Embed Size (px)
Citation preview

Bipolar Disorders - Bipolar Disorders - 20072007
Ronald A. Remick, MD, Ronald A. Remick, MD, FRCP(C)FRCP(C)
Consultant Psychiatrist Consultant Psychiatrist
Member, Board of Member, Board of Directors, MDADirectors, MDA
Phone : 604-682-2344 ext Phone : 604-682-2344 ext 6212162121
Email : [email protected] : [email protected]

EpidemiologyEpidemiology 1. Lifetime prevalence :1. Lifetime prevalence :
bipolar I : 0.8%bipolar I : 0.8%
bipolar II : 0.6% (Murphy, 2000)bipolar II : 0.6% (Murphy, 2000)
2. Bipolar disorder is the 62. Bipolar disorder is the 6thth leading leading cause ofcause of
disability, ages 15-44, worldwide…disability, ages 15-44, worldwide…
depression is 2depression is 2ndnd!!
3. At any given point in time, 60% of3. At any given point in time, 60% of
bipolars are not in treatmentbipolars are not in treatment

Mood Disorders and the Mood Disorders and the Workplace Workplace (new data)(new data)
30% of disability claims in Canada 30% of disability claims in Canada ($15-30 billion annually) due to ($15-30 billion annually) due to mood disorders (second only to mood disorders (second only to cardiovascular disease)…and cardiovascular disease)…and increasing!increasing!

Mood Disorders and the Mood Disorders and the Workplace Workplace (new data)(new data)
AbsenteeismAbsenteeism vs vs PresenteeismPresenteeismPresenteeismPresenteeism (lost productivity while at (lost productivity while at
work) – likely a more significant problem work) – likely a more significant problem with mood disorders than previously with mood disorders than previously recognized in Canadarecognized in Canada
Productivity loss from presenteeism due Productivity loss from presenteeism due to depression is 4 hours/week while loss to depression is 4 hours/week while loss from absenteeism is but 1 hour/week from absenteeism is but 1 hour/week (between $6-60 billion loss per annum)!(between $6-60 billion loss per annum)!

EpidemiologyEpidemiology1. Course of bipolar I is 9-10 cycles 1. Course of bipolar I is 9-10 cycles
during a lifetime – often stabilizing during a lifetime – often stabilizing after 4-5 cyclesafter 4-5 cycles
2. Without treatment – average 2. Without treatment – average depressive episode is 10 weeks, depressive episode is 10 weeks, average manic episode is 5 weeksaverage manic episode is 5 weeks
3. Sixty percent of patients have an 3. Sixty percent of patients have an increase in episode intensity/duration increase in episode intensity/duration with agewith age

What about the role of What about the role of ‘stress’ in bipolar illness?‘stress’ in bipolar illness?
1. 1. Disruption in sleep, but not Disruption in sleep, but not ‘stress’ per se can lead to a ‘stress’ per se can lead to a bipolar relapse.bipolar relapse.
2. Early childhood ‘trauma’ is 2. Early childhood ‘trauma’ is NOTNOT causative in bipolar illness. causative in bipolar illness. However,However,
a. a. sexual abusesexual abuse – may increase – may increase risk of suicide attemptsrisk of suicide attempts
b. b. physical abusephysical abuse – may increase – may increase risk of manic relapsesrisk of manic relapses
c. c. sexual/physical abusesexual/physical abuse – may – may lead to earlier illness onsetlead to earlier illness onset

Genetics of Bipolar Genetics of Bipolar IllnessIllness
1. Polygenic inheritance. Fifty 1. Polygenic inheritance. Fifty percent of bipolar patients have a percent of bipolar patients have a family history of bipolar illness.family history of bipolar illness.
2. Linkage studies (in several 2. Linkage studies (in several studies) have identified markers studies) have identified markers on chromosome 18 &22.on chromosome 18 &22.
3. Near future is identifying 3. Near future is identifying individuals at risk; long term individuals at risk; long term future – superior treatments. future – superior treatments.

