Embed Size (px)
Citation preview

Mediators of Inflammation
Biomarkers in Inflammatory Childhood Diseases
Guest Editors: Wilco de Jager, Dirk Holzinger, and Ger T. Rijkers

Biomarkers in Inflammatory Childhood Diseases

Mediators of Inflammation
Biomarkers in Inflammatory Childhood Diseases
Guest Editors: Wilco de Jager, Dirk Holzinger,and Ger T. Rijkers

Copyright © 2013 Hindawi Publishing Corporation. All rights reserved.
This is a special issue published in “Mediators of Inflammation.” All articles are open access articles distributed under the Creative Com-mons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.

Editorial Board
Anshu Agrawal, USAMuzamil Ahmad, IndiaSimi Ali, UKPhilip Bufler, GermanyHidde Bult, BelgiumElisabetta Buommino, ItalyDianne Cooper, UKGuanglin Cui, NorwayFulvio D’Acquisto, UKPhamMy-Chan Dang, FranceBeatriz De las Heras, SpainChiara De Luca, ItalyYves Denizot, FranceClara Di Filippo, ItalyBruno L. Diaz, BrazilMaziar Divangahi, CanadaAmos Douvdevani, IsraelStefanie B. Flohe, GermanyTania S. Frode, BrazilJulio Galvez, SpainChristoph Garlichs, GermanyRonald Gladue, USAHermann Gram, SwitzerlandOreste Gualillo, SpainElaine Hatanaka, Brazil
Nina Ivanovska, BulgariaYong Jiang, ChinaYona Keisari, IsraelAlex Kleinjan, The NetherlandsMagdalena Klink, PolandElzbieta Kolaczkowska, PolandDmitri V. Krysko, BelgiumPhilipp M. Lepper, GermanyChanglin Li, USAE. Lopez-Collazo, SpainAntonio Maccio, ItalyA. Malamitsi-Puchner, GreeceSunil Kumar Manna, IndiaFrancesco Marotta, ItalyDonna-Marie McCafferty, CanadaCeline Mehats, FranceBarbro Melgert, The NetherlandsVinod K. Mishra, USAEeva Moilanen, FinlandEric F. Morand, AustraliaJonas Mudter, GermanyMarja Ojaniemi, FinlandSandra Oliveira, BrazilAndrew Parker, SwitzerlandJonathan Peake, Austria
Vera L. Petricevich, MexicoPeter Plomgaard, DenmarkMarc Pouliot, CanadaMichal Amit Rahat, IsraelJean-Marie Reimund, FranceAlexander Riad, GermanyHuub Savelkoul, The NetherlandsNatalie J. Serkova, USASunit Kumar Singh, IndiaDirk E. Smith, USAHelen Steel, South AfricaDennis D. Taub, USAKathy Triantafilou, UKFumio Tsuji, JapanPeter Uciechowski, GermanyGiuseppe Valacchi, ItalyLuc Vallieres, CanadaJan van Amsterdam, The NetherlandsElena Voronov, IsraelJyoti J. Watters, USASoh Yamazaki, JapanSatoru Yui, JapanTeresa Zelante, SingaporeDezheng Zhao, USAFreek Zijlstra, The Netherlands

Contents
Biomarkers in Inflammatory Childhood Diseases, Wilco de Jager, Dirk Holzinger, and Ger T. RijkersVolume 2013, Article ID 745493, 2 pages
IL-1𝛽 and IL-6 Upregulation in Children with H1N1 Influenza Virus Infection, Antonio Chiaretti,Silvia Pulitano, Giovanni Barone, Pietro Ferrara, Valerio Romano, Domenico Capozzi, and RiccardoRiccardiVolume 2013, Article ID 495848, 8 pages
Evaluation of Clinical and Immunological Responses: A 2-Year Follow-Up Study in Children withAllergic Rhinitis due to House Dust Mite, Heleen Moed, Roy Gerth van Wijk, Rudi W. Hendriks,and J. C. van der WoudenVolume 2013, Article ID 345217, 8 pages
Evaluation of Adipokines: Apelin, Visfatin, and Resistin in Children with Atopic Dermatitis,Edyta Machura, Maria Szczepanska, Katarzyna Ziora, Dariusz Ziora, Elzbieta Swietochowska, MalgorzataBarc-Czarnecka, and Alicja Kasperska-ZajacVolume 2013, Article ID 760691, 8 pages
Circulating Cytokines and Growth Factors in Pediatric Pulmonary Hypertension, Mark Duncan,Brandie D. Wagner, Keri Murray, Jenna Allen, Kelley Colvin, Frank J. Accurso, and D. Dunbar IvyVolume 2012, Article ID 143428, 7 pages
Symptoms, but Not a Biomarker Response to Inhaled Corticosteroids, Predict Asthma in PreschoolChildren with Recurrent Wheeze, E. M. M. Klaassen, K. D. G. van de Kant, Q. Jobsis, S. T. P. Høvig,C. P. van Schayck, G. T. Rijkers, and E. DompelingVolume 2012, Article ID 162571, 7 pages
Update of Faecal Markers of Inflammation in Children with Cystic Fibrosis, Jung M. Lee,Steven T. Leach, Tamarah Katz, Andrew S. Day, Adam Jaffe, and Chee Y. OoiVolume 2012, Article ID 948367, 6 pages

Hindawi Publishing CorporationMediators of InflammationVolume 2013, Article ID 745493, 2 pageshttp://dx.doi.org/10.1155/2013/745493
EditorialBiomarkers in Inflammatory Childhood Diseases
Wilco de Jager,1 Dirk Holzinger,2,3 and Ger T. Rijkers4,5
1 Centre of Molecular and Cellular Intervention, Department of Paediatric Immunology, University Medical Centre Utrecht, Lundlaan6, 3584 EA Utrecht, The Netherlands
2 Department of Paediatric Rheumatology and Immunology, University Children’s Hospital Muenster, Muenster, Germany3 Institute of Immunology, University Hospital Muenster, 48147 Muenster, Germany4Department of Science, University College Roosevelt, Utrecht University Lange Noordstraat 1, 4330 AB Middelburg, The Netherlands5 Laboratory of Medical Microbiology and Immunology, St. Antonius Hospital, P.O. Box 2500, 3430 EM Nieuwegein, The Netherlands
Correspondence should be addressed to Wilco de Jager; [email protected]
Received 14 May 2013; Accepted 14 May 2013
Copyright © 2013 Wilco de Jager et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Biomarkers are of crucial importance in modern medicinefor risk-assessment, disease prevention, early diagnosis, drugtarget identification, drug response and monitoring of dis-ease activity. Biomarkers can be defined as characteristicswhich are measured and evaluated as indicators of a normalbiologic, or pathologic process, or pharmacologic responsestowards a therapeutic intervention [1]. Although the termbiomarker is relatively new, biomarkers have been used forconsiderable time, in fact as long as clinical medicine. Forexample, body temperature is a well-known biomarker forfever; serum levels of C-reactive protein (themost performedassay in hospital laboratories) is a marker for inflammationand glucose levels are used for diagnosis as well as therapeuticreadout for controlling diabetes.
For this special issue on Biomarkers in InflammatoryChildhood Diseases we took particular interest in studiesdealing with biomarkers for immune mediated childhooddiseases. Besides the fact that biomarkers for childhooddiseases are, due to ethical restrictions, small populationsizes, and limited sample volumes less available, in mostcases the normal reference range is extrapolated from adultpopulations or animal models and therefore not alwaysapplicable for paediatric patients. As the pediatric populationis in the process of development, bothmentally and physicallythey are at risk for other hazards in comparison with adults.Furthermore, when studying the various parameters of thehuman immune system changes are observed during agingwhich have to be taken in account in paediatric patients
[2]. Therefore, insight and progression of complex paediatricdiseases, in particular inflammatory diseases, can benefitfrom establishment and validation of a comprehensive set ofbiomarkers.
In this special Issue on Biomarkers in InflammatoryChildhoodDiseases, various paediatric diseases are discussedwhich are either chronic such as cystic fibrosis and allergicrhinitis or asthma, or acute disease with life threateningcomplications such as paediatric pulmonary hypertensionand H1N1 infection. Of interest to note is that there areseveral contributions which use or discuss non invasivesample to acquire biological material of a diseased organ,such as exhaled breath condensate from asthmatic children,and faeces of cystic fibrosis patients with potential intestinalinflammation. Furthermore, for optimal data mining severalresearchers also implemented state of the art new multiplextechnologies which can handle micro volumes of biologicalsamples, and produce more insight information in compari-son with classical methodologies.
Duncan and colleagues from Colorado, USA, reportpromising new data on circulating cytokines, in particularEGF, IL-6 and VEGF, which could predict adverse events inchildren with pulmonary hypertension. In a small cohort ofchildren with H1N1 infection, Chiaretti et al. from Rome,Italy, show that elevated IL-1𝛽 and IL-6 are associated withdisease severity, but not with ultimate outcome. Moed et al.have investigated the value of a set of both cellular as well ascytokine biomarkers in children with allergic rhinitis. While

2 Mediators of Inflammation
the biomarker profile was of use in establishing the severityof the allergic rhinitis, long term follow-up demonstratedreduction of allergic symptomswith persistence of the in vitrocellular abnormalities. Also in predicting which childrenwith wheezing symptoms would progress to asthma, as wasstudied by Klaassen et al. in Maastricht, clinical symptomsare better predictors than biomarkers in exhaled breath con-densate. In cystic fibrosis, pulmonary inflammation is amajorclinical expression of the disease and in the majority of casesrespiratory failure is the cause of mortality. Accumulatingdata now show that intestinal inflammation contributes tothe disease and Lee et al. from Sidney, Australia reviewthis evidence, in particular the value of faecal inflammatorymarkers such as calprotectin and S100A12. The final paperdeals with childhood obesity. Adipose tissue is amajor sourcefor adipokines, which include hormones such as leptin andadiponectin, cytokines, as well as proteins like apelin andresistin. Machura et al. from Zabrze in Poland have evaluatedthese adipokines in children with atopic dermatitis and findapelin and visfatin excellent biomarkers for atopic dermatitis.
This special issue on Biomarkers in Inflammatory Child-hood Diseases thus reflects the diversity of research inthis field and shows the potential of biomarker research inpaediatrics. Taken together, the strength of combining non-invasive sampling of biological samples such as saliva, urine,faeces and exhaled breath condensates, as well as multiplexanalysis methodologies which can handle small sized samplevolumes holds the future for biomarker research in paediatricpopulations.
Wilco de JagerDirk HolzingerGer T. Rijkers
References
[1] A. J. Atkinson Jr., W. A. Colburn, V. G. DeGruttola et al.,“Biomarkers and surrogate endpoints, preferred definitions andconceptual framework,” Clinical Pharmacology & Therapeutics,vol. 69, pp. 89–95, 2001.
[2] P. D. Rymkiewicz, Y. X. Heng, A. Vasudev, and A. Larbi, “Theimmune system in the aging human,” Immunologic Research,vol. 53, no. 1–3, pp. 235–250, 2012.

Hindawi Publishing CorporationMediators of InflammationVolume 2013, Article ID 495848, 8 pageshttp://dx.doi.org/10.1155/2013/495848
Research ArticleIL-1𝛽 and IL-6 Upregulation in Children with H1N1Influenza Virus Infection
Antonio Chiaretti,1 Silvia Pulitanò,2 Giovanni Barone,1 Pietro Ferrara,1
Valerio Romano,1 Domenico Capozzi,1 and Riccardo Riccardi1
1 Department of Pediatrics, Catholic University of the Sacred Heart, A. Gemelli Hospital, Policlinico Gemelli, Largo Gemelli,1-00168 Rome, Italy
2 Pediatric Intensive Care Unit, Catholic University of the Sacred Heart, A. Gemelli Hospital, 00168 Rome, Italy
Correspondence should be addressed to Antonio Chiaretti; [email protected]
Received 22 June 2012; Accepted 31 March 2013
Academic Editor: Ger Rijkers
Copyright © 2013 Antonio Chiaretti et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
The role of cytokines in relation to clinical manifestations, disease severity, and outcome of children with H1N1 virus infectionremains thus far unclear. The aim of this study was to evaluate interleukin IL-1𝛽 and IL-6 plasma expressions and their associationwith clinical findings, disease severity, and outcome of children with H1N1 infection. We prospectively evaluated 15 children withH1N1 virus infection and 15 controls with lower respiratory tract infections (LRTI). Interleukin plasma levels were measured usingimmunoenzymatic assays. Significantly higher levels of IL-1𝛽 and IL-6 were detected in all patients with H1N1 virus infectioncompared to controls. It is noteworthy tomention that inH1N1 patientswithmore severe clinicalmanifestations of disease IL-1𝛽 andIL-6 expressions were significantly upregulated compared toH1N1 patients withmild clinical manifestations. In particular, IL-6 wassignificantly correlatedwith specific clinical findings, such as severity of respiratory compromise and fever.No correlationwas foundbetween interleukin expression and final outcome. In conclusion,H1N1 virus infection induces an early and significant upregulationof both interleukins IL1𝛽 and IL-6 plasma expressions. The upregulation of these cytokines is likely to play a proinflammatory rolein H1N1 virus infection and may contribute to airway inflammation and bronchial hyperreactivity in these patients.
1. Introduction
In the last years the world has been facing a new pandemiacaused by an H1N1 influenza virus, the so-called H1N1/09virus, which contains a unique combination of gene segmentsthat has never been identified in humans or animals [1].This new pandemic strain is of particular concern becauseof its efficient person-to-person transmission responsible forincreased virulence and morbidity in humans [2, 3].
The novel influenza H1N1 virus was identified as a causeof febrile respiratory infections ranging from self-limitedto severe illness both in adults and children. Recent datareported that most cases of H1N1 infection with high rate ofhospitalizations occurred in children who aged 5–14 years.A small percentage of these patients can develop morecomplicated and severe symptoms, such as elevated fever,violent dry cough, pneumonia, and acute respiratory distress
syndrome (ARDS) [4, 5], requiring admission in PediatricIntensive Care unit (PICU) and mechanical ventilation [6].
Several hypotheses to explain this particular virulence ofH1N1 in children were advocated, including downregulationof type 1 interferon expression, apoptosis, and hyperin-duction of proinflammatory cytokines [7]. Upregulation ofinflammatory cytokines, such as the TNF-a, IL-1𝛽, IL-6, andIL-10, and a cytokine-mediated inflammatory response havealso been documented as responsible of severity of viral lunginfections [8]. Different viruses, such as respiratory syncytialvirus (RSV) and adenovirus, enhanced the production of IL-6 by human macrophages influencing the susceptibility andseverity of respiratory infections [9]. In addition, pulmonaryand systemic inflammatory stimuli, such as hypoxia andfever, induce the biosynthesis of interleukins (ILs) inmost celltypes, including respiratory endothelium and mast cells [10,11], thus determining the increase of vascular permeability

2 Mediators of Inflammation
and leukocyte accumulation in lung tissue [12, 13]. In theliterature the inflammatory role of IL-6 and IL-1𝛽 in bothsystemic and respiratory disorders such as meningitis, headinjury, and ARDS has also been reported [14, 15]. Moreover,recent studies demonstrated that influenza virus A elicits anacute inflammatory response characterized by the productionof pro-inflammatory cytokines, such as IL-33 and IL-6, ininfected lungs, suggesting a key role for these interleukinsin the pathogenesis of respiratory epithelial cell damageand lung inflammation [16, 17]. However, the role of mostcytokines in relation to clinical findings, disease severity, andoutcome of children with H1N1 virus infection remains thusfar unclear. Attempting to elucidate the immunemechanismsof inflammation and to clarify the role of interleukins IL-1𝛽 and IL-6 in children with H1N1 virus infection, weevaluated the plasma levels of these cytokines in 15 childrenwith H1N1 infection and 15 controls with lower respiratorytract infections (LRTI), to determine whether a correlationwith the expression of these molecular markers and clinicalfindings of these patients exists.
2. Patients and Methods
2.1. Study Population. We conducted a prospective observa-tional clinical study among children admitted from October2009 to December 2010 with the diagnosis of influenza H1N1virus infection and LRTI to the Pediatric Intensive Care Unit(PICU) and Pediatric Infectious Disease Unit (PIDU) of the“Agostino Gemelli” Hospital, Catholic University MedicalSchool, Rome, Italy. Patients with H1N1 influenza virus infec-tion were grouped according to age, etiology of virus infec-tion, findings of chest radiograph, clinical and laboratorycharacteristics, respiratory care, and final outcome (Table 1).We also decided to differentiate the patients with H1N1 virusinfection in two groups (severe and mild manifestationsof H1N1 infection) based on the severity of the symptomsand on the admission to the PICU. We considered severemanifestations of H1N1 influenza infection, the presenceof hypoxia at admission (SpO
2less than 82% in room
air), ARDS requiring mechanical ventilation or noninvasiveventilation (NIV) by Helmet, oxygen supplementation byVentimask orCPAPby facemask, severity of fever (more than39∘C at the moment of admission), presence and durationof cough, presence of specific radiological findings, suchas pneumothorax (PNX), pneumopericardium, and pneu-momediastinum, and other specific clinical manifestations,such as neurological involvement. Based on these admissionparameters, nine patients with severe manifestations of H1N1influenza virus infection were admitted to the PICU, whilethe other 6 patients with mild symptoms of H1N1 infectionwere admitted to the PIDU. Regarding the control group, 8infants with severe RSV bronchiolitis were admitted to thePICU, while the other 7 children with LRTI to the PIDU.Six infants with RSV bronchiolitis admitted to the PICUunderwent oxygen supplementation and NIV by Helmet,while the other 2 patients required mechanical ventilation.The other 7 infants belonging to the control group requiredonly oxygen supplementation and symptomatic treatment(Table 2).
Oral Oseltamivir (60mg twice daily for 5 days) wasadministered to all 15 patients with the diagnosis of influenzaH1N1 virus infection, and supportive therapy for ARDS wasstarted based on the severity of respiratory failure (Table 1).Fever was treated aggressively with paracetamol, while drycough with aerosol therapy. Chest X-ray was performedwithin the first 6 hours of hospital admission. Eventual chestCT scan was performed in all children with H1N1 infectionwith particular severity of respiratory impairment or withspecific findings at standard chest radiography (i.e., PNX,pneumopericardium, or pneumomediastinum). All patientswere isolated at the moment of the admission based ontheir clinical symptoms suspected for H1N1 infection orother acute respiratory illness. The throat/nose swabs andblood samples for both laboratory studies and cytokinesdetermination were taken at the moment of the admission.All the throat/nose swabs were sent to the microbiology forinfluenza virus detection and were analyzed for influenzaA, B, subtypes of A by influenza real-time RT-PCR test,and RSV infection. Tables 1 and 2 reported the clinical anddemographic characteristics of both patients and controlsstudied.
The outcome of patients was assessed upon dischargefrom the hospital using the Glasgow Outcome Score (GOS),which assigns a score of 1 to children who died, 2 to persistentvegetative state, 3 to severe neurologic deficits, 4 to mildneurologic deficits, and 5 to completely healthy children [18,19].
2.2. Plasma Sample Collection. In H1N1 patients we collectedblood samples using indwelling radial artery catheters inchildren admitted to the PICU or arterial puncture inchildren admitted to the PIDU after local painful treatment.All samples were obtained in the acute phase of the illness,at the moment of the admission of the patients, and beforestarting any treatment. The plasma samples were submittedfor microbiological and biochemical analysis (leukocyte andplatelet counts, serum C-reactive protein concentration, pro-calcitonin, glucose-protein concentration, electrolytes, acid-base study, BUN, etc.).
To measure interleukin levels all blood samples werecentrifuged for 10min at 5,000 rpm, and the supernatantswere immediately stored at −70∘C until analysis.
As controls, we used blood radial artery samples collectedfrom childrenwith the diagnosis of LRTI who had undergoneblood sample analysis at themoment of their admission to thePICU or PIDU.
The study was approved by the Institutional ReviewBoard, and the parents of participating children were in-formed about study and provided written informed consent.
2.3. Interleukin Assays. IL-1𝛽 and IL-6 were measured fromblood samples using commercial immunoenzymatic kits(Human Quantikine by R&D Systems) following the instruc-tions of the manufacturer. The sensitivity of the assay wastypically 0.70 pg/mL for IL-6 and 1 pg/mL for IL-1𝛽; no cross-reactivity or interference with other related interleukins wasobserved. Results were represented in pg/mL, and all assayswere performed in duplicate.

Mediators of Inflammation 3
Table1:Clinicalandradiologicalfin
ding
s,respira
tory
assessment,andcomplications
ofH1N
1infectedchild
ren.
Inbo
ldthem
ores
evereH
1N1p
atients.
Patie
nts
Fevera
tfirst
dayof
admission
Durationof
coug
h(days)
SpO
2at
admission
inroom
air
Chest
X-ray
Respira
tory
care
Antim
icrobial
therapy
Com
plications
Leng
thof
stay
inho
spita
l(days)
Outcome
(GOS)
139.6±0.5
878
%Pn
eumotho
rax
O 2supp
lementatio
nby
Ventim
ask
Ceft
riaxon
e,Clarith
romycin,
and
Oselta
mivir
Non
e11
5
239.7±0.4
678
%Pn
eumon
iaCP
APby
Helmet
(1da
y)+O
2byV
entim
ask
Ceft
riaxon
e,Oselta
mivir
Non
e10
5
339.1±0.6
870
%Interstitial
pneumon
ia,
pleuraleffu
sion
NIV
byfull-face
mask,EI/M
V(2
days
),CP
APby
Helmet
(4da
ys)
Ceft
riaxon
e,Clarith
romycin,
and
Oselta
mivir
Pneumorrachis
195
439.3±0.6
681%
Pneumon
iaO
2supp
lementatio
nby
Ventim
ask
Ceft
riaxon
e,Oselta
mivir
Non
e9
5
539.4±0.7
782%
Bilateral
pulm
onary
infiltrates
O2supp
lementatio
nby
Ventim
ask
Ceft
riaxon
e,Oselta
mivir
Non
e9
5
639.2±0.4
750
%Bilateral
pulm
onary
consolidation
EI/M
V(11d
ays),C
PAPby
Helmet
(4da
ys)
Ceft
riaxon
e,Clarith
romycin,
and
Oselta
mivir
Non
e27
5
739.7±0.6
676%
Bilateral
pulm
onary
infiltrates
O2supp
lementatio
nby
Ventim
ask
Ceft
riaxon
e,Oselta
mivir
Pneumom
ediastinum
115
839.2±0.3
582%
Pneumon
iaO
2supp
lementatio
nby
Ventim
ask
Ceft
riaxon
e,Oselta
mivir
Pneumop
ericardium
185
939.5±0.4
973%
Pneumotho
rax,
bilateral
pulm
onary
consolidation
NIV
byfull-face
mask
Ceft
riaxon
e,Oselta
mivir
Non
e18
5
1038.5±0.5
790
Interstitial
pneumon
iaO
2supp
lementatio
nKlaritromicin,
Oseltamivir
Non
e7
5
1138.7±0.2
492
Normal
O2supp
lementatio
nOseltamivir
Non
e4
512
38.2±0.4
594
Normal
Non
eOseltamivir
Non
e3
513
38.3±0.7
595
Normal
Non
eOseltamivir
Non
e3
5
1438.4±0.6
691
Hyperinflated
lung
O2supp
lementatio
nOseltamivir
Non
e6
5
1538.1±0.4
693
Normal
Non
eOseltamivir
Non
e3
5CP
AP:
continuo
uspo
sitivea
irway
pressure;E
I:endo
trachealintubatio
n;MV:
mechanicalventilation.

4 Mediators of Inflammation
Table2:Clinicalandradiologicalfin
ding
s,respira
tory
assessment,andcomplications
ofLR
TIchild
ren.
Inbo
ldthem
ores
evereL
RTIp
atients.
Patie
nts
Fevera
tfirstd
ayof
admission
Durationof
coug
h(days)
SpO
2atadmission
inroom
air
Chest
X-ray
Respira
tory
care
Antim
icrobial
therapy
Com
plications
Leng
thof
stayin
hospita
l(days)
Outcome
(GOS)
137.4±0.3
484
%Segm
ental
pulm
onary
atelectasia
CPAPby
Helmet
andO
2supp
lementatio
nAmoxicillin
Non
e4
5
237.5±0.2
582%
Segm
ental
pulm
onary
atelectasia
and
hyperinfl
ated
lung
Mecha
nicalventilation
andO
2supp
lementatio
n
Amoxicillin,
Ceft
riazon
eNon
e5
5
338.1±0.1
585%
Hyp
erinfla
ted
lung
O2supp
lementatio
nby
face
mask
Amoxicillin
Non
e3
5
438.3±0.2
381%
Hyp
erinfla
ted
lung
CPAPby
Helmet
andO
2supp
lementatio
nAmoxicillin
Non
e3
5
537.4±0.4
482%
Segm
ental
pulm
onary
atelectasia
CPAPby
Helmet
andO
2supp
lementatio
nAmoxicillin
Non
e2
5
637.2±0.6
381%
Hyp
erinfla
ted
lung
CPAPby
Helmet
andO
2supp
lementatio
nAmoxicillin
Non
e3
5
738.5±0.6
480
%Hyp
erinfla
ted
lung
Mecha
nicalventilation
andO
2supp
lementatio
n
Claritr
omicina
Amoxicillin
Non
e4
5
838.1±0.3
582%
Segm
ental
pulm
onary
atelectasia
CPAPby
Helmet
andO
2supp
lementatio
nAmoxicillin
Non
e4
5
937.5±0.2
493%
Segm
ental
pulm
onary
atele
ctasia
O2supp
lementatio
nAmoxicillin
Non
e5
5
1037.5±0.3
391%
Interstitial
pneumon
iaO
2supp
lementatio
nClaritrom
icina
Non
e5
5
1137.7±0.5
488%
Normal
O2supp
lementatio
nAmoxicillin
Non
e4
512
37.5±0.3
393%
Normal
Non
eAmoxicillin
Non
e2
513
38.1±0.4
391%
Normal
O2supp
lementatio
nAmoxicillin
Non
e3
5
1438.3±0.6
386%
Hyperinflated
lung
O2supp
lementatio
nAmoxicillin
Non
e3
5
1537.8±0.5
490%
Normal
O2supp
lementatio
nAmoxicillin
Non
e3
5CP
AP:
continuo
uspo
sitivea
irway
pressure;E
I:endo
trachealintubatio
n;MV:
mechanicalventilation.

