-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
1/23
Official reprint from UpToDate
www.uptodate.com2013 UpToDate
Author
Victoria Hendrick, MD
Section Editor
Paul Keck, MD
Deputy Editor
David Solomon, MD
Bipolar disorder in women: Preconception and prenatal
maintenance pharmacotherapy
Disclosures
All topics are updated as new evidence becomes available and
ourpeer review process is complete.
Literature review current through:Oct 2013. | This topic last
updated:Nov 16, 2013.
INTRODUCTION Euthymic bipolar patients often receive maintenance
pharmacotherapy prior to conception and during
pregnancy [1,2]. Onset of bipolar disorder in women typically
occurs during childbearing years [3], and most patients are at
risk for recurrent mood episodes [1].
This topic reviews preconception and prenatal maintenance
pharmacotherapy for bipolar patients. Indications for
maintenance pharmacotherapy during pregnancy, the teratogenic
risks of medications used for bipolar disorder,
preconception counseling and care for bipolar disorder, and the
general maintenance treatment of bipolar disorder arediscussed
separately.
DEFINITION OF BIPOLAR DISORDER Bipolar disorder is characterized
by episodes of mania (table 1), hypomania
(table 2), and major depression (table 3) [4]. The subtypes of
bipolar disorder include bipolar I and bipolar II . Patients
with
bipolar I disorder experience manic episodes, and nearly always
experience major depressive and hypomanic episodes.
Bipolar II disorder is marked by at least one hypomanic episode,
at least one major depressive episode, and the absence of
manic episodes. Additional information about the clinical
features and diagnosis of bipolar disorder is discussed
separately.(See "Bipolar disorder in adults: Clinical features"and
"Bipolar disorder in adults: Assessment and diagnosis", section
on
'Diagnosis'.)
MANAGEMENT
General principles Preconception and prenatal maintenance
treatment for bipolar patients is usually provided by
perinatal or general psychiatrists in collaboration with
obstetricians and primary care clinicians [ 5-8].
After considering medical advice about the risks of fetal
exposure to medications and the risks of avoiding preconception
and
prenatal maintenance pharmacotherapy, bipolar patients can
choose to [ 9]:
For bipolar patients who plan to or do become pregnant, we
suggest maintenance pharmacotherapy to prevent mood
episodes, based upon prospective observational studies that
found untreated pregnant patients were at increased risk of
recurrent mood episodes [2,10], as well as our clinical
experience and that of several authorities [ 1,11-14]. However,
for
patients with a mild lifetime course of illness, it is
reasonable to try to avoid pharmacotherapy during pregnancy.
Indications
for preconception and prenatal maintenance pharmacotherapy,
risks of avoiding maintenance pharmacotherapy, and specific
drugs suggested as preconception and prenatal maintenance
treatment are discussed separately. (See "Bipolar disorder in
women: Indications for preconception and prenatal maintenance
pharmacotherapy"and 'Risks of avoiding pharmacotherapy'
below and 'Specific drugs'below.)
In prescribing preconception and prenatal maintenance
pharmacotherapy, clinicians should attempt to use [1,5,15]:
(See "Bipolar disorder in women: Indications for preconception
and prenatal maintenance pharmacotherapy".)
(See "Bipolar disorder in adults: Teratogenic and postnatal
risks of pharmacotherapy".)
(See "Bipolar disorder in women: Contraception and preconception
assessment and counseling".)
(See "Bipolar disorder in adults: Maintenance treatment".)
Maintain existing pharmacotherapy throughout conception, the
pregnancy, and birth
Switch medications before they try to conceive to avoid drugs
with a greater risk of teratogenicityDiscontinue pharmacotherapy
prior to conception and restart medications during the second or
third trimester (when
organogenesis is completed).
Discontinue pharmacotherapy prior to conception and remain
medication-free throughout conception, the pregnancy,
and delivery.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
2/23
For euthymic bipolar patients who are receiving preconception or
prenatal maintenance treatment with lamotrigine, a
second-generation antipsychotic, orlithium, we suggest
continuing the same drug [15,16]. For patients who are
currently
treated with valproateorcarbamazepine, we suggest switching
treatment to avoid the teratogenic effects of these two
antiepileptics [11,17]. (See 'Switching from valproate or
carbamazepine to less teratogenic drugs'below and "Risks
associated with epilepsy and pregnancy", section on 'Effect of
antiepileptic drugs on the fetus'.)
Female bipolar patients who want to conceive and continue
maintenance treatment with valproateorcarbamazepinecan
consider in vitro fertilization and use of a gestational carrier
[8]. (See "Surrogate pregnancy".)
Medication doses generally need to be increased over the course
of pregnancy, especially in the second and third
trimesters, to prevent decreases in serum concentrations
[18-21]. This is because pregnancy causes physiologic changes
that alter pharmacokinetics (eg, increased extracellular fluid
volume and body fat increase the volume of distribution,
increased activity of hepatic enzymes increases metabolism, and
increased renal blood flow and glomerular filtration rate
increase renal elimination).
Recurrent bipolar mood episodes may occur despite preconception
or prenatal maintenance pharmacotherapy because of
problems with adherence [9]. Suggestions for improving adherence
are discussed separately. (See "Bipolar disorder in
adults: Maintenance treatment", section on 'Adherence'.)
Risk of adverse pregnancy and birth outcomes The risk of adverse
pregnancy and birth outcomes in women with
bipolar disorder who receive pharmacotherapy and women with
bipolar disorder who are not treated with pharmacotherapy
is discussed separately. (See "Bipolar disorder in women:
Contraception and preconception assessment and counseling".)
Teratogenic and postnatal risks of pharmacotherapy Following the
first trimester, the risk of teratogenesis decreases
and it is safer to prescribe drug combinations and higher doses.
The teratogenic and postnatal risks of medications
commonly used to treat bipolar disorder are discussed
separately. (See "Bipolar disorder in adults: Teratogenic and
postnatal risks of pharmacotherapy".)
Risks of avoiding pharmacotherapy For bipolar patients who are
receiving preconception or prenatal maintenance
pharmacotherapy, discontinuing treatment includes the following
risks [2,10,13,17,22]:
Switching from valproate or carbamazepine to less teratogenic
drugs For bipolar patients who plan to become
pregnant, are treated with valproateorcarbamazepine, and are
clinically stable (eg, euthymic for at least six months), we
suggest that clinicians attempt to switch maintenance treatment
to other drugs [ 11,23]. Valproate and carbamazepine are
generally regarded as teratogens, primarily based upon
observational studies of epilepsy patients [1,5,24,25]. In
addition,
prenatal exposure to these medications is associated with
developmental delay [26]. Specific drugs suggested as
preconception and prenatal maintenance treatment and the
teratogenic effects of valproate and carbamazepine are
discussed separately. (See 'Specific drugs'below and "Risks
associated with epilepsy and pregnancy", section on 'Fetal and
neonatal effects'.)
For bipolar patients who plan to become pregnant and decide to
switch from valproateorcarbamazepineto a less
teratogenic drug, we suggest changing pharmacotherapy at least
three to six months before patients try to conceive, to
assess the effectiveness of the new medication. Valproate or
carbamazepine are tapered and discontinued over 15 to 30
days; this approach appears to be associated with a lower risk
of recurrence than a faster taper [2]. The medication is
tapered by the same amount for each dose decrease. As an
example, valproate 2000 mg per day is decreased by 250 to
500 mg per day, every three to seven days. At the same time, the
new medication is started and titrated up.
Alternative medications may not work as well as
valproateorcarbamazepine, and switching medications can precipitate
a
Drugs with fewer known teratogenic effects
Monotherapy
Doses at the low end of the therapeutic range
It is not known if maintenance drugs that are discontinued
provide the same level of prophylactic efficacy after they are
restarted.
