Embed Size (px)
Citation preview

BIOMONITORING OF GENOTOXIC AND CYTOTOXIC
CHANGES AMONG PATIENTS EXPOSED TO DIGITAL
RADIOGRAPHS - A COMPARATIVE STUDY
DISSERTATION
Submitted to The Tamil Nadu Dr. M.G.R Medical University in
partial fulfillment of the requirement for the degree of
MASTER OF DENTAL SURGERY
BRANCH IX
ORAL MEDICINE AND RADIOLOGY
2012 - 2015

CERTIFICATE
This is to certify that this dissertation titled “Biomonitoring of
Genotoxic and Cytotoxic Changes Among Patients Exposed to Digital
Radiographs – A Comparative Study” is a bonafide research work done
by Dr. Meera Mathai under our guidance during her Post Graduate study
during the period of 2012-2015 under THE TAMIL NADU Dr. M.G.R.
MEDICAL UNIVERSITY, CHENNAI, in partial fulfillment for the degree
of MASTER OF DENTAL SURGERY IN ORAL MEDICINE AND
RADIOLOGY, BRANCH IX. It has not been submitted (partial or full) for
the award of any other degree or diploma.
Dr. TATU JOY. E M.D.S
Guide
Professor and HOD
Department of Oral Medicine and Radiology
Sree Mookambika Institute of Dental Sciences,
Kulasekharam.
Dr. HEMA. G M.D.S
Co- Guide
Reader
Department of Oral Medicine and Radiology
Sree Mookambika Institute of Dental Sciences,
Kulasekharam.

SREE MOOKAMBIKA INSTITUTE OF DENTAL
SCIENCES, KULASEKHARAM
ENDORSEMENT BY THE PRINCIPAL / HEAD OF THE INSTITUTION
This is to certify that this dissertation titled “Biomonitoring of
Genotoxic and Cytotoxic Changes among Patients Exposed to Digital
Radiographs – a Comparative Study” is a bonafide research work done by
Dr. Meera Mathai under the guidance of Dr. Tatu Joy E MDS, Professor
and Head, Department of Oral Medicine and Radiology, Sree Mookambika
Institute of Dental Sciences, Kulasekharam.
Dr. Elizabeth Koshi MDS
PRINCIPAL
Sree Mookambika Institute of Dental Sciences
V.P.M Hospital Complex
Padanilam, Kulasekharam.
KanyaKumari District.
Tamil Nadu - 629 161

ACKNOWLEDGEMENT
I extend my profound gratitude to my guide Dr. Tatu Joy E MDS, Professor
& Head of the Department for his invaluable guidance, co-operation, constant
encouragement and immense patience with me in every step of this endeavor. I thank
him for the trust he had in me that made me to complete this work.
I am thankful to my co- guide Dr. Hema G MDS Reader, Department of Oral
Medicine & Radiology for the support she showed me in completing this work.
Am grateful to Dr. Shashi Kiran M MDS Reader, Department of Oral
Medicine & Radiology for his constant enthusiasm, strive for perfection, and patience
he showed me for writing this study. With comforting words and smile, he persuaded
us to develop our presentation skill.
I take this opportunity to express my sincere gratitude to my teachers Dr.
Eugenia Sherubin, Dr. Raghupathy for the constant encouragement throughout the
course of this study
I would like to acknowledge the help & support given by Dr. Velayuthan
Nair, chairman and Dr. Rema V Nair director Sree Mookambika Institute of Dental
Sciences without which my study would not have been possible
It is my utmost privilege to acknowledge Dr. Issac Joseph Head of
Department Oral Pathology & Microbiology for his kindness by permitting me to use
the facilities in his department.

I am indebted to Dr. Deepa A G, Senior lecturer Department of Oral
pathology & microbiology for helping me with the study.
Am grateful to Dr. Pratheesh Sathyan Reader Department of Oral pathology
& Microbiology for his valuable suggestions in this work.
I thank Kalavathy, in the department of Oral Pathology & Microbiology for
helping me in the study.
I thank my batch mates, Dr. Redwin Dhas Manchil, Dr. Vineetha
Vijayakumar for their support and encouragement.
I would like to thank my juniors Dr. Indu Krishna, Dr. Melbia Shiny for
helping me to get through difficult times and for all emotional support and caring.
I thank Dr. George Jacob Dr. Gomakumar and Dr. Arun Mohan, my
fellow PGs in the department of Oral Pathology & Microbiology for being helpful,
and providing me with the support and encouragement for fulfilling thesis work.
I would like to thank Dr. Sainul Abideen Reader INDIAN INSTITUTE OF
SCIENCE AND RESEARCH for his immense kindness that made me possible to
write the thesis by providing me the articles.
I would like to thank Dr. Anand Reader Department of Community Dentistry,
Koorg Institute of Dental Science for helping me with my statistical work.
Words are less to express my deep gratitude to Emily Andrews, first best
friend then my mother, my loving father P. J. Mathai and caring brother Dr. Kiran
Mathai for their support and encouragement they have given me throughout my life.

I would like to thank my friend Dr. Arya Ravisankar for her immense faith
and support and positive energy she filled in me. I would extend my sincere gratitude
to Dr. Swathy Anand Senior lecturer Rajas Dental college for his support and
suggestions for writing this study.
I thank almighty for his blessings he had given on me in my life.

CONTENTS
NO TITLE PAGE NO
1 List of abbreviations i - ii
2 List of tables iii - iv
3 List of graphs v
4 List of colour plates vi
5 List of annexures vii
6 Abstract viii - ix
7 Introduction 1-3
8 Aim and objectives 4
9 Review of literature 5 -33
10 Materials and methods 34 - 42
11 Results and observations 43 - 53
12 Discussion 54 - 60
13 Summary and conclusion 61
14 Bibliography x - xxii
15 Annexures

i
LIST OF ABBREVEATIONS
PAP: Papanicolaou stain
MN: Micronucleus
NCRP: National Council on Radiation Protection and Measurements
FISH: Fluorescent insitu hybridization
MGG: May-Gruwald Giemsa
KR: Karyorrhexis
PN: Pyknosis
KL: Karyolysis
CC: Condensed chromatin
SCC: Squamous cell carcinoma
TB: Toluidine blue
FNAC: Fine Needle Aspiration Cytology
OSMF: Oral Sub Mucous Fibrosis
PMDs: Potentially Malignant Diseases
CBCT: Cone Beam Computed Tomography
CT: Computed Tomography
IOPA: Intra Oral Periapical radiograph
OPG: Orthopantomograph

ii
C2H5N+: Acrylonitrite group
D.P.X: Din butyl phthate in Xylene
SPSS: statistical package for social sciences

iii
LIST OF TABLES
Table No Title of the table
Table -1 Distribution of study subjects according to age and gender
Table - 2 Total No of cells having Micronucleus before and after
radiation/100 cells
Table – 3 Total No of Micronucleus before and after radiation/100
cells
Table – 4 Mean value & standard deviation of MN assay
Table – 5 Total No of cells having Karyorrhexis before and after
radiation/100 cells
Table – 6 Total No of cells having Karyolysis before and after
radiation/100 cells
Table – 7 Total No of cells having Pyknosis before and after
radiation/100 cells
Table – 8 Mean value & standard deviation of cytological changes

iv
Table – 9 Gender variation in micronucleus count
Table – 10 Gender wise comparison of micronucleus
Table – 11 Gender wise comparison of Karyorrhectic cell count
Table – 12 Gender wise comparison of Karyorrhexis
Table – 13 Gender wise comparison of karyolitic cell count
Table – 14 Gender wise comparison of karyolysis
Table – 15 Gender wise comparison of Pyknotic cell count
Table – 16 Gender wise comparison of pyknosis

v
LIST OF GRAPHS
Graph No
TITLE OF THE GRAPH
Graph - 1
Distribution of study subjects according to gender and age
Graph - 2
Mean changes in Genotoxic and Cytotoxic parameters
before and after radiation exposure among study subjects
Graph - 3
Gender wise comparison for micronucleus before and after
radiation exposure
Graph - 4
Gender wise comparison for Karyorrhexis before and after
radiation exposure
Graph - 5
Gender wise comparison for Karyolysis before and after
radiation exposure
Graph - 6
Gender wise comparison for Pyknosis before and after
radiation exposure

vi
LIST OF COLOUR PLATES
Color Plate No
Title of Color Plate
CP - 1
Armamentarium for sample collection
CP - 2
Planmeca Prolin XC machine
CP - 3
RAPID PAPTM
staining kit
CP - 4
Stained slides in slide box
CP- 5
Light microscope with AP viewer

vii
LIST OF ANNEXURES
Annexure No Title of Annexure
Annexure -1 Certificate from Institutional Human Ethics
Committee
Annexure - 2 Patient information sheet
English
Malayalam
Tamil
Annexure - 3 Patient consent form
English
Malayalam
Tamil
Annexure - 4 Case record form
Annexure - 5 Study observation sheet

ABSTRACT

Abstract
viii
Background of the study
The discovery of X- rays is considered as the discovery of the 20th
century. It
has its boon as it is an important tool for diagnosis and treatment in medical and
dental practice. However its bane remains as ionizing radiation is a well known
mutagen and carcinogen for the human population. It is largely known that there is no
safety in radiation doses and that the biological effects of exposure received would be
accumulated through time. In order to detect the effects of low dose ionizing radiation
in diagnostic radiology various sensitive analysis are needed.
Aim
The aim of this study is the evaluation of genotoxicity and cytotoxicity in
patients after exposure to digital radiographs.
Materials & methods
Clinically healthy patients who required orthodontic treatment were selected.
As a part of their treatment plan, they were exposed to x rays for making
orthopantomogram and lateral cephalogram. Smears were taken from the buccal
mucosa before exposure and 10±2 days after exposure. The smears were fixed and
stained with DNA specific PAP stain using RAPID PAPTM
staining kit. 100 cells were
analyzed on each slide under 40 × magnification using light microscope with the help
of AP viewer.

Abstract
ix
1. For the evaluation of Genotoxicity, presence of micronucleus was estimated.
2. For the determination of cytotoxicity, parameters taken were Karyorrhexis,
karyolysis and pyknosis.
Results
There was a significant increase in the number of micronuclei after radiation
exposure which indicates that the x rays can produce genotoxic damage to the cells.
There was also an increase in the number of other nuclear alterations after exposure
which indicated the increased cytotoxicity produced by radiation. There is no gender
predilection found in this study.
Conclusion
Radiography is one of the most valuable diagnostic tool used in
comprehensive dental care for diagnosis, treatment planning and for follow up. This
study concluded that even low level ionizing radiation can induce both genotoxic and
cytotoxic damage to the cells. Hence radiographs should be advised only when it is of
utmost necessity.
KEYWORDS: Ionizing radiation, Micronucleus, Karyorrhexis, Karyolysis, Pyknosis

INTRODUCTION

Introduction
1
Carcinogenesis is a multistep process governed by genetic or epigenetic
mechanisms and signaling pathways and in at least any one of those steps there will
be a change in cellular behavior and morphology due to mutations related to the
control of cell division, cell death and metastatic potential. Among the multiple
mutations found in human cancers such as gene amplification, chromosome
alterations and translocations, point mutation is very important.1 When the normal
function of DNA repair is altered as a result of mutation by various agents, the risk of
malignant transformation increases. Among these agents, ionizing radiation forms the
bulk of contribution to human exposure because of its wide use for diagnostic and
therapeutic purposes.
X rays are potent mutagenic agent capable of inducing both gene mutation and
chromosomal aberrations. They act directly on DNA molecule or indirectly through
the formations of reactive compounds that interact with DNA. In spite of their
mutagenic potential, X- rays are an important tool in diagnosing disease and are used
in both medical and dental practice. Taking the strong evidence for relationship
between DNA damage and carcinogenesis into considerations, it would be useful to
know the harmful effects induced by X- rays.
Accumulating evidence suggests that the radiographs which are widely used
for diagnosis in medical and dental practice can induce cytotoxic effects and cause
DNA damage. The nucleus (including its genetic material) is more radiosensitive than
the cytoplasmic structures of the cell. Therefore the elucidation of the genotoxic
effects induced by radiography is relevant to identify and minimize potential risk to
the patient.

Introduction
2
Research on these issues has to be primarily addressed on reduction in the
radiation dose to the patient. Although it is generally accepted that there is no safe
level of radiation exposure, the possible risk associated with the exposure to X-rays
must be outweighed against the clinical benefits. With this in mind, various methods
have been developed to detect radiation effects of low dose radiographic exposure.2
Biomonitoring studies have been used in health sciences for many years to
assist in diagnosing and staging diseases as well as to evaluate the risk assessment.
They give information concerning environmental exposure and susceptibility. These
studies are divided into three groups; first to define the exposure to mutagenic and/or
carcinogenic agents, second to show the biological effects on target tissues and third
to give information about the individual susceptibility.
Cytogenetic biomonitoring has been used in health sciences for many years in
diagnosing and staging diseases, as well as in risk assessment, and provides
information concerning levels of risk and susceptibility status. A variety of assays has
been proposed as potential tools in cytogenetic biomonitoring studies, including those
that assess metaphase chromosomal aberrations, sister chromatid exchanges and
deoxyribonucleic acid (DNA) damage and repair. However, these methods are
typically laborious and time-consuming or require highly trained technicians to
accurately read and interpret slides.
Biomarkers are biologic parameters that provide information about a
physiologic or pathologic state of an individual or population. National institute of
health defined the term biomarker as a characteristic that is objectively measured and
evaluated as an indicator of normal biological process, pathological processes or
pharmacological responses to a therapeutic intervention or other health care

Introduction
3
interventions.3 Molecular epidemiology research focuses on three types of
biomarkers; biomarker of exposure (chromosomal aberrations, micronucleus, sister
chromatid exchange), biomarker of susceptibility (genetic polymorphism) and
biomarkers of disease( tumor biomarker).4
Micronuclei and other nuclear abnormalities are biomarker that offers
additional endpoints for possible evaluation of chromosomal instability and different
cell death events (Karyorrhexis, pyknosis). Micronucleus can be evaluated in many
tissues involving any dividing cells like bladder, esophagus, bronchial nasal and
buccal mucosa.
Buccal epithelial cells provide an alternative source of tissue for human
monitoring to occupational and environmental toxic exposures. This tissue is under
direct radiation exposure during panoramic radiography and lateral cephalometric
radiography and in this way it is a primary target for radiation induced damage.
Furthermore this tissue has an advantage of rapid and easy sampling by brushing the
buccal mucosa. Accurately the presence of micronucleus is observed in exfoliated
epithelial tissues which are derived from the basal layer where the cell division takes
place and they migrate towards the surface within 5-14 days. In this manner, the
epithelial tissues can reflect damage occurred at this time.3
As there is a strong association between DNA damage and carcinogenesis, the
present study is aimed to evaluate the genotoxic and Cytotoxic effects of low level
ionizing radiation used in dental radiography on buccal epithelial cells by a simple
technique.

AIM & OBJECTIVES

Aim & Objectives
4
AIM
1. To compare the genotoxic and Cytotoxic changes after exposure to low level
diagnostic ionizing radiation
OBJECTIVES
1) To assess the number of micronuclei before and after digital radiographs
2) To assess Karyorrhexisbefore and after digital radiographs.
3) To assess karyolysisbefore and after digital radiographs.
4) To assess pyknosis before and after digital radiographs.
5) To assess the variation of these factors based on gender.

REVIEW OF LITERATURE

Review of Literature
5
The study of DNA damage in exfoliated cells collected from the oral cavity holds
great promise as a minimally invasive method for monitoring populations exposed to
genotoxic agents. The presence of micronuclei (MN) and other nuclear anomalies within
these cells has been known to be associated with genetic defects in genome maintenance,
accelerated ageing, exposure to genotoxic agents, oral cancer risk and neurodegenerative
diseases and was also used in chemo preventive studies.5
The first case of human injury was reported in the literature just a few months
following Roentgen's original paper in 1895 announcing the discovery of x-rays. As early
as 1902, the first case of x-ray induced cancer was reported in the literature.6
Radiation damage starts at the cellular level. The mechanism by which the
damage occurs can happen via
(a) direct action
(b) indirect action
A. Direct Action
Radiation may impact the DNA directly, causing ionization of the atoms
in the DNA molecule. This ionization results in the breakage of the macromolecule‟s
chemical bonds causing them to become abnormal structures which may lead to adverse
chemical reactions. Subsequent chromosomal damage includes abnormal replication, cell
death or temporary damage. If the radiation directly affects the somatic cells, the effects
on the DNA could result in radiation induced malignancy. If damage is to the

Review of Literature
6
reproductive cells, the result could be radiation induced congenital abnormality. This can
be visualized as a “direct hit” by the radiation on the DNA, and thus is a fairly
uncommon occurrence due to the small size of the target; the diameter of the DNA helix
is only about 2 nm.
B. Indirect Action
In the second scenario, the radiation interacts with non-critical target atoms or
molecules, usually water. This results in the production of free radicals, which are atoms
or molecules that have an unpaired electron and thus are highly reactive. These free
radicals can then attack critical targets such as the DNA. Because they are able to diffuse
only some distance in the cell, the initial ionization event does not have to occur so close
to the DNA in order to cause damage. Thus, damage from indirect action is much more
common than damage from direct action, especially for radiation that has a low specific
ionization.
When the DNA is attacked, either via direct or indirect action, damage is caused
to the strands of molecules that make up the double-helix structure. Most of this damage
consists of breaks in only one of the two strands and is easily repaired by the cell, using
the opposing strand as a template. If, however, a double-strand break occurs, the cell has
much more difficulty repairing the damage and may make mistakes. This can result in
mutations, or changes to the DNA code, which can result in consequences such as cancer
or cell death. Double-strand breaks occur at a rate of about one double-stand break to 25
single-strand breaks. Thus, most radiation damage to DNA is reparable.

