Embed Size (px)
Citation preview
BIOS222
Pathology and Clinical Science 2
www.endeavour.edu.au
Session 4
Lymphatic and
Haematological Disorders 2
Bioscience Department
© Endeavour College of Natural Health www.endeavour.edu.au 2
Session Learning Outcomes
At the end of the session, you should be able to
o Classify various types of anaemia in terms of their
aetiology and morphology.
o Identify the causes, pathophysiology and clinical
manifestations of various types of anaemia.
o Suggest appropriate investigations and
management for the conditions.
o Define and describe the haemoglobinopathies in
terms of their cause, pathophysiology, role of
hereditary trait, treatment and management.
© Endeavour College of Natural Health www.endeavour.edu.au 3
Session Plan
o The Anaemias:
• Classification of anaemia
• Iron deficiency anaemia
• Megaloblastic anaemia
• Anaemia of chronic disease
• Haemolytic anaemia
• Haemoglobinopathies
– Sickle cell anaemia
– Thalassemia
© Endeavour College of Natural Health www.endeavour.edu.au 4
Anaemia
Definition: A state in which there is decrease in the level of
haemoglobin in the blood below the reference level for the
age and sex of the individual.
o Normal reference range: (varies with age, gender and
ethnic origin of a person)
• Adult male 130-195 g/L
• Adult female 115-165 g/L
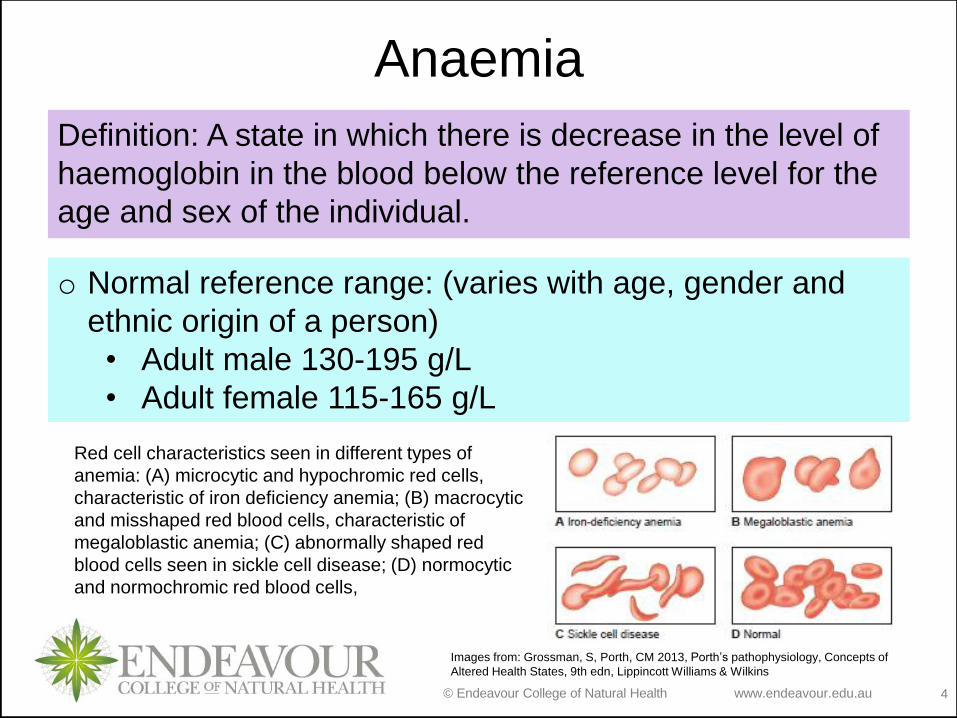
Red cell characteristics seen in different types of
anemia: (A) microcytic and hypochromic red cells,
characteristic of iron deficiency anemia; (B) macrocytic
and misshaped red blood cells, characteristic of
megaloblastic anemia; (C) abnormally shaped red
blood cells seen in sickle cell disease; (D) normocytic
and normochromic red blood cells,
Images from: Grossman, S, Porth, CM 2013, Porth’s pathophysiology, Concepts of
Altered Health States, 9th edn, Lippincott Williams & Wilkins
© Endeavour College of Natural Health www.endeavour.edu.au 5
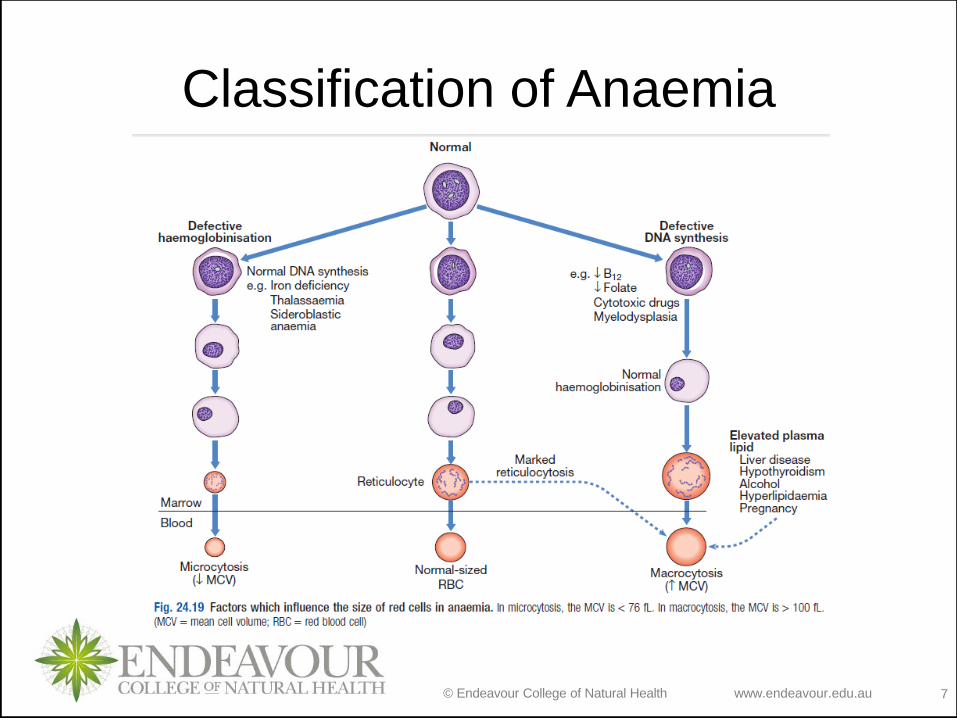
Classification of Anaemia
o Aetiological classification of anaemia:
• Inadequate nutrients to synthesize RBC
– Iron deficiency anaemia, Megaloblastic
anaemia
• Excessive loss of RBC
– Haemolytic anaemia: destruction of RBCs
• Genetic defect in Haemoglobin synthesis
– Thalassemia, Sickle cell anaemia
