Embed Size (px)
Citation preview

2/19/2015
1
Biopsy Techniques SHELLIE D. HILL DNP, RN, FNP-BC
Biopsy Techniques
Incisional biopsy - skin is removed using scalpel incision. This may involve taking part of the skin or removing a complete skin lesion
(excision biopsy).
Punch biopsy, which involves taking a small disc of full thickness skin
using a special punch biopsy instrument.
Shave biopsy, which involves removal of protruding, superficial skin
lesions.
Biopsy Techniques
Incisional biopsy
If the lesion is large and malignancy is not suspected it is acceptable to
perform an incomplete excision. This is often called an incision or
incisional biopsy. It is usually recommended that the specimen include
an area of normal skin.
An excisional biopsy should aim to remove the whole lesion, especially
if malignancy is suspected, with an edge or margin of normal skin
included around the lesion.

2/19/2015
2
Excisional Biopsy
Ellipse of skin has to be removed to obtain satisfactory closure. The long
axis of the ellipse should be in the direction to produce the best scar.
Langer's lines are a useful guide but wrinkle and contour lines (relaxed
skin tension lines) are also important.
Remember that lesions have three dimensions and it is important to
biopsy deeply enough, usually including some subcutaneous fat.
Close with a few neat Vicryl (nylon) sutures.
Be careful not to crush the specimen.
Rutowski, P., Zdzienicki, M., Zbigniew, N., & Van Akkooi, A. (2010). Surgery of Primary Melanomas. Cancers, 2(2), 824-841. doi: 10.3390/cancers2020824
3 to 1 length-to-width ratio
anesthetized with 1% lidocaine with or
without epinephrine.
30-gauge needle for patient comfort.
#15 scalpel blade held vertical to the skin. Don’t inward bevel. The first pass of the
scalpel on each wound edge should be smooth and continuous to prevent notching of the skin. A second pass of the blade may
be needed to extend these incisions down to the level of the fat.
Lift central island of skin with forceps and cut with scalpel.
Biopsy Techniques
Punch biopsy
punch biopsy is used when a full thickness biopsy is needed – usually
used for benign rashes and skin disorders to assist diagnosis.
Come in various sizes
A 4 mm punch is sufficient for non-facial lesions.
In granulomatous conditions or conditions with atypical features, 5
mm biopsies are preferred.
Biopsies of less than 3 mm may be difficult to process for histology.

2/19/2015
3
Punch biopsy
1. local anesthesia
2. stretch the skin at 90° to the tension lines
3. Rotate the skin punch into the dermis, being sure to obtain an
adequately deep specimen. Remove the punch when it enters the
subcutaneous fat
4. Raise the specimen above the incision. A 21 gauge needle is
advised rather than forceps that may crush the specimen
5. Cut the specimen free with iris scissors.
6. Close the wound if needed - A punch of 3 mm does not require a
suture but a larger one will need 1 or 2 sutures
Punch biopsy
Punch biopsy
Zuber, T. J. (2002). Punch Biopsy of the
Skin. American Family Physician, 65(6), 1155-1158.
Biopsy Techniques
Shave Biopsy
This is used with protruding skin lesions such as:
Skin tags
Actinic kertoses
Seborrhoeic keratoses
This type of biopsy is not appropriate for suspicious pigmented
lesions.
It usually requires local anesthetic.

2/19/2015
4
Shave biopsy
No suturing needed
Hemostasis is usually obtained with
aluminum chloride 20% solution or silver nitrate
Don’t crush specimen
(Pickett, 2011)
Anesthetic
Anesthetic Maximum Onset duration
Lidocaine 1% 4.5mg/kg (2 mg/lb.)
5-10 min 45-60 min
Lidocaine 1% with epinephrine
Do Not use on distal extremities, nose or penis.
7 mg/kg (3.5 mg/lb.)
5-7 min 1-2 hours
Suture Types
Suture type description Use for
Ethilon (nylon) Black, non-absorbable Good for wounds with tension – also good for
face if going non-absorbable
Prolene Like Ethilon but blue in color
Good for thick, dark eyebrows or hairy areas
Absorbable –natural (fast absorbing gut)
Absorbs 3-5 days, may cause reaction
Fine skin areas with low tension (lips/vermilion
border, mucous mem.
Vicryl absorbable - synthetic
Synthetic, can take up to 2 weeks for absorption
Deep sutures to get initial alignment and eliminate
surface tension
Staples Very strong Scalp
2/19/2015
5
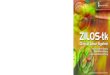
Suture guide
Body Region Suture type Removal
Scalp 5-0 or 4-0 or staples 5-7 days
Face 6-0 3-5 days
Eyelid 6-0 or 7-0 3-5 days
Eyebrow 6-0 or 5-0 3-5 days
Trunk 5-0 or 4-0 5-7 days
Extremities 5-0 or 4-0 7 days
Joint surface 4-0 10-14 days
Hand 5-0 7 days
Foot/Sole 4-0 or 3-0 7-10 days
References:
Nischal, U., K., N., & Khopkar, U. (2008). Techniques of skin biopsy and practical considerations. Journal of Cutaneous Aesthetic Surgery, 1(2), 107-111.
Pickett, H. (2011). Shave and Punch Biopsies for Skin Lesions. American Family Physician, 84(9), 995-1002.
Rutowski, P., Zdzienicki, M., Zbigniew, N., & Van Akkooi, A. (2010). Surgery of Primary
Melanomas. Cancers, 2(2), 824-841. doi: 10.3390/cancers2020824
Semer, N. (2007). Practical Plastic Surgery for Nonsurgeons: Hanley and Belfus.
Zuber, T. J. (2002). Punch Biopsy of the Skin. American Family Physician, 65(6), 1155-
1158.