Review of Literature
7
The general population is exposed to various types of radiation, mainly natural
and manmade radiation. Natural radiation is caused by terrestrial sources and cosmic
sources. Sources of manmade radiation includes medical and diagnostic treatment,
consumer and industrial products.7
AVERAGE ANNUAL EFFECTIVE DOSE OF IONIZING RADIATION.7
Source Dose [µSv]
Natural
Cosmic 0.4
Terrestrial
External 0.5
Radon 1.2
Other 0.3
Manmade
Medical X-ray diagnosis 2
Nuclear medicine 0.5
Other consumer products 0.08
Occupational 0.01
Fallout 0.01
Nuclear fuel cycle <0.01
Dental radiology ≤0.01

Review of Literature
8
DOSE LIMITS
After recognizing harmful effects of radiation and risks involved in the use
National Council on Radiation Protection and Measurements [NCRP] and International
Council on Radiological Protection has established guidelines for the limitations of
radiation received by both occupationally exposed to individuals and public.
EEFECTIVE DOSE FROM DIAGNOSTIC X-RAY EXAMINATIONS AND
EQUIVALENT BACKGROUND EXPOSURE.7
EXAMINATION EFFECTIVE DOSE
[µSv]
Equivalent background
exposure [days]
Extra oral
Panoramic 9-26 1-3
Cephalometric 3-6 0.5-1
CBCT [Galileo‟s] 70 9
CT 2000 243
Plain Skull 70 9
CHROMOSOMAL ABBERATIONS
To study the carcinogenic potential of ionizing radiation, Chromosomal alteration
is another important tool. Lea et al in 1946 had mentioned the chromosomal aberrations
due to ionizing radiations with the data obtained in plant cells and Drosophila. The types
and frequencies of induced chromosomal aberrations depend on the mutagen used and the
stage of the cell cycle treated.

Review of Literature
9
Ionizing radiations produce chromosomal aberrations in G 1 stage of cell cycle.
These chromosomal aberrations have been used to monitor human exposure to genotoxic
agents and in patients treated with cytotoxic drugs in peripheral lymphocytes. Structural
chromosome aberrations arise from direct DNA breakage, replication on a damaged DNA
template or inhibition of DNA synthesis and may involve both chromatids of the
chromosome or only one chromatid of the chromosome.
MICRONUCLEUS
The action of carcinogens can induce chromosomal instabilities such as deletions,
translocations, gain or loss of entire chromosomes, contributing to the development of
malignant cellular processes.8 Micronucleus (MN) is a small additional nucleus and is
readily identifiable by light microscopy. During the last few decades, it has generally
been used as a biomarker of chromosomal damage, genome instability and cancer risk.
The MN test provides a reliable measure of chromosome breakage and chromosome
loss.9 The level of baseline chromosome damage in untreated cancer patients and also in
various preneoplastic conditions is much higher than in cancer-free controls. Therefore,
MN scoring can be used as a bio-marker to identify different pre-neoplastic conditions
much earlier than the manifestations of clinical features and might specifically be
exploited in the screening of high-risk population for a specific cancer.10
The
micronucleus (MN) test has been extensively used in a variety of investigations to
understand the basic mechanisms underlying Genotoxicity.11

Review of Literature
10
HISTORICAL PERSPECTIVE
In the late 1800s and early 1900s Howell and Jolly described Feulgen – positive
nuclear bodies in human reticulocytes, known as Howell – Jolly bodies and representing
the chromosomes separated from the mitotic spindle.12
The micronucleus (MN) assay
was used for the first time in vitro in radiation experiments with roots of Vicia faba by
Evans et al. in 1959 and for in vivo bone marrow cell studies by Schmid et al in the early
seventies.13, 14
In the early 1970s the term micronucleus test was suggested for the first time by
Boller and Schmidt and Heddle who showed that this assay provided a simple method to
detect the genotoxic potential of mutagens after in vivo exposure of animals using bone
marrow erythrocytes.4 In 1982, the suitability of MN test for human biomonitoring
studies was first described by Stich & co- workers who used exfoliated cells of buccal
mucosa. They postulated that this test system can be used to study genotoxic effects in all
human tissues from which exfoliated cells can be obtained.15
A few years later it was
shown by Countryman and Heddle that peripheral blood lymphocytes could be used for
the micronucleus approach and they recommended using micronuclei as a biomarker in
testing schemes.
The Human Micronucleus [HUMAN] Project is an international collaborative
project aimed at studying the micronucleus frequency in human populations and
assessing the effects of protocol and scoring criteria on the values obtained. It was
established in 1997 and currently involves more than 35 laboratories worldwide. It has
three main goals; (a) compilation and comparison of base line micronucleus frequencies

Review of Literature
11
in human population to establish “normal base-line frequencies of DNA damage and
determine the main demographic, environmental and methodological variables that
impact on this index; (b) comparison of variable methods used to measure MN
frequencies in human blood and epithelial cells to identify the important methodological
variables and establish standard protocols to enable more reliable comparison of data
among laboratories and among populations; and (c) to establish prospective
epidemiological studies aimed at determining whether the MN frequency predicts risk of
cancer and other degenerative diseases associated with DNA damage and
ageing.16,17,18,19,20,21
The oral epithelium is composed of four strata of structural, progenitor, and
maturing cell populations, that is, the basal cell layer (stratum basale), prickle cell layer
(stratum spinosum), and the keratinized layer at the surface. A series of finger-like
structures called "rete pegs" project up from the lamina propria into the epidermal layer
producing an undulating basal cell layer effect. The oral epithelium maintains itself by
continuous cell renewal whereby new cells produced in the basal layer by mitosis migrate
to the surface replacing those that are shed. The basal layer contains the stem cells that
may express genetic damage (chromosome breakage or loss) as MN during nuclear
division. The daughter cells, which may or may not contain MN, eventually differentiate
into the prickle cell layer and the keratinized superficial layer, and then exfoliate into the
buccal cavity. Some of these cells may degenerate into cells with condensed chromatin,
fragmented nuclei (Karyorrhectic cells), Pyknotic nuclei, or completely lose their nuclear
material (karyolitic or "ghost" cells). In rare cases, some cells may be blocked in a

Review of Literature
12
binucleated stage or may exhibit nuclear buds (also known as "broken eggs" in buccal
cells), a biomarker of gene amplification.
These biomarkers of genome damage (Eg: MN, nuclear buds) and cell death (Eg:
apoptosis, karyolysis) can be observed in both the lymphocyte and buccal cell systems,
and thus provide a more comprehensive assessment of genome damage and MN in the
context of cytotoxicity and cytostatic effects. Micronuclei derived from acentric
chromosome fragment can be distinguished from those derived from whole chromosome
by FISH using a pancentromeric probe, which will detect the centromere in the
micronucleus. Thus, clastogenic and aneugenic events can be detected by the MN
technique.22
In various studies which evaluates MN in patients undergoing radiotherapy in
head and neck region, the most striking increase in the cytogenetic damage [150-300
MN/1000cells] was observed in early phase of treatment where they are exposed to a
cumulative dose of 3400-4000 cGy.23
Other authors reported 68 MN/1000 cells after
2000 cGy and 16 MN/ 1000 cells after treatment with 1000 cGy for 3 weeks.24, 25
Theories of Origin of MN
There are two predominant mechanisms leading to the formation of MN in a
mitotic cell: chromosomal breakage and dysfunction of the mitotic apparatus. Clastogens
induce chromosome breaks and yield acentric fragments. These chromosomal fragments
are directly included into micronuclei. In other mechanism, aneugenic agents prevent the
formation of the spindle apparatus during mitosis. As a result of it the whole
chromosomes lag behind at anaphase. The chromosome is surrounded by the nuclear

Review of Literature
13
envelope, forming micronuclei. Therefore the daughter cells have micronuclei containing
whole chromosomes.
Besides these two important mechanisms, MN may be formed due to broken
anaphase bridges. This may be because of dicentric chromatids, intermingled ring
chromosomes or union of sister chromatids. MN may not always represent the loss of
chromosomal material as it may be also be formed due to amplified DNA budding.
Causes of MN Formation
There are several of causes of MN formation. This may be noted spontaneously in
the normal healthy individual due to exposure to environmental pollutants, radiation, bio-
hazard materials, and drugs, other poisonous chemicals and free-radical injuries. The
other causes of MN formation are long standing chronic inflammation, heavy metal
poisoning, chemotherapy, radiation injuries, and various preneoplastic and neoplastic
conditions. Besides that a large number of genetic diseases, infections, and nutritional
deficiency are also responsible for MN formation. Direct DNA damage or breakage,
chromosomal aberrations, mitotic apparatus dysfunctions, and interference with DNA
synthesis are the possible explanations of MN formation. The mechanism by which the
chromosomes or chromatids getting eliminated from the daughter cells is not understood
fully.26
It may be probably those displaced at metaphase and gets predispose to “lag” at
this phase of cell division after other chromatids have moved to the other spindle poles.27
It has also been shown that some micronuclei can perform DNA synthesis and mitotic
condensation synchronously with the main nucleus further producing chromosome loss
and gain at successive mitotic cycles.28

Review of Literature
14
CATEGORY ETIOLOGY EXPLANATIONS
Spontaneous Healthy persons Exposure to environmental
pollutants, food/drink
habits etc.
Chronic
inflammation
Tobacco, Para-amino hippuric
acid, Ethylene oxide,
Formaldehyde, Crohn‟s disease,
oral Lichen
Planus etc.
Free radical injuries, Metabolic
dysfunction, Mitotic
spindle dysfunction
Genotoxicity Anti-neoplastic drugs, Pesticide Direct DNA damage, cell cycle
inhibition, mitotic
spindle toxins
Chemotherapy Cancer patients As above
Radiation injuries Increased MN frequency after
radiotherapy,
radiation-induced cancers
Direct DNA damage/ breakage,
accumulated in
consecutive populations
Pre-neoplastic
conditions
Oral submucosal fibrosis,
cervical intra-epithelial
lesions etc.
Chromosomal aberrations,
chromosome loss/breakage,
mitotic apparatus dysfunctions,
aneuploidy,
genetic instability
Neoplastic
conditions
Cervical carcinoma, oral
carcinomas, breast
Primary or secondary DNA
damage, Aneuploidy,

Review of Literature
15
carcinoma urothelial cancer,
Colon cancer
mitotic dysfunction genetic
instability
Genetic diseases Down syndrome, Xeroderma
pigmentosa
Various chromosomal aberrations,
DNA damage/breakage, genetic
instability
Infective Genital Chlamydiasis,
schistosoma haematobium
infection, Human papilloma
virus infection
Mechanisms exactly not known;
possibly interfere
With cellular division and
produce free radicals leading to
DNA damage. HPV is a DNA
virus and interferes with genes
involved in cell cycle.
Metabolic Megaloblastic anemia, vitamin
deficiencies
Interference with DNA synthesis
Details of the Methodology of MN Scoring on Smear
Either MGG or Papanicolaou‟s stained smear can be used for MN scoring. All the
cells with intact cell membrane should be included. Degenerated cells, cells with
obscured or altered morphology and large cell clusters or clumped groups should better
be avoided. Bi or multinucleated cells may show MN and should be counted and given a
score of one. Cells with multiple MN should be carefully looked for a possibility of
keratohyaline granules and if MN is confirmed morphologically, it should be given a
score of one. Overall score is usually expressed as number of micronucleated cells per
1,000 or 100 cells. With strict criteria, MN can be identified with confidence in
Papanicolaou‟s stained smear.26

Review of Literature
16
Morphology of Micronucleus
1 Location
Intra cytoplasmic near the main nucleus; generally within inner half of
cytoplasm. If the main nucleus is oval or spindly, MN is generally close
to one end of it. MN is always separated from the main nucleus.
2 Size 1/16th to 1/3rd the diameter of the main nucleus
3 Staining Generally same intensity or of more intensity with the main nucleus.
Occasionally paler.
4 Texture Same as the main nucleus. May be more clumped. Perimeter is smooth
suggesting a membrane. Non-refractile.
5 Shape Mostly oval or round; may be pyramidal, hemispheric, elliptical,
cylindrical or very rarely irregular.
6 Number Generally occurs singly in a cell. Very occasionally double. Triple or
more not seen or rare.
7 Others Plane of focus coincides or nearly same as the main nucleus.
8 Cells of
occurrence
Seen in the benign-appearing cells as well as frankly malignant or
dysplastic cell
9 Mimickers Stain deposits, bacteria, nuclear dusts, clumped cytoplasmic fragments,
partial Karyorrhexis or necrotic nucleus, carried over nuclear fragment
from other cells.

Review of Literature
17
MN SCORING CRITERIA
In 1976, Heddle introduced the scoring of micronucleus in lymphocytes after
exposure to genotoxic agents.29
Criteria for identifying micronuclei as given by Heddle
& Countryman (1976) are:
1. Diameter less than 1/3rd the main nucleus.
2. Non-refractility (to exclude small stain particles).
3. Color same as or lighter than the nucleus (to exclude large stain particles).
4. Location within 3 or 4 nuclear diameters of a nucleus; and not touching the
nucleus (to make frequency measurements meaningful).
5. No more than 2 micronuclei associated with one nucleus.
Belien et al [1995] also tried to make a standardization protocol for the counting of
micronuclei in exfoliated buccal cells.30
Paige E. Tolbert et al [1992] developed Criteria for the inclusion in the total cell
count which are the following: (1) cytoplasm intact and lying relatively flat; (2) little or
no overlap with adjacent cells; (3) little or no debris; and (4) nucleus normal and intact,
nuclear perimeter smooth and distinct.31
In order for a cell to be considered micronucleated, the cell must satisfy the above
criteria regarding inclusion in the total cell count and the putative micronucleus is
required to meet the following criteria: Fenech et al (2003)

Review of Literature
18
1. The diameter of the MN should be less than 1/3rd
of the main nucleus
2. MN should be separate or marginally overlap from the main nucleus as long as
there is a clear identification of the nuclear boundary.
3. Micronucleus have similar staining as the main nucleus
Nuclear Abnormalities in Buccal Cells
Besides the presence of MN, Tolbert et al in 1991 described other nuclear
abnormalities that can occur not only during physiological cellular differentiation but also
during cell death with DNA damage.25
In the cells these changes are produced in the
nuclei, it can be easily differentiated from the normal cells. These nuclear abnormalities
[NA] are Karyorrhexis (KR), Pyknotic nuclei (PN), karyolysis (KL), condensed
chromatin (CC) and nuclear buds. Among the various abnormalities the present study
focused on Karyorrhexis, karyolysis and pyknosis. The mechanisms by which each of
these abnormalities produced or its biological meaning is still unknown. Raj et al in 2001
described MN and NA presence has an effect on dose response after radiotherapy in
patients with oral Squamous cell carcinoma and suggested the use of these biomarkers to
assess the radio sensitivity.32
These NA are considered to be a biomarker for DNA
damage (MN), cell death evidence (CC, KR, PN, KL), different stages of necrosis
indicators (PN, KR, KL) and identifying response to cell damage (PN).3

Review of Literature
19
Karyorrhectic cell
The word is derived from Greek word ‘karyon’ meaning seed or nucleus and
‘rhexis’ meaning bursting. This is a destructive fragmentation of the nucleus of a dying
cell, where its chromatin is distributed irregularly throughout the cytoplasm. The cells
are characterized by more extensive appearance of nuclear chromatin aggregation. It is
usually preceded by pyknosis and can occur as a result of either apoptosis, senescence or
necrosis.
Pyknotic cell
The word pyknosis is derived from the Greek words ‘pyknono’ meaning to
condense or to thicken up. It is the irreversible condensation of chromatin in the nucleus
of a cell undergoing necrosis or apoptosis. The cells are characterized by a small
shrunken nucleus with a high density of nuclear material that is uniformly but intensely
stained. The nuclear diameter is usually 1/3rd
– 2/3rd
of that of a normal nucleus
Karyolitic cell
The word Karyolysis is derived from the Greek Word „karyon’ meaning seed or
nucleus and ‘lyein’ meaning to separate. There is a complete dissolution of the chromatin
of dying cells due to enzymatic degradation by endonucleases. It is usually preceded by
Karyorrhexis as a result of necrosis. The nucleus is completely depleted of DNA and
appears as a ghost like image that has no staining.

Review of Literature
20
The International Collaborative Project on Micronucleus Frequency in Human
Populations was organized to collect data on micronucleus [MN] frequencies in different
human populations and different cell types in 1999 & 2003. The information will be used
to:
1. Determine the extent of variation of „normal‟ values for different laboratories and
the influence of other factors potentially affecting baseline MN frequency. Eg:
age, gender and life-style.
2. Provide information on the effect of experimental protocol variations on MN
frequency measurements.
3. Design and test optimal protocols for the different cell types.
4. Determine the extent to which MN frequency is a valid biomarker of ageing and
risk for diseases such as cancer.
B.J. Majer et al [2001] reviewed the use of the micronucleus assay with
exfoliated epithelial cells as a biomarker for monitoring individuals at elevated risk of
genetic damage and in chemoprevention trials and concluded that the MEC assay is a
useful biomarker for the detection of human cancer risk in organs.15
Baseline frequencies for micronucleated cells in the BM are usually within the
0.5-2.5 Micronuclei/ 1,000 cells range. Cells with multiple micronuclei are rare in healthy
subjects but become more common in individuals exposed to radiation or other genotoxic
agents.