Mediators of Inflammation 5
2.4. Statistical Analysis. The nonparametric Mann-Whitneytest and t-test were used to perform statistical comparisonsbetween children withH1N1 virus infection and LRTI controlgroup for continuous variables. Analysis of variance was per-formed using Tukey-Kramer test to compare levels of IL-1𝛽and IL-6 in the studied population. Linear regression analysiswas used to evaluate the correlation between interleukinexpression and clinical manifestations in H1N1 patients.Coefficient of determination (𝑅2) was taken as a measureof the goodness of fit of the model. A P value < 0.05 wasconsidered significant. Statistical and database software usedincluded GraphPad version 5.0 (GraphPad Software, SanDiego, CA, USA) andMicrosoft Office Excel 2007 (MicrosoftCorporation, Redmond, WA, USA), respectively.
3. Results
3.1. Clinical and Laboratory Differences betweenH1N1 Patientsand Controls. We include in this study 15 patients with H1N1virus infection and 15 children with LRTI. Patients withH1N1 infection aged 2.8 years to 17.3 years, with a meanage of 7.9 years, while children with LRTI aged 1.1 yearsto 6.3 years, with a mean age of 3.7 years. Nine childrenwith severe H1N1 virus infection were admitted to our PICUdue to the severity of their respiratory compromise, whilethe other 6 patients to the PIDU. Among children withLRTI, 8 out of 15 were admitted to the PICU with thediagnosis of severe RSV bronchiolitis, while the other 7were admitted to the PIDU (4 with diagnosis of non-RSVbronchiolitis and 3 with diagnosis of influenza A (H2N3)virus infection). Regarding clinical differences between thetwo groups, H1N1 patients experienced higher median fever(39.2∘C) compared to controls (37.7∘C) (𝑃 < 0.0001). Coughwas a common symptom in both groups. However, H1N1patients more frequently suffered from a dry and longercough compared to LRTI patients (median 6 days versus4 days) (𝑃 < 0.0001). The most frequent pulmonaryabnormalities at chest X-ray were represented by pneumoniaand pulmonary consolidation in the H1N1 patients, while inLRTI children we detected atypical findings, such as hyper-inflated lungs and segmental pulmonary atelectasias. Twopatients with H1N1 infection showed PNX, while anotherthree children showed severe respiratory complications, suchas pneumopericardium, pneumomediastinum, and pneu-morrhachis at chest CT scan (Table 1). No pulmonary orsystemic complications were referred to LRTI group. Nodifferences in clinical manifestations, such as gastrointestinaland neurological symptoms, have been reported between thegroups. Regarding laboratory tests (blood cells and plateletcount, serum C-reactive protein, procalcitonin, GOT, GPT,CTN, and urea) no significant differences were detectedbetween H1N1 patients and LRTI controls. All children, bothpatients and controls, had a good outcome without anysignificant complications (GOS 5), but H1N1 patients had asignificantly longer time of hospitalization compared to thecontrol group (9 days versus 3 days: 𝑃 = 0.0013).
3.2. Interleukin Expression in H1N1 Patients and Controls.In H1N1 patients we detected different plasma levels of
0
25
50
75
100
125
150
175
Inte
rleuk
in co
ncen
trat
ions
(pg/
mL)
IL-6
𝑃 < 0.0001
IL-1𝛽
Figure 1: Levels of IL-1𝛽 and IL-6 in H1N1 patients are shown inthe figure. Box plot representation was used. The level of IL-6 wassignificantly higher than the level of IL-1𝛽 (𝑃 < 0.0001).
0
20
40
60
80
Inte
rleuk
in co
ncen
trat
ions
(pg/
mL)
IL-6
𝑃 < 0.0001
IL-1𝛽
Figure 2: Levels of IL-1𝛽 and IL-6 in LRTI patients are shown in thefigure. Box plot representation was used. IL-6 level was significantlyhigher compared to IL-1𝛽 (𝑃 < 0.0001).
interleukins. In these patients we found significantly (𝑃 <0.0001) higher levels of IL-6 (108.1 ± 22.8 pg/mL) comparedto IL-1𝛽 (17.2 ± 7.9 pg/mL) (Figure 1). Also in LRTI patientsthe mean plasma levels of IL-6 were significantly highercompared to the levels of IL-1𝛽 (49.0 ± 10.3 pg/mL versus8.1 ± 2.2 pg/mL) (𝑃 < 0.0001) (Figure 2).
3.3. Plasma Level Differences of Interleukin Expression betweenH1N1 Patients and Controls. Significantly higher levels ofinterleukin IL-6 and IL-1𝛽 were demonstrated in all patientswith H1N1 infection compared to controls. Comparedwith LRTI patients, H1N1 patients displayed significantlyincreased plasma levels of IL-6 (108.1 ± 22.8 pg/mL versus49.0 ± 10.3 pg/mL; 𝑃 < 0.0001) and IL-1𝛽 (17.2 ± 7.9 pg/mLversus 8.1 ± 2.2 pg/mL; 𝑃 < 0.0002) (Figure 3).
3.4. Correlation between Interleukin Expression with DiseaseSeverity and Clinical Manifestations in H1N1 Patients. Toelucidate the association between interleukin expression anddisease severity, we analyzed their plasma levels both inpatients with severe (9 patients) and mild symptoms (6patients) of H1N1 influenza virus infection. Compared tothe mild patients, severe H1N1 patients produced significant

6 Mediators of Inflammation
0
25
50
75
100
125
150
Inte
rleuk
in co
ncen
trat
ions
(pg/
mL)
IL-6 H1N1 IL-6 controls
𝑃 = 0.0002
𝑃 < 0.0001
IL-1𝛽 H1N1 IL-1𝛽 controls
Figure 3: Box plot representation was used. H1N1 patients hadsignificantly higher levels of IL-1𝛽 (𝑃 = 0.0002) and IL-6 (𝑃 <0.0001) when compared to controls.
0
25
50
75
100
125
150
Inte
rleuk
in co
ncen
trat
ions
(pg/
mL)
IL-6 severe IL-6 mild
𝑃 < 0.0001
𝑃 < 0.0001
IL-1𝛽 severe IL-1𝛽 mild
Figure 4: Box plot representation was used. H1N1 patients withsevere disease had significantly higher levels of IL-1𝛽 (𝑃 < 0.0001)and IL-6 (𝑃 < 0.0001) when compared to patients with mildsymptoms.
higher levels of IL-1𝛽 (22.6 ± 4.7 pg/mL versus 9.1 ±2.8 pg/mL; 𝑃 < 0.0001) and IL-6 (124.1 ± 11.8 pg/mL versus84.0 ± 8.6 pg/mL; 𝑃 < 0.0001) (Figure 4).
Moreover, to verify whether there was a correlationbetween interleukin up-regulation and clinical manifesta-tions in H1N1 patients, we compared the plasma levels ofthese cytokines with some clinical symptoms referred to thepatients. In particular, we detected a positive correlationbetween plasma level of IL-6 and fever with a coefficientof determination of 0.64 (𝑃 = 0.0004) (Figure 5). Finallywe found a negative correlation between IL-6 plasma leveland SpO
2at admission in room air with a coefficient of
determination of 0.53 (𝑃 = 0020) (Figure 6). No significantcorrelations were reported between interleukin expressionand other clinical and laboratoristic parameters, such as bio-chemical markers of inflammation (C-reactive protein andprocalcitonin), respiratory care, systemic complications, and,finally, outcome of all children, with H1N1 virus infection.
4. Discussion
Our study, despite the limited patient sample so far evaluated,provides evidence that H1N1 virus infection induces an early
3838.238.438.638.8
3939.239.439.639.8
40
60 70 80 90 100 110 120 130 140 150
Feve
r
IL-6 (pg/mL)
Figure 5: A scatter plot shows the relationship between fever andIL-6 plasma levels. The line represents the regression line (linearregression equation: fever = 0.02 × IL-6 + 36.8 𝑅2 = 0.64).
4550556065707580859095
60 70 80 90 100 110 120 130 140 150IL-6 (pg/mL)
SpO2
at ad
miss
ion
Figure 6: A scatter plot show the relationship between SpO2at
admission in room air and IL-6 plasma level.The line represents theregression line (linear regression equation: SpO
2= −0.38 × IL-6 +
122.9 𝑅2 = 0.53).
and significant up-regulation of interleukin IL-1𝛽 and IL-6plasma levels suggesting that these cytokines are responsiblefor different molecular reactions leading to airway inflamma-tion and disease severity. Compared to LRTI controls, H1N1infected children showed a strongly higher production ofboth IL-1𝛽 and IL-6 soon after virus lung infection, and thisoverexpression seems to correlate with the severity of clinicalcompromise assessed upon admission.We also observed thatin H1N1 patients with more severe clinical manifestations ofdisease, plasma levels of IL-1𝛽 and IL-6 were significantlyupregulated compared to H1N1 mild patients and that thisover expression was correlated with some specific clinicalmanifestations and a longer time of hospitalisation. Morein particular, IL-6 up-regulation was significantly correlatedwith the severity of respiratory compromise, testified bya lower SpO
2at admission and higher fever observed in
this subset of children, as previously reported in patientswith H1N1 virus infection [7]. No differences were reportedbetween plasma expression of these factors and final outcomeof patients and controls.
To date it is difficult to explain the exact role of ILsin the mechanisms of virus host response, because bothpro-inflammatory and immunoprotective actions have beenreported in previous researches. H1N1 virus infection causes

Mediators of Inflammation 7
the activation of the host macrophages and lymphocytesdetermining the release of pro-inflammatory cytokines. Theincreased expression of pro-inflammatory cytokines into thelung tissue may lead to higher blood vessel permeability,phagocytic cell recruitment, apoptosis of lung epithelialcells, and release of neutrophil-derived enzymes, such asmyeloperoxidase and elastase, responsible of severity of acutelung injury [20]. Our results are in agreement with thesestudies, as we showed a significant correlation between ILsup-regulation and severity of respiratory compromise inchildren with H1N1 virus infection. There are some possibleexplanations for this relationship. Up-regulation of IL-1𝛽and IL-6 may affect lung functioning because hypoxia is inturn responsible for the endogenous cytokine productionafter H1N1 lung infections [10]. Cytokine up-regulation maycause epithelial cell damage through different mechanisms.ILs have a direct toxic effect by increasing the productionof nitric oxide synthase, cyclooxygenase, and free radicalsand by favouring the release of the excitatory amino acidin experimental model of neurotoxicity and also in patientswith severe sleep apnea [21, 22],thus determining impairedpulmonary function [23]. Previous studies, in fact, reportedthe correlation between IL-1𝛽 and IL-6 up-regulation andsome clinical and radiological findings, such as pneumoniaand ARDS, both in experimental animal models and inchildren with naturally acquired seasonal influenza A [24–27]. More in particular, IL-1𝛽 and IL-6 have been identifiedas specific markers of the severity of acute lung injury duringH1N1 influenza virus infection [8] and it has also beenreported that IL-1𝛽 is an early and useful biomarker of theseverity and progression of lung inflammation in patientsundergoingmechanical ventilation and unresponsive to anti-microbiological treatment [28]. Our results are consistentwith these previous researches because children with moresevere clinical and radiological manifestations of H1N1 dis-ease severity, such asARDS and longer anddry cough, eliciteda more intensive production of IL-1𝛽 and IL-6 than H1N1mild patients, suggesting that this up-regulation exerted akey role in biochemical andmolecular processes affecting thelung soon after the infection leading to the development ofairway inflammation and bronchial hyperreactivity [29, 30].
Up to now it is difficult to explain if the observed ILsup-regulation in H1N1 patients can represent a protectivemechanisms for respiratory cell survival or it is secondary toa loss of physiological control of ILs biosynthesis. Availableclinical and experimental data does not permit a definitiveclarification of these findings. ILs plasma levels increase inseveral inflammatory diseases, such as allergen provocationand asthma. Recently, lymphocytes and in particular acti-vated T cells were revealed to express ILs receptors in theexperimental animal model of pulmonary sarcoidosis andchemical lung injury [31, 32]. So, it is possible that ILsupregulation is secondary to lymphocytes rapid activation byH1N1 virus infection and that this over-expression representsan important process in the mechanisms of inflammatoryhost response after viral lung infections [33, 34].
Previous studies, in fact, reported that different virallung infections are associated with early up-regulation ofcytokine biosynthesis suggesting that the changes of ILs
release may contribute to the development of airway inflam-mation and bronchial hyperreactivity [34]. In our study,IL-1𝛽 and IL-6 up-regulation, observed early after H1N1virus infection, was consistent with the timing of cytokineexpression in experimental models of virus infected humanalveolar macrophages, suggesting that this over expressionplays a key role in the mechanisms of inflammatory lungresponse [35]. The significant correlation between ILs upreg-ulation and severity of H1N1 virus infection observed inour patients might reflect an endogenous attempt againstmolecular mechanisms activated in the epithelium cellsof infected lung suggesting that ILs up-regulation acts indifferent fashion to amplify and propagate inflammation inthe airways. However, given that the statistical power to finda statistically significant association in a model of 15 patientsis very low, we need to be very cautious on interpreting thesedata, because only limited information is available on ILsexpression in children with viral lung infections.
In conclusion, our observations provide new evidencethat an immune response is activated at the early stage ofpandemic H1N1 influenza virus infection with up-regulatedproduction of plasma interleukins IL-1𝛽 and IL-6.These find-ings are consistent with previous experimental and clinicalstudies confirming a key role for both of these interleukinsin the pathogenesis of airway inflammation and bronchialhyperreactivity during virus lung infections. The increasedexpression of these cytokines may together be the underlyingcause of the observed clinical symptoms in severe H1N1patients, and defining the relationships between ILs expres-sion and the pathophysiology and clinical manifestations ofH1N1 may help to shed light on the molecular pathogenesisofH1N1 influenza and other human viral lung infections. Fur-ther clinical and experimental investigations are necessaryto identify the ILs target cells in the damaged lung and todiscover possible clinical applications of ILs in children withH1N1 influenza virus and other viral lung infections.
References
[1] R. J. Garten, C. T. Davis, C. A. Russell et al., “Antigenic andgenetic characteristics of swine-origin 2009 A(H1N1) influenzaviruses circulating in humans,” Science, vol. 325, no. 5937, pp.197–201, 2009.
[2] Y. Itoh, K. Shinya, M. Kiso et al., “In vitro and in vivocharacterization of new swine-origin H1N1 influenza viruses,”Nature, vol. 460, no. 7258, pp. 1021–1025, 2009.
[3] T. R.Maines, A. Jayaraman, J. A. Belser et al., “Transmission andpathogenesis of swine-origin 2009A(H1N1) influenza viruses inferrets and mice,” Science, vol. 325, no. 5939, pp. 484–487, 2009.
[4] M. Hasegawa, K. Hashimoto, M. Morozumi, K. Ubukata, T.Takahashi, and Y. Inamo, “Spontaneous pneumomediastinumcomplicating pneumonia in children infected with the 2009pandemic influenza A (H1N1) virus,” Clinical Microbiology andInfection, vol. 16, no. 2, pp. 195–199, 2010.
[5] T. Kamigaki and H. Oshitani, “Epidemiological characteristicsand low case fatality rate of pandemic (H1N1) 2009 in Japan,”PLoS Currents, vol. 1, Article ID RRN1139, 2009.
[6] “Epidemiological summary of pandemic influenza A, (H1N1)2009 virusOntario, Canada, June 2009,”Weekly EpidemiologicalRecord, vol. 84, no. 47, pp. 485–491, 2009.

8 Mediators of Inflammation
[7] X. Yu, X. Zhang, B. Zhao et al., “Intensive cytokine inductionin pandemic H1N1 influenza virus infection accompanied byrobust production of IL-10 and IL-6,” PLoS ONE, vol. 6, no. 12,Article ID e28680, 2011.
[8] A. Estella, “Cytokine levels in bronchoalveolar lavage and serumin 3 patients with 2009 influenza A(H1N1)v severe pneumonia,”Journal of Infection in Developing Countries, vol. 5, no. 7, pp.540–543, 2011.
[9] J. A. Patel, S. Nair, E. E. Ochoa, R. Huda, N. J. Roberts,and T. Chonmaitree, “Interleukin-6−174 and tumor necrosisfactor 𝛼−308 polymorphisms enhance cytokine production byhuman macrophages exposed to respiratory viruses,” Journal ofInterferon and Cytokine Research, vol. 30, no. 12, pp. 917–921,2010.
[10] E. Bona, A. L. Andersson, K. Blomgren et al., “Chemokine andinflammatory cell response to hypoxia-ischemia in immaturerats,” Pediatric Research, vol. 45, no. 4 I, pp. 500–509, 1999.
[11] M. Baggiolini, B. Dewald, and B. Moser, “Human chemokines:an update,” Annual Review of Immunology, vol. 15, pp. 675–705,1997.
[12] N.Maruo, I.Morita,M. Shirao, and S. I.Murota, “IL-6 increasesendothelial permeability in vitro,” Endocrinology, vol. 131, no. 2,pp. 710–714, 1992.
[13] I. Julkunen, T. Sareneva, J. Pirhonen, T. Ronni, K. Melen,and S. Matikainen, “Molecular pathogenesis of influenza Avirus infection and virus-induced regulation of cytokine geneexpression,” Cytokine and Growth Factor Reviews, vol. 12, no. 2-3, pp. 171–180, 2001.
[14] A. Chiaretti, O. Genovese, L. Aloe et al., “Interleukin 1𝛽 andinterleukin 6 relationship with paediatric head trauma severityand outcome,”Child’s Nervous System, vol. 21, no. 3, pp. 185–193,2005.
[15] C. L. Wu, Y. L. Lee, K. M. Chang et al., “Bronchoalveolarinterleukin-1𝛽: a marker of bacterial burden in mechanicallyventilated patients with community-acquired pneumonia,”Critical Care Medicine, vol. 31, no. 3, pp. 812–817, 2003.
[16] R. Le Goffic, M. I. Arshad, M. Rauch et al., “Infection withinfluenza virus induces IL-33 in murine lungs,” The AmericanJournal of Respiratory Cell and Molecular Biology, vol. 45, no. 6,pp. 1125–1132, 2011.
[17] A. G. Besnard, D. Togbe, N. Guillou, F. Erard, V. Quesniaux, andB. Ryffel, “IL-33-activated dendritic cells are critical for allergicairway inflammation,” European Journal of Immunology, vol. 41,no. 6, pp. 1675–1686, 2011.
[18] P. M. Shore, R. P. Berger, S. Varma et al., “Cerebrospinal fluidbiomarkers versus glasgow coma scale and glasgow outcomescale in pediatric traumatic brain injury: the role of young ageand inflicted injury,” Journal of Neurotrauma, vol. 24, no. 1, pp.75–86, 2007.
[19] C. M. Robertson, A. R. Joffe, A. J. Moore, and J. M. Watt,“Neurodevelopmental outcome of young pediatric intensivecare survivors of serious brain injury,” Pediatric Critical CareMedicine, vol. 3, no. 4, pp. 345–350, 2002.
[20] S. C. Ducrocq, P. G.Meyer, G. A. Orliaguet et al., “Epidemiologyand early predictive factors of mortality and outcome in chil-dren with traumatic severe brain injury: experience of a Frenchpediatric trauma center,” Pediatric Critical Care Medicine, vol. 7,no. 5, pp. 461–467, 2006.
[21] C. C. Chao, S. Hu, L. Ehrlich, and P. K. Peterson, “Interleukin-1and tumor necrosis factor-𝛼 synergistically mediate neurotox-icity: involvement of nitric oxide and of N-methyl-D-aspartate
receptors,” Brain, Behavior, and Immunity, vol. 9, no. 4, pp. 355–365, 1995.
[22] R. J. Kimoff, Q. Hamid, M. Divangahi et al., “Increased upperairway cytokines and oxidative stress in severe obstructive sleepapnoea,” European Respiratory Journal, vol. 38, no. 1, pp. 89–97,2011.
[23] S. S. Chang, C. A. V. Fragoso, P. H. van Ness, L. P. Fried, and M.E. Tinetti, “Association between combined interleukin-6 and c-reactive protein levels and pulmonary function in older women:results from the women’s health and aging studies I and II,”Journal of the American Geriatrics Society, vol. 59, no. 1, pp. 113–119, 2011.
[24] M. Seki, S. Kohno, M. W. Newstead et al., “Critical role ofIL-1 receptor-associated kinase-M in regulating chemokine-dependent deleterious inflammation inmurine influenza pneu-monia,” Journal of Immunology, vol. 184, no. 3, pp. 1410–1418,2010.
[25] M. Sato, M. Hosoya, and P. F. Wright, “Differences in serumcytokine levels between influenza virus A and B infections inchildren,” Cytokine, vol. 47, no. 1, pp. 65–68, 2009.
[26] T. Taga and T. Kishimoto, “Gp130 and the interleukin-6 familyof cytokines,” Annual Review of Immunology, vol. 15, pp. 797–819, 1997.
[27] P. Puneet, S. Moochhala, and M. Bhatia, “Chemokines inacute respiratory distress syndrome,” The American Journal ofPhysiology, vol. 288, no. 1, pp. L3–L15, 2005.
[28] G. U. Meduri, G. Kohler, S. Headley, E. Tolley, F. Stentz,and A. Postlethwaite, “Inflammatory cytokines in the BAL ofpatients with ARDS: persistent elevation over time predictspoor outcome,” Chest, vol. 108, no. 5, pp. 1303–1314, 1995.
[29] A. Z. El-Hashim and S.M. Jaffal, “Nerve growth factor enhancescough and airway obstruction via TrkA receptor- and TRPV1-dependent mechanisms,” Thorax, vol. 64, no. 9, pp. 791–797,2009.
[30] A. de Vries, F. Engels, P. A. J. Henricks et al., “Airway hyper-responsiveness in allergic asthma in guinea-pigs is mediated bynerve growth factor via the induction of substance P: a potentialrole for trkA,” Clinical and Experimental Allergy, vol. 36, no. 9,pp. 1192–1200, 2006.
[31] C. Dagnell, J. Grunewald,M. Kramar et al., “Neurotrophins andneurotrophin receptors in pulmonary sarcoidosis—granulomasas a source of expression,” Respiratory Research, vol. 11, article156, 2010.
[32] H. Fujimaki, T. T. Win-Shwe, S. Yamamoto, D. Nakajima,and S. Goto, “Role of CD4+ T cells in the modulation ofneurotrophin production inmice exposed to low-level toluene,”Immunopharmacology and Immunotoxicology, vol. 31, no. 1, pp.146–149, 2009.
[33] R. Linker, R. Gold, and F. Luhder, “Function of neurotrophicfactors beyond the nervous system: inflammation and autoim-mune demyelination,” Critical Reviews in Immunology, vol. 29,no. 1, pp. 43–68, 2009.
[34] L. Tortorolo, A. Langer, G. Polidori et al., “Neurotrophinoverexpression in lower airways of infants with respiratorysyncytial virus infection,” The American Journal of Respiratoryand Critical Care Medicine, vol. 172, no. 2, pp. 233–237, 2005.
[35] S. Becker, J. Quay, and J. Soukup, “Cytokine (tumor necrosisfactor, IL-6, and IL-8) production by respiratory syncytial virus-infected human alveolar macrophages,” Journal of Immunology,vol. 147, no. 12, pp. 4307–4312, 1991.

Hindawi Publishing CorporationMediators of InflammationVolume 2013, Article ID 345217, 8 pageshttp://dx.doi.org/10.1155/2013/345217
Research ArticleEvaluation of Clinical and Immunological Responses:A 2-Year Follow-Up Study in Children with Allergic Rhinitisdue to House Dust Mite
Heleen Moed,1 Roy Gerth van Wijk,2 Rudi W. Hendriks,3 and J. C. van der Wouden4
1 Department of General Practice, Erasmus MC-University Medical Center Rotterdam, P.O. Box 2040,3000 CA Rotterdam, The Netherlands
2 Department of Allergology, ErasmusMC-UniversityMedical Center Rotterdam, P.O. Box 2040, 3000 CARotterdam,TheNetherlands3 Department of Pulmonary Medicine, Erasmus MC-University Medical Center Rotterdam, P.O. Box 2040,3000 CA Rotterdam, The Netherlands
4Department of General Practice, VU University Medical Center, 1081 HZ, P.O. Box 7057, 1007 MB Amsterdam, The Netherlands
Correspondence should be addressed to Heleen Moed; [email protected]
Received 6 June 2012; Revised 3 April 2013; Accepted 4 April 2013
Academic Editor: Ger Rijkers
Copyright © 2013 Heleen Moed et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background. Allergic rhinitis is a disease with polarization towards Th2and a defect of regulatory T cells. Immunological changes
have been reported after immunotherapy treatment. However, there is not much known about the natural course of allergic rhinitiswith respect to clinical manifestation and the relation with immunological responses. Objective. To evaluate clinical symptoms ofallergic rhinitis, in relation to in vivo allergen-specific skin responses and in vitro allergen-specific effector and regulatory T cellsdetermined at baseline and after two years.Methods. From a large trial, 59 children were randomly selected.The following variableswere compared: clinical symptoms, allergen skin tests, specific IgE, T-cell proliferation, IL-5, IL-13, IFN-gamma, IL-10, TGF-beta,CD4+CD25hi cells, and Foxp3 expression. Results. Allergic symptoms had decreased after two years. Whereas skin test reactionscorrelated between years 0 and 2, there was no change in the size of the reaction. Also, proinflammatory reactions did not changeafter two years, with a positive correlation between years 0 and 2. No relevant changes were observed with respect to regulatorycells. Conclusion. Whereas, comparable to immunotherapy, allergic complaints decrease, the immunological changes of specificT-cell activity (both effector cells and regulator cells) which are observed after immunotherapy, do not change.
1. Introduction
Allergic rhinitis (AR) is a common chronic illness affecting10% to 20% of the children worldwide [1], and its prevalencehas significantly increased among children over the last twodecades. AR is clinically defined as a symptomatic disorderof the nose induced by an IgE-mediated inflammation afterexposure to an allergen. In the immediate response to anantigen (the early-phase allergic reaction), histamine andother inflammatory mediators are released from mast cellsin the nasal mucosa [2]. This causes the characteristic nasalsymptoms which include sneezing, itching, rhinorrhoea,and nasal congestion. A late-phase allergic reaction occursapproximately 4 to 12 hours after antigen exposure, with nasal
congestion as the predominant symptom. During this phase,inflammatory cells such as eosinophils and T cells infiltratethe mucosa. The Th
2-polarized immune response especially,
with secretion of cytokines such as IL-4, IL-5 and IL-13 and adefect of Th1 cells producing IFN-gamma, play a central rolein the late phase allergic response [2–4].
It has been observed that the immune response to aller-gens is the result of a fine balance between allergen-specificTh2cells and T regulatory cells (Tregs) [5]. Tregs include
a broad spectrum of CD4+ T-cell subpopulations such asnatural thymic-derived Treg cells (nTreg) characterized bytheir CD4+CD25+ phenotype expressing high levels of Foxp3[6] and inducible Tr
1cells (iTreg) which suppress immune
function by the secretion of IL10 and TGF-beta [7–9].