© Endeavour College of Natural Health www.endeavour.edu.au 6
Classification of Anaemia
oMorphological classification of Anaemia
• Based on size of RBC
– Macrocytic
– Normocytic
– Microcytic
• Based on Content of Haemoglobin in the
RBC
– Hypochromic
– Normochromic
© Endeavour College of Natural Health www.endeavour.edu.au 7
Classification of Anaemia
© Endeavour College of Natural Health www.endeavour.edu.au 8
General Signs and Symptoms,
Anaemia
o Symptoms:
• Fatigue
• Headache
• Tinnitus
• Fainting
• Breathlessness
• Angina
• Palpitation
• Intermittent
claudication
o Signs
• Pallor
• Tachycardia
• Systolic flow murmur
• Cardiac failure
• Papilloedema
© Endeavour College of Natural Health www.endeavour.edu.au 9
Iron deficiency anaemia
o Aetiology:
• Blood loss
• Malabsorption or dietary deficiency of Iron
• Increased physiological demands
o Pathophysiology:
Lack of Iron Decreased synthesis of Haemoglobin
Decreased RBC size with decreased heamoglobin
concentration Microcytic hypochromic anaemia
Impaired oxygen transport
© Endeavour College of Natural Health www.endeavour.edu.au 10
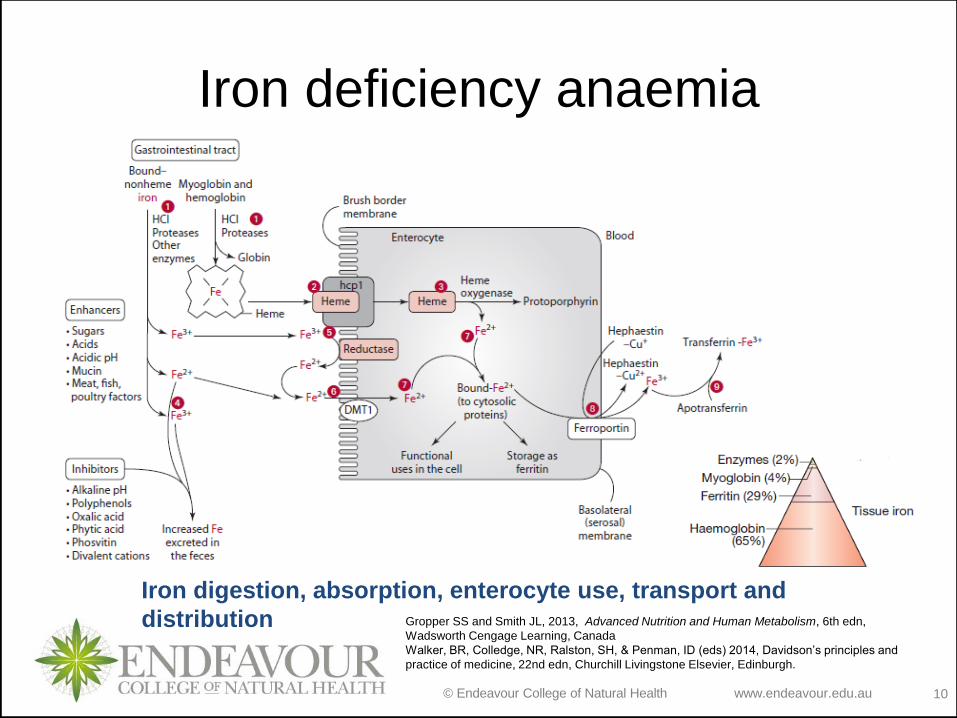
Iron deficiency anaemia
Iron digestion, absorption, enterocyte use, transport and
distribution Gropper SS and Smith JL, 2013, Advanced Nutrition and Human Metabolism, 6th edn,
Wadsworth Cengage Learning, Canada
Walker, BR, Colledge, NR, Ralston, SH, & Penman, ID (eds) 2014, Davidson’s principles and
practice of medicine, 22nd edn, Churchill Livingstone Elsevier, Edinburgh.
© Endeavour College of Natural Health www.endeavour.edu.au 11
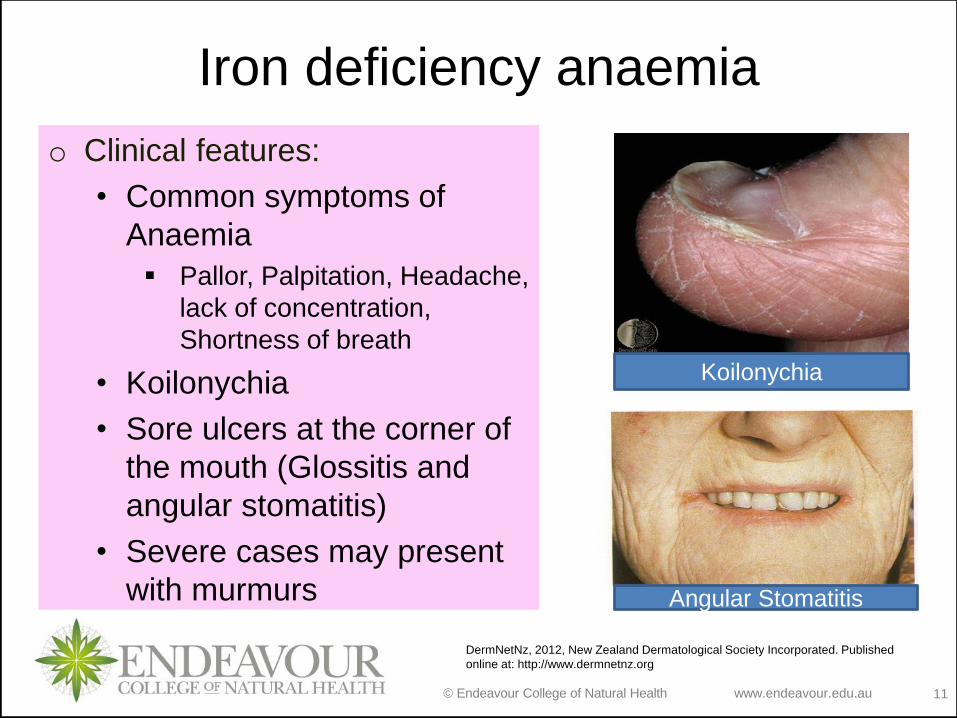
Iron deficiency anaemia
o Clinical features:
• Common symptoms of
Anaemia
Pallor, Palpitation, Headache,
lack of concentration,
Shortness of breath
• Koilonychia
• Sore ulcers at the corner of
the mouth (Glossitis and
angular stomatitis)
• Severe cases may present
with murmurs
Koilonychia
Angular Stomatitis
DermNetNz, 2012, New Zealand Dermatological Society Incorporated. Published
online at: http://www.dermnetnz.org
© Endeavour College of Natural Health www.endeavour.edu.au 12
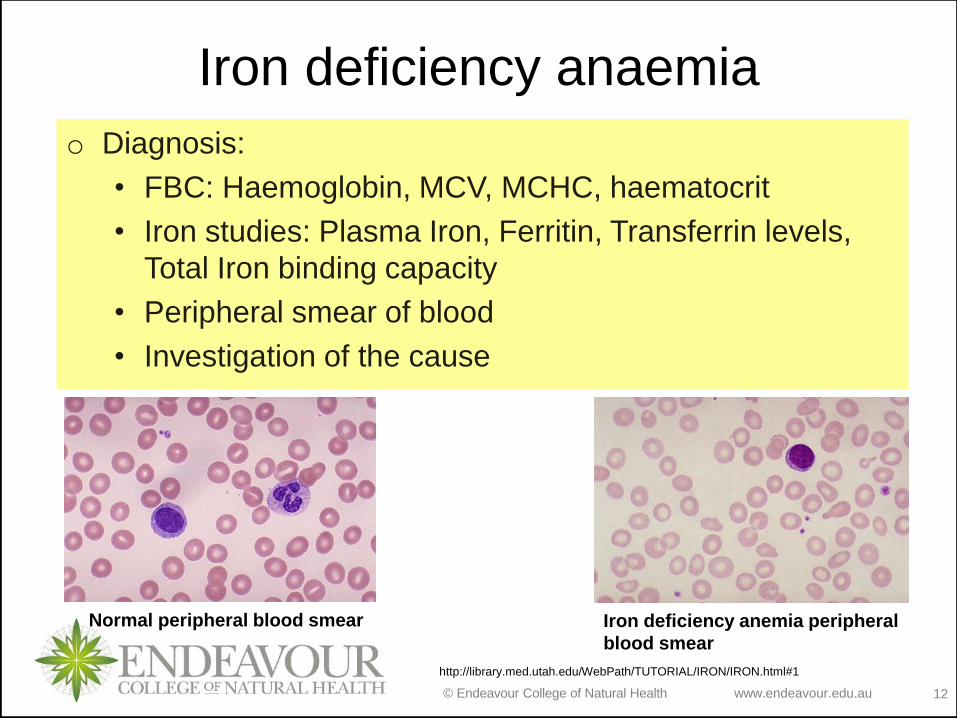
Iron deficiency anaemia
o Diagnosis:
• FBC: Haemoglobin, MCV, MCHC, haematocrit
• Iron studies: Plasma Iron, Ferritin, Transferrin levels,
