Embed Size (px)
Citation preview

Biopreservation of Red Blood Cells: Past, Present, and Future
Kirby L. Scott, Jelena Lecak, and Jason P. Acker
Preservation and long-term storage of red blood
cells (RBCs) is needed to ensure a readily available,
safe blood supply for transfusion medicine. Effective
preservation procedures are required at various
steps in the production of a RBC product including
testing, inventory, quality control, and product
distribution. Biopreservation is the process of main-
taining the integrity and functionality of cells
held outside the native environment for extended
Transfusion Medicine Reviews, Vol 19, No 2 (April), 2005: pp 127-1
storage times. The biopreservation of RBCs for
clinical use can be categorized based on the
techniques used to achieve biologic stability and
ensure a viable state after long-term storage. This
article reviews the history, science, current practi-
ces, and emerging technologies of current RBC
biopreservation approaches: hypothermic storage,
cryopreservation, and lyophilization.
A 2005 Elsevier Inc. All rights reserved.
From the Canadian Blood Services, Research and Develop-
ment, and Department of Laboratory Medicine and Pathology,
University of Alberta, Edmonton, Alberta, Canada.
The first two authors contributed equally to this work.
Address reprint requests to Jason Acker, PhD, 8249-114
Street, Edmonton, Alberta, Canada T6G 2R8. E-mail:
0887-7963/05/$ – see front matter
n 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.tmrv.2004.11.004
T HE DEVELOPMENT OF effective red
blood cell (RBC) biopreservation techniques
that maintain ex vivo RBC viability and function
represents the foundation of modern blood bank-
ing. The ability to preserve the integrity of RBCs
outside the native environment for extended
periods has not only separated blood donors and
recipients in space and time, but also has made it
possible for blood banks to provide safe, high-
quality blood products in an efficient and effective
manner. Most processes routinely performed by
donor centers and transfusion services, including
collection, controlled blood distribution, inventory
management, component production, compatibility
matching, transmissible disease testing, and trans-
port, rely on the ability to prevent or delay the
detrimental biochemical, biophysical, and morphol-
ogic effects of ex vivo RBC storage.
The major force driving the field of RBC
biopreservation is the enormous clinical need for
RBC products. Red blood cell transfusions save
lives by increasing RBC mass in patients that have
low oxygen–carrying capacity due to increased
RBC loss (traumatic/surgical hemorrhage), de-
creased bone marrow production (aplastic ane-
mias), defective hemoglobin (hemaglobinopathies
and thalassemias), and decreased RBC survival
(hemolytic anemias). However, as with any med-
ical procedure, the patients face potential risks
associated with hemotherapy, including immune-
and nonimmune-mediated transfusion-related ad-
verse reactions. Maintaining the quality and safety
of RBCs delivered to the patient, as well as the
overall clinical use of blood products, requires
effective techniques for the preservation of RBC
viability and function.
Each year, millions of RBC units are transfused
world wide because of application of biopreserva-
tion techniques to transfusion medicine. The
biopreservation of RBCs for clinical use can be
categorized based on the techniques used to achieve
biologic stability and/or ensure a viable state after
ex vivo storage. After a brief review of RBC
physiology, this paper will review the history,
science, current practices, and emerging tech-
nologies of the 3 main RBC biopreservation
approaches: hypothermic storage, cryopreserva-
tion, and lyophilization.
RED BLOOD CELL PHYSIOLOGY
As the goal of RBC biopreservation is to provide
viable and functional RBCs for patients requiring a
blood transfusion, knowledge of RBC physiology
is essential to assess the effectiveness of a
biopreservation approach, as well as the in vitro
and in vivo quality of transfused RBCs. Derived
from pluripotent stem cells in bone marrow
through a maturation process called erythropoiesis,
mature RBCs are biconcave disks approximately
7.2 lm in diameter, 1.5 to 2.5 lm thick, with a
mean volume of 90 fL.1 Erythropoiesis is predom-
inantly regulated by an erythroid growth factor,
erythropoietin, whose synthesis is regulated by
renal oxygen tension in response to such factors as
hemoglobin oxygen saturation, hemoglobin con-
centration, plasma 2,3 diphosphoglycerate (2,3-
DPG) levels, RBC mass, rate of blood flow, and
basal metabolic rate. The RBC maturation process
42 127

SCOTT, LECAK, AND ACKER128
involves 6 morphologically distinct developmental
stages: rubiblast, prorubicyte, rubicyte, metarubi-
cyte, reticulocyte, and mature RBC. With each
successive developmental stage, there is a reduc-
tion in cell volume, condensation of chromatin,
loss of nucleoli, decrease in the nucleus, RNA,
mitochondria, and an increase in hemoglobin
synthesis, resulting in a mature RBC, which lacks
a nucleus and organelles.
The primary function of RBCs is to transport
oxygen from the lungs to the body tissues, where
the exchange for carbon dioxide is facilitated
through synergistic effects of hemoglobin, carbonic
anhydrase, and band 3 protein, followed by carbon
dioxide delivery to the lungs for release. Successful
oxygen transport is dependent on efficacy of the
3 elements of RBC metabolism: the RBC mem-
brane, hemoglobin, and cellular energetics.
Like other cell membranes, the RBC membrane
is a fluid structure composed of a semipermeable
lipid bilayer with an asymmetrically organized
mosaic of proteins. Membrane lipids compromise
approximately 40% of the RBC membrane mass,
with equimolar quantities of unesterified choles-
terol and phospholipids, and small amounts of
free fatty acids and glycolipids.2 Membrane
proteins comprise approximately 52% of the
RBC membrane mass and can be categorized
into integral and peripheral proteins according to
their location relative to the lipid bilayer.2 Integral
membrane proteins, such as glycophorin and band
3 protein, transverse the membrane and contain
extensions into or out of the RBC. The main
function of integral membrane proteins is to carry
RBC antigens and to act as receptors and trans-
porters. In contrast, peripheral proteins are only
found on the cytoplasmatic surface of RBC
membrane forming the RBC cytoskeleton. The
major components of the RBC cytoskeleton are
spectrin, ankyrin, protein 4.1, actin, and adducin.3
These proteins form a mesh-like network of
microfilaments that strengthens the RBC mem-
brane while maintaining RBC shape and stabili-
ty.3 Unusual properties of the RBC membrane,
such as high elasticity, rapid response to stresses,
and the ability to undergo large membrane
extensions without fragmentation, have been
summarized by the term cellular deformability.
Cellular deformability allows human RBCs to
survive and deliver oxygen as they travel through
the microvasculature.
The second element of the RBC metabolism that
has to be maintained for RBCs to function
normally is hemoglobin. Hemoglobin is a conju-
gated protein consisting of 2 pairs of globin chains
and 4 heme groups, each containing a protopor-
phyrin group and an iron molecule in the ferrous
form.4 Hemoglobin constitutes 95% of the RBC
dry weight and its production is dependent on 3
processes: iron delivery, protoporphyrin synthesis,
and globin synthesis. The uptake and release of
oxygen by the hemoglobin molecule is controlled
by the RBC organic phosphate 2,3-DPG, which
binds to the cleft between globin chains, resulting
in a deoxyhemoglobin conformation that facilitates
the release of oxygen. Therefore, increased 2,3-
DPG levels triggered by tissue hypoxia will shift
the hemoglobin-oxygen dissociation curve to the
right, increasing oxygen delivery to the tissues.
Maintenance of the RBC membrane system and
hemoglobin function is dependent on energy
generation through RBC metabolic pathways.
There are 4 RBC metabolic pathways: the
Embden-Mayerhof pathway, in which most RBC
adenosine triphosphate (ATP) is generated through
the anaerobic breakdown of glucose; the hexose
monophosphate shunt, which produces NADPH
to protect RBCs from oxidative injury; the
Rapoport-Luebering shunt, responsible for the
production of 2,3-DPG for the control of hemo-
globin oxygen affinity; and finally, the methemo-
globin reduction pathway, which reduces ferric
heme iron to the ferrous form to prevent
hemoglobin denaturation.
Defects associated with any of the 3 above-
described elements of RBC metabolism are related
to the development and pathogenesis of the many
forms of inherited and acquired RBC abnormalities
that result in increased RBC destruction through
intra- or extravascular hemolysis, and therefore, an
in vivo survival of less than the normal 120 days.
During a normal life span, circulating RBCs
undergo metabolic and physical changes associated
with the process of senescence, such as membrane
vesiculation, decrease in cell size, increase of cell
density, alteration of cytoskeleton, enzymatic
desilylation, and phosphatidylserine exposure. At
the end of their life span, RBCs are recognized and
removed by the fixed macrophages in the reticu-
loendothelial system (RES). It has been estimated
that 5 million RBCs are endocytosed by RES
macrophages per second each day.5 These RBCs

