottom part, showing the detailsposes in (a) and (d).

Fig. 3. SEM images of TNTs after drug loading (indomethacin) and dip coating of a thin polymer layer, showing the top surface and cross-section of the chitosan layerdeposited by (a, b) one dip coating (thin) and (c) five dip coatings (thick); (d, e) the top and cross-section of the PLGA layer prepared by one dip coating (thin) and (f) five dipcoatings (thick).
K. Gulati et al. / Acta Biomaterialia 8 (2012) 449–456 453
significantly improve the drug delivery characteristics of thisattractive biomaterial [20,25,26,33]. The extended release of apoorly soluble drug, such as indomethacin, and drug nanocarriers(polymer micelles) was demonstrated, where drug release basedon diffusion was controlled by pore diameter through accuratedeposition of a plasma polymer [26,33]. In the present approach,instead of a reduction in pore diameters, we used a different poly-mer coating method called the dip-coating process to completelyclose the pores. Polymers with good molecular permeability and,more importantly, with a higher rate of degradability were se-lected to allow diffusion of the drug and solute molecules throughthe polymer layer covering the pores. Despite polymer depositionby dip coating not having the accuracy of the plasma depositionprocess, which requires a high vacuum and costly equipment, theadvantages of this method are its remarkable simplicity, low costand applicability to a wide range of orthopaedic medical implants.Both chitosan and PLGA are biodegradable and biocompatiblepolymers that have been used to improve the properties of im-plants, and both have been extensively explored for a number ofmedically related applications, including drug delivery [27–29].Chitosan has structural characteristics similar to glycosaminogly-cans, especially hyaluronic acid, which is abundant in the extracel-lular matrix [10,37,38]. Chitosan is able to attract proteins,promote cell attachment and adhesion, and also enhance implantintegration into bone tissue by preventing fibroblast growth[27,28,37]. PLGA has been proven to increase osseointegration, de-crease fibroblast growth and help stabilize implants [10,37,38].Both polymers degrade into non-toxic products that do not ad-versely affect cell metabolism [9,10].
Comparative drug release profiles of indomethacin loaded intoTNT implants with and without a polymer film (PLGA and chito-san) with different thicknesses are depicted in Fig. 4. Both the fast(burst) phase over the first 6 h and the overall release are pre-sented. The release characteristics are listed in Table 1, whichshows the release efficiency (% drug release) at various time inter-vals (1, 6 and 24 h, and 7, 14 and 24 days) and the time to completethe drug release. For uncoated TNT/Ti, the release kinetics can bedescribed in two phases, with a high percentage (77%) of the drug
released in the first 6 h (initial burst release), followed by slow re-lease over the following 4–5 days. The burst release can be ex-plained by the high concentration gradient across the pores, withthe large-diameter pores (�120 nm) allowing rapid release of drug.This release originates from drug loaded in the top part of the tita-nia nanotubes, not from drug incorporated into the polymer layer.By reducing pore diameters (60–80 nm) by the anodization pro-cess, it was possible to reduce the burst release by 50–60% andthe overall release could be extended to 7 days.
Significant changes in the drug release profile were observed asa result of coating a polymer film on the top of the TNT surface(Fig. 4). As expected, the drug release characteristics showed astrong dependence on the thickness of polymer layer, but werealso influenced by the chemical composition of the polymer. Again,two phases of drug release were observed; in the case of the thinchitosan film, the burst release was reduced from 77% to 40% (vs.uncoated TNTs), with the extended overall release increased from4 days to more than 9 days. Interestingly, the burst drug releasewith the thin PLGA layer was less reduced to 57% (vs. uncoated77%) but the overall release was significantly extended (19 days)in comparison with chitosan (9 days). From these results, it wasconcluded that the thin PLGA polymer layer provides a higher levelof burst release with a more extended release, whereas a thinchitosan layer provides a lower burst and shorter overall releasetime.
The drug release characteristics of TNT/Ti coated with thickpolymer films of chitosan and PLGA were different from thosecoated with thin films. For chitosan-modified TNT/Ti, the burst re-lease was similar to the thin film form (35%), but the thick PLGAfilm resulted in a dramatic reduction in burst release (<12%). Bothchitosan and PLGA showed a considerably extended overall drugrelease of more than 30 days, confirming the capability of this ap-proach to achieve a long and sustained drug release, which may berequired, for example, for effective anti-infection bone therapy.PLGA-coated TNT/Ti showed characteristic zero-order kinetics overa large range of drug release (12–100%). Zero-order release kineticsis desirable, because a uniform amount of drug is released in eachtime unit. These kinetics, typical for reservoir transdermal delivery

Fig. 4. Comparative drug release graphs of anti-inflammatory drug (indomethacin) from polymer-coated TNT/Ti. (a, b) Overall and burst drug release from uncoated TNT/Tiand TNT/Ti coated with thin and thick chitosan layers; and (c, d) overall and burst drug release from uncoated TNT/Ti and TNT/Ti coated with thin and thick PLGA layers.