Total Iron binding capacity
• Peripheral smear of blood
• Investigation of the cause
Normal peripheral blood smear Iron deficiency anemia peripheral
blood smear
http://library.med.utah.edu/WebPath/TUTORIAL/IRON/IRON.html#1
© Endeavour College of Natural Health www.endeavour.edu.au 13
Iron deficiency anaemia
o Management:
• Control chronic blood loss
• Increase dietary intake of iron
• Administering supplemental iron
• Iron transfusion in severe cases
© Endeavour College of Natural Health www.endeavour.edu.au 14
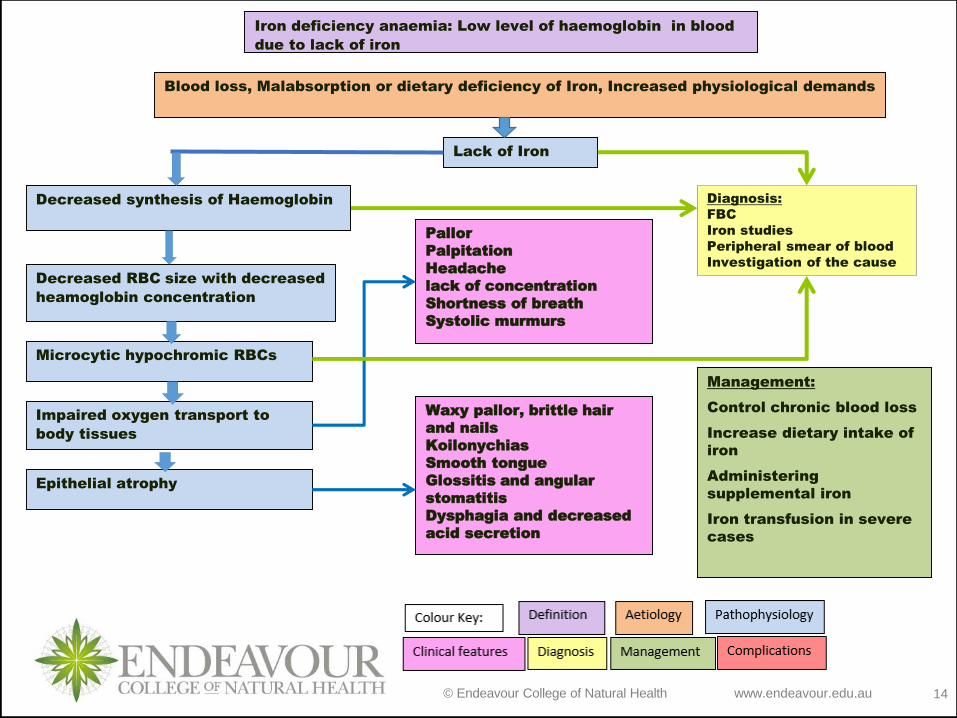
Iron deficiency anaemia: Low level of haemoglobin in blood
due to lack of iron
Blood loss, Malabsorption or dietary deficiency of Iron, Increased physiological demands
Lack of Iron
Decreased synthesis of Haemoglobin
Decreased RBC size with decreased
heamoglobin concentration
Microcytic hypochromic RBCs
Diagnosis:
FBC
Iron studies
Peripheral smear of blood
Investigation of the cause
Waxy pallor, brittle hair
and nails
Koilonychias
Smooth tongue
Glossitis and angular
stomatitis
Dysphagia and decreased
acid secretion
Management:
Control chronic blood loss
Increase dietary intake of
iron
Administering
supplemental iron
Iron transfusion in severe
cases
Impaired oxygen transport to
body tissues
Pallor
Palpitation
Headache
lack of concentration
Shortness of breath
Systolic murmurs
Epithelial atrophy
© Endeavour College of Natural Health www.endeavour.edu.au 15
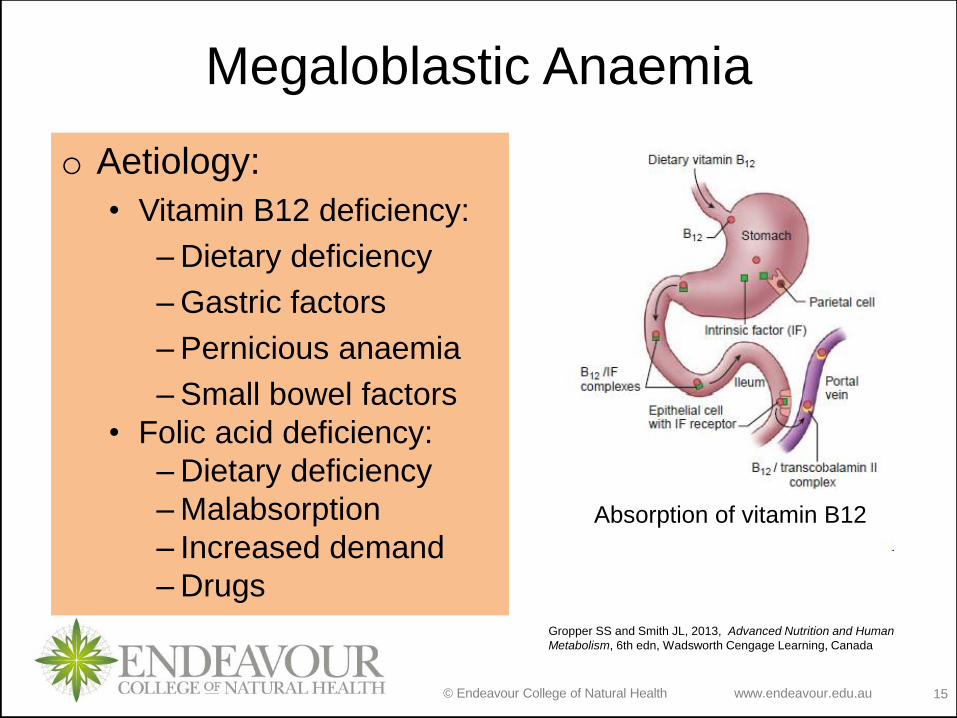
Megaloblastic Anaemia
o Aetiology:
• Vitamin B12 deficiency:
– Dietary deficiency
– Gastric factors
– Pernicious anaemia
– Small bowel factors
• Folic acid deficiency:
– Dietary deficiency
– Malabsorption
– Increased demand
– Drugs
Absorption of vitamin B12
Gropper SS and Smith JL, 2013, Advanced Nutrition and Human
Metabolism, 6th edn, Wadsworth Cengage Learning, Canada
© Endeavour College of Natural Health www.endeavour.edu.au 16
Megaloblastic Anaemia
o Pathophysiology:
• Lack of B12 and Folate Poor methionine
metabolism High plasma levels of homocysteine
and impaired DNA synthesis Cell with arrested
nuclear maturation but normal cytoplasmic
development (megaloblast) All proliferating cells
(bone marrow cells, buccal mucosa, tongue, small
intestine, cervix, vagina and uterus) exhibit
megaloblastosis.