BIOPRESERVATION OF RBCs 129
are replaced by RBC reticulocytes which are
released daily from the bone marrow storage pool.
Although RBC physiology has been exhaustive-
ly investigated, there are still many crucial ques-
tions left unanswered, such as the actual
biochemical structure and organization of the
RBC membrane, the exact determinants of RBC
shape, as well as the physiological mechanism of
RBC shape regulation, senescence, and destruc-
tion. Continuous research of the mechanisms of
RBC development, function, survival, and destruc-
tion is not only crucial for future advances in the
fields of hematology and transfusion medicine, but
also for the development of improved RBC storage
and preservation technologies.
HYPOTHERMIC STORAGE OF RBCS
The earliest and most widely investigated
approach to RBC biopreservation has been hypo-
thermic storage. After the discovery of ABO blood
groups in 1901 by Karl Landsteiner, there were 2
main obstacles blocking the path to successful
transfusions: blood clotting and in vitro loss of
RBC viability and function. Introduction of citrate
as an anticoagulant in 1914 by Hustin6 and glucose
as a preservative in 1916 by Rous and Turner7,8
were landmarks in blood banking.9 In the follow-
ing year, during the First World War, Robertson
pioneered the use of preserved human blood by
using glass bottles, Rous-Turner citrate-glucose
preservative solution, and iced jars packed with
sawdust.9 Robertson’s blood transfusion technique
quickly became an accepted resuscitation therapy.
The discovery of glucose-citrate preservation was
the first step toward modern blood banking.
Hypothermic preservation of RBCs is based on
the principle that biochemical events and molecular
Fig 1. Hypothermic storage does not fully preserve biophy
reactions can be suppressed by a reduction in
temperature. In the context of biopreservation,
hypothermic conditions are those in which the
temperature is lower than the normal physiological
temperature but higher than the freezing point of
the storage solution. As chemical reaction rates are
temperature dependent, cooling below normal
physiological temperatures inhibits metabolic pro-
cesses that deplete critical cellular metabolites and
accumulate injury. As changes in temperatures
have significant effects on the physicochemical
properties of aqueous systems, biochemical reac-
tion rates, and transport phenomena that will disrupt
cell homeostasis (reviewed in Refs. 10 and 11),
understanding the biochemical and physiological
implications of RBC hypothermic exposure has led
to the development of strategies to minimize
hypothermia-related injury.
Advances in RBC preservation were also made
in response to the discovery of more detailed
information regarding the biochemical and mor-
phologic RBC changes caused by nutrient de-
pletion and accumulation of wastes during
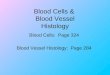
hypothermic ex vivo storage. These changes are
summarized by the term hypothermic storage
lesion (Fig 1). Adenosine triphosphate depletion
was one of the first elements of the hypothermic
storage lesion that closely correlated with post-
transfusional RBC survival.12,13 As ATP is neces-
sary for maintenance of electrolyte balance by
powering sodium-potassium cationic pumps, ATP
depletion has been associated with impairment of
ATP-dependent parameters of cell shape, increased
internal RBC viscosity coupled with a decrease in
critical hemolytic volume, RBC deformability and
filterability.14,15 Related to ATP depletion, a
distinct component of the hypothermic storage
sical, biochemical, and morphologic RBC properties.

SCOTT, LECAK, AND ACKER130
lesion is RBC membrane injury, which includes
lipid loss, microvesiculaton, macroaggregate for-
mation, progressive spheroechinocytosis, abnormal
RBC endocytosis, and reduced surface area to
volume ratio.15,16 Another key element in the
hypothermic storage lesion, which significantly
affects RBC function, is a loss of 2,3-DPG. A
deficiency in 2,3-DPG is associated with an
increased hemoglobin affinity for oxygen, which
is reflected by the decreased RBC ability to deliver
oxygen to tissues. The rapid disappearance of 2,3-
DPG from preserved blood has not been of high
concern because RBCs regain the ability to
synthesize 2,3-DPG after transfusion. However,
the restoration of 2,3-DPG in vivo requires up to
48 hours, and this period of altered oxygen affinity
may be significant in certain clinical conditions.17
Preserving RBC 2,3-DPG levels is therefore an
essential element in maintaining the ex vivo quality
of hypothermically stored RBCs. Although the
hypothermic storage lesion has been extensively
studied, its fundamental nature, together with the
cause, significance, and interrelationship of its
biochemical and physical component parameters
still remains to be elucidated.16,18
As the hypothermic storage lesion became a
recognized factor reducing posttransfusional RBC
viability, additive supplementation of storage sol-
utions progressively changed to improve the
quality of stored RBCs. Traditional anticoagulant
solutions acid-citrate-dextrose, citrate-phosphate-
dextrose, and citrate-phosphate-dextrose-adenine
were developed in the 1960s, when whole blood
was predominantly used in transfusion therapy.
These solutions are currently approved for hypo-
thermic whole blood storage up to 35 days.19
However, by the 1970s, component therapy started
to replace whole blood transfusions. Removal of
plasma during blood processing created several
problems for RBC transfusion therapy, including
excessively viscous RBC concentrates and de-
creased cell viability during hypothermic storage.20
Consequently, the currently licensed additive sol-
utions saline-adenine-glucose-mannitol (SAGM),
Adsol (AS-1), Nutricel (AS-3), and Optisol (AS-5)
were developed and prolonged the acceptable
hypothermic storage limit to the current duration
of 42 days.16,21,22
Red blood cell preservation is an excellent
example of how an understanding of cell metab-
olism and hypothermia-related injury can lead to
the development of improved preservation solu-
tions.23,24 Current additive solutions contain ade-
nine, which increases the adenylate pool and shifts
the equilibrium conditions toward ATP production,
so energy for the first half of the glycolysis
pathway and membrane integrity is maintained.
Glucose is supplemented as an essential nutrient
for the retention of cellular metabolism. Several
different approaches were shown to be effective in
reducing the rate of hemolysis and membrane loss
during storage, with the most popular ones being
the use of polyvinyl chloride (PVC) blood bags
plasticizedwith di (2-ethylhexyl) pthalate (DEHP)16
and the addition of membrane stabilizers such as
mannitol and citrate.22 Inorganic phosphate is
added to the storage medium to act both as
a buffer to the continuously decreasing pH and as
a substrate for the synthesis of 2,3-DPG. Bicar-
bonate buffering is effective for maintenance of
acidic pH and ATP levels by driving the diffusion
of carbon dioxide from PVC bags.22 Although
SAGM, AS-1, AS-2, and AS-5 are coupled with
citrate-phosphate-dextrose as the primary anticoag-
ulant bag, AS-3 requires additional glucose supple-
mentation provided by the citrate-phosphate-double
dextrose anticoagulant. All currently licensed addi-
tive solutions support the minimal 75%, 24-hour in
vitro survival and 1% hemolysis standard criteria set
by the American Association of Blood Banks for up
42 days of hypothermic storage at 18C to 68C.19
In addition to nutrient supplementation, several
storage parameters are manipulated to minimize
the hypothermic storage lesion. Because biochem-
ical reaction rates are temperature dependent,
storage at temperatures between 18C and 68Cminimizes RBC degradation by reducing RBC
metabolism by about 40 times.22 The pH con-
ditions, which are also strongly associated with the
RBC storage lesion, are affected by the volume and
osmolality of the storage solution, as well as by the
gas permeability of the storage container. The
acidic pH of current additive solutions maintains
ATP levels, but is detrimental to 2,3-DPG levels,
which fall bellow 10% of the initial value by 3
weeks of storage.17 Hfgman and Meryman25
proposed several practical procedures to extend
the maintenance of RBC 2,3-DPG levels during
hypothermic storage, including elevating the pH of
additive solutions, increasing the volume of the
additives, using hypotonic additives, and cooling
the RBCs to room temperature after collection.

BIOPRESERVATION OF RBCs 131
Leukoreduction has also been shown to improve
RBC hypothermic storage. Removal of metaboli-
cally active white blood cells from RBC concen-
trates minimizes glucose consumption, waste
product accumulation, and damage from leukocyte
enzymes, resulting in a significant decrease in
hemolysis during hypothermic storage.22
Although the quality of hypothermically stored
RBCs has improved with the use of anticoagulant/
additive solutions, these storage solutions do not
fully preserve RBC viability and function. Cellular
metabolism is not completely suppressed at hypo-
thermic temperatures. Therefore, there is a contin-
uous decrease in pH, accumulation of lactic acid,
and an increase in cellular injury, which neces-
sitates a shelf life of 42 days.21 Current research
suggests that the RBC hypothermic storage lesion
still significantly influences the efficacy of trans-
fusion as it is responsible for the association of
blood transfusion with an increased length of stay
in the hospital,26 impaired tissue oxygen use,27
proinflammatory and immunomodulatory effects,28
increased infections,29 multiple organ system
failure,30 and ultimately, increased morbidity and
mortality.31-34 The molecular mechanism by which
30% and 70% of transfused RBCs disappear from
the circulation after 1 and 3 days, respectively, is
still unknown.35 Moreover, at the end of the 42-day
shelf life, a transfused RBC unit will contain 25%
noncirculating RBC, whose removal by RES might
be a basis for at least a transient immune de-
pression.25 The currently accepted biologic marker
of RBC viability, which is minimal 24-hour
posttransfusional survival of 75% of RBCs, does
not reflect the clinical effects of transfusion.34 In
addition, in vivo assessment of RBC viability by
measurement of RBC recovery using radioactive
labeling with chromium 51 has many disadvan-
tages, including practical limits and sources of
error.16 As addressed by Beutler,18 a good surro-
gate test for the performance of viability studies in
human volunteers is yet to be developed.
Improvement of current RBC hypothermic
storage practices would have an enormous effect
on RBC availability, safety, and quality. Extending
hypothermic storage would improve blood logis-
tics by reducing RBC losses due to outdating, less
frequent need for shipping, and improved autolo-
gous and remote blood storage. For the last 2
decades, the focus of RBC biopreservation re-
search has been on lengthening the RBC hypo-
thermic storage post 42 days by modifications of
storage solution composition, blood collection
protocols, and devices. As a result, solutions
allowing 7-week hypothermic storage, such as
ErythroSol, MAP, and PAGGS-S/M, have been
developed for clinical use.23,36 In addition, several
rejuvenation solutions that regenerate ATP and
2,3-DPG levels of hypothermically stored RBCs
near or post-outdating have been developed 37; of
which Rejuvesol is currently the only solution
approved by the FDA. Because the rejuvenation
process is expensive and time-consuming, it is
usually reserved for autologous, rare, and unique
RBC units before cryopreservation.21
The basic RBC liquid storage methods estab-
lished in the 1940s still remain the standard of
practice, and progress in maintaining the quality
and function of ex vivo hypothermically stored
RBCs has been very slow.38 Recent trends in
transfusion medicine are toward an increased
emphasis on the quality of hypothermically stored
RBCs rather than extending the existing liquid
storage limits.23 As most of transfused patients
receive allogeneic RBCs 1 to 3 weeks after they
are donated, improved RBC storage systems that
maintain RBC quality would result in a superior
product for the patient, avoidance of unnecessary
transfusions and transfusion-associated disor-
ders.16 According to Valeri,39 for optimum sur-
vival and function, liquid preserved RBCs should
only be hypothermically stored in the currently
licensed preservative solutions for no more than 2
weeks. The continuously increasing need for a
safe, high-quality RBC product that is delivered to
patients in an efficient and effective manner will
ensure future advances in RBC hypothermic
biopreservation.
CRYOPRESERVATION OF RBCs
Cryopreservation is the process of preserving the
biologic structure and/or function of living systems
by freezing to and storage at ultralow temperatures.
As with hypothermic storage, cryopreservation
uses the beneficial effect of decreased temperature
to suppress molecular motion and arrest metabolic
and biochemical reactions. Below �1508C, a state
of bsuspended animationQ can be achieved as there
are very few biologically significant reactions or
changes to the physicochemical properties of the
system.40 In contrast to hypothermic storage, RBC
physiology, including hemoglobin structure, and