Table 1Drug release characteristics of prepared TNT/Ti implants loaded with indomethacin (model drug) and modified with thin and thick chitosan and PLGA polymer films. (Mean ± SD,n = 3).
Coating on drug loaded TNT Polymer thickness (lm) Drug release (%) 100% Drug released (no. of days)
6 h 1 day 7 days 14 days
Uncoated – 77 ± 4 90 ± 3 100 100 4 ± 1Chitosan thin 0.2–0.3 40 ± 2 51 ± 4 98 ± 2 100 9 ± 1Chitosan thick 2–2.5 35 ± 2 67 ± 3 88 ± 5 91 ± 4 30 ± 1PLGA thin 0.3–04 57 ± 1 61 ± 1 72 ± 2 90 ± 4 19 ± 2PLGA thick 1.5–2 12 ± 2 14 ± 1 36 ± 2 52 ± 2 31 ± 1
454 K. Gulati et al. / Acta Biomaterialia 8 (2012) 449–456
systems, are rarely reported for porous and implant devices. Oneexplanation for this behaviour may be that TNTs can act asnanoreservoirs and, because the difference in drug concentrationinside the nanotubes and outside the device is constant, the drivingforce for diffusion is constant, making zero-order kinetics possible.
The molecular transport from TNTs is mainly dependent on thethickness of the polymer layer and on its permeability for drugmolecules. The latter is related to the chemical composition ofthe polymer and its structure, charge and interfacial properties(hydrophobicity/hydrophicility). In addition, transport throughthe polymer is influenced by the rate of degradation of the poly-mer. SEM of the TNTs obtained after 30 days of release confirmedthat both polymer films remained on the surface, but there wasvisibly greater degradation of the chitosan layer. While PLGA ishighly hydrophobic, chitosan is hydrophilic; therefore, the perme-ability of particular drug molecules will be highly dependent ontheir relative hydrophobicity/hydrophilicity. Since indomethacinis hydrophobic and water insoluble, it is expected that the solubil-ity and diffusion of this drug through the PLGA matrix will begreater than through chitosan.
The drug release from TNT/Ti with thin polymer films showedfaster burst release for PLGA (57%) than for chitosan (40%), con-firming better penetration of indomethacin through the PLGAlayer. However, in the case of thick films, we observed the oppositesituation, with faster burst release for chitosan (32%) than for PLGA(12%), which can be explained by slower penetration of the solute(buffer solution) through the hydrophobic PLGA structures.Achieving polymer coatings with long-time release kinetics is morecomplicated due to the significant influence of both the degrada-tion rate and stability of the thick polymer layers. The superior per-formance of PLGA, with zero-order kinetics and extended drug
release for more than 30 days, in comparison with chitosan canbe explained by its lower degradation rate and the greater integrityof the PLGA polymer film.
The drug release characteristics of polymer-modified TNT/Tisuggest that, by appropriate selection of the polymer film and itsthickness, it is possible to tune the drug release profile of TNT/Tiimplants to the desired characteristics for a specific application,to ensure their optimal therapeutic dosage for the required time.Therefore, this approach has the flexibility to be applied to Ti im-plants for different purposes, from short drug release scenarios,for example to suppress inflammation, to middle-term (1–2 weeks) drug release, such as to prevent bacterial infection, andlong-term (>30 days) drug release for other therapies, includingimproving the osseointegration process, fracture repair and treat-ment of bone cancer. Moreover, TNTs can be used for loading morethen one drug, providing the ability to design TNT-based implantswith multiple drug release and complex bone therapies.