• Lack of B12 Focal demyelination affecting the
spinal cord, peripheral nerves, optic nerves and
cerebrum Neurological symptoms
© Endeavour College of Natural Health www.endeavour.edu.au 17
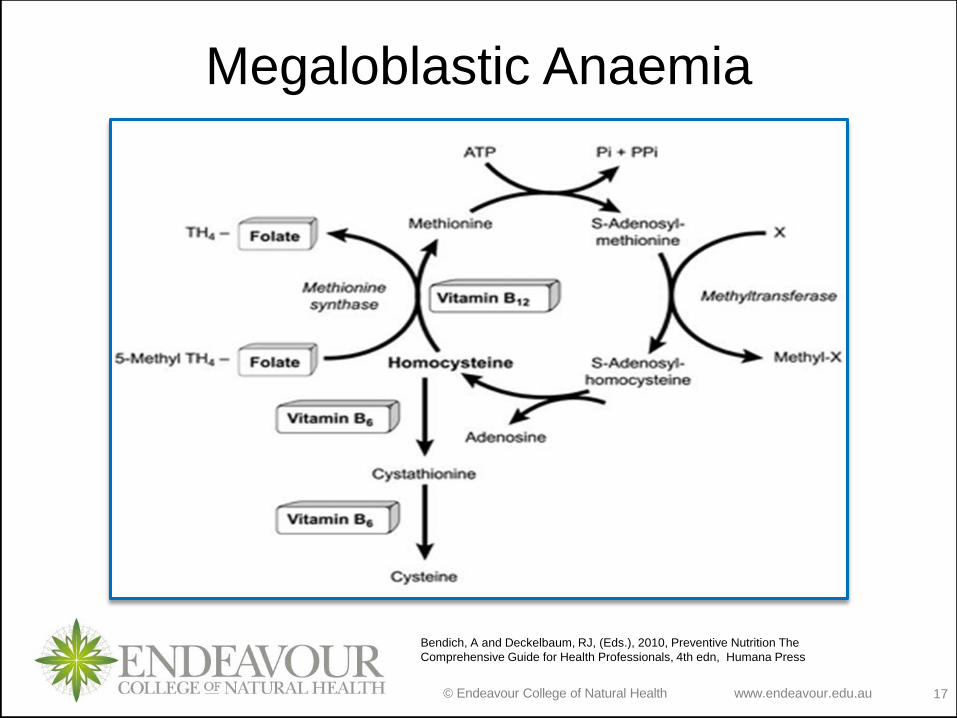
Megaloblastic Anaemia
Bendich, A and Deckelbaum, RJ, (Eds.), 2010, Preventive Nutrition The
Comprehensive Guide for Health Professionals, 4th edn, Humana Press
© Endeavour College of Natural Health www.endeavour.edu.au 18
Megaloblastic Anaemia
o Clinical features:
• Symptoms:
Malaise
Breathlessness
Paraesthesiae
Sore mouth
Weight loss
Altered skin
pigmentation
Impotence
Poor memory
Depression
Personality change
Hallucinations
Visual disturbance
© Endeavour College of Natural Health endeavour.edu.au 19
Megaloblastic Anaemia
• Signs
Smooth tongue
Angular cheilosis
Vitiligo
Skin pigmentation
Heart failure
Pyrexia
• Neurological findings in B12 deficiency Glove and stocking
paraesthesiae
Loss of ankle reflexes
diminished vibration sensation and proprioception
upper motor neuron signs
Dementia
Optic atrophy
Autonomic neuropathy
© Endeavour College of Natural Health www.endeavour.edu.au 20
Megaloblastic Anaemia
o Diagnosis:
• FBC: Haemoglobin, MCV, Blood cell counts
• Serum Ferritin
• Plasma lactate dehydrogenase (LDH)
• Peripheral smear of blood
• Bone marrow
• Investigation of the cause
© Endeavour College of Natural Health www.endeavour.edu.au 21
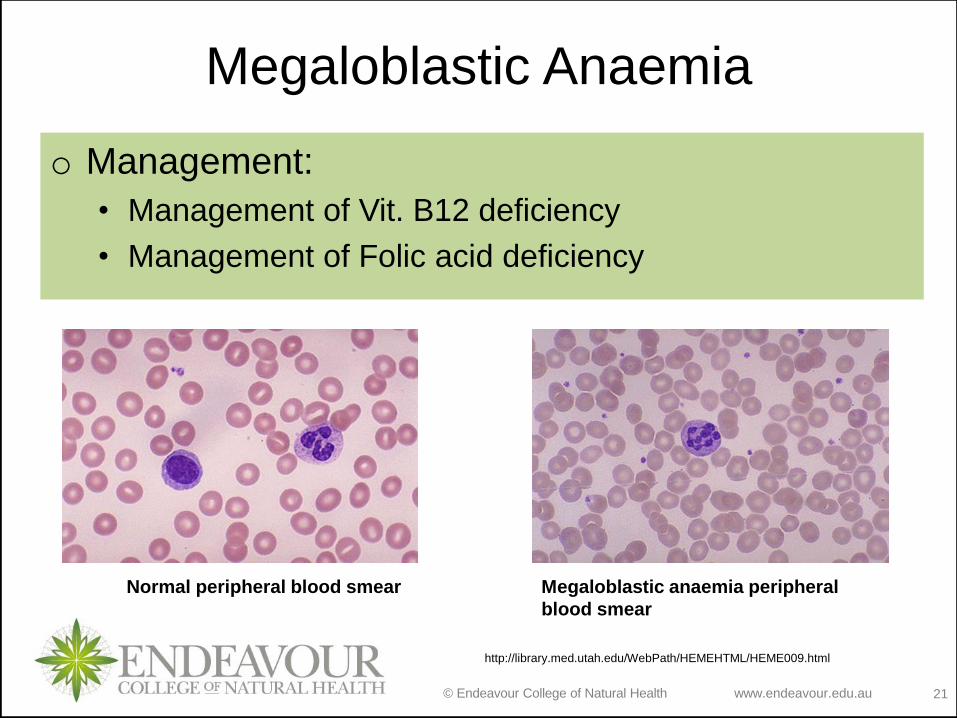
Megaloblastic Anaemia
Normal peripheral blood smear Megaloblastic anaemia peripheral
blood smear
http://library.med.utah.edu/WebPath/HEMEHTML/HEME009.html
o Management:
• Management of Vit. B12 deficiency
• Management of Folic acid deficiency
© Endeavour College of Natural Health www.endeavour.edu.au 22
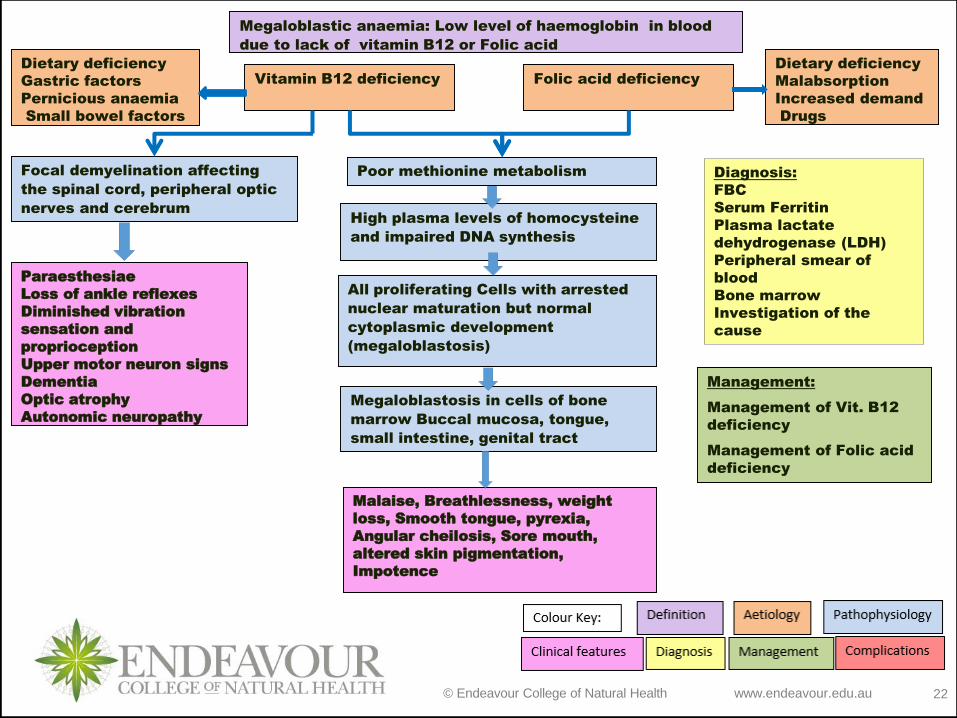
Megaloblastic anaemia: Low level of haemoglobin in blood