Evolving genetic conceptsEvolving genetic concepts(new data)(new data)
1. 1. endophenotypesendophenotypes are gene are gene intermediaries that turn on or turn off a intermediaries that turn on or turn off a specific genespecific gene
2. “Stress/adversity’ can influence 2. “Stress/adversity’ can influence endophenotypes. That is, stress or endophenotypes. That is, stress or adversity can turn on or turn off certain adversity can turn on or turn off certain genes that can either trigger depression genes that can either trigger depression ((vulnerabilityvulnerability) or protect from ) or protect from depression (depression (resiliencyresiliency))

STRESS and the BRAINSTRESS and the BRAIN(new data)(new data)
CRFCRF
ACTHACTH
adrenalineadrenaline
cAMPcAMP
BDNFBDNF
brain cell growthbrain cell growth

STRESS and the BRAINSTRESS and the BRAIN (new data)(new data) CRFCRF
ACTHACTH
adrenalineadrenaline STRESSSTRESS
cAMPcAMP
BDNFBDNF
brain cell growthbrain cell growth

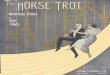
STRESS
Cortisol + Adrenaline
Limbic System
Hypothalamus
Pituitary
Adrenal Cortex
CRF
ACTHApoptosis/neuron death
HippocampalShrinkage Memory impairment
Mood dysregulation

DIAGNOSING BIPOLAR DIAGNOSING BIPOLAR DISORDERSDISORDERS

Diagnosis of depressionDiagnosis of depression
11.. A distinct mood change (depressed, A distinct mood change (depressed, irritable, anxious, etc) for at least irritable, anxious, etc) for at least two weekstwo weeks
2. Four or more 2. Four or more SIGECAPSSIGECAPS : :
SS leep leep CC oncentration oncentration
II nterest nterest A A ppetiteppetite
GG uilt uilt PP sychomotor activity sychomotor activity
EE nergy nergy S S uicide uicide

Diagnosis of mania/hypomaniaDiagnosis of mania/hypomania
1. A distinct mood change (elated, 1. A distinct mood change (elated, irritable, expansive, etc) for > one irritable, expansive, etc) for > one week (four days for hypomania)week (four days for hypomania)
2. Three or more 2. Three or more GST RAIDGST RAID : : GG randiosity randiosity RR apid thoughts apid thoughts SS leep(decreased) leep(decreased) AA gitation gitation TT alkative alkative II mpaired mpaired
judgementjudgement DD istractible istractible

Diagnosing bipolar illnessDiagnosing bipolar illness
1. Distinguish bipolar I (mania) from 1. Distinguish bipolar I (mania) from bipolarbipolar
II (hypomania)II (hypomania)
2. 2. ******Bipolar II is among the most Bipolar II is among the most frequentlyfrequently
missed diagnoses in psychiatrymissed diagnoses in psychiatry******
3. The diagnosis of bipolar II disorder is3. The diagnosis of bipolar II disorder is
risky, at best, without collateralrisky, at best, without collateral
information.information.



Diagnosis of hypomaniaDiagnosis of hypomania Doctors often fail to ask key questions Doctors often fail to ask key questions (*of a(*of a
family member and the patient)family member and the patient) that assist that assist in the diagnosis of bipolar II disorder :in the diagnosis of bipolar II disorder :
“ “ Has there been a period of time when you Has there been a period of time when you were feeling so good or hyper that other were feeling so good or hyper that other people thought you were not your normal people thought you were not your normal self, or were so hyper you got into self, or were so hyper you got into trouble?”trouble?”
“ “ What about a period of time when you What about a period of time when you were so irritable that you would shout at were so irritable that you would shout at people or start fights or arguments?”people or start fights or arguments?”