Table 1. Physical Changes and Associated Cryoinjury in
Response to Cooling Rate
Cooling Rate Physical Response Cryoinjury
Slow Extracellular ice
formation
RBC packing (mechanical
damage)
Water loss/volume
reduction
Membrane permeability
Ion leakage
Influx of extracellular
solute
Dehydration/solute
concentration
solute toxicity
(biochemical damage)
Rapid Supercooling Intracellular ice formation
(mechanical damage)
SCOTT, LECAK, AND ACKER132
membrane and cellular energetics, is unaffected by
extended storage in the frozen state.41,42 Cryopres-
ervation is the only current technology that
maintains ex vivo biologic function and provides
long-term product storage.
To take advantage of the protective effects of
low temperature and to successfully store RBCs
for extended periods using cryopreservation tech-
niques, damage during freezing and thawing must
be minimized. Over the last century, enormous
progress has been made in understanding the basic
elements responsible for low-temperature injury in
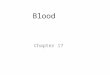
Fig 2. Two-factor hypothesis of cryoinjury. Temperatures above a
�8C, respectively. The snowflakes indicate the presence of ice cryst
RBCs and in the development of effective
techniques to protect RBCs from this cryoinjury.
Cryoinjury
Understanding the action of cryoprotective
agents and the damage that occurs during expo-
sure of RBCs to low temperatures has been central
to the development of protocols for the preserva-
tion of these cells for clinical and research
purposes. In 1972, the 2-factor hypothesis of
Mazur and colleagues43 eloquently summarized
the current understanding of the major forms of
damage that result from freezing, a hypothesis that
is still valid today (Table 1). When physiological
solutions are cooled below the freezing point,
water in the extracellular medium freezes out of
solution, resulting in the concentration of extra-
cellular solute in the unfrozen fraction (Fig 2). The
development of a chemical potential difference
across the cell membrane provides the driving
force for the efflux of water from the cell. With
additional cooling, more ice will form extracellu-
larly, and the cell will become increasingly
dehydrated. If the cooling rate is sufficiently slow,
the movement of water across the membrane will
maintain the intra- and extracellular composition
nd below the solution freezing point are indicated by +8C and
als in the extra- and/or intracellular environment.

BIOPRESERVATION OF RBCs 133
close to chemical equilibrium. At slow cooling
rates the cell has time to respond by exosmosis
resulting in cellular dehydration, volume reduc-
tion, and an increase in intracellular solute concen-
tration over time.
Red blood cell injury during slow cooling has
been correlated with excessive cell shrinkage44,45
and toxicity due to the increasing concentrations of
solutes.46-48 As injury during slow cooling is
dependent on the changing solution composition
and properties of the cryopreservation media, it is
commonly referred to as bsolution effectsQ injury.Pioneering work by James Lovelock in 1953
demonstrated that there was a critical temperature
range where intra- and extracellular salt concen-
trations exceed 0.8 mol/L during freezing, causing
irreversible damage to RBCs after prolonged
exposure and thawing.49 Support for the theory
of Lovelock that damage to RBCs during freezing
and thawing is the result of solution effects has
been expounded upon by Mazur et al50-52 and Pegg
and Diaper.46,47,53 In the late 1960s, Meryman
provided evidence that RBCs can maintain osmotic
equilibrium until a minimum cell volume is
reached at which time water molecules are
unavailable for exchange and the external osmotic
pressure gradient results in an irreversible change
in membrane permeability, ion leakage, and the
influx of extracellular solute.54 Other evidence
suggests that water loss and volume reduction,
rather than absolute electrolyte concentration, are
responsible for RBC injury that results from slow
cooling, perhaps through a mechanical resistance
to volume change.55,56 In addition to solution
effects injury as the mode of RBC cryoinjury, it
has been proposed that cell damage is a result of
physical forces exerted by interactions with ice
crystals57 and/or the tight packing of RBCs in
unfrozen channels.50,58,59
As the permeability of the plasma membrane to
water is temperature dependent, when cells are
cooled rapidly, the formation of ice in the external
solution and the concentration of extracellular
solutes occur much faster than the efflux of water
from the cell (Fig 2).60 As a result, the cytoplasm
becomes increasingly cooled below the freezing
point (supercooled) with an associated increase in
the probability of intracellular ice nucleation.
Although the mechanism by which intracellular
ice formation (IIF) occurs and the means by which
it damages the cell have not yet been resolved
(reviewed in Ref. 61), the current tenet is that IIF in
cells in suspension is an inherently lethal event that
should be avoided.61-64 In recent years, experi-
mental evidence suggests that dehydration, con-
centration of solutes, and membrane damage
associated with freezing are the primary sources
of RBC cryoinjury, with IIF being innocuous under
specific conditions.65-67
Considering the 2 primary sources of cryoinjury,
optimal RBC survival would be achieved at a
cooling rate that minimizes injury due to both
solution effects and IIF43 (Fig 2). The optimal
cooling rate for RBCs is dependent on the freezing
solution and can be modified by the addition of
chemical cryoprotectants (CPAs).68-70 For exam-
ple, RBCs collected in acid-citrate-dextrose and
frozen in the absence of a cryoprotective agent at
low cooling rates (18C/min to 58C/min) undergo
nearly complete hemolysis (N95%). As cooling
rates increase, hemolysis gradually decreases to a
minimum at 23008C/min. Further increases in
cooling rates result in an accumulation of damage.
Glycerol (10%) effectively reduces RBC cryoin-
jury at low cooling rates (18C/min to 108C/min)
but exerts a damaging effect at high cooling rates
(16008C/min to 20008C/min), whereas dextran
(10%) effectively reduces RBC hemolysis over a
wider range of cooling rates (2.58C/min to
35008C/min).70
In addition to the modes of cryoinjury
already discussed, extensive studies have asso-
ciated cell injury with a wide variety of other
physical and chemical events that occur during
freezing and thawing. Cytoplasmic supercool-
ing,71 ice nucleation and ice crystal morphology
and growth,57,63,72,73 osmotic stress,55,74,75 solute-
related stresses,48,76,77 thermal gradients,78,79 re-
crystallization,80 and/or devitrification81 during
rewarming all affect the post-thaw viability of
cryopreserved cells. The successful cryopreserva-
tion of RBCs is the result of extensive studies to
understand and protect against these interdependent
mechanisms of cryoinjury.
Cryoprotection
The chemicals, or CPAs, that are used for the
cryopreservation of RBC can be classified into 2
major groups based on their mechanism of action
and permeability across the plasma membrane.82,83
The first group, nonpermeating CPAs, include