Stopping treatment may increase the risk of recurrent mood
episodes, particularly if medications are discontinued
abruptly (eg, in less than two weeks). (See "Bipolar disorder in
women: Contraception and preconception assessment
and counseling", section on 'Relapse after discontinuing
pharmacotherapy'.)
Treating recurrent episodes during pregnancy may be difficult
and expose the fetus to more medications at higher
doses compared with pharmacologic maintenance of euthymia.
Postpartum mood episodes may occur more frequently in patients
who are not treated with maintenance
pharmacotherapy during pregnancy.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
3/23
recurrence of bipolar mood symptoms [27]. Thus, it is reasonable
to maintain valproate or carbamazepine for patients with a
history of poor outcomes using other medications, such as
lamotrigine, quetiapine, risperidone, and lithium. Patients
treated
with valproate or carbamazepine during pregnancy should also
receive high doses of folic acid(eg, 4 to 5 mg per day),
although the efficacy of folate supplementation in reducing the
risk of neural tube defects is not clear [ 28]. Managing
pregnant patients who receive valproate or carbamazepine is
discussed separately in the context of epilepsy, including the
use of folic acid. (See "Management of epilepsy and pregnancy",
section on 'Management during pregnancy and delivery'
and "Folic acid for prevention of neural tube defects", section
on 'Anticonvulsant therapy'.)
For bipolar patients who are maintained on
valproateorcarbamazepineand unexpectedly become pregnant, we
suggest
switching medications. (See 'Unplanned pregnancies'below.)
Monitoring patients Bipolar patients receiving preconception or
prenatal maintenance pharmacotherapy should be
regularly monitored for recurrence of manic and depressive
symptoms as well as medication side effects. Particular
attention is given to suicidal ideation and to psychotic
symptoms. Stable patients can be seen every one to two months.
For
patients who remit from an acute mood episode and remain stable,
monitoring can be tapered, with progressively longer
intervals between assessments. As an example, a patient who is
seen every two weeks at the time of remission can be
seen every two weeks for one to three more visits, then every
one to two months until parturition. More frequent visits
should be scheduled for patients who develop symptoms or side
effects; monitoring acutely ill patients is discussed
separately. (See "Bipolar disorder in pregnant women: Treatment
of mania and hypomania", section on 'Monitoring the
patient'.)
Adjunctive psychotherapy For bipolar patients who receive
preconception or prenatal maintenance pharmacotherapy,
we suggest adjunctive psychoeducation or cognitive-behavioral
therapy (CBT), based upon randomized trials that excluded
pregnant patients. Although no head-to-head trials have compared
these psychotherapies, we generally choose
psychoeducation because there are more data supporting its use,
it is easier to administer than CBT and thus usually more
available, and psychoeducation is generally an element of CBT.
The evidence of efficacy for reducing recurrent mood
episodes with other psychotherapies, such as family therapy and
interpersonal and social rhythm therapy, is not as strong.
(See "Bipolar disorder in adults: Maintenance treatment",
section on 'Adjunctive psychotherapy'.)
SPECIFIC DRUGS There are no randomized trials in bipolar
patients who plan to or do become pregnant to guide
preconception and prenatal maintenance pharmacotherapy; the
benefits and risks of treatment are thus based upon
randomized trials that excluded pregnant patients [29-31], as
well as observational studies, birth registries, and clinical
experience [18].
First line For euthymic, bipolar patients who plan to or do
become pregnant, we suggest lamotrigineas first line
maintenance treatment [5], based upon randomized trials that
excluded pregnant patients. There are more data supporting
the efficacy of lamotrigine for the general maintenance
treatment of bipolar disorder compared with quetiapineand
risperidone. In addition, a prospective observational study of
euthymic, pregnant bipolar patients found that relapse occurred
in significantly fewer patients who continued lamotrigine (N =
10) than patients who stopped pharmacotherapy (N = 16) (30
versus 100 percent) [10]. Further, the reproductive safety
profile of lamotrigine is generally regarded as favorable
[5,24,32],
and there is more experience using lamotrigine during pregnancy
compared with quetiapine and risperidone. Although there
are more data supporting the efficacy oflithiumthan lamotrigine,
the reproductive safety of lamotrigine is generally regarded
as comparable or superior to lithium.
Evidence for the efficacy oflamotrigine, quetiapine,
risperidone, and lithiumfor delaying or preventing bipolar mood
episodes
is discussed separately, as are the reproductive safety profile
of these drugs, and the dose schedule, side effect profile,
andpharmacology of lamotrigine. (See "Bipolar disorder in adults:
Maintenance treatment", section on 'Pharmacotherapy'and
"Bipolar disorder in adults: Teratogenic and postnatal risks of
pharmacotherapy"and "Pharmacology of antiepileptic drugs",
section on 'Lamotrigine'.)
Resistant patients Maintenance treatment for bipolar disorder
with lamotrigineis often not efficacious, based upon
randomized trials (which excluded pregnant patients) [29]. For
resistant bipolar patients who do not respond to or tolerate
preconception or prenatal maintenance lamotrigine, we suggest
quetiapineorrisperidone, based upon their efficacy and
adverse effects in randomized trials that excluded pregnant
patients [30,33]. (Response is defined as psychopathology that
is considerably less than full criteria for a mood episode, eg,
no more than two moderately or three mildly intense
symptoms.) No head-to-head trials have compared quetiapine and
risperidone. The specific choice is thus based upon other
factors, including past response to medications, side effect
profiles, comorbid general medical conditions, patient
preference, and cost.
Although there are more data supporting the maintenance efficacy
oflithiumthan quetiapineorrisperidone, study findings
suggest that quetiapine and risperidone are not associated with
an increased risk of major malformations [34-37], whereas
lithium is generally regarded as teratogenic [20,23,38]. In
addition, the preference for treating pregnant bipolar patients
with
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
4/23
quetiapine or risperidone rather than lithium is consistent with
practice guidelines from the United Kingdom National Institute
for Health and Clinical Excellence [9,39]. However, second
generation antipsychotics may cause metabolic complications.
(See 'Metabolic complications'below.)
To switch drugs, lamotrigineis tapered and discontinued over one
to two weeks while at the same time quetiapineor
risperidoneis started and titrated up. We generally taper
lamotrigine by the same amount for each dose decrease. As an
example, lamotrigine 200 mg per day is decreased by 50 mg per
day, every two to three days.
For resistant bipolar patients who do not respond to
preconception or prenatal maintenance treatment with
eitherquetiapine
orrisperidone, we suggest tapering and discontinuing the failed
medication over one to two weeks while at the same timethe other
drug is started and titrated up. The failed medication is generally
tapered by the same amount for each dose
decrease.
The efficacy ofquetiapineand risperidonefor the general
maintenance treatment of bipolar disorder is discussed
separately,
as is the dose, side effect profile (table 4), pharmacology, and
reproductive safety profile. (See "Bipolar disorder in adults:
Maintenance treatment"and "Bipolar disorder in adults:
Pharmacotherapy for acute mania, mixed episodes, and hypomania"
and "Second-generation antipsychotic medications: Pharmacology,
administration, and comparative side effects" and
"Bipolar disorder in adults: Teratogenic and postnatal risks of
pharmacotherapy", section on 'Second-generation'.)
Metabolic complications Second-generation antipsychotics may
cause hyperglycemia [40]. In pregnant women with
diabetes, hyperglycemia is associated with increased risks of
spontaneous abortion, congenital malformations, and
macrosomia. (See "Pregnancy risks in women with type 1 and type
2 diabetes mellitus", section on 'Fetal and
neonatalcomplications'.)