2/19/2015
1
Common
Dermatological
Issues in Primary
Care SHELLIE D. HILL DNP, RN, FNP-BC
General dermatology points
You must see the rash to diagnose the rash.
Be descriptive in documentation using proper definitions: macular,
bullae, confluent, diffuse, grouped etc.
Biopsy early if unsure of diagnosis especially if you think you will refer
the patient.
Be aware that all types of skin cancer are on the rise. There has
been an alarming increase of melanoma in people aged 18-39.
Acne

2/19/2015
2
Acne - pathogenesis
Follicular keratinization: keratin
becomes dense and blocks
secretion of sebum. These plugs
are called comedones (closed
and open)
Comedones interact with
androgens and bacteria (P.
acnes) leading to inflammation.
The distended follicle wall breaks
and the leaked contents into the
dermis lead to more inflammation
and foreign-body response
(papule, pustule, nodule)
Contributing factors:
Drugs (Lithium, glucocorticoids,
androgens)
Emotional stress
Occlusion and pressure on the skin
NOT caused by foods - ? milk
Acne - management
Mild acne:
Comedones are best treated with
topical retinoids (tretinoin,
adapalene)
Topical antibiotics (clindamycin and
erythromycin)
Benzoyl peroxide (good anti-
P.acnes)
Combination therapy is best (Benzoyl
peroxide + erythromycin gels PLUS
topical retinoids
Moderate acne:
Continue topical treatment and add
oral antibiotics (minocycline, doxy)
Consider oral contraception or
spironolactone
Acne - management
Severe acne - nodulocystic
Continue topical treatment and refer
to dermatologist for Isotretinoin.
Some ongoing studies on laser
treatments

2/19/2015
3
Rosacea
Chronic inflammation + increased
reactivity of capillaries
Preluded by episodic flushing and
blushing
Stage I – persistent erythema with
telangiectasia
Stage II – persistent erythema,
telangiectasia, papules and tiny
pustules
Stage III – persistent dark erythema,
dense telangiectasia, papules,
pustules, nodules
Rosacea
Acneiform but key differences in
rosacea vs. acne vulargis
May be associated with
rhinophyma from marked
sebaceous gland hyperplasia and
fibrosis
May be associated with red eye
as a result of chronic blepharitis
Rosacea
Traditional treatments
Topical metronidazole (first line for
most), Azelaic acid, pimecrolimus
cream, sulfacetamide cream
Oral antibiotics for papulopustular–
minocycline, doxy or tetracycline
Oral Isotretinoin in severe disease
Rhinophyma and telangiectasia
respond well to laser treatments

2/19/2015
4
Rosacea
New treatments
Many new are emerging
Pathogenesis now thought to be
bacterial produced from
Demodex mites
Topical Ivermectin
Brimonidine tartrate 0.33% gel – treats
erythema
Topical sodium sulfacetamide 10%
with sulfur 5% - good for inflammation
and erythema
Laser and IPL
Atopic dermatitis - Eczema
Atopic dermatitis
Pathogenesis:
Interaction of skin barrier, genetic,
environmental and immunologic
factors.
Dry skin = pruritus = scratch = rash

2/19/2015
5
Atopic Dermatitis
Presents differently with age
Infants – red skin, tiny vesicles on
“puffy” surface. Also scaling
exudation with crusts and cracks.
Atopic Dermatitis
Childhood – Lesions are more papular
with lichenification, erosions, and
crusts.
Common pattern antecubital,
popliteal fossae, neck and face
85% of eczema presents before age 5
Atopic Dermatitis
Adults – more lichenification and
excoriations.