SCOTT, LECAK, AND ACKER134
sugars, sugar alcohols, polymers, and starches such
as hydroxyethyl starch (HES), polyvinyl pyrroli-
done (PVP), and polyethylene oxide. These CPAs
are usually effective in millimolar concentrations
and generally act by dehydrating the cell at high
subfreezing temperatures, thereby reducing the
incidence of IIF and allowing rapid cooling before
intracellular solute concentrations reach critical
levels.62,82 Extracellular CPAs may also act by
stabilizing membranes and maintaining macro-
molecules in their native form.70,84,85 Some extra-
cellular solutes prevent RBC lysis in hypotonic
environments by promoting RBC leakage of
solutes in response to osmotic stress.56 The second
group of CPAs are those chemicals, like glycerol
and dimethyl sulfoxide, that permeate into cells.
These CPAs protect cells from injury caused by
slow cooling by preventing excessive volume
reduction and the lethal concentration of electro-
lytes, thereby reducing or abolishing the tempera-
ture at which a critical salt concentration is
reached.82,83,86,87 Permeant CPAs act to depress
the freezing point and lower the chemical potential
of a solution, reducing the amount of ice formed at
any given temperature.56,88 Glycerol is an attrac-
tive RBC CPA because it is relatively nontoxic at
high concentrations and readily permeates the cell
at 378C. However, post-thaw removal of glycerol is
necessary to prevent posttransfusion intravascular
hemolysis. Both permeant and nonpermeant CPAs
have been used successfully for the cryopreserva-
tion of RBCs.
Clinical Cryopreservation
After the serendipitous discovery of the cryo-
protective properties of glycerol in 1949 by Polge
et al,89 Smith90 reported in 1950 a method for
freezing whole blood to �798C with the addition
of glycerol that prevented hemolysis and main-
tained normal RBC morphology. In 1951, Mollison
and Sloviter91 successfully transfused human
RBCs diluted with equal parts 30% glycerol-saline
and frozen to �798C for up to 4 hours with
transfusion survival estimates of about 70%. The
inability to add and remove glycerol efficiently and
effectively under sterile conditions with apprecia-
ble recovery prevented the use of frozen blood in a
clinical setting until the early 1960s. The reversible
agglomeration technique of Huggins92 allowed for
the removal of glycerol in a closed system without
use of a centrifuge by aggregating RBCs using
low-ionic-strength, low-pH sugar solutions. How-
ever, this method resulted in poor recovery and an
increased loss of cellular potassium.93 High con-
centrations of glycerol made sedimentation using
manual centrifugal batch washing difficult. Reduc-
ing the glycerol concentration is also problematic
because rapid-freeze techniques and storage at
ultralow temperatures are required to avoid dam-
aging physical changes in ice crystals and second-
ary biologic changes. It was not until the
development of the continuous flow centrifuge
for plasma fractionation that the addition and
removal of high concentrations of glycerol became
possible.94 The ease and rate of sedimentation and
RBC tolerance to hypotonic solutions was further
improved by prewash dilution in hypertonic salt
solutions of decreasing tonicity, preshrinking the
RBCs and increasing their relative density.95
Currently, there are 2 methods clinically used for
the cryopreservation of RBCs: low glycerol/rapid
cooling96-98 and high glycerol/slow cooling.95,99
Low concentrations (15%-20%) of glycerol, rapid
cooling (b1008C/min), storage in liquid nitrogen
(�1968C) or nitrogen vapor (�1658C), with rapid
thawing in a 428C to 458C water bath is used
routinely by European blood banks. In Canada and
the United States, it is more common to use a high
concentration of glycerol (40%) in conjunction
with slow cooling (~18C/min), storage at �808C,and rapid thawing in a 378C water bath for the
cryopreservation of RBCs. In each case, controlled
addition and removal of glycerol is required to
prevent osmotic lysis of the RBCs and/or minimize
recipient exposure to the chemical CPA. Both
methods meet the standards set by the American
Association of Blood Banks requiring RBCs to be
frozen within 6 days of collection or before RBC
expiration with an additive.16,19 Post-thaw process-
ing must ensure adequate removal of the CPA,
minimal hemolysis, and RBC recovery of at least
80% of the original RBC volume after deglyc-
erolization. Deglycerolized RBCs must be stored at
4 8C and transfused within 24 hours of processing
with a 75% in vivo viability, 24 hours posttrans-
fusion, measured using a chromium, double-
labeling technique.
Initially, RBC cryopreservation offered a solu-
tion to the rapid outdating of liquid preserved
RBCs, whereas leukocyte, platelet, and plasma
depletion during storage and processing reduced

Table 2. Areas of RBC Cryopreservation Research
Reviewed in
Vitrification (ice-free cryopreservation) Refs. 68 and 95
Use of extracellular CPAs
(HES, PVP, dextran, albumin)
Refs. 111-114
Use of novel intracellular CPAs
(di- and polysaccharides)
Ref. 129
BIOPRESERVATION OF RBCs 135
the incidence of nonhemolytic febrile reactions,
allergic reactions, and alloimmunization from
transfusions.100 Advances in blood banking includ-
ing leukoreduction, component separation, additive
solutions, and improved donor testing now provide
amore safe and effective RBC product and extended
hypothermic storage. The use of frozen RBCs for
routine clinical use is not economically feasible
because of the labor-intensive, technically demand-
ing nature of processing and low-temperature
storage and the limited 24-hour shelf life of
deglycerolized units.101 As a result, frozen RBC
storage is limited to rare and autologous units and
military applications.102,103
An automated, functionally closed system (ACP
215) for the glycerolization and deglycerolization
of RBC units cryopreserved using 40% (wt/vol)
glycerol has been developed by the Haemonetics
Corporation (Braintree, Mass). The system uses
sterile connectors, inline filters, and a disposable
polycarbonate bowl with an external seal that
allows sequential processing of 2 RBC units.104,105
Acceptable RBC quality is maintained after pro-
cessing and storage up to 15 days in AS-3 at
48C.105 Extended post-deglycerolization storage
would ensure the safety of cryopreserved RBCs
by allowing time for quarantine and donor retesting
before the transfusion of allogeneic RBCs.
There are instances when RBCs stored at 48Cbeyond the regulated expiration date may need to
be cryopreserved, such as with certain rare or
unique RBC units. Biochemical modification of
RBCs with a rejuvenating solution of pyruvate,
inosine, phosphate, and adeneine has been shown
to increase RBC ATP, 2,3-DPG, and p50 levels
after extended hypothermic storage.37 Rejuvena-
tion of RBCs stored with37 or without106 an
additive (AS-1, AS-3, AS-5), cryopreserved,
washed, and stored at 48C for 24 hours show
acceptable in vitro and in vivo survival.
The current direction of RBC cryopreservation
research involves the development of novel meth-
ods to eliminate common problems and limitations
associated with glycerol-preserved RBCs while
accommodating the economic storage and distribu-
tion of a safe and effective product that can be easily
adapted for clinical use (Table 2). The 3 currently
active areas of RBC cryopreservation research
involve ice-free cryopreservation (vitrification),
the use of extracellular CPAs, and the cryoprotec-
tive effect of intracellular sugars (Table 3).
Vitrification of RBCs
The detrimental effects of ice formation can be
eliminated if the formation of ice is completely
avoided. In the context of cryopreservation, vitri-
fication is the process by which an aqueous
solution bypasses ice formation and becomes
an amorphous, glassy solid. By preventing the
formation of a crystalline solid (ice), and the
corresponding intra- and extracellular solute accu-
mulation, this method provides a means to signif-
icantly reduce the damage done to cells, tissues, and
organs during freezing.73,107 However, to vitrify a
sample, high concentrations of CPAs and/or ultra-
rapid cooling rates must be used. Devitrification, or
the formation of ice crystals in an amorphous
sample,108 can occur during suboptimal storage or
slow warming resulting in significant damage to
vitrified biologic systems.109,110
Vitrification is not a new concept as the first
attempts at freezing blood in the 1950s involved
ultra-rapid freezing and thawing of thin films or
droplets of blood, without a CPA additive, in liquid
air or liquid nitrogen with good recovery.68 This
technique allowed for direct collection, thawing,
and transfusion of the bvitrifiedQ RBCs.95 The
extreme cooling and thawing rates were technically
cumbersome and not clinically useful because of
the unsterile nature of the freezing apparatus and
the inability to accommodate freezing of large
volumes of blood. Although the addition of
extracellular solutes such as sugars (dextran),111
polymers (PVP),112 and starches (HES)113 im-
proved recovery at reduced freezing and thawing
rates, intravascular hemolysis after transfusion
resulted from subhemolytic damage.114
The primary obstacles preventing the successful
vitrification of RBCs in suspension is avoiding
toxicity because of the extremely high concen-
trations of CPAs necessary to vitrify suspensions at
a reasonable temperature and rate, and the occur-
rence of devitrification on rewarming. The glass-