Review of Literature
21
PAP STAIN
It is a multi-chromatic staining cytological technique developed by George
Papanicolaou in 1942 and subsequently modified by him in 1952 and 1960.
Classically it consists of 5 dyes and 3 solutions. A haematoxylin used for staining
nucleus. Orange – G counter stain to stain keratin. Second counter stain consists of 2
dyes, Eosin Y to stain superficial epithelial squamous cells. Light Green SF which stains
cytoplasm of other cells including non-keratinized squamous cells. Advantages of this
staining technique are chromatin patterns are well visible in it. It also has increased
cytoplasmic transparency. Even though the conventional staining method takes 40
minutes rapid PAP staining kits are available which finishes total staining in 3 minutes.
MICRONUCLEUS IN TOBACCO USERS
A study was conducted in 1987 in 50 clinically normal individuals and divided
into those having smoking habit and non- smokers. The frequencies of micronuclei
resulting from chromosome were about double in smokers as compared with non-
smokers and the frequencies of micronucleus from spindle disturbances were
insignificant in them.24
In 1997 a study was carried out in 54 clinically healthy individuals to analyze the
genotoxic effects of smokeless tobacco, smoking and non-smokers/non-users. It was
found that the number of micronucleus was significant in smokeless tobacco users and
smokers with similar results.33

Review of Literature
22
A study was conducted in 2001 among patients using khat (Catha Edulis- a
psycho stimulant plant leaf) consumers, tobacco users and alcohol habits and found an
increase in the number of micronucleus. They also added that the number was higher in
khat users and use of tobacco and alcohol had an added effect in the course of genetic
damage.34
A study carried out in 2011, among patients with pan chewing habits and gutkha
habit to find out the genotoxic effects on these agents using an MN assay found a
significant increase in the micronucleus and chromosomal aberration in those patients
and suggested the increased chances of cancer development in these patients.35
A cohort study was done in 2012, to assess the correlation of frequency of
micronucleus in smokers with the duration of habit. They found that the frequency of
micronucleus was higher in smokers than non- smokers and a direct correlation of
number of micronucleus with the duration of habit noted as their number increase with
duration of habit.36
A study done in 2013 to find out the alterations in buccal cells due to alcohol,
tobacco and combination of two. They found a significant increase in the number of
micronucleus in the patients with tobacco and alcohol habit than in control group. There
is no significant difference when compared with alcohol alone group with control group
and the results showed that these habits can produce cellular alterations which may
cumulatively lead to carcinomatous changes.37
A study conducted in 10 tobacco users in
the same year, to evaluate the presence of micronuclei and other nuclear abnormalities
and concluded that age, duration of exposure and other factors like smoking and intake of

Review of Literature
23
alcohol affects the frequencies of nuclear abnormalities. They found no increase in the
number of micronucleus in this patients.38
A study was carried out in 2013 to find out the Genotoxicity associated with betel
quid chewers. They grouped 50 individuals as those with betel quid habit alone, betel
quid with tobacco and healthy individuals. They concluded that the number of
micronucleus was higher in individuals with both betel quid and tobacco habit followed
by tobacco habit alone. In contrast to other studies, in their study, there was a higher
frequency of micronucleus among males compared with females.39
MICRONUCLEUS IN CANCER PATIENTS
A cohort study was conducted in 2003 in occupationally exposed workers using
MN in peripheral blood lymphocytes as a cancer biomarker and found that smoking habit
has no influence on the frequency of MN frequency.40
A comparative study was carried out in 2004 in normal, pre malignant and
malignant epithelium using exfoliated buccal cells and found an increase in their number
from normal to premalignant then to malignant epithelium.41
In 2005 a study was carried among oral Squamous cell carcinoma patients. They
found that the number of micronucleus was high at the time of diagnosis and there was an
increase in their number immediately after exposure to radiation therapy and suggested
the use of micronucleus assay as a marker to identify the tumor sensitivity.42

Review of Literature
24
A study was conducted in 2007 among cancer patients, patients in pre-cancer
stage and normal patients using MN assay. A step wise increase in the number of MN
from normal to premalignant and from premalignant to malignant patients was noted.
They concluded that the MN assay can be used as a prognostic indicator in this
lesions.43
In the same year; a study was conducted among patients with erosive and
atrophic lichen planus for the assessment of micronucleus in exfoliated cells and found a
significant increase in the MN frequency in these lesions than in normal individuals.44
In 2010, a study was conducted among 20 patients who had white lesions in the
oral cavity. All the lesions were stained with Toluidine Blue and samples were taken for
cytological evaluation. It is concluded that the frequency of MN were higher in those
patients, irrespective of TB staining.45
In 2010, a prospective study was conducted among breast cancer patients with
benign cases as control group. The patients were diagnosed by FNAC. They used
Acridine Orange, a fluorescent dye for the identification of micronucleus and found an
increase in their frequency.46
A study conducted in 2011 among patients who have potentially malignant
disorders and malignant lesions the presence of micronucleus and found that the number
of micronucleus was higher in malignant group than in patients who are diagnosed with
potentially malignant disorders. However, the number was higher than the clinically
healthy individuals who are the control group.47

Review of Literature
25
In 2014 a study was conducted among normal patients, leukoplakia, and
Squamous cell carcinoma using PAP staining and found that MN were higher in SCC
than in leukoplakia and healthy control. Hence, MN assay can be used as an important
biomarker for cytogenetic damage in oral leukoplakia and SCC.48
A study done among patients who are having tobacco related potentially
malignant disorders using MN assay. The sample was collected from the exfoliated
buccal epithelial cells of 8 leukoplakia, 7 OSMF patients and 15 healthy controls and
found a significant increase in their number in patients diagnosed with PMDs compared
to control group.49
MICRONUCLEUS IN OTHER CLINICAL SETTINGS
In 2001 a study was carried among 49 male workers who are exposed to
pesticides to assess the genotoxic effects of these chemicals with the help of MN assay in
peripheral blood lymphocytes and buccal epithelial cells. The results showed no increase
in the number of micronucleus in the samples collected from both sites. No correlation
was drawn with smoking and other habits.50
In the year 2010 a study was conducted among 23 chronic denture stomatitis
patients and analyzed the cytological changes comparing with the control group. The
results showed an increase in the cytological changes among these patients.51

Review of Literature
26
A study was done in 2011 among patients wearing dental prosthesis having white
lesions in the buccal mucosa. These lesions were stained with Toluidine Blue and were
categorized into positive and negative. The frequency of micronucleus increased in white
lesions but the increase in number was irrespective of vital staining.45
A study was carried among children in the same year, to evaluate the genotoxic
effects of various dental materials through MN assay. Buccal epithelial cells were
collected from children of various ages ranging from 4yrs to 12 years, who were
undergoing same type of dental treatment. Cells were collected before and at the end of
treatment. There was a significant increase in the number of bi-nucleated cells after the
treatment with cement based dental materials and monomer. They concluded that the
combination of cement-based dental material with monomers increases the cytotoxic
action of dental materials.52
In the same year, a study was done among full time tannery workers for the
assessment of Genotoxicity using MN assay. The samples were collected from buccal
epithelial cells. There was a significant increase in the MN frequency in them. There is a
direct relationship between the duration of exposure, smoking and alcoholism with that of
MN frequency.53
A study was conducted in 2012, among 10 chronic Periodontitis and 10
aggressive Periodontitis patients to find out DNA damage. They evaluated the presence
of micronucleus in peripheral lymphocytes but there was no correlation between two
groups.54

Review of Literature
27
MICRONUCLEUS IN IONIZING RADIATION
In the year 2000 a study carried among hospital workers who are occupationally
exposed to ionizing radiation using micronucleus centromere assay in peripheral
lymphocytes and found a higher number in them. In the studied population, smoking did
not yield any significant correlation.55
In the same year, a study was conducted among
workers in radiation department, to estimate the extent of exposure to workers using
peripheral lymphocytes. Even though the number of micronucleus was higher than the
control group, the annual dose of exposure was below the whole body exposure per
year.56
A similar study was conducted in 2002 aimed at preventing the risk of cancer
from exposure to ionizing radiation among hospital workers occupationally exposed to
these kinds of radiations. But even though the number of MN was higher than the control
group, it was not statistically significant. They also found that there is an increase in the
MN frequency in workers who are exposed to the smoking.57
In order to assess occupationally induced chromosomal damage, a study was
conducted among 29 industrial radiographers in 2002 and found an increase in the
number of micronucleated cells in them than control group. The increase in the number
of micronucleus correlates with age and it did not have any correlation with the duration
of exposure.58
A study was carried out in 2004, to find out the genotoxic effects of ionizing
radiation in patients exposed to dental panoramic radiographs. The results suggest that
the ionizing radiation induces a cytotoxic effect by increasing apoptosis and other nuclear

Review of Literature
28
alterations and the number of micronucleus was insignificant. In addition, they concluded
that the micronucleus improves the sensitivity in the detection of genotoxic effects.59
A study conducted in 2005, to assess the frequency of micronuclei (MN), which is
an indicator of DNA damage, in a population exposed to low levels of ionizing radiation
and found a significantly higher MN frequency than control group. In contradiction to
other studies they found that the smoking status did not affect micronuclei frequency
either in exposed workers or controls, while age was associated with increased MN
frequency in the exposed only.60
A study was conducted in 32 non- smokers who had been subjected to panoramic
radiographs to assess the possible genotoxic effect of radiation exposure for dental
diagnostic purpose and no significant increase in the frequency of cells with micronuclei
and total number of micronuclei after panoramic tomography was detected. But a
significant correlation between the age of investigated subjects and the initial frequency
of micronuclei in buccal cells was observed.61
In the same year, nuclear changes in tongue epithelial cells following panoramic
radiography was studied and the radiation emitted during panoramic radiographs
increased the number of nuclear anomalies (except micronuclei) in exfoliated cells of the
lateral border of the tongue. This effect was more pronounced when the patients were
exposed to a repeat radiograph, without however implying the increased risk of
irreversible tissue damage.62

Review of Literature
29
In the same year, a study was carried out among children following exposure to
radiation during dental radiography to evaluate DNA damage and cellular death.
Exfoliated cells are taken from buccal mucosa for cytological analysis. The results
indicates that the panoramic radiography might not induce chromosomal damage, but
may be cytotoxic.63
In 2008, s study was carried out to find out variation in the DNA damage
[micronucleus] and cellular changes like pyknosis, Karyorrhexis, karyolysis in adult and
children who are undergoing diagnostic radiographs. The results showed no significant
variation in the number of micronucleus and other nuclear alterations among adult and
children. The frequency of nuclear alterations except micronucleus was increased in both
groups after exposure.64
A study was done to assess the genotoxic effects of individuals who are subjected
to CBCT in 2010. They also assessed the other nuclear alterations like Karyorrhexis,
karyolysis and pyknosis. The results showed no significant increase in the MN frequency.
But the number of other nuclear alterations got increased to a significant level. They
concluded that cone beam CT may not be a factor that induces chromosomal damage, but
it is able to promote cytotoxicity.65
In the same year, a study was carried out in 18 healthy individuals who had taken
lateral and frontal radiographs for orthodontic purpose and evaluated DNA damage
(micronucleus) and cellular death (pyknosis, karyolysis and Karyorrhexis) in exfoliated
buccal mucosa cells and after the analysis of results, they concluded that the radiography

Review of Literature
30
may not be a factor in inducing chromosomal damage, but it does promote cytotoxicity as
there is an increase in the nuclear alterations except micronucleus.66
In the same year, DNA damage and cellular death in oral mucosa was evaluated
by comparing the samples taken from buccal mucosa and lateral border of tongue. The
samples were taken from both smokers and non- smokers. They found that X-ray
exposure were able to increase nuclear alterations closely related to cytotoxicity. The
most pronounced effects were seen in lateral border of tongue of smokers. They
concluded that the panoramic radiography is able to induce cellular death in both buccal
mucosa and tongue. The lateral border of tongue is more sensitive to cytotoxic insult
induced by ionizing radiation combined with continuous cigarette smoke exposure.67
The genotoxic effect of panoramic radiographs in children was evaluated in the
same year from the cytological analysis of buccal epithelial cells of 20 healthy children
who underwent panoramic dental radiography for diagnostic purpose. The cells were
attained with Feulgen reaction. There was no significant Genotoxicity seen. But there was
a significant increase in the Karyorrhexis and pyknosis, while karyolysis did not show
significant difference.68
In the year 2011, DNA damage and cellular death in exfoliated buccal mucosal
from individuals following digital lateral radiography was evaluated. The results pointed
out no statistically significant difference of MN in oral mucosal cells. But it was able to
increase other nuclear alterations like Karyorrhexis, karyolysis, pyknosis which are
closely related to cytotoxicity.69

Review of Literature
31
In the year 2012, a study was done to evaluate genotoxic and cytotoxic effects of
low level ionizing radiation used in digital panoramic radiography on gingival epithelial
cells. The frequency of formation of micronuclei was not significant with regard to age,
gender and after exposure to digital panoramic radiography. However this study showed
significant increase in the frequencies of nuclear alterations like Karyorrhexis, pyknosis,
condensed chromatin, karyolysis and indicative of cell death.70
In the same year a similar study was carried out but on buccal epithelial cells.
They assessed the MN frequency and other nuclear projections (buds and broken eggs)
and degenerative nuclear alterations (condensed chromatin, Karyorrhexis, karyolysis).
The results showed significant increase in MN frequency and other nuclear alterations.
They also showed that these alterations are higher in females than that of males.71
A study done in the same year in 60 clinically healthy individuals who underwent
panoramic radiography to evaluate the genotoxic effects using MN assay. The results
showed an increased frequency of micronucleus after exposure to ionizing radiation.
They concluded that considering the risk, panoramic radiographs should be advised
carefully.72
In the same year a study was conducted among clinically healthy children
undergoing orthodontic treatment. They were advised to take a complete set of
orthodontic radiographs, which includes lateral cephalographs, posteroantero-
cephalographs, panoramic radiographs, IOPA full set and bitewing. The cells were
analyzed for the genotoxic and cytotoxic damage. No significant increase in the MN

Review of Literature
32
frequency was seen. But there was rise in other nuclear alterations like Karyorrhexis,
karyolysis, pyknosis.73
A study was done in the same year to compare the effects of different types of
radiographic techniques using buccal cytochrome assay. The study comprised of 90
patients who are grouped into 3. First being patients taking IOPA radiographs, second
was those taking digital OPG and third were patients who are taking conventional OPG.
But the results came similar to the other studies which showed an increase in the
cytotoxicity without increase in MN frequency.74
In the same year a study was done to compare the effects of X- rays on gingival
and buccal epithelial cells using MN assay. 80 clinically healthy individuals were
selected for the study. Cells were collected from the maxillary anterior gingiva and
buccal mucosa. The slides were stained using PAP stain. Significant increase in the
number of micronucleus was noted in the anterior gingiva while buccal mucosa showed
no increase in the MN count. They concluded that the radiographs should be taken with
adequate protection measures and only when potential benefits outweigh the risk factor.2
In 2013, a comparative study was done using CBCT and conventional radiograph
for the assessment of genotoxic and Cytotoxic effects. The buccal mucosal cells were
collected from the patient before and 10 days after exposure. After the cytological
analysis, there is no increase in the number of MN which was indicator of the
Genotoxicity seen in either group, while there is a significant increase in the cytological
change. CBCT group presented a greater increase in the cell death than conventional

Review of Literature
33
radiographic group. They concluded that this variation may be due to increase exposure
of CBCT used for taking radiographs for orthodontic planning.75
A study conducted in 2014 to evaluate the possible genotoxic effects of
panoramic radiation by assessing the frequency of micronuclei formation in the
exfoliated buccal epithelium. They found that the X-radiation emitted during panoramic
radiography does induce some genotoxic changes in the form of increased frequency of
micronuclei in target buccal epithelial cells.76
A similar study to evaluate the possible genotoxic effects of routinely used
panoramic exposure in exfoliated buccal cells and keratinized gingiva which is measured
by micronucleus formation and concluded that the genotoxic effects of radiation exposure
from panoramic radiography showed a statistically significant increase in the MN
frequency in the buccal epithelial cells. But the correlation of age and the MN frequency
was noted in keratinized gingival cells. No such correlation was noted in buccal epithelial
cells.77

MATERIALS & METHODS

Materials & Methods
34
The study was planned & conducted in the department of Oral Medicine &
Radiology, Sree Mookambika Institute of Dental Sciences to find out the genotoxic and
cytotoxic changes among patients exposed to digital radiographs.
SAMPLE SIZE & ITS CHARACTERISTICS
The patients for the study were selected among the outpatients who visited the
department of Oral Medicine and Radiology. The study group comprised of clinically
healthy subjects who needed orthodontic treatment. Sample consists of 127 patients.
Sample size was calculated using software GPower version 3.1.7.
a. Inclusion criteria:
Patients undergoing digital radiographic examination for
orthodontic purposes
b. Exclusion criteria:
Patients undergoing radiographic examination for reasons other
than orthodontic treatment
Patients of age > 40 yrs
Patients who have a history of radiation exposure within the last
one year

Materials & Methods
35
Patients with any pre - malignant lesions/ conditions on the buccal
mucosa
Patients with malignant lesions
Patients with ulceration on the buccal mucosa
Patients with habits of smoking, alcoholism or tobacco chewing
Patients wearing prosthesis
Patients with any other clinical abnormalities on the buccal mucosa
After screening, information on the nature and potential benefits of the study was
explained to the patient. They were made to understand that the participation in
this study was purely voluntary and they had the option of exiting the study at any
point of time. And among the consenting volunteers who fit the inclusion and
exclusion criteria were selected. A formal informed written consent was taken
from all of them. A study protocol was approved by the Research Committee and
the Institutional Human Ethics Committee of Sree Mookambika Institute of
Medical Sciences. Kulasekharam. A detailed case history of the patient was taken
and a thorough clinical examination was done and recorded. Serial number was
also assigned to each patient.

