Embed Size (px)
Citation preview
ELECTRICAL SHOCK TRAUMA
Colin McFaul, PhD, Mei Li, MD, Ze Liang, and Raphael C. Lee, MD, ScD
Chicago Electrical Trauma Research Institute
Shanghai Power Hospital
Peking Union Medical College
Pritzker School of Medicine, The University of Chicago,
Chicago, Illinois 60637, U.S.A.
KEY WORDS: electrical injury, burn, membrane, electroporation, denaturation, tissue
Shortened Title: Electrical Injury
Send Proofs to: Raphael C. Lee, M.D., Sc.D.Department of Surgery, MC 6035The University of Chicago5841 South Maryland AvenueChicago, IL 60637Phone: (773) 702-6302 Fax: (773) 702-0661e-mail: [email protected]
1
Contents
Contents 2
Introduction 4
Electrical Transport within Tissues 6
Physicochemistry of Tissue Injury 9
Low Frequency Electric Shocks 9
Direct Electric Force Damage. 10
Thermal “Burn” Injury 17
Electro-conformational Denaturation of Transmembrane Proteins 20
Radiofrequency (RF) and Microwave Burns 22
Lightning Injury 23
Common Clinical Syndromes Following Electrical Injury 24
Diagnostic Imaging of Electrical Injury 25
Summary and Conclusions 27
Acknowledgements 28
References 29
2
Introduction
The development of electrical power has been one of the most impactful engineering feats of
modern humanity. As electric power penetrates further into society, it poses greater risk to
human society in terms of safety. Many citizens have experienced electric shock at least once in
their lifetime. The pain and fear generated from encounters with electricity usually prevents us
from further tampering with such a dangerous force. However, no matter how careful, accidents
can and do occur, especially among electrical workers who handle commercial electrical power
lines every day. Recently, use of electrical power in non-lethal weapons carried by law
enforcement has made it into the mainstream in some countries. The purpose of this chapter is to
provide a basic overview of the harmful effects of electrical force from both the engineering and
medical perspectives.
The range of clinical manifestations of electrical shock is not well documented. Many survivors
of accidental electrical shock never seek medical attention. The data that exists is from those who
do seek attention or from a few case studies of electrical workers. Furthermore, there is
considerable variation in how electrical injury and safety is managed across various countries. In
industrializing countries safety practices are often not the top priority, resulting in high rates of
injury. A study of burn injuries by Nursal et al. during a one-year (2000-2001) period indicated
that 21% of burn patients were victims of electrical injury (1). In highly industrialized nations,
electrical shock rates are on the decline. In the United States, electrocution remains the fifth
leading cause of fatal occupational injury with an estimated economic impact of more than 1
billion dollars annually (2). The rates of injury are highest among electrical workers, mostly
3
caused by ‘live’ electrical equipment, such as wiring, light fixtures, and overhead power lines
(3). A study in Virginia suggested that public utilities have the highest rate of fatal electrical
injuries among all industrial sectors. More than 90% of these injuries occur in men, mostly
between the ages of 20 and 34, with 4 to 8 years of experience on the job (4). Another study
found that the average age of victims was 37.5 years and the average experience was 11.3 years.
In yet another study, the incidence in a 9-year period was 8.3%, 96% of victims were male, and
the mean age was 32.7 years (5). For survivors, the injury pattern is very complex, with a high
disability rate due to accompanying neurologic damages and/or loss of limbs.
Away from the workplace, most electrical injuries are due to either indoor household low-
voltage (<1000 V) electrical contact or outdoor lightning strikes (6). An etiology study
conducted in India reveals that 60% of high-voltage electric burns were due to exposed electric
wires on farm or agricultural land, while low-voltage electric shocks happened mainly at home
(47%) and at professional utility places (29%) (3). Domestic household 60 Hz electrical shocks
are common and usually result in minor peripheral neurological symptoms or occasionally skin
surface burns. However, more complex injuries may result depending on the current path,
particularly following oral contact with household appliance cord disclosures or outlets by small
children (6). Compared to a high-voltage shock that is usually mediated by an arc, low-voltage
shocks are more likely to produce a prolonged, “no-let-go” contact with the power source. This
“no-let-go” phenomenon is caused by an involuntary, current-induced, muscle spasm (7). For
60 Hz electrical current, the “no-let-go” threshold for axial current passage through the forearm
is 16 mA for males and 11 mA for females (7,8).
There are roughly 30 human deaths annually in the United States due to lightning strikes and
approximately ten times that number of injuries (9,10). The range of lightning injury extent is
4
quite broad, depending upon the magnitude of exposure and the condition of the victim. Usually
lightning hits result in surface burns, complex neurological damage similar to blunt head trauma,
peripheral neurologic injury, and cardiac damage (11). Radiofrequency and microwave injuries
are less common. Nonetheless, they represent an important medical problem to understand. At
higher frequencies, when the wavelength is short enough to couple at the atomic level, the fields
can be ionizing as well as can cause molecular heating. Electrical trauma may produce such
complex patterns of injury because of variations in the source of the electricity, differences in
tissue-current interactions by electrical frequency, the variation in current density along its
pathway through the body, and variations in body size, body position and use of protective gear.
No two cases are the same.
Electrical Transport within Tissues
The fundamental bioengineering perspective is that the human body is considered to be a
compartmentalized (or lumped element) conducting dielectric. It consists of about 60% water by
weight: 33% intracellular and 27% extracellular (12). Body fluid in both the intracellular and
extracellular compartments is highly electrolytic, and these two compartments are separated by a
relatively impermeable, highly resistive plasma membrane. Current within the body is carried by
mobile ions in the body fluid. The concentration of mobile ions results in a conductivity of
approximately 1.4 S m-1 in physiological saline. While electrons are the charge carriers in
metallic conductors or electrical arcs, in the human body the charge carriers are ions. The
conversion from one to the other occurs at the skin surface through electrochemical reactions
(13).
5
At low frequencies (i.e., below radio frequencies), the electric current passing across the body
distributes such that the electric field strength is nearly uniform throughout any plane
perpendicular to the current path (14–16). As a consequence, the current density distribution
depends on the relative electrical conductivity of various tissues and the frequency of the current.
Experimental data support this basic concept. Sances et al. measured the current distribution in
the hind limb of anesthetized hogs (16). They found that major arteries and nerves experienced
the largest current density because of their higher conductivity. It was also observed that skeletal
muscles carried the majority of the current due to their predominant volumetric proportions.
At a macroscopic scale, upper limbs are mostly involved in electric shocks, especially the right
upper limb, as would be expected from dominant hand interactions with electrical sources (17).
Cela et al. modeled this using a multiresolution admittance method. In this method, a human arm
was initially split into uniformly-sized voxels. Within regions of uniform composition, voxels
were combined, greatly reducing the number of voxels in the model. Fine resolution was
maintained at material boundaries (18). The voxels were then connected as a network of
conductors, allowing the calculation of current density at each voxel. This model was applied to
predict the damage in skeletal muscle caused by cell lysis, and to simulate the injury pattern. The
simulation found that current density increases towards the distal part of the arm as the cross
sectional area decreases. The wrist has particularly high current density and damage due to the
constriction and the high fraction of less conductive bone. The overall impedance of this arm
model is 599 Ω, which is consistent with the estimated resistance of the human body (18).
Computational models of human high-voltage electrical shock suggest that the induced tissue
electric field strength in the extremities is high enough to electroporate skeletal muscle and
6
peripheral nerve cell membranes (19–22) and to possibly cause electroconformational
denaturation of membrane proteins.
At a more microscopic scale, low frequency current distribution within tissue is determined by
the density, shape and size of cells. The cell membrane acts as an insulating ion transport barrier
that mostly shields the cytoplasmic fluid from low frequency electrical current. In addition, the
presence of cells diminishes the area available for ionic current and, in effect, makes tissues less
conductive. As cell size increases, the membrane has less impact on a cell’s electrical properties,
because the volume fraction of the cell occupied by the membrane is inversely proportional to
the total cell radius (23). Similarly, the conductivity of skeletal muscle parallel to the long axis of
the muscle cells is greater than that perpendicular to this axis. Solid volume fraction of the
extracellular matrix can also be important in certain tissues and anatomic locations. For example,
the resistivity of cortical bone and epidermis is higher than other tissues because their free water
content is lower, as evidenced in the recent work by Kalkan et al. (24).