due to lack of vitamin B12 or Folic acid
Vitamin B12 deficiency
High plasma levels of homocysteine
and impaired DNA synthesis
All proliferating Cells with arrested
nuclear maturation but normal
cytoplasmic development
(megaloblastosis)
Diagnosis:
FBC
Serum Ferritin
Plasma lactate
dehydrogenase (LDH)
Peripheral smear of
blood
Bone marrow
Investigation of the
cause
Paraesthesiae
Loss of ankle reflexes
Diminished vibration
sensation and
proprioception
Upper motor neuron signs
Dementia
Optic atrophy
Autonomic neuropathy
Management:
Management of Vit. B12
deficiency
Management of Folic acid
deficiency
Malaise, Breathlessness, weight
loss, Smooth tongue, pyrexia,
Angular cheilosis, Sore mouth,
altered skin pigmentation,
Impotence
Folic acid deficiency
Dietary deficiency
Gastric factors
Pernicious anaemia
Small bowel factors
Dietary deficiency
Malabsorption
Increased demand
Drugs
Poor methionine metabolism
Megaloblastosis in cells of bone
marrow Buccal mucosa, tongue,
small intestine, genital tract
Focal demyelination affecting
the spinal cord, peripheral optic
nerves and cerebrum
© Endeavour College of Natural Health www.endeavour.edu.au 23
Anaemia of chronic disease
o Aetiology:
• Chronic infection
• Chronic inflammation
• Neoplasia
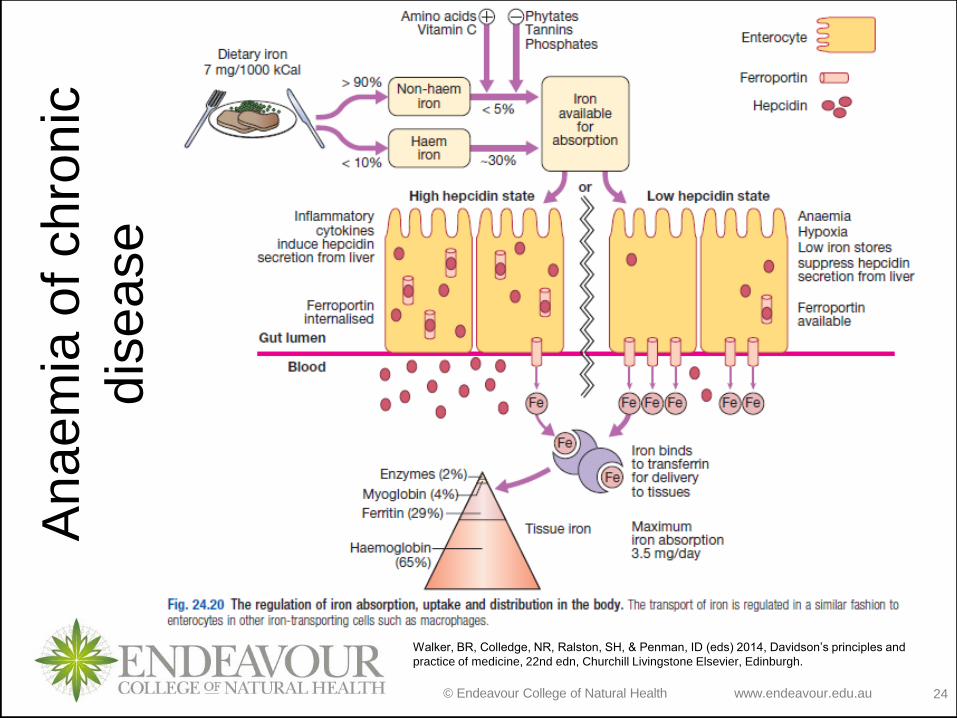
o Pathophysiology:
Pro-inflammatory cytokines in chronic disease
Induce hepcidin production by liver cells Hepcidin
binds to ferroportin and internalise ferroportin into
iron storing cells reduced release of iron Low
circulatory Iron Reduced Erythropoiesis
Normocytic normochromic anaemia
© Endeavour College of Natural Health www.endeavour.edu.au 24
Anaem
ia o
f chro
nic
dis
ease
Walker, BR, Colledge, NR, Ralston, SH, & Penman, ID (eds) 2014, Davidson’s principles and
practice of medicine, 22nd edn, Churchill Livingstone Elsevier, Edinburgh.