2/19/2015
6
Atopic Dermatitis -Management
Acute phase
Control of pruritus – oral
antihistamines
Wet dressings
Topical glucocorticoids
Topical Calcineurin Inhibitors (TCI’s)–
Tacrolimus, Pimecrolimus
Topical Mupirocin if secondary
infection – mostly S. aureus
Watch out for MRSA
Subacute and chronic
Hydration of skin – oil in bath followed
by emollients
Control of pruritus – oral
antihistamines
Topical glucocorticoids – bid x 2
weeks only – systemic should be
avoided
Topical TCI’s
Avoid exacerbating factors –
emotional stress, dry air, wool
Probiotics may aid in prevention
Atopic Dermatitis - New evidence
Some evidence that mometason
furoate is more effective for AD with
fewer side effects.
Oils with positive effects on AD –
sunflower seed, coconut and mineral
Negative effect on AD – olive oil
Bleach baths - positive effect on AD
+ decreases colonization of S. aureus
Impetigo
Pathogenesis
Gram-positive bacterial infection of
the epidermis occurring near
Staph aureus colonization
Usually Staph aureus but can be
streptococci or combination of
both
Types
Nonbullous – most common, papules
that progress to vesicles
surrounded by erythema then
pustules that break and form thick,
honey-colored crust

2/19/2015
7
Impetigo
Bullous – seen in young children,
vesicles enlarge to form flaccid
bullae (2-5mm) with clear yellow fluid
that rupture leaving thin, brown crust
Ecthyma – ulcerative lesions extend
through the epidermis and deep into
dermis, “punched-out” ulcers
covered with yellow crust
Diagnosis
Usually by clinical presentation
Impetigo
Management
Topical antibiotics – use when limited
number of lesions without bullae
Mupirocin tid x 10 days
Retapamulin bid x 5 days (>9mo)
Oral antibiotics – use when bullous or
many lesions
Doxycycline, Cephalexin or
amoxicillin-clavulanate x 7 days
Macrolides do not cover S. aureus or
strep well
Dermatitis
Irritant contact dermatitis
chemical irritant – detergents,
cement, fiberglass, poinsettias
Usually sharply demarcated to
exposure area. Starts with burning
or stinging before objective
findings. Itching can be delayed
Treatment – avoid irritant, barriers
Acutely treat with wet dressings,
topical or oral glucocorticoids

2/19/2015
8
Dermatitis
Allergic contact dermatitis
antigen causes reaction – nickel,
neomycin, plants
Dermatitis - allergic
Typically well demarcated, superimposed vesicles and papules
Distribution at exposure site
Allergic phytodermatitis occurs when sensitized individuals are exposed to wide variety of plant allergens
First exposure (sensitization) – dermatitis typically occurs 7-12 days after exposure
Dermatitis in previously sensitized patients can be less than 12 hours after exposure
Dermatitis - allergic
Allergens from plants are resins
(oils)
Blister fluid does not contain resin
and cannot spread dermatitis.
Smoke from burning plant does
not cause dermatitis but
particulate matter in the smoke
can

2/19/2015
9
Dermatitis - allergic
Treatment
Topical glucocorticoids are effective
for non-bullous lesions
Systemic glucocorticoids may be
necessary if severe or exudative
lesions
Systemic treatment should be 10-14
days and taper
My standard taper: Prednisone
10mg. 6 po daily for 2 days, 5 po daily
for 2 days, 4 po daily for 2 days, 3 po
daily for 2 days and 1 po daily for 2
days (#42)
Alternatively, Triamcinolone
acetonide (long-acting) can be
given IM
Dermatitis
Lichen simplex chronicus
Pathogenesis
A localized form of lichenification
occurring in circumscribed plaques
resulting from repetitive rubbing and
scratching. Can last for decades.
Sensitive skin – habitually itches
Difficult to treat – patients must stop
scratching
Occlusive dressings with
glucocorticoids
Oral antihistamines
Psoriasis
Pathogenesis
Psoriasis a complex, chronic,
multifactorial, inflammatory
disease that involves
hyperproliferation of the
keratinocytes in the epidermis,
with an increase in the epidermal
cell turnover rate
It is the most common autoimmune
disease in U.S.
Writer John Updike wrote “ The name
of the disease, spiritually speaking,
is Humiliation”