Treatment of Bipolar Treatment of Bipolar DisordersDisorders

Treatment of Bipolar Treatment of Bipolar DisordersDisorders
11. Bipolar disorder is a chronic illness:. Bipolar disorder is a chronic illness: a) Expect exacerbations and a) Expect exacerbations and
remissionsremissions b) Long term chemotherapy is the b) Long term chemotherapy is the
rule not the exceptionrule not the exception 2. It is risky, at best, to treat bipolar 2. It is risky, at best, to treat bipolar
patients in a vacuum i.e. without the patients in a vacuum i.e. without the involvement of family/significant othersinvolvement of family/significant others

Treatment of bipolar Treatment of bipolar illnessillness
1. PSYCHOLOGICAL 1. PSYCHOLOGICAL
INTERVENTIONSINTERVENTIONS
2. BIOLOGICAL 2. BIOLOGICAL INTERVENTIONSINTERVENTIONS

Treatment of bipolar Treatment of bipolar illnessillness
PSYCHOLOGICAL TREATMENTSPSYCHOLOGICAL TREATMENTS1. Psycho education :1. Psycho education : a. Mood Disorders Assoc of British a. Mood Disorders Assoc of British
ColumbiaColumbia b. internet/ readings, etcb. internet/ readings, etc2. Psychotherapy :2. Psychotherapy : a. Cognitive Behavioral Therapy (CBT) for a. Cognitive Behavioral Therapy (CBT) for
the depressive phase of illnessthe depressive phase of illness b. Cognitive Behavioral Therapy (CBT) to b. Cognitive Behavioral Therapy (CBT) to
prevent manic relapsesprevent manic relapses

Cognitive Behavioral Cognitive Behavioral Therapy (CBT)Therapy (CBT)
1. The evidence based 1. The evidence based psychotherapies (CBT – cognitive psychotherapies (CBT – cognitive behavioral therapy) are AS behavioral therapy) are AS EFFECTIVE as antidepressants in EFFECTIVE as antidepressants in mild/moderate MDD. mild/moderate MDD.
2. Cognitive therapy (CBT) is 2. Cognitive therapy (CBT) is accessible in British Columbia. accessible in British Columbia.

Cognitive Behavioral Cognitive Behavioral TherapyTherapy
CBT response rate(8-12 weekly CBT response rate(8-12 weekly sessions) – 65%sessions) – 65%
Core featuresCore features::
a. identify automatic maladaptive a. identify automatic maladaptive thoughts and distorted beliefs that thoughts and distorted beliefs that lead to depressive moodslead to depressive moods
b. learn strategies to modify these b. learn strategies to modify these beliefs and practice adaptive beliefs and practice adaptive thinking patternsthinking patterns
c. use a systematic approach to c. use a systematic approach to reinforce positive coping behaviorsreinforce positive coping behaviors

Cognitive Behavioral Cognitive Behavioral Therapy Therapy
CBT is accessible:CBT is accessible:
a. private psychologist (not covered by medicala. private psychologist (not covered by medical
insurance)insurance)
b. Changeways (www.changeways.com) - a b. Changeways (www.changeways.com) - a
group based CBT program offered at manygroup based CBT program offered at many
hospitals/mental health centers throughouthospitals/mental health centers throughout
BC (free – covered by medical insurance)BC (free – covered by medical insurance)
c. www.carmha.ca/publications - ‘anti-c. www.carmha.ca/publications - ‘anti-
depressant skills workbook’ (free download)-depressant skills workbook’ (free download)-
an outstanding self directed CBT workbookan outstanding self directed CBT workbook

Biological Treatments for bipolar Biological Treatments for bipolar disordersdisorders
1. LITHIUM1. LITHIUM
2. VALPROIC ACID2. VALPROIC ACID
3. CARBAMAZEPINE3. CARBAMAZEPINE
4. LAMOTROGINE4. LAMOTROGINE
5. ATYPICAL ANTIPSYCHOTICS5. ATYPICAL ANTIPSYCHOTICS
6. ANTIDEPRESSANTS6. ANTIDEPRESSANTS
7. OTHER ANTICONVULSANTS7. OTHER ANTICONVULSANTS

LithiumLithium** – wherefore – wherefore art thou?art thou?**old, old data!old, old data!