In addition, second-generation antipsychotics may cause obesity
[40,41]. Obesity during pregnancy is associated with an
increased risk of multiple obstetric complications, including
gestational diabetes mellitus and pre-eclampsia. (See "The
impact of obesity on female fertility and pregnancy".) Although
many clinicians use second-generation antipsychotics during
pregnancy [42], some authorities avoid them due to concerns
about excessive weight gain and gestational diabetes
[24,25,43].
Clinicians using second-generation antipsychotics in pregnant
patients should manage potential metabolic complications by
monitoring [9,23,39]:
Patients are assessed at baseline and every one to three months
during pregnancy [17,23]. In addition, a glucose tolerance
test is performed every four months. (See "Screening and
diagnosis of diabetes mellitus during pregnancy".)
Refractory patients Based upon clinical experience, many bipolar
patients do not respond to or tolerate sequential trials
of preconception or prenatal maintenance lamotrigine,
quetiapine, and risperidone. For these refractory patients, we
suggest
lithium[11,17]. (Response is defined as psychopathology that is
considerably less than full criteria for a mood episode, eg,
no more than two moderately or three mildly intense symptoms.)
Evidence for the efficacy of lithium includes the following:
Although lithiumis generally regarded as teratogenic due to
increased risks of cardiac defects (eg, Ebsteins anomaly)
[20,23,38], many authorities consider the absolute risk small
[1,5,24,25,44]. For pregnant patients using lithium, we suggest
prenatal screening for anomalies with high-resolution
ultrasonography at 16 to 18 weeks gestation, and depending upon
the
results, fetal echocardiography, which can aid decisions about
pregnancy termination, referral for delivery at a hospital with
Weight gain
Blood pressure
Fasting serum glucose, cholesterol, and triglyceride
concentrations. The normal reference range for cholesterol and
triglycerides is generally higher in pregnant women compared
with nonpregnant individuals (table 5). (See "Normal
reference ranges for laboratory values in pregnancy".)
Randomized tr ials (that excluded pregnant patients) have
demonstrated the benefit of maintenance treatment with
lithiumin bipolar disorder; these trials are discussed
separately. (See "Bipolar disorder in adults: Maintenance
treatment", section on 'Lithium'.)
A prospective observational study found that relapse occurred in
significantly fewer pregnant bipolar patients who
continued pharmacotherapy (N = 27, 85 percent received lithium)
than patients who stopped pharmacotherapy (N =
62) (37 versus 86 percent) [2].
A prospective observational study found that relapse occurred in
fewer pregnant bipolar patients who received
maintenance pharmacotherapy (N = 31, 97 percent received
lithium) than patients who did not (N = 10) (19 versus 40
percent; statistical significance not tested) [15].
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
5/23
the appropriate level of neonatal care, and postnatal
interventions for congenital malformations [1,8,25]. The
teratogenic
effects of lithium are discussed separately. (See "Bipolar
disorder in adults: Teratogenic and postnatal risks of
pharmacotherapy", section on 'Lithium'.)
For pregnant patients treated with lithium, we suggest using the
lowest amount necessary to achieve a therapeutic serum
concentration [20]. The total daily dose is often given in two
to three divided doses (rather than a single daily dose) using
controlled release preparations, to avoid high peak serum levels
[ 15,45,46]; however, it is not known whether this reduces
the risk of teratogenic effects [45]. Serum lithium
concentrations are checked every two to four weeks during
pregnancy,
until 36 weeks gestation, at which point levels should be
checked weekly [7,21,23]. The dose schedule for lithium, use of
serum concentrations to establish the proper dose, and lithium
toxicity are discussed separately. (See "Bipolar disorder in
adults and lithium: Pharmacology, administration, and side
effects".)
Additional laboratory monitoring oflithiumincludes thyroid and
renal function tests that are checked at baseline and repeated
every three months [23]. Normal reference ranges for laboratory
tests often differ for gravid and nongravid patients ( table
5). (See "Normal reference ranges for laboratory values in
pregnancy".)
Serum lithiumconcentrations generally decrease during pregnancy
and the doses required to effectively prevent bipolar
mood episodes thus increase [1,19]. These changes are a
consequence of increases in maternal glomerular filtration rate
and extracellular fluid volume and their impact upon
pharmacokinetics. As an example, renal excretion of lithium may
increase 30 to 100 percent [20,21,46]. During the second and
third trimesters, twice the prepregnancy dose of lithium may
be required to achieve therapeutic serum concentrations [45]. In
addition, serum lithium concentrations can be altered by
concomitant medications and other clinical factors (eg,
diarrhea). (See "Bipolar disorder in adults and lithium:
Pharmacology,
administration, and side effects", section on 'Prescribing
lithium'.)
Frequent urination, thirst, weight gain, and nausea are common
during pregnancy and can be exacerbated by lithium. Side
effects of lithium are discussed separately. (See "Bipolar
disorder in adults and lithium: Pharmacology, administration,
and
side effects", section on 'Lithium side effects' .)
For pregnant patients treated with lithium, delivery should
occur in facilities with the ability to resuscitate neonates, given
the
risks of postnatal complications [23]. Postnatal toxicity and
withdrawal secondary to lithium are discussed separately. (See
"Bipolar disorder in adults: Teratogenic and postnatal risks of
pharmacotherapy", section on 'Lithium'.)
We suggest withholding lithiumfor one to two days before a
scheduled delivery or at the onset of labor, consistent with
the
practice of many perinatal psychiatrists [7,21,47]. Although a
brief reduction in serum lithium concentrations may possibly
precipitate a postpartum relapse, the risk seems small. In a
prospective observational study of nine pregnant bipolar
patients treated with lithium in the third trimester, lithium
was withheld for one to two days before a scheduled delivery or
at
the onset of labor; maternal serum concentrations decreased from
a mean of 0.8 mEq/L (0.8 mmol/L) to 0.5 mEq/L (0.5
mmol/L), and none of the patients became symptomatic [ 47].
For pregnant patients treated with lithium, adequate hydration
must be maintained throughout labor, especially if the serum
level drawn at the time of delivery is high. During labor and
delivery, vascular volume can decrease through loss of blood as
well as diaphoresis [19]. Intravenous fluids are typically used
to prevent dehydration and lithium toxicity [7,17].
After delivery, lithiumis resumed when patients are medically
stable (provided breastfeeding is not planned) at doses lower
than those used during the third trimester, because maternal
glomerular filtration rates rapidly decrease to pregravid
levels
[47,48]. Patients treated with lithium prior to conception are
restarted on the prepregnancy dose. Patients not treated with
lithium prior to conception are usually started at a dose of 600
to 900 mg per day, which is then increased by 300 to 600 mgevery
one to five days based upon response, tolerability, and body mass
index. Serum concentrations are measured 24
hours after delivery and every three to five days until they
stabilize at a therapeutic level. (See "Bipolar disorder in adults
and
lithium: Pharmacology, administration, and side effects",
section on 'Lithium dose and serum concentrations'.)
The newborn should be monitored for symptoms of lithiumtoxicity
for up to 10 days after delivery [20,48], even if the
maternal serum lithium concentration at delivery is within
normal limits. Signs of neonatal toxicity at the time of
delivery
should prompt a cord serum level [23] and a neonatal
electrocardiogram [20,48]. Neonatal lithium toxicity and withdrawal
are
discussed separately. (See "Bipolar disorder in adults:
Teratogenic and postnatal risks of pharmacotherapy", section on
'Lithium'.)
UNPLANNED PREGNANCIES Unintended pregnancies in bipolar patients
are common and may precipitate mood
episodes. Two prospective observational studies of pregnant
bipolar pat ients (N = 89 and 26) found that the pregnancy wasnot
planned in 34 and 58 percent, and that unplanned pregnancy was
associated with recurrent prenatal mood episodes
[2,10].