Materials & Methods
36
Armamentarium
a) For sample selection and case history
A pair of sterile disposable gloves and disposable mouth masks
Stainless steel kidney tray, mouth mirror, straight probe and
tweezer
Glass tumbler with water
b) For taking digital radiographs
Planmeca digital orthopantomograph machine Prolin XC
c) For sample collection
Microscopic slide
Sterile wooden spatula
Bio spray in the RAPID – PAPTM
kit for fixing the sample
d) For staining the sample slide
RAPID – PAPTM
staining kit
Coplin jars
Filter/tissue paper
Cover slip
e) For cytological examination
Light microscope
AP View software

Materials & Methods
37
Brief procedure:
Sample collection
Patients were asked to rinse their mouth with water before making digital
radiographs. This helps to remove any food or artifacts that may interfere with the
analysis. Buccal epithelial cells were obtained using brush biopsy technique using a
wooden spatula. Oral mucosa is the first line of contact with hazardous agents and the
first barrier against potential carcinogens and is therefore susceptible to damage by these
agents before reflecting its effects systemically. It also provides an easy access to
samples collection. This technique is minimally invasive and painless and for these
reasons it is well tolerated among patients. After drying, the slides were fixed using
Biofix spray which comes along with the RAPID – PAP kit.
Digital orthopantomographs and lateral cepholograms were taken for the above
subjects with exposure of 68kV; 11mA; 18sec for orthopantomograph and 68kv 5mA;
17sec for lateral cepholograms.
The turnover rate for the appearance of MN in exfoliated buccal cells in otherwise
normal cell after exposure to an acute genotoxic event like ionizing radiation is estimated
to be between 8-12 days. The patient was recalled after 10±2 days and the sample was
collected again from the buccal mucosa using the same procedure because peak
expression of MN may vary depending on the effects of particular DNA damage on basal
cell turnover rate.

Materials & Methods
38
Nearly 60% of oral mucosal surface is stratified non-keratinized epithelia, which
allows cells in the most superficial layer to maintain their nuclei well defined and almost
intact which favours colorant absorption, ease of observation, proper identification of
nucleus and morphological characteristic of cell with the help of microscope.
Staining of slides
The colorant used should be basic and must have a high affinity to DNA in order
to obtain a contrast so that artifacts can be easily differentiated. In this study DNA
specific Papanicolaou stain was used. It is an acidic – basic stain which can produce a
contrast between the cytoplasm and nucleus and there by helps in reducing the bias
produced when non specific DNA stains are used.
The sample slides were stained using RAPID PAPTM
Papanicolaou’s stain kit.
It is a user friendly PAP staining kit by BIOLAB DIAGNOSTICS. Unlike the
conventional PAP staining, this kit allows the staining of slides in 3 minutes. It requires
minimum skills and laboratory aids for good results.
The RAPID – PAPTM
staining kit consists of
Biofix spray : for cell fixation
RAPID - PAPTM
NUCLEAR STAIN Haematoxylin solution
RAPID – PAPTM
CYTOPLASM STAIN OG-6 Solution [2A]

Materials & Methods
39
RAPID – PAPTM
CYTOPLASM STAIN Light Green SF-
Eosin[2B]
D.P.X GLASS MOUNTING MEDIUM
RAPID – PAPTM
DEHYDRANT Propanol
XYLENE
RAPID – PAPTM
WASH BUFFER Scotte’s tap water buffer
Haematoxylin nuclear stain is a natural stain which has an affinity for chromatin,
attaching to sulfate group in DNA molecule. It acts as acidic stain for basic
neutroproteins. Its pH is 2.5-3
Scotte’s tap water buffer: the pH of this solution varies from 8-8.5. This subjects
haematoxylin to alkaline conditions and changes its color from red to blue.
Alcohol acts a dehydrant which helps to minimize cellular distortion, reduce cell
lose from glass slide.
OG-6: it is an acidic dye that demonstrates attraction to the basic proteins like
parakeratin. It is a monochromatic stain which colors keratin brilliant green. The effect of
OG - 6 is evident if the smear has keratinized cells.
Light Green SF- Eosin:
Eosin gives pink color to cytoplasm of mature squamous cells and nucleoli.

Materials & Methods
40
Light green stains cytoplasm of metabolically active cells like parabasal cells,
intermediate squamous cells in blue. It has a C2H5N+ reactive group which possesses an
affinity for RNA of ribosomes.
Xylol: It acts as a clearing agent. It is a colorless, chemically non- reactive and has almost
the same refractive index as that of glass. Thus it helps to give transparency to image.
D.P.X Mountant: it acts as a permanent bond between the slide and cover slip, protects
the cell material from air drying and shrinkage. It also acts as a seal against oxidation and
fading of stain.
Reagent Preparation: cytoplasm stain is prepared by mixing equal volume of cytoplasm
stain 2A and 2B. It is then stored in an air tight bottle to prevent contamination from
water and other pollutants.
Steps in slide staining using RAPID PAPTM
kit
1. Dip the fixed smear for 3 minutes in tap water and blot the excess water
from the slide.
2. Dip 60 seconds in PAPID PAPTM
Nuclear Stain.
3. Add 3 drops of Scott Tap Water buffer and wash after 10 seconds. Blot
out the excess water from the slides.
4. Dip with the two changes in RAPID PAPTM
dehydrant for 30 seconds
each.

Materials & Methods
41
5. Dip in 45 seconds in working cytoplasm stain.
6. Wash in tap water and blot out excess water from the slide
7. Repeat dehydration in a second bath of RAPID PAPTM
dehydrant for 30
seconds and dry.
8. Dip in xylene, dry and mount with cover glass using a drop of D.P.X.
Cytological examination
The stained slides are examined using light microscope first in 10X magnification
and then 40X magnification. AP viewer software is used for the visualization of cells and
for taking photomicrographs. The cells are selected for scoring as per Tolbert’s criteria
(1992) (1) cytoplasm intact and lying relatively flat; (2) little or no overlap with adjacent
cells; (3) little or no debris; and (4) nucleus normal and intact, nuclear perimeter smooth
and distinct.
The micronucleus is identified with the help of the suggested criteria by Fenech et
al 2003
1. The diameter of the MN should be less than 1/3 rd
of the main nucleus
2. MN should be separate or marginally overlap from the main nucleus as
long as there is a clear identification of nuclear boundary.
3. MN have similar staining as the main nucleus

Materials & Methods
42
Apart from micronucleus, other cellular alterations are considered for the
cytological analysis. Among the various cellular alterations, the present study analyzed
the presence of Karyorrhexis, karyolysis, pyknosis.
Karyorrhectic cell: cells are characterized by more extensive appearance of nuclear
chromatin aggregation leading to fragmentation and eventual disintegration of nucleus
Pyknotic cell: cells are characterized by a small shrunken nucleus with a high density of
nuclear material that is uniformly but intensely stained. The nuclear diameter is usually
1/3rd
– 2/3rd
of normal nucleus
Karyolitic cell: nucleus id completely depleted of DNA and apparent as a ghost like
image that has no staining.
In the present study, with strict criteria, 100 cells in each slide were analyzed for
the presence of micronucleus and other nuclear alterations. The results were sent for
statistical analysis.

COLOUR PLATES

Colour plates
CP - 2: PLANMECA PROLIN XC MACHINE
CP – 1: ARMAMENTARIUM FOR SAMPLE COLLECTION

Colour plates
CP – 3: RAPID PAPTM
STAINING KIT
CP – 4: STAINED SLIDES IN SLIDE BOX

Colour plates
CP – 5: LIGHT MICROSCOPE & AP VIEWER

RESULTS & OBSERVATIONS

Results & Observations
43
The purpose of the study was to evaluate the genotoxic and Cytotoxic changes
after exposure to low level ionizing radiation. The study comprises of evaluating the
Genotoxicity by micronucleus assay and cytotoxicity by the presence of Karyorrhexis,
karyolysis, pyknosis before exposure and 10 days after exposure.
Statistical analysis: The data was expressed in means and standard deviation.
SPSS version 17.0 was used for statistical analysis. Paired t test was applied to find
statistical significant within the groups. P≤ 0.05 considered statistically significant.
Two samples were taken from 128 patients, one before exposure and one 10±2
days after exposure. In the total sample, 22 patients were males and 105 patients were
females. Total number of cells among all the samples having micronucleus was found
to be 245 before exposure and 1240 after exposure. Total number of micronucleus in
245 cells was 272 and in 1240 was 1575. A comparison of micronucleus was made
before and after exposure using paired t test. The mean value before exposure was
1.92±1.93 and after 9.76±6.70. The total number of cells showing Karyorrhexis was
392 before exposure and 462 after exposure. The mean value was 3.08±3.26 before
and 3.63±3.23 after exposure. The total number of cells showing karyolysis was 661
before and 881 after exposure. The mean value was 5.27±4.53 before and 6.38±5.44
after exposure. The total number of cells showing pyknosis was 815 before and 1011
after exposure. It has a mean value of 6.41± 4.36 before and 7.96±6.31 after exposure.
Gender wise comparison was made for each parameter. Among males the total
number of micronucleated cells was 33 before and 212 after exposure. The number of
Karyorrhectic cells was 51 before and 93 after exposures. The number cells showing
karyolysis was 116 before and 115 after exposure to X-rays. The number of Pyknotic
cells was 163 and 156 before and after exposure. Among females, the total number of

Results & Observations
44
micronucleus was 212 before exposure and 1028 after exposure with a mean of 2.01
and 9.76 respectively. The number of cells showing Karyorrhexis was 341 and 369
before and after exposure with a mean of 3.24 and 3.51 respectively. Number of
karyolitic cells in females before and after exposure was noted as 545 and 696 and the
mean values were 5.19 and 6.62. The number of Pyknotic cells was counted and it
was 652 and 855 before and after exposure with a mean of 6.2 before exposure and
8.14 after exposure.
Overall it was seen that both cytotoxic and genotoxic effects were increased
following radiation exposure.
TABLE 1: Distribution of study subjects according to age and gender
Gender Total number Mean Age t test p value and
significance
Males 22 21.95±2.33
1.147
0.253
NS Females 105 21.46±1.68
Total 127 21.55±1.81
P<0.05, NS – Non Significant
Micronucleus analysis
Samples collected from 127 patients, before and 10±2 days after exposure
were analyzed for the presence of micronucleus. 100 cells were examined in each
slide. The number of micronucleated cells were counted. Micronuclear cell frequency
was also noted along with it.

Results & Observations
45
Light microscope study
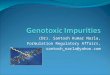
IMAGE 1: SHOWING NORMAL CELL AT 40 × MAGNIFICATION
IMAGE2: SHOWING MICRONUCLEATED CELL AT 40 × MAGNIFICATION

Results & Observations
46
IMAGE 3: SHOWING MICRONULEATED CELL WITH TWO
MICRONULCEUS AT 40 × MAGNIFICATION
IMAGE 4: SHOWING MICRONLCEATED CELL WITH MULTIPLE
MICRONUCLEUS AT 40 × MAGNIFICATION

Results & Observations
47
Image 1 shows the photomicrograph of a normal cell in 40 × magnification. It
is used as a standard for the size of normal nucleus. Image 2, image 3, image 4 are the
photomicrograph taken using AP viewer in the same magnification, which showed the
presence of micronucleus [single or multiple].
TABLE: 2 Total No of cells having Micronucleus before and after radiation/100 cells
Total No of cells having MN before
radiation
Total No of cells having MN after
radiation
245 1240
TABLE: 3 Total No of Micronucleus before and after radiation/100 cells
Total No of MN before radiation Total No of MN after radiation
272 1575
TABLE: 4 Mean value & standard deviation of MN assay
Comparison Mean Std. Deviation Paired t value P value
MICRO
NUCLEUS
Before 1.9291 1.93621
12.132 0.000
HS After 9.7638 6.70046
Table 2 shows the number of micronucleated cells while table 3 shows the
number of micronucleus seen in examination of all the samples taken before and after
radiation exposure. Table 4 shows the mean values and standard deviation of the
micronucleus examined. There is a steady increase in the number of micronucleated

Results & Observations
48
cell after radiation with highly significant P value of 0.000. Micronuclear cell
frequency also showed an increase after radiation exposure.
Other nuclear alterations
Samples taken from the patients before and 10±2 days after radiation exposure
are analyzed for other nuclear anomalies. In the present study examination of
Karyorrhexis, karyolysis and pyknosis was done among 100 cells in each slide.
IMAGE 5: SHOWING KARYORRHEXIS OF THE NUCLEUS IN 40 ×
MAGNIFICATION
TABLE: 5 Total No of cells having Karyorrhexis before and after radiation/100 cells
Total No of cells having Karyorrhexis
before radiation
Total No of cells having Karyorrhexis
after radiation
392 462

Results & Observations
49
IMAGE 6: SHOWING KARYOLYSIS IN CELL AT 40× MAGNIFICATION
TABLE: 6 Total No of cells having Karyolysis before and after radiation/100 cells
Total No of cells having Karyolysis
before radiation
Total No of cells having Karyolysis
after radiation
661 881
TABLE: 7 Total No of cells having Pyknosis before and after radiation/100 cells
Total No of cells having Pyknosis
before radiation
Total No of cells having Pyknosis after
radiation
815 1011

Results & Observations
50
IMAGE7: SHOWING PYKNOTIC NUCLEUS AT 40 × MAGNIFICATION
Image 5, image 6, image7 are the photomicrographs taken with the help of AP viewer
in 40 × magnification for showing nuclear alterations like Karyorrhexis, karyolysis
and pyknosis.
TABLE 8: Mean value & standard deviation of cytological changes
Comparison Mean Std.
Deviation
Paired t
value
P value
KARYORRHEXIS Before 3.0866 3.26361
1.372 0.173
NS After 3.6378 3.23343
KARYOLYSIS Before 5.2047 4.53442
1.906 0.059
NS After 6.3858 5.44824
PYKNOSIS Before 6.4173 4.36334
2.304 0.023
S After 7.9606 6.31501

Results & Observations
51
Table 8 shows the mean and standard deviation of other nuclear alterations.
There is a statistically significant increase in the pyknosis after radiation with a P
value of 0.023. The other nuclear alterations like Karyorrhexis, karyolysis also shows
an increase after radiation even though it is not statistically significant.
Gender wise comparison was made for micronucleus, Karyorrhexis, karyolysis
and pyknosis.
TABLE: 9 Gender variations in micronucleus count
GENDER MN cell count before exposure MN cell count after exposure
MALES 33 212
FEMALES 212 1028
TABLE: 10 Gender wise comparison of micronucleus
GENDER MN before exposure MN after exposure
MALES 1.5 9.636
FEMALES 2.019 9.76

Results & Observations
52
TABLE: 11 Gender wise comparison of Karyorrhectic cell count
GENDER Karyorrhectic cell count
before exposure
Karyorrhectic cell count after
exposure
MALES 51 93
FEMALES 341 369
TABLE: 12 Gender wise comparison of Karyorrhexis
GENDER Karyorrhexis before exposure Karyorrhexis after exposure
MALES 2.318 4.227
FEMALES 3.247 3.514
TABLE: 13 Gender wise comparison of karyolitic cell count
GENDER Karyolitic cell count before
exposure
Karyolitic cell count after
exposure
MALES 116 115
FEMALES 545 696

Results & Observations
53
TABLE: 14 Gender wise comparison of karyolysis
GENDER Karyolysis before exposure Karyolysis after exposure
MALES 5.272 5.227
FEMALES 5.19 6.628
TABLE: 15 Gender wise comparison of Pyknotic cell count
GENDER Number of Pyknotic cell
before exposure
Number of Pyknotic cell after
exposure
MALES 163 156
FEMALES 652 855
TABLE: 16 Gender wise comparison of pyknosis
GENDER Pyknosis before exposure Pyknosis after exposure
MALES 7.409 7.09
FEMALES 6.209 8.142

GRAPHS

Graphs
Graph1: Distribution of study subjects according to gender and age
Graph 2: Mean changes in Genotoxic and Cytotoxic parameters before
and after radiation exposure among study subjects
0
20
40
60
80
100
120
Males Females
22
105
21.95 21.46
Co
un
t
Gender
Total number
Mean Age
0
1
2
3
4
5
6
7
8
9
10
Before After Before After Before After Before After
MICRO NUCLEUS KARYOHEXIS KARYOLYSIS PYKNOSIS
1.9291
9.7638
3.0866 3.6378
5.2047
6.3858 6.4173
7.9606
Co
un
t

Graphs
Graph 3: Gender wise comparison for micronucleus before and after
radiation exposure
Graph 4: Gender wise comparison for Karyorrhexis before and after
radiation exposure
0
1
2
3
4
5
6
7
8
9
10
Before radiation exposure After radiation exposure
1.5
9.636
2.019
9.79
Me
an C
ou
nt
Males
Females
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Before radiationexposure
After radiation exposure
2.318
4.227
3.247 3.514
Me
an C
ou
nt
Males
Females

Graphs
Graph-5: Gender wise comparison for Karyolysis before and after
radiation exposure
Graph – 6: Gender wise comparison for Pyknosis before and after
radiation exposure
0
1
2
3
4
5
6
7
Before radiationexposure
After radiation exposure
5.272 5.227 5.19
6.628 M
ean
Co
un
t
Males
Females
0
1
2
3
4
5
6
7
8
9
Before radiation exposure After radiation exposure
7.409 7.09
6.209
8.142
Me
an C
ou
nt
Males
Females

DISCUSSION

Discussion
54
Cancer is a complex disease caused by altered gene expression resulting in
abnormal uncontrolled growth of tissue. The mutations in various genes causes
acceleration in cell division and inhibition of apoptosis, which is programmed cell death.
The amount of mutations accumulated within cancer cells cannot be explained solely by
the normal point mutation rate. There are several factors which can induce these kinds of
mutations and ionizing radiation is one among them. Because cancer may take several
years to develop and it is not always practicable to do epidemiological studies over such
long periods, use of biomarkers for the analysis of DNA damage can be used as a
predictive indicator of cancer risk.78
In medical and dental practice, x rays are used for diagnosis and treatment. It is a
well known fact that the ionizing radiations can induce DNA damage including double or
single strands breakage or DNA protein cross link damage. The specific character of
ionizing radiation which differentiates it from other physical carcinogens is its ability to
penetrate cells and deposit energy within the cells in random fashion, unaffected by usual
cellular barriers when presented to chemical agents. In this way, all cells in the body are
susceptible to damage caused by ionizing radiation. The amount of damage is related to
the physical parameters that determine the radiation dose received by particular tissue or
cell. By 1980, radiation induced cancer (in vivo) and cellular transformation (in vitro)
were well established.6 Considering the association of ionizing radiation and
carcinogenesis, various analyses have been introduced to detect the effects of low level
ionizing radiation used in diagnostic radiology.