2/19/2015
10
Psoriasis
Several different variants
Plaque psoriasis is the most common – 80-90%
Lesions present as sharply demarcated, erythematous plaques with a silvery, micaceous scale. Removal of these scales can cause pinpoint bleeding, known as Auspitz's sign.
plaques are commonly found on the elbows , knuckles, and knees. Can also be on the scalp, the lower back, the periumbilical region, and the intergluteal cleft.
Psoriasis
Guttate – type
Petite, mildly scaled, salmon-pink
papules, predominately on the
trunk, occurring 2-3 weeks after
acute episode of group-A
streptococci
Can spontaneously resolve in a
few weeks with no treatment but
more often evolves to chronic
plaque psoriasis
Psoriasis
Psoriatic arthritis
Can affect up to 30% of those with
cutaneous disease
Peripheral joint pain, stiffness and
damage – hands and feet
may be present without any visible
psoriasis (10%)
often involves fingertips, periungual
skin and nails

2/19/2015
11
Psoriasis - management
Daily topical emollients
Nonprescription tar preparations –
useful in combination with topical
corticosteroids
Topical corticosteroids (potent to
very potent)
Vitamin D analog or a retinoid –
more effective in combination with a
topical corticosteroid
Psoriasis
Treatment
Methotrexate may be used for as
long as it remains effective and well-
tolerated.
Cyclosporine is generally used
intermittently
Systemic retinoids
Combination therapy may be
helpful
Biologics
PUVA
Ichthyoses
Pathogenesis
Genetic, abnormal stratum
corneum formation and abnormal
keratins
Vulgaris type – Xerosis (dry skin) with
fine scaling, also larger adherent
tacked-down scales in fish scale
pattern
More than 50% of patients also have
atopic dermatitis
Xerosis and pruritus worse in winter
months

2/19/2015
12
Ichthyosis – KP
Keratosis pilaris
Common, genetic but etiology
unknown
Small, follicular, horny spines most
commonly found on shoulders,
upper arms and thighs
Incidence peaks at adolescence –
usually improves with age
Ichthyosis - KP
Treatment
Hydration of stratum corneum –
creams with urea bind water in the
stratum corneum
keratolytic agents – propylene glycol-
glycerin-lactic acid mixtures, 6%
salicylic acid in propylene glycol
and alcohol or alpha hydroxy
acids
topical corticosteroids or topical
retinoid – short courses
Rare, severe cases – oral retinoid
Pityriasis rosea
Pathogenesis
Herpes virus type 7 is suspected
Rare in infants and elderly
Pruritus – absent (25%), mild (50%),
or severe (25%)
A single herald patch (50-90% of
cases) precedes the exanthem
which develops over 1-2 weeks
Herald patch – oval, slightly raises,
salmon-red with fine collarette
scale at the periphery
Exanthem – fine scaling papules/
plaques, dull pink, oval, scattered
in “Christmas tree” pattern – rarely
on face

2/19/2015
13
Pityriasis Rosea
Management - symptomatic
oral antihistamines
topical antipruritic or
glucocorticoids
Self-limiting usually in 6-12 weeks,
can be up to 6 months
Recurrences are uncommon
Reassure PR is benign and not
contagious
Refer pregnant women who have
PR in first trimester
Dermatophytoses - tinea
Pathogenesis
Dermatophytes make keratinases that digest keratin and sustain existence of fungi in keratinized structures.
Transmitted by fomites from one person to another (less common by direct skin contact), animals and rarely soil
Predisposing factors: immunosuppression (including topical), atopy, ichthyosis, sweating, occlusion, geographical location, high humidity
Tinea
Clinical presentation varies by site of infection, immunologic response of the host and species of fungus
Can be dry scaling, macerated, moccasin-type, inflammatory, bullous or ulcerative
Tinea pedis (athlete’s foot)
Tinea manuum (hand)
Tinea cruris (jock-itch)
Tinea corporis (ringworm - trunk, legs & arms)
Tinea capitis (scalp)

2/19/2015
14
Tinea
Tinea
Management
Topical antifungal preparations:
applied bid to involved area for 4
weeks including at least one week
after lesions have cleared. Apply
3 cm beyond advancing margin
of lesion/s.
Imidazole (Lotrimin, Nizoral)
Allylamines (Lamisil, Naftin)
Naphthionates (Tinactin)
Substituted pyridone (Loprox)
Tinea
Systemic therapy:
Extensive corporis infection,
immunosuppression, failed topical
treatment, tinea capitis, tinea
barbae or tinea unguium
Griseofulvin 10mg/kg/day for 4
weeks
Itraconazole 200mg/day x 1 week
or 100mg/day x 2 weeks
Terbinafine 250mg/day x 2 weeks
Fluconazole 50-100mg/day or
150mg/weekly x 2-4 weeks