A basic requirement for the use of TNT/Ti implants in bone isthat they are biocompatible with respect to bone cells, principallycells of the osteoblast lineage. Therefore, the adhesion and prolifer-ation of human osteoblastic cells (HOS) on these substrates wasinvestigated. Comparison was made for cell adhesion on five sub-strates: plastic (control), Ti metal, uncoated TNT/Ti, chitosan-coated TNT/Ti and PLGA-coated TNT/Ti. The total number of cellsadherent on the surface of these substrates after different timesof attachment (1.5 and 7 h) was converted into a percentage ofthe total, and is graphically represented in Fig. 5. The number ofcells adherent on plastic was taken as 100%. Interestingly, it wasfound that cells attached more avidly to all the substrates com-pared with plastic at the early time of 1.5 h. Differences were ob-served in the osteoblast-binding properties of modified Ti

Fig. 5. Graphical representation of adhesion of osteoblastic cells on plastic (control), Ti surface, uncoated TNTs/Ti, TNTs/Ti coated with chitosan and TNTs/Ti coated with PLGA(thin films). Data shown are means ± SD of quadruplicate assays. Asterisks denote significant difference to the Ti surface (⁄⁄p < 0.01, ⁄⁄⁄p < 0.001); NS = not significant.
Fig. 6. Spreading of human osteoblastic cells imaged by confocal microscopy on: (a) Ti surface, (b) uncoated TNT/Ti, (c) TNT/Ti coated with chitosan and (d) TNT/Ti coatedwith PLGA. Phalloidin (red, cytoskeleton) and DAPI (blue, nuclei) stains show the clear spreading and morphological features of the attached cells. Interconnections betweencells are also evident (arrows). Scale bars represent 50 lm.
K. Gulati et al. / Acta Biomaterialia 8 (2012) 449–456 455
surfaces. As depicted in Fig. 5, after 1.5 h of cell incubation all Tisurfaces showed superior attachment of HOS osteoblasts to theplastic control surface (p < 0.01). TNT modification further en-hanced cell attachment. Of these, chitosan-coated TNT/Ti sub-strates gave greater cell attachment, which is not surprisingbecause positively charged chitosan chains, with a high densityof amino groups, attract proteins and promote cell adhesion[9,37]. These data indicate that polymer-coated TNT modificationsof Ti enhance the osteoblast-binding properties of Ti, indicative ofthe suitable and possibly superior biocompatibility of thesestructures.
The ability of the cells to spread on the different substrates wasshown by cytoskeletal staining and confocal microscopic analysis(Fig. 6). The cellular actin filament networks are stained with phal-loidin (red) and nuclei are stained with DAPI (blue). The images
show that the osteoblasts are well spread and attached to eachof the surfaces, indicating that both polymer coatings on the TNTwere able to support osteoblast attachment and viability. Theseresults are in agreement with previous studies showing that chito-san promotes the formation of ordered bone tissue, as it allows forthe growth, replication and cell-shape retention of osteoblasts[10,37,39]. Significantly, chitosan is also considered to be anti-bac-terial, with the ability to kill members of the Staphylococcus andCandida families [40] and bacteriostatic, with the ability to preventthe replication of members of the Pseudomonas family [41].
4. Conclusion
In summary, we report the preparation and characteristics of Tiimplants with a layer of titania nanotube arrays that have

456 K. Gulati et al. / Acta Biomaterialia 8 (2012) 449–456
extended drug release properties, biocompatibility for human oste-oblasts and potentially improved antibacterial properties. Thepreparation involves simple and inexpensive processes, includingelectrochemical generation of TNT arrays on a Ti surface, drugloading and dip-coating deposition of a thin layer of two biode-gradable polymers (chitosan and PLGA). The drug loading and re-lease of the water-insoluble drug indomethacin was explored asa model to reveal the drug release characteristics of the system.The ability to tune and extend the release of drug in both burstand slow phase with zero-order kinetics over 30 days, dependingon the thickness of polymer layer, is demonstrated. We alsoshowed the biocompatibility of these polymer coatings on TNTsusing human osteoblastic cells. The advantage of this system isthat it can be applied to a wide range of implants (Ti, Ti alloys,stainless steel) and different drugs, which means that it is suitablefor diverse orthopaedic applications and bone therapies, includingtreating bone infections, local delivery of anabolic agents such asBMPs for bone repair, antiresorptive agents, and targeted treat-ment of bone cancer and osteomyelitis.
Acknowledgments
The authors acknowledge the financial support of the AustralianResearch Council (DP 0770930) and the University of South Austra-lia for this work. Thanks to Dr Ghafar Servastani from Hanson Insti-tute for confocal imaging and Ms Renee Ormsby (Bone Cell BiologyGroup) for technical help with cell experiments. Thanks also toAdelaide Microscopy, University of Adelaide, for their support inusing SEM facilities.
Appendix A. Figures with essential colour discrimination
Certain figures in this article, particularly Figures 1–6, are diffi-cult to interpret in black and white. The full colour images can befound in the on-line version, at doi:10.1016/j.actbio.2011.09.004.