Discussion
55
The purpose of the present study was to evaluate the genotoxic and Cytotoxic
changes in patients after exposure to low level ionizing radiation.
Various biomarkers like assessment of metaphase chromosomal aberrations, sister
chromatid exchange can be used to determine the effects of ionizing radiation. But these
methods are very technique sensitive, expensive, time consuming and required expertise
to interpret the slides. Hence application of micronucleus test and other nuclear
anomalies in uncultured exfoliated cells has received great interest. These biomarkers
offer additional end points for possible evaluation of chromosomal instability, gene
amplification and different cell death events.
MN is formed during the transition metaphase-anaphase of the mitosis and they
are chromosomes left out as a result of mitotic apparatus damage [aneuploidogenic
effect] or chromosome fragments without centromere [clastogenic damage]. In both
cases, these genetic materials were unable to incorporate into daughter cells and can be
visible as a round or oval cytoplasmic chromatin masses next to the nucleus. They are
identified using the criteria put forward by Fenech et al in 2003.
Cytokinesis – Block MN assay in lymphocytes is the most popular technique of
MN assay. But lymphocytes must be stimulated to undergo mitosis and the changes are
visible at a later phase. But in case of diagnostic radiology in dental practice, the target
tissue of interest is buccal epithelial tissue. Epithelial cells need not be stimulated. These
cells show genotoxic effects within 1-3 weeks earlier than the lymphocytes. Epithelial
cells have high proliferative capacity and more than 90% of human cancers are epithelial
in origin. Therefore the application of MN test in epithelial cells is considered to a

Discussion
56
sensitive tool for assessing genotoxicity. Cells of buccal mucosa have limited DNA repair
capacity when compared to lymphocytes and therefore more accurately reflect genomic
instability. It is simple non- invasive and has good patient compliance.11
The samples for the study were taken before exposure and 10±2 days after
exposure. The harmful effects of ionizing radiation take place in the basal layer of
epithelium where cells undergo mitosis. Rapid turnover of the epithelial tissue brings
these cells to the surface when they exfoliate. Hence maximal rate of micronucleus
formation in exfoliated cells is seen 1-3 weeks after exposure to genotoxic agents.64
For
this reason a period of 10±2 days after exposure was adopted for the study.
Several staining methods have been used for the evaluation of micronucleus.
Although DNA specific stains are preferred for staining MN, the most commonly used
staining procedure is Feulgen staining reaction. However the staining procedure is
lengthy and also technique sensitive and may lead to under scoring of MN. In the present
study, PAP stain is used. It is done using RAPID- PAP TM
kit. It is rapid, easy to read and
the fixative used has a bactericidal effect and the nuclear stain stains both intranuclear
and extra nuclear DNA and cytoplasmic stain helps to maintain the transparency of the
cytoplasm and makes boundaries well demarcated.79
The added advantage is that it can
differentiate between cytoplasm of non- keratinized and keratinized cells where it appears
as blue/ green in former and pink/orange in latter. The nucleus appears blue/black.80
The present study consists of individuals with age ranging from 19-27years with a
mean of 21±1.8 and showed no statistical significance with respect to age. [P=0.253] This
was in accordance with a previous study conducted in Brazilian population with a mean

Discussion
57
age of 21 years.81
The influence of tobacco and alcohol is considered as a relevant factor.
In the study done by Stich & Rosin a synergistic effect in the formation of MN frequency
was noted in these patients.23
Thus in the present study all the patients recruited did not
have any habits. Based on the recent studies done by Shally Khanna et al on oral
squamous cell carcinoma patients and Uma et al on potentially malignant disorders,
where they found an increase in the number of micronucleus in these conditions, they are
excluded from the study.48, 49
A study done by Pollyanna Francielli et al among patients
wearing prosthesis who presented with white lesions on the buccal mucosa also showed
an increase in MN frequency.45
Hence these patients are also excluded from the study to
reduce bias. It has been postulated that as age advances, there is a progressive increase in
the spontaneous chromosome instability, decline in the DNA repair capacity and
increased chromosome loss. This leads to increase in the MN frequency as the age
advances.61
So patients of age more than 40 years were also not includes in the study.
A comparison of the MN values before and 10 days after radiation exposure was
calculated among 100 cells in each slide. There is a significant increase in the MN count
after exposure to ionizing radiation. Both the number and mean of micronucleated cells
was 245 before and after 1240 and 1.93±1.94 before and 9.76±6.70 after exposure with a
highly significant P value (P value: 0.000) This correlates with the studies done by
Sabrina Angeli.60
The Micronuclear cell frequency is increased [before: 272; after:
1575]. This result is comparable to the studies done by Manjushree Waingadae.72
Similar studies conducted by Popova et al and Fernanda Angelieri to find out the
genotoxic effects of low level ionizing radiation on buccal mucosa by evaluating the MN
frequencies before exposure as 0.04±0.06% & 2.34 ±1.49% respectively and after

Discussion
58
exposure as 0.05±0.06% and 2.81±1.64% respectively.61, 63
There is no gender
predilection noted in the present study. Even though, this result does not correlates with
the studies done by Ramakrishna Mahadevan, where a female predominance is noted,
present study result correlates with the study done by Anuradha et al.70, 71
The higher
frequency of micronucleus in buccal epithelial cells observed after X ray exposure
corroborates the data in the review done by D A Ribeiro et al.82
in which X ray radiation
are reported to be effective in inducing genetic damage. A high radiation dose of the
patients [panoramic radiograph and lateral cephalographs] could be a reason for the
positive result.
Apart from MN presence, other nuclear anomalies like Karyorrhexis, karyolysis,
pyknosis were also determined. Tolbert et al described these nuclear alterations as
phenomenon that can occur not only during physiological cellular differentiation but also
during cell death with DNA damage.25
Mechanisms leading to the production of these
abnormalities are still unknown. Among the various nuclear abnormalities, Karyorrhexis,
karyolysis and pyknosis are considered to be biomarker for cell death evidence, different
stages of necrosis indicators and identifying the response to cell damage respectively.
Karyorrhectic cell shows the destructive fragmentation of the nucleus where the
chromatin is distributed irregularly through the cytoplasm. Karyolysis is the complete
dissolution of chromatin in dying cells. The cell appears without nucleus like a ghost
image without staining. Pyknosis is the irreversible condensation of chromatin in the
nucleus of degenerating cell. The diameter of the nucleus is 1/3rd
– 2/3rd
of the normal
nucleus.

Discussion
59
The number of cells undergoing Karyorrhexis, karyolysis, and pyknosis is
estimated in 100 cells from each slide. For Karyorrhexis, the mean value was 3.08±3.26
before exposure and 3.63±3.23 after exposure and for karyolysis the mean values are
5.20±4.53 before exposure and 6.39±5.45 after exposure. There is an increase in these
nuclear abnormalities after exposure to ionizing radiation even though it is not very
statistically significant (P value:1.73 [Karyorrhexis] & 0.056 [karyolysis]) But it was in
contrast with the study done by Ana Elisa where a significant increase in the number of
Karyorrhectic cell were noted.62
The increase in karyolysis was not of much statistical
significance, which suggests that the cellular response to X rays does not induce a
cytotoxic effect that lead to necrosis. This results correlates with the study of Cerqueira
et al in 2004.59
But the mean value of pyknosis was 6.42±4.36 before exposure and
7.96±6.32 after 10 days. It has a P value of 0.02 which is statistically significant. These
result correlates with the study done by Anuradha et al where a significant increase in
the pyknosis is noted (P<0.001).70
The results suggest that since pyknosis is a nuclear
alteration indicative of apoptosis, there are multiple routes that leads cell to apoptosis.
But the study done by Cerqueira et al did not find significant increase in pyknosis in
exfoliated cells after exposure.59
But in the present study there is an overall increase in
the nuclear alterations after radiation exposure. Analogous results were described by
other authors. Considered in-toto such results supports the notion that low level ionizing
radiations are cytotoxic agents.

Discussion
60
This study has some areas which leave room for debate. Staining with Feulgen stain
which is recommended by most authors was not attempted as we felt that the PAP stain
has certain advantages which have been discussed. Other genotoxic factors and nuclear
alterations like condensed chromatin and nuclear buds etc were not assessed in the study.
Further larger studies are recommended to consolidate the findings and rectify the few
shortcoming of the present study.

SUMMARY & CONCLUSION

Summary & Conclusion
61
The objective of the study was to evaluate the genotoxic and cytotoxic changes
after low level ionizing radiation. Buccal epithelial cells were stained with RAPID
PAPTM
kit, before and 10 days after exposure. Genotoxic effect was evaluated by micro
nucleus assay which is found to be high after exposure. The various other nuclear
alterations like Karyorrhexis, karyolysis and pyknosis are evaluated and there is an
increase in these parameters after exposure. The result depends on the type, amount and
radiation dose absorbed and the individual’s capacity to withstand the action of genotoxic
agents. Future studies should evaluate populations according to age, different cell
collection procedures, DNA staining procedures and type of radiographs. The possibility
of other genotoxic factors and other nuclear changes should also be investigated.
Since the use of radiographs has become more frequent in dental practice as a
diagnostic measure, treatment planning or for follow up, their indication should always
follow the concept of maximum benefit with minimum risk. Our study indicates the
presence of genotoxic and cytotoxic changes after exposure. Radiographs should be made
carefully avoiding retakes and thereby decreasing the radiation dose thus reducing risk of
cytogenic damage. Thus based on the present study we cannot consider exposure from
low level ionizing radiation as risk –free and should be used only when necessary. Based
on the results of the study, low level ionizing radiation do carry their own level of risk in
inducing cellular and genetic changes and should be used with caution and only as and
when necessary.

BIBLIOGRAPHY

Bibliography
x
1. Alain Sarasin. An Overview of the Mechanisms of Mutagenesis And
Carcinogenesis. Mutat Res.2003;544: 99–106.
2. Sheik S, Pallagatti s, Grewal H, Kalucha A, Kaur H. Genotoxicity of digital
panoramic radiography on oral epithelial tissues. Quintessence
Int.2012;43(8):719-725.
3. Olivia Torres- Bugarin, Maria Guadalupe Zavala – Cerna, Arnulfo Nave,
Aurelio Flores- Garcia and Maria Luisa Ramos – Ibarra. Potential uses,
limitations and basic procedures of micronuclei and nuclear abnormalities in
buccal cells. Dis Markers.2014;1-13.
4. Bina Kashyap, Padala Sridhar Reddy. Micronuclei Assay of Exfoliated Oral
Buccal Cells: Means to Assess the Nuclear Abnormalities in Different
Diseases. J Cancer Res Ther. 2012;8(2):184-191.
5. David J. Brennera,B, Richard Dollc, Dudley T. Goodheadd, Eric J. Halla,
Charles E. Lande, John B. Little F, Jay H. Lubing, Dale L. Prestonh, R. Julian
Prestoni, Jerome S. Puskinj, Elaine Rone, Rainer K. Sachsk, Jonathan M.
Sametl, Richard B. Setlowm, And Marco Zaider. Cancer Risks Attributable to
Low Doses of Ionizing Radiation: Assessing What We Really Know.Proc Natl
Acad Sci U S A 2003;100(24):13761–13766.
6. John. B. Little. Radiation Carcinogenesis. Carcinogenesis. 2000;21(3):397-
404.
7. White &Pharaoh; principles of radiographic interpretation. 6th
edition.

Bibliography
xi
8. Dionatas Ulises de Oliveira Meneguetti, Francisco Carlos da Silva, Renato
André Zan, and Leandro José Ramos. Adaptation of the micronucleus
technique in Allium Cepa. Mutagenesis.2012;2(2):1-3.
9. Stefano Bonassi, Monica Neri, Riccardo Puntoni. Validation of Biomarkers as
Early Predictors of Disease. Mutat Res. 480–481 (2001) 349–358
10. Harshvardhan S. Jois, Alka D. Kale, Mohan Kumar K.P.Micronucleus as
Potential Biomarker of Oral Carcinogenesis. IJDA.2010; 2(2):197- 202.
11. Azeddine Elhajouji, Magdalena Lukamowicz, Zoryana Cammerer and
Micheline Kirsch-Volders. Potential Thresholds for Genotoxic Effects by
Micronucleus Scoring.Mutagenesis.2011;26(1):199–204.
12. Iise Decordier, Micheline Kirsch- Volders. Invitro micronucleus test: from
past to future. Mutat Res.2006; 607: 2-4.
13. H.J. Evans, G.J. Neary, F.Williamson. The relative biological efficiency of
single doses of fast neutrons and gamma-rays on Vicia faba roots and the
effect of oxygen. Part II Chromosome damage: the production of
micronuclei.Int J Radiat Biol.1959;3:216–229.
14. B. Matter, W. Schmid. Trenimon-induced chromosome damage in bone-
marrow cells of six mammalian species evaluated by the micronucleus test.
Mutat Res.1971;12:417–425.
15. B.J. Majer, B. Laky, S. Knasm¨Uller, F. Kassie. Use Of The Micronucleus
Assay With Exfoliated Epithelial Cells As A Biomarker For Monitoring
Individuals At Elevated Risk Of Genetic Damage And In Chemoprevention
Trials. Mutat Res. 2001;489:147–172.

Bibliography
xii
16. Michael Fenech, Nina Holland, Wushou P. Chang, Errol Zeiger, Stefano
Bonassi. The Human Micronucleus Project—An International Collaborative
Study On The Use Of The Micronucleus Technique For Measuring DNA
Damage In Humans. Mutat Res.1999;428: 271–283.
17. Michael Fenech, Stefano Bonassi, Julie Turner, Cecilia Lando, Marcello
Ceppi , Wushou Peter Chang, Nina Holland, Micheline Kirsch-Volders, Errol
Zeiger , Maria Paola Bigatti , Claudia Bolognesi, Jia Cao, Giuseppe De Luca,
Marina Di Giorgio, Lynnette R. Ferguson, Aleksandra Fucic, Omar Garcia
Lima, Valeria V. Hadjidekova, Patrizia Hrelia, Alicja Jaworska, Gordana
Joksic, A.P. Krishnaja, Tung-Kwang Lee, Antonietta Martelli, Michael J.
McKay, Lucia Migliore, Ekaterina Mirkova, Wolfgang-Ulrich Müller,
Youichi Odagiri, Thierry Orsiere, Maria Rosaria Scarf`I, Maria J. Silva,
Toshio Sofuni, Jordi Suralles, Giorgio Trenta, Irena Vorobtsova, Anne Vral
And Andrea Zijno.Intra and Inter-Laboratory Variation in the Scoring of
Micronuclei and Nucleo-plasmic Bridges In Binucleated Human Lymphocytes
Results Of An International Slide-Scoring Exercise By The HUMAN Project.
Mutat Res.2003;534: 45–64.
18. Michael Fenech, Nina Holland1, Errol Zeiger, Wushou P. Chang, Sema
Burgaz, Philip Thomas, Claudia Bolognesi, Siegfried Knasmueller, Micheline
Kirsch-Volders And Stefano Bonassi. The HUMAN and Human XL
International Collaboration Projects on Human Micronucleus Assays in
Lymphocytes and Buccal Cells—Past, Present and Future.Mutagenesis.2011;
26(1):239–245.