2/19/2015
15
Tinea (pityriasis) Versicolor
Pathogenesis
Not a dermatophyte infection but rather a yeast fungal infection (M. furfur)
Predisposing factors
Hot, humid climates, oily skin, hyperhidrosis, hereditary
Symptoms
Usually patients present for cosmetic reasons; occasionally mildly pruritic
Typically on trunk, back, abdomen and upper extremities; color varies; thin scale
Tinea Versicolor
Management
Ketoconazole shampoo- apply to affected area daily, leave on 10-15 minutes and rinse, use for 1 week
Selenium sulfide lotion or shampoo
Azole creams – qd or bid x 2 weeks
Terbinafine solution – bid x 7 days
Systemic therapy with ketoconazole, itraconazole and fluconazole are reserved for severe or resistant infections. Terbinafine and griseofulvin are not effective for tinea versicolor
Candidiasis
Candida is a genus of yeast that is
currently the most common cause
of fungal infections
Intertrigo – body folds
Interdigital – web spaces
Diaper dermatitis
Oral (thrush)
Genital (vaginitis or balanitis)
Characteristic features: multiple,
small erythematous “satellite”
lesions scattered along the edges
of larger erythematous macules
2/19/2015
16
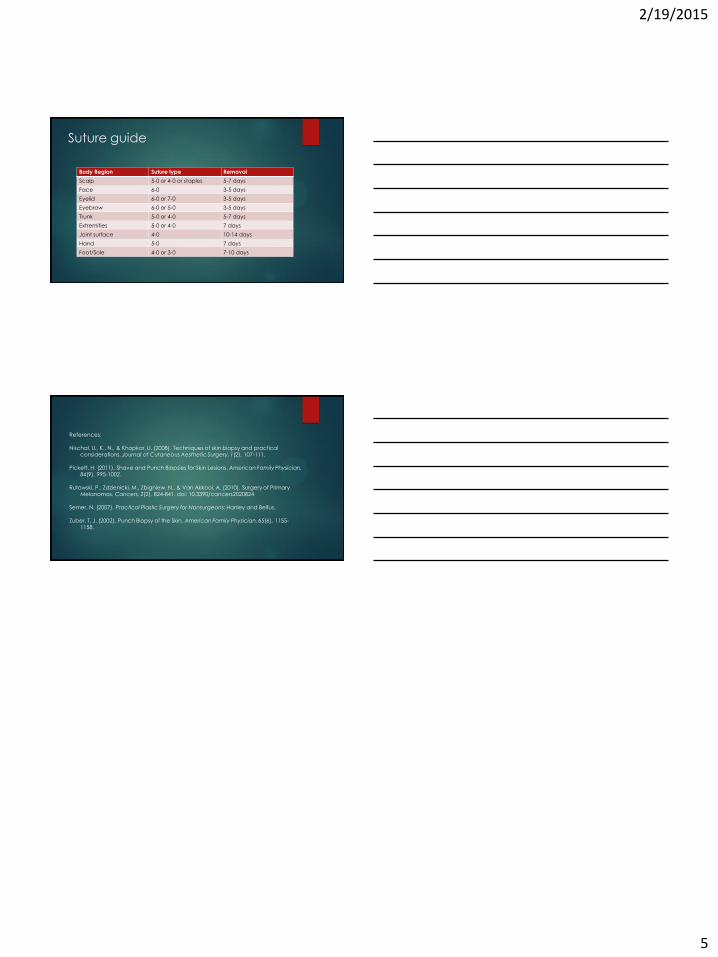
Candidiasis
Management
Prevention – keep areas dry, washing
with benzoyl peroxide bar,
miconazole powder
Topical antifungal creams applied
twice daily until clear (10 days)
Topical glucocorticoids short term
only
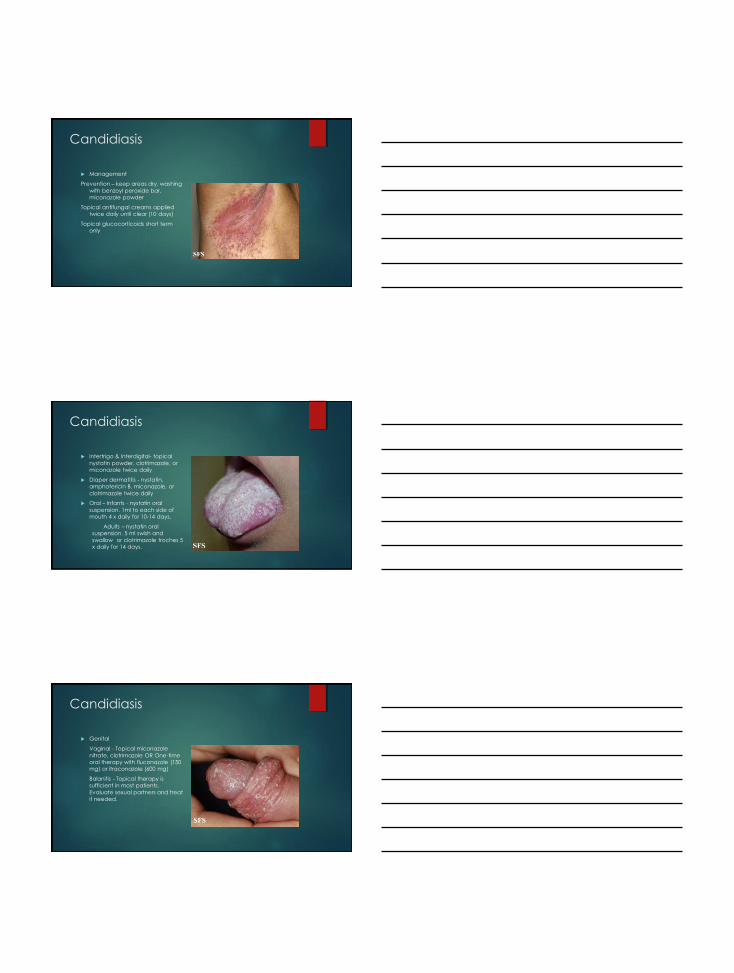
Candidiasis
Intertrigo & Interdigital- topical
nystatin powder, clotrimazole, or
miconazole twice daily
Diaper dermatitis - nystatin,
amphotericin B, miconazole, or
clotrimazole twice daily
Oral – Infants - nystatin oral
suspension. 1ml to each side of
mouth 4 x daily for 10-14 days.
Adults – nystatin oral
suspension. 5 ml swish and
swallow or clotrimazole troches 5
x daily for 14 days.
Candidiasis
Genital
Vaginal - Topical miconazole
nitrate, clotrimazole OR One-time
oral therapy with fluconazole (150
mg) or itraconazole (600 mg)
Balanitis - Topical therapy is
sufficient in most patients.
Evaluate sexual partners and treat
if needed.