LithiumLithium1. Expect “two thirds” response to lithium:1. Expect “two thirds” response to lithium:
33% - complete response33% - complete response
33% - significant mood 33% - significant mood
attenuationattenuation
33% - no response/intolerance33% - no response/intolerance
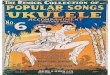
2. “anti-suicide” effect of lithium2. “anti-suicide” effect of lithium
3. lithium remains the ‘gold standard’ in 3. lithium remains the ‘gold standard’ in treating bipolar illness and is among the treating bipolar illness and is among the most effective and underutilized most effective and underutilized treatments in all of psychiatry! treatments in all of psychiatry!

Suicide attempts before, during, one year, Suicide attempts before, during, one year,
and two years post lithium treatmentand two years post lithium treatment
0
10
20
30
40
50
60
70
80

Valproic AcidValproic Acid
1. Valproic acid (divalproex; Depokoate; 1. Valproic acid (divalproex; Depokoate; Epival) is an effective antimanic agentEpival) is an effective antimanic agent
2. The evidence for the prophylactic efficacy 2. The evidence for the prophylactic efficacy of valproic is still not clear (one short RCT, of valproic is still not clear (one short RCT, pharmaceutical company sponsored)pharmaceutical company sponsored)
3. Valproic is far superior as an anti manic 3. Valproic is far superior as an anti manic rather than an antidepressant preventative rather than an antidepressant preventative agentagent
4. Serum levels appropriate (versus no 4. Serum levels appropriate (versus no defined therapeutic range with defined therapeutic range with carbamazepine)carbamazepine)

CarbamazepineCarbamazepine 1. Carbamazepine (Tegretol) is an effective 1. Carbamazepine (Tegretol) is an effective
antimanic agent (19 studies)antimanic agent (19 studies)
2. Carbamazepine is an effective prophylactic 2. Carbamazepine is an effective prophylactic agent (10 RCTs), but likely less effective than agent (10 RCTs), but likely less effective than lithium (Davis et al, 1999)lithium (Davis et al, 1999)
3. Carbamazepine appears to be a forgotten (yet 3. Carbamazepine appears to be a forgotten (yet very effective) treatment in bipolar illnessvery effective) treatment in bipolar illness
4. Oxcarbazepine (Trileptil) is being touted as a 4. Oxcarbazepine (Trileptil) is being touted as a ‘similar’ but ‘superior’ medication to ‘similar’ but ‘superior’ medication to carbamazepine, but recent studies shed some carbamazepine, but recent studies shed some doubtdoubt

Lamotrogine (Lamictal)Lamotrogine (Lamictal)
1. There is increasing evidence that 1. There is increasing evidence that lamotrogine is an effective agent in lamotrogine is an effective agent in treating both bipolar I and II depression.treating both bipolar I and II depression.
2. There is very limited (but some) 2. There is very limited (but some) evidence that lamotrogine is an effective evidence that lamotrogine is an effective anti-manic or prophylactic agent.anti-manic or prophylactic agent.
3. Lamotrogine has a relatively benign 3. Lamotrogine has a relatively benign (e.g. non sedative, weight neutral) side (e.g. non sedative, weight neutral) side effect profile. Dose range not effect profile. Dose range not determined but likely 100-300mg/daydetermined but likely 100-300mg/day

Other anticonvulsants in Other anticonvulsants in bipolar disorderbipolar disorder
There is There is NO NO evidence that evidence that gabapentin (Neurontin) or gabapentin (Neurontin) or topiramate (Topramax) has any topiramate (Topramax) has any benefit benefit at allat all in the treatment of in the treatment of bipolar depression, bipolar bipolar depression, bipolar mania, and/or the mania, and/or the preventative/prophylactic preventative/prophylactic treatment of bipolar illnesstreatment of bipolar illness