For euthymic bipolar patients who unintentionally become
pregnant during maintenance treatment with lamotrigine, a
second-
generation antipsychotic, or lithium, we suggest continuing the
same drug [15,16].
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
6/23
For bipolar patients who are maintained on
valproateorcarbamazepineand unexpectedly become pregnant, we
suggest
switching medications. We typically titrate up the new drug as
rapidly as tolerated, and then taper and discontinue the
antiepileptic over the course of a few days. The antiepileptic
is decreased the same amount for each dose reduction. As an
example, valproate 1500 mg per day is decreased by 500 mg every
one to two days. The choice of a new drug is discussed
elsewhere in this topic, as is management of patients who
decline switching medications. (See 'Specific drugs'above and
'Switching from valproate or carbamazepine to less teratogenic
drugs'above.)
Bipolar patients who unexpectedly become pregnant may decide to
discontinue maintenance pharmacotherapy. However,
stopping medications (particularly over a period of less than
two weeks) may increase the risk of recurrent mood episodes.
(See "Bipolar disorder in women: Contraception and preconception
assessment and counseling", section on 'Relapse after
discontinuing pharmacotherapy'.)
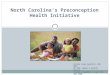
Determining the gestational age will inform the decision to use
maintenance pharmacotherapy in bipolar patients with
unplanned pregnancies. The period of greatest risk for the
teratogenic effects of medications is between the third and
eighth
week of gestation (weeks of gestation are counted from the first
day of the last menstrual period) (figure 1and figure 2).
Many unplanned pregnancies are discovered after this period of
greatest r isk has passed [1,49]; thus, discontinuing or
switching treatment at this point often puts the mother at risk
for relapse of a mood episode and provides minimal benefit to
the fetus [42].
FOLIC ACID SUPPLEMENTATION Folic acidis recommended for every
woman planning to conceive a child and is
discussed separately. (See "Nutrition in pregnancy", section on
'Folic acid'and "Folic acid for prevention of neural tube
defects"and "Management of epilepsy and pregnancy", section on
'Folic acid supplementation'.)
INFORMATION FOR PATIENTS UpToDate offers two types of patient
education materials, The Basics and Beyond
the Basics. The Basics patient education pieces are written in
plain language, at the 5 to 6 grade reading level, and they
answer the four or five key questions a patient might have about
a given condition. These articles are best for patients who
want a general overview and who prefer short, easy-to-read
materials. Beyond the Basics patient education pieces are
longer, more sophisticated, and more detailed. These articles
are written at the 10 to 12 grade reading level and are best
for patients who want in-depth information and are comfortable
with some medical jargon.
Here are the patient education articles that are relevant to
this topic. We encourage you to print or e-mail these topics to
your patients. (You can also locate patient education articles
on a variety of subjects by searching on patient info and the
keyword(s) of interest.)
These educational materials can be used as part of
psychoeducational psychotherapy. (See "Bipolar disorder in
adults:
Maintenance treatment", section on 'Psychoeducation'.)
The National Institute of Mental Health also has educational
material explaining the symptoms, course of illness, and
treatment of bipolar disorder in a booklet entitled "Bipolar
Disorder," which is available online at the website
http://www.nimh.nih.gov/health/publications/bipolar-disorder/complete-index.shtml
or through a toll-free number,
866-615-6464. The web site also provides references, summaries
of study results in language intended for the lay public,
and information about clinical trials currently recruiting
patients.
More comprehensive information is provided in many books written
for patients and family members, including The Bipolar
Disorder Survival Guide: What You and Your Family Need to Know,
written by David J. Miklowitz, PhD (published by The
Guilford Press, 2002); An Unquiet Mind: A Memoir of Moods and
Madness, written by Kay Jamison, PhD (published by
Random House, 1995); and Treatment of Bipolar Illness: A
Casebook for Clinicians and Patients, by RM Post, MD, and GS
Leverich, LCSW (published by Norton Press, 2008).
The Depression and Bipolar Support Alliance
(http://www.dbsalliance.orgor 800-826-3632) is a national
organization that
educates members about bipolar disorder and how to cope with it.
Other functions include increasing public awareness of
the illness and advocating for more research and services. The
organization is administered and maintained by patients and
family members, and has local chapters.
The National Alliance on Mental Illness (http://www.nami.orgor
800-950-6264) is a similarly structured organization devoted
to education, support, and advocacy for patients with any mental
illness. Bipolar disorder is one of their priorities.
SUMMARY AND RECOMMENDATIONS
th th
th th
Basics topics (See "Patient information: Bipolar disorder (The
Basics)"and "Patient information: Reducing the costs of
medicines (The Basics)".)
Beyond the Basics topics (See "Patient information: Bipolar
disorder (manic depression) (Beyond the Basics)"and
"Patient information: Reducing the costs of medicines (Beyond
the Basics)".)
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
7/23
Use of UpToDate is subject to the Subscription and License
Agreement.
Topic 16971 Version 5.0
Bipolar disorder is characterized by episodes of mania ( table
1), hypomania (table 2), and major depression (table 3).
(See 'Definition of bipolar disorder'above and "Bipolar disorder
in adults: Assessment and diagnosis", section on
'Diagnosis'.)
Bipolar disorder is a highly recurrent illness. For bipolar
patients who plan to or do become pregnant, we suggest
maintenance pharmacotherapy rather than no treatment (Grade 2C).
However, for patients with a mild lifetime course
of illness, it is reasonable to try to avoid pharmacotherapy
during pregnancy. (See 'General principles'above and
"Bipolar disorder in women: Indications for preconception and
prenatal maintenance pharmacotherapy"and 'Risks of
avoiding pharmacotherapy'above.)
In prescribing preconception or prenatal maintenance
pharmacotherapy for bipolar patients, clinicians should attempt
to
use drugs with fewer known teratogenic effects, monotherapy, and
doses at the low end of the therapeutic range.
Following the first trimester, the risk of teratogenesis
decreases and it is safer to prescribe drug combinations and
higher doses. (See 'General principles'above.)
Valproateand carbamazepineare generally regarded as teratogens.
For stable bipolar patients who plan to or do
become pregnant and are currently treated with valproate and
carbamazepine, we suggest switching treatment to a
less teratogenic drug rather than maintaining valproate or
carbamazepine (Grade 2C). However, it is reasonable to
maintain valproate or carbamazepine for patients with a history
of poor outcomes using other medications. (See
'Switching from valproate or carbamazepine to less teratogenic
drugs'above.)
For bipolar patients who plan to or do become pregnant, we
suggest lamotrigineas first line maintenance treatmentrather than
other medications (Grade 2C). (See 'First line'above.)
For patients who are unresponsive to or intolerant of
lamotrigine, we suggest quetiapineorrisperidonerather than
other medications (Grade 2C). (See 'Resistant
patients'above.)
For refractory patients who do not respond to sequential
maintenance treatment trials with lamotrigine, quetiapine, and
risperidone, lithiumis a reasonable option. Although lithium is
generally regarded as teratogenic due to increased risks
of cardiac defects, the absolute risk is considered low. (See
'Refractory patients'above.)
For bipolar patients with unplanned pregnancies, determining the
gestational age will inform the decision to use
maintenance pharmacotherapy. The period of greatest r isk for
the teratogenic effects of medications is between the
third and eighth week of gestation ( figure 1and figure 2). (See
'Unplanned pregnancies'above.)
Every woman planning to conceive a child should receive folic
acid. (See "Nutrition in pregnancy", section on 'Folic acid'
and "Folic acid for prevention of neural tube defects"and
"Management of epilepsy and pregnancy", section on 'Folic
acid supplementation'.)
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
8/23
GRAPHICS
DSM-5 diagnostic criteria for manic episode
A.A distinct period of abnormally and persistently elevated,
expansive, or irritable mood and abnormally
and persistently increased goal-directed activity or energy,
lasting at least one week and present most of
the day, nearly every day (or any duration if hospitalization is
necessary).