At higher frequencies, in RF and microwave ranges, the current distribution is dependent on
different parameters. The cell membrane is no longer an effective barrier to current passage, and
capacitive coupling of power across the membrane readily permits current passage into the
cytoplasm. Frequency-dependent factors like energy absorption and skin-depth effects govern
the field distribution in tissues. At the highest frequency ranges, including light and shorter
wavelengths, other effects such as scattering and quantum absorption effects become important
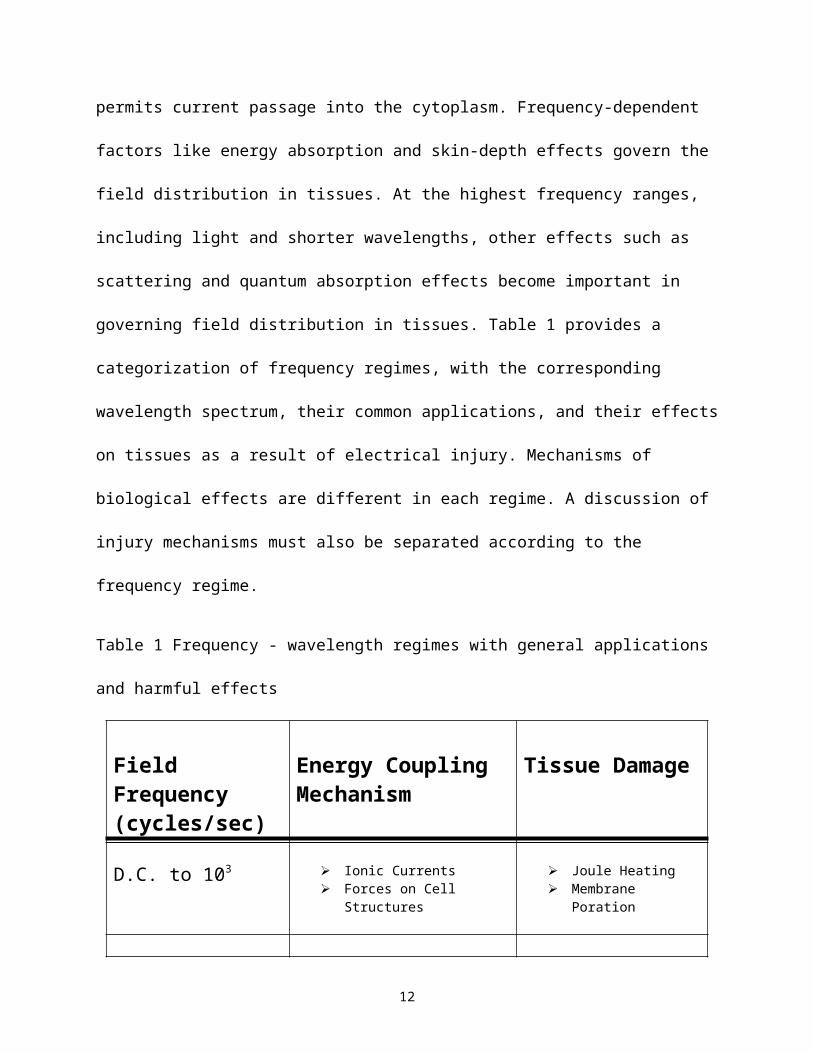
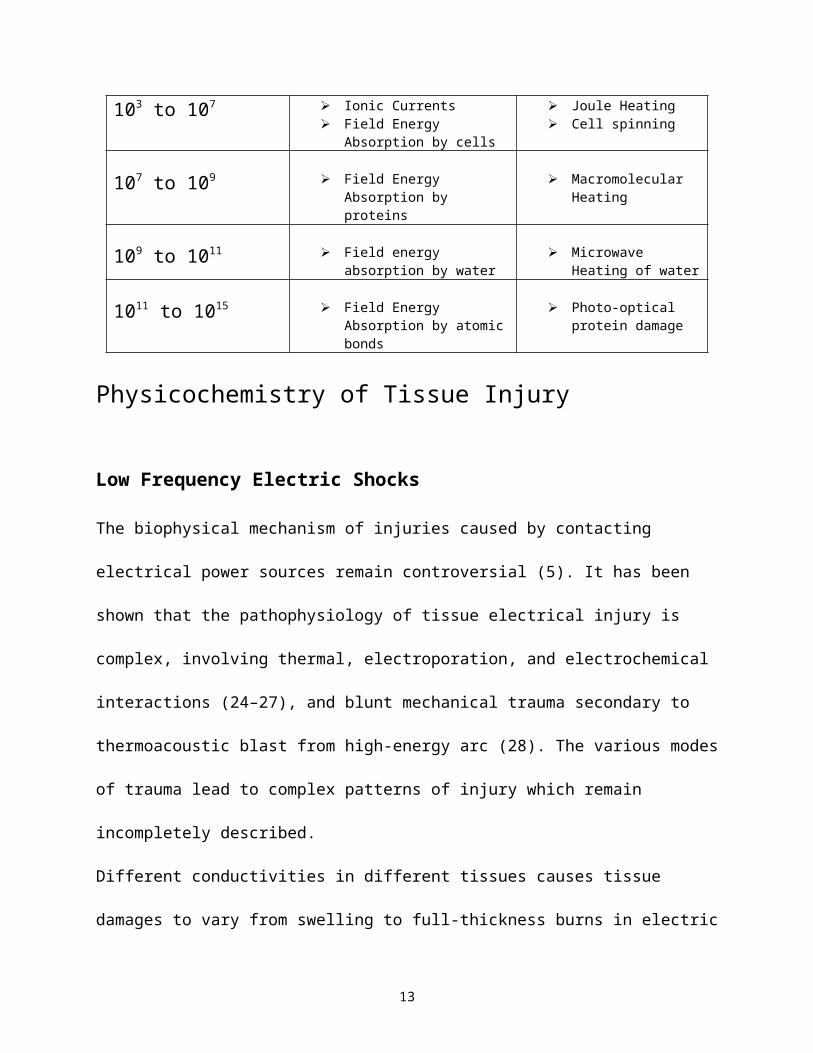
in governing field distribution in tissues. Table 1 provides a categorization of frequency regimes,
with the corresponding wavelength spectrum, their common applications, and their effects on
tissues as a result of electrical injury. Mechanisms of biological effects are different in each
7
regime. A discussion of injury mechanisms must also be separated according to the frequency
regime.
Table 1 Frequency - wavelength regimes with general applications and harmful effects
Field Frequency(cycles/sec)
Energy Coupling Mechanism
Tissue Damage
D.C. to 103 Ionic Currents Forces on Cell Structures
Joule Heating Membrane Poration
103 to 107 Ionic Currents Field Energy Absorption by
cells
Joule Heating Cell spinning
107 to 109 Field Energy Absorption by proteins
Macromolecular Heating
109 to 1011 Field energy absorption by water
Microwave Heating of water
1011 to 1015 Field Energy Absorption by atomic bonds
Photo-optical protein damage
Physicochemistry of Tissue Injury
Low Frequency Electric Shocks
The biophysical mechanism of injuries caused by contacting electrical power sources remain
controversial (5). It has been shown that the pathophysiology of tissue electrical injury is
complex, involving thermal, electroporation, and electrochemical interactions (24–27), and blunt
mechanical trauma secondary to thermoacoustic blast from high-energy arc (28). The various
modes of trauma lead to complex patterns of injury which remain incompletely described.
8
Different conductivities in different tissues causes tissue damages to vary from swelling to full-
thickness burns in electric shock. According to Ohm’s law, tissue damage in electric shock
shows typical patterns in which tissues with higher conductivity presenting more severe clinical
outcomes. Nerves, blood, mucous membranes, and muscles or moist hands possess the lowest
resistance in the human body. Thus the appearance may not reflect the situations of patients
properly; internal injuries can be severe, even when skin burns seem moderate. It is worth
mentioning one unique complication of electric shock: rhythmic disturbances of the heart.
Cardiac muscles are specialized smooth muscles that contract constantly. This synchronization of
muscle movement is governed by the sinus node, a group of cells within the heart that
spontaneously produce electrical impulses. A current of more than 50–100 mA can disturb these
impulses and develop ventricular fibrillation.
The understanding of electric injuries has deepened from simple burns by Joule heating to
complicated models of cell damages. These new concepts are helping physicians with better
management of electrical injury patients (29). In the most general terms, tissue damage exists
when proteins and other biomolecules, cellular organelle membranes or water content is altered.
Among all the components of the cells and tissues which can be damaged by an electrical shock,
it is the thin cell membrane which has the greatest vulnerability. Thus, the cell membrane
appears to be most important determinate of tissue injury accumulation.
The most important function of the cell membrane is to provide a diffusion barrier against free
ion diffusion (30). Because most metabolic energy of mammalian cells is used in maintaining
transmembrane ionic concentration differences (31), the importance of the structural integrity of
the lipid bilayer is apparent. The conductance of electropermeabilized membranes may increase
by several orders of magnitude. ATP production and in turn, ATP-fueled protein ionic pumps,
9
cannot keep pace, leading to metabolic energy exhaustion. Cell necrosis results if the membrane
is not sealed. Thus, in discussing tissue injury resulting from electrical shock, the principal focus
is directed at kinetics of cell membrane injury and the reversibility of that process. A simulation
study of membranes by Tarek (32) explains the electroporation phenomena in bilayers.