Typical/Atypical Typical/Atypical AntipsychoticsAntipsychotics
1. All are effective in mania. Limited 1. All are effective in mania. Limited evidence for effectiveness in prophylaxis or evidence for effectiveness in prophylaxis or in depressive episodes.in depressive episodes.
2. All atypical antipsychotic research is 2. All atypical antipsychotic research is pharmaceutical industry sponsored .pharmaceutical industry sponsored .
3. Significant concerns about weight gain, 3. Significant concerns about weight gain, dyslipidemia, & diabetes with atypicals; dyslipidemia, & diabetes with atypicals; especially olanzapine(Zyprexa) and especially olanzapine(Zyprexa) and clozapine(Clozaril) but alsoclozapine(Clozaril) but also risperidone(Risperdol) and quetiapine risperidone(Risperdol) and quetiapine (Seroquel)(Seroquel)

Medical Co-Morbidity and Life Medical Co-Morbidity and Life ExpectancyExpectancy
1.Individuals with schizophrenia and 1.Individuals with schizophrenia and affective disorders have increased risk of affective disorders have increased risk of death from medical causes and a shorter death from medical causes and a shorter lifespanlifespan
2.Comparing mortality in public mental 2.Comparing mortality in public mental health clinics in the USA with the general health clinics in the USA with the general population (1997-2000), patients lost population (1997-2000), patients lost decades of potential years of life (average decades of potential years of life (average 25 years)25 years)

Medical Co-Morbidity and Life Medical Co-Morbidity and Life Expectancy(cont)Expectancy(cont)
3. As in the general population the main 3. As in the general population the main cause of death is coronary heart disease cause of death is coronary heart disease (CHD), but to an even greater extent(CHD), but to an even greater extent
4. Cardiovascular standardized mortality 4. Cardiovascular standardized mortality rate in schizophrenia is approximately 2X rate in schizophrenia is approximately 2X the general population (2.3 in males and the general population (2.3 in males and 2.1 in females) Patients with both unipolar 2.1 in females) Patients with both unipolar and bipolar disorder also have increased and bipolar disorder also have increased mortality from CHDmortality from CHD

Cardiac/Metabolic Co-morbidityCardiac/Metabolic Co-morbidityHealth DeterminantsHealth Determinants
MedicationMedicationWeight gainWeight gainDiabetes/lipidsDiabetes/lipidsMetabolic Metabolic syndromesyndrome
Cardiac effectsCardiac effects
Patient FactorsPatient FactorsFailure to recognize Failure to recognize
illnessillnessRefusal of treatmentRefusal of treatmentNon-adherence with Non-adherence with
treatmenttreatment
LifestyleLifestyleSmokingSmokingSubstance abuseSubstance abuseDiet, exerciseDiet, exercisePovertyPoverty
Systemic FactorsSystemic FactorsLimited attention to medical Limited attention to medical
carecareSeparation of psychiatric Separation of psychiatric
and mental health careand mental health care““Falling between the Falling between the
cracks”cracks”

LifestyleLifestyleThe diet of individuals with SMI(Serious Mental The diet of individuals with SMI(Serious Mental
Illness) has been characterized as high fat,Illness) has been characterized as high fat, high in calories and high in simple high in calories and high in simple carbohydratescarbohydrates
Patients with SMI are less active then those in Patients with SMI are less active then those in the general population and are more likely to the general population and are more likely to walk as their sole form of physical activitywalk as their sole form of physical activity
Smoking rates are elevated in the SMI and range Smoking rates are elevated in the SMI and range between 32% and 92% in schizophrenia between 32% and 92% in schizophrenia samplessamples