References
[1] Long M, Rack HJ. Titanium alloys in total joint replacement – a materialsscience perspective. Biomaterials 1998;19(18):1621–39.
[2] Esteban J, Cordero-Ampuero J. Treatment of prosthetic osteoarticularinfections. Expert Opin Pharmacother 2011;12(6):899–912.
[3] Miclau T, Schmidt AH, Wenke JC, Webb LX, et al. Infection. J Orthop Trauma2010;24(9):583–6.
[4] Liu H, Webster TJ. Nanomedicine for implants: a review of studies andnecessary experimental tools. Biomaterials 2007;28(2):354–69.
[5] Tran PA, Sarin L, Hurt RH, Webster TJ. Opportunities for nanotechnology-enabled bioactive bone implants. J Mater Chem 2009;19(18):2653–9.
[6] Simchi A, Tamjid EE, Pishbin F, Boccaccini AR. Recent progress in inorganic andcomposite coatings with bactericidal capability for orthopaedic applications.Nanomed Nanotechnol Biol Med 2011;7:22–39.
[7] Larsson C, Thomsen P, Lausmaa J, Rodahl M, Kasemo B, Ericson LE. Boneresponse to surface modified titanium implants: studies on electropolishedimplants with different oxide thicknesses and morphology. Biomaterials1994;15:1062–74.
[8] Schwartz Z, Martin JY, Dean DD, Simpson J, Cochran DL, Boyan BD. Effect oftitanium surface roughness on chondrocyte proliferation, matrix production,and differentiation depends on the state of cell maturation. J Biomed Mater Res1996;30:145–55.
[9] Martin HJ, Schulz KH, Bumgardner JD, Schneider JA. Enhanced bonding ofchitosan to implant quality titanium via four treatment combinations. ThinSolid Films 2008;516(18):6277–86.
[10] Smith LJ, Swaim JS, Yao C, Haberstroh KM, Nauman EA, Webster TJ. Increasedosteoblast cell density on nanostructured PLGA-coated nanostructuredtitanium for orthopedic applications. Int J Nanomed 2007;2(3):493–9.
[11] Losic D, Simovic S. Self-ordered nanopore and nanotube platforms for drugdelivery applications. Expert Opin Drug Deliv 2009;6(12):1363–81.
[12] Popat KC, Eltgroth M, La Tempa TJ, Grimes CA, Desai TA. Titania nanotubes: anovel platform for drug-eluting coatings for medical implants. Small2007;3(11):1878–81.
[13] Popat KC, Leoni L, Grimes CA, Desai TA. Influence of engineered titaniananotubular surfaces on bone cells. Biomaterials 2007;28(21):3188–97.
[14] Song YY, Schmidt-Stein F, Bauer S, Schmuki P. Amphiphilic TiO2 nanotubearrays: an actively controllable drug delivery system. J Am Chem Soc2009;131(12):4230–3.
[15] Yao C, Slamovich EB, Webster TJ. Enhanced osteoblast functions on anodizedtitanium with nanotube-like structures. J Biomed Mater Res Part A2008;85A(1):157–66.
[16] Ghicov A, Schmuki P. Self-ordering electrochemistry: a review on growth andfunctionality of TiO2 nanotubes and other self-aligned MOx structures. ChemCommun 2009(20):2791–808.
[17] Peng L, Eltgroth ML, LaTempa TJ, Grimes CA, Desai TA. The effect of TiO2
nanotubes on endothelial function and smooth muscle proliferation.Biomaterials 2009;30(7):1268–72.
[18] Peng LL, Mendelsohn AD, LaTempa TJ, Yoriya S, Grimes CA, Desai TA. Long-term small molecule and protein elution from TiO2 nanotubes. Nano Lett2009;9(5):1932–6.
[19] Aninwene GE, Yao C, Webster TJ. Enhanced osteoblast adhesion to drug-coatedanodized nanotubular titanium surfaces. Int J Nanomed 2008;3(2):257–64.
[20] Vasilev K, Poh Z, Kant K, Chan J, Michelmore A, Losic D. Tailoring the surfacefunctionalities of titania nanotube arrays. Biomaterials 2010;31(3):532–40.
[21] Alpaslan E, Ercan B, Webster TJ. Anodized 20 nm diameter nanotubulartitanium for improved bladder stent applications. Int J Nanomed2011;6:219–25.