SCOTT, LECAK, AND ACKER136
forming tendency of certain alcohols in aqueous
solutions makes them attractive CPAs for use in
vitrification solutions but they are highly toxic at
the high concentrations (30%) required. The
addition of monosaccharides or disaccharides in
low concentrations (4%) has been shown to
neutralize the toxic effects of 35% 2,3-butanediol,
measured by decreased hemolysis after room
temperature storage.115 In addition, sugars readily
form stable glasses, effectively lowering the
required cooling and warming rates by raising the
glass-transition temperature of the solution.115
Although advances in RBC vitrification have not
been as rapid and apparent as the advances in
traditional RBC cryopreservation, they have pro-
vided an important insight into principles of
cryopreservation. However, there are still many
obstacles to overcome for RBC vitrification techni-
ques to be incorporated into transfusion medicine.
Extracellular Cryoprotection
Another alternative approach to traditional RBC
cryopreservation using glycerol is cryopreservation
with extracellular CPAs. The use of cryoprotective
extracellular macromolecules that are biodegrad-
able and well tolerated by the patient, such as some
sugars, polymers and starches, would have multi-
ple advantages. Because the extracellular additives
do not penetrate the RBC membrane, the osmotic
problems associated with the addition and removal
of glycerol would be avoided, and because the
extracellular CPAs are transfusable, the problems
associated with post-thaw deglycerolization would
be alleviated. Moreover, several of the extracellular
CPA colloids can also serve as blood volume
substitutes by immediately normalizing hypovole-
mia in cases of extreme blood loss. Although the
use of several transfusable additives, such as PVP,
dextran, serum albumin, glucose, and trehalose has
been assessed,116-118 HES has been investigated
most intensely as an extracellular RBC CPA.
Hydroxyethyl starch is easily synthesized from
starches, readily metabolized by the body, and
effective as a plasma extender. The results of
single-unit transfusions of HES-cryopreserved
(11.5% wt/wt) washed or unwashed RBCs have
been shown to be comparable to transfusions of
liquid stored RBCs. However, increased concen-
trations of plasma hemoglobin were apparent after
transfusion.119 Furthermore, plasma hemoglobin
levels are significantly higher in the absence of a
post-thaw washing step.119 Previous studies of this
nature indicated low levels of hemoglobinuria
associated with the transfusion of unwashed RBCs
cryopreserved with HES.120 The possibility of
renal toxicity due to increased plasma hemoglobin
resulted in recommendations for a pretransfusion
washing step. The inability to safely and com-
pletely eliminate post-thaw washing, the required
storage in liquid nitrogen or its vapor phase, and a
lack of data to support the safe use of HES in
multiple transfusions have prevented clinical ap-
plication of this extracellular CPA to date.
Cryopreservation Using Intracellular Sugars
An emerging area of cryopreservation research
involves the use of low concentrations of intracel-
lular sugars to stabilize cells during freezing and
thawing. It has been proposed that intracellular
sugars such as trehalose and sucrose protect critical
biologic structures during freezing and thawing
through the formation of a stable glassy ma-
trix,121,122 binding to sites previously stabilized
by water,123 and/or modulating the osmotic re-
sponse of the cells.124,125 In the absence of
conventional CPAs such as dimethyl sulfoxide or
glycerol, low concentrations of intracellular treha-
lose (b0.2 mol/L) has been shown to enhance the
survival of cryopreserved fibroblasts, keratinocytes,
and human oocytes.122,126 The major advantage of
intracellular, nontoxic sugars is the potential to
infuse freeze-thawed cells directly into patients
without the cumbersome steps involved in the
removal of traditional CPAs. Intracellular trehalose
has been used effectively in the cryopreservation of
platelets127 and hematopoietic stem cells.128 Al-
though the successful use of intracellular sugars in
the cryopreservation of RBCs has not been dem-
onstrated to date, it is an active area of research.129
LYOPHILIZATION AND DRY STORAGEOF RBCS
Lyophilization (freeze-drying) involves the re-
moval of most unbound water from biologic
materials through controlled freezing followed by
the sublimation of ice under vacuum.130,131 The
successful desiccation of RBCs and storage in the
dry state would offer numerous practical advan-
tages. Effective lyophilization prevents sample
shrinkage, minimizes chemical changes, and main-
tains product solubility to allow easy rehydration.
The adequate removal of residual moisture would

BIOPRESERVATION OF RBCs 137
accommodate easy storage and transport of a
compact, lightweight product, stable at room
temperature for extended periods. Eliminating the
need for expensive refrigeration devices would
substantially reduce the current cost associated
with the storage and transport of frozen blood
making lyophilized RBCs ideal for remote storage
and military applications. Despite claims to the
contrary,132,133 lyophilization of red cells to mois-
ture contents that facilitate stable storage at room
temperature for indefinite periods has not been
demonstrated to date.
Early work on the lyophilization of RBCs by
Meryman131,134 and MacKenzie and Rapatz135
focused on the use of extracellular agents such
as dextran, PVP, and polyethylene glycol to protect
cells during freezing, drying, and subsequent rehy-
dration. The successful recovery of RBCs after the
removal of up to 92% of the water and encouraging
posttransfusion survival in rats suggested that
clinical use of lyophilized RBC was feasible.134
However, the fragility of the RBC membrane after
the lyophilization process led to significant post-
rehydration lysis and resulted in efforts to desiccate
RBCs being abandoned in the late 1970s.
Efforts to lyophilize RBCs were renewed in the
early 1990s by Goodrich et al.132,133,136 These
authors reported successful rehydration of RBCs
that had been stored at ambient temperatures for
7 days at a low moisture content (1%-2%) with
acceptable maintenance of RBC metabolic, cellu-
lar, and rheologic properties.133 However, upon
further examination, electron micrographs revealed
membrane lesions visible as disruptions or dis-
continuities in the lipid bilayer in more than half
the lyophilized RBC population.136 A loss of
surface area caused by membrane vesiculation
inhibited the cells’ ability to regulate volume
changes in response to water influx after rehydra-
tion.136 In addition, they found that the most
effective lyophilization solutions contained mem-
brane stabilizing agents capable of permeating the
membrane, such as carbohydrates and polyols, as
well as high-molecular-weight polymers.136
Attempts to reproduce the work of Goodrich have
been unsuccessful.137
Engineering Desiccation-Tolerance in RBCs
In natural systems, desiccation is used as a
strategy to preserve biologic activity through times
of extreme environmental stress. Termed anhydro-
biosis, the ability to survive in a dry state for
extended periods has been identified in a variety of
diverse organisms including plants, bacteria, yeast,
nematodes, fungi, and crustaceans (reviewed in
Refs. 138 and 139). Studies of these organisms
have revealed a series of complex molecular and
physiological adaptations that permit survival
despite water loss exceeding 99%. Natural mech-
anisms of protection during desiccation include
scavenging of reactive oxygen species,140,141
down-regulation of metabolism,142,143 and the
accumulation of amphiphilic solutes (reviewed in
Refs. 141,144), proteins (reviewed in Refs.
141,145), and disaccharides.146 These naturally
occurring protective processes are being used as
the foundation for the development of new methods
for the preservation of desiccation-sensitive RBCs.
The best-characterized adaptation used by anhy-
drobiotes to protect biologic structures from envi-
ronmental stresses, including dehydration, cold and
extreme osmolarity, has been the synthesis of intra-
and extracellular disaccharides.138,139,147 In partic-
ular, the synthesis of sugars and sugar alcohols has
been correlated with the survival of organisms held
in the desiccated state (N99% body water lost) for
decades and even centuries. The mechanisms of
sugar protection is an active area of research that
includes the role of the glassy state in long-term
stabilization,121,148 and the interaction of sugars
with biologic molecules and supramolecular struc-
tures to afford stabilization.123,149,150 By incorpo-
rating sugars into preservation media, freeze-drying
(or lyophilization) has been used successfully for
the dehydration and storage of pharmaceutical
agents,151,152 bacteria,153-156 yeast,157-159
viruses,160 and liposomes.161 Current efforts are
focusing on the use of sugars in the desiccation of
nucleated and nonnucleated mammalian cells used
in transfusion and transplantation.
For sugars to be maximally effective at protect-
ing against the damaging effects of dehydration,
they need to be present on both sides of the
membrane.124,125,155,158,161,162 Among the key
impediments to using intracellular sugars in the
preservation of mammalian cells has been the
impermeability of the plasma membrane to these
molecules. Although the accumulation of glucose
via glucose transportors has been used as a means
to increase the desiccation tolerance of human
RBCs,136 the RBC is impermeable to trehalose and
other disaccharides that have been shown to be

SCOTT, LECAK, AND ACKER138
effective at stabilizing biologic structures during
drying. In addition, the amount of intracellular
sugar has been shown to be an important determi-
nant of cell survival after stress.122,126,159,163
Recent work with fibroblasts, keratinocytes, and
murine oocytes suggests that the minimum con-
centration of intracellular trehalose necessary for
freezing and desiccation tolerance is between 100
and 200 mmol/L.122,124,126 The utility of these
sugars for the stabilization of RBCs during drying
rests on the reversible permeabilization of the cell
and loading of suitable concentrations of sugars. A
number of approaches have been used to load
sugars into RBCs including electroporation164,165
and thermal and osmotic shock.166,167
Although the potential benefits are significant,
the technical and scientific challenges facing the
development of clinical and commercial methods
for the desiccation and dry storage of RBCs are
formidable. Although the introduction of intracel-
lular sugars has been shown to improve the survival
of cells after desiccation, little is known about the
mechanisms of damage or the protective effects of
sugars. Careful examinations of the molecular and
biophysical effects of drying and the stabilizing
effects of sugars in the cellular microenvironment
are needed. The basic science of desiccation and
dry storage of RBCs is only now emerging and
many of the issues involved in the translation of this
technology to transfusion medicine has not yet been
addressed. Fortunately, many of the scale-up and
processing issues involved in the desiccation and
dry storage of biologic material have been devel-
oped for the pharmaceutical and food science
industries.168,169 Continued interdisciplinary re-
search efforts are required to further develop this
rapidly emerging area of RBC biopreservation.
CONCLUSIONS
As there exists an enormous need in transfusion
medicine for compatible preservation technologies
that maintains the native function of RBCs for
extended storage periods, efforts to bring current
clinical RBC biopreservation practices in line with
emerging technologies need to be accelerated.
Although the biopreservation techniques devel-
oped in the 1960s have been effective, recent
advances in our understanding of RBC physiol-
ogy, hypothermia, cryoinjury, and desiccation
need to be adapted for use by the transfusion
medicine community. The direction of RBC
biopreservation must focus on methods that
accommodate the economic storage and distribu-
tion of a safe and effective product that can be
easily integrated with current blood banking
practices. As the need for effective preservation
technologies in blood banking will be the motiva-
tion for more concerted efforts in the biopreser-
vation sciences, there are encouraging prospects
for the future of RBC biopreservation.
REFE
RENCES1. Schwabbauer M: Normal erythrocyte production,
physiology and destruction. Clinical hematology: Principles,
procedures and correlations. Philadelphia, Lippincott, 1998,
pp 57 -72
2. Mohandas N, Chasis JA: Red blood cell deformability,
membrane material properties and shape: Regulation by
transmembrane, skeletal and cytosolic proteins and lipids.
Semin Hematol 30:171-192, 1993
3. Derick LH, Liu SC, Chishti AH, et al: Protein immunoloc-
alization in the spread erythrocyte membrane skeleton. Eur J
Cell Biol 57:317-320, 1992
4. Klinken SP: Red blood cells. Int J Biochem Cell Biol
34:1513-1518, 2002
5. Bratosin D, Estaquier J, Ameisen JC, et al: Molecular and
cellular mechanisms of erythrocyte programmed cell death:
Impact on blood transfusion. Vox Sang 83:307-310, 2002
6. Hustin A: Note sur une nouvelle methode de transfusion.
Annales et Bulletin des Seances: Societe des Sciences Medicales
et Naturelles de Bruxelles 72:104-111, 1914
7. Rous P, Turner JR: The preservation of living red blood cells
in vitro. I. Methods of preservation. J Exp Med 23:219-237,
1916
8. Rous P, Turner JR: The preservation of living red blood
cells in vitro II. The transfusion of kept cells. J Exp Med
23:239-248, 1916
9. Mollison PL: The introduction of citrate as an anticoag-
ulant for transfusion and of glucose as a red cell preservative. Br
J Haematol 108:13-18, 2000
10. Douzou P: Cryobiochemistry: An introduction. New
York, Academic Press, 1977, pp 1 -286
11. Taylor MJ: Physico-chemical principles in low tempera-
ture biology, in Grout BWW, Morris GJ (eds): The effects of
low temperatures on biological systems. London, Edward
Arnold Ltd, 1987, pp 3 -71
12. Bishop C: Some in vitro effects of adenine added to stored
blood. Transfusion 4:265-270, 1964
13. Brewer GJ, Powell RD: The adenosine triphosphate
content of glucose-6-phosphate dehydrogenase-deficient and
normal erythrocytes, including studies of a glucose-6-phosphate
dehydrogenase-deficient man with belevated erythrocytic ATP Q.J Lab Clin Med 67:726-740, 1966
14. Haradin AR, Weed RI, Reed CF: Changes in physical
properties of stored erythrocytes: Relationship to survival in
vivo. Transfusion 9:229-237, 1969