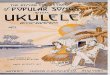
Metabolic Abnormalities Metabolic Abnormalities with Atypical Antipsychoticswith Atypical Antipsychotics
DrugDrug Weight Weight GainGain DiabetesDiabetes LipidsLipids
ClozapineClozapine ++++++ ++ ++
OlanzapineOlanzapine ++++++ ++ ++
RisperidonRisperidonee
++++ DiscrepantDiscrepant DiscrepantDiscrepant
QuetiapineQuetiapine ++++ DiscrepantDiscrepant DiscrepantDiscrepant
ZiprasidonZiprasidonee
+/-+/- __ __
AripiprazolAripiprazolee
+/-+/- __ __

Typical/Atypical Typical/Atypical AntipsychoticsAntipsychotics
1. All are effective in mania. Limited 1. All are effective in mania. Limited evidence for effectiveness in prophylaxis or evidence for effectiveness in prophylaxis or in depressive episodes.in depressive episodes.
2. All atypical antipsychotic research is 2. All atypical antipsychotic research is pharmaceutical industry sponsored .pharmaceutical industry sponsored .
3. Significant concerns about weight gain, 3. Significant concerns about weight gain, dyslipidemia, & diabetes with atypicals; dyslipidemia, & diabetes with atypicals; especially olanzapine(Zyprexa) and especially olanzapine(Zyprexa) and clozapine(Clozaril) but alsoclozapine(Clozaril) but also risperidone(Risperdol) and quetiapine risperidone(Risperdol) and quetiapine (Seroquel)(Seroquel)

Do not rashly use every new product of which the Do not rashly use every new product of which the peripatetic siren sings. Consider what surprising peripatetic siren sings. Consider what surprising reactions may occur in the laboratory from the reactions may occur in the laboratory from the careless mixing of unknown substances. Be as careless mixing of unknown substances. Be as considerate of your patient and yourself as you considerate of your patient and yourself as you are of the test tube.are of the test tube.
- Sir William Osler- Sir William Osler

Managing Managing depressive and depressive and manic relapsesmanic relapses

Managing depressive Managing depressive and manic relapsesand manic relapses
““don’t throw out the baby don’t throw out the baby with the bathwater”with the bathwater”


Managing Depressive Managing Depressive RelapseRelapse
1. Don’t throw out the baby with the 1. Don’t throw out the baby with the bathwater!bathwater!
2. The risk of an antidepressant induced 2. The risk of an antidepressant induced manic manic
switch in both bipolar I/II is < 10%switch in both bipolar I/II is < 10%
3. Treatment options:3. Treatment options:
a. second mood stabilizer (I), especially a. second mood stabilizer (I), especially lamotroginelamotrogine
b. antidepressant (II,I)/lamotrogineb. antidepressant (II,I)/lamotrogine
c. CBT(I,II)c. CBT(I,II)
d. ECT(I,II)d. ECT(I,II)



Managing Managing Manic/Hypomanic Manic/Hypomanic
RelapseRelapse1. Don’t throw out the baby with the bath 1. Don’t throw out the baby with the bath
water.water.
2. Other treatment options :2. Other treatment options :
a. hospital care (I)a. hospital care (I)
b. no treatment intervention (II)b. no treatment intervention (II)
c. second mood stabilizer (I/II)c. second mood stabilizer (I/II)
d. atypical /typical antipsychotic (I/II)d. atypical /typical antipsychotic (I/II)
e. benzodiazepine (II)e. benzodiazepine (II)
f. ECT (I)f. ECT (I)

Prevention of future Prevention of future manic relapses – manic relapses –
Ulysses AgreementUlysses Agreement1. Set it up BEFORE manic relapse 1. Set it up BEFORE manic relapse
with doctors, family, employers, with doctors, family, employers, etc.etc.
2. Put it in writing…outline the 2. Put it in writing…outline the type of treatment e.g. type of treatment e.g. hospitalization, antipsychotic hospitalization, antipsychotic medication, etc.medication, etc.