B.During the period of mood disturbance and increased energy or
activity, three (or more) of the following
symptoms (four if the mood is only irritable) are present to a
significant degree and represent a noticeablechange from usual
behavior:
1) Inflated self-esteem or grandiosity.
2) Decreased need for sleep (eg, feels rested after only three
hours of sleep).
3) More talkative than usual or pressure to keep talking.
4) Flight of ideas or subjective experience that thoughts are
racing.
5) Distractibility (ie, attention too easily drawn to
unimportant or irrelevant external stimuli), as reported
or observed.
6) Increase in goal-directed activity (either socially, at work
or school, or sexually) or psychomotor
agitation (ie, purposeless non-goal-directed activity).
7) Excessive involvement in activities that have a high
potential for painful consequences (eg, engaging
in unrestrained buying sprees, sexual indiscretions, or foolish
business investments).
C.The mood disturbance is sufficiently severe to cause marked
impairment in social or occupational
functioning or to necessitate hospitalization to prevent harm to
self or others, or there are psychotic
features.
D.The episode is not attributable to the physiological effects
of a substance (eg, a drug of abuse, a
medication, other treatment) or to another medical
condition.
NOTE:A full manic episode that emerges during antidepressant
treatment (eg, medication,
electroconvulsive therapy) but persists at a fully syndromal
level beyond the physiological effect of that
treatment is sufficient evidence for a manic episode and,
therefore, a bipolar I diagnosis.
NOTE:Criteria A through D constitute a manic episode. At least
one lifetime manic episode is
required for the diagnosis of bipolar I disorder.Reprinted with
permission from the Diagnostic and Statistical Manual of Mental
Disorders, Fifth Edition, (Copyright 2013). American Psychiatric
Association. All Rights Reserved.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
9/23
DSM-5 diagnostic criteria for hypomanic episode
A.A distinct period of abnormally and persistently elevated,
expansive, or irritable mood and abnormally
and persistently increased activity or energy, lasting at least
four consecutive days and present most of the
day, nearly every day.
B.During the period of mood disturbance and increased energy and
activity, three (or more) of the
following symptoms (four if the mood is only irritable) have
persisted, represent a noticeable change from
usual behavior, and have been present to a significant
degree:
1) Inflated self-esteem or grandiosity.
2) Decreased need for sleep (eg, feels rested after only three
hours of sleep).
3) More talkative than usual or pressure to keep talking.
4) Flight of ideas or subjective experience that thoughts are
racing.
5) Distractibility (ie, attention too easily drawn to
unimportant or irrelevant external stimuli), as reported
or observed.
6) Increase in goal-directed activity (either socially, at work
or school, or sexually) or psychomotor
agitation.
7) Excessive involvement in activities that have a high
potential for painful consequences (eg, engaging
in unrestrained buying sprees, sexual indiscretions, or foolish
business investments).
C.The episode is associated with an unequivocal change in
functioning that is uncharacteristic of the
individual when not symptomatic.
D.The disturbance in mood and the change in functioning are
observable by others.
E.The episode is not severe enough to cause marked impairment in
social or occupational functioning or to
necessitate hospitalization. If there are psychotic features,
the episode is, by definition, manic.
F.The episode is not attributable to the physiological effects
of a substance (eg, a drug of abuse, a
medication, or other treatment).
NOTE:A full hypomanic episode that emerges during antidepressant
treatment (eg, medication,
electroconvulsive therapy) but persists at a fully syndromal
level beyond the physiological effect of that
treatment is sufficient evidence for a hypomanic episode
diagnosis. However, caution is indicated so that
one or two symptoms (particularly increased irritability,
edginess, or agitation following antidepressant
use) are not taken as sufficient for a diagnosis of a hypomanic
episode, nor necessarily indicative of a
bipolar diathesis.
NOTE:Criteria A through F constitute a hypomanic episode.
Hypomanic episodes are common in
bipolar I disorder but are not required for the diagnosis of
bipolar I disorder.Reprinted with permission from the Diagnostic
and Statistical Manual of Mental Disorders, Fifth Edition,
(Copyright 2013). American Psychiatric Association. All Rights
Reserved.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
10/23
DSM-5 diagnostic criteria for bipolar major depression
A.Five (or more) of the following symptoms have been present
during the same two-week period and
represent a change from previous functioning; at least one of
the symptoms is either (1) depressed mood or
(2) loss of interest or pleasure.
NOTE:Do not include symptoms that are clearly attributable to
another medical condition.
1) Depressed mood most of the day, nearly every day, as
indicated by either subjective report (eg, feels
sad, empty, hopeless) or observations made by others (eg,
appears tearful). (NOTE: In children and
adolescents can be irritable mood.)
2) Markedly diminished interest or pleasure in all, or almost
all, activities most of the day, nearly every
day (as indicated by either subjective account or
observation)
3) Significant weight loss when not dieting or weight gain (eg,
a change of more than 5 percent of body
weight in a month), or decrease or increase in appetite nearly
every day. (NOTE: In children, consider
failure to make expected weight gain.)
4) Insomnia or hypersomnia nearly every day
5) Psychomotor agitation or retardation nearly every day
(observable by others, not merely subjective
feelings of restlessness or being slowed down)
6) Fatigue or loss of energy nearly every day
7) Feelings of worthlessness or excessive or inappropriate guilt
(which may be delusional) nearly every
day (not merely self-reproach or guilt about being sick)
8) Diminished ability to think or concentrate, or
indecisiveness, nearly every day (either by their
subjective account or as observed by others)
9) Recurrent thoughts of death (not just fear of dying),
recurrent suicidal ideation without a specific plan,
or a suicide attempt or a specific plan for committing
suicide
B.The symptoms cause clinically significant distress or
impairment in social, occupational, or other
important areas of functioning.
C.The episode is not attributable to the direct physiological
effects of a substance or to another medical
condition.
NOTE:Criteria A through C represent a major depressive
episode.
NOTE:Responses to a significant loss (eg, bereavement, financial
ruin, losses from a natural disaster, a
serious medical illness or disability) may include the feelings
of intense sadness, rumination about the loss,
insomnia, poor appetite, and weight loss noted in Criterion A,
which may resemble a depressive episode.
Although such symptoms may be understandable or considered
appropriate to the loss, the presence of a
major depressive episode in addition to the normal response to a
significant loss should also be carefully
considered. This decision inevitably requires the exercise of
clinical judgement based on the individual's
history and the cultural norms for the expression of distress in
the context of loss.
D.The occurence of the major depressive episode is not better
explained by schizoaffective disorder,
schizophrenia, schizophreniform disorder, delusional disorder,
or other specified and unspecified
schizophrenia spectrum and other psychotic disorders.
Specify:
With anxious distress
With mixed features
With rapid cycling
With melancholic features
With atypical features
With psychotic features
With catatonia
With peripartum onset
With seasonal pattern
Adapted with permission from the Diagnostic and Statistical
Manual of Mental Disorders, Fifth Edition, (Copyright
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
11/23
2013). American Psychiatric Association. All Rights
Reserved.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
12/23
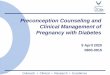
Selected adverse effects of antipsychotic medications for
schizophrenia
Weight
gain/diabetes
mellitus
Hyper-
cholesterolemiaEPS/TD
Prolactin
elevationSedation
An
First generation agents
Chlorpromazine +++ +++ + ++ +++
Fluphenazine + + +++ +++ +
Haloperidol + + +++ +++ ++
Loxapine ++ ND ++ ++ ++
Perphenazine ++ ND ++ ++ ++
Pimozide + ND +++ ++ +
Thioridazine* ++ ND + +++ +++
Thiothixene ++ ND +++ ++ +
Trifluoperazine ++ ND +++ ++ +
Second generation agents
Aripiprazole + +
Asenapine + + ++ ++
Clozapine +++ +++ +++
Iloperidone ++ ++ + +
Lurasidone + + ++
Olanzapine +++ +++ + ++
Paliperidone ++ + ++ +++ +
Quetiapine ++ +++ ++
Risperidone ++ + ++ +++ +
Ziprasidone + + +
Adverse effects may be dose dependent.EPS: extrapyramidal
symptoms; TD: tardive dyskinesia; ND: no data.* Thioridazine is
also associated with dose-dependent retinitis pigmentosa. Refer to
text. Clozapine also causes granulocytopenia or agranulocytosis in
approximately 1 percent of patients requiring regularblood cell
count monitoring.Adapted from:
Treatment Guidelines from The Medical Letter, August 2010; Vol.