© Endeavour College of Natural Health www.endeavour.edu.au 25
Anaemia of chronic disease
o Diagnosis:
• FBC: Haemoglobin, MCV
• Iron studies: Serum Iron, Ferritin, Transferrin levels,
Total Iron binding capacity
• Serum soluble transferrin receptor
• Bone marrow
o Management:
• Measures to reduce the severity of the underlying
disorder
© Endeavour College of Natural Health www.endeavour.edu.au 26
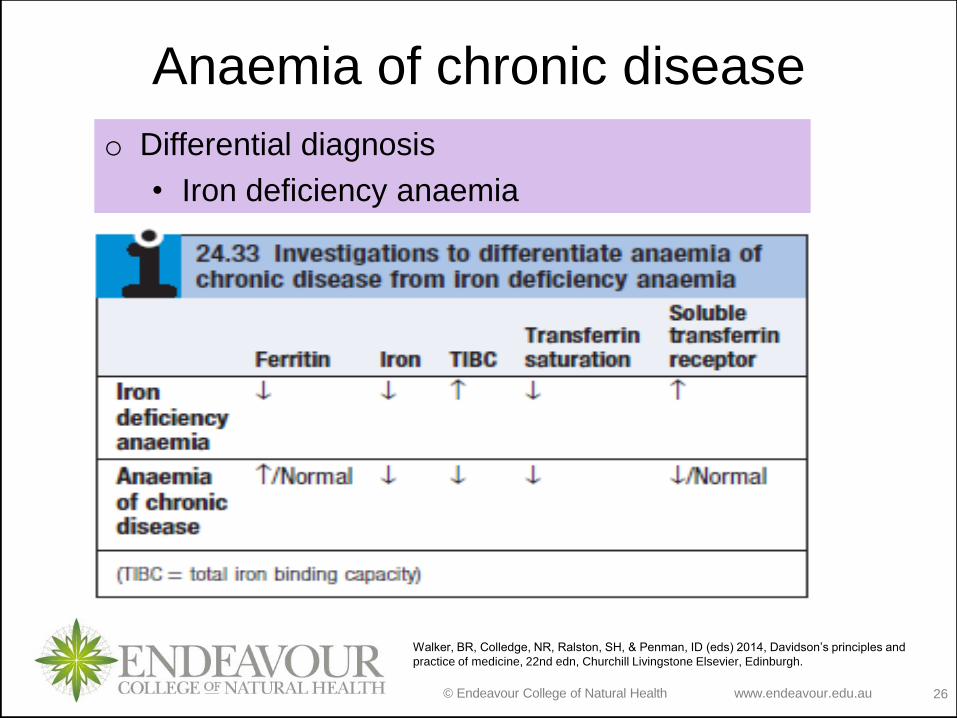
Anaemia of chronic disease
o Differential diagnosis
• Iron deficiency anaemia
Walker, BR, Colledge, NR, Ralston, SH, & Penman, ID (eds) 2014, Davidson’s principles and
practice of medicine, 22nd edn, Churchill Livingstone Elsevier, Edinburgh.
© Endeavour College of Natural Health www.endeavour.edu.au 27
Haemolytic anaemia
o Definition: Anaemia resulting from increased rate of RBC
destruction
o Types:
• Extravascular haemolysis:
– Rapid red cell destruction in the reticuloendothelial
cells in the liver or spleen.
– No free haemoglobin in the plasma.
• Intravascular haemolysis:
– Red cell lysis within the blood stream
– Free haemoglobin is released into the plasma
© Endeavour College of Natural Health www.endeavour.edu.au 28
Haemolytic anaemia
o Aetiology:
• Inherited causes of haemolysis
– Red cell membrane defect: hereditory
spherocytosis/elliptocytosis
– Haemoglobin abnormalities: Thalassemia, sickle
cell disease
– Red cell enzyme deficiencies: G6PD deficiency,
Pyruvate kinase deficiency , pyrimidine
5’nucleotidase deficiency
© Endeavour College of Natural Health www.endeavour.edu.au 29
Haemolytic anaemia
o Aetiology:
• Acquired causes of haemolysis
– Immune: autoimmune diseases, haemolytic
diseases of newborn, transfusion reactions, drug
induced
– Non immune – acquired membrane defects,
mechanical causes, secondary to systemic
diseases related to liver and kidneys, Infections,
Drugs and chemicals, Burns
© Endeavour College of Natural Health www.endeavour.edu.au 30
Haemolytic anaemia
o Clinical features:
• Severe pallor, shortness of breath and heart failure
• Episodic jaundice in some patients
• Young children may show failure to thrive
• Gall bladder stones due to excessive bilirubin
formation in chronic cases
• Increased pulmonary hypertension due to hypoxic
conditions and right ventricular failure
© Endeavour College of Natural Health www.endeavour.edu.au 31
Haemolytic anaemia
o Diagnosis:
• Full blood count
• Peripheral blood smear
• Red blood cell enzymes
• Serum bilirubin, lactate
dehydrogenase
• Urine and stool
examination
• Bone marrow
• Coomb’ test for
antibodies against red
cells
o Management:
• Treatment of underlying cause
• Corticosteroids
• Blood transfusion
© Endeavour College of Natural Health www.endeavour.edu.au 32
Haemoglobinopathies
o Definition: The diseases caused by mutations of the
genes encoding the globin chains of the haemoglobin
molecule.
o Types:
• Qualitative abnormalities
– Alteration in the amino acids structure/sequence
– Example: Sickle cell anaemia
• Quantitative abnormalities
– reduced rate of production of one or other of the
globin chains
– Example: Thalassemias
© Endeavour College of Natural Health www.endeavour.edu.au 33
Sickle cell Anaemia
o Definition: an inherited disorder in which an abnormal
haemoglobin (HbS) leads to chronic haemolytic anaemia,
pain, and organ failure.