2 Mediators of Inflammation
From the recent literature it becomes clear that it maybe possible to interfere with the natural course of ARby specific immunotherapy (SIT) [9–13]. SIT may inducechanges that skew Th
2- to Th
1-type responses [14] and by
means of tolerance induction. One of the key mechanismsbehind this tolerance induction includes induction of Treg-type cytokines (IL-10 and TGF-beta) [9, 10] and increasedfrequencies of CD4+CD25+ cells [11].
There is an unexplained variability in the clinical courseof allergic rhinitis—with persistence in some individuals andeither progression or remission in others. There is a lack oflongitudinal investigations examining the natural history ofAR. In the present study, we investigate the natural courseof AR regarding clinical manifestations of the disorder andimmunological responses in a followup of 2 years in childrenwith house dust mite allergy. We evaluate clinical symptoms,in vivo skin responses due to allergen and in vitro allergen-specific effector T cells and Treg cells during the naturalcourse of the disease.
2. Methods
2.1. Study Design. This study is a part of the randomizedplacebo-controlled trial ISRCTN91141483 which evaluatessublingual immunotherapy with low-dose house dust miteallergen (2.03mcg/mLor 700 BU/mLDer p1) in childrenwithAR [15, 16]. Patients entered the study either in September–December 2005 or in September–December 2006 for a periodof approximately two years. Written informed consent wasobtained. The study was approved by the Ethical ReviewBoard of ErasmusMC-UniversityMedical Center Rotterdam.
As described elsewhere, [16] neither this low-dose formof SLIT was effective with regard to the reduction of allergycomplaints, asthma complaints, intake of rescue medicationand disease-specific quality of life, nor was there any differ-ence in reported side effects (both local and general) betweenSLIT or placebo treatment, indicating that the dosis of theinvestigated product was a low to mediate reaction. Analysisof placebo (𝑛 = 30) and verum (𝑛 = 29) groups separately inchildren participating in the present study revealed neitherdifferences between verum and placebo regarding clinicalsymptoms (𝑃 value varied between 0.06 and 0.86) nor invivo skin responses (𝑃 value between 0.17 and 0.80) or invitro measurements of pro-inflammatory markers (𝑃 valuebetween 0.16 and 0.85) or regulatory T cells (𝑃 value between0.10 and 0.89).Therefore, we decided tomerge the two groupsand consider them as one group which received placeboduring two years. This merged group forms the basis for thepresent study.
2.2. Patient Selection. From themain trial, fifty-nine childrenwere randomly selected and invited to participate in this elab-orate study. As in the main study, children (aged 6–18 years)with AR and established HDM allergy were selected from theelectronic medical records in general practice. The inclusioncriteria were presence of specific IgE antibodies to HDM inserum (≥0.7 kU/L), a history of allergic rhinitis during at least1 year and a nasal symptom score of at least 4 out of 12 (see
below). Before scoring symptoms, nasal corticosteroids werewithheld for 4 weeks before the study period. During the totalstudy period patients were allowed to use rescue medication(provided by us, i.e., levocetirizine tablets, xylometazolinenasal spray, and levocabastine eyedrops) or another allergyor asthma medication as long as they wrote it down on theirdiary cards (see below). The presence of asthma was assessedusing the International Study of Asthma and Allergies inChildhood (ISAAC) core questionnaire [17].
2.3. Measurement of Nasal, Eye, or Asthma Symptoms. Allparticipants or their parents scored their nasal, eye, andasthma (lung) symptoms on diary cards at baseline (1 monthin October or in November) and after two years (3 months inSeptember–December). Nasal symptoms (sneezing, itchingnose, watery running nose, and nasal blockage), eye symp-toms (itching, tearing, and redness), and asthma symptoms(wheeze/breathless and dry cough during night) were scoredon a 0–3 scale (0 = none, 1 = mild, 2 = moderate, and 3 =severe). In total, a maximal daily cumulative nasal symptomscore of 12, eye symptom score of 9, and lung symptom scoreof 6 could thus be obtained.
A mean symptom score was determined by calculatingthe mean daily score over the entire diary period (i.e., onemonth at baseline and three months after 2 years). Onlydiaries with at least 50% of the filled-out pages were includedin the analyses. In case patients used additional medicationfor their allergy or asthma, theywere asked to document theiruse in the patient diary throughout the 2-year period.
2.4. Skin Testing. Allergy skin testing was performed atbaseline and after 2 years by intracutaneous injection of0.02mL Dermatophagoides pteronyssinus in the forearm(concentration 30 SQU/mL, manufactured by ALK-Abello,Nieuwegein, The Netherlands). We chose to perform anintracutaneous skin test rather than the usual skin prick testbecause intracutaneous injection of the allergen is the mostfeasible and convenient way to induce a late-phase responseafter the early-phase skin response [18]. As a positive control,histamine (concentration of 0.01mg/mL) was injected, andthe negative control was dilution buffer. Reactions were readafter 15min (early response) and after 6 h (late response).Thearea of the skin response in mm2 was measured by a speciallydeveloped scanning programme. The early-phase responsewas expressed as a histamine equivalent intra-cutaneousindex or HEIC index. The late-phase response was expressedas the area of the skin response in mm2. Children were notallowed to take antihistamines within 24 h before skin testing.
2.5. Detection of House Dust Mite-Specific IgE. Serum IgEantibodies to D. pteronyssinus were determined using theCAP-RAST system (Pharmacia, Uppsala, Sweden), accordingto the manufacturers instructions.
2.6. House-Dust-Mite-Specific T-Cell Proliferation. Blood wasdrawn at baseline and after 2 years before skin testing.Peripheral blood mononuclear cells (PBMCs) were isolated

Mediators of Inflammation 3
from heparinized blood by density centrifugation on Ficoll-Paque Plus (GE Healthcare, Uppsala, Sweden). PBMCs wereused in a lymphocyte proliferation test (LPT). Cells wereresuspended in complete medium (RPMI + HEPES + gluta-max supplemented with gentamicin (Gibco, Gibco BRL, LifeTechnologies, Rockville, MD, USA) and 5% heat-inactivatedhuman serum (Sanquin, Rotterdam, The Netherlands) andstimulated by culturing in the presence or absence of 2 IR/mLD. pteronyssinus (Stallergenes, France). All cell cultures wereperformed in quadruplicate in a final volume of 200mL witha cell concentration of 2 × 106 cells/mL in 96-well round-bottomed microtitre plates. To determine HDM-specificproliferative responses, cells were cultured for 5 days at 37∘C,5% CO
2, and 95% humidity. During the last 16 h, cells were
pulsed with 0.5 𝜇Ci/well 3H thymidine (Pharmacia, UK).Radioactivity was measured with a 𝛽-plate reader, and theproliferative capacity was assessed by the stimulation index(SI), calculated as the ratio of mean 3H thymidine uptakein stimulated to that in non-stimulated cultures. The SI wasconsidered positive when it exceeded 2.0.
2.7. House-Dust-Mite-Specific Cytokine Production by ELISA.To determine HDM-specific cytokine production, 1mL ofPBMCs with a concentration of 2 × 106 cells/mL was culturedin duplicate in a 24-well plate with or without 2 IR/mL D.pteronyssinus (Stallergenes France). After 5 days of culture,supernatants were harvested and stored at −20∘C until test-ing. IL-5, IL-13, IFN-𝛾, IL10, and TGF-beta cytokine produc-tion was measured following the manufacturer’s instructions(eBioscience, San Diego, CA, USA or R&D Systems, Abing-don, UK). HDM-induced cytokine production was assessedby subtracting the cytokine concentration of nonstimulatedfrom that of stimulated culture supernatants.
2.8. Detection of CD4+CD25hi Cells by FACS. For pheno-typical analysis, cells were washed with FACS buffer (0.05%NaN3, 2% BSA in PBS) and stained for 30min on ice
protected from light. For the detection of CD4+CD25hiT cells the following anti-human antibodies were used:FITC-conjugated anti-hCD3 (UCHT1, eBioscience), PE-conjugated anti-hCD25 (M-A251, BD) APC-conjugated anti-hCD4 (RPA-T4, eBioscience). Aspecific binding was pre-vented by the use of 2% Heat Inactivated (HI) human ABserum during staining. Afterwards the cells were washedthree times with FACS buffer and measured. Data acquisi-tion was performed by flow cytometry (FACSCalibur; BDBiosciences) and data analysis was performed using FlowJosoftware (Treestar, Coata Mesa, CA)).
2.9. Measurement of Foxp3 Levels by Means of Real-TimeQuantitative PCR. Quantitative RT-PCR for hFoxP3 wasperformed on RNA isolated from HDM-stimulated PBMC’s(as described above). Total RNA was isolated with RNeasyMini Kit (Qiagen) and treated with DNAseI, according tomanufacturer’s protocol. 100 ng RNA was used as a templatefor cDNA synthesis, using Superscript II reverse transcriptase(Invitrogen) and random hexamer primers. QuantitativePCR was performed with Taqman Universal PCRMastermix
Table 1: Baseline characteristics of the study population.
𝑁 = 59
Age, years (mean, SD) 11.6 (3.0)Gender, male (𝑛, %) 28 (47.5%)Wheeze/dyspnea last year (𝑛, %) 37 (62.7%)Multisensitization (𝑛, %) 49 (83.1%)
(Applied Biosystems), preformulated primers (hFoxP3 andhousekeeping gene hHPRT) and probe mixes (“Assay onDemand”, Applied Biosystems). PCR conditions were 2minat 50∘C, 10min at 95∘C, followed by 40 cycles of 15 s at95∘C and 60∘C for 1min using an ABI PRISM 7300 (AppliedBiosystems). PCR amplification of the housekeeping genewas performed during each run for each sample to allownormalization between samples.
2.10. Statistical Analysis. Values are presented as mean (withstandard deviation, SD), median (with interquartile range,IQR), and median estimated difference between baseline(year 0) and year 2. Comparisons were performed by non-parametric analysis, using Wilcoxon signed rank test forcomparisons between baseline data and data after 2 years.TheSpearman rank test (𝑅
𝑠) was used to assess the correlations
between year 0 and year 2. A 𝑃 value of 0.05 was consideredstatistically significant. All analyses were performed usingstatistical software SPSS (version 18).
3. Results
The baseline characteristics of the 59 children included inthe study are described in an earlier study [19]. Of the 59children, 42 (71.8%) completed the 2-year study period. Themost important values are summarized in Table 1. Meanand median values (with SD or IQR) of clinical symptoms,in vivo allergen-induced skin tests, and in vitro specificpro-inflammatory and regulatory responses are displayed inTable 2.
Clinical symptoms of the nose, eye and lung all decreasedsignificantly two years after baseline measurement. Table 3shows a median paired estimated difference of −1.34 (𝑃 <0.0001) for nose symptoms, −0.29 (𝑃 = 0.02) for eyesymptoms and −0.33 (𝑃 < 0.0001) for lung symptoms. Therewas a significant positive correlation between values of year0 and year 2 for all clinical symptoms (𝑅
𝑠between 0.56 and
0.61; 𝑃 < 0.0001).Reactions of in vivoHDMspecific skin tests (both early as
well as late skin reactions) did not significantly change whenmeasured two years after the baseline measurement (Table 3,𝑃 = 0.09 or 𝑃 = 0.07, resp., Table 3). Whereas there were nosignificant changes in time, skin responses showed a positivecorrelation when skin responses of year 0 and year 2 werecompared (𝑅
𝑠= 0.44; 𝑃 = 0.005 for the early skin response
or 𝑅𝑠= 0.5; 𝑃 = 0.001 for the late skin response).
Relevant proinflammatory variables for AR (i.e., HDMspecific IgE, T-cell proliferation, IL-5, IL-13, and IFN-gamma)

4 Mediators of Inflammation
Table 2: Mean (SD), median (IQR), and number of different variables for year 0 and year 2.
Year 0 Year 2Mean SD Median IQR 𝑁 Mean SD Median IQR 𝑁
Clinical symptomsNose (score from 0–12) 3.8 2.2 3.62 3.46 59 2.3 1.95 1.84 2.06 52Eye (score from 0–9) 1.15 1.32 0.67 1.39 59 0.65 1.1 0.21 0.79 52Lung (score from 0–6) 0.87 1.13 0.37 1.33 59 0.36 0.9 0.028 0.15 52
HDM-specific skin testEarly skin test (HEIC) 1.72 0.61 1.69 0.76 52 1.96 0.78 1.7 0.87 42Late skin test (mm2) 871.4 771.6 759.2 1389.8 59 1112.4 904.6 1044.5 1418.28 42
HDM-specific proinflammatory responseSpecific IgE (kU/L) 43.23 34.78 38.1 62.45 59 47.58 34.81 45.6 62.3 53Proliferation (SI) 6.84 6.18 4.78 5.52 59 5.59 6.73 3.29 5.22 41IL-5 (pg/mL) 892.93 1963.66 329.66 793.15 59 384.4 549.35 194.82 515.00 41IL-13 (pg/mL) 848.54 1243.31 313.05 1206.3 59 875.31 783.25 1183.44 1494.64 41IFN-gamma (pg/mL) 97.81 123.61 55.67 139.94 59 58.39 101.85 26.93 72.73 41
HDM-specific regulatory responseCD4+CD25hi (% of CD3+) 0.44 0.26 0.39 0.32 59 0.88 0.46 0.73 0.44 41FoxP3 (relative expression) 3.22 2.41 2.39 2.47 59 2.8 1.75 2.4 2.65 41IL-10 (pg/mL) 81.75 157.33 21.32 95.02 59 21.81 39.0 9.24 24.7 41TGF-beta (pg/mL) 105.13 258.26 0.00 27.27 59 221.35 383.86 58.72 305.75 41
SD: standard deviation.IQR: Inter Quartile Range.
were comparable between year 0 and year 2 (Table 3,𝑃 > 0.05except for IFN-gamma which showed a significant decrease).Whereas values did not significantly increase or decrease,there was a significant correlation between data from year 0and year 2 for all these markers (𝑅
𝑠between 0.35 and 0.86),
except for IL-5 (𝑅𝑠= 0.27).
The frequency of regulatory CD4+CD25hi cells hadincreased two years after baseline measurement. However,other markers characteristic for regulatory cells (Foxp3, IL-10, TGF-beta) did not increase in time (in fact for IL-10 adecrease could be detected, Table 3). Correlations betweenyear 0 and year 2 for these variables were nonsignificant(except for IL-10).
Figure 1 summarizes the above-described findings witha decrease of clinical symptoms after 2 years in combi-nation with a positive correlation between data of year 0and year 2 (represented by nasal symptoms in Figure 1(a)),comparable skin-test values for year 0 and year 2, witha positive correlation between the two years (early skintest is presented in Figure 1(b)), no significant change inproinflammatory reactions (in Figure 1(c) represented asspec IgE) with a high correlation between measurementsduring the two years, and an increase of CD4+CD25hiTreg cells without a correlation between the two years ofmeasurement (Figure 1(d)). As can be seen in this figure,there is no difference in any of the values between patientsreceiving placebo treatment or verum-SLIT treatment (whichthey received during a period of two years in the originaltrial).
4. Discussion
Results of the present study show clinical symptoms rated byallergic patients at baseline and two years later in combinationwith immunological parameters measured in vivo or in vitro.In a time period of two years, clinical symptoms of the nose,eye, and lung significantly decrease in children with house-dust-mite-induced AR. Although children rate their allergycomplaints as being less than at the beginning of the study,this decrease is not reflected in a decrease of one of theimmunological parameters.
A possible explanation for the reduction of symptomsis that allergic rhinitis decreases in time. Whereas thereare many studies determining symptoms during followup ofSLIT treatment, there is little information on the possibilityof spontaneous remission of allergic rhinitis [12, 20]. Somestudies have reported the relationship between age andimprovement or decline of rhinitis over the years [21–23].During an 8-year follow-up of patients with allergic rhinitis,Nihlen et al. [21] found a 20% remission rate, which washigher in older patients. Broder et al. [22] described thatremission with allergic rhinitis was more likely when theduration of the disease was shorter than 5 years.
Another plausible explanation for the reduction of symp-toms might be that, due to participation in a study, patientsare more aware of their allergy and take more care oftheir complaints, which may result in a reduction of theirsymptoms. In this study, patients took (placebo) medicationduring a period of two years. The effect of placebo treatmentis substantial in patients participating in a study evaluatingSLIT.

Mediators of Inflammation 5
Table 3: Paired estimated difference between year 2, and 0 (median, CIs and 𝑃-value) and Spearman correlation.
Paired estimated difference CorrelationMedian 95% CI∗ Sign.# 𝑅
𝑠
† Sign.Clinical symptoms
Nose (score from 0–12) −1.34 −1.86 −0.85 <0.0001 0.56 <0.0001Eye (score from 0–9) −0.29 −0.62 −0.05 0.02 0.56 <0.0001Lung (score from 0–6) −0.33 −0.58 −0.13 <0.0001 0.61 <0.0001
HDM-specific skin testEarly skin test (HEIC) 0.16 −0.03 0.35 0.09 0.44 0.005Late skin test (mm2) 199.85 −12.55 458.2 0.07 0.5 0.001
HDM-specific pro-inflammatory responseSpecific IgE (kU/L) 1.95 −0.79 6.45 0.17 0.86 <0.0001Proliferation (SI) −0.67 −2.02 0.89 0.39 0.38 0.015IL-5 (pg/mL) −132.1 −450.62 69.51 0.19 0.27 0.087IL-13 (pg/mL) 133.92 −210.18 538.48 0.46 0.36 0.022IFN-gamma (pg/mL) −44.84 −82.33 −4.00 0.01 0.35 0.027
HDM-specific regulatory responseCD4+CD25hi (% of CD3+) 0.44 0.3 0.56 <0.0001 0.18 0.27FoxP3 (relative expression) −0.12 −0.67 0.41 0.64 0.24 0.13IL-10 (pg/mL) −39.34 −67.66 −10.56 0.002 0.357 0.024TGF-beta (pg/mL) 41.43 0.00 144.01 0.18 0.032 0.84
∗CI: confidence interval Hodges Lehman.#𝑃-value, Wilcoxon.𝑅𝑠†: Spearman rank correlation between year 0 and year 2.
Whereas from this study it becomes clear that complaintsof patients with AR decrease over time, it is demonstrated in abirth cohort study that the prevalence of patients developingAR increases over the time [24]. Therefore, when childrenget older the change of developing AR is increasing, but forthe patients with complaints of AR the change of havingcomparable complaints two years later is decreasing.
Skin responses (measured directly after intradermal aller-gen injection and a late response with induction of inflam-matory cells) remain constant over time. Whereas theseresponses are comparable at baseline and after two years,these data show a positive correlation, which means thatvalues which are high at baseline are also high after twoyears, and low values remain low during the two years. Ittherefore appears that sensitization persists even in the caseswith remission of symptoms. This is underlined by a studyof Bodtger and Linneberg [25] who describe that in adultpatientswith house dustmite allergy, only 5.5%of the patientsshow a remission of specific IgE after eight years, whereasremission of symptoms occurred in 32.4% of the patients.Also, a recent study of Kong et al. [26] describes that five yearsafter skin testing 96% remain skin test positive.
AR is characterized by high levels of allergen-specificIgE and secretion of the Th
2cytokines IL-4, IL-5 and IL-
13 [3, 27, 28]. In this study, we do not see a decrease ofthese inflammatory markers two years after the baselinemeasurement, whereas patients rate their symptoms as betterthan before. In contrast to our findings, in patientswhodonotreceive immunotherapy, allergen-specific T-cell responsescan be reduced by means of specific immunotherapy (SIT).
The literature shows that SIT is able to reduce allergiccomplaints in combination with a reduction of allergen-induced T-cell proliferation [14] and a shift in the Th2/Th1cytokine balance, favouring type-1 T cells [29]. This shiftcould be a result of either decreased IL-4 production afterallergen stimulation [14] or enhanced IFN-𝛾 expression [30].Some studies have found a reduction of allergen-specific IgEin combination with an increase of specific IgG levels dueto SIT [30–32]. In the large randomized study [16], of whichthis present study is a component, we determined IgG1 andIgG4 levels in 163 children at year 0 and year 2. These resultsshow that IgG levels remain constant over the time with avery high correlation between year 0 and year 2 (𝑅 is 0.74for IgG and 0.83 for IgG4), which emphasises that the dose ofallergen administratedmight have been insufficient to inducetolerance.
Different studies demonstrate the effect of immunother-apy on regulatory mechanisms [9–12]. They describe a sig-nificant increase of IL-10, and TGF-𝛽 in patients undergoingSIT compared to untreated atopic patients (or patients receiv-ing placebo). Moreover, the number of CD4+CD25+ cellsexpressing the transcription factor Foxp3 was increased afterallergen stimulation in the immunotherapy group [13]. Inour study, results related to regulatory T cells are conflicting.Whereas we see an increase of CD4+CD25+ cells, there isno correlation between data of year 0 and data of year 2.Moreover, othermarkers regarding regulation of the immuneresponse (i.e., Foxp3, IL-10 and TGF-beta) do not increase.In fact, IL-10 decreases in time. From this, it is unlikely thatregulatory cells play a role in this present study; self-rated

6 Mediators of Inflammation
0
2
4
6
8
10
12
0 2 4 6 8 10 12Nose—year 2
Nos
e—ye
ar 0
𝑅𝑠 = 0.56 𝑃 < 0.0001
(a)
4
3
2
1
0
43210
𝑅𝑠 = 0.44 𝑃 = 0.005
Early skin test—year 2
Early
skin
test—
year
0
(b)
0
20
40
60
80
100
0 20 40 60 80 100
Specific IgE—year 2
Spec
ific I
gE—
year
0
𝑅𝑠 = 0.86 𝑃 < 0.0001
(c)
0.5
1
0
1.5
2
0.5 10 1.5 2CD4+CD25hi —year 2
CD4+
CD25
hi—
year
0
𝑅𝑠 = 0.18 𝑃 = 0.27
(d)
Figure 1: Correlation between clinical and immunological values determined at baseline and two years later. (a) patient rated nose symptoms(𝑛 = 52), (b) response of early skin test (𝑛 = 42), (c) specific IgE (𝑛 = 53), and (d) regulatory CD4+CD25hi T cells (𝑛 = 41). Open bullets:verum SLIT-treatment during two years, closed bullets: placebo treatment during two years (see Section 2), dashed lines: median values, and𝑅𝑠: Spearman Rank test.
allergy symptoms do decrease, but this is not the result ofan increase of regulatory cells. However, we have to keep inmind that the number of patients used to answer this questionis small, and we should be conservative with respect to thisstatement.
A limitation of the present study is that only 42 out of 59children (71%) wanted to participate two years later. Some ofthese childrenwere lost to followup (a total of seven children),and others still participated in the main SLIT study but didnotwant to do additional skin testing or venapuncture (a totalof ten children). However, the total number of 42 children isstill an acceptable number to study possible immunologicalmechanisms in relation to symptoms in a period of two years.
From this study, it can be concluded that whereas, compa-rable to SIT, allergic complaints decrease, the immunologicalchanges of HDM-specific T-cell activity (both effector cells
and regulator cells) which are observed after immunotherapydo not change. This decrease in clinical symptoms might beexplained by the placebo effect, since patients participatedin a study and took (placebo) medication during a periodof two years. It may be concluded that SIT plays an activerole in tolerance induction in the patients immune system;whereas during the two years of this study, allergic complaintsreduce without any difference in immunological parametersas determined in this study.
Acknowledgments
The authors thank all patients and their parents for partic-ipation in the study and Margaretha Lambers (Departmentof Lung Diseases, Erasmus MC) for performing the labora-tory tests. This study was sponsored by ARTU-Biologicals,

Mediators of Inflammation 7
Lelystad,TheNetherlands.The authors declare that they haveno conflict of interests.
References
[1] J. L. Brozek, J. Bousquet, C. E. Baena-Cagnani et al., “AllergicRhinitis and its Impact on Asthma (ARIA) guidelines: 2010Revision,” Journal of Allergy and Clinical Immunology, vol. 126,no. 3, pp. 466–476, 2010.
[2] I. Hansen, L. Klimek, R. Mosges, and K. Hormann, “Mediatorsof inflammation in the early and the late phase of allergicrhinitis,” Current Opinion in Allergy and Clinical Immunology,vol. 4, pp. 159–163, 2004.
[3] E. W. Gelfand, “Inflammatory mediators in allergic rhinitis,”Journal of Allergy and Clinical Immunology, vol. 114, no. 5, pp.S135–S138, 2004.
[4] M. Wagenmann, L. Schumacher, and C. Bachert, “The timecourse of the bilateral release of cytokines and mediators afterunilateral nasal allergen challenge,” Allergy, vol. 60, no. 9, pp.1132–1138, 2005.
[5] M. Akdis, J. Verhagen, A. Taylor et al., “Immune responsesin healthy and allergic individuals are characterized by a finebalance between allergen-specific T regulatory 1 and T helper2 cells,” Journal of Experimental Medicine, vol. 199, no. 11, pp.1567–1575, 2004.
[6] S. Hori, T. Nomura, and S. Sakaguchi, “Control of regulatory Tcell development by the transcription factor Foxp3,” Science, vol.299, no. 5609, pp. 1057–1061, 2003.
[7] S. Romagnani, “Regulatory T cells: which role in the pathogen-esis and treatment allergic disorders?” Allergy, vol. 61, no. 1, pp.3–14, 2006.
[8] H. Groux, A. O’Garra, M. Bigler et al., “A CD4+ T-cell subsetinhibits antigen-specific T-cell responses and prevents colitis,”Nature, vol. 389, no. 6652, pp. 737–742, 1997.
[9] M. Jutel, M. Akdis, F. Budak et al., “IL-10 and TGF-𝛽 cooperatein the regulatory T cell response to mucosal allergens in normalimmunity and specific immunotherapy,” European Journal ofImmunology, vol. 33, no. 5, pp. 1205–1214, 2003.
[10] C. A. Akdis, T. Blesken, M. Akdis, B. Wuthrich, and K. Blaser,“Role of interleukin 10 in specific immunotherapy,” Journal ofClinical Investigation, vol. 102, no. 1, pp. 98–106, 1998.
[11] J. N. Francis, S. J. Till, and S. R. Durham, “Induction of IL-10+CD4+CD25+T cells by grass pollen immunotherapy,” Journalof Allergy and Clinical Immunology, vol. 111, no. 6, pp. 1255–1261,2003.
[12] A. O. Eifan, T. Akkoc, A. Yildiz et al., “Clinical efficacy andimmunological mechanisms of sublingual and subcutaneousimmunotherapy in asthmatic/rhinitis children sensitized tohouse dust mite: an open randomized controlled trial,” Clinicaland Experimental Allergy, vol. 40, no. 6, pp. 922–932, 2010.
[13] K. Nieminen, E. Valovirta, and J. Savolainen, “Clinical outcomeand IL-17, IL-23, IL-27 and FOXP3 expression in peripheralblood mononuclear cells of pollen-allergic children duringsublingual immunotherapy,” Pediatric Allergy and Immunology,vol. 21, pp. e174–e184, 2010.
[14] C. Ebner, U. Siemann, B. Bohle et al., “Immunological changesduring specific immunotherapy of grass pollen allergy: reducedlymphoproliferative responses to allergen and shift from TH
2
to TH1in T-cell clones specific for Phi p 1, a major grass pollen
allergen,” Clinical and Experimental Allergy, vol. 27, no. 9, pp.1007–1015, 1997.
[15] C. M. A. de Bot, H. Moed, M. Y. Berger et al., “Ran-domized double-blind placebo-controlled trial of sublingualimmunotherapy in children with house dust mite allergy inprimary care: study design and recruitment,” BMC FamilyPractice, vol. 9, article 59, 2008.
[16] C. M. de Bot, H. Moed, M. Y. Berger et al., “Sublingualimmunotherapy not effective in house dust mite allergic chil-dren in primary care,” Pediatric Allergy and Immunology, vol.23, no. 2, pp. 151–159, 2012.
[17] M. I. Asher, U. Keil, H. R. Anderson et al., “International studyof asthma and allergies in childhood (ISAAC): rationale andmethods,” European Respiratory Journal, vol. 8, no. 3, pp. 483–491, 1995.
[18] G. O. Solley, G. J. Gleich, R. E. Jordon, and A. L. Schroeter, “Thelate phase of the immediate wheal and flare skin reaction. Itsdependence upon IgE antibodies,” Journal of Clinical Investiga-tion, vol. 58, no. 2, pp. 408–420, 1976.
[19] H. Moed, R. Gerth Van Wijk, J. C. De Jongste, and J. C. VanDer Wouden, “Skin tests, T cell responses and self-reportedsymptoms in children with allergic rhinitis and asthma due tohouse dust mite allergy,” Clinical and Experimental Allergy, vol.39, no. 2, pp. 222–227, 2009.
[20] N. Pham-Thi, P. Scheinmann, R. Fadel et al., “Assessment ofsublingual immunotherapy efficacy in children with house dustmite-induced allergic asthma optimally controlled by phar-macologic treatment and mite-avoidance measures,” PediatricAllergy and Immunology, vol. 18, no. 1, pp. 47–57, 2007.
[21] U. Nihlen, L. Greiff, P. Montnemery et al., “Incidence andremission of self-reported allergic rhinitis symptoms in adults,”Allergy, vol. 61, pp. 1299–1304, 2006.
[22] I. Broder, M. W. Higgins, K. P. Mathews, and J. B. Keller, “Epi-demiology of asthma and allergic rhinitis in a total community,Tecumseh,Michigan. IV. Natural history,” Journal of Allergy andClinical Immunology, vol. 54, no. 2, pp. 100–110, 1974.
[23] T. M. Huurre, H. M. Aro, and J. J. K. Jaakkola, “Incidence andprevalence of asthma and allergic rhinitis: a cohort study ofFinnish adolescents,” Journal of Asthma, vol. 41, no. 3, pp. 311–317, 2004.
[24] M. Westman, P. Stjarne, A. Asarnoj et al., “Natural course andcomorbidities of allergic and nonallergic rhinitis in children,”Journal of Allergy and Clinical Immunology, vol. 129, pp. 403–408, 2012.
[25] U. Bodtger and A. Linneberg, “Remission of allergic rhinitis:an 8-year observational study,” Journal of Allergy and ClinicalImmunology, vol. 114, no. 6, pp. 1384–1388, 2004.
[26] W. Kong, J. Chen, Y. Wang et al., “A population-based 5-yearfollow-up of allergic rhinitis in Chinese children,” AmericanJournal of Rhinology and Allergy, vol. 26, pp. 315–320, 2012.
[27] E. A. Wierenga, M. Snoek, H. M. Jansen, J. D. Bos, R. A. W. VanLier, andM. L. Kapsenberg, “Human atopen-specific types 1 and2 T helper cell clones,” Journal of Immunology, vol. 147, no. 9, pp.2942–2949, 1991.
[28] S. Till, R. Dickason, D.Huston et al., “IL-5 secretion by allergen-stimulated CD4+ T cells in primary culture: relationship toexpression of allergic disease,” Journal of Allergy and ClinicalImmunology, vol. 99, no. 4, pp. 563–569, 1997.
[29] M. Jutel, W. J. Pichler, D. Skrbic, A. Urwyler, C. Dahinden, andU. R. Muller, “Bee venom immunotherapy results in decreaseof IL-4 and IL-5 and increase of IFN-𝛾 secretion in specificallergen-stimulated T cell cultures,” Journal of Immunology, vol.154, no. 8, pp. 4187–4194, 1995.