8 (96):61. www.medicalletter.org.1.
[1]
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
13/23
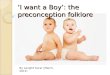
Normal reference ranges in pregnant women
Nonpregnant
adult*
First
trimester
Second
trimester
Third
trimesterReferences
Hematology
Erythropoietin (U/L) 4-27 12-25 8-67 14-222 1-3
Ferritin (ng/mL) 10-150 6-130 2-230 0-116 1-8
Folate, red blood cell
(ng/mL)
150-450 137-589 94-828 109-663 6, 9, 10
Folate, serum (ng/mL) 5.4-18.0 2.6-15.0 0.8-24.0 1.4-20.7 1, 6,
9-13
Hemoglobin (g/dL) 12-15.8 11.6-13.9 9.7-14.8 9.5-15.0 2, 3, 6,
7, 13
Hematocrit (percent) 35.4-44.4 31.0-41.0 30.0-39.0 28.0-40.0 1,
2, 5, 6,
13-15
Iron, total binding
capacity (g/dL)
251-406 278-403 Not reported 359-609 7
Iron, serum (g/dL) 41-141 72-143 44-178 30-193 2, 7
Mean corpuscular
hemoglobin (pg/cell)
27-32 30-32 30-33 29-32 5
Mean corpuscular
volume (xm )
79-93 81-96 82-97 81-99 5, 6, 13, 14
Platelet (x10 /L) 165-415 174-391 155-409 146-429 5, 6, 14, 16,
17
Mean platelet volume
(m )
6.4-11.0 7.7-10.3 7.8-10.2 8.2-10.4 5
Red blood cell count
(x10 /mm )
4.00-5.20 3.42-4.55 2.81-4.49 2.71-4.43 5, 6, 13, 14
Red cell distribution
width (percent)
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
14/23
Factor VIII (percent) 50-150 90-210 97-312 143-353 17, 25
Factor IX (percent) 50-150 103-172 154-217 164-235 17
Factor XI (percent) 50-150 80-127 82-144 65-123 17
Factor XII (percent) 50-150 78-124 90-151 129-194 17
Fibrinogen (mg/dL) 211-496 244-510 291-538 301-696 5, 17, 20,
21,
23, 24, 87
Homocysteine (mol/L) 4.4-10.8 3.34-11 2.0-26.9 3.2-21.4 6, 9,
10-12
International
Normalized Ratio
0.9-1.04 0.86-1.08 0.83-1.02 0.80-1.09 19, 24
Partial thromboplastin
time, activated (sec)
26.3-39.4 23.0-38.9 22.9-38.1 22.6-35.0 5, 17, 19, 24
Plasminogen activator
inhibitor-1 (PAI-1)
antigen (pg/mL)
17.3 +/ 5.7 17.7 +/ 1.9 Not reported 66.4 +/ 4.9 87
Plasminogen activator
inhibitor-1 (PAI-1)
activity (arbitrary units)
9.3 +/ 1.9 9.0 +/ 0.8 Not reported 31.4 +/ 3.0 87
Prothrombin time (sec) 12.7-15.4 9.7-13.5 9.5-13.4 9.6-12.9 5,
17, 24
Protein C, functional
(percent)
70-130 78-121 83-133 67-135 19, 25, 26
Protein S, total
(percent)
70-140 39-105 27-101 33-101 17, 25, 26
Protein S, free (percent) 70-140 34-133 19-113 20-65 25, 26
Protein S, functional
activity (percent)
65-140 57-95 42-68 16-42 25
Tissue plasminogen
activator (ng/mL)
1.6-13 1.8-6.0 2.36-6.6 3.34-9.20 17, 19, 87
Tissue plasminogen
activator inhibitor-1
(ng/mL)
4-43 16-33 36-55 67-92 17
von Willebrand measurements
von Willebrand factor
antigen (percent)
75-125 62-318 90-247 84-422 20, 27, 28
ADAMTS-13, von
Willebrand cleaving
protease
40-170 40-160 22-135 38-105 20, 28
Blood chemical constituents
Alanine transaminase
(U/L)
7-41 3-30 2-33 2-25 4, 5, 8, 29
Albumin (g/dL) 4.1-5.3 3.1-5.1 2.6-4.5 2.3-4.2 29-32
Alkaline phosphatase
(U/L)
33-96 17-88 25-126 38-229 4, 5, 8, 29, 30
Alpha-1 antitrypsin
(mg/dL)
100-200 225-323 273-391 327-487 5
Amylase (U/L) 20-96 24-83 16-73 15-81 4, 5, 33, 34
Anion gap (mmol/L) 7-16 13-17 12-16 12-16 5
Aspartate transaminase
(U/L)
12-38 3-23 3-33 4-32 4, 5, 8, 29
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
15/23
Bicarbonate (mmol/L) 22-30 20-24 20-24 20-24 5
Bilirubin, total (mg/dL) 0.3-1.3 0.1-0.4 0.1-0.8 0.1-1.1 4,
29
Bilirubin, unconjugated
(mg/dL)
0.2-0.9 0.1-0.5 0.1-0.4 0.1-0.5 5, 29
Bilirubin, conjugated
(mg/dL)
0.1-0.4 0-0.1 0-0.1 0-0.1 29
Bile acids (mol/L) 0.3-4.8 0-4.9 0-9.1 0-11.3 29, 35
CA-125 antigen (/mL) 7.2-27.0 2/2-268 12-25.1 16.8-43.8 88, 89,
90
Calcium, ionized
(mg/dL)
4.5-5.3 4.5-5.1 4.4-5.0 4.4-5.3 5, 31, 36, 37
Calcium, total (mg/dL) 8.7-10.2 8.8-10.6 8.2-9.0 8.2-9.7 4, 5,
30, 32,
36-38
Ceruloplasmin (mg/dL) 25-63 30-49 40-53 43-78 5, 39
Chloride (mEq/L) 102-109 101-105 97-109 97-109 4, 5, 40
Creatinine (mg/dL) 0.5-0.9 0.4-0.7 0.4-0.8 0.4-0.9 4, 5, 46
Gamma-glutamyltranspeptidase (U/L)
9-58 2-23 4-22 3-26 4, 5, 8, 29
Lactate dehydrogenase
(U/L)
115-221 78-433 80-447 82-524 4, 5, 32, 8
Lipase (U/L) 3-43 21-76 26-100 41-112 33
Magnesium (mg/dL) 1.5-2.3 1.6-2.2 1.5-2.2 1.1-2.2 4, 5, 30-32,
36,
38
Osmolality (mOsm/kg
H20)
275-295 275-280 276-289 278-280 38, 41
Phosphate (mg/dL) 2.5-4.3 3.1-4.6 2.5-4.6 2.8-4.6 4, 5, 30, 31,
42
Potassium (mEq/L) 3.5-5.0 3.6-5.0 3.3-5.0 3.3-5.1 4, 5, 15,
31,
32, 38, 40
Prealbumin (mg/dL) 17-34 15-27 20-27 14-23 5
Protein, total (g/dL) 6.7-8.6 6.2-7.6 5.7-6.9 5.6-6.7 5, 31,
32
Sodium (mEq/L) 136-146 133-148 129-148 130-148 4, 5, 15, 31,
32, 38, 41
Urea nitrogen (mg/dL) 7-20 7-12 3-13 3-11 4, 5, 40
Uric acid (mg/dL) 2.5-5.6 2.0-4.2 2.4-4.9 3.1-6.3 4, 5, 41
Metabolic and endocrine tests
Aldosterone (ng/dL) 2-9 6-104 9-104 15-101 43, 44, 45
Angiotensin converting
enzyme (U/L)
9-67 1-38 1-36 1-39 39, 46
Alpha-fetoprotein
(ng/mL)
0-8.5 Not reported 50-425 50-590 84, 86
Cortisol (g/dL) 0-25 7-19 10-42 12-50 5, 45
Hemoglobin A
(percent)
4-6 4-6 4-6 4-7 36, 47, 48
Parathyroid hormone
(pg/mL)
8-51 10-15 18-25 9-26 30
Parathyroid hormone-
related protein (pmol/L)
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
16/23
Renin, plasma activity
(ng/mL/h)
0.3-9.0 Not reported 7.5-54.0 5.9-58.8 40, 44