Direct Electric Force Damage.A cell within an applied DC or low-frequency electric field will experience electric forces which
will act most forcefully across and along the surface of the cell membrane. The forces acting
across the membrane can alter membrane protein conformation and disrupt the structural
integrity of the lipid bilayer. The magnitude of the forces acting across the membrane is related
to the induced transmembrane potential Vm. Vm depends on a variety of factors, such as the intra-
and extracellular medium conductivity, cell shape and size, the external electric field strength E
as well as how the electric field vector orients with respect to the point of interest on the cell
membrane (22–24).
Given that most cells are either somewhat spheroidal or cylindrical in shape, the relationship
between the externally applied electric field and the induced transmembrane potential can be
simplified to either of two simple forms. Under physiologic tissue conditions, the peak
magnitude of induced transmembrane potential Vm (VPm) at the electrode-facing poles of spherical
cells can be expressed as:
V pm = 1.5 Rcell cos (· (1+(f / fs)2)-1/2 · Epeak, (1)
Where Rcell is the radius of the cell, Epeak is the peak field strength in the tissue surrounding the
cell, is the angle off axis from the field direction, fs is the sub--dispersion frequency limit
below which the cell charging time is short compared to rate of field change, and f is the field
10
frequency (23). For cylindrical shaped cells, such as skeletal muscle and nerve cells, aligned in
the direction of the field (herein assigned the z coordinate), the induced transmembrane potential
takes a different form. Under these circumstances an electrical space constant parameter
becomes useful in describing the electrical properties of the cell. The induced transmembrane
potential can be expressed as a function of z:
Vpm (z) A m sinh (z / m) (1+(f / fs)2)-1/2 Epeak (2)
Where m is the electrical space constant of the cell, A is a variable that depends on cell length,
the position z = 0 corresponds to the mid-point of the cell (34). The bottom of Figure 1 illustrates
schematically the spatial variation of Vpm (z) on the cell size for both of these cases. Of course,
physically larger cells like skeletal muscle and peripheral nerve oriented in the direction of the
electrical field would experience an induced transmembrane potential of greater magnitude than
smaller cells.
Under normal physiological conditions, the cell’s outer plasma membrane is an electrical
transport barrier, restricting current passage through the cell. That leads to an induced
transmembrane potential (23). Thus larger cells are more vulnerable to membrane disruption by
electrical shock current.
Equations (1) and (2) are valid as long as the electrical properties of the cell membrane remain
constant. The natural transmembrane potential of mammalian cells has a magnitude of less than
100 mV (36). When an extracellular imposed electric field results in an induced transmembrane
potential difference magnitude of greater than 200-300 mV across a mammalian cell membrane,
molecular alterations occur that can lead to membrane disruption with subsequent loss of
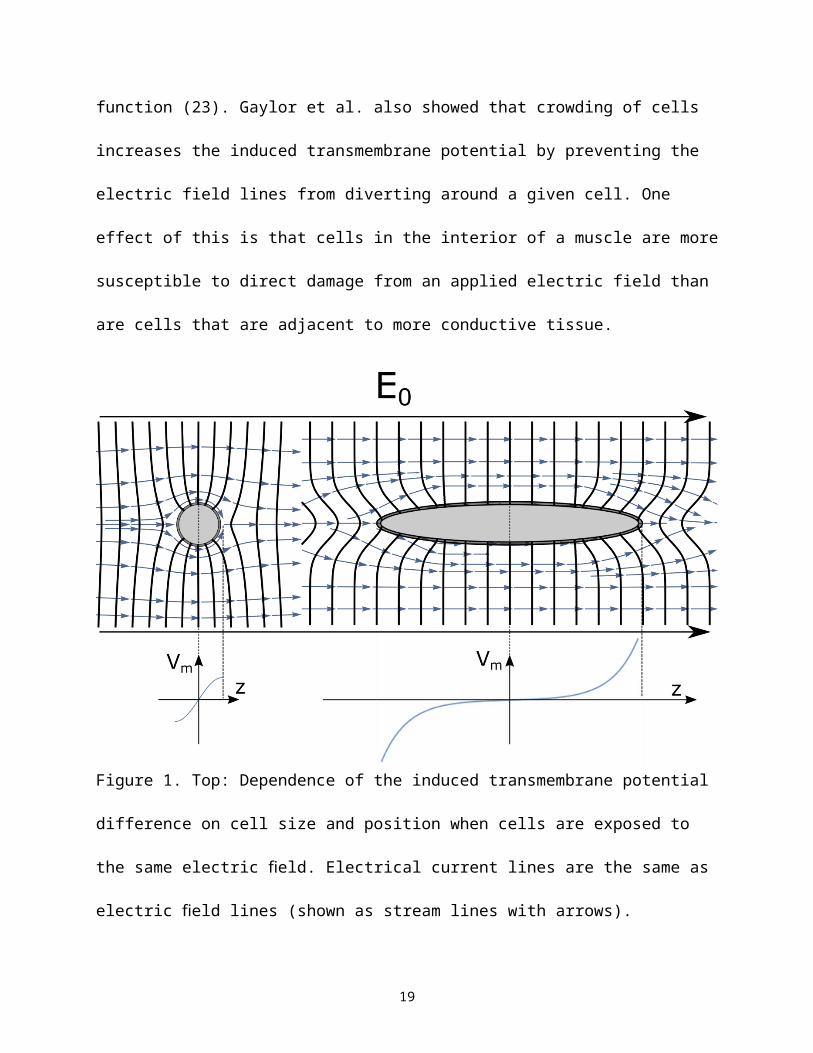
membrane transport barrier function (23). Gaylor et al. also showed that crowding of cells
11
increases the induced transmembrane potential by preventing the electric field lines from
diverting around a given cell. One effect of this is that cells in the interior of a muscle are more
susceptible to direct damage from an applied electric field than are cells that are adjacent to more
conductive tissue.
Figure 1. Top: Dependence of the induced transmembrane potential difference on cell size and
position when cells are exposed to the same electric field. Electrical current lines are the same as
electric field lines (shown as stream lines with arrows). Constant voltage lines are shown in
darker color without arrows. Bottom: the transmembrane potential difference as a function of
position along the direction of the applied electric field. The longer cell has a much larger
transmembrane potential at its ends than the shorter cell.
12
The principal mechanisms of damage are electroporation of the lipid bilayer and electro-
conformational denaturation of the membrane proteins. Electro-conformational damage to
membrane proteins has been well documented for voltage-gated membrane protein channels
(37,38). The processes occur quickly, on the order of milliseconds, after strong fields are applied.
Electroporation is the biophysical process of cell membrane disruption resulting from an
electrical field in the plasma membrane of such magnitude that re-ordering of lipids in the lipid
bilayer takes place (33,37,38). Investigation of electroporation of many cells within a tissue was
initially driven by the need for a better understanding of the pathophysiology of electrical injury
(39–41). In the early 90’s, it was studied in connection with cardiac defibrillation shocks (42,43).
More recently, tissue electroporation has begun to be envisioned as a potential therapeutic tool in
the medical field. It has found useful applications at both the single and multicellular level in 1)
enhanced cancer tumor chemotherapy (electrochemotherapy, (44,45); 2) localized gene therapy
((46,47); 3) transdermal drug delivery and body fluid sampling (48–50); 4) introduction of
foreign DNA into cells; 5) introduction of enzymes, antibodies, viruses, and other agents or
particles for intracellular assays; 6) cell fusion; 7) to insert or embed macromolecules into the
cell membrane; 8) to sample microenvironments across membranes (51); 9) gene delivery in
human embryonic stem cells (52), gene transfer in whole embryos (53) and gene repair in
mammalian cells (54). Recent reviews and books published have extensively treated this subject
(33–35,50,55–58).
The process of cell membrane electroporation can be simulated as a chemical reaction that
involves the rearrangement of phospholipids in the bilayer portion of the cell membrane. Bier et
al. constructed a thermodynamic model of this process. It is driven by energy differences of the
minimum energy state in pore formation and the bilayer state equaling the line tension minus the
13
Kelvin Polarization stresses within the defect. This leads to an estimate of pore radius of
0.36 nm, consistent with previous reports (59).
Whether cells survive electroporation depends on whether the defects are transient or stable.
Stability of defects is governed by the magnitude of the imposed transmembrane potential, the
duration for which it is imposed, membrane composition and the membrane temperature. The
time required to electroporate a cell is also dependent on these same variables and typically
ranges from tens of microseconds to milliseconds. After application of a brief electroporating
field pulse, the transiently electroporated membrane will spontaneously seal. Sealing follows
removal of water from the membrane defects. Sealing kinetics are often orders of magnitude
slower than the field relaxation because the forces driving the molecular sealing events are not as
strong as those caused by the electroporating electric field. Sealing of electropores requires
reordering of membrane lipids and removal of water molecules from the pore, both time and
energy consuming processes (44–46).