BIOPRESERVATION OF RBCs 139
15. Card RT: Red cell membrane changes during storage.
Transfus Med Rev 2:40 -47, 1988
16. Hess JR, Greenwalt TJ: Storage of red blood cells: New
approaches. Transfus Med Rev 16:283-295, 2002
17. Valeri CR, Collins FB: Physiologic effects of 2,3-DPG–
depleted red cells with high affinity for oxygen. J Appl Physiol
31:823-827, 1971
18. Beutler E: Back to the future in RBC preservation.
Transfusion 40:983-985, 2000
19. Fridey SL (ed): Standards for blood banks and transfusion
services. Bethesda, MD, American Association of Blood Banks,
2003, pp 161-163
20. Moore GL: Additive solutions for better blood preserva-
tion. CRC Crit Rev Clin Lab Sci 25:211-229, 1987
21. Harmening DM: Modern blood banking and transfusion
practices. Philadelphia, PA, F.A. Davis Company, 1999, pp 9 -11
22. Hfgman CF: Preparation and preservation of red cells.
Vox Sang 74:177-187, 1998
23. Hfgman CF: Liquid-stored red blood cells for transfusion:
A status report. Vox Sang 76:67 -77, 1999
24. Beutler E: Preservation of liquid red cells, in Rossi EC,
Simon TL, Moss GS (eds): Principles of transfusion medicine.
Baltimore, Williams & Wilkins, 1991, pp 47 -56
25. Hfgman CF, Meryman HT: Storage parameters affecting
red blood cell survival and function after transfusion. Transfus
Med Rev 13:275-296, 1999
26. Martin CM, Sibbald WJ, Lu X, et al: Age of transfused
red blood cells is associated with ICU length of stay. Clin Invest
Med 17:B21, 1994
27. Marik PE, Sibbald WJ: Effect of stored-blood transfu-
sion on oxygen delivery in patients with sepsis. JAMA 269:
3024-3029, 1993
28. Blajchman MA: Immunomodulation and blood transfu-
sion. Am J Ther 9:389-395, 2002
29. Leal-Noval SR, Jara-Lopez I, Garcia-Garmndia JL, et al:
Influence of erythrocyte concentrate storage time on post-
surgical morbidity in cardiac surgery patients. Anesthesiology
98:815-822, 2003
30. Zallen G, Offner PJ, Moore EE, et al: Age of transfused
red blood cells is an independent risk factor for postinjury
multiple organ failure. Am J Surg 178:570-572, 1999
31. Vamvakas EC, Taswell HF: Long-term survival after
blood transfusion. Transfusion 34:471-477, 1994
32. Whyte GS: The transfused population of Canterbury, New
Zealand and its mortality. Vox Sang 54:65 -70, 1988
33. Purdy FR, Tweeddale MG, Marrick PM: Association of
mortality with age of blood transfused in septic ICU patients.
Can J Anaesth 44:1256 -1261, 1997
34. Ho J, Sibbald WJ, Chin-Yee IH: Effects of storage on
efficacy of red cell transfusion: When is it not safe? Crit Care
Med 31:S687-S697, 2003
35. Bratosin D, Estaquier J, Ameisen JC, et al: Molecular
and cellular mechanisms of erythrocyte programmed cell
death: Impact on blood transfusion. Vox Sang 83:307-310
2002 (suppl 1)
36. Walker WH, Netz M, Ganshirt KH: 49 day storage of
erythrocyte concentrates in blood bags with the PAGGS-
mannitol. Beitr Infusionsther 26:55 -59, 1990
37. Valeri CR, Pivacek LE, Cassidy GP, et al: The survival,
function and hemolysis of human RBCs stored at 4 8C in
additive solution (AS-1, AS-3 or AS-5) for 42 days and then
biochemically modified, frozen, thawed, washed and stored at
4 8C in sodium chloride and glucose solution for 24 hours.
Transfusion 40:1341 -1345, 2000
38. Hamasaki N, Yamamoto M: Red blood cell function and
blood storage. Vox Sang 79:191-197, 2000
39. Valeri CR: Status report on the quality of liquid and
frozen red blood cells. Vox Sang 83:193-196, 2002
40. Mazur P: Basic problems in cryobiology, in Timmerhaus
KD (ed): Advances in cryogenic engineering, vol 9. New York,
Plenum Press, 1964, pp 28-37
41. Lecak J, Scott K, Young C, et al: Evaluation of red blood
cells stored at �80 8C in excess of 10 years. Transfusion
44:1306-1313, 2004
42. Valeri CR, Ragno G, Pivacek LE, et al: An experiment
with glycerol-frozen red blood cells stored at �80 8C for up to
37 years. Vox Sang 79:168-174, 2000
43. Mazur P, Leibo SP, Chu EHY: A two-factor hypothesis of
freezing injury: Evidence from Chinese hamster tissue-culture
cells. Exp Cell Res 71:345-355, 1972
44. Meryman HT: The exceeding of a minimum tolerable cell
volume in hypertonic suspension as a cause of freezing injury, in
Wolstenholme GE, Connor M (eds): The frozen cell. London
Churchill, 1970, pp 51 -64
45. Zade-Oppen AMM: Posthypertonic hemolysis in sodium
chloride systems. Acta Physiol Scand 73:341-364, 1968
46. Pegg DE, Diaper MP: The effect of initial tonicity on
freeze/thaw injury to human red cells suspended in solutions of
sodium chloride. Cryobiology 28:18 -35, 1991
47. Pegg DE, Diaper MP: On the mechanism of injury to
slowly frozen erythrocytes. Biophys J 54:471-488, 1988
48. Lovelock JE: The denaturation of lipid-protein complexes
as a cause of damage by freezing. Proc R Soc Lond B 147:427-
434, 1957
49. Lovelock JE: The haemolysis of human red blood cells
by freezing and thawing. Biochim Biophys Acta 10:414-426,
1953
50. Mazur P, Cole KW: Influence of cell concentration on the
contribution of unfrozen fraction and salt concentration to the
survival of slowly frozen human erythrocytes. Cryobiology
22:509-536, 1985
51. Mazur P, Rigopoulos N: Contributions of unfrozen
fraction and of salt concentration to the survival of slowly
frozen human erythrocytes: Influence of warming rate. Cryobi-
ology 20:274-289, 1983
52. Mazur P, Rall WF, Rigopoulos N: Relative contributions
of the fraction of unfrozen water and of salt concentration to the
survival of slowly frozen human erythrocytes. Biophys J
36:653-675, 1981
53. Pegg DE, Diaper MP: The bunfrozen fractionQ hypothesisof freezing injury to human erythrocytes: A critical examination
of the evidence. Cryobiology 26:30 -43, 1989
54. Meryman HT: Modified model for the mechanism
of freezing injury in erythrocytes. Nature 218:333-336,
1968
55. Meryman HT: Osmotic stress as a mechanism of freezing
injury. Cryobiology 8:489-500, 1971
56. Meryman HT: Freezing injury and its prevention in living
cells. Annu Rev Biophys 3:341-363, 1974
57. Ishiguro H, Rubinsky B: Mechanical interactions between
ice crystals and red blood cells during directional solidification.
Cryobiology 31:483-500, 1994