Thyroid-stimulating
hormone (IU/mL)
[American Thyroid
Association
recommendation]**
0.34-4.25 0.60-3.40 0.37-3.60 0.38-4.04 4, 5, 49
0.1-2.5 0.2-3.0 0.3-3.0 85
Thyroxine-binding
globulin (mg/dL)
1.3-3.0 1.8-3.2 2.8-4.0 2.6-4.2 5
Thyroxine, free (ng/dL) 0.8-1.7 0.8-1.2 0.6-1.0 0.5-0.8 5,
49
Thyroxine, total (g/dL) 5.4-11.7 6.5-10.1 7.5-10.3 6.3-9.7 5,
32
Triiodothyronine, free
(pg/mL)
2.4-4.2 4.1-4.4 4.0-4.2 Not reported 49
Triiodothyronine, total
(ng/dL)
77-135 97-149 117-169 123-162 5
Vitamins and minerals
Copper (g/dL) 70-140 112-199 165-221 130-240 50, 51, 5
Selenium (g/L) 63-160 116-146 75-145 71-133 5, 50
Vitamin A (retinol)
(g/dL)
20-100 32-47 35-44 29-42 5
Vitamin B12 (pg/mL) 279-966 118-438 130-656 99-526 6, 10
Vitamin C (ascorbic
acid) (mg/dL)
0.4-1.0 Not reported Not reported 0.9-1.3 52
Vitamin D,
1,25-dihydroxy (pg/mL)
25-45 20-65 72-160 60-119 30, 36
Vitamin D, 24,25-
dihydroxy (ng/mL)
0.5-5.0 1.2-1.8 1.1-1.5 0.7-0.9 53
Vitamin D, 25-hydroxy
(ng/mL)
14-80 18-27 10-22 10-18 30, 53
Vitamin E (-tocopherol)
(g/mL)
5-18 7-13 10-16 13-23 5
Zinc (g/dL) 75-120 57-88 51-80 50-77 5, 13, 50
Autoimmune and inflammatory mediators
C3 complement (mg/dL) 83-177 62-98 73-103 77-111 5
C4 complement (mg/dL) 16-47 18-36 18-34 22-32 5
C-reactive protein
(mg/L)
0.2-3.0 Not reported 0.4-20.3 0.4-8.1 54
Erythrocyte
sedimentation rate
(mm/h)
0-20 4-57 7-47 13-70 55
Immunoglobulin A
(mg/dL)
70-350 95-243 99-237 112-250 5
Immunoglobulin G
(mg/dL)
700-1700 981-1267 813-1131 678-990 5
Immunoglobulin M
(mg/dL)
50-300 78-232 74-218 85-269 5
Sex hormones
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
17/23
Dehydroepiandrosterone
sulfate (mol/L)
1.3-6.8 2.0-16.5 0.9-7.8 0.8-6.5 56
Estradiol (pg/mL)
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
18/23
Left vent, fractional
shortening (percent)
35-36 35-37 3.5 35-36 69, 70
Left vent ejection
fraction (percent)
60-73 61-75 61-63 60-73 69, 70
Atrial natriuretic peptide
(pg/mL)
Not reported Not reported 28.1-70.1 Not reported 73
B-type natriuretic
peptide (pg/mL)
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
19/23
reactive fibrinolysis . References values are from Cerneca et al
and Choi et al: Tissue plasminogen activator levels change with
plasmafibrinogen concentrations during pregnancy . Reference values
are from Mannuci et al: Changes in health and disease of the
metalloprotease that cleaves vonWillebrand factor . Reference
values are from Bacq Y et al: Liver function tests in normal
pregnancy: a prospective study of 102pregnant women and 102 matched
controls . Reference values are from the fi fteenth edition
ofHarrison's Principles of Internal Medicine .** The American
Thyroid Association recommends these TSH ranges if individual
laboratories do not determine theirown trimester-specific reference
ranges. Range is for premenopausal females and varies by menstrual
cycle phase. Reference values are from Leiserowitz GS et al:
Creatine kinase and its MB isoenzyme in the third trimester andthe
peripartum period .Reference values are from Dunlop W: Serial
changes in renal haemodynamics during normal humanpregnancy
.References:
[19]
[17,19]
[28]
[29]
[85]
[74]
[79]
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
20/23
Beguin Y, Lipscei G, Thourmsin H, et al: Blunted erythropoietin
production and decreased erythropoiesis in earlypregnancy. Blood
78(1):89, 1991.
1.
Bianco I, Mastropietro F, D'Aseri C, et al: Serum levels of
erythropoietin and soluble transferrin receptor duringpregnancy in
non--thalassemic and -thalassemic women. Haematologica 85:902, 2000
[PMID: 10980626].
2.
Milman N, Graudal N, Nielsen OJ: Serum erythropoietin during
normal pregnancy: Relationship to hemoglobinand iron status markers
and impact of iron supplementation in a longitudinal,
placebo-controlled study on 118women. Int J Hematol 66:159, 1997
[PMID: 9277046].
3.
Larsson A, Palm M, Hansson L-O, et al: Reference values for
clinical chemistry tests during normal pregnancy.BJOG 115:874, 2008
[PMID: 18485166].
4.
Lockitch G: Handbook of Diagnostic Biochemistry and Hematology
in Normal Pregnancy. Boca Raton, FL, CRCPress, 1993.
5.
Milman N, Bergholt T, Byg KE, et al: Reference intervals for
haematological variables during normal pregnancyand postpartum in
434 healthy Danish women. Eur J Haematol 79:39, 2007 [PMID:
17598837].
6.
Romslo I, Haram K, Sagen N, et al: Iron requirement in normal
pregnancy as assessed by serum ferritin, serumtransferring
saturation and erythrocyte protoporphyrin determinations. Br J
Obstet Gynaecol 90:101, 1983[PMID: 6824608].
7.
Van Buul EJA, Steegers EAP, Jongsma HW, et al: Haematological
and biochemical profile of uncomplicatedpregnancy in nulliparous
women; a longitudinal study. Neth J Med 46:73, 1995.
8.
Milman N, Byg KE, Hvas AM, et al: Erythrocyte folate, plasma
folate and plasma homocysteine during normalpregnancy and
postpartum: A longitudinal study comprising 404 Danish women. Eur J
Haematol 76:200, 2006[PMID: 16412135].
9.
Walker MC, Smith GN, Perkins SL, et al: Changes in homocysteine
levels during normal pregnancy. Am J ObstetGynecol 180:660, 1999
[PMID: 10076144].