The threshold transmembrane potential for induction of membrane electroporation is remarkably
similar across cell types. The threshold Vm for electroporation has been found to be in the range
300-350 mV (60–63). Several authors have developed models to explain the experimentally
observed values of Vm required for electroporation and associated transmembrane aqueous
dynamics (40,64). Using empirical data as parameters in an asymptotic approximation (39), the
threshold Vm is predicted to be approximately 250 mV, consistent with reported experimental
data.
Generally, for most media-suspended, isolated cells with a typical diameter of 10 - 20 µm, the
DC field strength threshold for electroporation is in the range of 1 kV cm-1. By comparison, the
fields required to alter large cells are much less. Due to their relatively long length, skeletal
14
muscle cells, up to 8 cm long in large animals, and nerve cells, up to 2 m long, have much lower
electroporation thresholds. Therefore, muscle and nerve cell membranes are likely to be damaged
with electrical fields as small as 60 V cm-1.
The distribution of electropore formation in a cell placed in an applied field was addressed by
DeBruin and Krassowska (65,66). Expanding from previous theoretical models, and including
the fact that the membrane charging time of about 1 µs is very short compared to a 1 ms field
duration, they concluded that supraphysiological Vm at the pole caps is large enough to create
pores, and thereby effectively prevent a further increase in Vm in these areas. This confirms early
experimental findings which show a saturation of Vm that is independent of the field strength for
high-voltage shocks (52–54). After the effect of ionic concentrations is included, DeBruin and
Krassowska’s model is able to confirm asymmetries in Vm observed in respect to the
hyperpolarized (anode-facing) and hypopolarized (cathode-facing) pole of a cell (61,62,70).
Although the pore sealing time in the range of seconds predicted by the model is in agreement
with some published experimental results (71), others have found longer sealing times in the
range of several minutes (60,61,72). This might be explained by the fact that: 1) this model is
based on pure lipid bilayers instead of cell membranes embedded with proteins, and 2) it only
considers primary pores formed by Vm during the shock and not the secondary pores formed after
the external field pulse ends, that provide transport routes for macromolecules.
Bhatt et al measured electroporation damage accumulation using isolated, cooled in vitro rat
biceps femoris muscles (25). After the initial impedance measurement, an electric field pulse was
delivered to the muscle creating tissue field pulse amplitudes ranging between 30-120 V cm-1, in
the range of typical forearm field strengths in high-voltage electrical shock. The duration of the
DC pulses ranged from 0.5-10 ms. These short pulses reduce Joule heating to insignificant
15
levels. Field pulses were separated by 10 s to allow thermal relaxation. The drop in the low
frequency electrical impedance in the muscle tissue following the application of short-duration
DC pulses indicated skeletal muscle membrane damage. A decrease in muscle impedance
magnitude occurs following DC electric field pulses that exceed 60 V cm-1 magnitude and 1 ms
duration. These results indicate that the field strength, pulse duration, and number of pulses are
all factors that determine the extent of electroporation damage.
Based on these results, Block et al. (27) electrically shocked fully anesthetized female Sprague-
Dawley rats through cuff-type electrodes wrapped around the base of the tail and one ankle using
a current-regulated DC power supply. The objective was to determine whether electroporation of
skeletal muscle tissue in-situ could lead to substantial necrosis. The study involved
histopathological analysis and diagnostic imaging of an anesthetized animal hind limb. A series
of 4 ms DC-current pulses, each separated by 10 s to allow complete thermal relaxation back to
baseline temperature before the next field pulse, was applied. The electric field strength
produced in the thigh muscle was estimated to range from 37-150 V cm-1, corresponding to
applied currents ranging from 0.5 – 2 A. These tissue fields were suggested to be on the same
level as that experienced by many victims of high-voltage electrical shock. Muscle biopsies were
obtained from the injured as well as the collateral control legs six hours post shock, and
subjected to histopathological analysis. Sections of electrically shocked muscle revealed
extensive vacuolization and hypercontraction-induced degeneration band patterns which were
not found in un-shocked contra-lateral controls (Figure 2 of (27)). The fraction of
hypercontracted muscle cells increased with the number of applied pulses. These results are
consistent with the investigators’ hypothesis that non-thermal electrical effects alone can induce
cellular necrosis. The pathologic appearance of the shocked muscle was similar to that seen in
16
malignant hyperthermia, indicating that electroporation may lead to Ca2+-influx into the
sarcoplasm. A similar muscle injury pattern has been described in a human electrical injury
victim published by deBono in a clinical case report (73). These results suggested that direct
electrical injury of skeletal muscle in-situ can lead to the commonly seen pattern of injury in
electrical shock victims even in the absence of pathologically significant Joule heating.
Thermal “Burn” Injury Passage of electrical current through electrically conducting media leads to Joule heating that can
lead to severe burn injury in electrical shock victims. Burn injury is used here to specifically
refer to tissue injury by damaging supraphysiological temperatures. Burn effects are related to
lysis of cell membranes and protein denaturation often followed by recognizable changes in the
optical properties of tissue. There are two different potential outcomes for the denatured protein,
which depend on the initial molecular structure and configuration. The first occurs when the
native folded conformational state of the protein, held by intra-molecular bonds, is different from
the most favored conformation without intramolecular bonds (the thermodynamically lowest
energy level). When this protein is heated, the intramolecular bonds are broken and it denatures
to one of several preferred lower energy states from which it will not spontaneously return to the
native conformation. Conceivably, if the primary structure of the protein is undamaged it may be
plausible to reconfigure the protein using chaperone-assisted mechanisms similar to those which
establish its initial folding after biosynthesis. The second possibility occurs when the native
folded state of the protein is the same as the most energetically preferred conformation in the
absence of intramolecular crosslinks. In this case, the protein is able to spontaneously refold to
its native state.
17
The speed of the transition from natural to denatured states is governed by the Arrhenius rate
equation which states that when the kinetic energy of the molecule exceeds a threshold
magnitude Eia (for activation energy), the transition to the ith state will occur (in this case from
natural to denatured state). For a large number of molecules at temperature T the fraction Γ with
a kinetic energy above Ea is governed by the Maxwell-Boltzmann relation (65),
Γi = exp(-Eia / kBT) (4)
where kB is Boltzmann's constant. Because the strength of bonds retaining the folding
conformation of macromolecules is dependent on the nature of the chemical bond, the value of
Eia is dependent on molecular structure. Despite this complexity the net rate of denaturation of
cellular structures containing many different proteins is also often describable in terms of
Equation 4. For example, the accuracy of this equation in describing thermal damage to cell
membranes has been reported to be reasonable (74–76). Even the thermal injury to intact tissues
like human skin is reasonably described by the simple Equation 4. It has been known for more
than 50 years that the rate at which damage accumulates in heated skin can be estimated by
convolving Equation 4 with the temperature history. The resulting expression is called the "heat
damage" equation (77),
d / dt = A (5)
where Ω is a parameter reflective of the extent of damage, and A is a frequency factor that
describes how often a configuration from which reaction is energetically possible occurs, which
is also dependent on molecular structure. The shape of the temperature-time curve predicted by
Equation 5 is the same as the human skin temperature vs. time scald burn curve measured by
18
Henriques and Moritz (78). This temperature-time curve shape has also been obtained for heat
damage to isolated cells (76).
Because the lipid bilayer components of the cell membranes are held together only by forces of
hydration, the lipid bilayer is the most vulnerable to heat damage (79). Even at temperatures of
only 6°C above normal (i.e. 43°C) the structural integrity of the lipid bilayer is lost (80). In
effect, the warmed lipid bilayer goes into solution, rendering the membrane freely permeable to
small ions. At slightly higher temperatures, published reports indicate that the contractile
mechanism of muscle cells is destroyed immediately following exposure to 45°C and above (81).
Experiments on fibroblasts demonstrated that heat-induced membrane permeabilization also
begins to appear above 45°C (82).
Bischof et al investigated the effect of supraphysiological temperatures on isolated rat muscle
cells using a thermally controlled microperfusion stage (83). Cells were loaded with the
membrane permeable fluorescent dye precursor calcein-AM. After entering the cell, the
precursor is converted by nonspecific esterases into the membrane impermeable fluorescent
Calcein. Using quantitative fluorescent microscopy, these authors measured time-resolved dye
leakage from the muscle cells at several supraphysiological temperatures. In addition, using
Equations 4 and 5, the authors determined the activation energy necessary to thermally induce
membrane permeabilization in the isolated muscle cells to be 32.9 kcal mol-1 (83). Reported
activation energy values for thermal damage in other cell types are in the range from
30 – 140 kcal mol-1 (76).