2/19/2015
17
Molluscum Contagiosum
Pathogenesis
Molluscum Contagiosum Virus (MCV
types 1-4) closely related to
poxvirus
Transmission – skin to skin contact
Typical features – papules or small
nodules, pearly white or skin
colored, round, oval, umbilicated.
Inflammatory “halo”
Distribution – isolated single lesion,
multiple, scattered discrete lesions
or clustered. Can occur
anywhere.
MCV
Autoinoculation is common
Usually asymptomatic but can be pruritic
Benign and self-limiting within 6 months
Treatment
prevention of spread (auto or to others), resolution of pruritus, prevention of scarring from trauma or secondary infection
Curettage or cryosurgery
Topical imiquimod, cantharidin tretinoin, lactic acid, salicylic acid, silver nitrate
Erythema infectiosum (Fifth
disease)
Pathogenesis
Parvovirus – DNA virus
Most common in young – 60%
young adults are seropositive
Transmitted by aerosol droplet
Symptoms
Prodrome of fever, malaise,
headache, coryza - 2 days before
rash
Edematous erythematous plaques on
the cheeks and erythematous lacy
rash on trunk and extremities

2/19/2015
18
Erythema infectiosum
Headache, sore throat, fever,
myalgia, nausea, cough,
conjunctivitis may coincide with
rash
Infected adults likely to have
arthralgia
Management
Symptomatic
Self limiting – 3 weeks
Hand-foot-mouth disease
Pathogenesis
Coxsackievirus
Typically occurs < 10 years of age
Highly contagious – transmitted by
oral-oral and fecal-oral
5-10 painful oral ulcers, cutaneous
lesions (palms, soles, buttocks) can
be asymptomatic or painful
Hand-foot-mouth disease
Low grade fever, malaise, less
commonly arthralgia, diarrhea
Management
Symptomatic
Course 7-10 days