““Grey zones” in bipolar Grey zones” in bipolar illness…or topics for future illness…or topics for future
presentationspresentations 1.“Stressful life problems” versus mild 1.“Stressful life problems” versus mild
depressive relapsedepressive relapse
2. The role of psychological “adversity” in 2. The role of psychological “adversity” in bipolar illnessbipolar illness
3.. To treat or not treat hypomania3.. To treat or not treat hypomania
4. Social/family/vocational stigma4. Social/family/vocational stigma
5. “ Doctor should we have children?”5. “ Doctor should we have children?”
6. Bipolar illness and creativity6. Bipolar illness and creativity

What’s the deal with childhood What’s the deal with childhood bipolar illness?bipolar illness? (*new data)(*new data)
1. The onset in bipolar illness can be in 1. The onset in bipolar illness can be in late adolescence, particularly in late adolescence, particularly in children of bipolar parents.children of bipolar parents.
2. The diagnosis of childhood bipolar 2. The diagnosis of childhood bipolar illness (i.e. ages 5-15)is very different in illness (i.e. ages 5-15)is very different in USA compared to Canada, where USA compared to Canada, where childhood bipolar illness is virtually childhood bipolar illness is virtually nonexistent.nonexistent.

What’s the deal with childhood What’s the deal with childhood bipolar illness?bipolar illness?
3. In Canada, the onset of bipolar illness 3. In Canada, the onset of bipolar illness typically begins with a lengthy depressive typically begins with a lengthy depressive episode.episode.
4. In the USA, children with mood 4. In the USA, children with mood lability/irritability, anxiety and insomnia are lability/irritability, anxiety and insomnia are often given a diagnosis of childhood bipolar often given a diagnosis of childhood bipolar illness.illness.
5. The USA position is not consistent with 5. The USA position is not consistent with decades of age of onset research, genetic decades of age of onset research, genetic studies, or current diagnostic criteria for studies, or current diagnostic criteria for bipolar disorders.bipolar disorders.

““Doctor, should we have children?”Doctor, should we have children?”1. The risks are real, but small (2% versus 1. The risks are real, but small (2% versus
15%).15%).
2. Illness severity is not related to the 2. Illness severity is not related to the severity of the illness in the family.severity of the illness in the family.
3. Illness onset is at least twenty years in the 3. Illness onset is at least twenty years in the future with extensive new develop- ments future with extensive new develop- ments and treatments on the way.and treatments on the way.
4. Bipolar illness, without any other risk 4. Bipolar illness, without any other risk factors, in a parent is certainly not an factors, in a parent is certainly not an exclusion to having and effectively exclusion to having and effectively parenting children.parenting children.

The relationship between The relationship between creativity and bipolar illnesscreativity and bipolar illness
1. Many studies have shown that 1. Many studies have shown that between 20 and 35% of artists between 20 and 35% of artists (musicians, painters, writers, poets, (musicians, painters, writers, poets, etc) develop bipolar illness where the etc) develop bipolar illness where the rate of bipolar illness in the population rate of bipolar illness in the population is about 2%.is about 2%.
2. The higher rate of bipolar illness 2. The higher rate of bipolar illness cannot be explained by ‘stressful’ life cannot be explained by ‘stressful’ life style, poverty, etc.style, poverty, etc.

The relationship between The relationship between creativity and bipolar illnesscreativity and bipolar illness
3. Severe manic and depressive episodes 3. Severe manic and depressive episodes impair creative output.impair creative output.
4. Creativity and bipolar illness have a 4. Creativity and bipolar illness have a familial (i.e. genetic) link.familial (i.e. genetic) link.
5. Touched with Fire : Manic Depressive 5. Touched with Fire : Manic Depressive Illness and the Artistic Temperment. by Illness and the Artistic Temperment. by Kay Redfield Jamieson (1993)Kay Redfield Jamieson (1993)