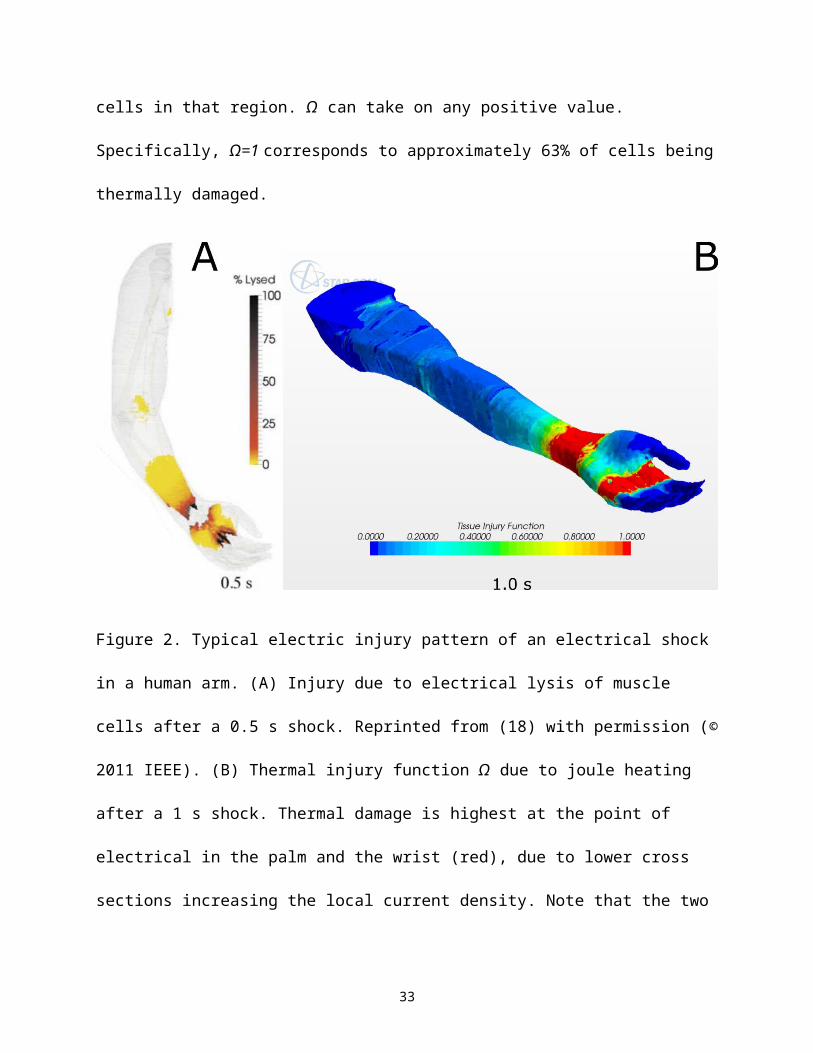
Figure 2 illustrates the difference between electroporation damage and thermal damage. Panel A
shows the development of electrical lysis of cells in the muscle caused by a model shock (18). In
19
this case, a 0.5 s, 4.5 kV alternating current shock was applied between the palm and the
shoulder, modeling a worst-case scenario 10 kV shock between the hands. Panel B shows the
thermal injury function Ω resulting from a similar 1 s model shock. Joule heating is highest in the
regions of highest current density. These are the regions where the current is constrained to a
smaller cross section area. The most notable such regions are the wrist and the point of electrical
contact (the palm in this case). Figure 2 shows the difference between electroporation and
thermal damage: regions that show no thermal damage can show electroporation damage, and
regions that show significant thermal damage can show little to no electroporation injury. It is
important to point out that a thermal injury function value Ω=1 in a given region does not
correspond to thermal injury of all cells in that region. Ω can take on any positive value.
Specifically, Ω=1 corresponds to approximately 63% of cells being thermally damaged.
Figure 2. Typical electric injury pattern of an electrical shock in a human arm. (A) Injury due to
electrical lysis of muscle cells after a 0.5 s shock. Reprinted from (18) with permission (© 2011
20
IEEE). (B) Thermal injury function Ω due to joule heating after a 1 s shock. Thermal damage is
highest at the point of electrical in the palm and the wrist (red), due to lower cross sections
increasing the local current density. Note that the two damage scales are not directly comparable,
because a value of Ω=1 does not correspond to injury of all cells in that volume.
Electro-conformational Denaturation of Transmembrane Proteins Imposed supraphysiologic transmembrane potential differences can produce
electroconformational changes of membrane proteins, ion channels, and ion pumps.
Approximately 30% of cell membrane consists of proteins, some of them embedded into the
bilayer, others spanning across the entire membrane. Many of them carry electric charges from
amino acids with acidic or basic side groups that can be acted on directly by an intense Vm
(charge separation or charge induction through dissociation). In addition, each amino acid has an
electrical dipole moment of about 3.5 D (1 Debye = 3.336×10-30 C m) giving the proteins an
overall dipole moment that, in the case of an -helical protein structure, can reach 120 D (84). In
a strong external electric field those molecules will orient themselves and thereby change their
conformation to increase the effective dipole moment in the direction of that field.
If the field strength becomes sufficiently intense, those field-induced changes can cause
irreversible damage to membrane proteins. In particular ion channels and pumps with their
selective voltage-gated charge transport mechanisms (e.g., Ca2+ specific channel) are highly
sensitive to differences in Vm. Chen et al. investigated the effects of large magnitude Vm pulses
on voltage-gated Na+ and K+ channel behavior in frog skeletal muscle membrane using a
modified double vaseline-gap voltage clamp. They found in both channel types, but more
drastically in K+ channels, reductions of channel conductance and ionic selectivity by the
21
imposed Vm (37). Further, these authors were able to demonstrate that these changes are not
caused by the field-induced channel currents (Joule heating damage) but rather by the magnitude
and polarity of the imposed Vm (85). In the most recent work, Clausen et al. (86) studied the
effects of shock and electroporation on the acute loss of force in skeletal muscles and the role of
the Na+ and K+ pumps in the force recovery after electroporation. Ionic pumps alone are
sufficient to compensate a simple mechanical leakage. They report that electroporation induces
reversible depolarization, partial rundown of Na+, K+ gradients, cell membrane leakage and loss
of force. The consequences of this effect may underlie the transient nerve and muscle paralysis in
electrical injury victims.
Radiofrequency (RF) and Microwave Burns
Every year a few cases of RF (radio frequency) or microwave field injuries require medical
attention in the United States. The victims are usually industrial workers. Above the low
frequency regime (>10 kHz), tissue response strongly depends upon the field frequency. In the
10 - 100 MHz RF range, two types of tissue heating occur, Joule and dielectric heating, with
Joule heating outweighing dielectric heating. Small molecules like water, when not bound, are
able to follow the field up to the gigahertz range (87). However, at microwave frequencies
(100 MHz - 100 GHz), dielectric heating is more significant than Joule heating because both
bound and free water is excited by microwave radiation. Molecular dipoles of macromolecules
have lower natural frequencies, so that their most efficient induction frequency is in the
radiofrequency range.
Exposure to ambient microwave fields is known to cause burn trauma. Microwave burns have
different clinical manifestations than low frequency electrical shocks (88–91). At low frequency,
22
the epidermis is a highly resistive barrier, whereas in the microwave regime, electrical power
readily passes the epidermis in the form of capacitive coupling with very little energy
dissipation. Consequently, the epidermis may not be burned unless it is very moist. The
microwave field penetration into tissue has a characteristic depth in the range of 1 cm, resulting
in direct heating of sub-epidermal tissue water. The rate of tissue heating is dependent not only
on the amplitude of tissue electric field, but also on the density of dipoles. For example,
microwave heating is much slower in fatty tissues (91,92).
Lightning Injury
Lightning arcs result from dielectric breakdown in air caused by buildup of free electrical
charges on the surface of clouds. The current through an arc can be enormous, but the duration is
quite brief (1 - 10 ms). The primary current is confined to the surface of conducting objects
connected by the arc. Peak lightning current range between 30,000 - 50,000 A, which is able to
generate temperatures near 30,000 K. This abrupt heating generates a high-pressure
thermoacoustic blast wave known as thunder.
An individual directly struck by lightning will experience current for a brief period of time.
Initially, the surface of the body is charged by the high electric field in the air. This can cause
breakdown of the epidermis, and several hundred amperes to flow through the body for a
1 - 10 µs period, which is long enough to induce electroporation. Following this, a much smaller
current persists for several milliseconds, in which time the body is discharging into the ground.
The duration of current flow is relatively short, so there is no substantial heating except a
breakdown of the epidermis. However, disruption of cell membrane can wreak havoc on nerve
and muscle tissues.
23
When lightning reaches the ground, it spreads out radially from the contact point. A substantial
shock current can be experienced by a person walking nearby, if their feet are widely separated.
For example, with an average lightning current of 20,000 A, a step length of 50 cm, and an
individual located 10 m away from strike point, the voltage drops between the legs can reach
1500 V. This can induce a 2 - 3 A current flow through the body between the legs for a 10 µs
period.