8 Mediators of Inflammation
[30] S. R. Durham and S. J. Till, “Immunologic changes associatedwith allergen immunotherapy,” Journal of Allergy and ClinicalImmunology, vol. 102, no. 2, pp. 157–164, 1998.
[31] M. G. Tari, M. Mancino, and G. Monti, “Efficacy of sub-lingual immunotherapy in patients with rhinitis and asthmadue to house dust mite. A double-blind study,” Allergologia etImmunopathologia, vol. 18, no. 5, pp. 277–284, 1990.
[32] K. Gehlhar,M. Schlaak,W.M. Becker, andA. Bufe, “Monitoringallergen immunotherapy of pollen-allergic patients: the ratio ofallergen-specific IgG4 to IgG1 correlates with clinical outcome,”Clinical and Experimental Allergy, vol. 29, no. 4, pp. 497–506,1999.

Hindawi Publishing CorporationMediators of InflammationVolume 2013, Article ID 760691, 8 pageshttp://dx.doi.org/10.1155/2013/760691
Clinical StudyEvaluation of Adipokines: Apelin, Visfatin, and Resistin inChildren with Atopic Dermatitis
Edyta Machura,1 Maria Szczepanska,1 Katarzyna Ziora,1 Dariusz Ziora,2
Elzbieta Swietochowska,3 MaBgorzata Barc-Czarnecka,1 and Alicja Kasperska-Zajac4
1 Department of Pediatrics, Medical University of Silesia, Ulica 3-go Maja 13-15, 41-800 Zabrze, Poland2Department of Pneumonology and Tuberculosis, Medical University of Silesia, Ulica Koziołka 1, 41-803 Zabrze, Poland3Department of Biochemistry, Medical University of Silesia, Ulica Jordana 19, 41-808 Zabrze, Poland4Department of Internal Diseases, Allergology and Clinical Immunology, Medical University of Silesia, Ulica Ceglana 35, 40-952Katowice, Poland
Correspondence should be addressed to Edyta Machura; [email protected]
Received 9 July 2012; Revised 27 December 2012; Accepted 28 December 2012
Academic Editor: Wilco de Jager
Copyright © 2013 Edyta Machura et al.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Very little is known about the role of adipokines in atopic dermatitis (AD) in children. This study aimed at analyzing theserum levels of resistin, apelin, and visfatin in children with AD in relation to body weight, AD severity, and gender. Serumconcentration of adipokines was measured in 27 children with AD and in 46 healthy subjects. Selected biochemical parameterswere evaluated and skin prick test was performed. Serum levels of resistin and apelin were significantly higher, whereas serumvisfatin concentration was significantly lower in children with AD versus healthy controls, although an increase in resistin levelswas exclusively demonstrated in boys. In AD group, a significant increase in apelin levels in girls was documented. There wasno relationship between adipokines levels and the degree of allergic sensitization. Receiver operating characteristic curve analysisdemonstrated that the serum apelin cutoff value differentiating children with AD from those without was >137.8 pg/mL. Resistinand visfatin cutoff values were >3.8 ng/mL and ≤ 2.13 ng/mL, respectively. Apelin and visfatin can serve as excellent indicators todistinguish children with AD from those without disease.
1. Introduction
Increasing literature evidence indicates that obesity is arisk factor for the development of asthma [1, 2]. Exactmechanisms for the links between obesity and asthma are notwell understood, although a possible role for adipokines hasbeen indicated [3, 4].
Recent studies showed that adipose tissue is far morethan a site for energy storage and it is in fact an activeendocrine, paracrine, and also immune organ secreting mul-tiple bioactivemediators, called adipokines.These adipokinesinclude hormones (leptin, adiponectin), cytokines (TNF-𝛼, IL-6, IL-10, and visfatin), and other proteins (apelin,resistin), which participate in numerous physiological andpathological processes [5, 6]. The deregulated synthesisand/or secretion of adipokines towards the proinflammatory
compounds was observed in obesity and obesity-relateddisorders [5]. In addition, several studies suggest that someof adipokines are involved in the pathogenesis of otherinflammatory disorders including asthma [7], inflammatorybowel disease [8], rheumatoid arthritis [9], and psoriasis[10]. Several reports pointed at the proinflammatory role ofleptin and anti-inflammatory role of adiponectin in asthma,but the data are currently equivocal [4, 7]. It seems thatanother adipokine, resistin, may be also involved in asthmapathogenesis and severity [11]. Our recent studies revealedaltered apelin and visfatin levels in childhood atopic asthma[12, 13].
In contrast to asthma, studies in children that investigatethe relationship between obesity and AD are few but withcontroversial results [2, 14]. Also data related to the role andpotential significance of adipokines in AD are limited [7].

2 Mediators of Inflammation
Since AD is characterized as a chronic inflammatory dis-order, we hypothesized that abnormalities in adipokineserum levels might occur. Therefore in the present study,we estimated apelin, visfatin, and resistin serum levels inchildren with AD.The adipokine concentrations were relatedto body weight and AD severity. Additionally, possible dif-ferences in adipokine levels between boys and girls were alsoexplored.
2. Materials and Methods
Twenty-seven children (mean age 9.9 ± 0.77 range 4.3–17.5 y)suffering from mild to severe AD were enrolled into thestudy. AD was diagnosed according to the criteria describedby Hanifin and Rajka [15]. The severity of dermatitis wasestimated according to the SCORAD index (ranging from 0to 103 points) [16]. Based on the total score, 6 children wereclassified as mild (<25 points), 12 children as moderate (25–50 points), and 9 children as severe (>50 points) AD. All thechildren had positive skin prick tests (SPTs) to ≥1 allergens. Apositive SPT was defined as a mean diameter of at least 3mmin the presence of negative diluents and positive histaminecontrols.The degree of allergic sensitization wasmeasured bythe whole size of SPTs. Children with concomitant asthmaand rhinitis were excluded from this study. The patientswere not treated with any antihistamines, topical steroids, orcalcineurin inhibitors for at least 1 week before enrolmentinto the study (only emollients were applied). They were freeof any systemic steroids during the preceding 8 weeks. Thecontrol group consisted of 46 healthy children (mean age11.04 ± 0.62, range 4−17 y) with a negative history of allergicdisease, the normal level of total serum IgE, and negativeresults of skin prick test to a panel of aeroallergens (dustmite, mixed grass or tree pollen, cat and dog; Allergopharma,Reinbek,Germany). Children included into the control groupattended the outpatient pediatric clinic for nonimmunolog-ical, noninflammatory health problems and needed venouspuncture.
The present study was approved by the Ethics Committeeof the Medical University of Silesia in Katowice. Writteninformed consent was obtained from children’s parents.
2.1. Specific Measurements
2.1.1. AnthropometricMeasurements. Bodymass index (BMI)(body weight (kg)/height squared (m−2), and standard devi-ation (SD) score for BMI (BMI-SDS) were calculated accord-ing to the current Polish population normal range [17].
2.1.2. Biochemical Measurements. The fasting blood sampleswere collected in themorning between 7:00AMand 9:30AMfollowing an overnight fasting. The serum was separated bycentrifugation at 1300 g for 10min at +4∘C and immediatelystored at −70∘C until analyzed. Biochemical parameters,including C-reactive protein (CRP), triglycerides (TGs), totalcholesterol (TC), and high-density lipoprotein cholesterol(HDL-C), were measured, using chemistry analyzer (Cobas
6000, Roche Diagnostic, Switzerland). Low-density lipopro-tein cholesterol (LDL-C) was calculated by the Friedewaldformula (LDL-C = TC −HDL-C − TG/5).
2.1.3. Apelin, Visfatin, and Resistin Measurements. Serumvisfatin C-terminal and apelin-12 concentrations were mea-sured by commercial enzyme immunoassay kit according tothe manufacturer’s protocol (human recombinant visfatin C-terminal, human recombinant apelin-12 (Phoenix Pharma-ceuticals, Inc., Burlingame, CA, USA)). The concentrationsof apelin-12 and visfatin C-terminal were determined onthe basis of standard curve carried out for serial dilutionavailable in kit standards. Absorbance was measured usingspectrophotometer (𝜇Quant, Microplate Reader, Bio-Tek,Winooski, VT, USA) at 450 nm wavelengths. Acquired datawere analyzed using KC Junior Software (v.1.31.5, Bio-TekInstruments, Winooski, VT, USA). The sensitivity valuesfor visfatin and apelin-12 were 2.17 ng/mL and 0.07 ng/mL,respectively. The intra- and interassay errors for visfatin were<10% and<15% and 8.2% and<15% for apelin-12, respectively.
Serum resistin concentration was measured by com-mercially available enzyme-linked immunosorbent assay kit(Mediagnost, Reutlingen, Germany). The concentration ofresistinwas determined on the basis of standard curve carriedout for serial dilution available in kit standards (humanrecombinant resistin). Immunocomplex detection was deter-mined on the basis of reaction with rabbit polyclonal anti-body antihuman immunoglobulin (IgG) conjugated withhorseradish peroxides and then with TMB substrate solution(TMB substrate, slow kinetic, Sigma-Aldrich, St. Louis, MO,USA). Absorbance was measured using spectrophotometer(𝜇Quant, Microplate Reader, Bio-Tek, Winooski, VT, USA)at 450 nm wavelengths. Acquired data were analyzed usingKC Junior Software (v.1.31.5, Bio-Tek Instruments, Winooski,VT, USA). The sensitivity for resistin was 0.012 ng/mL, andthe intra- and interassay errors were 4.66% and 4.79%,respectively.
2.2. Statistical Analysis. The statistical analysis was per-formed using Statistica 6.0 software (StatSoft, Inc., Tulsa,OK, USA) and data presented as mean values ± SE. Mann-Whitney 𝑈 test was used for comparisons between groups.Correlations were calculated using the Spearman rank test.Accuracy of the diagnostic adipokines measurement test wasassessed using the receiver operating characteristic (ROC)curve analysis. ROC analysis was performed using MedCalcsoftware (v11.3.5.0). For all tests, values of 𝑃 < 0.05 wereconsidered statistically significant.
3. Results
Characteristics of the 27 children with AD and the 46 healthycontrol subjects are presented in Table 1. Both groups weresimilar in age (𝑃 = NS). In AD group, 25.79% (𝑛 = 6) ofchildren were obese as well as 13.04% (𝑛 = 6) in healthychildren. Despite this, the mean values of BMI and BMI-SDS of AD children were similar as compared to those ofthe healthy group. Normal weight was defined as BMI-SDS

Mediators of Inflammation 3
Table 1: Demographic and clinical characteristics of children withatopic dermatitis and healthy children.
Characteristics Children with AD(𝑛 = 27)
Healthychildren(𝑛 = 46)
Age, years, mean ± SE 9.9 ± 0.99 11.7 ± 3.7
Sex, 𝑛 M: 10; F: 17 M: 19; F: 27Duration of AD, years,mean ± SE 6.24 ± 0.37 —
SCORAD, mean ± SE 47.67 ± 67
Serum total IgE, IU/mL,mean ± SE 768.23 ± 174.3# 50.11 ± 0.93
Eosinophils, % (𝑛,cells/𝜇L), mean ± SE
8.5 ± 1.38‡ 2.21 ± 0.4
(488.4 ± 80.61)† (155.05 ± 13.42)Positive SPT, 𝑛 (%) 100 (100) 0Total SPT wheal size, mm,mean ± SE 22.9 ± 2.43 —
BMI 18.1 ± 1.44 18.76 ± 0.56
BMI-SDS 0.83 ± 0.41 0.18 ± 0.26
CRP (mg/L) 2.68 ± 1.9 1.01 ± 0.2
TG (mmol/L) 1.09 ± 0.13 0.97 ± 0.04
TC (mmol/L) 4.34 ± 0.015 3.99 ± 0.03
LDL-C (mmol/L) 2.29 ± 0.015 1.99 ± 0.06
HDL-C (mmol/L) 1.86 ± 0.01 1.5 ± 0.02
BMI: body mass index; BMI-SDS: body mass index-standard deviationscores; CRP: C-reactive protein; FEV1, HDL-C: high-density lipoproteincholesterol; IgE: immunoglobulin E; IU: international unit; LDL-C: low-density lipoprotein cholesterol; SE: standard error; SPT: skin prick test; TC:total cholesterol; TG: triglyceride.All 𝑃 values from Mann-Whitney’s 𝑈-test. ‡𝑃 < 0.05, †𝑃 < 0.01, and #
𝑃 <
0.0002.
between −2.0 and +2.0. Obesity was defined as BMI-SDS >2.0. Underweight was defined as BMI-SDS < −2. Childrenwith AD had higher IgE levels and higher percentage andblood eosinophil numbers.
3.1. Comparison of Serum Adipokine Levels between Childrenwith AD and Control Group. Mean values of serum levelsof apelin, visfatin, and resistin in all children are shown inTable 2. Serum levels of apelin and resistin were significantlyhigher in the total group of AD children than those of controlgroup (𝑃 < 0.001, 𝑃 < 0.003). However, the increase in theresistin level was seen only in boys. In contrast, serum visfatinlevel was significantly lower in AD children as compared tothat of healthy subjects (𝑃 < 0.001). In AD children, afterstratifying by gender, there was a significant increase in apelinlevels in girls as compared to those of boys (𝑃 < 0.01).On the other hand, no differences in any measured clinicaland laboratory parameters, including age, BMI, BMI-SDS, orseverity of disease between boys and girls, were observed.In the control group, serum levels of all adipokines weresignificantly higher in girls than in boys (𝑃 < 0.001).
3.2. Comparison of Serum Adipokine Levels/BMI Ratiobetween Children with AD and Control Group. As serum
Table 2: Mean values of adipokine serum levels in children withatopic dermatitis and healthy children.
Mean adipokineserum levels
Children with AD(𝑛 = 27; M/F: 10/17)
Healthy children(𝑛 = 46; M/F: 19/27)
Apelin, pg/mLAll subjects 157.52 ± 2.76 130.18 ± 0.89∗
Boys 149.10 ± 4.42 124.69 ± 0.76∗
Girls 162.47 ± 3.01‡ 134.05 ± 0.84∗∧
Visfatin, ng/mLAll subjects 1.84 ± 0.04 2.54 ± 0.03∗
Boys 1.78 ± 0.03 2.37 ± 0.03∗
Girls 1.88 ± 0.05 2.66 ± 0.03∗∧
Resistin, ng/LAll subjects 4.07 ± 0.03 3.82 ± 0.05†
Boys 4.04 ± 0.05 3.46 ± 0.04∗
Girls 4.09 ± 0.03 4.07 ± 0.04∧
Data as shown as mean ± standard error. 𝑃 values fromMann-Whitney’s𝑈-test. ∗𝑃 < 0.001 AD versus control.†𝑃 < 0.003 AD versus control.‡𝑃 < 0.01 AD girls versus AD boys.∧𝑃 < 0.001 healthy girls versus healthy boys.
Table 3: The adipokine serum levels/BMI ratio in AD children andhealthy controls.
Adipokine serumlevels/BMI
Children with AD(𝑛 = 27; M/F: 10/17)
Healthy children(𝑛 = 46; M/F: 19/27)
Apelin pg/mL/BMI(kg/m2)
All subjects 9.06 ± 0.20 7.18 ± 0.19∗
Boys 8.54 ± 0.28 7.3 ± 0.66
Girls 9.37 ± 0.42 7.09 ± 0.36∗
Visfatin ng/mLBMI/(kg/m2)
All subjects 0.11 ± 0.00 0.14 ± 0.00∗
Boys 0.10 ± 0.01 0.14 ± 0.01∗
Girls 0.11 ± 0.01 0.14 ± 0.01∗
Resistin ng/mL/BMI(kg/m2)
All subjects 0.23 ± 0.01 0.21 ± 0.01
Boys 0.23 ± 0.02 0.20 ± 0.01
Girls 0.24 ± 0.01 0.21 ± 0.01
Data as shown as mean ± standard error. P values fromMann-Whitney’s𝑈-test.∗AD versus control 𝑃 < 0.001.
adipokine levels are dependent on the amount of adiposetissue, adipokine levels were adjusted for BMI by dividing themeasured concentration by BMI. Mean values of adipokineserum levels/BMI ratios are shown in Table 3. We foundthat apelin levels/BMI ratio was significantly higher andvisfatin level/BMI ratio was lower in children with AD whencompared with healthy children (𝑃 < 0.001). However, asignificant increase in apelin level/BMI ratio was seen only ingirls. The apelin/BMI ratio showed no difference in compar-ison to the control group (𝑃 = 0.08). No difference between

4 Mediators of Inflammation
BMI adjusted serum concentrations of resistin between ADchildren and healthy subjects was found. After stratifying bygender, there was no difference in adipokines/BMI ratio inthe particular groups both in AD and in healthy children.Among the 73 children enrolled in this study, there were18 normal-weight children with AD and 38 healthy normalweights. No differences in serum resistin, visfatin, and apelinlevels between normal weight and obese AD children wereobserved as well (data not shown).
3.3. Correlations between Adipokines and Clinical and Labo-ratory Parameters. Wehave documented only few significantcorrelations between adipokines levels and other parameters(Table 4).
In children with AD, a strong positive correlation wasfound between visfatin concentration and TG levels. Inaddition, serum apelin levels correlated positively with serumvisfatin levels. Serum resistin levels inversely correlated withage of AD children. Adipokines showed no correlation withBMI and BMI-SDS, SCORADindex, duration of AD, andwith degree of allergic sensitization. SCORADindex valuescorrelated exclusively with serum IgE levels. No correlationwas found between BMI and severity of AD.
No correlation between age, BMI and BMI-SDS, IgE, andserum adipokines was found in examined healthy children,but strong positive correlation between serum TG levels andresistin, visfatin, and apelin was observed. In addition incontrol group, serum levels of resistin correlated significantlywith both serum visfatin and apelin levels; also serum apelinlevel correlated with serum visfatin level.
In order to evaluate the diagnostic value of serumadipokine levels for differentiation children with AD fromall examined children, we performed receiver operatingcharacteristic analysis (ROC). When the cutoff value forapelin was set to 137.8 pg/mL, the sensitivity and specificityfor AD were 96.3% (95% CI: 81.0–99.9) and 86.96% (95%CI: 73.7–95.1), respectively. For resistin, the cut-off valuewas ≥3.8 ng/mL, the sensitivity and specificity for AD were96.3% (95% CI: 81.0−99.0) and 52.17 (95% CI: 36.9–67.1),and for visfatin the cut-off value was ≤2.13, the sensitivityand specificity were 92.59% (95% CI: 75.7–99.1%) and 97.83(95% CI: 88.5–99.9%) (Figure 1). The area under the ROCfor apelin was 0.981, and for visfatin was 0.988 indicatingthat serum levels of both adipokines are the best biomarkersdifferentiating subjects with atopic dermatitis from healthychildren (Figure 2).
4. Discussion
The current study was designed to examine the circulatingapelin, resistin, and visfatin levels in children with AD,who had no current additional allergic symptoms such asasthma and allergic rhinitis. To eliminate the possible effectof obesity on adipokine levels, BMI adjusted serum concen-tration of adipokines was also assessed. We demonstratedthat in children with AD elevated apelin concentrations andapelin/BMI ratio are accompanied by decreased visfatin levelsand visfatin/BMI ratio. However, an increase in apelin/BMI
Table 4: Significant correlations between adipokine serum levelsand other parameters in children with atopic dermatitis and healthychildren.
Examined significant correlation 𝑅 𝑃
Atopic dermatitisVisfatin and triglycerides 0.97 0.02Visfatin and apelin 0.49 0.008Resistin and age −0.41 0.03SCORAD and IgE 0.65 0.0002
Healthy controlsVisfatin and TG 0.97 0.03Resistin and TG 0.99 0.001Apelin and TG 0.99 0.0003Resistin and apelin 0.98 0.019Resistin and apelin 0.9 0.004Apelin and visfatin 0.96 0.03
Spearman’s rank test, 𝑃 < 0.05; TG: triglyceride.
ratio was seen only in girls. Moreover, the difference in alladipokine levels betweenADand healthy childrenwas found,despite similar body weight. This finding suggests that theseadipokines may be implicated in the immunopathogenesis ofAD, independently of their confirmed role in obesity.
Data about the behaviour of adipokines inADare limited.Only three studies evaluating leptin or adiponectin in ADwere conducted. Nagel et al. showed a negative associationbetween serum adiponectin levels and atopic dermatitis, andever diagnosed eczema, and found no association betweencirculating leptin concentration and AD symptoms in chil-dren [7]. They also did not confirm the significant differencein serum leptin between AD children and control group.It was in accordance with the study of Bostanci et al. Thismanuscript has documented additionally that local steroidapplication did not influence circulating leptin levels [18].In contrast to this data, Kimata documented elevated serumleptin in AD children [19]. The role of adipokines such asapelin, visfatin, and resistin in patients with AD has not beeninvestigated so far.
Apelin is a more recently identified adipokine, whichexists in different isoforms, and acts thorough the binding toa specific G-protein-coupled receptor named API, present onendothelial cells, vascular smooth myocytes, and cardiomy-ocytes [20, 21]. Apelin synthesis in adipocytes is stronglyupregulated by insulin, and plasma apelin level markedlyincreases in obese and hyperinsulinemic mice and humans[22] its excretion is induced by hypoxia [23]. In addition,TNF-alpha may act as a key player in the upregulationof apelin expression in adipocytes both in obese and leanhuman [24]. It has been reported that apelin has a regulatoryeffect on cardiovascular system, appetite, drinking behav-iors, neoangiogenesis, lymphangiogenesis, fibrogenesis, andtumor growth [25, 26]. However, the data on apelin arecontroversial. Lately, Reinehr et al. in their longitudinal studyrevealed the lack of association between apelin and obesity inchildren [27].
The possible role of apelin in allergic inflammation hasnot been widely studied in both human and animal models,

Mediators of Inflammation 5
120
130
140
150
160
170
180
190
Apel
in (p
g/m
L)
Control AD
>137.8
Specificity:
Sensitivity:96.3
87
(a)
≤2.13Sensitivity:
Specificity:
1.4
1.6
1.8
2
2.2
2.4
2.6
2.8
3
Visf
atin
(ng/
mL)
Control AD
92.6
97.8
(b)
3
3.2
3.4
3.6
3.8
4
4.2
4.4
4.6
Resis
tin(n
g/m
L)
Control AD
>3.8Sensitivity:
Specificity:52.2
96.3
(c)
Figure 1: Interactive dot diagram comparing levels of (a) apelin, (b) visfatin, and (c) resistin levels between children with atopic dermatitisand healthy children.
yet. However, in our previous papers we confirmed highapelin concentration in children with asthma [12].
The origin and the role of increased apelin levels in serumamong examined children with AD remain unclear. Sinceneoangiogenesis is a feature of AD skin lesion [28], it seemsthat apelinmay be involved also in this chronic inflammatorydisorder.
Surprisingly, among children with AD we observed adecreased serum level of visfatin compared with healthy chil-dren, and this finding suggests that visfatinmayhave a protec-tive effect against AD in children. We have also documentedin children with atopic asthma similar reduced concentrationof visfatin [13]. In this study, we excluded children presentingsimultaneously with both AD and asthma symptoms tolink the adipokines changes exclusively to AD. Visfatin(PBEF-pre-B cell, colony-enhancing factor) is a growth factorfor early B-lymphocytes, and it is highly expressed andsecreted by human visceral fat (hence the term “visfatin”)[29]. Plasma concentration of visfatin strongly correlateswith the amount of fat. Visfatin upregulates the productionof the pro- and anti-inflammatory cytokines, for example,interleukin-1𝛽, (IL-1𝛽), TNF-𝛼, IL-1Ra, IL-6, and IL-10 and
increases the surface expression of costimulatory molecules,for example, CD54, CD40, and CD80 in monocytes [8].Moreover, visfatin enhances production of chemokines suchas CXCL8, CXCL10, and CCL20 in human keratinocytes[30]. Increased visfatin expression and/or visfatin plasmaconcentrations have been identified in a variety of chronicinflammatory diseases, including rheumatoid arthritis [9],inflammatory bowel disease [8], and psoriasis [10]. There areconflicting reports about the relationship between obesityand circulating levels of visfatin. Some researchers reportedincreased visfatin plasma levels in obese adult women [31]or obese children [32], whereas others observed no apparentrelationship between overweight and/or obesity and serumvisfatin concentrations [33], or even noted a negative corre-lation [34].
We observed significantly higher levels of serum resistinin AD than in controls, but this feature was seen only in boys.However, BMI adjusted serum concentration of resistin wassimilar in both groups. Our results suggest that the globalincrease in resistin levels in our AD boys might correlatewith the amount of adipose tissue. Further studies shouldexplore if resistin may be one of the factors explaining