Bibliography
xiii
19. Nina Holland, Claudia Bolognesi, Micheline Kirsch-Volders, Stefano Bonassi,
Errol Zeiger, Siegfried Knasmueller, Michael Fenech.The Micronucleus Assay
in Human Buccal Cells as a Tool for Biomonitoring DNA Damage: The
HUMANProject Perspective on Current Status and Knowledge Gaps. Mutat
Res.2008: 659:93–108.
20. Nina Holland, Alexandra Fucic, Domenico Franco Merlo, Radim Sram and
Micheline Kirsch-Volders. Micronuclei in Neonates and Children: Effects of
Environmental, Genetic, Demographic and Disease
Variables.Mutagenesis.2011;26(1):51–56.
21. Stefano Bonassi, Barbara Biasotti, Micheline Kirsch-Volders, Siegfried
Knasmueller, Errol Zeiger, Sema Burgaz, Claudia Bolognesi, Nina Holland,
Philip Thomas And Michael Fenech. State of the Art Survey of the Buccal
Micronucleus Assay— A First Stage in the HUMN XL Project Initiative.
Mutagenesis.2009;24(4):295–302.
22. A.T. Natarajan. Chromosome Aberrations: Past, Present and Future. Mutat
Res.2002: 504:3–16.
23. H. F. Stich, R H San, M P Rosin. Adaptation of DNA repair and micronucleus
tests to human cell suspensions and exfoliated cells. Ann N Y Acad
Sci.1983;407: 93-105.
24. F Sarto, S Finotto, L Giacomelli, D Mazzotti, R.Tomainin, A G Levis. The
micronucleus assay in exfoliated cells of human buccal mucosa.
Mutagenesis.1987;2:11-17.

Bibliography
xiv
25. P.E. Tolbert, C.M. Shy, J.W. Allen. Micronucleus and other anomalies in
buccal smears. Afield test in snuff users. Am J Epidemiol.1991;134;840-850.
26. Swapan Samanta and Parnab Dey. Micronucleus and its Application.Diagn
Cytopathol.2010;40(1): 84-90.
27. Judith H. Ford, Carolyn J. Schultz, and Anthony T. Correll. Chromosome
Elimination in Micronuclei: A Common Cause of Hypoploidy. Am J Hum
Genet.1988;( 43):733-740.
28. Daniela Cimini, Daniela Fioravanti, E. D. Salmon and Francesca Degrassi.
Merotelic Kinetochore Orientation versus Chromosome Mono-Orientation in
the Origin of Lagging Chromosomes in Human Primary Cells. J Cell
Sci.2002;115:507-515.
29. Wolfgang –Ulrich Muller, Michael Nusse, Bete M Miller, Anne Slavotinek,
Silvia Viaggi, Christian Streffer. Micronuclei; A Biological Indicator of
Radiation Damage. Mutat Res.1996; 366:163-169.
30. J.A.M.Belien, M.P.Copper, B J.M.Braakhuis, G.B-Snow and
J.P.A.Baak.Standardization of Counting Micronuclei: Definition of A Protocol
to Measure Genotoxic Damage In Human Exfoliated
Cells.Carcinogenesis.1995;16(10):2395-2400.
31. Paige E Tolbert, Carl M Shy and James W Allen. Micronucleus and Other
Nuclear Anomalies in Buccal Smears; Methods Development. Mutat
Res.1992;271:69-77.
32. Raj HG, Kohli E, Rohil V, Dwarakanath BS, Parmar VS, Malik S, Adhikari
JS, Tyagi YK, Goel S, Gupta K, Bose M, Olsen CE.Acetoxy-4-

Bibliography
xv
methylcoumarins confer differential protection from aflatoxin B(1)-induced
micronuclei and apoptosis in lung and bone marrow cells.
MutatRes.2001;494(1-2):31-40.
33. Yusuf Ozkul, Hamiyet Donmez Aydin Erenmemisoglu, Halil Demirtas and
Nalan Imamoglu.Induction of Micronuclei by Smokeless Tobacco on Buccal
Mucosa Cells of Habitual Users.Mutagenesis.1997;12(4):285-287.
34. Fekadu Kassie, Firouz Darroudi, Michael Kundi, Rolf Schulte-Hermann and
Siegfried Knasm Ulle.Khat (Catha Edulis) Consumption Causes Genotoxic
Effects in Humans.Int. J. Cancer.2001;92:329–332.
35. V.Ramakrishnan, S.Gowthamkumarands. Govindaraju Cytogenetic Analysis
of Micronuclei, Sister Chromatid Exchange and Chromosomal Aberrations in
Pan Masala Chewers.Int J PharmaBio Sci.2011:2(3):B112-B134.
36. Noushin Jalayer Naderi, Sareh Farhadi, Samaneh Sarshar. Micronucleus
Assay of Buccal Mucosa Cells in Smokers with the History of Smoking Less
and More Than 10 Years. Indian Journal of Pathology and
Microbiology.2012;55(4):433-438.
37. Sachin Jindal, Ishita Chauhan, Harshaminder Kaur Grewal. Alteration in
Buccal Mucosal Cells Due To the Effect of Tobacco and Alcohol by
Assessing the Silver-Stained Nucleolar Organizer Regions and Micronuclei.
Jcytol.2013;30(3):174-178.
38. Gurjeet Kaur and Ajit Pal Singh.Evaluation of Micronuclei and Other Nuclear
Abnormalities in Buccal Cells of Tobacco Chewers.Hum Biol.2013;2(2):185-
192.

Bibliography
xvi
39. Himadri Kalita, Dulal Chandra Boruah, Karabi Dutta and Rajlakshmi Devi.
Genotoxic Effect on Buccal Epithelial Cells of Betel Quid Chewers by
Micronuclei Assay. Asian J Exp Biol Sci.2013;4(3):491-494.
40. Ariana Znaor, Aleksandra Fuèiæ, Marija Strnad, Danica Barkoviæ, Mladen
Škara, Izet Hozo.Micronuclei in Peripheral Blood Lymphocytes as A Possible
Cancer Risk Biomarker: A Cohort Study of Occupationally Exposed Workers
in Croatia. Croat Med J.2003;44:441-446.
41. A. Halder, T. Chakraborty, K. Mandal, P. K. Gure, S. Das, R. Raychowdhury,
A. K. Ghosh And M. De. Comparative Study of Exfoliated Oral Mucosal Cell
Micronuclei Frequency in Normal, Precancerous and Malignant
Epithelium.Int J Hum Genet.2004;4(4):257-260.
42. Kumari Rimpu, Chaugule Arun, Goyal Pk.Karyoanomalic Frequency during
Radiation Therapy. J Cancer Res Ther.2005;1(3):187-190.
43. Rashmi Saran, Ravindra K. Tiwari, Penagaluru Paradhanandan Reddy,Yog
Raj Ahuja. Risk Assessment of Oral Cancer in Patients with Pre-Cancerous
States of the Oral Cavity using Micronucleus Test and Challenge Assay.Oral
Oncol.2008;44:354– 360.
44. Waranun Buajeeb, Petcharat Kraivaphan,Cholticha Amornchat, Terdphong
Triratana.Frequency of Micronucleated Exfoliated Cells in Oral Lichen
Planus. Mutat Res.2007;627:191–196.
45. Pollyanna Francielli De Oliveira Augusto Faria Andrade Fernanda Ferreira
Malheiros Suzie Aparecida De Lacerda, Alessandra Aparecida Campos A
José Eduardo Zaia A Andréa De Oliveira Cecchi. Evaluation of The

Bibliography
xvii
Frequency Of Micronuclei inExfoliated Cells from Oral Lesions
PreviouslyIdentified By Toluidine Blue; Acta Cytol.2011;55:344–349.
46. Parnab Dey, Swapan Samanta and Shaily Susheilia. Micronucleus Assay in
Buccal Smears of Breast Carcinoma Patients.Diagn
Cytopathol.2010;40(8):664666.
47. Parvathidevi,Thimmarasa V B, Vishal Mehrotha, Pallak Arora. Micronucleus
Assay for Evaluation of Genotoxicity in Potentially Malignant and Malignant
Disorders. JIOMR.2011;23(2):97-100.
48. Shally Khanna, Anupam Purwar, Narendra Nath Singh, Gadiputi Sreedhar,
Shailendra Singh, Saurabh Bhalla.Cytogenetic Biomonitoring of Premalignant
and Malignant Oral Lesions by Micronuclei Assessment: A Screening
Evaluation.European J Gen Dent.2014;3(1):46- 52.
49. Uma.A.N, Dhananjay.S.K, Tirou Aroul, Satvinder Bakshi Singh,
Lokeshmaran.A.Comparative Cytogenetic Study of Exfoliative Oral Mucosal
Cells in Tobacco Related Potentially Malignant Disorders in A South Indian
Population. IJOART.2014;3(8): 6-12.
50. Susana Pastor, Sara Gutierrez, Amadeu Creus, Antonina Cebulska-
Wasilewska, Ricard Marcos. Micronuclei in Peripheral Blood Lymphocytes
and Buccal Epithelial Cells of Polish Farmers Exposed to Pesticides. Mutat
Res.2001;495:147–156.
51. Elisângela de Fátima Rezende, Maria Cristina Mendes-Costa, Johnson
Campideli Fonseca,Alex de Oliveira Ribeiro. Nuclear anomalies in the buccal
cells of children under dental treatment. RSBO.2011;8(2):182-188.

Bibliography
xviii
52. Mariza A, Mastsumoto, Juliane Castatio, Roberto Y Kawakami and D A
Ribeiro. Cytological damage in exfoliated oral mucosal cells in elderly people
suffering from denture stomatitis. Gerontology.2010;27(3):183-185.
53. Sudha Sellappa, Shibily Prathyumnan, Shyn Joseph, and Kripa S Keyan.
Micronucleus Test in Exfoliated Buccal Cells from Chromium Exposed
Tannery Workers.Int J Biosci Biochem Bioinforma.2011;1(1):58-62.
54. Haritha Avula, Ashank Mishra, Ruchi Pandey, Murali Krishna, Butchi Babu
Kalakonda, Jayakumar Avula.The Micronucleus Test to Evaluate Cytogenetic
Damage in Patients with Periodontitis.J Periodontol Implant
Dent.2012;4(2):29-33.
55. H. Thierens, A Vral, R. Morthier, B. Aousalah And L. De Ridder. Cytogenic
Monitoring Of Hospital Workers Occupationally Exposed To Ionizing
Radiation Using The Micronucleus Centromere
Assay.Mutagenesis.2000;15(3): 245- 249.
56. Jasminka Batanjac. Enhanced Frequency of Chromosomal Aberrations in
Workers Occupationally Exposed to Ionizing Radiations.The Scientific
Journal Facta Universitatis Series: Medicine and Biology.2000;7(1):46 – 48.
57. Francesa Maffei, Sabrina Angelini Giorgio Cantelli Forti, Vittorio Lodi,
Francesco Saverio Violantae, Stefano Mattioli, Patriz Hrelia. Micronucleus
Frequencies in Hospital Workers Occupationally Exposed to Low Levels.
Mutagenesis.2002;17(5):405-409.

Bibliography
xix
58. I. Sari-Minodier, T. Orsière, L. Bellon, J. Pompili, C. Sapin, A. Botta.
Cytogenetic Monitoring Of Industrial Radiographers Using The Micronucleus
Assay; Mutat Res.2002;521:37–46.
59. E.M.M. Cerqueira, I.S. Gomes-Filho, S. Trindade, M.A. Lopes, J.S. Passos B,
G.M. Machado-Santelli.Genetic Damage In Exfoliated Cells From Oral
Mucosa Of Individuals Exposed To X-Rays During Panoramic Dental
Radiographies. Mutat Res.2004;562:111–117.
60. Sabrina Angelinia. B Rajiv Kumarb,C Fabio Carbonea, Francesca Maffeia,
Giorgio Cantelli Fortia, Francesco Saverio Violanteb. D VittorioLodib.D,
Stefania Curtib.D, Kari Hemminkib.C, Patrizia Hreliaa. Micronuclei in
Humans Induced By Exposure to Low Level of Ionizing Radiation: Influence
of Polymorphisms In DNA Repair Genes. Mutat Res.2005;570:105–117.
61. L Popova, D Kishkilova, V B Hadjidekova, R P Hristova, P Atanasova, V.V
Hadjidekova, D Ziya and VGHadjidekova. Micronucleus Test in Buccal
Epithelium Cells from Patients Subjected To Panoramic Radiography.
Dentomaxillofac Radiol.2007;36:168–171.
62. Ana Elisa Da Silva, Pantelis Varvaki Rados, Isabel Da Silva Lauxen, Luhana
Gedoz, Eduardo Aydos Villarinho, Vania Fontanella. Nuclear Changes in
Tongue Epithelial Cells Following Panoramic Radiography. Mutat
Res.2007;632:121–125.
63. F. Angelieri, de Oliverira G R, Sannomiya EK, D A Ribeiro. DNA damage
and cellular death in oral mucosa cells of children who have undergone
panoramic radiography. Pediatr Radiol.2007;37(6):561-565.

Bibliography
xx
64. Da Ribeiro, G De Oliveira, Gm De Castro and F Angelieri; Cytogenetic
Biomonitoring in Patients Exposed To Dental X-Rays: Comparison between
Adults and Children.Dentomaxillofac Radiol.2008;37:404–407.
65. V Carlin1, A J Artioli, Ma Matsumoto, H N Filho, E Borgo, CT F Oshima and
D A Ribeiro; Biomonitoring of DNA Damage and Cytotoxicity in individuals
exposed to cone beam computed tomography.Dentomaxillofac
Radiol.2010;39:295–299.
66. F Angelieri, V Carlin, DM Saez, R Pozzi and D A Ribeiro. Mutagenicity and
Cytotoxicity Assessment in Patients Undergoing Orthodontic
Radiographs.Dentomaxillofac Radiol.2010; 39:437–440.
67. Fernanda Angelieri, Tatiana de Cassia, Goncalves Moleirinho, Viviane Carlin,
Celina Tizuko Fujiama Oshima, Daniel Araki Ribeiro. Biomonitoring of oral
epithelial cells in smokers and non- smokers submitted to panoramic X-ray:
comparison between buccal mucosa and lateral border of tongue.Clin Oral
Investig.2010;14(6):669- 674.
68. Eman A El Ashiry, Eman A Abi Hager, Abeer S Gawish. Genotoxic effectsof
panoramic radiographs in children. J Clin Pediatr Dent.2010;35(1):69-74.
69. D.A. Ribeiro, Sannomiya E K, Pozzi R, Miranda S R, Angelieri F. Cellular
death but not genetic damage in oral mucosal cells after exposure to digital
lateral radiography. Clin Oral Investig.2011;15(3):357-360.
70. Anuradha Pai, Rakesh C. Sharma, Raghavendra Mahadev Naik, Yadavalli
Guruprasad. Biomonitoring of Genotoxic and Cytotoxic Effects of Gingival

Bibliography
xxi
Epithelial Cells Exposed to Digital Panoramic Radiography.J Orofac
Sci.2012;4(2):124-128.
71. Ramalekshmi Mahadevan, Manikandan Kumaraswamy, S. Kailasm, S. Manoj
Kumar; Genetic Damage in Exfoliated Cells from Oral Mucosa of Individuals
Exposed To X- Rays After PanoramicRadiography; A Cross- Sectional
Study.J Indian Acta Oral Med Radiol.2012;24(2):102-105.
72. Manjushri Waingade, Raghavendra S Medikeri. Analysis of micronucleus in
buccal cells in patients subjected to panoramic radiography. Indian J Dent
Res.2012;23(5):574-578.
73. Lorenzoni D.C, Cuzzuol Fracaloni A.C, Carlin V, D. A. Ribeiro, Santo Anna
E.F. Cytogenic biomonitoring in children submitting toa complete set of
radiographs. Angle Orthod.2012;82(4):585-590.
74. Thomas.P, Ramani P, Premkumar P Natesan A, Sherlin H J, Chandrasekhar T.
Micronucleus and other nuclear anomalies in buccal mucosa following
exposure to X-ray radiation. Anal Quant Cytol Histol.2012;34(3):161-169.
75. Lorenzoni D C, D A Ribeiro, Santanna EF. Mutagenicity and cytotoxicity in
patients submitted to ionizing radiation. Angle Orthod.2013;83(1):104-109.
76. Vidya KB, Anupama N. Kalappanava, Muniyappa M. Genotoxic Effects of
Panoramic Radiation by Assessing the Frequency of Micronuclei Formation in
Exfoliated Buccal Epithelium.Int J Res Med Sci.2014;2(2):541-544.
77. Pallak Arora, Parvathi Devi, Sartaj Singh Wazir. Evaluation of Genotoxicity
in Patients Subjected to Panoramic Radiography by Micronucleus Assay on
Epithelial Cells of Oral Mucosa.J Dent (Tehran).2014;11(1):47-55.

Bibliography
xxii
78. Michael Fenech. Biomarkers of genetic damage for cancer epidemiology.
Toxicology.2002;181:411-416.
79. Sarika Laxman Dindgire, Suchitra Gosavi, Ramniwas M. Kumawat, Sindhu
Ganvir, Vinay Hazarey. Comparative Study of Exfoliated Oral Mucosal Cell
Micronucleus Frequency in Potentially Malignant and Malignant Lesions.
IJOMP.2012; 3(2):15-20.
80. John D Bancroft. Theory and practice of histological technique. 6th
Edition.
81. Miyaji CK, Colus IM. Cytogenic biomonitoring of Brazilian dentists
occupationally exposed to low doses of X-radiation. Pesqui Odontol
Bras.2002;16(3):196-201.
82. Da Ribeiro. Cytogenetic Biomonitoring in Oral Mucosa Cells Following
Dental X-Ray. Dentomaxillofac Radiol. 2012;41: 181–184.