Common Clinical Syndromes Following Electrical Injury
Clinical manifestations of electrical shock depend on the magnitude, frequency and duration of
the imposed fields within the tissues that exist in the current path through the body. It is no
surprise that workers coming in contact with high energy industrial electrical power sources
experience rapid Joule heating of tissues throughout the current path. Total thermal destruction
of tissues throughout the current path can result. Because of the high heat capacity of water,
thermal injury dynamics accrue on a time frame of seconds in most cases. With more rapid
kinetics, electroporation of tissues, especially skeletal muscle and peripheral nerve can occur.
Brief accidental electrical shocks involving several hundred volts are common among
electricians and others working with electrical power. This may not result in a large thermal burn
but will result in neuromuscular dysfunction and pain. Electroporation is the most likely
pathophysiologic process linking the neuromuscular dysfunction to the electrical shock. Acute
symptoms most often resolve in a few days. However, many of these shock victims will develop
late generalized musculoskeletal pain, loss of balance control, and neuropsychological
symptoms. Although the precise mechanisms linking a local brief electrical shock to generalized
24
peripheral and central neurological problems remains under investigation, it is clear that this
sequalae is common (93–96).
The most common anatomical contact point with of electrical current is to the arm and hand.
Regarding the pattern of thermal injury, Joule heating is mostly concentrated at the wrist because
of the small cross-sectional area and the lower conductivity of skin and bone. The second skin
burn wound is usually at the flexor aspect of the elbow, and the third at the armpit. As the energy
decreases along the arm, so does the damage. The skin burn wound varies depending on the
condition of the victim when the incident happens. Where the skin is burned along the current
path, the deeper tissues are as well. Patients can suffer from long term rarefaction of bone and
protracted residual wounds for months to years after recovery.
Electrical injury causes damage to the peripheral nerves and spinal cord, which can lead to
cognitive and emotional changes. Patients exhibit lower attention, verbal memory, learning
ability, and executive function, while experiencing higher incidents of depression and poor anger
control. Research shows the relationship with changes in both cerebra and cognitive circuits, for
example including hypermetabolism in the cerebellum-limbic system.
Diagnostic Imaging of Electrical Injury
Because most of the damage caused by electrical shock occurs beneath the skin, it is important to
discuss how to achieve tissue injury detection and localization. There are two basic cellular
abnormalities in electrical injury: altered protein structure and disrupted cell membranes. In
addition, there can be blood coagulation, tissue edema, elevated tissue pressures and other
25
abnormalities that affect molecular transport. From the clinical perspective, it is important to
recognize areas of damaged cells and interrupted blood flow.
Magnetic resonance imaging (MRI) methods are particularly well suited for detection of changes
in protein folding, disruption of cell membranes and tissue edema. Most useful are MRI methods
based upon measurement of water proton behavior. Since water behavior will change in the
presence of denatured proteins, and osmotic swelling will follow disruption of cell membranes,
the typical MRI equipment in hospitals can measure these changes associated with electrical
injury.
Technetium99m-PYP (pyrophosphate) is widely used as a radiolabel tracer for various forms of
soft tissue injury including electrical trauma because it is believed to follow the calcium
movement in cellular function (97). Increased tracer accumulation in muscle tissue indicates loss
of cell membrane integrity, tissue edema and is predictive of tissue injury. The in vivo rat hind
limb electrical injury model described by Block et al. monitored the uptake of Tc99m-PYP in the
electrically shocked tissue as a function of the magnitude of DC current (27). Either 0.5, 1.0 or
1.85 A of direct current was applied to the rat’s hind limb, and compared to intravenous saline
infusions as the sham-treatment. Their results indicated that Tc99m-PYP does accumulate in
electroporated tissue and the level of the tracer accumulation is positively correlated to the tissue
field pulses applied. This indicates that quantitative imaging of Tc99m-PYP uptake may be
developed further as an indicator of the extent of electroporation or other membrane injury.
A recent report by Park et al. measured cerebral blood volume (CBV) of electrical injury patients
(98). In that study, electric injury patients exhibiting cognitive dysfunction were imaged to
measure CBV. It was found that greater CBV correlated with various clinical measures of
26
cognitive function. Because CBV can be measured with gadolinium contrast enhanced MRI, this
may allow more quantitative means of diagnosing electrical injury and the concomitant cognitive
impairment, as well as leading to more effective treatment.
Summary and Conclusions
Given the importance of electrical power to human culture, the problem of electrical injury is one
that will continue to exist for the foreseeable future. Electrical injury has been poorly understood
and less than optimally managed in the past. Better understanding of injury mechanisms,
anatomical patterns of injury, and therapy are required. A prompt, accurate clinical diagnosis of
electrical injury is one of the most difficult tasks in the medical field (6) because it usually calls
upon an understanding of the complex interactions between the electric current and human
tissue. Specifically an accurate and complete diagnosis is complicated by:
1. The exact tissue damage mechanism and damage level, which depend on a host of
parameters including the characteristics of the power source (DC or AC current, voltage,
frequency, etc.), path and duration of the closed circuit, area and impedance of the contact
spot. Correspondingly, there is a whole spectrum of damage characteristics depending on the
values of these parameters. The physician needs to do 4-dimensional (spatial plus temporal)
detective work in order to arrive at a correct diagnosis.
2. Electrical damage to the tissues is not easily detectable by visual inspection or physical
examination. Often sequelae will not manifest themselves for a while: electrically injured
tissue may initially appear viable, only to become visibly necrotic at a later point (in a
number of days) (99–101).
27
The molecular structure of biological systems can be severely altered by the effects of high-
energy commercial frequency electrical power. The mechanisms of damage include cell
membrane electroporation, Joule heating, and electroconformational changes (denaturation) of
proteins and other macromolecules. Rehabilitation and reconstruction needs in the electrically
injured are usually not obvious at the initial evaluation. The reintegration of the individual into
their pre-injury living situation often becomes a real challenge. Aside from physically obvious
impairments (loss of limb etc.) it is not uncommon for an electrician to develop a phobia towards
electricity after being injured. The more in-depth understanding of the underlying mechanism of
injury will lead to a more specific treatment regime that may prevent some of the late sequelae of
electrical injury.
Acknowledgements
Parts of the research presented were funded by grants from the Electric Power Research Institute
(RP WO-2914 and RP WO-9038), the National Institutes of Health (NIGMS 5-R01 GM53113)
and Commonwealth Edison. The authors thank Zhou-xian Pan for assistance in editing this
chapter.
28
References
1. Nursal TZ, Yildirim S, Tarim A, Caliskan K, Ezer A, Noyan T. Burns in southern Turkey: electrical burns remain a major problem. J Burn Care Res. 2003;24(5):309–314.
2. Bureau of Labor Statistics. Industry Injury and Illness Data. Injuries, Illnesses, and Fatalities. (accessed 2017 Jul 14).
3. McCann M, Hunting KL, Murawski J, Chowdhury R, Welch L. Causes of electrical deaths and injuries among construction workers. Am J Ind Med. 2003 Apr 1;43(4):398–406.
4. Gourbière E, Cabanes J, Lambrozo J. Work #x2014; Related electrical burns among workers of Electricite de France: A review of 938 cases during the ten-year period 1980 to 1989. In: 1992 14th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. 1992. p. 2821–3.
5. Hunt JL. Soft tissue patterns in acute electric burns. In: Electrical trauma: the pathophysiology, manifestations, and clinical management. Cambridge University Press, Cambridge; 1992. p. 83–104.
6. National Safety Council. Research and Statistical Services. NSC Research & Statistical Services. (accessed 2017 Jul 24).
7. Dalziel CF, Lee WR. Lethal electric currents. IEEE Spectr. 1969 Feb;6(2):44–50.
8. Dalziel CF, Ogden E, Abbott CE. Effect of frequency on let-go currents. Electr Eng. 1943 Dec;62(12):745–9.
9. National Weather Service. NWS Lightning Fatalities. (accessed 2017 Jul 27).
10. Holle RL. A Summary of Recent National-Scale Lightning Fatality Studies. Weather Clim Soc. 2015 Sep 17;8(1):35–42.
11. Whitcomb D, Martinez JA, Daberkow D. Lightning injuries. South Med J. 2002;95(11):1331–1335.
12. Duling BR. The Kidney. In: Physiology. St. Louis: The C. V. Mosby Company; 1983. p. 824.
13. Geddes LA, Baker LE. The specific resistance of biological material—a compendium of data for the biomedical engineer and physiologist. Med Biol Eng. 1967;5(3):271–293.
14. Lee RC, Kolodney MS. Electrical injury mechanisms: dynamics of the thermal response. Plast Reconstr Surg. 1987;80(5):663–671.
15. Daniel RK, Ballard PA, Heroux P, Zelt RG, Howard CR. High-voltage electrical injury: Acute pathophysiology. J Hand Surg. 1988 Jan 1;13(1):44–9.