2/19/2015
19
Herpes (HSV-1 & HSV-2)
Pathogenesis
DNA virus. Once an individual is infected, HSV persists in sensory ganglia proximal to site of infection, recurring when immunity is lessened
Labialis (oropharyngeal): HSV-1 (80-90%), HSV-2 (10-20%)
Urogenital: HSV-1 (10-30%), HSV-2 (70-90%)
Transmission
Infected person sheds virus at peripheral site, mucosal surface or secretion and inoculates close contacts at susceptible mucosal surface or break in skin
HSV1 & HSV2
Worldwide, 90% are seropositive
for HSV-1 by 4th decade of life
HSV-1 infections can be severe
and cause encephalitis especially
immunocompromised hosts
Typical features: prodrome -
vesicles in groups on a
erythematous base-pustules-ulcers
Diagnosis: viral culture, serology,
immunofluorescence, Tzanck
HSV-1 & HSV-2
Treatment
HSV-1: topical acyclovir cream
Acyclovir 200-400mg 5 x daily
Famciclovir 1500mg as single dose
Valacyclovir 2 gram bid x 1 day
HSV-2: initial outbreak: acyclovir 400mg tid x 7-10 days
Famciclovir 250mg tid x 7-10 days
Valacyclovir 1 gram bid x 7-10 days
Recurrent outbreaks: acyclovir 800mg tid for 2 days
Famciclovir 1000mg bid x 1 day
Valacyclovir 1 gm daily for 5 days
Suppressive therapy for HSV-2

2/19/2015
20
Herpetic whitlow
< 20 years of age usually HSV-1, >
20 years of age usually HSV-2
HSV infection of fingers that can
occur as a complication of
primary HSV-1 or HSV-2 by
inoculation of the virus through a
break in skin barrier (commonly a
torn cuticle)
painful
Herpes Zoster
Pathogenesis
Viral infection caused by reactivation
of varicella-zoster virus (VZV)
Primary infection (varicella) resolves
and the viral particles remain
dormant in the dorsal root or
sensory ganglia. When hosts
immune systems fails to suppress
replication of VZV, reactivation
occurs.
Persons who have had previous
varicella infections or vaccination
may develop herpes zoster.
Herpes zoster
Rash and pain: erythematous
papules-vesicles-pustules-crust
Course in healthy people = 7-10
days
Usually affects one dermatome
but 2-3 neighboring dermatomes
may be affected.
Post herpetic neuralgia (PHN)
Diagnosis: history and clinical
examination – lab not beneficial

2/19/2015
21
Herpes zoster
Treatment
Antivirals: acyclovir 800mg 5 x daily for 7-10 days
Valacyclovir 1000mg tid x 7 days
Famciclovir 500mg tid x 7 days
Mixed data for using oral steroids to prevent PHN
Pain control: gabapentin, opioids
Referral needed
Ophthalmicus
Oticus – triad of facial paralysis, ear pain and vesicles in auditory canal
Measles
Vaccine became available in
1963
Travelers with measles continue to
bring the disease into the U.S.
Highly contagious – transmitted by
aerosol droplet, can live up to two
hours on a surface or airspace.
90% of close contacts of infected
persons that are not immune will
become infected
Infected people are contagious from
four days before to four days after
the rash appears
Measles
Can be very serious – especially
age <5 or >20. 1-2/1000 mortality
2014: 644 cases from 27 states
From January 1 to February 6,
2015, 121 cases from 17 states -
most of these part of a large,
ongoing outbreak in Disneyland
The majority of the people who
got measles were unvaccinated,
under vaccinated or status was
unknown

2/19/2015
22
Measles
Symptoms: 7-14 days after
exposure
high fever, cough, coryza and
conjunctivitis
2-3 days later - Koplik spots
3-5 days – maculopapular erythema
that appear on the face at the
hairline and spread downward to
the neck, trunk, arms, legs, and
feet. Some papular and confluent
– fever may spike when rash
appears
Measles
If measles is suspected, report to local health
department and obtain serum and throat
swab for testing
Close follow up
Seborrheic keratosis
Most common benign epithelial
tumors
Hereditary, start after age 30
Evolve over months to years
Early lesions small, slightly elevated
papule, later – larger plaque
Late lesions – plaque with warty
surface “stuck on” appearance

2/19/2015
23
Seborrheic keratosis
Management
Rule out malignancy first – punch
biopsy
Cryosurgery with liquid nitrogen – only
effective on flat lesions
Curettage is best followed by light
cautery to prevent recurrence
Careful application of trichloroacetic
acid
Ammonium lactate and alpha
hydroxy acids have been reported
to reduce the height of lesions
Actinic keratosis
Precancerous - actual
percentage that progress to
squamous cell carcinoma remains
unknown, estimates vary from as
low as 0.1% to as high as 10%
Biopsy – initial or treatment
resistant
Single or multiple, discrete, dry,
rough, adherent scaly lesions
Occur on sun-exposed skin
Gently abrading lesions usually
causes pain – helpful diagnostic
finding
Actinic keratosis
Therapy is generally well tolerated
and simple; therefore, treatment
of all actinic keratosis is warranted.
Medical management
Prevention - sunscreen
5-Fluorouracil – bid for 1 month
Imiquimod – 2-3 x weekly for 1 month
Ingenol mebutate – 2-3 consec. days
Topical diclofenac sodium 3% gel –
bid for 3 months