[22] Park J, Bauer S, Schlegel KA, Neukam FW, von der Mark K, Schmuki P. TiO2nanotube surfaces: 15 nm – an optimal length scale of surface topography forcell adhesion and differentiation. Small 2009;5(6):666–71.
[23] Oh S, Brammer KS, Li YSJ, Teng D, Engler AJ, Chien S, et al. Stem cell fatedictated solely by altered nanotube dimension. Proc Natl Acad Sci USA2009;106(7):2130–5.
[24] Park J, Bauer S, von der Mark K, Schmuki P. Nanosize and vitality: TiO2
nanotube diameter directs cell fate. Nano Lett 2007;7(6):1686–91.[25] Losic D, Cole MA, Dollmann B, Vasilev K, Griesser HJ. Surface modification of
nanoporous alumina membranes by plasma polymerization. Nanotechnology2008;19(24):245704.
[26] Simovic S, Losic D, Vasilev K. Controlled drug release from porous materials byplasma polymer deposition. Chem Commun 2009;46(8):1317–9.
[27] Ueno H, Yamada H, Tanaka I, Kaba N, Matsuura M, Okumura M. Acceleratingeffects of chitosan for healing at early phase of experimental open wound indogs. Biomaterials 1999;20(15):1407–14.
[28] Kung S, Devlin H, Fu E, Ho KY, Liang SY, Hsieh YD. The osteoinductive effect ofchitosan–collagen composites around pure titanium implant surfaces in rats. JPeriodontal Res 2011;46(1):126–33.
[29] Webster TJ, Smith TA. Increased osteoblast function on PLGA compositescontaining nanophase titania. J Biomed Mater Res Part A 2005;74A(4):677–86.
[30] Nokhodchi A, Javadzadeh Y, Siahi-Shadbad MR, Barzegar-Jalali M. The effect oftype and concentration of vehicles on the dissolution rate of a poorly solubledrug (indomethacin) from liquisolid compacts. J Pharm Pharm Sci2005;8(1):18–25.
[31] Paulose M, Peng L, Popat KC, Varghese OK, La Tempa TJ, Bao N, et al.Fabrication of mechanically robust, large area, polycrystalline nanotubular/porous TiO2 membranes. J Membr Sci 2008;319(1–2):199–205.
[32] Kant K, Losic D. A simple approach for synthesis of TiO2 nanotubes withthrough-hole morphology. Phys Status Solidi RRL 2009;3(5):139–41.
[33] Aw MS, Simovic S, Addai-Mensah J, Losic D. Polymeric micelles in porous andnanotubular implants as a new system for extended delivery of poorly solubledrugs. J Mater Chem 2011;21(20):7082–9.
[34] Atkins GJ, Bouralexis S, Evdokiou A, Hay S, Labrinidis A, Zannettino AC, et al.Human osteoblasts are resistant to Apo2L/TRAIL-mediated apoptosis. Bone2002;31(4):448–56.
[35] Atkins GJ, Welldon KJ, Holding C, Haynes DR, Howie DW, Findlay DM.Polyethylene particles induce a catabolic phenotype in human primaryosteoblasts and osteocytes. Biomaterials 2009;30:3672–81.
[36] Jung UW, Song KY, Kim CS, Lee YK, Cho KS, Kim CK, et al. Effects of a chitosanmembrane coated with polylactic and polyglycolic acid on bone regenerationin a rat calvarial defect. Biomed Mater 2007;2(3):S101–5.
[37] Balasundaram G, Webster TJ. An overview of nano-polymers for orthopedicapplications. Macromol Biosci 2007;7(5):635–42.
[38] Webster TJ, Miller DC, Thapa A, Haberstroh KM. In vitro vascular cell adhesionand proliferation on alkaline degraded poly-lactic/glycolic acid polymers. In:Aizenberg J, McKittrick JM, Orme CA, editors. Biological biomimetic materials:properties to function. Warrendale, PA: Materials Research Society; 2002. p.51–6.
[39] Bumgardner JD, Wiser R, Gerard PD, Bergin P, Chestnutt B, Marin M, et al.Chitosan: potential use as a bioactive coating for orthopaedic and craniofacial/dental implants. J Biomater Sci Polym Ed 2003;14(5):423–38.
[40] Muzzarelli RAA, Muzzarelli C, Tarsi R, Miliani M, Gabbanelli F, Cartolari M.Fungistatic activity of modified chitosans against Saprolegnia parasitica.Biomacromolecules 2001;2(1):165–9.
[41] Singla AK, Chawla M. Chitosan: some pharmaceutical and biological aspects –an update. J Pharm Pharmacol 2001;53(8):1047–67.