16. Sances A, Myklebust J, Larson S, Darin J, Swiontek T, Prieto T, et al. Experimental Electrical Injury Studies. : J Trauma-Inj Infect Crit Care. 1981 Aug;21(9).
17. Sokhal AK, Lodha KG, Kumari M, Paliwal R, Gothwal S. Clinical spectrum of electrical burns – A prospective study from the developing world. Burns. 2017 Feb 1;43(1):182–9.
29
18. Cela CJ, Lee RC, Lazzi G. Modeling cellular lysis in skeletal muscle due to electric shock. Biomed Eng IEEE Trans On. 2011;58(5):1286–1293.
19. Tropea BI, Lee RC. Thermal injury kinetics in electrical trauma. J Biomech Eng. 1992;114(2):241–250.
20. Diller KR. The Mechanisms and Kinetics of Heat Injury Accumulation. Ann N Y Acad Sci. 1994 May 1;720(1):38–55.
21. Reilly JP. Scales of Reaction to Electric Shock. Ann N Y Acad Sci. 1994 May 1;720(1):21–37.
22. Lee R. Injury by electrical forces: Pathophysiology, Manifestations, and therapy. Curr Probl Surg. 1997 Sep;34(9):677, 679–764.
23. Gaylor DC, Prakah-Asante K, Lee RC. Significance of cell size and tissue structure in electrical trauma. J Theor Biol. 1988 Jul 21;133(2):223–37.
24. Kalkan T, Demir M, Ahmed ASMS, Yazar S, Dervisoglu S, Uner HB, et al. A dynamic study of the thermal components in electrical injury mechanism for better understanding and management of electric trauma: an animal model. Burns. 2004 Jun 1;30(4):334–40.
25. Bhatt DL, Gaylor DC, Lee RC. Rhabdomyolysis due to pulsed electric fields. Plast Reconstr Surg. 1990;86(1):1–11.
26. Lee RC, Astumian RD. The physicochemical basis for thermal and non-thermal “burn” injuries. Burns. 1996 Nov 1;22(7):509–19.
27. Block T, Aarsvold J, Matthews II KL, Mintzer RA, River LP, Capelli-Schellpfeffer M, et al. The 1995 Lindberg Award: Nonthermally Mediated Muscle Injury and Necrosis in Electrical Trauma. J Burn Care Res. 1995 Dec;16(6):21A–31A.
28. Capelli-Schellpfeffer M, Lee RC, Toner M, Diller KR. Correlation between electrical accident parameters and injury. IEEE Ind Appl Mag. 1998 Mar;4(2):25–31,41.
29. Koumbourlis AC. Electrical injuries. Crit Care Med. 2002 Nov;30(11 Suppl):S424-430.
30. Parsegian A. Energy of an ion crossing a low dielectric membrane: solutions to four relevant electrostatic problems. Nature. 1969;221(5183):844–846.
31. Mandel LJ. Bioenergetics of Membrane Transport Processes. In: Membrane Physiology. Springer, Boston, MA; 1987. p. 295–310.
32. Tarek M. Membrane Electroporation: A Molecular Dynamics Simulation. Biophys J. 2005 Jun 1;88(6):4045–53.
33. Weaver JC, Chizmadzhev YA. Theory of electroporation: A review. Bioelectrochem Bioenerg. 1996 Dec 1;41(2):135–60.
34. Ho SY, Mittal GS. Electroporation of Cell Membranes: A Review. Crit Rev Biotechnol. 1996 Jan 1;16(4):349–62.
35. Neumann E, Kakorin S, Tœnsing K. Fundamentals of electroporative delivery of drugs and genes. Bioelectrochem Bioenerg. 1999 Feb 1;48(1):3–16.
36. Cevc G. Membrane electrostatics. Biochim Biophys Acta BBA-Rev Biomembr. 1990;1031(3):311–382.
30
37. Chen W, Lee RC. Altered ion channel conductance and ionic selectivity induced by large imposed membrane potential pulse. Biophys J. 1994 Aug 1;67(2):603–12.
38. Lee RC, Aarsvold JN, Chen W, Astumian RD, Capelli-Schellpfeffer M, Kelley KM, et al. Biophysical mechanisms of cell membrane damage in electrical shock. In: Seminars in neurology. Thieme Medical Publishers, Inc.; 1995. p. 367–374.
39. Lee RC, Gaylor DC, Bhatt D, Israel DA. Role of cell membrane rupture in the pathogenesis of electrical trauma. J Surg Res. 1988;44(6):709–719.
40. Glaser RW, Leikin SL, Chernomordik LV, Pastushenko VF, Sokirko AI. Reversible electrical breakdown of lipid bilayers: formation and evolution of pores. Biochim Biophys Acta BBA - Biomembr. 1988 May 24;940(2):275–87.
41. Neu JC, Krassowska W. Asymptotic model of electroporation. Phys Rev E. 1999;59:3471.
42. Tung L. Electrical injury to heart muscle cells. Electr Trauma Pathophysiol Manif Clin Manag. 1992;361–400.
43. Tung L, Tovar O, Neunlist M, Jain SK, O’neill RJ. Effects of Strong Electrical Shock on Cardiac Muscle Tissuea. Ann N Y Acad Sci. 1994 May 1;720(1):160–75.
44. Mir LM, Glass LF, Sersa G, Teissié J, Domenge C, Miklavcic D, et al. Effective treatment of cutaneous and subcutaneous malignant tumours by electrochemotherapy. Br J Cancer. 1998 Jun;77(12):2336–42.
45. Heller R, Jaroszeski MJ, Reintgen DS, Puleo CA, DeConti RC, Gilbert RA, et al. Treatment of cutaneous and subcutaneous tumors with electrochemotherapy using intralesional bleomycin. Cancer. 1998 Jul 1;83(1):148–57.
46. Aihara H, Miyazaki J. Gene transfer into muscle by electroporation in vivo. Nat Biotechnol. 1998;16(9):867–870.
47. Mir LM, Bureau MF, Gehl J, Rangara R, Rouy D, Caillaud J-M, et al. High-efficiency gene transfer into skeletal muscle mediated by electric pulses. Proc Natl Acad Sci. 1999 Apr 13;96(8):4262–7.
48. Pliquett U, Langer R, Weaver JC. Changes in the passive electrical properties of human stratum corneum due to electroporation. Biochim Biophys Acta BBA - Biomembr. 1995 Nov 1;1239(2):111–21.
49. Prausnitz MR, Lee CS, Liu CH, Pang JC, Singh T-P, Langer R, et al. Transdermal transport efficiency during skin electroporation and iontophoresis. J Controlled Release. 1996 Feb 1;38(2):205–17.
50. Teissié J, Eynard N, Gabriel B, Rols MP. Electropermeabilization of cell membranes. Adv Drug Deliv Rev. 1999 Jan 4;35(1):3–19.
51. Woods LA, Gandhi PU, Ewing AG. Electrically Assisted Sampling across Membranes with Electrophoresis in Nanometer Inner Diameter Capillaries. Anal Chem. 2005 Mar 1;77(6):1819–23.
52. Kim J, Do H, Choi S, Cho H, Park K, Yang H-M, et al. Efficient gene delivery in differentiated human embryonic stem cells - ProQuest. Exp Mol Med. 2005 Feb;37(1):36–44.
53. Pierreux C, Poll A, Jacquemin P, Lemaigre F, Rousseau G. Gene Transfer into Mouse Prepancreatic Endoderm by Whole Embryo Electroporation. J Pancreas. 2005;6(2):128–35.
54. Hu Y, Parekh-Olmedo H, Drury M, Skogen M, Kmiec EB. Reaction parameters of targeted gene repair in mammalian cells. Mol Biotechnol. 2005 Mar 1;29(3):197–210.
31
55. Weaver JC. Electroporation: A general phenomenon for manipulating cells and tissues. J Cell Biochem. 1993 Apr 1;51(4):426–35.
56. Jordan CA, Neumann E, Sowers AE. Electroporation and electrofusion in cell biology. Springer Science & Business Media; 2013.
57. Chang DC, Chassy BM, Saunders J, Sowers AE. Guide to Electroporation and Electrofusion. Academic Press; 2012. 592 p.
58. Lynch P, Davey MR. Electrical manipulation of cells. Springer Science & Business Media; 2012.
59. Bier M, Gowrishankar TR, Chen W, Lee RC. Electroporation of a lipid bilayer as a chemical reaction - Bier - 2004 - Bioelectromagnetics - Wiley Online Library. Bioelectromagnetics. 2004 Dec;25(8):634–7.
60. Bier M, Hammer SM, Canaday DJ, Lee RC. Kinetics of sealing for transient electropores in isolated mammalian skeletal muscle cells. Bioelectromagnetics. 1999 Jan 1;20(3):194–201.