ANNEXURES


CONSENT FORM PART 1 OF 2
INFORMATION FOR PARTICIPANTS OF THE STUDY
1. Name of the Principal Investigator:
Meera Mathai
Post Graduate student
Department of Oral Medicine and Radiology,
Sree Mookambika Institute of Dental Sciences,
Kulasekharam, KanyaKumari District-629161
2.Name of the Guide: Dr. P.G.Agnihothri M.D.S Professor & H.O.D
Department of oral medicine and Radiology.
Sree Mookambika Institute of Dental Sciences.
Kulasekharam, KanyaKumari District-629161
Dear Volunteers,
We welcome you and thank you for your keen interest in participation in this
research project. Before you participate in this study, it is important for you to understand
why this research is being carried out. This form will provide you all the relevant details of
this research. It will explain the nature, the purpose, the benefits, the risks, the discomforts,
the precautions and the information about how this project will be carried out. It is important
that you read and understand the contents of the form carefully. This form may contain
certain scientific terms and hence, if you have any doubts or if you want more information,
you are free to ask the study personnel or the contact person mentioned below before you
give your consent and also at any time during the entire course of the project.

2. Name of the Co-Guide: Dr. Hema.G. MDS.
Reader
Department of oral medicine and Radiology.
Sree Mookambika Institute of Dental Sciences.
Kulasekharam, KanyaKumari District-629161
4.Institute:
Sree Mookambika Institute of Dental Sciences,
V.P.M Hospital complex, Padanilam, Kulasekharam,
Kanyakumari – 629161
Tamilnadu
5. Title of the study:
“Biomonitoring of genotoxic and cytotoxic effects among patients exposed to digital
radiographs- a comparitative study .”
6 .Background information:
You are undergoing orthodontic treatment in which radiographs are
compulsory and in our study we are making you as a subject taking two salivary
samples without causing any discomfort to you people. The analysis of sample gives
an idea about your exposure to x-rays and gives a precaution about your exposure in
future.
7.Aims and Objectives:
1. To compare genotoxic and cytotoxic before and after radiation
2. To study the changes in the micronuclei before and after radiation
3. To compare whether there is any cytological changes before and after
radiation

8.Scientific justification of the study:
Exposure to x-rays are hazardous to body and public will be under impression
that even minor expoure radiation is hazardous. Here we are trying to establish that
though the patient is exposed to radiation, the exposure is going to be minimum with
minimum damages to human being. Here an attempt is made to explain individuals,
with a detailed experiments to appreciate that the toxicity will be minimum.
9.Procedure for the study:
• Once you are enrolled into the study a roll no will be implemented to represent the
name.
• Patients are advised to wash their mouth with water to remove debris from the site.
• Buccal epithelial cells are obtained using brush biopsy technique using a soft bristle
tooth brush, immediately before exposure and 10 days after exposure.
• The solution will be sent for cytological evaluation.
10.Expected risks for the participants:
• Abrasion to buccal mucosa.
11.Expected benefits of research for the participants:
• You will not be required to pay for the lab tests.
• You can enquire about the outcome of the procedures and your details.
12.Maintenance of confidentiality:
• You have the right to confidentiality regarding the privacy of your medical
information
(Personal details, results of physical examinations, investigations, and your
medical history).
• By signing this document, you will be allowing the research team investigators, other
study Personnel, sponsors, institutional ethics committee and any person or agency
required by law to view your data, if required.
• The results of clinical tests and therapy performed as part of this research may be
included in your medical record.

• The information from this study, if published in scientific journals or presented at
scientific meetings, will not reveal your identity.
13.Why have I been chosen to be in this study?
Chosen because of groping under the inclusion and exclusion criteria
Need of good sampling size
No invasive procedure that harm your health and helps in diagnosis and
helpful for the society
14.How many people will be in the study?
126 15.Agreement of compensation to the participants (In case of a study
related injury): Patient will be taken care in case of complication and medical treatment will
be provided in the institution.
16.Anticipated prorated payment, if any, to the participant(s) of the
study: No
17.Can I withdraw from the study at any time during the study
period?
• The participation in this research is purely voluntary and you have the right to
withdraw from this study at any time during the course of the study without giving
any reasons.
• However, it is advisable that you talk to the research team prior to stopping
information.
18.If there is any new findings/information, would I be informed? Yes

19.Expected duration of the participant’s participation in the study:
1 year
20.Any other pertinent information: Not applicable
21. Whom do I contact for further information?
Place: Kulasekharam
Date:
Signature of Principal Investigator
Signature of the participant
For any study related queries, you are free to contact :
Meera Mathai
Post Graduate student.
Department of Oral Medicine and Radiology,
Sree Mookambika Institute of Dental Sciences,
Kulasekharam, KanyaKumari District-629161.
Mobile No: 08281538491

CONSENT FORM
PART 2OF 2
PARTICIPANT CONSENT FORM
The details of the study has been explained to me in writing
and the details have been fully explained to me. I am aware that the results of the e
study may not be directly beneficial to me but will help in the advancement or medical
sciences. I confirm that the understood the study had the opportunity to ask questions. I
understood that my participation in the study is voluntary and that I am free to withdraw
it any time, without giving any reason, without the medical cure that will normally be
provided by the hospital being affected I agree not to restrict the use of any data or
results that arise from this study provided such a use is only for scientific purpose I
have been given an information sheet giving details of the study. I fully consent to
participate in the study titled “ Biomonitoring of genotoxic and cytotoxic changes
among patients exposed to digital radiographs”- a comparative study
Serial / ref no
Name of the participant: Address of the Participant:
Contact number of the Participant:
Signature/Thumb impression of the participant/ Legal guardian
Witnesses:
1.
2.
Date:
Place: Kulasekharam

k½X]Xw þ 1]T\hpambn klIcn¡p¶ hyànIfpsS Adhntebv¡v
]nbs¸« k¶² tkhI³/tkhI,
R§Ä \n§sf kzmKXw sN¿p¶p. AtXmsSm¸w Cu ]T\hpambn
klIcn¡m\pÅ k¶²XtbmSv \μn tcJs¸Sp¯p¶p. \n§Ä Cu
]T\ n ]s¦Sp¡p¶Xn\v ap³]v Cu ]T\w F n\mWv \S¯s¸Sp¶Xv
F¶v Adntb-Xp-v. AXn\m Cu t^md¯n KthjW]T\¯nsâ
hnhc§fpw aäpw hniZambn tcJs¸Sp nbncn¡p¶p. Cu ]T\ nsâ coXn,
Dt±iw, ]tbmP\w, A]ISkm²yX, t¢iw, ap³IcpXÂ, F§s\ Cu ]T\w
ap³t]m«p sIm-pt]mIp¶p F¶n§s\ FÃm hnhc§fpw t^md nÂ
tcJs¸Sp nbncn¡p¶p. kZbw Cu hnhc§Ä hmbn p a\Ênem¡phm³
A yÀ°n¡p¶p. Cu hnhc§fn imkvX]camb ]Z§Ä DÅXn\mÂ
kwib\nhmcW¯n\p ][m\ ]T\IÀ¯mhnt\mtSm Xmsg
tcJs¸Sp¯nbncn¡p¶ hyànItfmtSm t^mdw H¸nSp¶Xn\p ap³t]m
Asæn Cu ]T\ nsâ Imemh[n Xocp¶hsctbm kao]n¡mhp¶XmWv.

1. ][m\ ]T\IÀ¯mhv/KthjI
tUm. aocm a¯mbn
_ncpZ\m´c _ncpZ hnZymÀ°n
Un mÀ«vsaâv Hm v Hmd saUnkn³ Bâv tdUntbmfPn,
io aqImw_nI C³Ìnäyq«v Hm v sUâ kb³kkv,
hn.]n. Fw. tlmkv]nä tImw¹Ivkv, ]S\new
IpetiJcw, I\ymIpamcn þ 629 161
2. ][m\ amÀ¤ZÀin
tUm. ]n.Pn AántlmXn,
s]m^kÀ,
Un mÀ«vsaâv Hm v Hmd saUnkn³ Bâv tdUntbmfPn
io aqImw_nI C³Ìnäyq«v Hm v sUâ kb³kkv,
hn.]n. Fw. tlmkv]nä tImw¹Ivkv, ]S\new
IpetiJcw, I\ymIpamcn þ 629 161
3. klamÀ¤ZÀin
tUm. tla.Pn.
doUÀ
Un mÀ«vsaâv Hm v Hmd saUnkn³ Bâv tdUntbmfPn
io aqImw_nI C³Ìnäyq«v Hm v sUâ kb³kkv,
hn.]n. Fw. tlmkv]nä tImw¹Ivkv, ]S\new
IpetiJcw, I\ymIpamcn þ 629 161
2

4. ]T\tIμw
io.aqImw_nI C³Ìnäyq«v Hm^v
sUâ kb³kv, hn.]n.Fw.
tlmkv]nä tImw¹Ivkv, ]S\new,
IpetiJcw, I\ymIpamcn 629 161
5. ]T\¯nsâ ioÀjIw
tcmKnIfn UnPnäÂ
FIvkvtdbv¡p tijapÅ P\nXnI
Xe¯nepw, IWnIXe¯nepw DÅ
amä§fpsS \nÀ®bw
6. ]Ým¯e hnhcw: UnPnä FIvkvtd aqew Ihnfnsebpw,
tamWIfnsebpw, tImi§fnepÅ \yq¢nbkn\p amä§Ä D-mhm³
km²yXbp-v. CXn\m UnPnä FIvkvtd D]tbmK¯n i²
sNept¯-XmWv.
7. e£y§fpw Dt±i§fpw: 1) FIvkvtdbv¡v ap³]pw, ]n³]papÅ
Pot\mtSmIvkn¡pw, ssktämtSmIvkn¡pw Bb amä§sf XmcXayw sN¿pI
2) FIvkvtdbv¡p ap³]pw, ]n³]papÅ \yq¢nbknse amä§Ä
]Tn¡pI
3) FIvkvtdbv¡v ap³]pw, ]n³]papÅ IWnImXe nepÅ amä§Ä
I-p]nSn¡pI.
8. KthjWw \S¯phm\pÅ \ymboIcWw: tdUntbj³ a\pjycnÂ
A]ISImcnbmWv F¶v ]e ]T\§fneqsSbpw sXfnbn¡s¸«n«p-v.
\yq¢nbknepÅ ]e Xc nepÅ amä§Ä P\nXnI XIcmdpIfntebv¡v
shfn w hoip¶hbmWv. Cu ]T\w FIvkvtd FSp¡p¶Xpaqeap-mIp¶
amä§Ä P\nXnIXe nepw IWnImXe nepw ]cntim[n¡p¶p.
3

9. ]T\coXn :
1) ]T\¯nsâ `mKambn hyàn¡v Hcp \¼À \ÂIp¶XmWv.
2) \n§fpsS apgph³ hnhc§fpaS§nb tIkv lnÌdnbnÂ
tcJs¸Sp¯p¶XmWv.
3) Bhiym\pkcWambn NnX§Ä FSp¡mhp¶XmWv.
4) shÅw D]tbmKn¨v hmbv hr¯nbm¡m\mhiys¸Sp¶p
5) arZphmb Hcp _jv D]tbmKn¨v Ihnfn \n#o¶pw \n§fpsS
Dan\ocnsâ Hcp km¼nÄ FSp¡p¶p.
6) CtX coXnbn ]¯p Znhk¯n\ptijw c-mw kmw]nÄ
FSp¡p¶p.
7) tijw AXv ]cntim[\IÄ¡mbn Ab¡p¶p.
10) ]Xo£n¡p¶ A]ISkm²yXIÄ
sNdnb coXnbn thZ\ (achn¸n¡m\pÅ acp¶pIÄ
D]tbmKn¨v Cu thZ\bpw CÃm¯m¡mhp¶XmWv.
11) ]Xo£n¡mhp¶ ]tbmP\§Ä
1) em_v sSÌpIÄ¡v \n§Ä XpI \ÂtI-XnÃ
2) \n§Ä¡v Cu KthjW nsâ hnhc§Ä Xnc¡mhp¶XmWv.
12) hyànhnhc§fpsS kzImcyX:
1) tcmKhnhc§fpw aäv hyànhnhc§fpw kzImcyambn
kq£n¡s¸Sp¶Xmbncn¡pw
2) Cu t^md¯n H¸nSp¶Xv hgn \nbaw A\pimkn¡p¶
coXnbn ]T\¯n DÄs¸Sp¶ hyànIÄ¡v \n§fpsS
hnhc§Ä ]cntim[n¡mhp¶XmWv.
4

3) Cu ]T\¯nsâ hnhc§Ä imkvXm\p]m[nIfmb
]kn²oIcW§fntem, IqSn BtemN\Ifntem
shfns¸Sp¯t¼mÄ \n§fpsS kzImcyX
kq£n¡s¸Sp¶XmWv
13) F´psIm-v \n§Ä XncsªSp¡s¸«p?
1) ]T\¯n\v \Ã iXam\w BfpIÄ BhiyamWv.
2) ]e Iq«n¡pd¨nepIÄs¡mSphn \n§Ä DÄs¸Sp¶
hn`mKs¯ XncsªSp¯p
3) \n§fpsS klIcWw aqew kaql¯n\v klmbhpw
\·bpw D -mIp¶p.
14) FX BfpIÄ Cu ]T\¯n DÄs¸Sp¶p?126
15) \jvS]cnlmc DS¼Sn? (]T\hpambn _Ôs¸«v Fs´¦nepw]cn¡p - mbmÂ)
]T\hnt[bambn GsX¦nepw Xc n tcmKw k¦oÀ®ambmÂtcmKnsb Cu Øm]\ n hnZKv² NnInÕ¡p hnt[b\m¡p¶XmWv.
16) GsX¦nepw hn[¯n thX\w e`n¡ptam?CÃ
17) Ft¸mÄ thWsa¦nepw F\n¡v Cu ]T\ n \n¶v ]n³amdmtam?
ImcWw hyàam¡msX Ft¸mÄ thWsa¦nepw \n§Ä¡v Cu]T\¯n \n¶pw ]n·mdmhp¶XmWv. F¦nepw AXn\v ap³]mbnKthjIcpambn kwkmcn¡p¶Xv \ÃXmWv.
6

18) ]T\hpambn _Ôs¸« Fs´¦nepw ]pXnb hnhc§Ä Ds-¦nÂFs¶ Adnbn¡p¶XmtWm?
AsX
19) ]Xo£n¡p¶ ]T\Imemh[n ?Hcp hÀjw
20) asäs´¦nepw hnhcw ?CÃ
21) hnhc§Ä¡v _Ôs¸tS-Xv Bsc?
tUm.aocm a¯mbn_ncpZm\´c _ncpZ hnZymÀ°n/\n
_ncpZm\´c _ncpZ hnZymÀ°n/\n
Un¸mÀ«vsaâv Hm^v Hmd saUnkn³ Bâv tdUntbmfPn
io aqImw_nI C³Ìnäyq«v Hm v sUâ kb³kkv,
hn.]n. Fw. tlmkv]nä tImw¹Ivkv, ]S\new
t^m¬ tUm.aocm a¯mbn þ 08281538491
C.sabnÂ,sF.Un.: [email protected]
Øew: ][m\ KthjIsâ H¸v
XobXn k¶² tkhI³/ tkhI
7

k½X]Xw þ 2
Cu ]T\¯nepÅ Fsâ ]¦mfn¯w kz´w XmÂ]cy]Imcw
amXamsW¶pw, Ft¸mÄ thWsa¦nepw tNmZy§Ä _Ôs¸«htcmSv
tNmZn¡msa¶pw, Cu ]T\¯n \n¶pw ImcWw tcJs¸Sp¯msX
Ft¸mÄ thWsa¦nepw F\n¡v ]n³hm§msa¶pw Rm³ a\Ênem¡p¶p.
Cu ]T\mhkm\w shfs¸Sp¶ AdnhpIfpw, tcJIfpw, imkvX]camb
Dt±i§Ä¡p D]tbmKn¡m³ Rm³ k½Xn¡p¶p. ]Tt\mt±iw
hnhcn¡p¶ hniZmwi§Ä \ÂInbn«p-v.
“ ------------------þtcmKnIfn UnPnä FIvkvtdbv¡p tijapÅ P\nXnI Xe¯nepw,
IWnIXe¯nepw DÅ amä§fpsS \nÀ®bw” F¶ Cu ]T\hpambn
klIcn¡m³ Fsâ ]cn]qÀ® k½Xw Adnbn¡p¶p.
tUm.aocm a¯mbn
t]cv (k¶² tkhI³/tkhI) k¶² tkhIsâtbm/
_Ôs¸Sm\pÅ \¼À tkhIbpsStbm hnemkw
km£nIÄ H¸v/hnc ASbmfw
(kz´w/\nba]cmb
1. kwc£I³)
2.
XobXn:
Øew:

Jl◊Rp T•Ym
Tϧ I - 2
BnÆp Te˙LtTY⁄dLÙ] RLYp T•Ym
1. BnYÙ[o
U⁄. ¡WÙ UjRÙn ÿ’L˚X ThPRÙ¨
KWp ˘U•£u Utflm ˙W•˙VÙX¥
c ÍLÙm©LÙ Tp U⁄j’YU˚] Lp̨, œX˙NLWm.
Lu≤VÙœU¨.
2. YØLÙh•
U⁄. ©.¥. Ad°≤ ˙LÙjߨ
˙TWÙ£¨Vo, R˚X˚UVÙ[o
KWp ˘U•£u Utflm ˙W•˙VÙX¥
c ÍLÙm©LÙ Tp U⁄j’YU˚] Lp̨, œX˙NLWm.
Lu≤VÙœU¨.
3. ’˚Q YØLÙh•
U⁄. ˙aUÙ. ¥.
√Po (’˚Q ˙TWÙ£¨Vo)
KWp ˘U•£u Utflm ˙W•˙VÙX¥
c ÍLÙm©LÙ Tp U⁄j’YU˚] Lp̨, œX˙NLWm.
Lu≤VÙœU¨.
4. Bn‹ ®˚XVm
c ÍLÙm©LÙ Tp U⁄j’YU˚] Lp̨, œX˙NLWm,
Lu≤VÙœU¨ UÙYhPm. R™rSÙ”.
5. R˚Xl◊ : •¥hPp F”Lßo ÍXm HtT”m Àu Utflm ß—dL∞u UÙt\eL˚[ Jl©h” TÙojRp.
Ußl©tœ¨V Ru]ÙoYX˙W,
RÙeLs CkR BnÆp Te˙LtL YkR˚Udœ Su±, CkR BnÆp Te˙LtTRtœ
ÿu CkR BnÆu ÿd°Vj’Ym Utflm Ru˚U A±k’ ˘LÙs[ ˙Yi”m. CkR
T•Ym BnÆu ÿ›ÆTWeL˚[Ÿm EeLfidœ ˘R¨Ædœm. BnÆp Te˙LtTRtœ
ÿu CkR T•Yj˚R ÿ›Y’m T•j’ ◊¨k’ ˘LÙiP ©u Te˙LtL ˙Yi”m. CkR
T•Yjßp £X U⁄j’Y Utflm A±ÆVp ˘NÙtLs Es[]. BRXÙp G˙R‡m
Nk˙RLeLs HtThPÙp CkR T•Yjßu Cflß´p œ±l©h”s[ ST¨Pm BnÆp
Te˙LtTRtœ ÿu ˘R∞‹ ˘T\ ˙Yi”m

6. BnÆu ©uTXm :
•¥hPp F”Lߨ]Ùp Y⁄m Lßo≈f— LiQm Utflm D¨u ˘NpL∞u ®⁄‹⁄L˚[
TÙßj’ ˘Np˚X UWQU˚PV ˘Nn°\’. G]˙Y CR˚] U]ßp ˘LÙi” •¥hPp F”Lß˚W
GfN¨d˚LŸPu TVuT”jR ˙Yi”m.
7. œ±d˙LÙs :
• F”Lßo ˘NnYRtœ ÿu Utflm ©u Àu Utflm ß—L∞u HtT”m UÙt\eL˚[ Jl©h”
TÙojRp.
• F”Lßo £°h˚Ndœ ÿu Utflm ©u ®Ÿd- V≥p HtT”m UÙt\eLs.
• F”Lßo ÍXm ˘NpL∞p H˙R‡m UÙt\eLs HtT”Y˚R LiP±Rp.
8. A±ÆVp NÙufl (©uTXm) :
Lßo≈f— U≤R C]jßtœ ATÙVUÙ] Jufl. •.Gu.H. A[Æp Y⁄°u\ L⁄‹dœ¨V
UÙt\m ˘Np ˙NRÙWjßu BWmT NÙu\Ùœm. CkR Bn‹ œ˚\kR F”Lߨ]Ùp LiQjßp
Y⁄°u\ ˘Np Utflm ß—dL∞u UÙt\j˚R LiP±V ˘NnVlT”°\’.
9. YØÿ˚\ :
CkR BnÆp øeLs Te˙Lt˙\©u ReLfidLÙ] R≤ CXdL Gi YZeLlT”m.
RiΩWÙp YÙn˘LÙlT∞j’ —jRm ˘Nn’ ˘LÙs[‹m.
™⁄’YÙ] ©Wx ÍXm YÙn Li]jßp C⁄k’ ˘NpL˚[ F”Lßo £°h˚Ndœ ÿu
Utflm Tj’ SÙhLfidœ ©u‡m G”dL ˙Yi”m.
˘NpL∞u UÙt\eLs Bn‹ ®˚XVjßp LiP±VlT”m.
10. GßoU˚\ Æ˚[‹Ls :
• LiQjßp EWÙn‹
11. HtT”m Su˚ULs :
• BnÆtLÙL TQm G’‹m RW ˙R˚Y´p˚X
• BnÆu ÿ•‹L˚[ øeLs A±k’ ˘LÙs[XÙm.

12. RLY- u TÙ’LÙl◊ :
EeLfi˚PV RLYpLs A˚]j’m TÙ’LÙdLlT”m GkR ®˚X´¤m
˘Y∞´PlTPÙ’.
øeLs CkR BnÆp Te˙Lt\©u GeL[’ BnYÙ[o EeLfi˚PV RLYpL˚[
˘R¨k’ ˘LÙs[ ÿ•Ÿm. ˙U¤m ˙R˚Y HtThPÙp GjßdLp L™h•´Pÿm
LÙi©dLlT”m.
BnÆu ÿ•‹Ls EeLfi˚PV U⁄j’Y RLYp T•Yjßp (˙LÙl©p) Tß‹
˘NnVlT”m.
CkR Bn‹ ÿ•‹ ˘Y∞´PlT”m ˘TÙ›’ EeL[’ RLYpLs ˘Y∞´PlTPÙ’.
13. CkR BnÆp øeLs ˙NoYRtLÙ] LÙWQm?
øeLs CkR BnÆu ˙Nol◊ Utflm Æ”l◊ Yœl◊L∞u Es A˚UVlT”YRÙp
BnÆu ˙R˚YVÙ] UÙߨdLÙL‹m
NÍLjßu Ut\m U⁄j’Y ÿu˙]t\jßtLÙL
14. BnÆu UÙߨ Gi¶d˚L ? 126
15. SxP¬” :
BnÆp HtT”m UÙt\eLfidLÙ] £°h˚N Bn‹ ®˚XVjßp YZeLlT”m.
16. SxP¬” TQm : TQm G’‹m YZeLTPÙ’.
17. BnÆp C⁄k’ GkR ˙SWjߤm GkR LÙWQÿm Cu± ÆXLXÙm
18. BnÆu ÿu˙]t\jßp HtT”m UÙt\eLs ˘R¨ÆdLlTP ˙Yi”m
19. BnÆu LÙX AYLÙNm? J⁄ Bi”
20. ˙Yfl GkR RLYpLfim ˙R˚Y Cp˚X
21. ˘RÙPo◊ ˘LÙs[ ˙Yi•V STo :
CPm :
BnYÙ[o ˚L˘VÙlTm
˙Rß :
Teœ˘TflTYo ˚L˘VÙlTm
U⁄. ¡WÙ UjRÙn
ÿ’L˚X ThPRÙ¨,
JWp ˘U•£u Utflm ˙W•˙VÙX¥,
c ÍLÙm©LÙ Tp U⁄j’YU˚] Lp̨, œX˙NLWm.
˘RÙ˚X˙T£ Gi : 08281538491
™u AgNp : [email protected]

Jl◊Rp T•Ym
TÙLm : 2
Teœ˘TflTY¨u Jl◊Rp T•Ym
CkR BnÆu ÿ› ÆTWeLfim G›j’ ÍXUÙL‹m, ƨYÙL‹m, Gu≤Pm
·\lThP’. G]dœ CkR BnÆu Æ˚[‹Ls GkR TV‡m RWÆp˚X Gu\Ù¤m, U⁄j’Y
A±ÆV- u ˙UmTÙh•tLÙL TVuT”jRlT”m Gufl A±˙Yu. SÙu CkR BnÆp GkR
®oTkRÿm CpXÙUp Teœ˘Tfl°˙\u. ˙U¤m CkR BnÆu GpXÙ ÆßLs Utflm
Æßÿ˚\L˚[Ÿm A±˙Yu. GkR Nk˙RÙLjßtœm ˙LsÆ ˙LhL˙YÙ ApX’ BnÆp
C⁄k’ ÆXL˙YÙ GpXÙ E¨˚ULfim G]dœ Ei” Gufl A±˙Yu. CkR BnÆu
Æ˚[‹Ls GkR A±ÆVp TVuTÙh•tœm TVuT”jR G]dœ R˚P´p˚X. G]dœ CRtœ
ÿuTÙL BnÆu RLYp T•Ym ˘LÙ”dLlThP’. G]dœ CkR BnÆp Teœ˘T\ ÿ›
NmURm.
BnÆu ˘TVo :
•¥hPp F”Lßo ÍXm HtT”m Àu Utflm ß—dL∞u UÙt\eL˚[
Jl©h” TÙojRp.
œ±l◊ Gi :
˘TVo :
ÿLY¨ :
˘RÙ˚X˙T£ Gi : ˚L˘VÙlTm
NÙh£ : 1
2
CPm :
˙Rß :

CASE RECORD FORM
Date of examination: OP File no.:
Personal details:
1. Name : 2. Age: 3. Sex: 4. Educational status: 5. Occupation : 6. Income : ( per year)
7. Address:
Ph no:
8. Number of family members: 9. Habits :
Do you? Yes NoSmoke Chew tobacco Alcohol
10. Any systemic diseases?
Disease Yes No On treatment? Diabetic Hypertensive CAD Stroke Hypercholesterolemia TB Hypothyroid BA Epilepsy

11. Presenting complaint:
12. History of presenting complaints:
13. Family history
14. Past history: Do you have? Yes No radiation exposure within one year
prosthetic rehabilitation Pre-malignancy/ malignancy Hospital admissions Any other abnormalities in buccal mucosa
15. General Examination:
Pulse rate
Respiratory rate
Temperature
BP
JVP
Signs of Yes No Pallor Jaundice Cyanosis Clubbing Pedal oedema Regional lymphadenopathy

Local examination: Any abnormalities in Yes No Gingiva Buccal mucosa Labial mucosa Palate Tongue Floor of the mouth
Check list: Information sheetConsent form Personal details Biopsy number (before radiation)Biopsy number (after radiation)

NO
AGE
SEX
MN BEFORE
MN AFTER
KR BEFORE
KR AFTER
KL BEFORE
KL AFTER
PN BEFORE
PN AFTER
1 21yrs F 4 15 1 4 0 2 5 4 2 20yrs F 2 15 5 9 10 9 10 2 3 23yrs F 3 12 0 6 17 8 3 5 4 21yrs M 1 10 3 5 5 6 11 8 5 21yrs M 0 15 0 8 5 3 8 8 6 20yrs F 5 12 4 4 5 5 7 9 7 19yrs M 1 4 1 0 20 12 4 4 8 20yrs F 4 9 3 12 3 6 9 8 9 24yrs M 2 15 0 10 0 9 9 2
10 23yrs F 0 1 1 1 0 20 3 6 11 21yrs F 2 5 0 3 5 7 1 12 12 24yrs F 2 4 0 2 14 20 0 2 13 20yrs F 3 5 1 1 6 27 2 0 14 21yrs F 2 4 3 2 8 8 4 11 15 23yrs F 0 3 0 0 8 14 5 4 16 20yrs F 0 14 0 4 5 2 7 7 17 24yrs M 1 2 2 3 9 8 7 7 18 24yrs F 0 9 0 2 8 8 3 8 19 20yrs F 4 0 6 2 3 5 5 18 20 21yrs F 2 6 0 3 0 18 5 12 21 21yrs F 4 4 5 3 9 1 3 9 22 20yrs M 0 7 0 3 2 6 5 3 23 23yrs F 0 3 2 1 9 7 6 5 24 21yrs F 3 8 1 2 13 13 1 5 25 24yrs F 3 13 2 4 3 5 10 4 26 23yrs F 5 6 3 1 0 1 13 3 27 23yrs F 11 0 11 9 0 34 5 2 28 24yrs F 9 9 9 0 3 2 5 10 29 23yrs F 7 14 3 2 3 3 2 7 30 20yrs F 1 9 0 0 4 6 16 0 31 21yrs M 1 8 0 17 2 1 7 1 32 27yrs M 3 5 6 4 4 16 5 5 33 27yrs M 3 11 6 0 4 8 5 5 34 21yrs F 2 12 3 4 5 11 3 0 35 22yrs F 3 6 13 1 0 4 6 5 36 22yrs M 3 6 0 7 6 4 7 5 37 22yrs M 4 7 0 4 2 3 4 6 38 23yrs F 1 3 4 1 2 6 4 5 39 20yrs M 2 3 5 2 1 1 1 14 40 20yrs F 0 7 0 1 3 10 2 4 41 24yrs F 3 5 10 4 3 7 3 7 42 23yrs F 2 1 0 0 6 1 14 3 43 22yrs F 0 9 0 10 3 7 2 7 44 21yrs F 2 16 4 3 2 4 2 4 45 22yrs F 4 1 1 6 3 10 2 18 46 23yrs F 1 12 6 3 3 3 10 4 47 22yrs F 2 4 1 0 5 1 6 7 48 23yrs F 2 16 1 11 3 13 2 2 49 23yrs F 3 8 7 6 5 13 4 750 19yrs F 8 2 5 0 1 7 13 11 51 22yrs F 0 11 1 6 0 14 6 8
VALUES OF STUDY

52 23yrs F 2 3 4 3 0 5 0 6 53 23yrs F 1 14 0 6 0 5 8 11 54 23yrs F 1 11 4 3 6 6 7 16 55 24yrs F 2 4 1 0 0 13 13 4 56 23yrs F 1 21 2 0 11 1 7 6 57 20yrs F 0 8 3 0 8 7 5 2 58 19yrs F 1 1 1 3 0 7 18 15 59 20yrs F 1 8 4 0 4 8 10 4 60 20yrs F 1 12 2 4 6 3 11 10 61 20yrs F 2 3 2 3 8 3 5 9 62 20yrs F 1 8 4 5 1 5 14 2 63 23yrs F 0 13 5 3 1 3 4 6 64 20yrs F 0 6 3 6 7 9 8 7 65 25yrs M 3 19 4 6 10 1 10 9 66 20yrs F 3 16 6 7 9 3 14 11 67 20yrs F 1 6 5 2 4 8 18 7 68 20yrs F 6 9 4 3 13 0 10 18 69 20yrs F 2 5 7 0 3 3 21 10 70 20yrs F 0 4 2 1 2 0 4 1 71 19yrs M 0 4 1 2 3 2 23 12 72 23yrs M 2 11 8 0 20 5 2 7 73 23yrs F 1 5 9 7 4 0 2 4 74 22yrs F 7 12 24 4 6 9 3 4 75 20yrs F 2 11 1 0 25 3 0 1 76 20yrs F 2 12 4 3 5 3 8 3 77 20yrs F 3 2 3 4 19 12 2 3 78 23yrs F 4 3 5 0 2 7 4 4 79 22yrs F 2 21 2 0 9 1 6 6 80 21yrs F 0 10 4 2 17 7 1 10 81 21yrs F 2 5 0 1 6 4 8 11 82 20yrs F 2 6 4 4 7 13 4 2 83 23yrs F 1 7 2 2 3 5 3 17 84 23yrs F 1 12 0 6 6 15 4 9 85 23yrs F 3 11 1 8 3 5 4 5 86 23yrs F 2 13 3 0 7 10 2 8 87 23yrs F 2 25 12 14 0 6 4 4 88 23yrs F 2 18 3 5 3 2 4 24 89 22yrs F 1 2 2 1 6 4 2 13 90 19yrs F 1 7 2 5 4 4 2 14 91 19yrs F 1 27 1 4 4 4 6 15 92 21yrs F 2 3 0 5 4 4 6 14 93 22yrs F 3 13 4 7 6 3 8 7 94 19yrs F 2 10 3 3 3 10 8 3 95 22yrs M 0 6 0 5 3 7 5 27 96 19yrs F 0 6 4 5 5 3 5 17 97 19yrs F 2 7 5 7 7 3 3 20 98 20yrs F 2 11 1 9 3 5 7 23 99 19yrs F 0 7 0 3 4 10 4 19
100 20yrs F 1 24 5 9 3 0 3 10 101 20yrs F 3 5 7 3 5 5 4 25 102 22yrs F 0 33 3 0 5 9 6 13 103 22yrs M 0 12 2 7 2 3 8 9 104 22yrs F 2 25 1 2 3 4 4 0

105 21yrs F 1 6 6 2 13 5 14 3 106 23yrs M 1 13 0 5 1 5 15 3 107 23yrs F 0 19 3 2 12 2 3 3 108 28yrs F 0 10 5 2 2 3 6 2 109 23yrs F 2 12 0 2 4 2 7 3 110 22yrs F 0 22 3 3 2 2 7 3 111 22yrs F 0 3 1 3 5 8 13 4 112 23yrs F 0 32 2 2 5 2 6 5 113 19yrs F 2 11 5 2 7 2 12 6 114 19yrs M 0 10 4 2 10 1 9 4 115 20yrs M 5 4 4 1 0 1 8 4 116 20yrs F 1 5 1 0 4 6 5 4 117 22yrs M 1 31 3 0 3 3 7 3 118 20yrs M 0 9 2 2 4 10 3 10 119 20yrs F 3 13 0 2 1 0 7 3 120 24yrs F 0 3 4 2 7 22 4 2 121 21yrs F 1 6 0 4 2 6 10 36 122 20yrs F 3 12 3 0 5 1 0 7 123 19yrs F 0 21 2 7 3 9 9 12 124 23yrs F 0 18 5 9 6 2 10 11 125 23yrs F 6 11 6 3 8 4 12 18 126 20yrs F 1 15 3 9 8 12 5 9 127 19yrs F 2 11 2 10 4 7 9 26