6 Mediators of Inflammation
0
20
40
60
80
100
Sens
itivi
ty
0 20 60 80 10040100-specificity
Apelin (pg/mL)Visfatin (ng/mL)Resistin (ng/mL)
Apelin 0.981 0.019Resistin 0.683 0.067
Visfatin 0.988 0.012
Adipokine serum levels
Area under the ROC curve Standard error 95% confidence
interval0.918–0.999
0.563–0.787
0.928–1.000
Figure 2: Comparison of receiver operating characteristic (ROC)curves for apelin, resistin, and visfatin between children with atopicdermatitis and healthy children.
the relation between obesity and AD. There are only fewpublications on resistin in human asthma. One study of chil-dren showed a protective association between serum resistinconcentration and risk for asthma [35]. On the contrary,LaRochelle et al. documented that plasma resistin levelswere significantly higher in adult patients with moderate-to-severe persistent asthma than in control and increasedwith disease severity [11]. However, Arshi et al. did notfind any difference in resistin levels between children withasthma and healthy children [36]. Resistin is expressed inbrown and white adipose tissues and is a member of thefamily of cysteine-rich proteins called resistin-like molecules[37]. Circulating monocytes and macrophages seem to beresponsible for resistin production in human [5]. Resistin hasproinflammatory properties and upregulates the expressionof monocyte chemoattractant protein 1 (MCP-1) as well asvascular cell adhesionmolecule 1 (VCAM-1) and intercellularadhesion molecule 1 (ICAM-1) in endothelial cells, whichhave been known to contribute in the pathogenesis of allergicinflammation [5]. Macrophage exposure to resistin has beenshown to induce expression of tumor necrosis factor-alpha(TNF-alpha) and IL-12 and IL-6 [38].
In the current study, also obese AD children had sim-ilar levels of all adipokines as normal-weight AD children.
The lack of relationship between adipokine levels and BMIor BMI-SDS may be explained by differences in fat distri-bution. Unfortunately in this study, the measures of centralobesity were not estimated. Since visceral fat is supposedto be more metabolically active than subcutaneous fat, thecorrelation of adipokine levels and central obesity requiresfurther evaluation. We have not found difference in serumadipokine levels in different degrees of both AD severity andallergic sensitization and total IgE. Additionally, the degreeof AD severity showed no correlation with obesity. Recently,Silverberg et al. in a retrospective case-control study found anassociation between prolonged obesity (>2,5 years) in earlychildhood and increased odds ratio of AD and severity ofAD. Nevertheless, they performed their examination withoutthe application of a widely established AD scoring systems(SCORAD, Eczema Area and Severity Index) [2].
We demonstrated a significant difference in serum apelinlevels between boys and girls including children with AD.In the control group, sex differences in apelin, resistin, andvisfatin levels were observed. It should be emphasized, thatother studies in children and adolescents have shown girls tohave greater resistin concentration [39], but gender-relateddifferences in visfatin levels were not observed [31]. Themost interesting finding, which is the strength of the currentstudy, is that apelin and visfatin serve as good markersdifferentiating AD children from healthy ones. However, it isdifficult to establish if altered adipokine levels play a causativerole in AD or if they have changed secondary to chronicallergic inflammation.
The study has some limitations. Firstly, the sample sizewas rather small to represent all the children with atopicdermatitis. This was because the children were selectedaccording to specific criteria—high total and specific IgE orpositive SPT, without rhinitis or asthma. It is very difficultto collect an extensive number of AD children withoutconcomitant disorder whichmay affect adipokine concentra-tions. Secondly, the wide range of age in examined childrenwith AD, although similar to control, may be considered as adrawback of this study. Thirdly, a cross-sectional analysis ofthis study precludes any temporal or cause-effect conclusions.
In conclusion, this preliminary study provides the evi-dence of significantly higher apelin and decreased level ofvisfatin in atopic dermatitis. Additional prospective studieswith a larger number of patients and application of otheradipokines are needed to clarify the precise mechanismand their significance in the immunopathogenesis of AD inchildren.
Funding
Thiswork was financially supported byGrants KNW-1-103/10from the Medical University of Silesia in Katowice, Poland.
References
[1] M. E. Jensen, C. E. Collins, P. G. Gibson, and L. G. Wood,“The obesity phenotype in children with asthma,” PaediatricRespiratory Reviews, vol. 12, no. 3, pp. 152–159, 2011.

Mediators of Inflammation 7
[2] J. I. Silverberg, E. Kleiman, H. Lev-Tov et al., “Associationbetween obesity and atopic dermatitis in childhood: a case-control study,” Journal of Allergy and Clinical Immunology, vol.127, no. 5, pp. 1180–1186, 2011.
[3] S. A. Shore, “Obesity, airway hyperresponsiveness, and inflam-mation,” Journal of Applied Physiology, vol. 108, no. 3, pp. 735–743, 2010.
[4] T. Jartti, L. Saarikoski, L. Jartti et al., “Obesity, adipokines andasthma,” Allergy, vol. 64, no. 5, pp. 770–777, 2009.
[5] N. Ouchi, J. L. Parker, J. J. Lugus, and K. Walsh, “Adipokines ininflammation andmetabolic disease,”Nature Reviews Immunol-ogy, vol. 11, no. 2, pp. 85–97, 2011.
[6] N.Maenhaut and J. Van deVoorde, “Regulation of vascular toneby adipocytes,” BMCMedicine, vol. 16, pp. 9–25, 2011.
[7] G. Nagel, W. Koenig, K. Rapp, M. Wabitsch, I. Zoellner,and S. K. Weiland, “Associations of adipokines with asthma,rhinoconjunctivitis, and eczema in German schoolchildren,”Pediatric Allergy and Immunology, vol. 20, no. 1, pp. 81–88, 2009.
[8] A. R. Moschen, A. Kaser, B. Enrich et al., “Visfatin, anadipocytokine with proinflammatory and immunomodulatingproperties,” Journal of Immunology, vol. 178, no. 3, pp. 1748–1758, 2007.
[9] M. Otero, R. Logo, R. Gomez et al., “Changes in plasma levels offat-derived hormones adiponectin, leptin, resistin and visfatinin patients with rheumatoid arthritis,” Annals of the RheumaticDiseases, vol. 65, no. 9, pp. 1198–1201, 2006.
[10] H. Nakajima, K. Nakajima, M. Tarutani, R. Morishige, and S.Sano, “Kinetics of circulatingTh17 cytokines and adipokines inpsoriasis patients,”Archives of Dermatological Research, vol. 303,no. 6, pp. 451–455, 2011.
[11] J. LaRochelle, J. Freiler, J. Dice, and L. Hagan, “Plasma resistinlevels in asthmatics as a marker of disease state,” Journal ofAsthma, vol. 44, no. 7, pp. 509–513, 2007.
[12] E. Machura, K. Ziora, D. Ziora et al., “Serum apelin-12 levelis elevated in schoolchildren with atopic asthma,” RespiratoryMedicine, vol. 107, no. 2, pp. 196–201, 2012.
[13] E. Machura, K. Ziora, D. Ziora et al., “Serum visfatin levelsare decreased in schoolchildren with atopic asthma,” Neuroen-docrinology Letters, vol. 33, pp. 559–564, 2012.
[14] D. Van Gysel, E. Govaere, K. Verhamme, E. Doli, and F. DeBaets, “Body mass index in Belgian schoolchildren and itsrelationshipwith sensitization and allergic symptoms,”PediatricAllergy and Immunology, vol. 20, no. 3, pp. 246–253, 2009.
[15] J. M. Hanifin and G. Rajka, “Diagnostic features of atopicdermatitis,” Acta Dermato-Venereologica, vol. 92, pp. 44–47,1980.
[16] European Task Force on Atopic Dermatitis, “Severity scoring ofatopic dermatitis: the SCORAD index,” Dermatology, vol. 186,pp. 23–31, 1993.
[17] I. Palczewska and Z. Niedzwiedzka, “Somatic developmentindices in children and youth of Warsaw,” Medycyna WiekuRozwojowego, vol. 5, supplement 1, pp. 18–118, 2001.
[18] I. Bostanci, O. Atli, N. Celebi, A. Tasar, E. Alpkarakoc, and Y.Dallar, “Serum leptin level in children with atopic dermatitis-treated topical steroids,” Pediatric Allergy and Immunology, vol.15, no. 3, pp. 267–269, 2004.
[19] H. Kimata, “Elevated serum leptin in AEDS,”Allergy, vol. 57, no.2, p. 179, 2002.
[20] K. Tatemoto, M. Hosoya, Y. Habata et al., “Isolation andcharacterization of a novel endogenous peptide ligand for thehuman APJ receptor,” Biochemical and Biophysical ResearchCommunications, vol. 251, no. 2, pp. 471–476, 1998.
[21] M. J. Kleinz, J. N. Skepper, and A. P. Davenport, “Immunocy-tochemical localisation of the apelin receptor, APJ, to humancardiomyocytes, vascular smooth muscle and endothelial cells,”Regulatory Peptides, vol. 126, no. 3, pp. 233–240, 2005.
[22] J. Boucher, B. Masri, D. Daviaud et al., “Apelin, a newlyidentified adipokine up-regulated by insulin and obesity,”Endocrinology, vol. 146, no. 4, pp. 1764–1771, 2005.
[23] K.Geiger, A.Muendlein,N. Stark et al., “Hypoxia induces apelinexpression in human adipocytes,” Hormone and MetabolicResearch, vol. 43, no. 6, pp. 380–385, 2011.
[24] D. Daviaud, J. Boucher, S. Gesta et al., “TNFalpha up-regulatesapelin expression in human and mouse adipose tissue,” TheFASEB Journal, vol. 20, no. 9, pp. 1528–1530, 2006.
[25] C. Carpene, C. Dray, C. Attane et al., “Expanding role for theapelin/APJ system in physiopathology,” Journal of Physiologyand Biochemistry, vol. 63, no. 4, pp. 359–373, 2007.
[26] S. Rayalam, M. A. Della-Fera, T. Kasser, W. Warren, and C. A.Baile, “Emerging role of apelin as a therapeutic target in cancer:a patent review,” Recent Patents on Anti-Cancer Drug Discovery,vol. 6, pp. 367–372, 2011.
[27] T. Reinehr, J. Woelfle, and C. L. Roth, “Lack of associationbetween apelin, insulin resistance, cardiovascular risk factors,and obesity in children: a longitudinal analysis,” Metabolism,vol. 60, pp. 1349–1354, 2011.
[28] D. A. Groneberg, C. Bester, A. Grutzkau et al., “Mast cellsand vasculature in atopic dermatitis—potential stimulus ofneoangiogenesis,” Allergy, vol. 60, no. 1, pp. 90–97, 2005.
[29] A. Fukuhara, M. Matsuda, M. Nishizawa et al., “Visfatin: aprotein secreted by visceral fat that Mimics the effects ofinsulin,” Science, vol. 307, no. 5708, pp. 426–430, 2005.
[30] N. Kanda, C. S. Hau, Y. Tada, A. Tatsuta, S. Sato, and S.Watanabe, “Visfatin enhances CXCL8, CXCL10, and CCL20production in human keratinocytes,” Endocrinology, vol. 152,no. 8, pp. 3155–3164, 2011.
[31] B. Zahorska-Markiewicz, M. Olszanecka-Glinianowicz, J.Janowska et al., “Serum concentration of visfatin in obesewomen,”Metabolism, vol. 56, no. 8, pp. 1131–1134, 2007.
[32] S. Araki, K. Dobashi, K. Kubo et al., “Plasma visfatin concentra-tion as a surrogatemarker for visceral fat accumulation in obesechildren,” Obesity, vol. 16, no. 2, pp. 384–388, 2008.
[33] C. C. Chen, T. C. Li, C. I. Li et al., “The relationship betweenvisfatin levels and anthropometric and metabolic parameters:association with cholesterol levels in women,” Metabolism, vol.56, no. 9, pp. 1216–1220, 2007.
[34] C. Pagano, C. Pilon, M. Olivieri et al., “Reduced plasmavisfatin/pre-B cell colony-enhancing factor in obesity is notrelated to insulin resistance in humans,” Journal of ClinicalEndocrinology and Metabolism, vol. 91, no. 8, pp. 3165–3170,2006.
[35] K. W. Kim, Y. H. Shin, K. E. Lee, E. S. Kim, M. H. Sohn, and K.E. Kim, “Relationship between adipokines and manifestationsof childhood asthma,” Pediatric Allergy and Immunology, vol.19, no. 6, pp. 535–540, 2008.
[36] M. Arshi, J. Cardinal, R. J. Hill, P. S. W. Davies, and C. Wain-wright, “Asthma and insulin resistance in children,” Respirology,vol. 15, no. 5, pp. 779–784, 2010.
[37] C. M. Steppan, S. T. Bailey, S. Bhat et al., “The hormone resistinlinks obesity to diabetes,”Nature, vol. 409, no. 6818, pp. 307–312,2001.
[38] S. Leivo-Korpela, L. Lehtimaki, K. Vuolteenaho et al., “Adipo-kine resistin predicts anti-inflammatory effect of glucocorti-coids in asthma,” Journal of Inflammation, vol. 8, article 12, 2011.

8 Mediators of Inflammation
[39] M. Gerber, A. Boettner, B. Seidel et al., “Serum resistin levels ofobese and lean children and adolescents: biochemical analysisand clinical relevance,” Journal of Clinical Endocrinology andMetabolism, vol. 90, no. 8, pp. 4503–4509, 2005.

Hindawi Publishing CorporationMediators of InflammationVolume 2012, Article ID 143428, 7 pagesdoi:10.1155/2012/143428
Research Article
Circulating Cytokines and Growth Factors in PediatricPulmonary Hypertension
Mark Duncan,1, 2, 3, 4 Brandie D. Wagner,5 Keri Murray,1 Jenna Allen,1 Kelley Colvin,6
Frank J. Accurso,1 and D. Dunbar Ivy6
1 Section of Pediatric Pulmonology, School of Medicine, University of Colorado and Children’s Hospital Colorado,Aurora, CO 80045, USA
2 Obesity Research Center, King Saud University, Riyadh, Saudi Arabia3 Biodesix Inc., Boulder, CO 80045, USA4 Division of Endocrinology, Metabolism and Diabetes, School of Medicine, University of Colorado Denver, MS 8106,12801 E. 17th Avenue, RC 1 South, Room 7103, Aurora, CO 80045, USA
5 Department of Biostatistics and Informatics, Colorado School of Public Health, University of Colorado Denver,Aurora, CO 80045, USA
6 Section of Pediatric Cardiology, School of Medicine, University of Colorado and Children’s Hospital Colorado,Aurora, Colorado 80045, USA
Correspondence should be addressed to Mark Duncan, [email protected]
Received 23 June 2012; Revised 25 October 2012; Accepted 15 November 2012
Academic Editor: Dirk Holzinger
Copyright © 2012 Mark Duncan et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background. Management of pediatric pulmonary hypertension (PH) remains challenging. We have assessed a panel of circulatingproteins in children with PH to investigate their value as predictive and/or prognostic biomarkers. From these determinations,we aim to develop a practical, noninvasive tool to aid in the management of pediatric PH. Methods. Twelve cytokines and growthfactors putatively associated with lung or vascular disease were examined in plasma specimens from 70 children with PH usingmultiplex protein array technology. Associations between hemodynamics, adverse events, and protein markers were evaluated.Results. Epidermal growth factor (EGF) and IL-6 were associated with important hemodynamics. Of the twelve proteins, VEGFand IL-6 were significantly, univariately associated with the occurrence of an adverse event, with odds ratios (95% confidenceintervals) of 0.56 (0.33–0.98) and 1.69 (1.03–2.77), respectively. When hemodynamic predictors were combined with proteinmarkers, the ability to predict adverse outcomes within the following year significantly increased. Conclusions. Specific circulatingproteins are associated with hemodynamic variables in pediatric PH. If confirmed in additional cohorts, measurement of theseproteins could aid patient care and design of clinical trials by identifying patients at risk for adverse events. These findings alsofurther support a role for inflammation in pediatric PH.
1. Introduction
Pulmonary hypertension (PH) encompasses a diverse groupof disorders, all characterized by an elevation in pulmonaryarterial pressure and pulmonary vascular resistance (PVR)[1]. Pediatric PH is associated with significant morbidityand mortality, and differs from PH as manifest in adults inseveral important ways, such as the development of PH ina growing lung [1]. Medical treatment of pediatric PH hasbeen challenging due to a lack of accessible, noninvasive,
objective measures that can aid in managing these patients[2]. Specifically, there is a need for better tools for prognosisand assessment of the progression of the disease [1, 3, 4].
Outcomes of most interest to clinicians and PH patientsinclude death, hospitalization for PH-related events, rightventricular failure, initiation of intravenous prostanoidtherapy, and lung transplantation. Although definitive, theseend points are often difficult to study in pediatric PHdue to their infrequent occurrences and the requirementfor long-term followup. Currently, disease progression is

2 Mediators of Inflammation
most commonly assessed through a 6-minute walk dis-tance and hemodynamic assessments, but both of thesesuffer from practical drawbacks and neither is thoroughlyvalidated in the pediatric population. These limitations incurrent outcomes and prognostic variables have spurred oursearch for reliable, noninvasive, objective, and cost-effectivealternatives that are easily measured in children [1, 4].Circulating protein biomarkers have the potential to meetthese objectives [5].
The role of inflammation in the pathobiology of PHhas recently been emphasized [6–9]. Cytokine- and growthfactor-dependent mechanisms lead to inflammatory cellrecruitment and are prominent in PH [9–11]. Of thesefactors, interleukin (IL)-6 is possibly the most studied [7, 12–15]. For example, IL-6 administration in rats induces PH,and IL-6 augments hypoxia-induced PH. In addition, it hasbeen reported recently that transgenic mice overexpressingIL-6 display PH, vascular remodeling, and an exaggeratedresponse to hypoxia [16]. Further, circulating levels ofcytokines are reportedly important in the pathogenesis ofa wide range of other conditions including chronic heartfailure [17], acute renal failure [18], and sepsis [19].
Recent developments in protein array technology allowhigh throughput, multiplex analysis with excellent sen-sitivity, precision, and specificity. The approach is alsocost effective and uses minimal sample because all theanalytes are measured on a single chip simultaneously. Therequirement for low sample volumes is of special interestin the management of pediatric patients. We thereforeapplied a protein array approach that provides accurate andprecise quantification of twelve proteins with known lungor vascular effects in a cohort of pediatric patients with PH.Our objective was to determine whether there is a clinicallyrelevant association between any of the panel constituents,individually or combined, with hemodynamic parameters,disease prognosis, and relevant adverse outcomes. Ourhypothesis was that measurement of these factors could beprognostic in pediatric PH.
2. Materials and Methods2.1. Patient Population. Prior approval for these studies wasobtained from the Colorado Multiple Institutional ReviewBoard (COMIRB, approval #05-0551). Written informedconsent was obtained from the parents or guardians ofall children who served as subjects of the investigation,and when appropriate, from the subjects themselves. Thesestudies comply with the Health Insurance Portability &Accountability Act of 1996. Plasma samples were collectedfrom 70 pediatric patients with PH ranging in age fromnewborn to 21.3 years old. Samples were obtained betweenNovember 2001 and May 2008. All patients were beingtreated with appropriate therapies to manage their PHduring sample collection (Table 1) [20]. Patients were clas-sified as idiopathic pediatric pulmonary arterial hyperten-sion (IPAH) or associated pulmonary arterial hypertension(APAH) according to published criteria [2].
2.2. Data Variables. In this study, disease prognosis/severitywas determined using hemodynamic parameters measured
Table 1: Patient demographics and clinical measurements.
Patient demographics (no of subjects =70)
Female—no. (%) 37 (52.9%)
APAH—no. (%) 45 (64.3%)
Congential heart disease 31 (44.3%)
Chronic lung disease 11 (15.7%)
Clotting disorders 10 (14.3%)
Age (years)—median (IQR) 8.0 (4.4–13.0)
Therapies
Mono therapy 23 (32.9%)
Dual therapy 23 (32.9%)
Triple therapy 10 (14.3%)
Calcium channel blockers 22 (31.4%)
PDE-5 inhibitors 29 (41.4%)
Endothelin receptor blockers 25 (35.7%)
Prostacyclin 23 (32.9%)
Epoprostenol 12 (17.1%)
IV Treprostinil 8 (11.4%)
Inh Iloprost 3 (4.3%)
CATH variables—median (IQR) (n = 59)
Pulmonary artery pressure, mm Hg 34 (23–56)
Pulmonary capillary wedge pressure,mm Hg
8 (6–10)
Right atrial pressure, mm Hg 5 (3–7)
Cardiac index, L/min ×m2 3.5 (3.0–4.3)
Pulmonary vascular resistance index,wood units ×m2 5.6 (4.1–13.9)
PVR/SVR 0.48 (0.27–0.76)
Vasoreactivity (% change in mPAPw/NO)
−21.1 (−29.5 to −12.8)
Follow-up time (months)—median(min–max)
36 (12–89)
Adverse outcomes 16 (22.9%)
Within 12 months 9 (12.9%)
First observed outcome
Expired 10
Transplantation 0
Initiation of IV prostanoids 8
in the cardiac catheterization laboratory during a routinepulmonary hypertension visit. The data were obtained withthe patient breathing room air, prior to testing pulmonaryreactivity with the use of vasodilator therapy. For right-heart catheterization, we used a Swan-Ganz catheter in thefemoral vein or internal jugular vein to determine meanright atrial pressure (RAP), mean pulmonary artery pres-sure (PAP), pulmonary capillary wedge pressure (PCWP),cardiac index (CI), and pulmonary vascular resistance index(PVRi). Invasive arterial monitoring was used to measurethe systemic vascular resistance index (SVRi). We used Fickwith assumed oxygen consumption in those patients withshunts and thermodilution in all others to measure cardiac

Mediators of Inflammation 3
output and then calculate cardiac index. Most subjectswere ventilated because they were children. In addition, thereactivity to inhaled nitric oxide was calculated by takingthe difference in mean PAP between room air and withnitric oxide. The adverse outcome used in the predictivemodels was defined as initiation of intravenous prostanoids(epoprostenol or treprostinil), transplantation, and/or deathoccurring within 12 months from the collection of the bloodsample. Admission for right heart failure is a rare eventin children and was not included in the adverse outcomedefinition.
2.3. Circulating Protein Measurements. Blood (5 mL) wasdrawn, plasma isolated, and this was frozen at −70◦Cuntil analysis. Protein determinations were performed on anEvidence Analyzer (Randox Laboratories, Northern Ireland)according to the manufacturer’s protocol for the simulta-neous quantification of the following analytes: interleukin-1alpha (IL-1α), interleukin-1beta (IL-1β), interleukin-2 (IL-2), interleukin-4 (IL-4), interleukin-6 (IL-6), interleukin-8(IL-8), interleukin-10 (IL-10), tumor necrosis factor alpha(TNFα), gamma interferon cytokine (IFNγ), monocytechemotactic protein-1 (MCP-1), endothelial growth factor(EGF), and vascular endothelial growth factor (VEGF).Values for individual proteins measured by this multiplexedprotein array technology have been shown to correlate withsingle ELISA measurements. Further, intra- and interassaycoefficients of variation of less than 10% are typical formost protein measured by this multiplexed approach withthis system [21]. Determinations were made in duplicateand all calculations were based on the average of the twomeasurements for each sample. Values below the limit ofdetection were set to a value of 0.
2.4. Statistical Analysis. Descriptive statistics were calculatedusing mean ± standard deviations or medians and theinterquartile range (IQR) for continuous variables andpercentages for categorical variables. Protein measurementswere transformed (log base 2) and anchored at 1. Compar-isons across groups were made by Wilcoxon rank sum orchi-squared tests, as appropriate. Spearman rank correlationcoefficients were used to estimate the association betweenthe hemodynamic variables and protein markers. Logisticregressions were fit to investigate the association between thedichotomous adverse outcome variable (outcome observedwithin 12 months) and the protein measurements. Meanstandardization and principal component analysis (PCA)were performed for dimension reduction across the proteinmeasurements, resulting in a single value representing aweighted combination of all twelve markers. A score statisticwas used to select the principal component (PC) mostassociated with the outcome and the best subset of two PCsand clinical variables in a multivariate logistic regression.The predictive ability of the model was investigated using ac-index (area under the ROC curve). The improvement inrisk prediction associated with the addition of the proteinbiomarker PC was assessed by calculation of a net reclassi-fication improvement (NRI) measure [22]. To estimate the
predictive ability of the logistic regressions to an independentset of observations, c-indices were calculated using theleave-out-one cross-validation approach. All analyses wereperformed using SAS version 9.2 software (SAS Institute Inc.,Cary, NC, USA, 2008).
3. Results
The study population consisted of 70 pediatric patientswith PH: 36% IPAH and 64% with APAH. Of these,80% of patients were treated with at least one therapy(Table 1). The median PAP was elevated at 34 mm Hg (theinterquartile range (IQR) was 23–56 mm Hg) with a medianRAP value of 5 mm Hg (IQR, 3–7 mm Hg). Nine (13%)patients experienced an adverse event within 12 months ofsample collection. These patients had worse mPAP levelsranging from 30 to 76 with a median of 65.5 mm Hg as wellas a median PVRI of 15.5 Wood Units × m2 ranging from5.1–20.4. Only 39 of the 48 patients with vasoreactivity testshad complete data in order to assess the responder statusbased on the pediatric definition [23]. Based on these data2 (5%) were classified as responders and neither of thesepatients experienced an adverse event. Individual proteinmeasurements are displayed separately by diagnostic group(Figure 1). There were no significant differences between theIPAH and APAH groups for any of the protein levels.
Cardiac catheterization was performed for all patientsin the initial evaluation for PH. Thereafter, only 59 (84%)of the patients had a catheterization performed on thesame day as blood collection for the correlation analysis,and of these, 48 individuals also had a vasoreactivity testin response to inhaled nitric oxide (NO). The followingpairs of hemodynamic and circulating protein markers hadcorrelation coefficients (r) significantly different from zero:IL-1α and CI (r = −0.31, CL = −0.53 to −0.04); EGF andmPAP (r = −0.45, CL = −0.63 to −0.21); EGF and PVRi(r = −0.37, CL = −0.57 to −0.12); EGF and PVR/SVR(r = −0.42, CL =−0.62 to−0.17); IL-6 and mPAP (r = 0.27,CL = 0.01 to 0.49); IL-6 and PVRi (r = 0.32, CL = 0.06 to0.53). None of the biomarkers correlated with the change inmean PAP in response to inhaled NO.
To assess the potential additive predictive ability ofthe proteins we measured, a series of logistic regressionmodels predicting adverse outcome within 1 year wereestimated. The first of these were univariate models thatwere estimated to determine the association of each proteinindividually with the adverse outcome variable. VEGF andIL-6 were significantly associated with the adverse outcome:(OR (95% CI) were as follows: 0.56 (0.33–0.98) and 1.69(1.03–2.77), respectively. In addition to VEGF, IL-1β, IL-2, IL-4, MCP1, and EGF also had negative associations,indicating that lower values of these proteins were associatedwith the adverse event outcome. PCA was performed onthe protein marker data to condense the 12 measurementsto a few orthogonal components. The 3rd component wassignificantly associated with the outcome, with higher valuescorresponding to an increased risk of an adverse event.The risk associated with this protein index was weighted