61. Gabriel B, Teissié J. Direct observation in the millisecond time range of fluorescent molecule asymmetrical interaction with the electropermeabilized cell membrane. Biophys J. 1997 Nov 1;73(5):2630–7.
62. Gabriel B, Teissié J. Mammalian cell electropermeabilization as revealed by millisecond imaging of fluorescence changes of ethidium bromide in interaction with the membrane1Presented at the 14th BES symposium in Vingstedcentret (Denmark), 1998.1. Bioelectrochem Bioenerg. 1998 Nov 1;47(1):113–8.
63. Gowrishankar TR, Chen W, Lee RC. Non-Linear Microscale Alterations in Membrane Transport by Electropermeabilizationa. Ann N Y Acad Sci. 1998 Sep 1;858(1):205–16.
64. Chizmadzhev YA, Arakelyan VB, Pastuhenko VF. Electric breakdown of bilayer lipid membranes. J Electroanal Chem Interfacial Electrochem. 1979 Jan 1;104:63–70.
65. DeBruin KA, Krassowska W. Modeling Electroporation in a Single Cell. I. Effects of Field Strength and Rest Potential. Biophys J. 1999 Sep 1;77(3):1213–24.
66. DeBruin KA, Krassowska W. Modeling Electroporation in a Single Cell. II. Effects of Ionic Concentrations. Biophys J. 1999 Sep 1;77(3):1225–33.
67. Hibino M, Shigemori M, Itoh H, Nagayama K, Kinosita K. Membrane conductance of an electroporated cell analyzed by submicrosecond imaging of transmembrane potential. Biophys J. 1991 Jan 1;59(1):209–20.
68. Kinosita K, Hibino M, Itoh H, Shigemori M, Hirano K ’ichi, Kirino Y, et al. Events of membrane electroporation visualized on a time scale from microsecond to seconds. Guide Electroporation Electrofusion. 1992;29–46.
69. Knisley SB, Grant AO. Asymmetrical electrically induced injury of rabbit ventricular myocytes. J Mol Cell Cardiol. 1995 May 1;27(5):1111–22.
70. Hibino M, Itoh H, Kinosita K. Time courses of cell electroporation as revealed by submicrosecond imaging of transmembrane potential. Biophys J. 1993 Jun 1;64(6):1789–800.
71. Neumann E, Sprafke A, Boldt E, Wolf H. Biophysical considerations of membrane electroporation. In: Chang DC, Chassy BM, Saunders J, Sowers AE, editors. Guide to electroporation and electrofusion. San Diego: Academic Press; 1992. p. 77–90.
72. Rols MP, Teissié J. Electropermeabilization of mammalian cells. Quantitative analysis of the phenomenon. Biophys J. 1990 Nov 1;58(5):1089–98.
32
73. DeBono R. A histological analysis of a high voltage electric current injury to an upper limb. Burns. 1999 Sep 1;25(6):541–7.
74. Moussa NA, McGrath JJ, Cravalho EG, Asimacopoulos PJ. Kinetics of Thermal Injury in Cells. J Biomech Eng. 1977 Aug 1;99(3):155–9.
75. Rocchio CM. The kinetics of thermal damage to an isolated skeletal muscle cell. Massachusetts Institute of Technology, Department of Electrical Engineering and Computer Science; 1989.
76. Cravalho EG, Toner M, Gaylor DC, Lee RC. Response of cells to supraphysiological temperatures: experimental measurements and kinetic models. Cambridge University Press; 1992.
77. Henriques Jr FC. Studies of thermal injury; the predictability and the significance of thermally induced rate processes leading to irreversible epidermal injury. Arch Pathol Chic. 1947;43(5):489–502.
78. Moritz AR, Henriques Jr FC. Studies of Thermal Injury: II. The Relative Importance of Time and Surface Temperature in the Causation of Cutaneous Burns*. Am J Pathol. 1947;23(5):695.
79. Gershfeld NL, Murayama M. Thermal instability of red blood cell membrane bilayers: Temperature dependence of hemolysis. J Membr Biol. 1988 Dec 1;101(1):67–72.
80. Moussa NA, Tell EN, Cravalho EG. Time Progression of Hemolysis of Erythrocyte Populations Exposed to Supraphysiological Temperatures. J Biomech Eng. 1979 Aug 1;101(3):213–7.
81. Gaylor D. Role of electromechanical instabilities in electroporation of cell membranes. PhD thesis. MIT, Cambridge; 1989.
82. Merchant FA, Holmes WH, Capelli-Schellpfeffer M, Lee RC, Toner M. Poloxamer 188 Enhances Functional Recovery of Lethally Heat-Shocked Fibroblasts. J Surg Res. 1998 Feb 1;74(2):131–40.
83. Bischof JC, Padanilam J, Holmes WH, Ezzell RM, Lee RC, Tompkins RG, et al. Dynamics of cell membrane permeability changes at supraphysiological temperatures. Biophys J. 1995 Jun 1;68(6):2608–14.
84. Tsong TY, Astumian RD. Electroconformational coupling and membrane protein function. Prog Biophys Mol Biol. 1987 Jan 1;50(1):1–45.
85. Chen W, Han Y, Chen Y, Astumian D. Electric Field-Induced Functional Reductions in the K+ Channels Mainly Resulted from Supramembrane Potential-Mediated Electroconformational Changes. Biophys J. 1998 Jul 1;75(1):196–206.
86. Clausen T, Gissel H. Role of Na+,K+ pumps in restoring contractility following loss of cell membrane integrity in rat skeletal muscle. Acta Physiol Scand. 2005 Mar 1;183(3):263–71.
87. Chou CK. Radio Frequency Hyperthermia in Cancer Therapy. In: Bronzino JD, editor. Biologic Effects of Nonionizing Electromagnetic Fields. Boca Raton, FL: CRC Press; 1995. p. 1424–8.
88. Sneed PK, Gutin PH, Stauffer PR, Phillips TL, Prados MD, Suen S, et al. Thermoradiotherapy of recurrent malignant brain tumors. Int J Radiat Oncol. 1992;23(4):853–61.
89. Rhoon GCV, Zee J van der, Broekmeyer-Reurink MP, Visser AG, Reinhold HS. Radiofrequency capacitive heating of deep-seated tumours using pre-cooling of the subcutaneous tissues: Results on thermometry in Dutch patients. Int J Hyperthermia. 1992 Jan 1;8(6):843–54.
90. Nicholson CP, Grotting JC, Dimick AR. Acute microwave injury to the hand. J Hand Surg. 1987 May 1;12(3):446–9.
33
91. Alexander RC, Surrell JA, Cohle SD. Microwave Oven Burns to Children: An Unusual Manifestation of Child Abuse. Pediatrics. 1987 Feb 1;79(2):255–60.
92. Surrell JA, Alexander RC, Cohle SD, Lovell Jr FR, Wehrenberg RA. Effects of microwave radiation on living tissues. J Trauma Acute Care Surg. 1987;27(8):935–939.
93. Pliskin NH, Fink J, Malina A, Moran S, Kelley KM, CAPELLI-SCHELLPFEFFER M, et al. The neuropsychological effects of electrical injury: new insights. Ann N Y Acad Sci. 1999;888(1):140–149.
94. Kelley KM, Tkachenko TA, Pliskin NH, Fink JW, Lee RC. Life after electrical injury: Risk factors for psychiatric sequelae. Ann N Y Acad Sci. 1999;888(1):356–363.
95. Aase DM, Fink JW, Lee RC, Kelley KM, Pliskin NH. Mood and cognition after electrical injury: a follow-up study. Arch Clin Neuropsychol Off J Natl Acad Neuropsychol. 2014 Mar;29(2):125–30.
96. Ramati A, Pliskin NH, Keedy S, Erwin RJ, Fink JW, Bodnar EN, et al. Alteration in Functional Brain Systems after Electrical Injury. J Neurotrauma. 2009 Sep 10;26(10):1815–22.
97. Shen AC, Jennings RB. Kinetics of Calcium Accumulation in Acute Myocardial Ischemic Injury. Am J Pathol. 1972 Jun;67(3):441–52.
98. Park C, Seo CH, Jung MH, Joo SY, Jang S, Lee HY, et al. Investigation of cognitive circuits using steady-state cerebral blood volume and diffusion tensor imaging in patients with mild cognitive impairment following electrical injury. Neuroradiology. 2017 Jul 8;1–7.
99. Baxter CR. Present concepts in the management of major electrical injury. Surg Clin North Am. 1970;50(6):1401–1418.
100. Artz CP. Electrical injury simulates crush injury. Surg Gynecol Obstet. 1967;125(6):1316.
101. Hammond J, Ward CG. The use of Technetium-99 pyrophosphate scanning in management of high voltage electrical injuries. Am Surg. 1994;60(11):886–888.
34





