o Aetiology:
• Inherited as an autosomal recessive trait
• Substitution of one glutamic acid to valine in the
amino acid chain of Beta Haemoglobin
o Pathophysiology:
Abnormal haemoglobin →Sickle shaped RBC → Early
destruction of RBC
© Endeavour College of Natural Health www.endeavour.edu.au 34
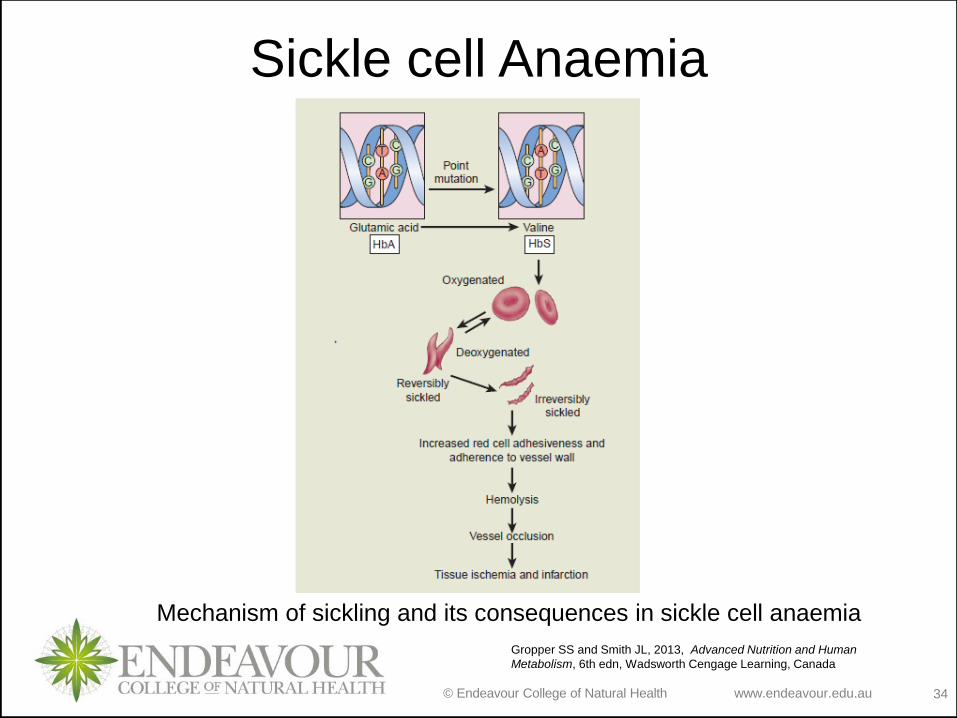
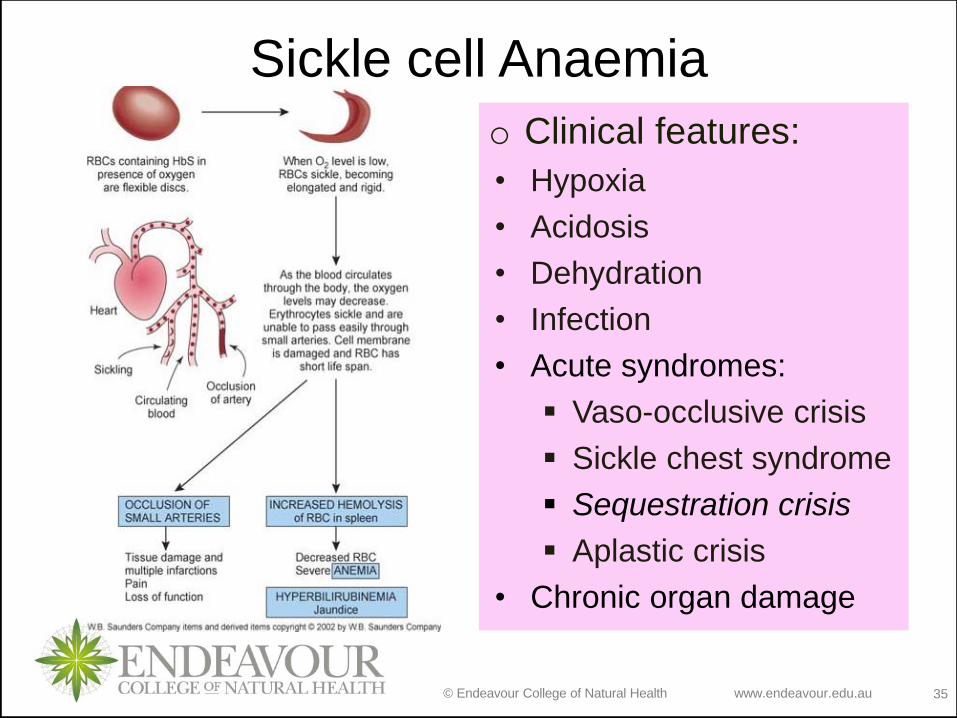
Sickle cell Anaemia
Mechanism of sickling and its consequences in sickle cell anaemia
Gropper SS and Smith JL, 2013, Advanced Nutrition and Human
Metabolism, 6th edn, Wadsworth Cengage Learning, Canada
© Endeavour College of Natural Health www.endeavour.edu.au 35
Sickle cell Anaemia
o Clinical features:
• Hypoxia
• Acidosis
• Dehydration
• Infection
• Acute syndromes:
Vaso-occlusive crisis
Sickle chest syndrome
Sequestration crisis
Aplastic crisis
• Chronic organ damage
© Endeavour College of Natural Health www.endeavour.edu.au 36
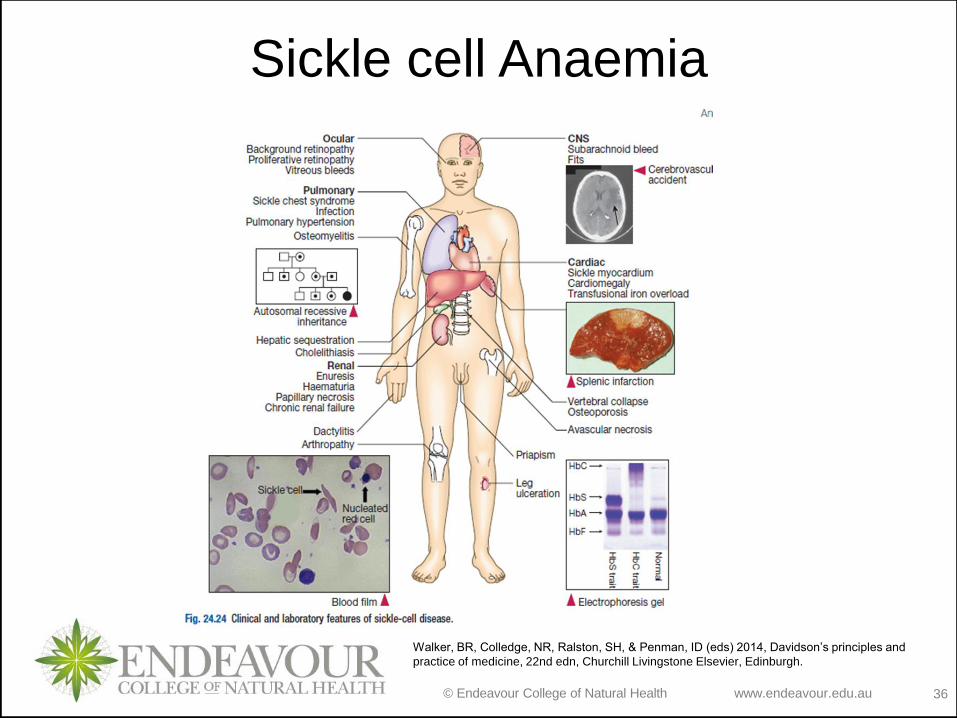
Sickle cell Anaemia
Walker, BR, Colledge, NR, Ralston, SH, & Penman, ID (eds) 2014, Davidson’s principles and
practice of medicine, 22nd edn, Churchill Livingstone Elsevier, Edinburgh.