4 Mediators of Inflammation
IPAH APAH
(n = 25) (n = 45)
IL1a IL1b IL2 IL4 IL6 IL8 IL10 VEGF IFNG MCP1 EGF1248
163264
128256512
1024
(pg/
mL
)
TNFα
Figure 1: Biomarker characteristics: the distribution of the 12cytokine and growth factor measurements based on disease clas-sification. The y-axis is displayed on the log (base 2) scale. Filledareas indicate the interquartile range (distance between 25th and75th percentiles), the middle line corresponds to the median, andthe whiskers contain data within 1.5 interquartile ranges. None ofthe differences was statistically significant.
by higher values of IL-1α and IL-6 and lower VEGF values(Figure 2). This finding corresponds well with the resultsfrom the univariate analyses and gave a c-index of 0.81.
Score statistics were used to identify the top predictiveclinical markers and determine the added value of a proteinmarker index over the top clinical predictor. The resultingclinical model identified PAP as the top predictor. Usingthis model as a base model, the PCs of the proteinmeasurements were added as predictors and the selectionprocess was repeated. After mPAP, the 4th PC was the toppredictor indicating it contains information orthogonal tothe hemodynamic variable. The risk associated with the 4thPC was weighted by higher values of MCP1 and IL-6 andlower IL-10 values. To evaluate the added predictive value ofthe protein measurements in addition to mPAP, ROC curves,corresponding c-indices, and NRI measures were utilized(Figure 3). The inclusion of these two proteins increased thec-index from 0.81 to 0.90. The predicted probabilities fromboth models were also compared. Significant improvementwas seen with the addition of the protein measurements (NRIP value = 0.01) indicating that their inclusion enhanced themodels ability to correctly classify patients. This result wasverified with a resampling approach used to estimate themodels predictive ability when applied to an independent setof observations. The estimated c-indices for the model withmPAP alone, and with mPAP and the protein measurements,were 0.69 and 0.82, respectively.
4. Discussion
Our data (Table 1) indicate a surprisingly high morbidity andmortality, even in children with mild pulmonary hyperten-sion, and they underscore the fact that this is a very high-riskgroup. This observation stimulated our efforts to developa practical and noninvasive approach to the managementof pediatric pulmonary hypertension that can be used in aroutine setting. Of interest and clinical relevance is the factthat we have shown that by simply adding the quantificationof a set of plasma proteins, it is possible to markedly
improve our ability to predict outcomes in children with PH.Specifically, the addition of a protein index, weighted mostlyby IL-6, IL-10, and MCP-1 concentrations, significantlyincreased the probabilities for those patients with an adverseevent compared to hemodynamic measurements alone.When investigating the plasma proteins univariately, VEGFand IL-6 were associated with occurrence of an adverse eventand EGF and IL-6 were correlated with mean PAP andPVRi. In addition, we identified a combination of all twelveproteins which associated well with adverse events and hadsimilar predictive ability compared to the top hemodynamicpredictor.
Interest in the role of cytokines and growth factors in thedevelopment of PH has grown. Recent evidence is consistentwith the view that circulating factors and inflammatorycells contribute to remodeling in chronic PH [11, 24, 25].Circulating and lung levels of the proinflammatory cytokineIL-6 are increased in patients with idiopathic PH and PHassociated with inflammatory diseases [12–15]. IL-6 may alsobe a mediator of disease in PH because overexpression of IL-6 in a mouse model exacerbated PH by both proproliferativeand antiapoptotic mechanisms [16]. Other studies confirman important role for IL-6 in PH. For example, IL-6 treatedmice are prone to develop hypoxia-induced pulmonaryhypertension [26] which may be mediated in part byan inflammatory process [27]. In our study, we foundthat increased levels of circulating IL-6 were significantlyassociated with an increased risk of an adverse event butwhen considered multivariately with PAP, CI, and VEGF,it was replaced with an anti-inflammatory cytokine, IL-10.Interestingly, IL-6 and IL-10 levels were positively associatedwith each other.
Recently there has also been increased interest in the roleof VEGF in pulmonary arterial hypertension. Studies indi-cate VEGF may be an important mediator of lung growth.VEGF is responsible for angiogenesis and vasculogenesis,and animal models indicate that when VEGF signaling isimpaired, this contributes to the pathogenesis of PH [28,29]. Alternatively, growth factors may be important for themaintenance of continued lung growth in patients withpulmonary arterial hypertension, and a favorable phenotypemay be associated with increased VEGF and EGF. Farkas etal. [30] found a similar inverse relationship between VEGFand PAP in rats and Lassus et al. [31] reported decreasedcirculating plasma levels of VEGF in human infants withPH.
The search for biomarkers that are useful in the man-agement of pediatric PH is in its infancy, but the idealmarker would be obtained noninvasively, easily measured,and would offer high sensitivity and specificity. Currently, thebrain natriuretic peptide system and neurohumoral markershave been evaluated in children with PH [32–34].
Our study demonstrates that quantification of a panelof cytokines and growth factors has potential applicationsin clinical trial design by identifying patients at risk foran adverse event. In addition, patients at higher risk foran adverse event may need to be treated more aggressivelywith continuous intravenous therapy or listed for lungtransplantation.

Mediators of Inflammation 5
Non-event
−3
−2
−1
0
1
2
3
43r
d P
C
Event<1 year
(a)
0.6
0.5
0.4
0.3
0.2
0.1
0
−0.1
−0.2
−0.3
−0.4
−0.5
−0.6
PC
load
ings
EG
F
IFN
G
IL-2
IL-1
0
IL-4
IL-6
IL-8
MC
P-1
TN
Fα
VE
GF
3rd PC (11.4%)4th PC (10.5%)
IL-1α
IL-1β
(b)
Figure 2: Dimension reduction using principal component analysis: the third PC was found to be the most associated with outcome. (a) Thedistribution of the 3rd PC is displayed separately by outcome. Filled areas indicate the interquartile range (distance between 25th and 75thpercentiles), the middle line corresponds to the median, and the whiskers contain data within 1.5 interquartile ranges. (b) The PC loadingsfor the 3rd and 4th PCs are displayed. The 3rd PC is heavily loaded by positive IL-1α and IL-6 and negative VEGF values, whereas the 4thPC is heavily weighted by positive IL-6 and MCP-1 and negative IL-10 values.
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Sen
siti
vity
1-specificity
PAP (c = 0.81)PAP and Pr PC (c = 0.9)
(a)
0 0.2 0.4 0.6 0.8 1
0
0.2
0.4
0.6
0.8
1
Probabilities from base model
Pro
babi
litie
s fr
om b
ase
+pr
otei
n m
odel
Non-eventEvent <1 year
(b)
Figure 3: Added value of proteins toward outcome prediction. (a) Comparison of the ROC curves indicate an improvement in discriminativeability with the addition of the 4th PC calculated from the protein measurements. c-indices for each model are also displayed. (b) Thereclassification of estimated probabilities for the logistic regression model which included protein markers as a predictor versus the modelbased on PAP alone. The dots represent those observations associated with an event and the open circles with a nonevent. Higher percentagesof events and nonevents are desired above and below the reference line, respectively. The corresponding reclassification index was significant(P = 0.01) indicating a significant improvement in prediction with the addition of the proteins.
5. Conclusions
This study adds to the growing body of literature indicatingthat inflammation is important in pediatric PH and thatcirculating (blood) biomarkers can be important tools in
prediction and prognostic evaluation of pediatric patientswith PH. It is envisioned that future use of biomarkerswill guide appropriate treatment selection. The potential forgrowth factors, EGF and VEGF, to aid in the management ofPH is important and novel. Serial sampling and assessment

6 Mediators of Inflammation
of longitudinal changes might provide important additionalinsights, but these findings indicate that even a single pointin time determination can predict the future clinical course.We intentionally examined a heterogeneous group of patientsin this study in order to explore patterns of biomarkerexpression. It is clear that the next step is to validate thesefindings in a larger scale study including several groups ofwell-characterized subjects. We suggest that, based on ourfindings, additional evaluation of cytokines and growth fac-tors is warranted because there is growing evidence that thesedeterminations may be relevant for disease management.
Abbreviation
APAH: Associated pulmonary arterial hypertensionCI: Cardiac indexEGF: Endothelial growth factorIFNγ: Gamma interferon cytokineIL: InterleukinIPAH: Idiopathic pulmonary arterial hypertensionIQR: Interquartile rangeNO: Nitric oxideMCP-1: Monocyte chemoattractant protein-1NRI: Net reclassification improvementPAP: Pulmonary artery pressurePCWP: Pulmonary capillary wedge pressurePH: Pulmonary hypertensionPVR: Pulmonary vascular resistanceRAP: Right arterial pressureSVR: Systemic vascular resistanceTNFα: Tumor necrosis factor alphaVEGF: Vascular endothelial growth factor.
Authors’ Contribution
M. Duncan and B. D. Wagner contributed equally to thiswork.
Acknowledgments
This study was supported in part by UO1-HL081335, Clini-cal Proteomics Center in Lung Disease, NIH, Colorado CTSAGrant 1 UL1 RR025780 from NCRR/NIH, P50 HL084923,P50 specialized centers of clinically oriented research fromNIH/NHLBI and MO1-RR00069, General Clinical ResearchCenters Program, NCRR, NIH, and The Jayden DeLucaFoundation. The authors are grateful to Randox Laboratoriesfor their partial support of this work.
References
[1] S. H. Abman and D. D. Ivy, “Recent progress in understandingpediatric pulmonary hypertension,” Current Opinion in Pedi-atrics, vol. 23, no. 3, pp. 298–304, 2011.
[2] D. Ivy, “Advances in pediatric pulmonary arterial hyperten-sion,” Current Opinion in Cardiology, vol. 27, no. 2, pp. 70–81,2012.
[3] S. Erzurum, S. I. Rounds, T. Stevens et al., “Strategic plan forlung vascular research: an NHLBI-ORDR workshop report,”
American Journal of Respiratory and Critical Care Medicine,vol. 182, no. 12, pp. 1554–1562, 2010.
[4] I. M. Robbins, T. M. Moore, C. J. Blaisdell, and S. H. Abman,“Improving outcomes for pulmonary vascular disease,” Amer-ican Journal of Respiratory and Critical Care Medicine, vol. 185,no. 9, pp. 1015–1020, 2012.
[5] E. Soon, A. M. Holmes, C. M. Treacy et al., “Elevated levelsof inflammatory cytokines predict survival in idiopathic andfamilial pulmonary arterial hypertension,” Circulation, vol.122, no. 9, pp. 920–927, 2010.
[6] R. T. Schermuly, H. A. Ghofrani, M. R. Wilkins, and F.Grimminger, “Mechanisms of disease: pulmonary arterialhypertension,” Nature Reviews Cardiology, vol. 8, no. 8, pp.443–455, 2011.
[7] R. Mathew, “Inflammation and pulmonary hypertension,”Cardiology in Review, vol. 18, no. 2, pp. 67–72, 2010.
[8] L. C. Price, S. J. Wort, F. Perros et al., “Inflammation inpulmonary arterial hypertension,” Chest, vol. 141, no. 1, pp.210–221, 2012.
[9] S. Hall, P. Brogan, S. G. Haworth, and N. Klein, “Contributionof inflammation to the pathology of idiopathic pulmonaryarterial hypertension in children,” Thorax, vol. 64, no. 9, pp.778–783, 2009.
[10] P. M. Hassoun, L. Mouthon, J. A. Barbera et al., “Inflamma-tion, growth factors, and pulmonary vascular remodeling,”Journal of the American College of Cardiology, vol. 54, no. 1,supplement 1, pp. S10–S19, 2009.
[11] R. M. Tuder, J. C. Marecki, A. Richter, I. Fijalkowska, andS. Flores, “Pathology of pulmonary hypertension,” Clinics inChest Medicine, vol. 28, no. 1, pp. 23–42, 2007.
[12] M. Humbert, G. Monti, F. Brenot et al., “Increasedinterleukin-1 and interleukin-6 serum concentrations insevere primary pulmonary hypertension,” American Journalof Respiratory and Critical Care Medicine, vol. 151, no. 5, pp.1628–1631, 1995.
[13] K. Hashimoto, K. Nakamura, H. Fujio et al., “Epoprostenoltherapy decreases elevated circulating levels of monocytechemoattractant protein-1 in patients with primary pul-monary hypertension,” Circulation Journal, vol. 68, no. 3, pp.227–231, 2004.
[14] R. M. Tuder, M. Chacon, L. Alger et al., “Expression ofangiogenesis-related molecules in plexiform lesions in severepulmonary hypertension: evidence for a process of disorderedangiogenesis,” Journal of Pathology, vol. 195, no. 3, pp. 367–374, 2001.
[15] T. M. Yu, Y. H. Chen, J. Y. Hsu et al., “Systemic inflammation isassociated with pulmonary hypertension in patients undergo-ing haemodialysis,” Nephrology Dialysis Transplantation, vol.24, no. 6, pp. 1946–1951, 2009.
[16] M. K. Steiner, O. L. Syrkina, N. Kolliputi, E. J. Mark, C.A. Hales, and A. B. Waxman, “Interleukin-6 overexpressioninduces pulmonary hypertension,” Circulation Research, vol.104, no. 2, pp. 236–244, 2009.
[17] M. Testa, M. Yeh, P. Lee et al., “Circulating levels of cytokinesand their endogenous modulators in patients with mild tosevere congestive heart failure due to coronary artery diseaseor hypertension,” Journal of the American College of Cardiology,vol. 28, no. 4, pp. 964–971, 1996.
[18] A. K. Kadiroglu, D. Sit, A. E. Atay, H. Kayabasi, A. Altintas,and M. E. Yilmaz, “The evaluation of effects of demographicfeatures, biochemical parameters, and cytokines on clinicaloutcomes in patients with acute renal failure,” Renal Failure,vol. 29, no. 4, pp. 503–508, 2007.

Mediators of Inflammation 7
[19] C. E. Ventetuolo and M. M. Levy, “Biomarkers: diagnosis andrisk assessment in sepsis,” Clinics in Chest Medicine, vol. 29,no. 4, pp. 591–603, 2008.
[20] R. J. Barst, J. S. R. Gibbs, H. A. Ghofrani et al., “Updatedevidence-based treatment algorithm in pulmonary arterialhypertension,” Journal of the American College of Cardiology,vol. 54, no. 1, pp. S78–S84, 2009.
[21] S. P. FitzGerald, J. V. Lamont, R. I. McConnell, and E. O.Benchikh, “Development of a high-throughput automatedanalyzer using biochip array technology,” Clinical Chemistry,vol. 51, no. 7, pp. 1165–1176, 2005.
[22] M. J. Pencina, R. B. D’Agostino, R. B. D’Agostino, and R.S. Vasan, “Evaluating the added predictive ability of a newmarker: from area under the ROC curve to reclassificationand beyond,” Statistics in Medicine, vol. 27, no. 2, pp. 157–172,2008.
[23] R. J. Barst, M. D. McGoon, C. G. Elliott, A. J. Foreman etal., “Survival in childhood pulmonary arterial hypertension:insights from the registry to evaluate early and long-termpulmonary arterial hypertension disease management,” Circu-lation, vol. 125, pp. 113–122, 2012.
[24] D. L. Burke, M. G. Frid, C. L. Kunrath et al., “Sustainedhypoxia promotes the development of a pulmonary artery-specific chronic inflammatory microenvironment,” AmericanJournal of Physiology, vol. 297, no. 2, pp. L238–L250, 2009.
[25] M. Mandegar, Y. C. B. Fung, W. Huang, C. V. Remillard, L. J.Rubin, and J. X. J. Yuan, “Cellular and molecular mechanismsof pulmonary vascular remodeling: Role in the developmentof pulmonary hypertension,” Microvascular Research, vol. 68,no. 2, pp. 75–103, 2004.
[26] S. M. Golembeski, J. West, Y. Tada, and K. A. Fagan,“Interleukin-6 mild pulmonary hypertension and augmentshypoxia-induced pulmonary hypertension in mice,” Chest,vol. 128, supplement 6, pp. 572S–573S, 2005.
[27] L. Savale, L. Tu, D. Rideau et al., “Impact of interleukin-6 on hypoxia-induced pulmonary hypertension and lunginflammation in mice,” Respiratory Research, vol. 10, article no.6, 2009.
[28] T. R. Grover, T. A. Parker, J. P. Zenge, N. E. Markham, J.P. Kinsella, and S. H. Abman, “Intrauterine hypertensiondecreases lung VEGF expression and VEGF inhibition causespulmonary hypertension in the ovine fetus,” American Journalof Physiology, vol. 284, no. 3, pp. L508–L517, 2003.
[29] S. Nadeau, J. Baribeau, A. Janvier, and T. Perreault, “Changesin expression of vascular endothelial growth factor and itsreceptors in neonatal hypoxia-induced pulmonary hyperten-sion,” Pediatric Research, vol. 58, no. 2, pp. 199–205, 2005.
[30] L. Farkas, D. Farkas, K. Ask et al., “VEGF amelioratespulmonary hypertension through inhibition of endothelialapoptosis in experimental lung fibrosis in rats,” Journal ofClinical Investigation, vol. 119, no. 5, pp. 1298–1311, 2009.
[31] P. Lassus, M. Turanlahti, P. Heikkila et al., “Pulmonaryvascular endothelial growth factor and Flt-1 in fetuses, inacute and chronic lung disease, and in persistent pulmonaryhypertension of the newborn,” American Journal of Respiratoryand Critical Care Medicine, vol. 164, no. 10 I, pp. 1981–1987,2001.
[32] A. Bernus, B. D. Wagner, F. Accurso, A. Doran, H. Kaess,and D. D. Ivy, “Brain natriuretic peptide levels in managingpediatric patients with pulmonary arterial hypertension,”Chest, vol. 135, no. 3, pp. 745–751, 2009.
[33] A. E. Lammers, A. A. Hislop, and S. G. Haworth, “Prog-nostic value of B-type natriuretic peptide in children with
pulmonary hypertension,” International Journal of Cardiology,vol. 135, no. 1, pp. 21–26, 2009.
[34] M. E. Van Albada, F. G. Loot, R. Fokkema, M. T. R. Roofthooft,and R. M. F. Berger, “Biological serum markers in themanagement of pediatric pulmonary arterial hypertension,”Pediatric Research, vol. 63, no. 3, pp. 321–327, 2008.

Hindawi Publishing CorporationMediators of InflammationVolume 2012, Article ID 162571, 7 pagesdoi:10.1155/2012/162571
Research Article
Symptoms, but Not a Biomarker Response to InhaledCorticosteroids, Predict Asthma in Preschool Children withRecurrent Wheeze
E. M. M. Klaassen,1 K. D. G. van de Kant,1 Q. Jobsis,1 S. T. P. Høvig,1
C. P. van Schayck,2 G. T. Rijkers,3, 4 and E. Dompeling1
1 Department of Paediatric Pulmonology, School for Public Health and Primary Care (CAPHRI), Maastricht UniversityMedical Centre (MUMC), P.O. Box 5800, 6202 AZ Maastricht, The Netherlands
2 Department of General Practice, CAPHRI, MUMC, P.O. Box 5800, 6202 AZ Maastricht, The Netherlands3 Department of Medical Microbiology and Immunology, Sint Antonius Hospital, P.O. Box 2500,3430 EM Nieuwegein, The Netherlands
4 Department of Sciences, Roosevelt Academy, P.O. Box 94, 4330 AB Middelburg, The Netherlands
Correspondence should be addressed to E. M. M. Klaassen, [email protected]
Received 10 July 2012; Revised 14 November 2012; Accepted 15 November 2012
Academic Editor: Dirk Holzinger
Copyright © 2012 E. M. M. Klaassen et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. A reliable asthma diagnosis is challenging in preschool wheezing children. As inhaled corticosteroids (ICS) are moreeffective in asthmatics than in children with transient wheeze, an ICS response might be helpful in early asthma diagnosis. Methods.175 children (aged two–four years) with recurrent wheeze received 200 μg Beclomethasone extra-fine daily for eight weeks.Changes in Exhaled Breath Condensate (EBC) biomarkers (pH, interleukin (IL)-1α, IL-2, IL-4, IL-5, IL-10, IFN-γ, sICAM, andCCL-11), Fractional exhaled Nitric Oxide (FeNO), airway resistance, and symptoms were assessed. At six years of age a child wasdiagnosed as transient wheezer or asthmatic. Adjusted logistic regression analysis was performed with multiple testing correction.Results. 106 transient wheezers and 64 asthmatics were analysed at six years of age. Neither changes in EBC biomarkers, nor FeNO,airway resistance, or symptoms during ICS trial at preschool age were related to asthma diagnosis at six years of age. However,asthmatics had more airway symptoms before the start of the ICS trial than transient wheezers (P < 0.01). Discussion. Althoughsymptom score in preschool wheezing children at baseline was associated with asthma at six years of age, EBC biomarkers, airwayresistance, or symptom response to ICS at preschool age could not predict asthma diagnosis at six years of age.
1. Introduction
Asthma is one of the most commonly occurring chronicdiseases in children. It mostly develops in early childhoodand is characterized by recurrent episodes of wheezing,breathlessness, and coughing due to airway inflammationand airway hyperresponsiveness [1]. However, in the major-ity of children symptoms are virally induced and transient(so-called transient wheezers) [2]. So, the associated airwaysymptoms are subjective and not specific for asthma. More-over, young children are not able to perform lung functiontests. Consequently, a diagnosis of asthma at young agehas proven to be difficult [1, 2]. Objective measurements
of airway inflammation require invasive procedures such asbronchoalveolar lavage, bronchial biopsy, and induced spu-tum and therefore are not routinely used. Effective asthmatreatment is available in the form of inhaled corticosteroids(ICS). ICS are less effective in children with airway symptomsnot due to asthma [1, 3]. As a result of difficulties inproper asthma diagnosis, true asthmatics are often “under-treated,” whereas children with transient symptoms areoften “overtreated” [4]. Although international guidelinesadvocate a trial treatment with ICS for a likely diagnosis ofasthma in young children, so far studies addressing responseto ICS as a diagnostic tool in children have been scarce [1].

2 Mediators of Inflammation
Exhaled Breath Condensate (EBC) is a noninvasive toolto assess biomarkers of airway inflammation [5]. Based onthe ICS response of inflammation biomarkers in EBC atpreschool age, a prediction of asthma at a later age might bepossible. Besides, ICS-induced changes in Fractional exhaledNitric Oxide (FeNO), airway resistance, and symptomsmight contribute to an early asthma diagnosis. Therefore,our study aim was to assess whether an ICS response basedon changes in biomarkers in EBC, FeNO, airway resistance,and symptoms in preschool-aged wheezing children has apredictive value for an asthma diagnosis at age six years.
2. Methods
2.1. Study Population. Participants from the ADEM study(Asthma DEtection and Monitoring study registered atclinicaltrial.gov: NCT 00422747) were included. The ADEMstudy is a long-term case-control study that started in 2006in The Netherlands and aimed to develop a noninvasiveinstrument for early asthma diagnosis by using biomarkersof airway inflammation in exhaled breath (condensate), andearly lung function measurements (airway resistance). Thestudy protocol has been described previously [6]. In total,252 children aged two to four years were included: 202children with recurrent wheezing symptoms (≥2 wheezingepisodes until inclusion according to the International Studyof Asthma and Allergies in Childhood (ISAAC) question-naire) and 50 healthy controls without wheezing episodesuntil inclusion [7]. For the present analysis only the childrenwith recurrent wheezing symptoms were included.
2.2. Study Design. The main study objective was to assesswhether an ICS response in biomarkers in EBC at preschoolage was able to predict an asthma diagnosis at six years ofage. Besides, the diagnostic value of the ICS response inFeNO, airway resistance, and symptoms for the predictionof asthma at age six years was assessed. For this purpose,an ICS trial was started in preschool children with recurrentwheeze. Airway medication (such as ICS and β2-agonists)was temporarily stopped prior to measurement. Childrenwho were not able to discontinue ICS from four weeksbefore the trial were excluded from analyses. In case ofclear symptoms of an airway infection, the measurementwas postponed for four weeks. During the initial visit EBCwas collected, FeNO and airway resistance were assessed,and questionnaires were completed (for details see below).Subsequently, recurrent wheezing children received 100 μgICS (Beclomethasone) extra-fine two times a day via theAeroChamber (Trudell Medical International, ON, Canada)for eight weeks. Symptom relieve by using salbutamol(Airomir, Teva Pharma NL, Haarlem, The Netherlands)distributed by an AeroChamber was allowed during thetrial. At the end of the ICS trial, all measurements werereassessed. Compliance to ICS was assessed by weightingICS canisters before and after the trial. Children who useda minimum of 80% of the prescribed medication wereconsidered compliant (used for the per protocol subanalysis).
Children were followed-up until six years of age. At this agea definite asthma diagnoses was made (see further).
The study protocol was approved by the Dutch CentralCommittee on Research Involving Human Subjects (CCMO:NL17407.000.07/2007-001817-40, The Hague, The Nether-lands). All parents gave written informed consent.
2.3. Asthma Diagnosis. At the age of six years, a definitediagnosis (transient wheezer or true asthmatic) was madeby two paediatric pulmonologists. An asthma diagnosis wasbased on symptoms, lung function (reversibility to a β2-agonist and bronchial hyperresponsiveness), and medicationuse. Next to this clinical assessment a diagnosis was assessedby a computer calculated algorithm. In this algorithm,asthma was diagnosed in case two out of the following threefeatures were present: (1) positive symptoms (coughing ≥1night(s) a week, ≥2 episodes of wheezing during the lasttwelve months, some days wheeze during colds or exerciseor night time, two out of the following three items; somedays wheeze during colds or during exercise in combinationwith night time coughing; every day, most days or severaldays wheeze during colds, during exercise or during the nighttime; cough during the night time) [7, 8], (2) presence oflung function abnormalities (a 20% fall in Forced expiratoryvolume in one second (FEV1) induced by a provocativeconcentration of histamine <2 mg/mL, or bronchodilatorreversibility ≥9% (see below)) [9], and (3) ICS use. Incase of disagreement between the clinical diagnosis and thecomputer calculated diagnosis, children were reassessed bythe two paediatric pulmonologists who decided on the finaldiagnosis.
Bronchial hyperresponsiveness and reversibility mea-surements were performed according to the ERS guideline[10]. FEV1 was assessed in each child by means of theMasterScreen Pneumo (Jaeger, Wuerzburg, Germany). Thehighest FEV1 of three technically satisfactory curves was usedfor analysis. A challenge test was performed using histaminedissolved in physiologic saline in doubling concentrationsfrom 0.032 to 16 mg/mL. Concentrations were increaseduntil a fall of≥20% (PC20) in FEV1 was measured or the finaldilution was reached. Thereafter, all children directly received400 μg salbutamol, and FEV1 was reevaluated after fifteenminutes. The change in FEV1 was expressed as a percentageof the predicted value.
2.4. Biomarkers of Inflammation in Exhaled Breath Conden-sate. EBC was collected during ten minutes of tidal breathinginto a mask with a two-way nonrebreathing valve connectedto a closed glass condenser with recirculation unit developedat our institute [5]. Directly after EBC collection and pHmeasurement (Radiometer, Zoetermeer, The Netherlands),samples were stored at −80◦C until further analysis. Aselection of proinflammatory cytokines ((interleukin (IL)-1α), T-helper 1 cytokines (interferon-γ (IFN-γ) and IL-2),T-helper 2 cytokines (IL-4 and IL-5)), an antiinflammatorycytokine (IL-10), a chemokine (Eotaxin (CCL-11)), and anadhesion molecule (soluble Intercellular Adhesion Molecule1 (sICAM1)) were used for analysis. These biomarkers were