2/19/2015
24
Actinic keratosis
Surgical management
Photodynamic therapy - painful
Cryosurgery
Curettage or excision – scarring
Laser
Combination topical with cryosurgery
Pyogenic granuloma
Rapidly developing vascular lesion
usually following minor trauma.
Benign but send in for confirmation
and r/o malignancy
Solitary, smooth surface, red,
brown/black with or without
crusts/erosions
Bleeds easily
shave excision and cautery
surgical excision with primary closure
- if large
Cutaneous Carcinomas
Most common cancer in the U. S.
Each year, more new cases of skin
cancer than cancers of the
breast, prostate, lung and colon
combined (Skin Cancer
Foundation, 2011)
Melanoma is the deadliest form of
skin cancer, killing approximately
8,650 Americans in 2009 (Skin
Cancer Foundation, 2011)
Overall, the literature research
revealed evidence that PCPs
could reduce morbidity and
mortality of skin cancer if they
focus screening on patients at risk.

2/19/2015
25
Cutaneous Carcinomas
Major Risks:
a personal or 1st degree relative with
melanoma
immunosuppressive therapy after
transplant
more than 100 nevi or more than 4
dysplastic nevi
received 250 or more PUVA
treatments
radiation as a child for cancer,
Risks:
naturally red or blonde hair color
Freckles easily
50 to 100 nevi or dysplastic nevi
burns easily, tans poorly
history of many sunburns
age >50
Basal Cell Carcinoma (BCC)
The bad news – most common skin cancer in U.S. and many other countries
The good news – slow growing and usually do not metastasize
Characteristic features
Waxy papules with central depression
Pearly
Rolled border
Bleeding
Crusting
Erosion or ulceration
Basal Cell Carcinoma

2/19/2015
26
BCC
Treatment
Biopsy – Excise if can, shave may be
acceptable if large or in difficult
place
Refer
Squamous Cell Carcinoma (SCC)
Second most common skin cancer
and higher mortality than BCC
Twice as frequent in men as in
women and rarely appears before
age 50 (Nolen et al., 2011)
Some form grow slowly, some quickly
Common features
Raised, firm, skin-colored or pink
Keratotic papule or plaque
SCC

2/19/2015
27
SCC
Treatment
biopsy – shave biopsy can miss
well-differentiated SCC
refer
Malignant Melanoma
The good news – only about 5% of
skin cancers
The bad news – Three times as
many deaths each year
compared to nonmelanoma skin
cancer
Most often in skin but can be from
melanocytes in eyes, ears, GI
tract, genital or oral mucous
membranes (Habif, et al., 2011)
Melanoma
Common features
Can be found anywhere on body
Plaque – few mm-several cm
Irregular borders
Varied colors
Nodular
Nonpalpable tan or brown macule
– lentigo melanoma
ABCDE

2/19/2015
28
Melanoma
Melanoma
Treatment
Refer
References:
CDC. (2015a). Centers for Disease Control and Prevention: Measles. Retrieved February 2015 http://www.cdc.gov/measles/index.html
CDC. (2015b). Centers for Disease Control and Prevention: Public Health Image Library - measles. Retrieved February 2015 http://phil.cdc.gov/phil/home.asp
Dermnet Skin Disease Atlas. (2015). Retrieved January 6, 2015, from http://www.dermnet.com/
Dermquest Images. (2015). Retrieved January 7, 2015, from https://www.dermquest.com/image-library/ Lyons, F., & Ousley, L. (2015). Dermatology for the Advanced Practice Nurse. New York, New York: Springer.
Medscape. Retrieved January, 2015, from http://www.medscape.com/nurses
Nolen, M. E., Beebe, V. R., King, J. M., Bryn, N., & Limaye, K. M. (2011). Nonmelanoma skin cancer part 1. Journal of the Dermatology Nurses' Association, 3(5), 260-283.
Samuel Freire da Silva, M. D. (January 2015). Dermatology Atlas. Retrieved January, 2015, from
http://www.atlasdermatologico.com.br/index.jsf
Son D, H. A. (2014). Overview of Surgical Scar Prevention and Management. Journal of Korean Medical Science, 29(6),
751-757.
Wolff, K., Johnson, R. A., & Suurmond, D. (2005). Fitzpatrick's Color Atlas & Synopsis of Clinical Dermatology (fifth ed.).
New York: McGraw-Hill.