10.
Lpez-Quesada E, Vilaseca MA, Lailla JM: Plasma total
homocysteine in uncomplicated pregnancy and inpreeclampsia. Eur J
Obstet Gynecol Reprod Biol 108:45, 2003 [PMID: 19899161].
11.
zerol E, zerol I, Gkdeniz R, et al: Effect of smoking on serum
concentrations of total homocysteine, folate,vitamin B12, and
nitric oxide in pregnancy: A preliminary study. Fetal Diagn Ther
19:145, 2004.
12.
Qvist I, Abdulla M, Jgerstad M, et al: Iron, zinc and folate
status during pregnancy and two months afterdelivery. Acta Obstet
Gynecol Scand 65:15, 1986 [PMID: 3716775].
13.
Balloch AJ, Cauchi MN: Reference ranges for haematology
parameters in pregnancy derived from patientpopulations. Clin Lab
Haemat 15:7, 1993 [PMID: 8472501].
14.
Singh HJ, Mohammad NH, Nila A: Serum calcium and parathormone
during normal pregnancy in Malay women.J Matern Fetal Med 8:95,
1999 [PMID: 10338062].
15.
AzizKarim S, Khurshid M, Rizvi JH, et al: Platelets and
leucocyte counts in pregnancy. J Pak Med Assoc 42:86,1992.
16.
Choi JW, Pai SH: Tissue plasminogen activator levels change with
plasma fibrinogen concentrations duringpregnancy. Ann Hematol
81:611, 2002 [PMID: 12454697].
17.
Belo L, Santos-Silva A, Rocha S, et al: Fluctuations in
C-reactive protein concentration and neutrophil activationduring
normal human pregnancy. Eur J Obstet Gynecol Reprod Biol 123:46,
2005 [PMID: 16260340].
18.
Cerneca F, Ricci G, Simeone R, et al: Coagulation and
fibrinolysis changes in normal pregnancy increased levelsof
procoagulants and reduced levels of inhibitors during pregnancy
induce a hypercoagulable state, combinedwith a reactive
fibrinolysis. Eur J Obstet Gynecol Reprod Biol 73:31, 1997 [PMID:
9175686].
19.
Lattuada A, Rossi E, Calzarossa C, et al: Mild to moderate
reduction of a von Willebrand factor cleaving protease(ADAMTS-13)
in pregnant women with HELLP microangiopathic syndrome.
Haematologica 88(9):1029, 2003.
20.
Francalanci I, Comeglio P, Liotta AA, et al: D-Dimer
concentrations during normal pregnancy, as measured byELISA. Thromb
Res 78:399, 1995 [PMID: 7660356].
21.
Kline JA, Williams GW, Hernandez-Nino J: D-Dimer concentrations
in normal pregnancy: New diagnosticthresholds are needed. Clin Chem
51:825, 2005 [PMID: 15764641].
22.
Morse M: Establishing a normal range for D-dimer levels through
pregnancy to aid in the diagnosis of pulmonaryembolism and deep
vein thrombosis. J Thromb Haemost 2:1202, 2004 [PMID:
15219216].
23.
Liu XH, Jiang YM, Shi H, et al: Prospective, sequential,
longitudinal study of coagulation changes duringpregnancy in
Chinese women. Int J Gynaecol Obstet 105(3):240, 2009.
24.
Lefkowitz JB, Clarke SH, Barbour LA: Comparison of protein S
functional and antigenic assays in normalpregnancy. Am J Obstet
Gynecol 175:657, 1996 [PMID: 8828430].
25.
Faught W, Garner P, Jones G, et al: Changes in protein C and
protein S levels in normal pregnancy. Am J ObstetGynecol 172:147,
1995 [PMID: 7847526].
26.
Wickstrm K, Edelstam G, Lwbeer CH, et al: Reference intervals
for plasma levels of fibronectin, von Willebrandfactor, free
protein S and antithrombin during third-trimester pregnancy. Scand
J Clin Lab Invest 64:31, 2004[PMID: 13035697].
27.
Mannucci PM, Canciani MT, Forza I, et al: Changes in health and
disease of the metalloprotease that cleaves von
Willebrand factor. Blood 98(9):2730, 2001.
28.
Bacq Y, Zarka O, Brchot JF, et al: Liver function tests in
normal pregnancy: A prospective study of 102pregnant women and 102
matched controls. Hepatology 23:1030, 1996 [PMID: 8621129].
29.
Ardawi MSM, Nasrat HAN, BA'Aqueel HS: Calcium-regulating
hormones and parathyroid hormone-relatedpeptide in normal human
pregnancy and postpartum: A longitudinal study. Eur J Endocrinol
137:402, 1997[PMID: 9368509].
30.
Handwerker SM, Altura BT, Altura BM: Serum ionized magnesium and
other electrolytes in the antenatal periodof human pregnancy. J Am
Coll Nutr 15:36, 1996 [PMID: 8632112].
31.
Hytten FE, Lind T: Diagnostic Indices in Pregnancy. Summit, NJ,
CIBA-GEIGY Corporation, 1975.32.Karsenti D, Bacq Y, Brchot JF, et
al: Serum amylase and lipase activities in normal pregnancy: A
prospectivecase-control study. Am J Gastroenterol 96:697, 2001
[PMID: 11280536].
33.
Strickland DM, Hauth JC, Widish J, et al: Amylase and isoamylase
activities in serum of pregnant women.Obstet Gynecol 63:389, 1984
[PMID: 6199704].
34.
Carter J: Serum bile acids in normal pregnancy. BJOG 98:540,
1991 [PMID: 1873244].35.Mimouni F, Tsang RC, Hertzbert VS, et al:
Parathyroid hormone and calcitriol changes in normal and
insulin-dependent diabetic pregnancies. Obstet Gynecol 74:49, 1989
[PMID: 2733941].
36.
Pitkin RM, Gebhardt MP: Serum calcium concentrations in human
pregnancy. Am J Obstet Gynecol 127:775,1977 [PMID: 848531].
37.
Shakhmatova EI, Osipova NA, Natochin YV: Changes in osmolality
and blood serum ion concentrations inpregnancy. Hum Physiol 26:92,
2000.
38.
Louro MO, Cocho JA, Tutor JC: Assessment of copper status in
pregnancy by means of determining the specificoxidase activity of
ceruloplasmin. Clin Chim Acta 312:123, 2001 [PMID: 11580917].
39.
Dux S, Yaron A, Carmel A, et al: Renin, aldosterone, and
serum-converting enzyme activity during normal and
40.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
21/23
Modified and reproduced with permission from: Abbassi-Ghanavati
M, Greer LG. Reference Table of Normal LaboratoryValues in
Uncomplicated Pregnancies. In: Cunningham FG, Leveno KJ, Bloom S,
Hauth JC, Rouse DJ, Spong CY.Williams Obstetrics, 23rd Edition. New
York: McGraw-Hill, 2010. Copyright 2010 The McGraw-Hill Companies,
Inc.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
22/23
Periods of sensitivity during development
Reproduced with permission from: Unborn Patient: Prenatal
Diagnosis and Treatment.Harrison, Golbus, Filly (eds).
Philadelphia, Saunders, 1990. p. 44. Copyright 1990 Elsevier.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...
e 23 02/12/2013 04:43
-
8/13/2019 Bipolar disorder in women - Preconception and prenatal
maintenance pharmacotherapy.pdf
23/23
The developing fetus
Reproduced with permission from: Moore, K. The developing human:
Clinically orientedembryology, WB Saunders, Philadelphia 1982.
Copyright 1982 Elsevier.
olar disorder in women: Preconception and prenatal maintenance
p...
http://www.uptodate.com/contents/bipolar-disorder-in-women-preconce...