Mediators of Inflammation 3
analysed by using the multiplex immunoassay (LuminexCorporation, Austin, TX, USA) as described previously[5, 11–13]. Values under the detection limit receiveda randomly generated value between zero and the detectionlimit [12].
2.5. Fractional Exhaled Nitric Oxide. As previouslydescribed, FeNO was collected offline in a 500 mL inertballoon during tidal breathing and measured by using anitric oxide monitoring system (NIOX, Aerocrine, Solna,Sweden) [6].
2.6. Airway Resistance. Airway resistance was measuredduring tidal breathing by means of the MicroRint (MicroMedical, Rochester Ltd, UK) as described before [6, 14].The median of at least 5 technically acceptable airwayinterruptions during an expiratory peak flow was used foranalysis. Measurements were performed before and fifteenminutes after inhalation of 300 μg of salbutamol via a spacer(AeroChamber).
2.7. Symptom Score. Parents completed a questionnaireon airway symptoms [8]. Based on this questionnaire asymptom score was computed by adding six items (coughduring daytime, cough at night, wheeze during daytime,wheeze at night, dyspnoea during daytime, and dyspnoea atnight) on a Likert scale (every day = 1, most days = 2, somedays = 3, a few days = 4, and not at all = 5). The minimal scorewas six, and the maximal score was 30 (no day and night timesymptoms).
2.8. Statistical Analysis. Data were analysed using SPSS 18(SPSS Inc., Chicago, IL, USA). Due to the skewed distri-butions, biomarkers in EBC were log transformed whichsuccessfully imparted a normal distribution. Differences inbaseline characteristics between transient wheezers and trueasthmatics were evaluated by using the chi-square test forcategorical variables and the independent t-test for con-tinuous parametric variables. The effect of each individualpotential predictor (both before the ICS trial and changesduring ICS) on asthma diagnosis at six years of age wastested by separate logistic regression models. Models wereadjusted for possible confounders (gender, atopy, eczema,previous ICS use, first degree relative with asthma, smokingexposure, and season of measurement). Data were presentedfor intention to treat analysis unless otherwise specified. Pvalues were corrected for multiple testing by False DiscoveryRate (FDR) for each hypothesis [15]. Differences wereconsidered statistically significant when the FDR correctedP value was <0.05.
2.9. Power Analysis. The primary outcome measure is thedefinite asthma diagnosis at six years of age. In a populationof young children with recurrent airway symptoms, theprevalence of asthma at six years of age is 30% [16]. In thecurrent study, including 202 children with recurrent wheeze,this will result in at least 50 children with asthma taken intoaccount a drop out rate of 10%. Based on an earlier study in
children with asthma and healthy controls aged 6–16 years,differences in concentrations of IL-1α, IL-2, IL-4, IFN-γ,CCL-11, and sICAM were found of, respectively, 4.5, 13.2,2.9, 11.3, 0.9, and 80.0 pg/mL [17]. If we assume comparabledifferences in for example CCL-11 in the present populationbetween asthmatics and transient wheezers with a power of90% and an alpha of 0.05, 39 asthmatics and 78 transientwheezers are needed.
3. Results
3.1. Baseline Characteristics. Of the 202 recurrent wheezersincluded in the ADEM study, 175 parents gave informedconsent to participate in the ICS trial. One participant wasexcluded from analysis as an asthma diagnosis could notbe assessed due to missing data. Four children (all trueasthmatics) were unable to stop their regular ICS medicationand were therefore excluded from further analysis. In total,170 (65 asthmatics and 105 transient wheezers) childrenwere included in the intention to treat analysis and 103 (42asthmatics and 61 transient wheezers) in the per protocolanalysis (as they used a minimum of 80% prescribed ICS).Figure 1 presents the study flow chart. Agreement betweenclinical and computed diagnosis was reached in 83% beforeand 89% after clinical reassessment.
Baseline characteristics are displayed in Table 1. Pre-school children in the asthmatic group used significantlymore ICS and short-acting β2-agonists in the preceding yearcompared to the transient wheeze group. Besides, atopyat preschool age was significantly more frequent in trueasthmatics. At six years of age, ICS and short-acting β2-agonists were used in 40/43% of the asthmatics and 2/6%of the transient wheezers, respectively. Atopy was present in45% of the asthmatics and 31% of the transient wheezers atsix years of age.
3.2. Analysis at Baseline. EBC and FeNO were successfullycollected in all children (100%). With the exception ofEotaxin (89%), all EBC markers were above the detectionlimit in more than 98% of the samples. Prebronchodilatorand postbronchodilator airway resistance were successfullyassessed in 95% and 97% of the children, respectively. Thesymptom score was present in all children (100%). No statis-tically significant differences in biomarkers of inflammationin EBC, FeNO, or airway resistance were observed betweenboth groups at preschool age (Table 2). However, childrenwith an asthma diagnosis at six years of age had significantlymore symptoms (lower symptom score) at preschool agecompared to transient wheezers (odds ratio = 0.85; 95%confidence interval = 0.77–0.93; P < 0.01 FDR corrected).
3.3. Changes Induced by Inhaled Corticosteroids. No statis-tically significant changes between transient wheezers andasthmatics in biomarkers in EBC, FeNO, airway resistance orsymptom score were induced by the ICS trial (Table 3). FeNOlevels in the total group neither showed significant changes(median ppb (interquartile range) before the ICS trial: 8.4(4.2–14.3), after the ICS trial: 9.6 (4.5–15.4); P = 0.45).

4 Mediators of Inflammation
ADEM: Asthma detection and monitoring; ICS: inhaled corticosteroids.
Per protocol: only compliant children (at least 80% of the prescribed study medication was used).
Informed consent forthe ICS study N = 175
Included N = 174
Not able to stop ICS N = 4
Per protocol N = 103
Incomplete data N = 1
Not compliant N = 67
ADEM studyrecurrent wheeze N = 202
Intention to treat N = 170
Figure 1: Study flow chart.
Table 1: Characteristics at baseline for transient wheezers and trueasthmatics.
TransientwheezeN = 105
AsthmaN = 65
TotalN = 170
Mean age (SD) 3.3 (0.6) 3.3 (0.6) 3.3 (0.6)
Gender: male/female (n) 55/50 37/28 92/78
Atopy†, %∗ 20 35 26
Eczema, % 36 47 40
Use of ICS, %∗ 12 26 18
Use of short-actingβ2-agonists, %∗ 31 54 40
Asthma first degreerelatives, %
36 44 39
Smoking exposure, % 30 31 31∗P < 0.05 between transient wheezers and true asthmatics; †atopy is definedas a positive (≥0.35 kU/L); Phadiatop Infant test (Phadiatop Infant, Phadia,Uppsala, Sweden); SD: standard deviation.
3.4. Subanalysis per Protocol. Results of the study did notchange when only compliant children were included in theanalysis (per protocol analysis).
4. Discussion
Presently, no adequate diagnostic tool is available for anearly asthma diagnosis in preschool wheezing children.This study addressed the question whether response to ICS
treatment of biomarkers of inflammation in EBC, FeNO,airway resistance, and symptoms at preschool age couldpredict an asthma diagnosis at six years of age. Changes inbiomarkers in EBC, FeNO, airway resistance, or symptomsinduced by an eight-week ICS treatment at preschool agewere not related to an asthma diagnosis at six years of age.However, it was demonstrated that children with asthma atsix years of age had more respiratory symptoms at preschoolage compared to transient wheezers. Also, medication useand atopy at baseline were significantly higher in asthmaticscompared to transient wheezers.
Collection of EBC is a noninvasive method in whichbiomarkers expected to reflect airway inflammation can beassessed, and most influence of the systemic metabolism isavoided. Previously our research group has shown differencesof biomarkers of inflammation between asthmatics andhealthy children [17]. Moreover, a higher concentration formultiple biomarkers was noted in children with more severewheeze compared to children without wheeze in the presentpopulation [13]. In adult populations with asthma, it wasdemonstrated that several biomarkers in EBC significantlychanged after ICS treatment [18, 19]. Differences of ICSresponse based on changes in biomarkers in children havenot yet been investigated. In the present study, none of theselected biomarkers in EBC before or changes during theICS treatment were associated with an asthma diagnosis atsix years of age. Besides, FeNO assessed before or a changeduring ICS treatment at preschool age was not associatedwith an asthma diagnosis at six years of age. FeNO levelsin the total group neither showed significant changes. Dataon the effectiveness of predicting an ICS response by FeNO

Mediators of Inflammation 5
Table 2: Baseline analysis at preschool age.
Median (IQR) transient wheeze Median (IQR) asthma OR 95% CI
IL-1α, in pg/mL 34.0 (15.6–83.7) 44.2 (18.3–97.6) 1.10 0.84–1.44
IL-2, in pg/mL 55.5 (35.7–76.8) 57.0 (43.1–81.2) 1.32 0.80–2.16
IL-4, in pg/mL 8.8 (4.8–13.9) 9.6 (6.0–14.5) 1.15 0.70–1.88
IL-5, in pg/mL 29.8 (17.8–58.7) 37.2 (19.4–80.6) 1.21 0.85–1.73
IL-10, in pg/mL 4.5 (2.8–6.9) 5.2 (3.2–8.4) 1.09 0.72–1.65
IFN-γ, in pg/mL 28.1 (17.5–44.6) 27.1 (16.0–44.2) 0.88 0.67–1.16
sICAM, in pg/mL 190.4 (94.8–416.2) 265.5 (104.1–516.4) 1.08 0.79–1.48
CCL-11, in pg/mL 8.3 (5.2–12.5)) 8.0 (5.3–14.6) 0.90 0.71–1.15
pH 6.0 (5.7–6.3) 5.8 (5.6–6.2) 0.66 0.34–1.28
FeNO, in ppb 6.7 (3.7–13.3) 8.9 (5.4–18.1) 1.02 0.98–1.05
Airway resistance before medication§ 1.4 (0.3) 1.5 (0.4) 2.15 0.83–5.56
Airway resistance after medication§ 1.2 (0.4) 1.3 (0.3) 2.06 0.70–6.01
Bronchodilator response§ 0.1 (0.3) 0.0 (0.5) 1.44 0.45–4.55
Total symptom score∗ 27 (25–29) 25 (20–28) 0.85 0.77–0.93∗
False Discovery Rate (FDR) corrected P < 0.01; §mean (standard deviation).IL: interleukin; IFN-γ: interferon-γ; sICAM: soluble Intercellular Adhesion Molecule; CCL-11: Eotaxin; FeNO: Fractional exhaled Nitric Oxide; OR: oddsratio; 95% CI: 95% confidence interval. Analysis adjusted for gender atopy, eczema, previous inhaled corticosteroids use, asthma first relative, smokingexposure, and season of measurement. The transient wheeze group is the reference group.
Table 3: Changes induced by inhaled corticosteroids related to anasthma diagnosis.
OR 95% CI
IL-1α 0.96 0.78–1.19
IL-2 0.99 0.71–1.38
IL-4 0.90 0.64–1.28
IL-5 0.97 0.76–1.24
IL-10 0.87 0.65–1.16
IFN-γ 0.93 0.73–1.20
sICAM 0.97 0.77–1.22
CCL-11 0.94 0.75–1.17
pH 0.99 0.61–1.60
FeNO 1.01 0.99–1.04
Airway resistance before medication 0.80 0.33–1.93
Airway resistance after medication 1.51 0.55–4.16
Total symptom score decreased Ref.
Total symptom score equal 0.74 0.27–2.04
Total symptom score increased 0.65 0.30–1.39
IL: interleukin; IFN-γ: interferon-γ; sICAM: soluble Intercellular AdhesionMolecule; CCL-11: Eotaxin; FeNO: Fractional exhaled Nitric Oxide; OR:odds ratio; 95% CI: 95% confidence interval; Ref.: reference category.Analysis adjusted for gender atopy, eczema, previous inhaled corticosteroidsuse, asthma first relative, smoking exposure, and season of measurement.The transient wheeze group is the reference group. Due to violation oflinearity assumption in log transformation, results for total symptom scoreare split up into three equal categories.
in children are conflicting [20–22]. Asthma is expected tobe predominated by an eosinophilic airway inflammationwhile transient wheeze is characterised by a neutrophilicinflammation [23–25]. ICS are believed to mainly have an
antieosinophilic inflammation effect [1, 3, 24]. Therefore,ICS are expected to be more effective in asthmatics comparedto transient wheezers. However, increasing evidence pointstowards overlap between eosinophilic and neutrophilicinflammation in both asthma and transient wheeze [26, 27].Due to this overlap, changes in inflammation biomarkersinduced by ICS treatment might be less pronounced, andthese changes may not be able to distinguish betweentransient wheezers and true asthmatics, as was observedin our study. It would be interesting to study differenceswith healthy children as well. Previously we did demonstratedifferences between baseline measurements of biomarkers inEBC in healthy children and children with recurrent wheezein the same cohort [12]. However, due to ethical constraintsthe healthy children have not been included in the trial.
Airway resistance in preschool children has been foundto be predictive for asthma symptoms at six years of age[28]. Besides, bronchodilator reversibility was able to predicteffectiveness of anti-inflammatory therapy in young childrenwith asthma [20]. No ICS response for airway resistance orreversibility was demonstrated in the present study. Theseresults should be interpreted with caution as the childrenparticipating in our study in general had mild symptomsbefore and during ICS treatment, thus leaving little room forimprovement.
Even though most children had only mild symptoms,symptoms at preschool age were positively associated withan asthma diagnosis at six years of age. This associationremained highly significant after multiple testing corrections.However, changes in symptoms during ICS treatment werenot related to the asthma diagnosis at six years of age. Thisresult can be interpreted twofold. First, as symptoms weremild there was not enough room for improvement duringICS treatment. Second, improvement in symptoms was

6 Mediators of Inflammation
equal for asthmatics and for transient wheezers. Either way,differentiation of true asthmatics from transient wheezersbased on symptom reduction due to ICS treatment was notpossible in our study. It will be interesting to address thisissue in a population with more severe symptoms.
The major strength of this study is the longitudinaldesign that enabled the assessment of an ICS response ofseveral biomarkers at preschool age and an asthma diagnosisat six years of age. A second strength of this study is the highfollow-up rate. Information to assess an asthma diagnosiswas available in all but one child at six years of age. Thirdly,measurements were feasible and noninvasive which madethem suitable for young children. Feasibility of assessingbiomarkers in EBC was increased by the use of a double-jacketed condenser with heated breath recirculation unit aswas developed at our institute [5]. Due to this efficientcondenser system EBC could be collected in a relatively shortcollection time. Besides, multiple biomarkers could be mea-sured in a small sample by the highly sensitive multiplexedliquid bead arrays with good to excellent reproducibility[11, 17]. Finally, we chose to administer Beclomethasoneextra-fine. Previous research demonstrated that the use ofsmall particles in young children are effective and safeand are expected to result in increased and more uniformdeposition in the lower respiratory tracts. This minimizesthe necessary dosage for administration [29, 30]. However,some limitations need to be addressed. Firstly, measurementof biomarkers of inflammation in EBC is a technique thatstill needs more validation and standardisation. Despite theserestrictions, our research group has extensive experienceon the use of EBC as a noninvasive technique to assessbiomarkers in airway inflammation [5, 6, 17]. Secondly, asasthma is heterogeneous by nature, difficulties might arisewhen assessing an asthma diagnosis. In the present study,both a clinical and a computer algorithm were used for anasthma diagnosis. The degree of accordance between theclinical and algorithm diagnosis was high, and mismatcheswere reevaluated in order to prevent an incorrect diagnoses.Finally, it can be argued whether a period of eight weeksICS is sufficient to assess changes in biomarkers in EBC,FeNO, airway resistance, and symptoms at preschool age topredict an asthma diagnosis at six years of age. Accordingto international guidelines a treatment trial with ICS of atleast eight weeks in preschool children can give guidance tothe presence of asthma [1]. Therefore, changes in biomarkersin EBC, airway resistance, FeNO, and symptoms are to beexpected after eight weeks.
5. Conclusions
In conclusion, in this study we demonstrated that, althoughsymptoms at preschool age were predictive for an asthmadiagnosis at age six years, changes in biomarkers of inflam-mation in EBC, FeNO, airway resistance, and symptomsinduced by ICS at preschool age could not predict an asthmadiagnosis at six years of age. In the absence of a properdiagnostic tool for asthma at young age, adequate care andmanagement of children with airway symptoms remains
hampered. Although no predictive value of biomarkers inEBC could be demonstrated in the present study, EBCbiomarkers might still be of additional value for an asthmadiagnosis. In the future, we will determine whether profilesof EBC biomarkers in combination with other parameterssuch as clinical features, exhaled volatile organic compounds,and gene expression can be of value in predicting an asthmadiagnosis.
Conflict of Interests
The authors state that they have no conflict of interests todeclare.
Acknowledgments
The authors thank medical students of the MaastrichtUniversity Kiki Vangangelt, Nedim Dzino, Imke Duijf,Brenda Thonissen, Esther Kalicharan and Emily Cohenfor their outstanding assistance during the measurements;Frank Nijpels and other workers from Instrument Devel-opment Engineering and Evaluation (IDEE), the MaastrichtUniversity for their contribution to the development ofthe condenser; TEVA Pharma NL for providing the studymedication and the AeroChambers; the parents and childrenfor their participation.
References
[1] S. E. Pedersen, S. S. Hurd, R. F. Lemanske et al., “Global strat-egy for the diagnosis and management of asthma in children5 years and younger,” Pediatric Pulmonology, vol. 46, no. 1, pp.1–17, 2011.
[2] O. E. Savenije, R. Granell, D. Caudri et al., “Comparison ofchildhood wheezing phenotypes in 2 birth cohorts: ALSPACand PIAMA,” Journal of Allergy and Clinical Immunology, vol.127, no. 6, pp. 1505–1512.e14, 2011.
[3] S. Schokker, E. M. W. Kooi, T. W. de Vries et al., “Inhaled cor-ticosteroids for recurrent respiratory symptoms in preschoolchildren in general practice: randomized controlled trial,”Pulmonary Pharmacology and Therapeutics, vol. 21, no. 1, pp.88–97, 2008.
[4] D. Caudri, A. H. Wijga, H. A. Smit et al., “Asthma symptomsand medication in the PIAMA birth cohort: evidence forunder and overtreatment,” Pediatric Allergy and Immunology,vol. 22, no. 7, pp. 652–659, 2011.
[5] P. P. Rosias, C. M. Robroeks, K. D. van de Kant et al., “Fea-sibility of a new method to collect exhaled breath condensatein pre-school children,” Pediatric Allergy and Immunology, vol.21, no. 1, pp. e235–e244, 2010.
[6] K. D. Van De Kant, E. M. Klaassen, Q. Jobsis, A. J. Nijhuis, O.C. Van Schayck, and E. Dompeling, “Early diagnosis of asthmain young children by using non-invasive biomarkers of airwayinflammation and early lung function measurements: studyprotocol of a case-control study,” BMC Public Health, vol. 9,article 210, 2009.
[7] R. Beasley, U. Keil, E. Von Mutius, and N. Pearce, “Worldwidevariation in prevalence of symptoms of asthma, allergicrhinoconjunctivitis, and atopic eczema: ISAAC,” The Lancet,vol. 351, no. 9111, pp. 1225–1232, 1998.

Mediators of Inflammation 7
[8] C. V. E. Powell, P. McNamara, A. Solis, and N. J. Shaw, “Aparent completed questionnaire to describe the patterns ofwheezing and other respiratory symptoms in infants andpreschool children,” Archives of Disease in Childhood, vol. 87,no. 5, pp. 376–379, 2002.
[9] R. Pellegrino, G. Viegi, V. Brusasco et al., “Interpretative strate-gies for lung function tests,” European Respiratory Journal, vol.26, no. 5, pp. 948–968, 2005.
[10] M. R. Miller, J. Hankinson, V. Brusasco et al., “Standardisationof spirometry,” European Respiratory Journal, vol. 26, no. 2, pp.319–338, 2005.
[11] W. De Jager, H. Te Velthuis, B. J. Prakken, W. Kuis, and G.T. Rijkers, “Simultaneous detection of 15 human cytokines ina single sample of stimulated peripheral blood mononuclearcells,” Clinical and Diagnostic Laboratory Immunology, vol. 10,no. 1, pp. 133–139, 2003.
[12] K. D. G. van de Kant, K. Koers, G. T. Rijkers et al., “Can exhaledinflammatory markers predict a steroid response in wheezingpreschool children?” Clinical and Experimental Allergy, vol. 41,no. 8, pp. 1076–1083, 2011.
[13] K. D. G. Van De Kant, E. M. M. Klaassen, Q. Jobsis et al.,“Wheezing in preschool children is associated with increasedlevels of cytokines/chemokines in exhaled breath condensate,”Journal of Allergy and Clinical Immunology, vol. 126, no. 3, pp.669–671, 2010.
[14] P. J. F. M. Merkus, H. G. M. Arets, T. Joosten et al.,“Measurements of interrupter resistance: reference values forchildren 3-13 yrs of age,” European Respiratory Journal, vol. 20,no. 4, pp. 907–911, 2002.
[15] D. Curran-Everett, “Multiple comparisons: philosophies andillustrations,” American Journal of Physiology, vol. 279, no. 1,pp. R1–R8, 2000.
[16] R. J. Kurukulaaratchy, M. H. Fenn, L. M. Waterhouse, S. M.Matthews, S. T. Holgate, and S. H. Arshad, “Characterizationof wheezing phenotypes in the first 10 years of life,” Clinicaland Experimental Allergy, vol. 33, no. 5, pp. 573–578, 2003.
[17] C. M. H. H. T. Robroeks, G. T. Rijkers, Q. Jobsis etal., “Increased cytokines, chemokines and soluble adhesionmolecules in exhaled breath condensate of asthmatic chil-dren,” Clinical and Experimental Allergy, vol. 40, no. 1, pp. 77–84, 2010.
[18] G. E. Carpagnano, M. P. Foschino Barbaro, O. Resta et al.,“Exhaled markers in the monitoring of airways inflammationand its response to steroid’s treatment in mild persistentasthma,” European Journal of Pharmacology, vol. 519, no. 1-2,pp. 175–181, 2005.
[19] K. Matsunaga, T. Ichikawa, S. Yanagisawa et al., “Clinicalapplication of exhaled breath condensate analysis in asthma:prediction of FEV1 improvement by steroid therapy,” Respira-tion, vol. 78, no. 4, pp. 393–398, 2009.
[20] S. Zielen, M. Christmann, M. Kloska et al., “Predicting shortterm response to anti-inflammatory therapy in young childrenwith asthma,” Current Medical Research and Opinion, vol. 26,no. 2, pp. 483–492, 2010.
[21] A. Zacharasiewicz, N. Wilson, C. Lex et al., “Clinical use ofnoninvasive measurements of airway inflammation in steroidreduction in children,” American Journal of Respiratory andCritical Care Medicine, vol. 171, no. 10, pp. 1077–1082, 2005.
[22] M. W. Pijnenburg, E. M. Bakker, W. C. Hop, and J. C. DeJongste, “Titrating steroids on exhaled nitric oxide in childrenwith asthma: a randomized controlled trial,” American Journalof Respiratory and Critical Care Medicine, vol. 172, no. 7, pp.831–836, 2005.
[23] D. Snijders, S. Agostini, F. Bertuola et al., “Markers ofeosinophilic and neutrophilic inflammation in bronchoalve-olar lavage of asthmatic and atopic children,” Allergy, vol. 65,no. 8, pp. 978–985, 2010.
[24] D. C. Cowan, J. O. Cowan, R. Palmay, A. Williamson, andD. R. Taylor, “Effects of steroid therapy on inflammatory cellsubtypes in asthma,” Thorax, vol. 65, no. 5, pp. 384–390, 2010.
[25] P. M. C. Pitrez, S. Brennan, and P. D. Sly, “Inflammatoryprofile in nasal secretions of infants hospitalized with acutelower airway tract infections,” Respirology, vol. 10, no. 3, pp.365–370, 2005.
[26] C. Marguet, F. Jouen-Boedes, T. P. Dean, and J. O. Warner,“Bronchoalveolar cell profiles in children with asthma, infan-tile wheeze, chronic cough, or cystic fibrosis,” AmericanJournal of Respiratory and Critical Care Medicine, vol. 159, no.5 I, pp. 1533–1540, 1999.
[27] J. Douwes, P. Gibson, J. Pekkanen, and N. Pearce, “Non-eosinophilic asthma: importance and possible mechanisms,”Thorax, vol. 57, no. 7, pp. 643–648, 2002.
[28] D. Caudri, A. H. Wijga, M. O. Hoekstra et al., “Predictionof asthma in symptomatic preschool children using exhalednitric oxide, Rint and specific IgE,” Thorax, vol. 65, no. 9, pp.801–807, 2010.
[29] B. R. Davies and W. D. Carroll, “The use of inhaledcorticosteroids in the wheezy under 5-year-old child,” Archivesof Disease in Childhood, vol. 96, no. 2, pp. 61–66, 2011.
[30] I. Amirav, M. T. Newhouse, S. Minocchieri, J. A. Castro-Rodriguez, and K. G. Schuepp, “Factors that affect the efficacyof inhaled corticosteroids for infants and young children,”Journal of Allergy and Clinical Immunology, vol. 125, no. 6, pp.1206–1211, 2010.