© Endeavour College of Natural Health www.endeavour.edu.au 37
Sickle cell Anaemia
o Diagnosis:
• FBC: Hb
• Blood film
examination
• HbS screening:
Exposing red cells to
a reducing agent
such as sodium
dithionite
• Haemoglobin
electrophoresis
o Management:• Prophylaxis,
vaccination
• Aggressive
rehydration,
analgesics, O2,
antibiotics,
transfusion
• Allogeneic stem cell
transplants
• Hereditary trait
counselling
© Endeavour College of Natural Health www.endeavour.edu.au 38
Thalassaemia
o Definition: an inherited impairment of haemoglobin
production, in which there is partial or complete failure to
synthesise either the α- or β-globin chains of HbA.
o Types:
• Beta thalassaemia
– Thalassaemia minor
– Thalassaemia major
• Alpha thalassaemia
© Endeavour College of Natural Health www.endeavour.edu.au 39
Thalassaemia
o Aetiology:
• Beta thalassaemia: Multiple point mutations in the β -
globin gene causing a defect in β-chain synthesis
• Alpha thalassaemia: Deletion of alpha gene alleles on
chromosome 16
o Pathophysiology:
Genetic mutation→reduced rate of production of one or
other of the globin chains→ alpha to non-alpha chains
ratio altered → the excess chains precipitate within RBC
precursors → formation of abnormal haemoglobin with
less affinity for oxygen → RBC membrane damage and
haemolysis→ Microcytic Hypochromic anaemia
© Endeavour College of Natural Health www.endeavour.edu.au 40
Beta Thalassaemia
o Clinical features:
• Severe, blood transfusion–dependent anemia
Anaemia
• Bone marrow hyperplasia early in life.
• Impaired bone growth and Bone deformities
• Splenomegaly , Hepatomegaly
o Complications:
• Iron overload leading to Cardiac, hepatic, and
endocrine diseases and organ damage
© Endeavour College of Natural Health www.endeavour.edu.au 41
Beta Thalassaemia
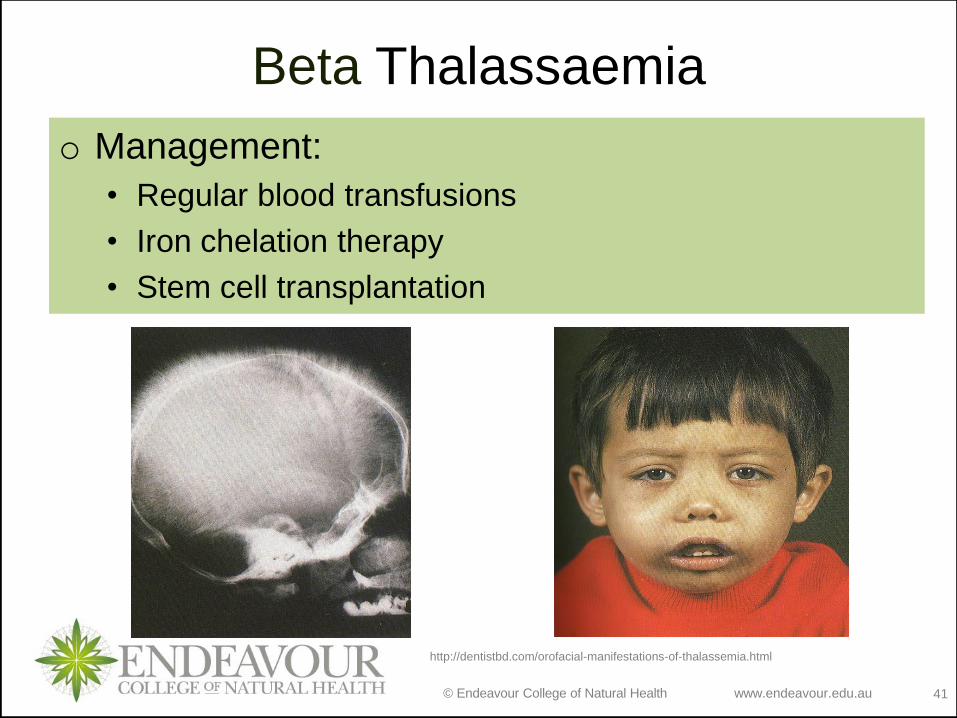
o Management:
• Regular blood transfusions
• Iron chelation therapy
• Stem cell transplantation
http://dentistbd.com/orofacial-manifestations-of-thalassemia.html
© Endeavour College of Natural Health www.endeavour.edu.au 42
Alpha Thalassaemia
o Clinical features: related to the number of gene
deletions
• One gene deletion: no clinical effect.
• Two genes deletion: mild hypochromic anaemia.
• Three gene deletion: Haemoglobin H disease.
• Four gene deletion: stillborn baby (hydrops fetalis).
o Management:
• Folic acid supplementation
• Transfusion if required
• Avoidance of iron therapy
© Endeavour College of Natural Health www.endeavour.edu.au 43
Reading and Resourceso Crowley LV, 2012, An Introduction to Human Diseases – Pathology and
Pathophysiology Correlations, 9th edn, Jones and Bartlett Learning
o Grossman SC & Porth CM 2014, Porth’s Pathophysiology- Concepts of
Altered Health States, 9th edn. Wolters Kluwer Health - Lippincott, Williams
& Wilkins
o Hinson, J, Raven, P & Chew, S 2010, The endocrine system: basic science
and clinical conditions, 2nd edn, Churchill Livingstone Elsevier, Edinburgh
o Jamison, JR 2006, Differential diagnosis for primary care: a handbook for
health care practitioners, 2nd edn, Churchill Livingstone Elsevier,
Edinburgh.
o Jarvis, C, 2012 Physical Examination & Health Assessment, 6th ed.,
Elsevier Saunders, Philadelphia.
o Kumar, P & Clark, M 2012, Kumar and Clark’s clinical medicine, 8th edn,
Saunders Elsevier, Edinburgh.
o Kumar, V, Abbas, AK & Aster, JC 2015, Robbins & Cotran pathologic basis
of disease, 9th edn, Elsevier Saunders, Philadelphia.
© Endeavour College of Natural Health www.endeavour.edu.au 44
Reading and Resourceso Lee, G & Bishop, P 2009, Microbiology and infection control for health
professionals, 4th edn, Pearson Education, Frenchs Forest, NSW.
o McCance, KL, Heuther, SE, & Brashers, VL 2014, Pathophysiology: the
biologic basis for disease in adults and children, 7th edn, Elsevier.
o Michael-Titus, A, Revest, P & Shortland, P 2010, The nervous system: basic
science and clinical conditions, 2nd edn, Churchill Livingstone Elsevier,
Edinburgh
o Mosby’s dictionary of medicine, nursing and health professions 2013, 9th
edn, Elsevier, St. Louis, MO.
o Tortora, GJ & Derrickson, B 2014, Principles of anatomy and physiology,
14th edn, John Wiley & Sons, Hoboken, NJ.
o VanMeter, KC & Hubert, RJ 2014, Gould's pathophysiology for the health
professions, 5th edn, Elsevier, St Louis, MO.
o Walker, BR, Colledge, NR, Ralston, SH, & Penman, ID (eds) 2014,
Davidson’s principles and practice of medicine, 22nd edn, Churchill
Livingstone Elsevier, Edinburgh.
© Endeavour College of Natural Health www.endeavour.edu.au 45
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and
communicated to you by or on behalf of
the Endeavour College of Natural Health pursuant to
Part VB of the Copyright Act 1968 (the Act).
The material in this communication may
be subject to copyright under the Act.
Any further reproduction or
communication of this material by you
may be the subject of copyright
protection under the Act.
Do not remove this notice.