SCOTT, LECAK, AND ACKER140
58. Nei T: Mechanism of freezing injury to erythrocytes:
Effect of initial cell concentration on the post-thaw hemolysis.
Cryobiology 18:229-237, 1981
59. Pegg DE: The effect of cell concentration on the recovery
of human erythrocytes after freezing and thawing in the
presence of glycerol. Cryobiology 18:221-228, 1981
60. Mazur P: Kinetics of water loss from cells at subzero
temperatures and the likelihood of intracellular freezing. J Gen
Physiol 47:347-369, 1963
61. Karlsson JOM, Cravalho EG, Toner M: Intracellular ice
formation: Causes and consequences. Cryo Letters 14:323-334,
1993
62. Mazur P: Freezing of living cells: Mechanisms and
implications. Am J Physiol 247:C125-C142, 1984
63. Toner M: Nucleation of ice crystals inside biological
cells, in Stenponkus PL (ed): Advances in low temperature
biology, vol 2. London, JAI Press Ltd, 1993, pp 1-51
64. Muldrew K, McGann LE: Mechanisms of intracellular ice
formation. Biophys J 57:525-532, 1990
65. Muldrew K, Acker JP, Elliott JAW, et al: The water to ice
transition: Implications for living cells, in Fuller BJ, Lane N,
Benson EE (eds): Life in the frozen state. New York, CRC
Press, 2004, pp 67-108
66. Acker JP, McGann LE: Innocuous intracellular ice
improves survival of frozen cells. Cell Transplant 11:563-571,
2002
67. Fowler R, Toner M: Prevention of hemolysis in rapidly
frozen erythrocytes by using a laser pulse. Ann N Y Acad Sci
858:245-252, 1998
68. Luyet B, Rapatz G: A review of basic researches on the
cryopreservation of red blood cells. Cryobiology 6:425-482,
1970
69. Scheiwe MW, Nick HE, Kfrber C: An experimental study
on the freezing of red blood cells with and without hydroxyethyl
starch. Cryobiology 19:461-477, 1982
70. Rapatz G, Sullivan JJ, Luyet BJ: Preservation of
erythrocytes in blood containing various cryoprotective agents,
frozen at various rates and brought to a given final temperature.
Cryobiology 5:18 -25, 1968
71. Diller KR: Intracellular freezing: Effect of extracellular
supercooling. Cryobiology 12:480-485, 1975
72. Karlsson JOM, Cravalho EG, Borel Rinkes IHM, et al:
Nucleation and growth of ice crystals inside cultured hepato-
cytes during freezing in the presence of dimethyl sulfoxide.
Biophys J 65:2524-2536, 1993
73. Luyet BJ, Gehenio PM: The mechanism of injury and
death by low temperature. Biodynamica 3:33-99, 1940
74. Steponkus PL, Wolfe J, Dowgert MF: Stresses induced by
contraction and expansion during a freeze-thaw cycle: A
membrane perspective, in Morris GJ, Clarke A (eds): Effects
of low temperatures on biological membranes. Toronto,
Academic Press, 1981, pp 307-322
75. Muldrew K, McGann LE: The osmotic rupture hypothesis
of intracellular freezing injury. Biophys J 66:532-541, 1994
76. Levitt J: A sulfhydryl-disulfide hypothesis of frost injury
and resistance in plants. J Theor Biol 3:355-391, 1962
77. Karow AM, Webb WR: Tissue freezing: A theory for
injury and survival. Cryobiology 2:99 -108, 1965
78. Farrant J, Morris GJ: Thermal shock and dilution shock
as the causes of freezing injury. Cryobiology 10:134-140,
1973
79. Lovelock JE: Haemolysis by thermal shock. Br J
Haematol 1:117-129, 1955
80. Forsyth M, MacFarlane DR: Recrystallization revisited.
Cryo Letters 7:367-378, 1986
81. Karlsson JOM: A theoretical model of intracellular
devitrification. Cryobiology 42:154-169, 2001
82. Meryman HT: Cryoprotective agents. Cryobiology 8:
173 -183, 1971
83. McGann LE: Differing actions of penetrating and non-
penetrating cryoprotective agents. Cryobiology 15:382 -390,
1978
84. Crowe JH, Crowe LM, Carpenter JF, et al: Interactions of
sugars with membranes. Biochim Biophys Acta 947:367-384,
1988
85. Anchordoguy TJ, Rudolph AS, Carpenter JF, et al: Modes
of interaction of cryoprotectants with membrane phospholipids
during freezing. Cryobiology 24:324-331, 1987
86. Lovelock JE: The mechanism of the protective action of
glycerol against haemolysis by freezing and thawing. Biochim
Biophys Acta 11:28 -36, 1953
87. Lovelock JE: The protective action of neutral solutes
against haemolysis by freezing and thawing. Biochem J 56:
265 -270, 1954
88. Mazur P: Cryobiology: The freezing of biological
systems. Science 168:939-949, 1970
89. Polge C, Smith AU, Parkes AS: Revival of spermatozoa
after vitrification and dehydration at low temperatures. Nature
164:666, 1949
90. Smith AU: Prevention of hemolysis during freezing and
thawing of red blood cells. Lancet 2:910, 1950
91. Mollison PL, Sloviter HA: Successful transfusion of
previously frozen human red cells. Lancet 10:862-864, 1951
92. Huggins CE: Reversible agglomeration: A practical
method for removal of glycerol from frozen blood, in Spielmann
W, Seidl S (eds): Modern problems in blood preservation.
Stuggart, Fischer Verlag, 1970, pp 138-155
93. Valeri CR, Runck AH, Brodine CE: Recent advances in
freeze-preservation of red blood cells. JAMA 208:489-492,
1969
94. Haynes LL, Tulis JL, Pyle HM, et al: Clinical use of
deglycerolized frozen blood. JAMA 173:1657, 1960
95. Meryman HT, Hornblower M: A method for freezing and
washing red blood cells using a high glycerol concentration.
Transfusion 12:145-156, 1972
96. Rowe AW, Eyster E, Kellner A: Liquid nitrogen
preservation of red blood cells for transfusion: A low
glycerol-rapid freeze procedure. Cryobiology 5:119 - 128,
1968
97. Krijnen HW, De Wit JJ, Kuivenhoven CJ, et al: Glycerol
treated human red cells frozen with liquid nitrogen. Vox Sang
9:559-572, 1964
98. Pert JH, Moore R, Schork PK: Low-temperature
preservation of human erythrocytes: Biochemical and clinical
aspects. Bibl Haematol 19:47 -53, 1965
99. Tullis JL, Kethel MM, Pyle HM, et al: Studies on the in
vivo survival of glycerolized and frozen human red blood cells.
JAMA 168:399-404, 1958
100. Meryman HT: Frozen red cells. Transfus Med Rev
3:121-127, 1989
101. Hess JR: Red cell freezing and its impact on the supply
chain. Transfus Med 14:1 -8, 2004