Hindawi Publishing CorporationMediators of InflammationVolume 2012, Article ID 948367, 6 pagesdoi:10.1155/2012/948367
Review Article
Update of Faecal Markers of Inflammation in Children withCystic Fibrosis
Jung M. Lee,1 Steven T. Leach,1 Tamarah Katz,2 Andrew S. Day,3 Adam Jaffe,1, 2
and Chee Y. Ooi1, 4
1 School of Women’s and Children’s Health, Faculty of Medicine, University of New South Wales, High Street, Sydney, NSW, Australia2 Department of Respiratory Medicine, Sydney Children’s Hospital Randwick, Sydney, NSW, Australia3 Department of Paediatrics, University of Otago (Christchurch), Christchurch, New Zealand4 Department of Gastroenterology, Sydney Children’s Hospital Randwick, Sydney, NSW, Australia
Correspondence should be addressed to Chee Y. Ooi, [email protected]
Received 22 June 2012; Accepted 1 August 2012
Academic Editor: Wilco de Jager
Copyright © 2012 Jung M. Lee et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
There is evidence of intestinal inflammation in patients with CF. Intestinal inflammation may negatively impact the nutritionalstatus of patient with CF, which adversely affects pulmonary function and survival. This paper provides an up-to-date review ofintestinal inflammation in CF and an evaluation of utility of two specific faecal inflammatory markers (S100A12 and calprotectin).
1. Introduction
Cystic fibrosis (CF) is the most common, life-shortening,recessive disease in Caucasians with an average lifeexpectancy of 40 years [1]. In the majority of cases,mortality in CF is due to respiratory failure. CF is causedby mutations in the gene that encodes for the cystic fibrosistransmembrane conductance regulator (CFTR) protein [2,3]. The CFTR protein functions on the apical surface ofepithelial cells as a cyclic AMP-dependent chloride and abicarbonate channel [4, 5]. Absent or defective CFTR leadsto viscous luminal secretions in affected organs particularlyin the lungs, intestines, and pancreas.
The nutritional status of CF patients is a major deter-minant of pulmonary and survival outcomes. Longitudinalcohort studies in CF report a distinct survival advantageamong patients with better nutritional status [6–8]. Morespecifically, poor nutritional status is not only stronglylinked to poorer lung function but was also an independentrisk factor for early death in children with CF. Severalfactors contribute to impaired nutritional status in CF. Theseinclude malabsorption, recurrent sinopulmonary infections,increased energy expenditure, and suboptimal intake [9].The malabsorptive state in CF is likely multifactorial. The
primary cause of malabsorption is due to maldigestion frompancreatic exocrine insufficiency. However, children withCF can continue to have malabsorption despite pancreaticenzyme replacement therapy (PERT) administration. It hasbeen previously suggested that the presence of an acidicintestinal milieu, that impairs enzyme activity, contributesto the failure of PERT in nutrient assimilation in CF. Morerecently, intestinal inflammation has been hypothesized asanother contributing factor.
2. Intestinal Inflammation in Cystic Fibrosis
There is increasing evidence of intestinal inflammation inCF. Although the exact underlying mechanism is unknown,there have been several pathogenic mechanisms proposed(Figure 1). As a primary consequence of a defective CFTR,intestinal mucus secretions are viscid and inspissated dueto dehydration, are in an acidic milieu, and have alteredglycosylation of mucins [10, 11]. Such environmentalchanges may predispose to alterations in the balance and/orcomposition of the gut flora (dysbiosis), resulting in mucosalinflammation. Indeed, evidence to support the presenceof alterations in gut microbiota (or dysbiosis) has been

2 Mediators of Inflammation
Mu
cosa
Lum
en
Low pH due to exocrine pancreatic insufficiency
Inflammatorystimuli
Increasedinflammatory
response
Neutrophils
Intestinal epithelial
cells
Mucus layer
Bacterial overgrowthand altered
bacterial composition
CFTR
Detectable in stool
S100A12S100A9
Thick mucusS100A8
Intestinal dysmotility
Repeated and/or chronic antibiotic exposure
(e.g., IL-1, LPS )
Figure 1: Proposed pathogenesis of intestinal inflammation in cystic fibrosis.
reported in murine models of CF. Quantitative PCR ofbacterial 16S RNA in CF mice revealed a >40-fold increasein bacterial load in the small intestine alone [11]. In CFmice with proven dysbiosis, expression of inflammation-related genes decreased when these mice were treated withantibiotics, hence supporting the link between intestinaldysbiosis and inflammation in CF. Furthermore reductionof intestinal bacteria significantly improved the growth ofCF mice but had no effect on growth of wild-type mice[10]. Intestinal dysmotility was also observed in CF mice,and attributed to the further development of dysbiosisand bacterial overgrowth [11]. Secondary factors such asintestinal resection (e.g., due to meconium ileus) or earlyand/or repeated antibiotic exposure to treat sinopulmonaryinfection(s) may also influence gut microbial ecology. It hasalso been suggested that inflammation is induced by anincreased and abnormal antigenic load, which is a resultof the inadequate digestive enzymes present in the smallintestines [12].
Smyth et al. [13] previously reported measurementsof intestinal inflammatory proteins from whole gut lavageof 21 children with pancreatic insufficient (PI) CF and12 controls. This study demonstrated increased produc-tion of inflammatory biomarkers including albumin, IgG,IgM, interleukin- (IL-) 1β, IL-8, neutrophil, elastase, andeosinophilic cationic protein in children with CF. In aseparate study that compared duodenal mucosal specimens(obtained endoscopically) from 14 PI CF patients, 20 healthycontrols, and 4 non-CF patients with PI chronic pancreatitis,an increased mononuclear cell infiltrate which expressed
intercellular adhesion molecule (ICAM)-1, IL-2 receptoralpha (CD25), IL-2, and interferon-γ was observed inthe lamina propria of duodenal mucosal specimens fromCF children [14]. Interestingly, 2 CF patients who hadcommenced PERT prior to the endoscopy had evidenceof intestinal inflammation. Furthermore, small intestinalinflammation was not observed in subjects with non-CF PIchronic pancreatitis, suggesting that PI itself is unlikely thecause of intestinal inflammation.
Bruzzese and colleagues [15] were the first investigatorsto evaluate noninvasive methods for measuring intestinalinflammation using faecal calprotectin and rectal nitricoxide production. Mean (SD) faecal calprotectin levels weresignificantly higher in 30 children with PI CF compared to30 healthy controls (219 (94) μg/g versus 46 (31) μg/g), butsignificantly lower than 15 children with active inflammatorybowel disease (IBD) (309 (86) μg/g). However the incidenceof intestinal inflammation was similar with 29 of the 30 CFand all 15 of the IBD children having abnormal levels ofcalprotectin. Twenty of these children with CF, 20 controls,and 15 children with active IBD went on to have rectalnitric oxide production measured by the rectal dialysis bagtechnique. Similarly, nitric oxide levels were significantlyhigher in children with CF than controls but did not differto those with IBD. Bruzzese and colleagues then went onto give 10 CF children a probiotic, Lactobacillus casei strainGG (LGG) once a day for 4 weeks and remeasured faecalcalprotectin and rectal nitric oxide levels. Notably, bothbiomarkers of calprotectin and nitric oxide were significantlyreduced in 8 and 5 of the 10 children, respectively, suggesting

Mediators of Inflammation 3
an association between intestinal inflammation and modifi-cations in intestinal microflora.
In a more recent study, Werlin et al. [16] conducted wire-less capsule endoscopy in 41 CF patients including 13 whowere pancreatic sufficient (PS), thereby permitting directinspection of the small intestinal mucosa for endoscopicabnormalities. Signs of small intestinal inflammation includeedema, erythema, mucosal breaks, and frank ulceration in26 of the CF patients (of which 6 were PS). Those withPI generally had more pronounced mucosal changes thanthose with PS. When faecal calprotectin was obtained from asubset of these CF patients, it was normal in all 9 PS patients(23.2 ug/g) and elevated in those with PI (257.7 ug/g).
Bruzzese et al. evaluated whether abnormal intestinalmicroflora may result in an abnormal immune/inflammatory response elsewhere, such as in the lungs[17]. Using a randomized, placebo-controlled, crossoverstudy they looked at whether or not the administrationof LGG is associated with a reduction in pulmonaryexacerbations in CF. Thirty-eight children and adults with PICF were randomized to 6 months of LGG supplementationor placebo and then after a 4-week, wash-out period crossedover to the placebo and LGG group respectively. Theincidence of pulmonary exacerbations and the number ofhospital admissions were significantly higher in the placebogroup than the LGG group. Outcomes were consistentlybetter when looking at groups in parallel or longitudinally.A similar study was conducted by Weiss et al. [18].This study involved 10 patients with PI CF who receivedprobiotics (Lactobacillus acidophilus, Lactobacillus bulgaricus,Bifidobacterium bifidum, and Streptococcus thermophiles)every day for 6 months. A significant reduction in pulmonaryexacerbation was observed during the 6 months interventionperiod. Although Bruzzese et al. [17] and Weiss et al. [18]showed a reduction in pulmonary exacerbations, concurrentmeasurement of biomarkers of intestinal inflammation wasnot performed.
In addition, a possible trend between intestinal inflam-mation (as measured by faecal calprotectin) and nutritionalstatus was reported by Werlin et al. [16]. The interpretationsarising from this study, however, were limited by thereporting of mean BMI values despite having a mixedpaediatric and adult population. Based on the studiesconducted so far, there is convincing evidence that intestinalinflammation is present in CF, particularly those with PI.However the potential clinical implication of this has notbeen fully explored. Gastrointestinal inflammation is a mod-ifiable factor, which may impair nutrient absorption and,therefore, negatively impact on growth. Not all patients withintestinal inflammation had overt gastrointestinal symptomsand endoscopic evaluation is invasive, costly, and timeconsuming. The ability to identify and monitor intestinalinflammation noninvasively is therefore advantageous.
3. Faecal Inflammatory Markers
As discussed, several biomarkers have been previously usedto detect intestinal inflammation in patients with CF. These
biomarkers include S100A12, calprotectin (S100A8/S100A9),IL-8, albumin, lactoferrin, IL-1, IgM, IgG, neutrophil elas-tase, tumour necrosis factor-α, and eosinophil cationicprotein (ECP) [13, 15, 16]. The S100 proteins, calprotectinand S100A12, will be discussed in detail.
Both of these S100 biomarkers have been validatedfor use in another chronic inflammatory condition of theintestines, namely, IBD. Furthermore, both calprotectin andS100A12 have been used as markers of airway and/orsystemic inflammation in CF. On the other hand, the otherbiomarkers listed have been poorly studied in both CF andintestinal inflammation.
3.1. S100 Proteins. The human calcium-binding S100 pro-teins have been proposed to be sensitive markers of inflam-mation. S100 proteins comprise a family of more than20 calcium-binding proteins with various intracellular andextracellular roles including calcium sensing, regulation ofcell growth, cell migration, and protein phosphorylation[19–22]. A number of S100 proteins, in particular S100A8(MRP8, calgranulin A), S100A9 (MRP14, calgranulin B) andS100A12 (calgranulin C) have innate immune functions,are expressed in phagocytes [21] and are associated withinflammation.
3.2. Calprotectin (S100A8/S100A9). The proteins S100A8and S100A9 are found in granulocytes, monocytes, and earlydifferentiation stages of macrophages and each has individualintracellular and extracellular functions [22]. Furthermore,S100A9 associates with S100A8 in a complex referredto as calprotectin, which is a heterogeneous arrangementof S100A8 and S100A9. Importantly, calprotectin is alsoinduced under inflammatory conditions. Thus, calprotectinis not a disease-specific marker for CF. Nevertheless, over twodecades ago the protein complex, calprotectin, was identifiedin the serum of individuals with CF and was termed the CF-associated antigen (CFA). This complex is a heterodimer thatis secreted by a novel pathway and is present systemically orin particular fluids in a variety of inflammatory conditions[23]. S100A8 and S100A9 are found in various cell types,including neutrophils, monocytes, macrophages, dendriticcells, epithelial cells, microvascular endothelial cells, andfibroblasts, generally as a result of activation [24]. TheS100A8/S100A9 complex comprises 60% of the cytoso-lic protein in neutrophils. Inflammatory triggers such ascytokines (e.g., IL-1) or bacterial products (e.g. LPS) activatemonocytes and intestinal epithelial cells [25]. This stimulatesspecific expression and secretion of calprotectin by intestinalepithelial cells resulting in the elevated fecal calprotectinlevels in faeces. Calprotectin also activates macrophages withan interaction with toll-like receptor 4 (TLR4) inducinga positive feedback. Calprotectin activates endothelial cellsinducing expression of endothelial adhesion molecules.This activation stimulates leucocyte adherence promotingrecruitment of leucocytes to inflamed intestinal tissue. TLR4is activated on neutrophils amplifying inflammation byreleasing cytokines (IL-1, TNF-α) and reactive oxygen species(ROS). Calprotectin is released by neutrophils from this

4 Mediators of Inflammation
activation [26]. Furthermore, calprotectin may also alter thegut microbiota by chelating zinc, an essential metabolite forbacteria survival [27].
Studies reporting the use of faecal calprotectin in patientswith CF have been already been discussed. Faecal calprotectinhas been more extensively evaluated as a biomarker ofintestinal inflammation in IBD. Faecal calprotectin is able todiscriminate adults with active IBD from those with irritablebowel syndrome with 100% sensitivity and 97% specificityusing a cutoff of 30 mg/g [28, 29]. Similar distinctionshave also been made for paediatric patients with activeIBD [29–31]. von Roon et al. evaluated the diagnosticprecision of fecal calprotectin for IBD using prospectivestudies comparing fecal calprotectin against the histologicaldiagnosis and calculated a sensitivity of 95% and a specificityof 91% for the diagnosis of IBD (versus non-IBD diagnoses)[32]. Furthermore, faecal calprotectin levels were associatedwith the degree of IBD activity evaluated with clinical,endoscopic, and histological parameters [28–30, 33].
In addition, calprotectin has also been measured in theserum and respiratory tract secretions in CF patients. Goldenet al. [34] measured serum calprotectin levels in childrenwith CF, many of who had infective pulmonary exacerba-tions at the time of measurement. Serum calprotectin levelswere higher in the CF group than in healthy controls. Itwas concluded that serum calprotectin provided a betterassessment of acute airway inflammation than traditionalserum biomarkers of inflammation (such as white-cell countand C-reactive protein).
Recent data suggests that there may be interactionsbetween the production of S100 proteins and the underlyinggenetic abnormalities in CF. Renaud et al. [2] reportedpotential regulation of the expression of the S100A8 andS100A9 genes by mutations in CFTR. This associationsupports the possibility that CF may have a primaryinflammatory component, due to altered epithelial barrierfunction and decreased innate immunity at this level. Thismay occur at the respiratory and gastrointestinal epithelialborders. Thomas et al. [35] also suggested that inflammationis a primary component of CF related to an underlyingabnormal immune response. In this study, CF mice (carryingthe G551D mutation) had an altered immune response tobacterial products (e.g., LPS).
3.3. S100A12. In contrast to the broad expression pattern ofcalprotectin, S100A12 is more restricted primarily to gran-ulocytes [21, 22, 24]. S100A12 acts independently withoutS100A8 or S100A9 during calcium dependent signalling.S100A12 is exclusively released after inflammatory activationof granulocytes. S100A12 exerts inflammatory effects on avariety of cell types through binding to the receptor ofadvanced glycation end products (RAGE). RAGE ligationactivates Nuclear-Factor-(NF-) κB and related intracellularsignalling pathway with the consequent production of pro-inflammatory mediators [36]. The interaction with RAGEand receptors on endothelial cells also induces leucocyteadhesion and transmigration. Stimulation of granulocytes inan autocrine fashion results in release of cytokines like IL-1,
TNF, and ROS production. This positive feedback triggers anadditional release of S100A12 by mucosal and intraluminalgranulocytes. S100A12 is therefore closely related to granu-locyte activation.
The role of S100A12 in intestinal inflammation in CF hasnot been fully evaluated [37]. Similar to calprotectin, the roleof S100A12 as a biomarker of intestinal inflammation hasbeen better defined in IBD, where faecal S00A12 is shownto be a valid and reliable noninvasive biomarker of intestinalinflammation. S100A12 was elevated in stools collected fromchildren shown to have extensive bowel inflammation (n =20; 142.4 ± 125 mg/kg) compared to controls with nobowel condition (n = 24; 2.8 ± 4.8 mg/kg) (P < 0.0001)[38]. Furthermore, receiver operator curve analysis indicatedthat faecal S100A12 distinguished gut inflammation with96% sensitivity and 92% specificity with cutoff of 10 mg/kgand area under the curve of 99.2%. In addition, S100A12levels were stable in stool even when stool samples werestored at room temperature for up to 7 days. A furtherstudy expanded upon these findings for both S100A12 (andcalprotectin) [31]. Children with intestinal symptoms wereenrolled prospectively with faecal S100A12 and calprotectinmeasured. Half of these children were diagnosed withactive IBD upon review of mucosal biopsies. Both S100A12(median 55.2 mg/kg) and calprotectin (1265 mg/kg) wereelevated in the children with active IBD (n = 31) incontrast to the children without any inflammatory changespresent (n = 30) (S100A12 median 1.1 mg/kg, P < 0.0001;calprotectin median 30.5 mg/kg; P < 0.0001). Furthermore,S100A12 (using a cutoff of 10 mg/kg) gave a sensitivityand specificity of 97%, respectively, for the detection ofinflammation whereas calprotectin (cutoff 50 mg/kg) gave asensitivity of 100% and specificity of 67%.
In CF, Foell et al. [21] ascertained that S100A12 levelswere raised in the serum and sputum of affected patients.The population included individuals with end-stage lungdisease and others having an infective exacerbation (ratherthan young children). Mucosal expression of S100A12 wasincreased in lung biopsy samples (immunohistochemistry)and levels of S100A12 were increased in serum and spu-tum samples. Furthermore, the levels of this protein wereincreased at the time of an infective exacerbation and fellafter successful treatment, potentially playing the role of asurrogate serum marker for infectious exacerbations.
4. Areas for Future Research
Future work is required to better understand the underlyingmechanisms in the development of intestinal inflammation.As alterations in the gut microbiota have been implicated,the use of next generation high throughput sequencingtechnology to investigate the gut microbiota in CF shouldbe considered. The direct effects of intestinal inflammationon nutritional and pulmonary status have not yet been fullyinvestigated. Further work is also required to determine themost reliable biomarker(s) of intestinal inflammation in CF.In addition, the roles of targeted anti-inflammatory therapiesfor the gut as well as use of pro- and prebiotics require furtherevaluation, with promising clinical implications.

Mediators of Inflammation 5
5. Conclusion
In conclusion, there is clear evidence of intestinal inflamma-tion in CF, particularly those with PI. Intestinal inflamma-tion may negatively impact the nutritional status of patientwith CF, which in turn adversely affects pulmonary functionand survival. Small therapeutic studies using probiotics haveshown reduction in pulmonary infective exacerbations andhave lead to reductions in levels of faecal inflammatorymarkers. Faecal biomarkers of inflammation, especiallycalprotectin and S100A12, have promising roles in theidentification of these patients. Greater insights into theintestinal milieu in CF and its systemic implications aremuch needed.
Acknowledgments
The authors thank The Australian Cystic Fibrosis ResearchTrust, The Royal Australasian College of Physicians Foun-dation (Servier Staff Research Fellowship), and The SydneyChildren’s Hospital Foundation for their support and gen-erosity.
References
[1] J. R. Yankaskas, B. C. Marshall, B. Sufian, R. H. Simon, andD. Rodman, “Cystic fibrosis adult care: consensus conferencereport,” Chest, vol. 125, no. 1, supplement, pp. 1S–39S, 2004.
[2] W. Renaud, M. Merten, and C. Figarella, “Increased coex-pression of CFTR and S100 calcium binding proteins MRP8and MRP14 mRNAs in cystic fibrosis human tracheal glandcells,” Biochemical and Biophysical Research Communications,vol. 201, no. 3, pp. 1518–1525, 1994.
[3] J. R. Riordan, J. M. Rommens, B. S. Kerem et al., “Identifica-tion of the cystic fibrosis gene: cloning and characterization ofcomplementary DNA,” Science, vol. 245, no. 4922, pp. 1066–1073, 1989.
[4] P. M. Quinton, “Chloride impermeability in cystic fibrosis,”Nature, vol. 301, no. 5899, pp. 421–422, 1983.
[5] M. M. Reddy and P. M. Quinton, “Selective activation ofcystic fibrosis transmembrane conductance regulator Cl- andHCO3- conductances,” Journal of the Pancreas, vol. 2, no. 4,pp. 212–218, 2001.
[6] M. Corey, F. J. McLaughlin, M. Williams, and H. Levison, “Acomparison of survival, growth, and pulmonary function inpatients with cystic fibrosis in Boston and Toronto,” Journal ofClinical Epidemiology, vol. 41, no. 6, pp. 583–591, 1988.
[7] H. C. Lai, M. Corey, S. Fitzsimmons, M. R. Kosorok, and P. M.Farrell, “Comparison of growth status of patients with cysticfibrosis between the United States and Canada,” AmericanJournal of Clinical Nutrition, vol. 69, no. 3, pp. 531–538, 1999.
[8] M. Corey, K. Gaskin, P. Durie, H. Levison, and G. Forstner,“Improved prognosis in CF patients with normal fat absorp-tion,” Journal of Pediatric Gastroenterology and Nutrition, vol.3, supplement 1, pp. S99–S105, 1984.
[9] P. B. Pencharz and P. R. Durie, “Pathogenesis of malnutritionin cystic fibrosis, and its treatment,” Clinical Nutrition, vol. 19,no. 6, pp. 387–394, 2000.
[10] O. Norkina, T. G. Burnett, and R. C. De Lisle, “Bacterialovergrowth in the cystic fibrosis transmembrane conductanceregulator null mouse small intestine,” Infection and Immunity,vol. 72, no. 10, pp. 6040–6049, 2004.
[11] R. C. De Lisle, “Altered transit and bacterial overgrowth inthe cystic fibrosis mouse small intestine,” American Journal ofPhysiology, vol. 293, no. 1, pp. G104–G111, 2007.
[12] A. B. Ballinger, C. Camacho-Hubner, and N. M. Croft,“Growth failure and intestinal inflammation,” QJM, vol. 94,no. 3, pp. 121–125, 2001.
[13] R. L. Smyth, N. M. Croft, U. O’Hea, T. G. Marshall, and A.Ferguson, “Intestinal inflammation in cystic fibrosis,” Archivesof Disease in Childhood, vol. 82, no. 5, pp. 394–399, 2000.
[14] V. Raia, L. Maiuri, G. de Ritis et al., “Evidence of chronicinflammation in morphologically normal small intestine ofcystic fibrosis patients,” Pediatric Research, vol. 47, no. 3, pp.344–350, 2000.
[15] E. Bruzzese, V. Raia, G. Gaudiello et al., “Intestinal inflam-mation is a frequent feature of cystic fibrosis and is reducedby probiotic administration,” Alimentary Pharmacology andTherapeutics, vol. 20, no. 7, pp. 813–819, 2004.
[16] S. L. Werlin, I. Benuri-Silbiger, E. Kerem et al., “Evidenceof intestinal inflammation in patients with cystic fibrosis,”Journal of Pediatric Gastroenterology and Nutrition, vol. 51, no.3, pp. 304–308, 2010.
[17] E. Bruzzese, V. Raia, M. I. Spagnuolo et al., “Effect of Lacto-bacillus GG supplementation on pulmonary exacerbations inpatients with cystic fibrosis: a pilot study,” Clinical Nutrition,vol. 26, no. 3, pp. 322–328, 2007.
[18] B. Weiss, Y. Bujanover, Y. Yahav, D. Vilozni, E. Fireman,and O. Efrati, “Probiotic supplementation affects pulmonaryexacerbations in patients with cystic fibrosis: a pilot study,”Pediatric Pulmonology, vol. 45, no. 6, pp. 536–540, 2010.
[19] J. A. Tibble, G. Sigthorsson, S. Bridger, M. K. Fagerhol, andI. Bjarnason, “Surrogate markers of intestinal inflammationare predictive of relapse in patients with inflammatory boweldisease,” Gastroenterology, vol. 119, no. 1, pp. 15–22, 2000.
[20] B. E. Golden, P. A. Clohessy, G. Russell, and M. K. Fagerhol,“Calprotectin as a marker of inflammation in cystic fibrosis,”Archives of Disease in Childhood, vol. 74, no. 2, pp. 136–139,1996.
[21] D. Foell, S. Seeliger, T. Vogl et al., “Expression of S100A12 (EN-RAGE) in cystic fibrosis,” Thorax, vol. 58, no. 7, pp. 613–617,2003.
[22] R. Donato, “Intracellular and extracellular roles of S100proteins,” Microscopy Research and Technique, vol. 60, no. 6,pp. 540–551, 2003.
[23] D. Foell, H. Wittkowski, T. Vogl, and J. Roth, “S100 proteinsexpressed in phagocytes: a novel group of damage-associatedmolecular pattern molecules,” Journal of Leukocyte Biology,vol. 81, no. 1, pp. 28–37, 2007.
[24] N. S. M, “The S100 family of multipurpose calcium-bindingproteins,” Journal of Cutaneous Pathology, vol. 25, no. 10, pp.521–529, 1998.
[25] D. Foell, H. Wittkowski, and J. Roth, “Monitoring diseaseactivity by stool analyses: from occult blood to molecularmarkers of intestinal inflammation and damage,” Gut, vol. 58,no. 6, pp. 859–868, 2009.
[26] P. Brandtzaeg, T. O. Gabrielsen, I. Dale, F. Muller, M.Steinbakk, and M. K. Fagerhol, “The leucocyte proteinL1 (calprotectin): a putative nonspecific defence factor atepithelial surfaces,” Advances in Experimental Medicine andBiology, vol. 371, pp. 201–206, 1995.
[27] P. G. Sohnle, M. J. Hunter, B. Hahn, and W. J. Chazin, “Zinc-reversible antimicrobial activity of recombinant calprotectin(migration inhibitory factor-related proteins 8 and 14),”Journal of Infectious Diseases, vol. 182, no. 4, pp. 1272–1275,2000.

6 Mediators of Inflammation
[28] J. Tibble, K. Teahon, B. Thjodleifsson et al., “A simple methodfor assessingintestinal inflammation in Crohn’s disease,” Gut,vol. 47, pp. 506–513, 2000.
[29] S. K. Bunn, W. M. Bisset, M. J. Main, and B. E. Golden, “Fecalcalprotectin as a measure of disease activity in childhoodinflammatory bowel disease,” Journal of Pediatric Gastroen-terology and Nutrition, vol. 32, pp. 171–177, 2001.
[30] S. K. Bunn, W. M. Bisset, M. J. C. Main, E. S. Gray, S.Olson, and B. E. Golden, “Fecal calprotectin: validation asa noninvasive measure of bowel inflammation in childhoodinflammatory bowel disease,” Journal of Pediatric Gastroen-terology and Nutrition, vol. 33, no. 1, pp. 14–22, 2001.
[31] M. A. Sidler, S. T. Leach, and A. S. Day, “Fecal S100A12 andfecal calprotectin as noninvasive markers for inflammatorybowel disease in children,” Inflammatory Bowel Diseases, vol.14, no. 3, pp. 359–366, 2008.
[32] A. C. von Roon, L. Karamountzos, S. Purkayastha et al.,“Diagnostic precision of fecal calprotectin for inflammatorybowel disease and colorectal malignancy,” American Journal ofGastroenterology, vol. 102, no. 4, pp. 803–813, 2007.
[33] F. Costa, M. G. Mumolo, M. Bellini et al., “Role of faecal cal-protectin as non-invasive marker of intestinal inflammation,”Digestive and Liver Disease, vol. 35, no. 9, pp. 642–647, 2003.
[34] B. E. Golden, P. A. Clohessy, G. Russell, and M. K. Fagerhol,“Calprotectin as a marker of inflammation in cystic fibrosis,”Archives of Disease in Childhood, vol. 74, no. 2, pp. 136–139,1996.
[35] G. R. Thomas, E. A. Costelloe, D. P. Lunn et al., “G551D cysticfibrosis mice exhibit abnormal regulation of inflammation inlungs and macrophages,” Journal of Immunology, vol. 164, no.7, pp. 3870–3877, 2000.
[36] M. A. Hofmann, S. Drury, C. Fu et al., “RAGE mediates anovel proinflammatory axis: a central cell surface receptor forS100/calgranulin polypeptides,” Cell, vol. 97, no. 7, pp. 889–901, 1999.
[37] C. Y. Ooi, J. M. Lee, S. Leach, T. Katz, A. S. Day, and A. Jaffe,“Intestinal inflammation in CF: stool markers and correlationwith pancreatic enzymes,” Journal of Cystic Fibrosis, vol. 11,supplement 1, p. S114, 2012.
[38] N. S. H. de Jong, S. T. Leach, and A. S. Day, “Fecal S100A12:a novel noninvasive marker in children with Crohn’s disease,”Inflammatory Bowel Diseases, vol. 12, no. 7, pp. 566–572, 2006.

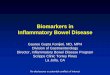



![Pretreatment inflammatory indices predict Bevacizumab … · 2020. 8. 8. · However, we know less about the roles that inflammatory indices play as biomarkers for GBM patients[30-33]](https://img.pdfslide.net/doc/110x75/602dc614c34cdc70c244751e/pretreatment-inflammatory-indices-predict-bevacizumab-2020-8-8-however-we.jpg)