BIOPRESERVATION OF RBCs 141
102. Hess JR, Thomas MJG: Blood use in war and disaster:
Lessons from the past century. Transfusion 43:1622 -1633, 2003
103. Lelkens CC, Noorman F, Koning JG, et al: Stability after
thawing of RBCs frozen with high- and low-glycerol method.
Transfusion 43:157-164, 2003
104. Valeri CR, Ragno G, Pivacek LE, et al: In vivo survival
of apheresis RBCs, frozen in 40-percent (wt/vol) glycerol and
stored after deglycerolization for 15 days at 4 8C in AS-3 for up
to 21 days. Transfusion 41:933-939, 2001
105. Valeri CR, Ragno G, Pivacek LE, et al: A multicenter
study of in vitro and in vivo values in human RBCs frozen with
40-percent (wt/vol) glycerol and stored after deglycerolization
for 15 days at 4 degrees C in AS-3: Assessment of RBC
processing in the ACP 215. Transfusion 41:933-939, 2001
106. Valeri CR, Zaroulis CG, Vecchione JJ, et al: Therapeutic
effectiveness and safety of outdated human red blood cells
rejuvenated to restore oxygen transport function to normal,
frozen for 3 to 4 years at �80 C, washed, and stored at 4 C for
24 hours prior to rapid infusion. Transfusion 20:159-170, 1980
107. Fahy GM, MacFarlane DR, Angell CA, et al:
Vitrification as an approach to cryopreservation. Cryobiology
21:407-426, 1984
108. MacFarlane DR: Devitrification in glass-forming aque-
ous solutions. Cryobiology 23:230-244, 1986
109. Fahy GM, Levy DI, Ali SE: Some emerging principles
underlying the physical properties, biological actions and utility
of vitrification solutions. Cryobiology 24:196-213, 1987
110. Pegg DE: Ice crystals in tissues and organs, in Pegg DE,
Karow Am (eds): The biophysics of organ cryopreservation
147:117 -140, 1997
111. Strumia MM, Colwell LS, Strumia PV: The preservation
of blood for transfusion. V. Post-transfusion survival of red cells
modified with sugars, frozen, and stored in the frozen state. J
Clin Med 56:587-593, 1963
112. Bloom ML, Witebski E, Rinfret AP, et al: Rapidly, hard-
frozen blood: Evaluation of progress and clinical survival. Bibl
Haematol 23:642-645, 1965
113. Knorpp CT, Merchant WR, Gikas PW, et al: Hydrox-
yethyl starch: Extracellular cryophylactic agent for erythrocytes.
Science 157:1312-1313, 1967
114. Williams RJ: The surface activity of PVP and other
polymers and their antihemolytic capacity. Cryobiology
20:521-526, 1983
115. Boutron P, Peyridieu J: Reduction in toxicity for red
blood cells in buffered solutions containing high concentrations
of 2,3-butanediol by trehalose, sucrose, sorbitol or mannitol.
Cryobiology 31:367-373, 1994
116. Pellerin-Mendes C, Million L, Marchand-Arvier M, et
al: In vitro study of the protective effect of trehalose and dextran
during freezing of human red blood cells in liquid nitrogen.
Cryobiology 35:173-186, 1997
117. Strumia MM, Strumia PV: Recovery and survival of
human red cells frozen with albumin, dextran and lactose-
albumin. Bibl Haematol 19:61 -68, 1964
118. Meryman HT: Freezing and vitrification of red cells,
recollections and predictions, in Sibinga S, Cash JD (eds):
Transfusion medicine: Quo vadis? Boston, Kluwer Academic,
2001, pp 69-85
119. Horn E-P, Sputtek A, Standl T, et al: Transfusion of
autologous, hydroxyethyl starch-cryopreserved red blood cells.
Anesth Analg 85:739-745, 1997
120. Sputtek A, Singbartl G, Langer R, et al: Cryopreserva-
tion of red blood cells with the non-penetrating cryoprotectant
hydroxyethyl starch. Cryo Letters 16:283-288, 1995
121. Crowe JH, Carpenter JF, Crowe LM: The role
of vitrification in anhydrobiosis. Annu Rev Physiol 60:73 -103,
1998
122. Eroglu A, Russo MJ, Bieganski R, et al: Intracellular
trehalose improves the survival of cryopreserved mammalian
cells. Nat Biotechnol 18:163-167, 2000
123. Crowe JH, Crowe LM, Carpenter JF: Preserving dry
biomaterials: The water replacement hypothesis. Part 1.
Biopharm 4:28 -33, 1993
124. Chen T, Acker JP, Eroglu A, et al: Beneficial effect of
intracellular trehalose on the membrane integrity of dried
mammalian cells. Cryobiology 43:168-181, 2001
125. Acker JP, Fowler A, Lauman B, et al: Survival of
desiccated mammalian cells: Beneficial effects of isotonic
media. Cell Preserv Technol 1:129-140, 2002
126. Eroglu A, Toner M, Toth TL: Beneficial effect of
microinjected trehalose on the cryosurvival of human oocytes.
Fertil Steril 77:152-158, 2002
127. Wolkers WF, Walker NJ, Tablin F, et al: Human platelets
loaded with trehalose survive freeze-drying. Cryobiology
42:79 -87, 2001
128. Buchanan SS, Gross SA, Acker JP, et al: Cryopreser-
vation of stem cells using trehalose: Evaluation of the method
using a human hematopoietic cell line. Stem Cells Dev 13:
295 -305, 2004
129. Brumfiel G: Just add water. Nature 428:14-15, 2004
130. MacKenzie AP: The physico-chemical basis for the
freeze-drying process. Dev Biol Stand 36:51 -67, 1977
131. Meryman HT: Freeze-drying, in Meryman HT (ed):
Cryobiology. New York, Academic Press, 1966, 609 -663
132. Goodrich RP, Sowemimo-Coker SO, Zerez CR, et
al: Preservation of metabolic activity in lyophilized human
erythrocytes. Proc Natl Acad Sci U S A 89:967-971,
1992
133. Sowemimo-Coker SO, Goodrich RP, Zerez CR, et al:
Refrigerated storage of lyophilized and rehydrated, lyophilized
human red cells. Transfusion 33:322-329, 1993
134. Meryman HT: Drying of living mammalian cells. Ann
N Y Acad Sci 85:729-739, 1960
135. MacKenzie AP, Rapatz GL: Freeze-drying preservation
of human erythrocytes. Cryobiology 8:384, 1971
136. Goodrich RP, Sowemimo-Coker SO: Freeze-drying of
red blood cells, in Steponkus PL (ed): Advances in Low
Temperature Biology, vol 2. London, JAI Press Ltd, 1993,
pp 53 -99
137. Spieles G, Heschel I, Rau G: An attempt to recover
viable human red blood cells after freeze-drying. Cryo Letters
17:43 -52, 1996
138. Crowe JH, Hoekstra FA, Crowe LM: Anhydrobiosis.
Annu Rev Physiol 54:579-599, 1992
139. Leopold AC: Membranes, metabolism and dry organ-
isms. Ithaca, Cornell University Press, 1986, pp 374
140. Ingram I, Bartels D: The molecular basis of dehydration
tolerance in plants. Annu Rev Plant Physiol Plant Mol Biol
47:377-403, 1996
141. Oliver AE, Leprince O, Wolkers WF, et al: Non-
disaccharide–based mechanisms of protection during drying.
Cryobiology 43:151-167, 2001

SCOTT, LECAK, AND ACKER142
142. Hand SC, Podrabsky JE: Bioenergetics of diapause and
quiescence in aquatic animals. Thermochim Acta 349:31-42,
2000
143. Hand SC, Hardewig I: Down-regulation of cellular
metabolism during environmental stress: Mechanisms and
implications. Annu Rev Physiol 58:539-563, 1996
144. Rice-Evans CA, Miller NJ, Paganga G: Antioxidant
properties of phenolic compounds. Trends Plant Sci 2:152-159,
1997
145. Blackman SA, Obendorf RL, Leopold AC: Desiccation
tolerance in developing soybean seeds: The role of stress
proteins. Physiol Plant 93:630-638, 1995
146. Crowe LM: Lessons from nature: The role of sugars
in anhydrobiosis. Comp Biochem Physiol, A 131:505-513,
2002
147. Storey KB, Storey BT: Physiology, biochemistry and
molecular biology of vertebrate freeze tolerance: The wood frog,
in Fuller BJ, Lane N, Benson EE (eds): Life in the frozen state.
New York, CRC Press, 2004, pp 234-274
148. Wolfe J, Bryant G: Freezing, drying, and/or vitrification
of membrane-solute-water systems. Cryobiology 39:103-129,
1999
149. Gaber BP, Chandrasekhar I, Pattabiraman N: The
interaction of trehalose with the phospholipid bilayer: A
molecular modeling study, in Leopold AC (ed): Membranes,
metabolism and dry organisms. Ithaca, Cornell University Press
NY, 1986, pp 231-241
150. Crowe JH, Crowe LM, Carpenter JF: Preserving dry
biomaterials: The water replacement hypothesis. Part 2.
Biopharm 5:40 -43, 1993
151. Franks F: Thermomechanical properties of amorphous
saccharides: Their role in enhancing pharmaceutical product
stability. Biotechnol Genet Eng Rev 16:281-292, 1999
152. Kreilgaard L, Frokjaer S, Flink JM, et al: Effects of
additives on the stability of recombinant human factor XIII
during freeze-drying and storage in the dried solid. Arch
Biochem Biophys 360:121 -134, 1998
153. Billi D, Wright DH, Helm RF, et al: Engineering
desiccation tolerance in Escherichia coli. Appl Environ Micro-
biol 66:1680-1684, 2000
154. Israeli E, Shaffer BT, Lighthart B: Protection of freeze-
dried Escherichia coli by trehalose upon exposure to environ-
ment conditions. Cryobiology 30:519-523, 1993
155. Leslie SB, Israeli E, Lighthart B, et al: Trehalose and
sucrose protect both membranes and proteins in intact
bacteria during drying. Appl Environ Microbiol 61:3592-3597,
1995
156. Potts M: Desiccation tolerance of prokaryotes. Microbiol
Rev 58:755-805, 1994
157. Leslie SB, Teter SA, Crowe LM, et al: Trehalose lowers
membrane phase transitions in dry yeast cells. Biochim Biophys
Acta 1192:7 -13, 1994
158. Cerrutti P, Segovia de Huergo M, Galvagno M, et al:
Commercial baker’s yeast stability as affected by intracellular
content of trehalose, dehydration procedure and the physical
properties of external matrices. Appl Microbiol Biotechnol
54:575-580, 2000
159. Slaughter JC, Nomura T: Intracellular glycogen and
trehalose contents as predictors of yeast viability. Enzyme
Microb Technol 14:64 -67, 1992
160. Bieganski RM, Fowler A, Morgan JR, et al: Stabilization
of active recombinant retroviruses in an amorphous dry state
with trehalose. Biotechnol Prog 14:615-620, 1998
161. Crowe LM, Crowe JH, Rudolph AS, et al: Preservation
of freeze-dried liposomes by trehalose. Arch Biochem Biophys
242:240-247, 1985
162. Garcia de Castro A, Lapinski J, Tunnacliffe A:
Anhydrobiotic engineering. Nat Biotechnol 18:473, 2000
163. Garcia de Castro A, Tunnacliffe A: Intracellular
trehalose improves osmotolerance but not desiccation tolerance
in mammalian cells. FEBS Lett 487:199-202, 2000
164. Kinosita K, Tsong TY: Formation and resealing of pores
of controlled sizes in human erythrocyte membrane. Nature
268:438-441, 1977
165. Kinosita K, Tsong TY: Survival of sucrose-loaded
erythrocytes in the circulation. Nature 272:258-260, 1978
166. Franco RS, Barker R, Novick S, et al: Effect of inositol
hexaphosphate on the transient behavior of red cells following a
DMSO-induced osmotic pulse. J Cell Physiol 129:221-229,
1986
167. Harrison M, Isaacson C, Rathinavelu P, et al: Resealing
of protein tyrosine kinase substrates into human erythrocytes by
rapid freezing and thawing in liquid nitrogen, in Magnani M,
DeLoach JR (eds): The use of resealed erythrocytes as carriers
and bioreactors, vol 326. New York, Plenum Press, 1992,
pp 111-118
168. Levine H: Amorphous food and pharmaceutical systems.
Cambridge, Royal Society of Chemistry, 2002, pp 1-351
169. Rahman S, Rahman MS: Handbook of food preserva-
tion. New York, Marcel Dekker, 1999, pp 1-809